Embed Size (px)
Citation preview

Dysmotility of the small intestine in achalasia
T. SCHMIDT, A. PFEIFFER, N. HACKELSBERGER, R. WIDMER, C. PEHL & H. KAESS
Department of Gastroenterology and Hepatology, StaÈdtisches Krankenhaus MuÈ nchen-Bogenhausen,
Akademisches Lehrkrankenhaus, Englschalkingerstrasse 77, D-81925 Munich, Germany
Summary During recent years there has been in-
creasing evidence for extraoesophageal dysfunction in
achalasia. The aim was to investigate whether motil-
ity of the small intestine is abnormal in achalasia.
Thirteen patients (eight men, ®ve women) aged 52 (33±
85) years were studied. They had all previously un-
dergone treatment with pneumatic balloon dilatation
and were free of dysphagia when examined. Ambula-
tory 24-h motility was recorded in the upper jejunum
under standardized caloric intake with a digital da-
talogger and catheter-mounted pressure transducers
located beyond the ligament of Treitz. Visual analysis
was performed by two observers and data underwent
quantitative analysis of phasic contractile events
using a computer program. Normal values were ob-
tained from 50 healthy controls. In the fasting state, a
complete loss of cyclic MMC activity (n � 2), an ab-
normally prolonged phase II (n � 2) and disturbances
in the aboral migration of phase III (n � 5) were ob-
served. Postprandial motor response was absent
(n � 2) or frequently showed a contraction frequency
below the normal range (n � 5). Further abnormali-
ties consisted in hypomotility during phase II (n � 3)
and in a reduced frequency of migrating clustered
contractions in the fasting (n � 2) or postprandial
state (n � 2). In addition, motor events not present in
any healthy subject, giant migrating contractions
(n � 5), retrograde clustered contractions (n � 6) and
repetitive retrograde contractions (n � 3) were iden-
ti®ed. Each patient exhibited ®ndings out of the range
of normal. Dysmotility of the proximal small intestine
is present in achalasia.
Keywords achalasia, small bowel manometry, small
bowel motility.
INTRODUCTION
Achalasia is a motor disorder of the oesophagus char-
acterized by a loss of peristaltic activity of the tubular
oesophagus and by a defective relaxation of an often
hypertensive lower oesophageal sphincter.1 Whatever
the pathogenetic process, it has long been assumed to
be con®ned to the oesophagus. However, in recent
years, there has been increasing evidence for extra-
oesophageal dysfunction in achalasia involving the
stomach,2±5 the gallbladder,3 the sphincter of Oddi6
and the autonomic nervous system.7,8 Abnormal small
bowel motility with a reduced occurrence and a dis-
turbed aboral migration of phase III of the migrating
motor complex (MMC) has been observed during 4-h
recordings with stationary perfused-tube manometry.9
In the last decade, the application of ambulatory long-
term manometry10±12 has resulted in a better under-
standing of the enormous variability of human small
bowel motility, and long-term recordings may allow
the MMC to be better characterized.13,14 Postprandial
motility has, to our knowledge, not been investigated
in achalasia. Therefore, the aim of the present study
was to study fasting and digestive motility in patients
with achalasia by ambulatory 24-h manometry.
MATERIALS AND METHODS
Patients and controls
The achalasia group comprised 13 patients (eight men,
®ve women) aged 52 (33±85) years. The mean duration
of the disease was 3 years, with a range from 3 months
to 20 years. The diagnosis of achalasia was made in all
patients by upper gastrointestinal radiology, endoscopy
and oesophageal manometry. All patients had been
treated with pneumatic dilatation (1±3 sessions) before
the motility studies. According to Vantrappen &
Hellemans,15 the clinical result was classi®ed as good
in ®ve patients or excellent in eight patients, respec-
tively. A barium swallow performed before the motil-
ity study did not reveal oesophageal retention. All
Address for correspondenceDr Thomas Schmidt, Department of Gastroenterology, Hos-pital Bogenhausen, Englschalkingerstrasse 77, D-81925 Mu-nich, Germany. Tel: 049 89 92702061; fax: 049 89 92702486.Received: 11 June 1997Accepted for publication: 4 August 1998
Neurogastroenterol. Mot. (1999) 11, 11±17
Ó 1999 Blackwell Science Ltd 11

patients were free of gastrointestinal symptoms when
studied. Except small bowel manometry, no extra-
oesophageal motility studies or autonomic function
tests were performed. No patient was taking any
medication known to affect gastrointestinal motility,
and no history of diabetes mellitus, neuropathy or
malignancy was present. Normal values for jejunal
motility were obtained in 50 healthy volunteers (28
men, 22 women), aged 26 (19±46) years. All controls
were `tube-naive' and were studied according to the
same protocol as reported previously.16,17
The study protocol was approved by the local ethics
committee and was in accordance with the updated
Declaration of Helsinki. Informed consent was ob-
tained from each subject.
Study protocol
After an overnight fast, intubation of the small intes-
tine was performed transnasally on day I. Using ¯uo-
roscopic control the recording catheter was positioned
with its proximal sensor at the ligament of Treitz.18
Subjects were ambulatory, and physical activity was
not restricted. Activities were documented in a diary.
At 18:00 h a standardized evening meal was ingested
consisting of bread, cheese, sausages and fruit yoghurt
(600 kcal; 40% proteins, 40% carbohydrate, 20% fat).
Intake of tap water was allowed ad libitum. Day II was
spent fasting, until manometry was stopped after a
total recording period of 24 h.
Digital recording system
Intraluminal pressure was recorded with two piezo-
resistive strain gauge transducers spaced at 15-cm in-
tervals in the distal part of a ¯exible polyurethane
catheter (OD 2.3 mm, Keller AG, Winterthur, Swit-
zerland). A catheter with six transducers spaced at 3-
cm intervals was used in three patients and 20 con-
trols, respectively. Calibration of the catheters was
performed in a water bath at 37 °C for 30 min before
each measurement. Pressure data were sampled from
each sensor at a rate of 3 Hz and were stored on a 2-
MByte portable data logger (PMT Megalogger, Dr Ul-
rich Hoppe, GoÈ ttingen, Germany).
Data analysis
Data were downloaded to a personal computer (486 DX
2, ESCOM Computers, Munich, Germany) without
any reduction. Both visual and computer-aided analysis
were undertaken. All visual analysis steps were per-
formed independently by two observers. For automated
analysis, a computer program described in detail else-
where19 was used.
According to the subject's diary, each recording pe-
riod was subdivided into a diurnal and a nocturnal
period (usually from 23:00 to 06:00 h) reference to the
waking (W) or sleeping (S) state of the subject and
marked by mouse operation as regions of interest. In a
similar way, fasting motility, its constituent phases
and postprandial activity were marked and stored on
separate computer ®les. Fasting motility was subdi-
vided into three phases.20 Phase I was de®ned as motor
quiescence.20 Phase II (irregular contractile activity)
was de®ned to start when the contractile activity at
any recording site exceeded more than two phasic
contractions per 10 min.21 Phase III was de®ned as a
rhythmic series of uninterrupted contractions at a
maximal rate of 10±12 min)1 and a duration of more
than 2 min followed by motor quiescence.20 Aboral
migration velocity phase III was determined visually by
dividing the length of the recording segment (15 cm) by
the time taken for the onset of phase III to traverse this
distance.20 MMC cycle length was de®ned as the time
period between the end of successive phase III activi-
ties at the distal recording site. Incomplete MMC cy-
cles were excluded from data analysis. Postprandial
motility was de®ned as the time period from the be-
ginning of the meal to the return of either phase III or
phase I.12
Phase II, III and postprandial contractile activity
underwent rejection of artefacts and quantitative au-
tomated analysis of contractions.19 Brie¯y, phasic
pressure events exceeding an amplitude of 9.7 mmHg,
a duration of 2.8 sec and an area under the curve of
18.4 sec ´ mmHg were considered by the algorithm as
a real contraction. From the data ®les of recognized
contractions, the mean values for contraction fre-
quency (min±1) and contraction amplitude (mmHg)
were calculated.
Finally, phase II and postprandial motility were
screened visually on separate occasions by two ob-
servers for special motor patterns, migrating clustered
contractions (MCCs), retrograde clustered contractions
(RCCs), giant migrating contractions (GMCs) and re-
petitive retrograde contractions. The observers used
the following de®nitions, and only motor events rec-
ognized by both observers were included in the data
analysis. A MCC was de®ned as a rhythmic series of 3±
10 phasic contractions occurring at a frequency of 10±
12 min)1 22 preceded and followed by at least 30 sec of
absent motor activity12 and showing aboral migration
through the whole recording segment of 15 cm. RCCs
were de®ned as MCCs exhibiting migration in an oral
direction. A GMC was de®ned as a single contraction
12 Ó 1999 Blackwell Science Ltd
T. Schmidt et al. Neurogastroenterology and Motility

with a duration of more than 10 sec and an amplitude
of at least 30 mmHg.23 The frequency (per h of phase II
and fed activity, respectively) and migration velocity
(cm sec)1) of MCCs, RCCs and GMCs were calculated.
Repetitive retrograde contractions were de®ned as
groups of single contractions being retropropagated
over at least two recording sites. Only the recordings
with six closely spaced pressure tranducers were
screened for this motor event.
Statistical analysis
Results of visual and computerized analysis were en-
tered into a preprogrammed database (Paradox 1.0;
Borland International Inc., Scotts Valley, CA, USA) for
further statistical workup. The replicate observations
within an individual over the 24-h recording period
[for example the duration of several phase II(W) epi-
sodes] were ®rst averaged to obtain a mean value for
each parameter [a mean duration of phase II(W) for
that individual]. Results were expressed as mean (of
the means) � SEM unless otherwise stated. For com-
parisons, the independent two-sample t-test was ap-
plied. Differences were considered signi®cant at
P < 0.05. For each parameter, the total range of the
values obtained in healthy controls was de®ned as
normal motility.
RESULTS
Fasting motility
MMC cycle In two patients, no phase III activity was
identi®ed over the 24-h period, and only isolated ap-
parently irregular contractions were recorded. The data
characterizing the MMC activity in the remaining 11
patients are shown in Table 1. In the waking (W) and
sleeping (S) state, there was a trend towards a longer
mean MMC cycle length in the patient group caused by
an increased duration of phase II (P < 0.05). In two
patients, both the MMC(W) and the MMC(S) cycle
length exceeded the upper limit of controls due to a
prolonged phase II(W).
Phase II The parameters characterizing phasic con-
tractile activity during phase II are summarized in
Table 2. For the group of achalasia patients, the mean
values for phase II contraction frequency and for the
frequency of migrating clustered contractions (MCCs)
were lower compared with normal subjects (P < 0.05).
In one patient, phase II(W) and phase II(S) contraction
frequency were below the normal range. Two other
patients exhibited hypomotility only during phase
II(W) together with an abnormally low MCC frequen-
cy.
Phase III Phase III activities with an aboral migration
did not differ between patients and controls in terms of
contraction frequency, contraction amplitude and ab-
oral migration velocity. In ®ve patients, disturbed ab-
oral migration of phase III was found, affecting
44 � 15% (range 14±100%) of all phase III activities
over the 24-h period. In these individuals, phase III was
Table 1 Characteristics of the MMC cycles recorded in thewaking (W) and sleeping (S) state in achalasia patients withpreserved MMC activity (n = 11) and healthy controls (n = 50).Values are means � SEM; t-test.
Achalasia Controls
MMC(W)Cycle length [min] 126 � 14* 101 � 5Phase I [min] 12 � 4 16 � 2Phase II [min] 110 � 12* 81 � 5Phase III [min] 3.7 � 0.4 4.4 � 0.2
MMC(S)Cycle length [min] 103 � 4* 85 � 3Phase I [min] 46 � 8 46 � 3Phase II [min] 52 � 6* 34 � 3Phase III [min] 5.0 � 0.2 5.4 � 0.2
*P < 0.05 vs controls.
Table 2 Parameters of phase IIactivity recorded in the waking(W) and sleeping (S) state inachalasia patients with preservedMMC activity (n = 11) and heal-thy controls (n = 50). Values aremeans � SEM; t-test.
Achalasia Controls
Phase II(W)Contraction frequency [min)1] 1.4 � 0.3* 2.0 � 0.1Contraction amplitude [mmHg] 24.3 � 1.9 23.0 � 0.5Migrating Clustered Contractions [h)1] 4.5 � 0.7* 7.5 � 0.6
Phase II(S)Contraction frequency [min)1] 0.7 � 0.3* 1.3 � 0.1Contraction amplitude [mmHg] 25.1 � 1.6 24.1 � 1.0Migrating clustered contractions [h)1] 3.9 � 1.0* 6.2 � 0.6
*P < 0.05 vs controls.
Ó 1999 Blackwell Science Ltd 13
Volume 11, Number 1, February 1999 Jejunal motility in achalasia

either recorded simultaneously at adjacent recording
sites or exhibited a premature distal start and a si-
multaneous ending (Fig. 1).
Postprandial motility
The data on postprandial motility are summarized in
Table 3. After the standardized evening meal, both
patients with absent MMC activity did not show a
digestive motor response. For the group comprising the
remaining 11 patients, a reduced mean contraction
frequency (P < 0.001) was observed compared with
controls. In ®ve patients, the postprandial contraction
frequency was below the normal range.
In addition, the group of achalasics showed a ten-
dency towards a lower mean value for the occurrence
of MCCs compared with the mean value found in
controls (P < 0.05). In two patients, the MCC frequen-
cy was below the normal range.
The duration of digestive motility and the post-
prandial contraction amplitude were not different be-
tween patients and controls.
Special motor patterns
Motor events, not observed in any healthy subject,
were present during fasting and postprandial motility
in the patient group (Fig. 1). Giant migrating contrac-
tions were identi®ed in ®ve patients. They occurred
with a mean frequency (range) of 2.1 � 0.8 (0.2±7.0) h)1,
were characterized by an amplitude of 69 � 7 (48±
83) mmHg, a duration of 12.2 � 0.6 (11±14) sec and
were propagated aborally at a velocity of 4.3 � 0.7 (2.1±
6.0) cm sec)1. Six patients exhibited retrograde clus-
tered contractions. These clusters occurred with a fre-
quency of 1.9 � 0.6 (0.8±4.0) h)1 and showed migration
in an oral direction at a velocity of 1.3 � 0.3 (0.8±
2.3) cm sec)1. Repetitive retrograde contractions were
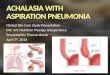
Figure 1 Upper tracings: disturbed aboral migration of phase III of the migrating motor complex in achalasia. Compressed view ofjejunal motility recordings obtained with two intraluminal pressure sensors located at the ligament of Treitz and 15 cm distally.Normal aboral migration of phase III in a healthy subject (left), simultaneous occurrence of phase III at both recording sites (middle)and premature distal start and simultaneous ending of phase III (right) in two achalasia patients. Lower tracings: expanded view offurther abnormal motor events in achalasia patients not present in any healthy subject. Motility was recorded with two intra-luminal pressure sensors at 15-cm intervals (left), and with six sensors at 3-cm intervals (middle and right tracing) distal to theligament of Treitz. Left: a giant migrating contraction, characterized by an increased amplitude and a prolonged duration comparedwith normal phasic small bowel contractions. Middle: clustered contractions with retrograde migration. Right: repetitive retro-grade contractions.
14 Ó 1999 Blackwell Science Ltd
T. Schmidt et al. Neurogastroenterology and Motility

seen in all three patients who had been studied with six
closely spaced pressure sensors. The pattern consisted
of groups of 2±10 single contractions separated by in-
tercontractile intervals ranging from 11 to 22 sec. Each
single contraction was retropropagated over 2±4 re-
cording sites (3±9 cm) at a mean velocity of 1.2 � 0.2
(0.7±2.3) cm sec)1. Over the 24-h period, 1±3 episodes
of this motor pattern were identi®ed.
Summary of abnormal manometric ®ndings
In our 13 achalasia patients, 37 ®ndings not present in
the control group were observed (number of patients):
absent MMC activity (n � 2), prolonged MMC cycle
length/phase II (n � 2), disturbed aboral migration of
phase III (n � 5), hypomotility (n � 3) and reduced
migrating clustered contractions in phase II (n � 2),
absent postprandial motor response (n � 2), hypomo-
tility (n � 5) and reduced migrating clustered con-
tractions (n � 2) during postprandial motility, giant
migrating contractions (n � 5), retrograde clustered
contractions (n � 6), repetitive retrograde contractions
(n � 3). Each patient had at least one of these motor
abnormalities (Table 4).
DISCUSSION
In achalasia, a well-de®ned motor disorder of the oeso-
phagus, evidence for extraoesophageal dysfunction is
accumulating. Morphological studies have shown
fragmentation of parasympathetic nerves as well as
degeneration of ®bres in the vagal trunc.24±26 Further-
more, a reduction of cells and neuronal depigmentation
in the dorsal motor nuclei of the vagus nerve have been
observed.27,28 Functional studies have demonstrated, at
least in some patients, a reduced gastric acid secretion
during sham feeding or insulin-induced hypo-
glycaemia,29±31 as well as an alteration of gastric
emptying consisting in a more rapid emptying of liq-
uids2,3 and a delayed emptying of solids.5 The biliary
system may be affected by impaired gallbladder con-
tractility3 and sphincter of Oddi hypertension.6 Finally,
autonomic function studies have provided evidence for
impairment in the sympathetic and parasympathetic
nervous system.7,8
On the motor activity of the small intestine, only very
few observations are available. In 1983, Erckenbrecht
et al.9 studied nine achalasia patients with stationary
short-term duodenojejunal manometry. In ®ve of these
pateints no phase III activity was recorded over a fasting
Table 3 Parameters of post-prandial motility in achalasia pa-tients with preserved digestivemotor response (n = 11) andhealthy controls (n = 50). Valuesare means � SEM; t-test.
Achalasia Controls
Duration of postprandial motility [min] 255 � 18 263 � 13Contraction frequency [min)1] 1.4 � 0.3** 3.1 � 0.2Contraction amplitude [mmHg] 23.7 � 1.0 23.7 � 0.5Migrating clustered contractions [h)1] 6.2 � 1.3* 10.8 � 0.9
**P < 0.001 vs controls; *P < 0.05 vs controls.
Table 4 Summary of abnormal manometric ®ndings in the group of 13 achalasia patients
Pt.No.
Absentphase IIIactivity
ProlongedMMCcyclelength
Disturbedmigrationof phaseIII
Phase IIhypomotility*
ReducedMCCs in phase II
Absentpostprandialmotorresponse
Postprandialhypomotility*
ReducedMCCspost-prandialy GMCsz RCCs§ RRCs±
1 + +2 + + +3 +4 +5 + +6 + + + +7 + + + +8 + + +9 + +
10 +11 + + + + +12 + + + + + +13 + + +
*Contraction frequency below the normal range; ymigrating clustered contractions; zgiant migrating contractions; §retrogradeclustered contractions; ±repetitive retrograde contractions.
Ó 1999 Blackwell Science Ltd 15
Volume 11, Number 1, February 1999 Jejunal motility in achalasia

period of 4 h, and four patients had activity fronts which
occurred simultaneously at the duodenal and the jejunal
level. In 1990, Kellow et al.32 reported on an achalasia
patient with chronic painless diarrhoea due to small
bowel bacterial overgrowth. In a 24-h fasting recording,
no MMCs were seen in the duodenum and jejunum.
Our data con®rm and extend these observations in
that there are at least some patients with achalasia in
whom phase III activity is completely absent and re-
placed by a motor activity of single irregular contrac-
tions similar to that seen in the previous case report.32
Other patients seem to have alterations of the normal
aboral migration of phase III, either with a simulta-
neous occurrence, as observed by Erckenbrecht et al.,9
or with a premature distal start.
Futhermore, quantitative computer-aided analysis of
individual small bowel contractions, not available in
the previous studies,9,32 demonstrated that hypomo-
tility during phase II can be present in some patients as
another feature of abnormal fasting motility.
Postprandial motility has, to our knowledge, not
been investigated in achalasia. Our two patients with
absent MMC activity had no motor response to the
ingested meal. Five of the remaining 11 patients (45%)
showed postprandial hypomotility compared with
controls. A reduced occurrence of migrating clustered
contractions, a highly coordinated physiological motor
pattern12,16 which provides mixing and aboral trans-
port of luminal contents,33 was an additional abnor-
mality in some patients in the digestive period and
during phase II. Oesophageal stasis is unlikely to ex-
plain postprandial hypomotility. Since gastric empty-
ing and autonomic function tests were not performed
in our patients, we cannot exclude that disturbed gas-
tric emptying of solids5 and dysfunction of extraoeso-
phageal vagal ®bres34,35 could play a role.
The site and nature of the lesion responsible for the
observed motor abnormalites are unclear at present. In a
histological study by light microscopy of transmural
biopsies,4 normal neuronal densities in the jejunal
Auerbach's plexus were found, in contrast to the well-
known depletion of ganglion cells in the distal oesoph-
agus.25 This ®nding, however, does not exclude the
presence of dysfunction. As the initiation and aboral
migration of phase III are products of the enteric nervous
system,36,37 the absent or reduced MMC activity and
disturbances of phase III migration point to a neuro-
pathic process at the level of the myenteric plexus.
Similar manometric observations have been made in
patients with neuropathic pseudo±obstruction syn-
dromes38,39 and it is well known that achalasia-like
oesophageal motor disorders can be a manifestation of
more widespread visceral neuropathies with clinically
apparent pseudo-obstruction syndromes.40±42 Two oth-
er abnormalities in our patients, postprandial hypomo-
tility and reduced MCC activity, also point to an
underlying neuropathic process, as they have recently
been identi®ed as manometric features of diabetic
neuropathy.43
Finally what could be the consequences of our ®nd-
ings? Clinically, nonoesophageal gastrointestinal
symptoms seem to be less frequent in achalasia than in
patients with other oesophageal contraction abnor-
malities,44 and no symptoms attributable to disturbed
small bowel function were present in our patients.
Whether small intestinal hypomotiliy during phase II
or the digestive period changes small intestinal transit
is unknown at present. Gastrocecal transit in the
fasting state, assessed by the H2 lactulose breath test,
has been reported to be not signi®cantly different from
healthy controls,2 and no postprandial transit studies
have, to our knowledge, been performed. Owing to its
housekeeping function,45 the absent MMC or a re-
duced MMC activity can be associated with bacterial
overgrowth of the small intestine,20,23,46 as in the pa-
tient described by Kellow et al.32 Data on the rela-
tionship between abnormal motility and changes of the
intestinal micro¯ora, which have recently been ob-
tained in radiation enteropathy,23 are not available in
achalasia at present.
In summary, jejunal motility in achalasia is charac-
terized by disturbed generation and impaired aboral
migration of phase III, postprandial hypomotility and
several other motor abnormalities. We conclude that
disturbed motor function in achalasia is not limited to
the oesophagus, but also can involve the small intestine.
REFERENCES
1 Castell DO. Achalasia and diffuse esophageal spasm. AnnInt Med 1976; 136: 571±9.
2 Eckardt VF, Krause J, Bolle D. Gastrointestinal transit andgastric acid secretion in patients with achalasia. Dig DisSci 1989; 34: 665±71.
3 Annese V, Caruso N, Accadia L, Gabrielli A, Modoni S,Frusciante V, Federici T. Gallbladder function and gastricliquid emptying in achalasia. Dig Dis Sci 1991; 36: 1116±20.
4 Csendes A, Smok G, Braghetto I, Gonzalez P, HenriquezCsendes P, Pizurno D. Histological studies of Auerbach'splexuses of the esophagus, stomach, jejunum and colon inpatients with achalasia of the esophagus: correlation withgastric acid secretion, presence of parietal cells and gastricemptying of solids. Gut 1992; 33: 150±4.
5 Benini L, Castellani G, Sembenni C, Bardelli Caliari S,Volino C, Vantini I. Gastric emptying of solid meals inachalasia patients after successful pneumatic dilatation ofthe cardia. Dig Dis Sci 1994; 39: 733±7.
6 Hagemueller F, Classen M. Motility of Oddi's sphincter inParkinson's disease, progressive systemic sclerosis andachalasia. Endoscopy 1988; 20: 189±92.
16 Ó 1999 Blackwell Science Ltd
T. Schmidt et al. Neurogastroenterology and Motility

7 Auer P, SoÈ llenboÈhmer C, Frieling T, Strohmeyer G, LuÈ bkeHJ. Impaired autonic function in patients with achalasia ofthe esophagus. Gastroenterology 1994; 106: A461 (abstract).
8 Eckardt VF, Stenner F, Liewen H, Koop H, Bernhard G.Autonome FunktionsstoÈ rung bei Patienten mit Achalasie.Neurogastroenterol Mot 1995; 7: 55±61.
9 Erckenbrecht JF, Berges W, Wienbeck M. InterdigestiveDuÈ nndarmmotilitaÈt bei Achalasie, Z Gastroenterol 1983;21: 429 (abstract).
10 Gill RC, Kellow JE, Wingate DL. The migrating motorcomplex at home. Gastroenterology 1987; 92: 1405 (ab-stract).
11 Lindberg G, Iwarzon M, Stal P, Seensalu R. Digital ambu-latory monitoring of small-bowel motility. Scand J Gas-troenterol 1990; 25: 216±24.
12 Husebye E, Skar A, Aalen O, Osnes M. Digital ambulatorymanometry of the small intestine in healthy adults. DigDis Sci 1990; 35: 1057±67.
13 Quigley EMM. Intestinal manometry ± technical advances,clinical limitations. Dig Dis Sci 1992; 37: 10±3.
14 Husebye E. Should interdigestive motility of small intes-tine be recorded by long-term ambulatory or short-termstationary manometry. Dig Dis Sci 1995; 40: 792 (letter).
15 Vantrappen G, Hellemans J. Treatment of achalasia andrelated motor disorders. Gastroenterology 1980; 79: 144±54.
16 Schmidt T, Hackelsberger N, Widmer R, Meisel C, PfeifferA, Kaess H. Ambulatory 24-hour jejunal motility in diar-rhea-predominant irritable bowel syndrome. Scand J Gas-troenterol 1996; 31: 581±9.
17 Schmidt T, Pfeiffer A, Hackelsberger N, Widmer R, MeiselC, Kaess H. Effect of intestinal resection on human smallbowel motility. Gut 1996; 38: 859±63.
18 Schmidt T, Widmer R, Pfeiffer A, Kaess H. Effect of thequarternary ammonium compound trospium chloride on24 hour jejunal motility in healthy subjects. Gut 1994; 35:27±33.
19 Widmer R, Schmidt T, Pfeiffer A, Kaess H. Computerizedanalysis of ambulatory long-term jejunal motility. Scand JGastroenterol 1994; 29: 1076±82.
20 Vantrappen G, Janssens J, Hellemans J, Ghoos Y. The in-terdigestive motor complex of normal subjects and pa-tients with bacterial overgrowth of the small intestine. JClin Invest 1977; 59: 1158±66.
21 HellstroÈm PM, Husebye E, Kraglund K. Methodology formotility studies in the small intestine: a Scandinavianconsensus. Eur J Surg 1991; Suppl. 564): 51±62.
22 Summers RW, Anuras S, Green J. Jejunal manometry pat-terns in health, partial intestinal obstruction, and pseu-doobstruction. Gastroenterology 1983; 85: 1290±300. .
23 Husebye E, Skar V, Hoeverstad T, Iversen T, Melby K.Abnormal intestinal motor patterns explain enteric colo-nization with gram-negative bacilli in late radiation en-teropathy. Gastroenterology 1078±89; 1995: 109: .
24 Cassella RR, Ellis FH, Brown AL. Fine-structure changes inachalasia of the esophagus. Am J Pathol 1965; 46: 279±88.
25 Smith B. The neurolgical lesion in achalasia of the cardia.Gut 1970; 11: 388±91.
26 De la Fuente A, Garcia-Calvo M, Ramon Y, cajal S, PayaJM, Cuesta G. Alteraciones ultrastructurales del nerviovago en la acalasia del eso fago. Rev Esp Enf Ap Digest 1977;51: 659±66.
27 Casella RR, Brown AL, Sayre GP, Ellis FH. Achalasia of theesophagus: pathologic and etiologic considerations. AnnSurg 1964; 160: 474±87.
28 Qualman SJ, Haupt HM, Yang P, Hamiltion SR. Esopha-geal Lewy bodies assocoated with ganglion cell loss inachalasia. Similarity to Parkinson's disease. Gastroenter-ology 1984; 87: 848±56.
29 Woolam GL, Maher B, Ellis FR. Vagal nerve fuction inachalasia of the esophagus. Surg Forum 1967; 18: 362±5.
30 Elder JB, Gillespie G. The vagus and achalasia. Gut 1969;10: 1045±69.
31 Dooley CP, Taylor IL, Valenzuela JE. Impaired acid secre-tion and pancreatic polypeptide release in some patientswith achalasia. Gastroenterology 1983; 84: 809±13.
32 Kellow JE, Gill RC, Wingate DL, Calam JE. Small bowelmotor activity and bacterial overgrowth. J Gastroint Mot1990; 2: 180±3.
33 Scheemann M, Ehrlein HJ. Postprandial patterns of caninejejunal motility and transit of luminal content. Gastroen-terology 1986; 90: 991±1000.
34 Chung SA, Diamant NE. Small intestinal motility infasted and postprandial states: effect of transient va-gosmypathetic blockade. Am J Physiol 1987; 252: G301±8.
35 Thompson GG, Ritchie HD, Wingate DL. Patterns of smallintestinal motility in duodenal ulcer patients before andfollowing vagotomy. Gut 1982; 23: 517±23.
36 Wingate DL. Backwards and forewards with the migratingmotor complex. Dig Dis Sci 1981; 26: 641±66.
37 Sarna S. Cyclic motor activity. Migrating motor complex1985. Gastroenterology 1985; 98: 894±909.
38 Stanghellini V, Camilleri M, Malagelada JR. Chronic id-iopathic intestinal pseudo-obstruction: clinical and intes-tinal manometric ®ndings. Gut 1987; 28: 5±12. .
39 Lindberg G, Iwarzon M, Veress B. Small bowel motilitypatterns in patients with chronic intestinal pseudoob-struction. Gut 1994; 35 (Suppl. 4): A185 (abstract).
40 Gerl A, Storck M. Paraneoplastic chronic intestinal pseu-doobstruction as a rare complication of bronchial car-cinoid. Gut 1992; 33: 1000±3.
41 Christensen J, Dent J, Malagelada JR, Wingate DL. Pseu-doobstruction. Gastroenterol Inl 1990; 3: 107±9.
42 Schuf¯er MD. Chronic intestinal pseudo-obstruction. MedClin North Am 1981; 65: 1331±58.
43 Hackelsberger N, Schmidt T, Renner R, Widmer R, PfeifferA, Kaess H. Ambulatory long-term jejunal manometry indiabetic patients with cardiac autonomic neuropathy. Ne-urogastroenterol Mot 1997; 9: 77±83.
44 Clouse RE, Eckert TC. Gastrointestinal symptoms of pa-tients with esophageal contraction abnormalities. Dig DisSci 1986; 31: 236±40.
45 Code CF, Schlegel JF. The gastrointestinal interdigestivehousekeeper: motor correlates of the interdigestive myo-electric complex in the dog. In: Daniel EE, ed. Proceedingsof the 4th International Symposium on GastrointestinalMotility. Vancouver, British Columbia: Mitchell Press,1974: 631±4.
46 Stotzer PO, BjoÈ rnsson ES, Abrahamsson H. Interdigestiveand postprandial motility in small-intestinal bacterialovergrowth. Scand J Gastroenterol 1996; 31: 875±80.
Ó 1999 Blackwell Science Ltd 17
Volume 11, Number 1, February 1999 Jejunal motility in achalasia