Embed Size (px)
Citation preview
Dynamics of the Collateral Circulation inPatients with Subelavian Steal
By ROBERT J. MARSHALL, M.D., M.R.C.P., AND EmIL L. MANTINI, M.D.
W HEN the proximal portion of the sub-clavian artery is occluded, numerous
anastomotic vessels in the neck and chest wallare available to maintain the circulation to thearm." 2 Another collateral pathway, consistingof both vertebral arteries,3 has recently cre-ated much interest. Contorni4 showed, by theuse of selective arteriography, that dye passedup the right vertebral artery to its junctionwith the basilar artery and then down theleft vertebral artery to enter the left sub-clavian artery distal to its site of occlusion.Reivich et al.5 confirmed and amplified thisobservation. The term "subelavian steal" wasintroduced by the Newv England Journal ofMedicine6 and has been widely adopted, sinceit is succinct and euphonious. Numerous sub-sequent reports have described clinical, ra-diologic, and surgical aspects of the condi-cion,7-23 and it has also been the subject of arecent symposium.24
Since the procedure of arteriography per semay result in local hemodynamic changes, theneed for caution in assessing the significanceof reversed vertebral flow has properly beenstressed.25 27 The purpose of this study wasto confirn, by the use of an alternativetechnic, the authenticity of the radiographicappearances that form the basis for the diag-nosis of the subelavian steal.
Case ReportsTwo patients were selected for study from a
total of 12 in whom we have demonstrated, byselective arteriography, the occurrence of retro-grade flow in a vertebral artery secondary toproximal occlusion of the ipsilateral subclavian (orinnominate) artery.
From the Departments of Medicine and Surgery,West Virginia University School of Medicine, Mor-gantown, West Virginia.
Supported by Grant HE 07758-02, U. S. PublicHealth Service.
Circulation, Volume XXXI, February 1965
Case 1A 54-year-old man complained of the sudden
onset of pain and blueness of the right foot. Nopulses were palpable in the lower limbs. An ab-dominal aortogram showed complete occlusionbelow the level of the renal arteries; there wasalso segmental occlusion of the left superficialfemoral artery with well-developed collateral ves-sels, and occlusion of the right anterior tibialartery. Treatment consisted of thromboendarterec-tomy of the terminal aorta, both common andexternal iiliac arteries, and both common femoralarteries; part of the left iliac system was replacedwith a Dacron prosthesis. Subsequently, the circu-lation to both lower limbs was greatly improved,although claudication in the right calf continued.
In addition to these problems a delayed anddiminished pulse in the left arm was noted, butthere were no symptoms suggestive of cerebrovas-cular ischemia on exercise of this arm.
Special Brachiocephalic StudiesRight retrobrachial arteriography showed stenosis
at the origin of the right vertebral artery, goodfilling of this artery, and reversed flow in the leftvertebral artery (fig. 1) with subsequent filling ofthe distal left subelavian artery. Occlusion ofthe left subelavian artery at its origin was laterconfirmed by injecting dye into the aortic arch.There was only a slight decrease in systolic bloodpressure in the brachial artery of the affected arm,but the pulse was delayed and damped (fig. 2). Anindicator-dilution curve was obtained by samplingfrom the left brachial artery at 40 ml. per minutefollowing injection by hand into the innominate ar-tery of 5 mg. cardio-green dye dissolved in 1 ml.of water. The indicator appeared in about 6 sec-onds, reached maximal concentration in about 9seconds, and almost completely cleared prior tothe onset of "recirculation" (fig. 3). This demon-stration of a short circuit between the innominateand the distal left subclavian arteries confirmedthe authenticity of the radiographic findings.
Case 2A 46-year-old man complained of intermittent
claudication for 4 years and of numbness of theleft hand and arm. The numbness was worse duringexercise of the arm and was associated with blurringof vision of the left eye and occasionally with cir-cumoral numbness. The left arm tired easily. The
249
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

5MARSL1HIALL, MIANTINI
Figure 1
Bgliht el't)raehCoial artctiogtam ini p)atic nt (case 1) wfithl oc,elision of p-roxinal polt ion of lcft.snlhCeluiani ciItcli1i. Left. Good fillinig of tight vcetcbral (triter!, which is tgla-. Center (213secoid late). Bicvetci-d flowc in lcft certceial at-tet l. Righit (2/3 second latie). Conti ast incdclinin;etesists in left ccictel)rcil co/tenl.
1)1003} t1pessole was 145 885 into. fig (right aLrm.Yl)aInd 9937,17n11u. Jig (left ainn). rhe left brachialplise vas W(eak and dela ecl. Botlh femoral polisesw^et-e weak and bruits Nvere heatrdc over eaclh. Nodistal polises wet-e felt in the left loxver lim-ib. Ar-teriograins showed imultiple atreas of stetoosis inmajo)r vessels: the left ecotinioni iliac artery xxassexei-elv diseased; there xvas molerate atheiro-sclerosis of the r-iglht comiimon iliac artetrv; ther-ewere seveie steinosis at the origini of the right inl-ternial carotid artcrxv stettosis of the left internalcai-otid at te Ny, anId model-eatelv sexer-e steniosis actthe origini of the right subelavian airtery; thepr-oxiinial part of the left sutbelaxian- artery wasoccllldecd, and the dlistal par-t of this vessel filled
Figure 2
Pr-essuIre ptdses fraoi artiC trel ( ab)o\ ) aii(I leftbocehial ctnteiy (bhelow) in ctse 1. Nate fle dclay(tnd /ainpii-t in the latter pdtlse. Calibrcitioas fatOthe aottic are/2i atre ottl the left aitcl for tie brachlictlar-tery1f oVI the 1rig/lt.
)v meats of reversed flox dlowxv the left xerteblhtarterv.
Spcial BraI3rch/tiocc'pha/ic StuldiesAui Odotan-Ledin catheter, xhicih had been ad-
vxanceci to the aoi-tic ari-cl via percotaiteous p1ine-torie of the riglht femioral artery it ordler, to ol)tailcoiitirast filimiis of the brachliocephalic xessels, xvasacivatieedi fo- a short distance inito tlhe left commiiiioncarotid air teirx. A cardiac catheter xvas introduced toan arim veinb l)prcut-taeonus puncture alnd placeclwith its tip in the lov sinperior vena rcava. A 19-gage M1ayo arterial nieedle xvas placed in the left
I
Injection intoinnominate a.,sampling f imnleft brachiol a,
10 seconds
Figure 3
In dicat oi-dilittiotn c nrce obtainied froiti left br-aczicalartet y aftc r injectioin of carcdia-greei c/ice into thzeitninoinate alter!, (iiijeetiatc tinme narked by ar--irotc). F/eic apid appectattee time (6 secatids) andIpeak coniceit/i atioti (.9 seeciics) wcere duec to shiitnt-in,g of t/te dye viai the eollaterctl ccn-tebrctl cireitla-ticoit shocni in figurev 1.
(/in i/ ,lati~.Vdme N\'XxI tcbimirY 1965
25 v
H H 7 7 74
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
COLLATERAL CIRCULATION IN SUBCLAVIAN STEAL
mg/L.
A --2
Injection into SVC, 4sampling from Left
6
Brachial Artery (LBA) 6
\_/ -~~~~~~~~~8
10
-o-1O seconds -_
B
Inojection into Left Carotid Artery
(LCA), sampling from LBA (control)
Injection into LCA, samplingfrom LB A (reactive hyperomia)
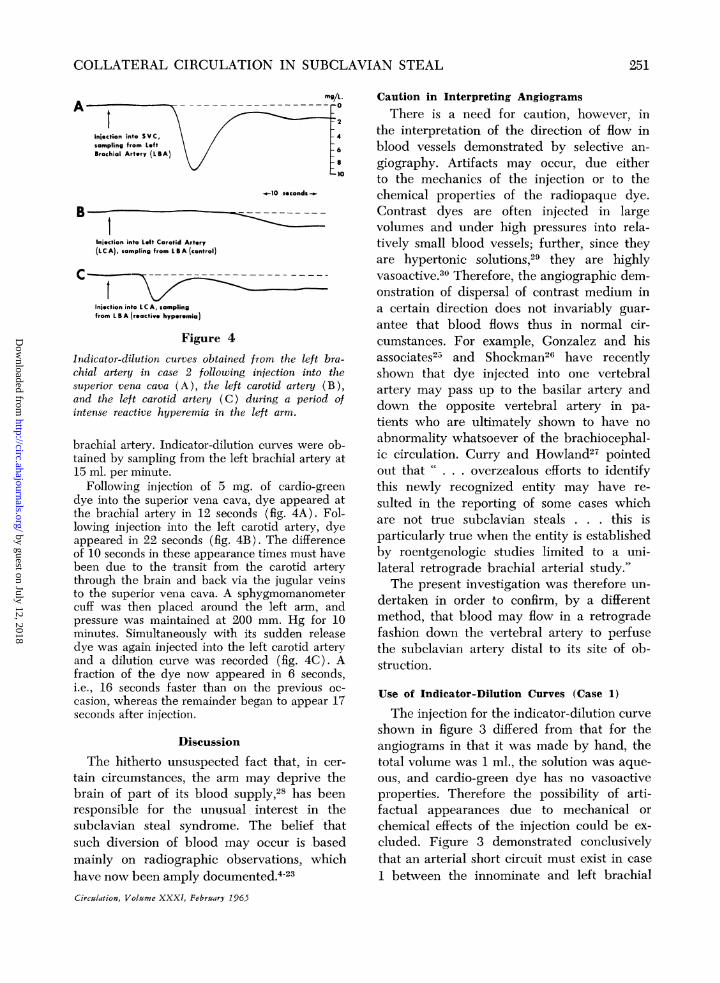
Figure 4
Indicator-dilution curves obtained from the left bra-chial artery in case 2 following injection into thesuperior vena cava (A), the left carotid artery (B),and the left carotid artery (C) during a period ofintense reactive hyperemia in the left arm.
brachial artery. Indicator-dilution curves were ob-tained by sampling from the left brachial artery at15 ml. per minute.
Following injection of 5 mg. of cardio-greendye into the superior vena cava, dye appeared atthe brachial artery in 12 seconds (fig. 4A). Fol-lowing injection into the left carotid artery, dyeappeared in 22 seconds (fig. 4B). The differenceof 10 seconds in these appearance times must havebeen due to the transit from the carotid arterythrough the brain and back via the jugular veinsto the superior vena eava. A sphygmomanometercuff was then placed around the left arm, andpressure was maintained at 200 mm. Hg for 10minutes. Simultaneously with its sudden releasedye was again injected into the left carotid arteryand a dilution curve was recorded (fig. 4C). Afraction of the dye now appeared in 6 seconds,i.e., 16 seconds faster than on the previous oc-
casion, whereas the remainder began to appear 17seconds after injection.
DiscussionThe hitherto unsuspected fact that, in cer-
tain circumstances, the arm may deprive thebrain of part of its blood supply,28 has beenresponsible for the unusual interest in thesubclavian steal syndrome. The belief thatsuch diversion of blood may occur is basedmainly on radiographic observations, whichhave now been amply documented.23Circulation, Volume XXXI, February 1965
Caution in Interpreting AngiogramsThere is a need for caution, however, in
the interpretation of the direction of flow inblood vessels demonstrated by selective an-giography. Artifacts may occur, due eitherto the mechanics of the injection or to thechemical properties of the radiopaque dye.Contrast dyes are often injected in largevolumes and under high pressures into rela-tively small blood vessels; further, since theyare hypertonic solutions,29 they are highlyvasoactive. Therefore, the angiographic dem-onstration of dispersal of contrast medium ina certain direction does not invariably guar-antee that blood flows thus in normal cir-cumstances. For example, Gonzalez and hisassociates25 and Shockman26 have recentlyshown that dye injected into one vertebralartery may pass up to the basilar artery anddown the opposite vertebral artery in pa-tients who are ultimately shown to have noabnormality whatsoever of the brachiocephal-ic circulation. Curry and Howland27 pointedout that C. overzealous efforts to identifythis newly recognized entity may have re-sulted in the reporting of some cases whichare not true subelavian steals . . . this isparticularly true when the entity is establishedby roentgenologic studies limited to a uni-lateral retrograde brachial arterial study."The present investigation was therefore un-
dertaken in order to confirm, by a differentmethod, that blood may flow in a retrogradefashion down the vertebral artery to perfusethe subelavian artery distal to its site of ob-struction.
Use of Indicator-Dilution Curves (Case 1)
The injection for the indicator-dilution curveshown in figure 3 differed from that for theangiograms in that it was made by hand, thetotal volume was 1 ml., the solution was aque-ous, and cardio-green dye has no vasoactiveproperties. Therefore the possibility of arti-factual appearances due to mechanical orchemical effects of the injection could be ex-cluded. Figure 3 demonstrated conclusivelythat an arterial short circuit must exist in case1 between the innominate and left brachial
251
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

MARSHALL, MANTINI
arteries even when the left arm is at rest, sincedye appeared in the left brachial artery 6 sec-onds after its injection into the innominate ar-tery. In a person with a normal brachiocephal-ic circulation, dye could not have appeareduntil it had circulated through the brain (orright arm), returned to the right side of theheart, circulated through the lungs, and thenpassed via the aorta to the brachial artery.This would take 20 to 30 seconds. Thus, thedilution curve confirmed the authenticity ofthe angiograms.
Stimuli Increasing the Demand of theUpper Limb for Blood
Since in most persons there is a potentialcommunication via the circle of Willis be-tween the cerebral and the vertebral-basilarcirculations, it appeared possible that, in thepresence of an unusual demand by the affect-ed- arm, blood might be drained backwardsfrom the carotid as well as from the vertebralcirculation. To test this hypothesis, circum-stances were sought in which retrograde per-fusion of an affected subelavian artery waslikely to be maximal.The requirement of the resting upper limb
for blood is small, the total arterial flow (100to 200 ml. per minute) being only a smallfraction of the cephalic blood flow. Moderateexercise, however, increases the blood flowthrough skeletal muscle by 10-fold or more.3Therefore, when a normal arm is exercised,its arterial inflow can very readily exceed thetotal cephalic blood flow. During reactivehyperemia induced by sudden release of ablood pressure cuff previously inflated aroundthe upper arm to 200 mm. Hg for 10 minutes.the blood flow through the limb for severalseconds is even greater than that during ex-ercise.32 This is a simple and reproducibleprocedure, and we used it in our studies incase 2 in order to provide the situation inwhich retrograde flow was most likely to bedemonstrable.
Use of Indicator-Dilution Curves (Case 2)When the injection was made into the left
carotid artery with the left arm at rest, dyewvas not detected in the left brachial artery
until 22 seconds had elapsed. Thus, no shortcircuit existed between the carotid and thedistal subclavian artery. The injection wasthen repeated simultaneously with the re-lease of an arterial occlusion cuff around theleft arm. A fraction of the injected dye nowappeared in the left brachial artery within 6seconds; the remainder appeared about 17seconds after the injection. The initial frac-tion of the dye, and hence a fraction of thecarotid blood flow, must have reached theleft brachial artery by means of a short cir-cuit. The most likely route was via the in-ternal carotid and the posterior communicat-ing arteries and then, by further reversal offlow, the basilar and left vertebral arteries.The possibility cannot be excluded, however,that the circuit was extracranial, for example,via anastomoses between the occipital andvertebral arteries.2 8These observations confirm the clinical sus-
picion that the amount of retrograde flow inthe left vertebral artery may be increasedduring exercise of the left arm. Whether ornot symptoms of cerebral ischemia are in-duced by such exercise depends upon thestate of the other cerebral blood vessels. Incase 2, in addition to the occlusion of theleft subclavian artery, severe narrowing in-volved the right and left internal carotid ar-teries and the origin of the right subclavianartery. In other patients, in whom involve-ment of the other arteries is mild or absentand the reserve of the cerebral circulation isgreater, adequate compensation occurs for theincreased vertebral run-off, and symptoms donot occur.
Importance of Anatomic Variations
Variations in the anatomy of the brachio-cephalic vessels are numerous. In another caserecently studied by us, an anomalous left sub-clavian artery coexisted with coarctation ofthe aorta, and resulted in a delayed anddamped left radial pulse (fig. 5) similar tothat in case I (fig. 2). A right retrobrachialarteriogram showed late filling of the left sub-clavian artery via reversed flow in the left in-ternal mammary and other arteries, but not
Circalation, Volume XXXI, February 1965
252
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
COLLATERAL CIRCULATION IN SUBCLAVIAN STEAL
mm Hg
r 160
- - 1 second - - -
Ae ECG Ar
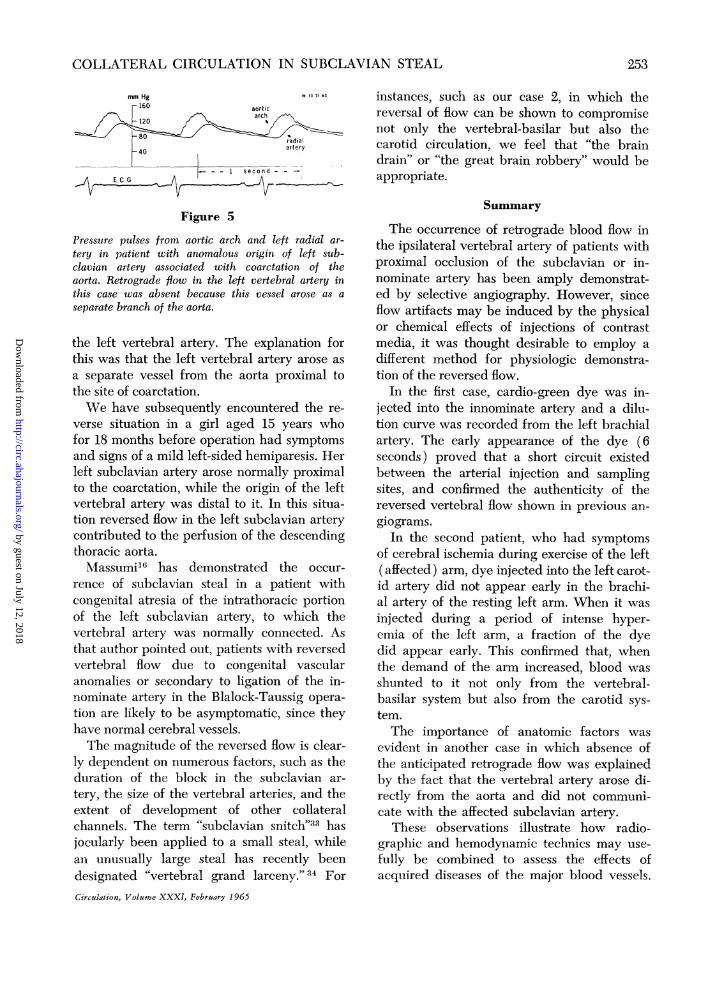
Figure 5
Pressure pulses from aortic arch and left radial ar-
tery in patient with anomalous origin of left sub-clavian artery associated with coarctation of theaorta. Retrograde flow in the left vertebral artery inthis case was absent because this vessel arose as a
separate branch of the aorta.
the left vertebral artery. The explanation forthis was that the left vertebral artery arose as
a separate vessel from the aorta proximal tothe site of coarctation.
XVe have subsequently encountered the re-
verse situation in a girl aged 15 years whofor 18 months before operation had symptomsand signs of a mild left-sided hemiparesis. Herleft subelavian artery arose normally proximalto the coarctation, while the origin of the leftvertebral artery was distal to it. In this situa-tion reversed flow in the left subclavian arterycontributed to the perfusion of the descendingthoracic aorta.Massumi16 has demonstrated the occur-
rence of subclavian steal in a patient withcongenital atresia of the intrathoracic portionof the left subclavian artery, to which thevertebral artery was normally connected. Asthat author pointed out, patients with reversedvertebral flow due to congenital vascularanomalies or secondary to ligation of the in-nominate artery in the Blalock-Taussig opera-
tion are likely to be asymptomatic, since theyhave normal cerebral vessels.The magnitude of the reversed flow is clear-
ly dependent on numerous factors, such as theduration of the block in the subclavian ar-
tery, the size of the vertebral arteries, and theextent of development of other collateralchannels. The term "subclavian snitch"33 hasjocularly been applied to a small steal, whilean unusually large steal has recently beendesignated "vertebral grand larceny."34 For
Circulation, Volume XXXI, February 1965
instances, such as our case 2, in which thereversal of flow can be shown to compromisenot only the vertebral-basilar but also thecarotid circulation, we feel that "the braindrain" or "the great brain robbery" would beappropriate.
Summary
The occurrence of retrograde blood flow inthe ipsilateral vertebral artery of patients withproximal occlusion of the subclavian or in-nominate artery has been amply demonstrat-ed by selective angiography. However, sinceflow artifacts may be induced by the physicalor chemical effects of injections of contrastmedia, it was thought desirable to employ adifferent method for physiologic demonstra-tion of the reversed flow.
In the first case, cardio-green dye was in-jected into the innominate artery and a dilu-tion curve was recorded from the left brachialartery. The early appearance of the dye (6seconds) proved that a short circuit existedbetween the arterial injection and samplingsites, and confirmed the authenticity of thereversed vertebral flow shown in previous an-giograms.
In the second patient, who had symptomsof cerebral ischemia during exercise of the left(affected) arm, dye injected into the left carot-id artery did not appear early in the brachi-al artery of the resting left arm. When it wasinjected during a period of intense hyper-emia of the left arm, a fraction of the dyedid appear early. This confirmed that, whenthe demand of the arm increased, blood wasshunted to it not only from the vertebral-basilar system but also from the carotid sys-tem.The importance of anatomic factors was
evident in another case in which absence ofthe anticipated retrograde flow was explainedby thb fact that the vertebral artery arose di-rectly from the aorta and did not communi-cate with the affected subclavian artery.
These observations illustrate how radio-graphic and hemodynamic technics may use-fully be combined to assess the effects ofacquired diseases of the major blood vessels.
253
H 13 71 63
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from
MARSHALL, MANTINI
References
1. GRAY, H.: Anatomy of the Human Body. Goss,C. M., editor: Ed. 27. Philadelphia, Lea &Febiger, 1959.
2. BOSNIAK, M. A.: Cervical arterial pathways as-sociated with brachiocephalic occlusive disease.Am. J. Roentgenol. 91: 1232, 1964.
3. TAGARIELLO, P.: I1 circolo collaterale nella lig-atura dell' arteria succlavia. Chir. org. movi-mento 36: 321, 1951.
4. CONTORNI, L.: I1 circolo collaterale vertebro-vertebrale nella obliterazione dell' arteria suc-clavia alla sue origine. Minerva chir. 15: 268,1960.
5. REIVICH, M., HOLLING, H. E., ROBERTS, B., AN-DTOOLE, J. F.: Reversal of blood flow throughthe vertebral artery and its effect on cerebralcirculation. New England J. Med. 265: 878,1961.
6. EDITORIAL: A new vascular syndrome-"The sub-clavian steal." New England J. Med. 265: 912,1961.
7. MANNICK, J. A., SUTER, C. G., AND HUME, D. M.:The "'subelavian steal" syndrome: a furtherdocumentation. J.A.M.A. 182: 254, 1962.
8. SIMON, M., RABINOv, K., AND HORENSTEIN, S.:Proximal subclavian artery occlusion and re-versed vertebral blood flow to the arm. Clin.Radiol. 13: 201, 1962.
9. NORTH, R. R., FIELDS, W. S., DE BAKEY, M. E.,AND CRAWFORD, E. S.: Brachial-basilar insuffi-ciency syndrome. Neurology 12: 810, 1962.
10. WILLIAMS, C. L., SCOTT, S. M., AND TAKARO, T.:Subclavian steal. Circulation 28: 14, 1963.
11. SPROUL, G.: Basilar artery insufficiency secondaryto obstruction of left subelavian artery. Circu-lation 28: 259, 1963.
12. BOSNIAK, M. A.: A collateral pathway throughthe vertebral arteries associated with obstruc-tion of the innominate and proximal subclavianarteries. Radiology 81: 89, 1963.
13. IRVINE, W. T., LUCK, R. J., SUTTON, D., ANDWALPITA, P. R.: Intrathoracic occlusion ofgreat vessels causing cerebrovascular insuffi-ciency. Lancet 1: 1177, 1963.
14. IRELAND, J. T.: Reversed flow in the vertebralartery in association with subclavian occlusion.Scottish M. J. 8: 308, 1963.
15. KESTELOOT, H., AND LANTIN, F.: Circulation in-versee dans l'artere vertebrale dans l'occlusionorificielle de l'artere sous-claviere. Etude clin-ique et radiologique d'un cas. Acta cardiol.18: 78, 1963.
16. MASSUMI, R. A.: The congenital variety of the
"1subclavian steal." Circulation 28: 1149, 1963.17. GONSETTE, R., ANDRE-BA-LISAUX, G., AND LANTIN,
F.: Syndrome de suppleance vertebro-sous-claviere. Ann. Radiol. 6: 61, 1963.
18. PHILP, T., SAMUEL, E., AND DUNCAN, J. G.:Reversed vertebral artery blood flow in sub-clavian artery obstruction. Clin. Radiol. 14:310, 1963.
19. STEINBERG, I., AND HALPERN, M.: Roentgen mani-festations of subclavian steal syndrome. Am. J.Roentgenol. 90: 528, 1963.
20. FISCHER, M. J., AND MATTEY, W. E.: Subclaviansteal syndrome. Am. J. Roentgenol. 90: 532,1963.
21. ASHBY, R. N., KARRAS, B. G., AND CANNON, A. H.:Clinical and roentgenographic aspects of sub-clavian steal syndrome. Am. J. Roentgenol. 90:535, 1963.
22. PARROTT, J. C.: The subclavian steal syndrome.Arch. Surg. 88: 661, 1964.
23. ETHIER, R.: Observations on retrograde vertebralartery blood flow. Am. J. Roentgenol. 91: 1245,1964.
24. Symposium on the "subelavian steal." In Siekert,R. G., and Whisnant, J. P., eds.: FourthPrinceton Conference on Cerebral VascularDiseases. New York, Grune & Stratton. In press.
25. GONZALEZ, L., WEINTRAUB, R. A., WIOT, J. F.,AND LEWIS, C.: Retrograde vertebral arteryblood flow. A normal phenomenon. Radiology82: 211, 1964.
26. SHOCKMAN, A. T.: Retrograde vertebral arteryflow as an artifact of technique. Am. J.Roentgenol. 91: 1258, 1964.
27. CURRY, J. L., AND HOWLAND, W. J.: Subclaviansteal syndrome. Pitfalls in its diagnosis. Am. J.Roentgenol. 91: 1254, 1964.
28. TOOLE, J. F.: Reversed vertebral-artery flow. Sub-clavian-steal syndrome. Lancet 1: 872, 1964.
29. MARSHALL, RI. J., AND SHEPHERD, J. T.: Effect ofinjections of hypertonic solutions on blood flowthrough the femoral artery of the dog. Am. J.Physiol. 197: 951, 1959.
30. READ, R. C.: Cause of death in cardioangiog-raphy. J. Thoracic & Cardiovasc. Surg. 38: 685,1959.
31. BLACK, J. E.: Blood flow requirements of thehuman calf muscle after walking and running.Clin. Sc. 18: 89, 1959.
32. PATTERSON, G. C., AND WHELAN, R. F.: Reactivehyperemia in the human forearm. Clin. Sc. 14:197, 1955.
33. HEYMAN, A.: Quoted in reference 24.34. DAVES, M. L., AND TREGER, A.: Vertebral grand
larceny. Circulation 29: 911, 1964.
Circulation, Volume XXXI, February 1965
I2.54
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from

ROBERT J. MARSHALL and EMIL L. MANTINIDynamics of the Collateral Circulation in Patients with Subclavian Steal
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1965 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.31.2.249
1965;31:249-254Circulation.
http://circ.ahajournals.org/content/31/2/249located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. and Rights Question and Answer
Permissionsthe Web page under Services. Further information about this process is available in thewhich permission is being requested is located, click Request Permissions in the middle column ofClearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of the CopyrightCirculationoriginally published in Requests for permissions to reproduce figures, tables, or portions of articlesPermissions:
by guest on July 12, 2018http://circ.ahajournals.org/
Dow
nloaded from