Embed Size (px)
Citation preview

Dynamics of Dental Pulp & Periapical Pathologies
Deepti AwasthiP G student
CONTENTS
• Introduction• Development• Anatomy• Structural features• Blood vessels• Lymph vessels• Nerves • Functions• Differences in primary & permanent pulp
organ

• Age changes• Classification of pulpal pathologies Reversible pulpitis Irreversible pulpitis Acute apical periodontitis Phoenix abscess Periapical granuloma Radicular cyst External resorption Internal resorption Pulp necrosis• Conclusion• References
Definition
Dental pulp, a small mass of connective tissue, blood vessels, and nerves located in a chamber within the dentin layer of a tooth. The pulp chamber is found in the crown and the root of a tooth.
Mosby's Medical Dictionary, 8th edition. © 2009, Elsevier
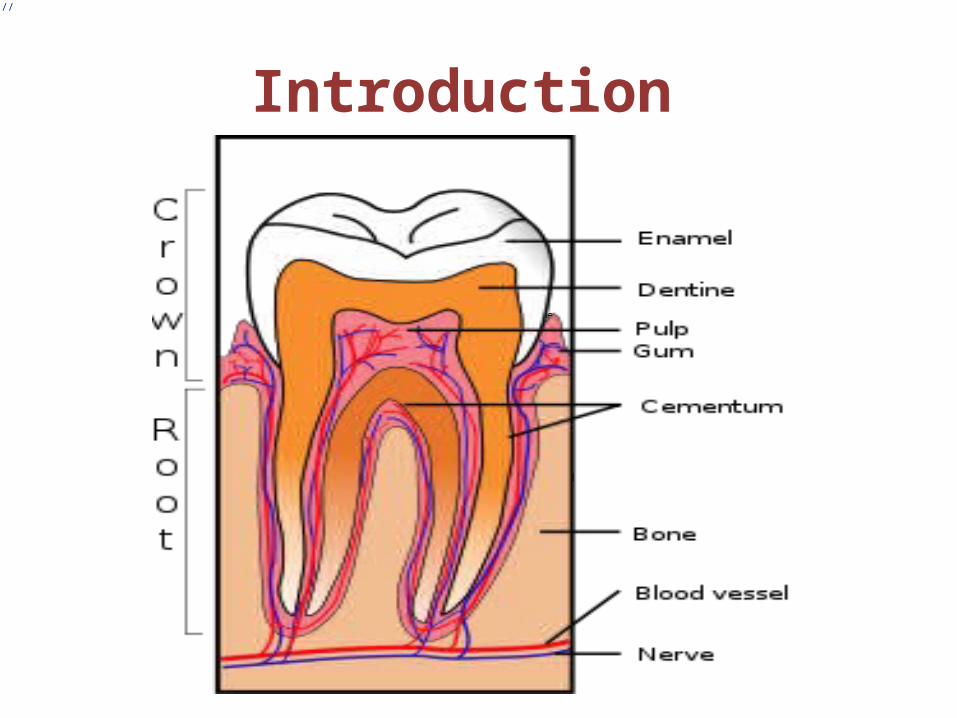
Introduction
://

Development
Regeneration of tooth pulp dentin
ANATOMY
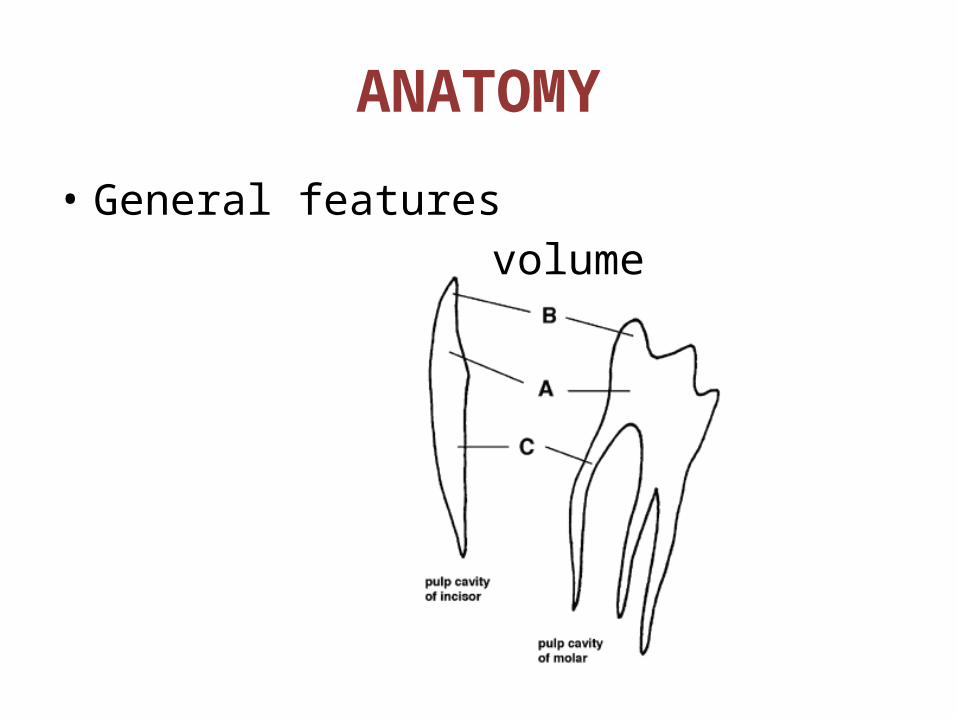
• General features volume
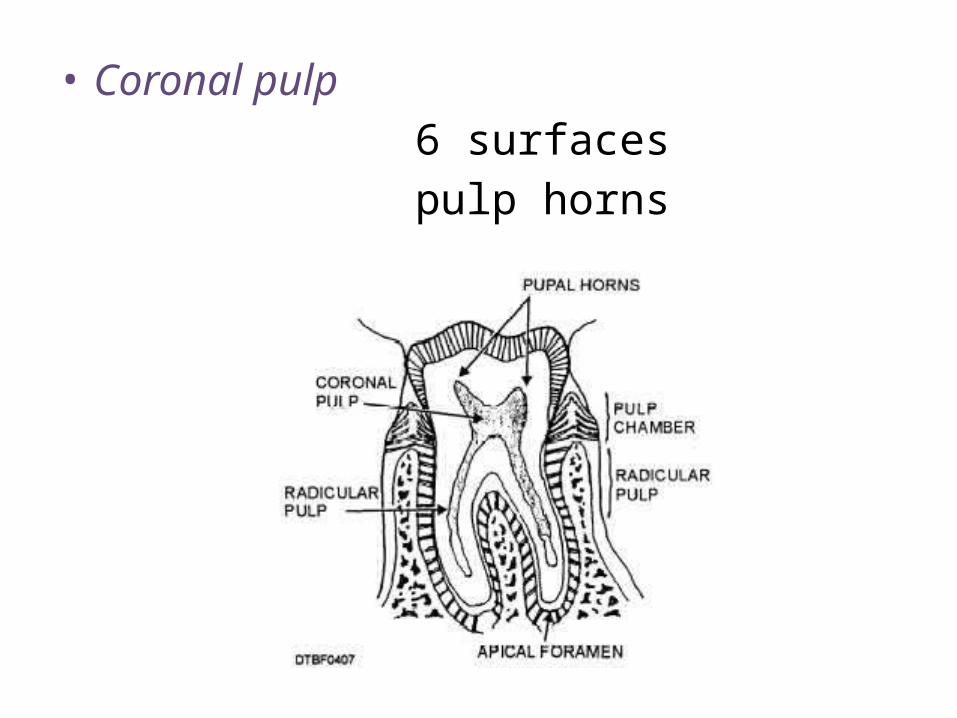
• Coronal pulp 6 surfaces pulp horns
• Radicular pulp single , multiple tubular shape growth –more dentin – pulp gets
narrower

• Apical foramen avg. size in adults location & shape may undergo
changes frequently , there are 2 or more
foramina seperated by a portion of dentin & cementum or by cementum only.
orbans
• Accessory canals from radicular pulp laterally through the
root dentin to the pdl tissue apical third clinically significant in spread of infection
Mechanism of accessory canal formation :
Textbook of Endodontics – Nisha Garg
STRUCTURAL FEATURES
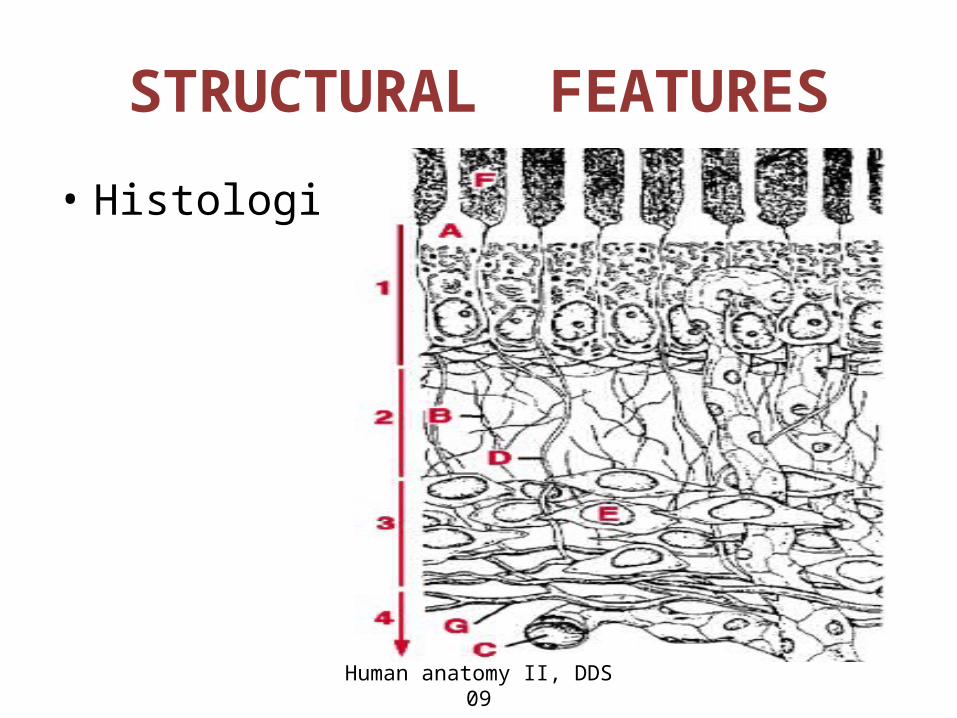
• Histologically,
Human anatomy II, DDS 09
• Principal cells : odontoblasts fibroblasts undifferentiated mesenchymal macrophages lymphocytes dendritic cells• Intercellular substances :
Intercellular substances
• Dense & gel like• Acid muco polysaccharide & protein
polysaccharide• During early development, chondroitin A,B &
hyaluronic acid.• Lends support to the cells of the pulp• Transport of nutrients & metabolites• Gag –hydrophilic,forms a gel – high tissue fluid
pressure.orbans

Fibroblasts
• Most numerous• Function –• Stellate shape & extensive processes• Electron micrograph – RER , mitochondria etc• Young pulp – divide & are active in protein
synthesis• Older pulp – spindle shaped , fibrocytes• Mature & immature pulp-
orbans

• Dual function• Inflammation & healing
• Fibres – type I & III length – 10 – 100nm cross striation at 64 nm• After root completion, pulp matures &
bundles of collagen fibres increase in number.• Apical region
orbans
• Fibres are more numerous in radicular pulp than coronal & greatest concentration of collagen occurs in the most apical portion of the pulp. This is of practical significance as engaging the pulp with a barbed broach in the apex region affords a better oppurtunity to remove the tissue intact.
Textbook of endodontics
Undifferentiated mesenchymal cells
• Totiopotent cell• Light microscope – large polyhedral cell ,large
lightly stained centrally placed nucleus.• Decrease in old age – reduces the
regenerative potential of the pulp
orbans
Odontoblasts
• 2nd most prominent• Adjacent to the predentin with cell bodies in the
pulp & processes in the dentinal tubules.• Diameter- 5-7 um• Length – 25-40 um • Cell bodies – large oval nuclei , fills the basal part
of the cell• Adjacent to the nucleus basally, RER & golgi app• Pulpal predentin junction – no organelles
orbans
• Odontoblasts mainly synthesize type I collagen ,proteoglycans & also secretes dentin sialoprotein, alkaline phosphatase , phosphophoryn involved in extracellular mineralization.
Pathways of pulp

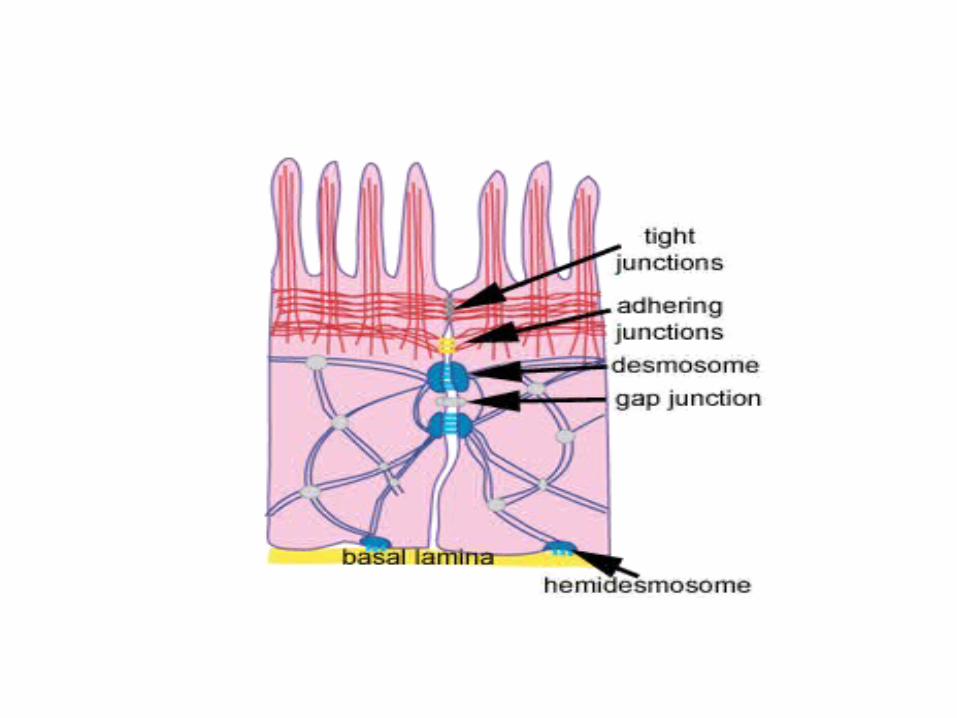
• Cell junctions : macula adherens tight junctions gap junctions• More cylindrical & longer – crown• More cuboid – middle of root• Ovoid & spindle shaped – close to apex• Releases IL-8 , chemotactic for neutrophils• Nitric oxide synthetase – vasodilation & blood
pressure regulationBerkowitz
DEFENCE CELLS
• Histiocyte / macrophage –
• Inactive –difficult to distinguish from fibroblasts
• Pulpal inflammation- exhibit granules & vacuoles in their cytoplasm , nuclei increases
• Small blood vessels & capillaries• Aggregate of vesicles or phagosomes
orbans
• Dendritic cells
• Similar to langerhan’s• In deciduous teeth – odontoblasts• Increase in areas affected by caries, attrition
or restorative procedures• Immunocompetent cells in deciduous teeth
increased in number during shedding.
Tencates
• Lymphocytes
• Mast cells – vessels in the inflamed pulp.
• Plasma cells – antibodies light microscope – nucleus
appears small & concentric cart wheel appearance
Orbans
lymphocyte Mast cell

BLOOD VESSELS
• The blood vessels – arise from inferior or superior alveolar artery & drain by same veins
• Small arteries & arterioles – apical canal & pursue a direct route to the coronal pulp. Along their course they give off numerous branches in the radicular pulp that passes peripherally to form plexus in the odontogenic region .
• Pulpal pressure – among the highestTencates
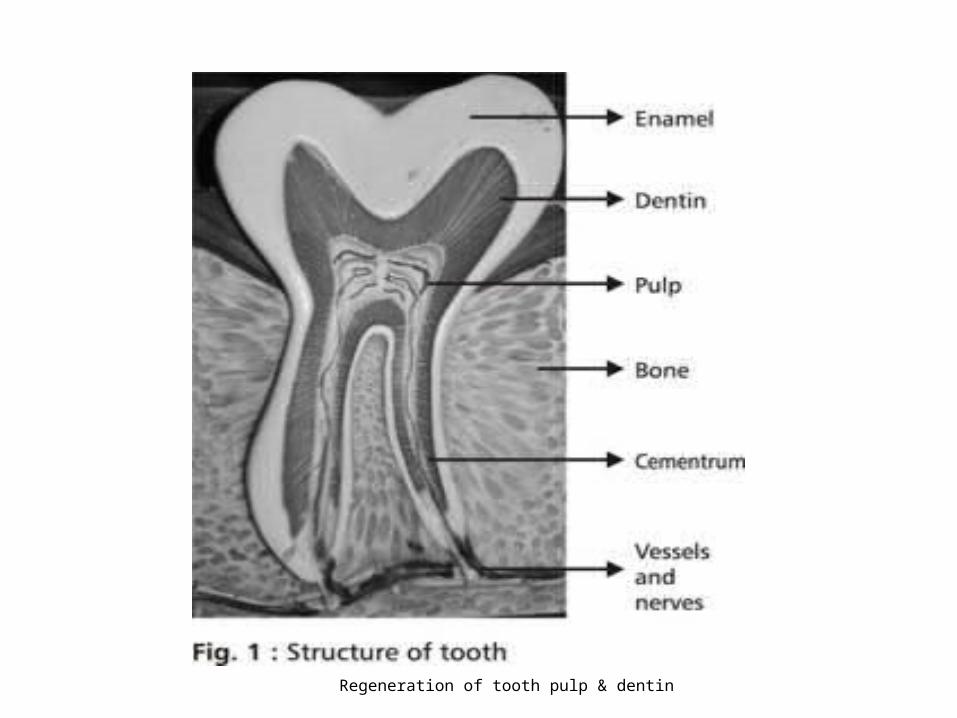
Regeneration of tooth pulp & dentin
LYMPH VESSELS
• Endothelium lined tubes that join thin walled lymph venules or veins in the central pulp.
• Capillaries – thin walls• Central part of the pulp.• Lymph vessel draining the pulp & pdl – common
outlet.• Anterior teeth – submental • Posterior teeth – submandibular & deep cervical
nodes
NERVES
• non-myelinated • 150-1200• Larger fibre range 5 & 13 um, majority are
smaller than 4 um• Perineurium & epineurium – thin• Parietel layer, plexus of rashkow• pulp horns
berkovitz

• The mature deciduous teeth-well innervated, esp coronal pulp , has many nerve endings terminating in or near odontoblast layer , with a few penetrating into dentin.
• No clear evidence that any sensation other than pain can be experienced fron pulp.
• The sensory nerves of the pulp arise from the trigeminal nerve.
Pathways of pulp
Textbook of endodontics
A$ - myelinated faster pulp- dentin junction sharp,pricking, localized
C – sympathetic efferents non myelinated throughout the pulp dull & more diffuse pain
• EPT stimulates A delta fibres first because of their lower threshold. As intensity of stimulus is increased, some of the C fibres also get stimulated.
• The relatively late appearance of A fibres in the pulp may explain why EPT tends to be unreliable in young teeth since A fibres are more easily stimulated than C fibres.
Pathways of pulp

FUNCTIONS
INDUCTIVE
FORMATIVE
NUTRITIVE
PROTECTIVE
DEFENSIVE/REPARATIVE
Tencates

Differences in primary & permanent pulp tissues
• PRIMARY PULP• Function for only about 8yrs & 3 mths
duration• 3 time periods :
1. Period of growth of pulp organ : in about 1yr time , the crown & roots of the
teeth develop
orbans
2. Period of maturation of pulp: root is completed & resorption of root
begins at about 3yrs to 9 mths of age3. Regression of pulp : period of regression of deciduous radicular
pulp depends on the time from the completion of the permanent crown till the time of permanent tooth eruption.
• Max. life of primary pulp organ : 9yrs & 6mths.
orbans

• PERMANENT PULP ORGAN• The pulp undergoes development for about
12 yrs ,4mths.( crown calcification to root completion )
• Primary teeth – 4yrs, 2mths• Period of pulp aging is much accelerated in
primary teeth.• Maxillary arches require slightly longer to
complete each process of development.
orbans
AGE CHANGES
• Most conspicuous change – decreasing volume of the pulp chamber & root canal
• In old teeth , RC is often a thin channel. sometimes almost completely
obliterated.• Continued restriction in pulp volume –
decrease in vascular supply & initiates other age changes.
orbans
• Cell changes
• Reduction in size & no. of cytoplasmic organelles.
• 20 yrs of age , cells gradually reduce in no. until age 70 ,cell density has decreased by
about half.
orbans
Fibrosis
• Radicular pulp – arranged longitudnally in bundles
• Coronal pulp – random/diffuse• Any external trauma – localized fibrosis or
scarring effect.• Collagen increase is noted in media &
adventitia layer of blood vessel

Vascular changes
• Reduced vascularity• Blood flow is decreased.• Calcification in the walls of blood vessels –
near apical foramen• Atherosclerotic plaques may appear
Tencates

Pulp stones
• Denticles• Calcified masses appearing in either or both
the coronal & root portions of the pulp organ• Usually are asymptomatic, unless impinge on
nerve or blood vessel.

• CLASSIFICATION
• Acc to structure : true false
• Acc to relation with Dentin : free attached embedded
Textbook of endodontics


True
• Similar to dentin• Close to the apical foramen• Development – inclusion of remnants of HERS within the pulp. they induce the cells of the pulp to differentiate into odontoblasts which form the dentin masses.
Tencates

False
• Appear as concentric layers of calcified tissues• They appear within a bundle of collagen
fibres.• Some arise around vessels.• In the centre – remnants of necrotic &
calcified cells.• Phlebolith – may serve as nidi for false
denticles.
Tencates
• Free – • Attached-• Embedded-
• 90% - > 50yrs of age • 80% - 30-50 yrs of age • 66% - 10-30 yrs of age
Tencates
Diffuse calcification
• Irregular calcific deposits in the pulp tissue usually following collagenous fibre bundles or blood vessels.
• usually found in the root canal , whereas denticles are more in coronal pulp.
orbans

CLASSIFICATION
• Acc to Grossman:1. Pulpitis a) Reversible symptomatic asymptomaticb) Irreversible o acute responsive to cold responsive to heat
Textbook of endodontics
o chronic Asymptomatic hyperplastic pulpitis internal resorption
2. Pulp degenerationa) calcificb) Others necrosis
WHO Classification
• K04.4 – AAP• K04.5 – CAP• K04.6 – PA with sinus• K04.60 – PA with sinus to max antrum• K04.61 - PA with sinus to nasal cavity• K04.62- PA with sinus to oral cavity• K04.63 - PA with sinus to skin• K04.7 - PA without sinus• K04.8 - PC• K04.80 - apical & lateral cyst • K04.81 - Residual cyst• K04.82 - inflammatory paradental cystPathways of pulp
Ingle’s Classification
A. Painful Pulpoperiapical Pathologies 1. AAP 2. Advanced AP a. Acute Apical Abscess b. phoenix abscess c. suppurative apical periodontitis
B. Non – Painful 1. Condensing osteitis 2. CAP - incipient stage 3. CAP - Periapical granuloma - periapical cyst - suppurative apical periodontitis

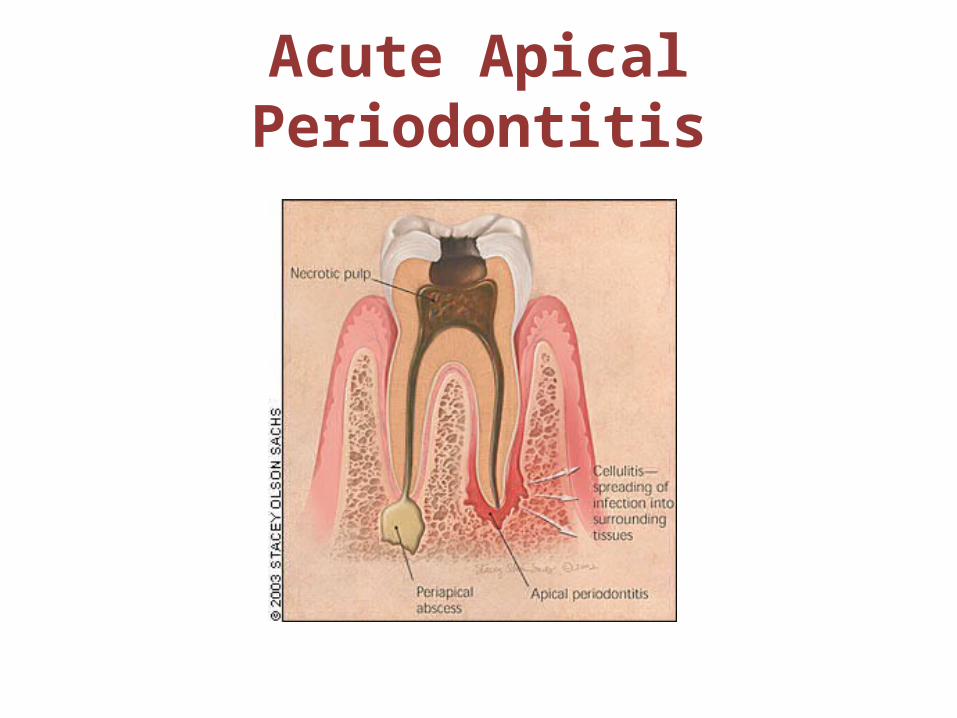
Acute Apical Periodontitis

Acute Apical Abscess
Phoenix Abscess
• An acute inflammatory reaction superimposed on an existing chronic lesion, such as cyst or granuloma.
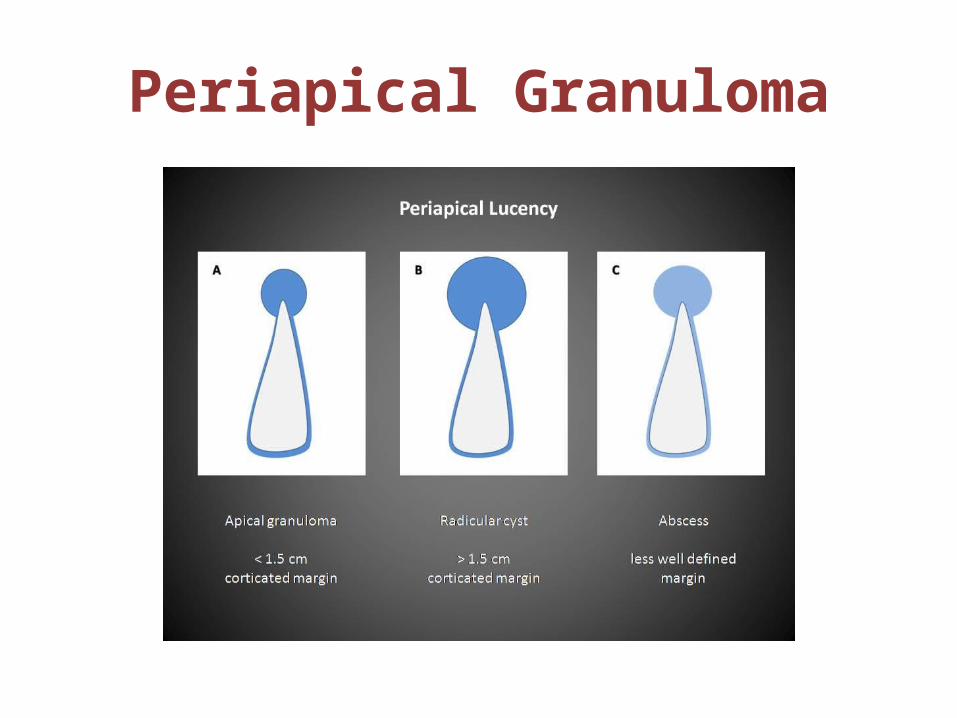
Periapical Granuloma

Radicular Cyst

External Root Resorption

Internal Resorption
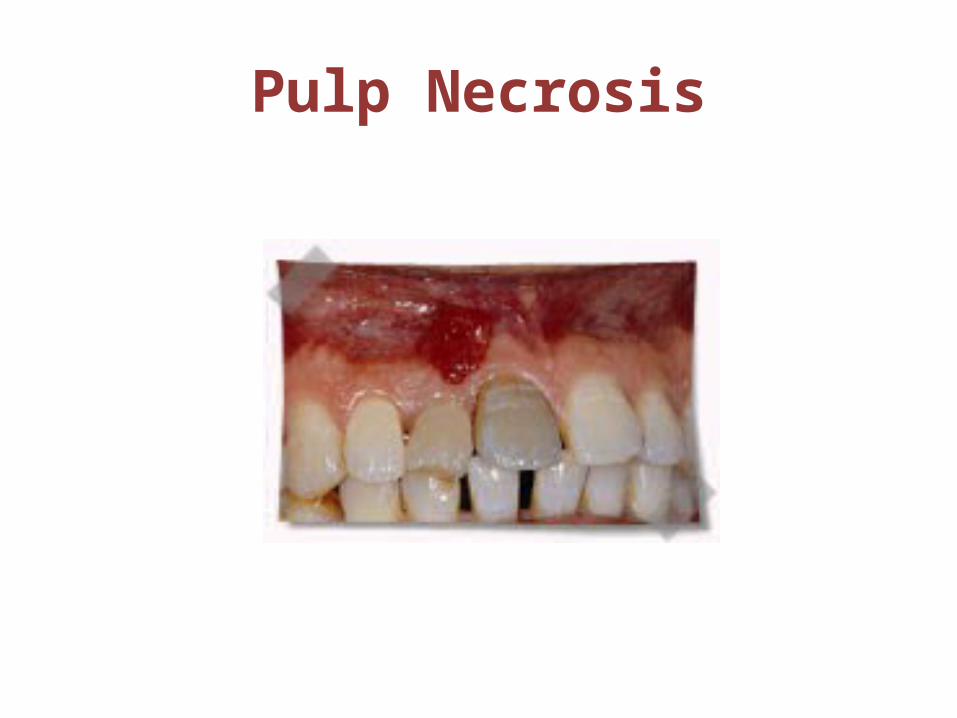
Pulp Necrosis

• Effect of posture on pulpal flow
In normal upright posture , there is less pressure effect in the structure of head. Lying down increases blood flow to pulp by removal of both gravitational & baroreceptor effect.
Textbook of endodontics

• Regeneration of pulp dentin
Regeneration of tooth pulp & dentin

conclusion
References
• Orban’s Oral Histology &Embryology- 12th ed• Pathways of the pulp –stephen Cohen 9th ed• Textbook of endodontics – Nisha garg & Amit garg• Oral histology –Tencates• Berkovitz • Regeneration of tooth pulp and dentin : trends
and advances. Sarang Sharma, Vimal Sikri.Annals of Neurosciences, Volume 17, Number 1, January 2010