Embed Size (px)
Citation preview

Dynamic Immune Phenotypes of B and T Helper CellsMark Distinct Stages of T1D ProgressionTania Habib,1 S. Alice Long,1 Peter L. Samuels,1 Archana Brahmandam,2 Megan Tatum,1 Andrew Funk,1
Anne M. Hocking,1 Karen Cerosaletti,1 Michael T. Mason,1 Elizabeth Whalen,3 David J. Rawlings,2,4
Carla Greenbaum,3 Jane H. Buckner,1 and the Type 1 Diabetes TrialNet Study Group
Diabetes 2019;68:1240–1250 | https://doi.org/10.2337/db18-1081
Multiple studies of B- and T-cell compartments and theirresponse to stimuli demonstrate alterations in estab-lished type 1 diabetes (T1D). Yet it is not known whetherthese alterations reflect immune mechanisms that initi-ate islet autoimmunity, promote disease progression, orare secondary to disease. To address these questions,we used samples from the TrialNet Pathway to Preven-tion study to investigate T-cell responses to interleukin(IL)-2 and regulatory T cell–mediated suppression, thecomposition of the B-cell compartment, and B-cellresponses to B-cell receptor and IL-21 receptor engage-ment. These studies revealed stage-dependent T- andB-cell functional and immune phenotypes; namely, earlyfeatures that differentiate autoantibody-positive at-riskfirst-degree relatives (FDRs) from autoantibody-negativeFDRs and persisted through clinical diagnosis; late fea-tures that arose at or near T1D diagnosis; and dynamicfeatures that were enhanced early and blunted at laterdisease stages, indicating evolving responses along thecontinuum of T1D. We further explored how these spe-cific phenotypes are influenced by therapeutic interven-tions. Our integrated studies provide unique insights intostable and dynamic stage-specific immune states anddefine novel immune phenotypes of potential clinicalrelevance.
The natural history of type 1 diabetes (T1D) has beenstudied extensively with respect to development of islet-reactive autoantibodies, b-cell function, and metabolic
markers of disease progression (1–3). This has paralleledan improved understanding of genetic risk factors andenvironmental factors that influence disease susceptibility.As a result, progress has been made in trials aimed atpreserving insulin secretion in established T1D (1,4–6).However, to determine the optimal type and timing ofimmunotherapies to prevent and treat T1D (7), a betterunderstanding of the immune mechanisms that drive pre-clinical disease in the at-risk population and interindividualimmune heterogeneity will be required.
The strong genetic link with HLA class II alleles andother genes that participate in T-cell function underscoresthe importance of CD4+ T cells in T1D. In the NODmouse,CD4+ effector T cells (Teffs) are required for diabetesprogression (8). Increased frequencies of CD4+, T helper17, and follicular T helper (Tfh) cells have been reported inboth new-onset and established T1D (9–15). Tfh cells arealso increased in autoantibody-positive (autoAb+) childrenwith impaired glucose tolerance, suggesting the evolutionof a pathogenic Tfh population poised to promote B-cellresponses during disease progression (15). Functionalconsequences likely underlie these phenotypes, as CD4+
Teffs are resistant to regulatory T-cell (Treg) suppression(16,17) and exhibit altered responses to cytokines, havinga blunted response to interleukin (IL)-2 (18,19) and anenhanced response to IL-6 (20), in established T1D.
Emerging data also implicate B cells in the developmentof the autoimmune T-cell response in numerous diseasesettings (21–23). In NOD mice, B cells are required for
1Translational Research Program, Benaroya Research Institute, Seattle, WA2Center for Immunity and Immunotherapies, Seattle Children’s Research Institute,Seattle, WA3Diabetes Clinical Research Program, Benaroya Research Institute, Seattle, WA4Departments of Pediatrics and Immunology, University of Washington School ofMedicine, Seattle, WA
Corresponding author: Jane H. Buckner, [email protected]
Received 10 October 2018 and accepted 15 March 2019
This article contains Supplementary Data online at http://diabetes.diabetesjournals.org/lookup/suppl/doi:10.2337/db18-1081/-/DC1.
T.H. and S.A.L. contributed equally to this work.
© 2019 by the American Diabetes Association. Readers may use this article aslong as the work is properly cited, the use is educational and not for profit, and thework is not altered. More information is available at http://www.diabetesjournals.org/content/license.
1240 Diabetes Volume 68, June 2019
IMMUNOLOGY
AND
TRANSPLANTATIO
N

shaping productive CD4+ T-cell responses, via their capac-ity to process and present islet antigen via MHC class IIand as the dominant antigen-presenting cell for self-reactive CD4+ T cells (21,24). Furthermore, genome-wideassociation studies and genotype–phenotype studies inhuman autoimmune diseases have identified several var-iant alleles that impact B-cell homeostasis, function, andtolerance checkpoints (25–31). The beneficial outcomes ofinterventions that target T cells (5,32) and B cells (4,33)provide amechanistic framework for T- and B-cell–mediatedautoimmune pathogenesis. They also indicate that a morecomplete understanding of the temporal evolution andcooperation of T- and B-cell phenotypes during the naturalhistory of T1D is warranted.
The aim of this study was to define the temporalevolution of CD4+ Teff and B-cell phenotypes in T1D de-velopment and progression in at-risk subjects. Our resultsreveal distinct phenotypes in the T- and B-cell compart-ments at an early stage of autoimmunity, characterized byblunted IL-2 signaling in CD4+ Teffs, enhanced responses toIL-21 in the naive B-cell population, and an expansion oftransitional B cells. As individuals progress toward clinicaldisease, we observed the acquisition of Teff resistance,a decrease in the B-cell response to IL-21, and attenuatedB-cell receptor (BCR) responses. Our findings suggest thatearly tolerance checkpoints are altered in B cells, which maypredispose to enhanced autoreactivity. This early change inB cells in disease may be potentiated through T-cell helpthat is driven by blunted responses to IL-2 in Teffs and anenhanced IL-21 response in the B-cell population. By com-parison, later in disease, the Teff resistance to suppression ispredominant, suggesting an acquired trait.
RESEARCH DESIGN AND METHODS
Human SubjectsThe study was approved by the Benaroya Research In-stitute (BRI) institutional review board, and all subjectsgave written informed consent. Cohorts are described inSupplementary Tables 1–5. The Type I Diabetes TrialNetPathway to Prevention (PTP) Trial (TN01 Trial, formerlythe TrialNet Natural History Study; NCT00097292) has beenpreviously published (34,35), as have TrialNet’s Rituximabtrial (NCT00279305) (33) and the Immune Tolerance Net-work’s T1DAL trial (32). The subjects with establishedT1D and healthy individuals were participants in the BRIImmune-Mediated Disease Registry and Repository. Allsamples were assayed in a blinded manner. Frozen sam-ples were used for all assays. Assays on each thawedsample were prioritized based on required cell number foranalysis. Data from samples were excluded when viabilitywas ,40% and when data were not reliable due to lowevent count or responses were not detected in the same-day internal control.
Immunophenotyping and Phospho-Flow CytometryIL-2/phosphorylated (p)STAT5 phospho-flow cytometrywas performed as described previously (18). In brief, cells
were activated with 25 IU/mL IL-2 for 10 min. For IL-21/pSTAT3 phospho-flow, thawed peripheral blood mono-nuclear cells (PBMCs) were rested in serum-free X-VIVO15 medium for 1 h, washed with PBS, and stimulated withrecombinant human IL-21 (0.1 ng/mL or 50 ng/mL)(Miltenyi Biotec, Auburn, CA) for 10 min. Cells for bothcytokine stimulation assays were fixed with BD PhosflowBuffer I and permeabilized using BD Phosflow Buffer IIIprior to staining with antibodies against pSTAT5 (pY694),CD25, CD4, and CD45RO or pSTAT3 (pY705), CD3, CD4,CD45RA, CD8, and CD20 for IL-2 and IL-21, respectively.Teffs were defined as CD4+CD25dim.
BCR signaling was performed as previously described(31). For BCR signaling, PBMCs were thawed, rested for1 h at 37°C in RPMI supplemented with 1% human serum(Gemini Bio-Products, West Sacramento, CA), and thenstimulated with F(ab9)2 fragment goat anti-human IgM(10 mg/mL) and F(ab9)2 goat anti-human IgD (10 mg/mL).Cells were fixed, permeabilized as above, and then stainedusing antibodies against CD27, CD20, and pPLC-g2(Y759).
Antibodies are listed in Supplementary Table 6. Datawere acquired using the following flow cytometers: BDLSR-II (B-cell immunophenotyping), BD FACSCalibur (IL-2/pSTAT5 phospho-flow and BCR signaling), and BDFACSCanto II (IL-21/pSTAT3 phospho-flow) (BD Bioscien-ces). All flow cytometric analysis was performed withFlowJo software (Tree Star, Inc.).
Treg Suppression AssayTeff resistance was determined using an in vitro Treg-mediated suppression assay (36,37). In brief, CD4+ T cellsdepleted of CD25hi cells were isolated from PBMCs usinga no-touch Miltenyi CD4 T Cell Isolation Kit II and positiveMiltenyi CD25 Microbeads II prior to staining with car-boxyfluorescein succinimidyl ester (Sigma-Aldrich). CD25+
CD127lo Tregs from a single healthy donor were sorted,expanded, and frozen as described and used a constantsource of Tregs for all suppression assays as previouslydescribed (37). CD4+CD25dim T cells (Teff) were culturedat 100,000 cells/well. Tregs were added at ratios of 1:4 and1:8 (Treg/Teff) and Dynabeads CD3/CD28 T Cell Expanderbead (Life Technologies) added at a ratio of 1:25 (beads/Teffs). On day 4, proliferation of live Teff was determinedby carboxyfluorescein succinimidyl ester dye dilution afterstaining cells with CD25, CD4, and LIVE/DEAD Far-RedDead Cell Stain Kit (Thermo Fisher Scientific).
Statistical AnalysisStatistical analysis was performed using GraphPad Prism7.04 software or R 3.4.3 software. False discovery rate wascontrolled using the Benjamini-Hochberg procedure, andP values ,0.05 were considered statistically significant.Values were considered outliers when they exceeded 1.5times interquartile range below the first quartile as de-termined using R or when detected using the ROUTmethod in Prism. To assess the significance of each patient
diabetes.diabetesjournals.org Habib and Associates 1241

feature while controlling for all others, IL-2 response andTeff resistance to Treg suppression were each modeled asdependent variables via simple and multivariable linearregression after each was logit transformed. In the simpleregression models, age and number of autoAbs were usedas the independent model features. For the multivariableregression, independent variables included: 1) fixed traitsincluding HLA, sex, and age, 2) progression status (non-progressor or progressor), number of autoAbs, and timepoint, and 3) clinical parameters: glucose (2-h oral glucose
tolerance test [OGTT]) and area under the curve (AUC)C-peptide (2-h OGTT). B-cell immunophenotyping andIL-21 response analyses used multivariable linear regressionwith log2-transformed response data and autoantibody-negative (autoAbneg) first-degree relatives (FDRs) as thereference group and adjusted for age, glucose (2-h OGTT),AUC C-peptide (2-h OGTT), and number of autoantibodies.IL-21/pSTAT3 response was modeled using a linear mixed-effects model in which we modeled the repeated measuresusing a random effect for individual. Because age is a known
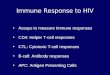
Figure 1—Teff response to IL-2 and Teff suppression by Treg is decreased in autoAb+ subjects. A: IL-2–mediated STAT5 phosphorylation inautoAbneg FDRs was compared with autoAb+ nonprogressors (Non-Prog) and autoAb+ progressors (Prog) in CD4+CD25dimCD45RO+
memory T cells at time 1, ages#18 years. Cells were activated with 25 IU/mL IL-2 for 10 min and then fixed, permeabilized, and stained withantibodies against pSTAT5 (pY694), CD25, CD4, and CD45RO. Percentage positive pSTAT5 was determined based on media stimulation ofthe same sample as shown in Supplementary Fig. 1A. Significance was determined using a Mann-Whitney two-tailed test. B: IL-2/pSTAT5response of Teff stratified by number of autoantibodies (numeric 0–4: includes autoAbneg FDRs, autoAb+ nonprogressors, and autoAb+
progressors) at time 1, ages #18 years. AutoAbs include microinsulin autoAb, GAD65 standard, IA-2, ICA, ICA512, and Zn transporter (ifassayed). Significance was determined using a one-way ANOVA (Kruskal-Wallace test) with Benjamini-Hochberg procedure for controllingfalse discovery rate. None of the comparisons was statistically significant. C: Treg suppression of CD4+CD25dim Teff in autoAbneg FDRs wascompared with autoAb+ nonprogressors and autoAb+ progressors in total CD4+ T cells at time 1. Percent suppression was determined asin Supplementary Fig. 1B. Significance was determined using Mann-Whitney two-tailed tests. None of the two-way comparisons werestatistically significant. D (left panel): Paired analysis of percent suppression between time 1 and time 2 for all autoAb+ subjects(nonprogressors and progressors) seropositive for two or more autoAbs. Significance was determined using a two-tailed Wilcoxonmatched-pairs signed rank test. D (right panel): Percent suppression of Teff stratified by number of autoantibodies (numeric 0–4: includesautoAbneg FDRs, autoAb+ nonprogressors, and autoAb+ progressors). AutoAbs include microinsulin autoAb, GAD65 standard, IA-2, ICA,ICA512, and Zn transporter (if assayed). Significance was determined using a one-way ANOVA (Kruskal-Wallace test) with Benjamini-Hochberg procedure for controlling false discovery rate. 0 vs. 3 autoAbs: P = 0.014; q = 0.06. All other comparisons were not statisticallysignificant.
1242 B and T Helper Cells in T1D Progression Diabetes Volume 68, June 2019

covariate for IL-2 response and transitional B-cell homeo-stasis (38,39), we limited our univariate analyses of thesedata to subjects #18 years of age.
RESULTS
Classification of At-Risk SubjectsAll at-risk individuals were participants in the Type 1 Di-abetes TrialNet PTP Trial (34,35) and classified as autoAbneg
or autoAb+ FDRs. Samples were obtained at two timepoints 6–12 months apart. Two cohorts of the autoAb+
individuals were selected: autoAb+ progressors and autoAb+
nonprogressors based on whether they developed clinicalT1D at or near the second time point. Due to limitedsample volumes, not all assays were conducted on eachindividual. Thus, three independent PTP cohorts wereused: cohort 1 for IL-2 response and Teff resistance(Supplementary Table 1), cohort 2 for B-cell immunophe-notyping and BCR signaling (Supplementary Table 2), andcohort 3 for IL-21 response (Supplementary Table 3).Supplementary Table 4 provides a summary of the cohortsfor age, sex, number of autoantibodies, and metabolicstatus, showing that they are well matched for age and sex.
IL-2 Response Is Decreased in AutoAb+ Subjects Priorto Disease OnsetWe and others have reported reduced IL-2 response in CD4+
CD45RO+ memory T cells associated with T1D and T1D-associated risk alleles (18,19,40,41). In this study, weassessed whether this phenotype precedes diagnosis inour risk-stratified cohort. We did not observe a dimin-ished IL-2 response in CD4+CD25+ T cells (data not shown),but did find that the IL-2 response in memory CD4+
CD25dimCD45RO+ T cells was decreased in autoAb+ subjectscompared with autoAbneg FDRs, most significantly betweenautoAb+ nonprogressors versus autoAbneg FDRs (Fig. 1A andSupplementary Fig. 1A). Within the CD4+ memory subset,decreased IL-2 signaling did not correlate with number ofautoAbs (Fig. 1B), which was confirmed by a multivariablemodel using autoAbneg FDRs as a reference group and adjust-ing for age. IL-2 response was negatively correlated withthe presence of autoAbs, irrespective of the number ofautoAbs or progressor status (autoAb+ nonprogressors: bcoefficient: 20.428, P , 0.05; autoAb+ progressors: bcoefficient: 20.601, P , 0.05). Together, these data dem-onstrate a decrease in IL-2 response among Teffs that ispresent early in the autoimmune process prior to or uponacquisition of autoantibodies.
Teff Resistance Increases With Disease ProgressionWe and others have previously shown that CD4+ Teffsare resistant to Treg suppression in established T1D(16,17,42–44). In this study, we tested whether Teff re-sistance occurs prior to T1D diagnosis using an in vitrosuppression assay (Supplementary Fig. 1B). There was nosignificant difference in CD4+CD25dim Teff suppressionbetween autoAbneg FDRs and autoAb+ subjects or within theautoAb+ cohort based on progression (Fig. 1C). However, we
did observe a significant decrease in suppression betweentime 1 and time 2 in autoAb+ subjects with two or moreautoantibodies. Stratification by number of autoantibodiesacross both time points revealed that percent suppressionwas significantly decreased in subjects with three autoAbs,as compared with autoAbneg FDRs (Fig. 1D). Multivariableregression analysis using autoAbneg FDR as the referencegroup and adjusting for age, glucose, and C-peptide con-firmed this significant association between development ofautoantibodies and percent suppression and revealed a sig-nificant relationship between Teff resistance and autoAb+
progressor status. Increased Teff resistance (decreased Teffsuppression) was positively correlated with number ofautoantibodies (b coefficient: 0.259; P , 0.001). Together,these findings suggest that Teff resistance is an acquiredtrait that, in part, correlates with increased autoimmunity.
Alterations in B-Cell Homeostasis in AutoAb+ SubjectsReflect Loss of Peripheral ToleranceWe have previously reported that individuals with long-standing T1D display an expanded population of transi-tional B cells and anergic (BND) B cells, a decrease in CD19+
CD27+ memory B cells, as well as an attenuated responseto BCR activation (29). More recently, Smith et al. (45)reported the loss or phenotypic alteration of high-affinityinsulin autoantigen-binding B cells from the peripheralBND anergic B-cell compartment of autoAb+ individualswith prediabetes, subjects with new-onset T1D, and someautoAbneg FDRs that correlated with a transient loss oftotal anergic BND B cells. Because these phenotypes reflectaltered B-cell tolerance, and pathogenic autoantibodiesmay result from B- and/or CD4+ T-cell–driven processes,we first determined whether altered B-cell homeostasisprecedes established disease. We found a modest decreasein naive B-cell frequency in autoAb+ progressors as com-pared with autoAbneg FDRs with no significant differencesin the memory and total B-cell frequencies between thecohorts (Supplementary Fig. 2). However, transitional Bcells were increased in the autoAb+ cohorts as comparedwith autoAbneg FDRs at time 1, with a similar trend at time2 (Fig. 2A and data not shown). In contrast, BND anergic Bcells were significantly decreased in the autoAb+ cohortscompared with autoAbneg FDRs most prominently at time2 (Fig. 2B and data not shown). Multivariable regressionanalyses using autoAbneg FDRs as the reference group andcontrolling for age and clinical variables confirmed theseresults. In this model, transitional B cells were increased inautoAb+ nonprogressors (b coefficient: 0.47; P = 0.065)and autoAb+ progressors (b coefficient: 1.075; P = 0.001) attime 1, and BND anergic B cells were decreased in autoAb+
nonprogressors (b coefficient: 21.202; P , 0.01) at time2. Glucose, C-peptide, and number of autoantibodies werenot significantly correlated with transitional B cell fre-quency in either autoAb+ nonprogressors or progressors,when controlling for age (data not shown). In contrast,glucose was a significant variable in the best fit model forBND B cell frequency at time 2 and was negatively correlated
diabetes.diabetesjournals.org Habib and Associates 1243

with percentage of BND B cells in autoAb+ progressors(b coefficient: 20.628; P = 0.012). Collectively, these datareveal homeostatic alterations in the B-cell compartment atperipheral tolerance checkpoints during progression to T1D,suggesting that B-cell–intrinsic mechanisms may contributeto an increased risk for the development of autoreactiveB-cell responses during the natural history of disease.
BCR Signaling Is Decreased in AutoAb+ Subjects WhoProgress to T1DOur prior studies demonstrated that BCR proximal signalsare blunted in naive and memory B cells in established T1D(29). In this study, we assessed proximal BCR responses bymeasuring phosphorylation of PLCg2 in the risk-stratifiedcohorts (Supplementary Fig. 3A–C). Fold change pPLCg2in B cells was not different between autoAbneg FDRs andautoAb+ subjects, but a significant decrease was seen inautoAb+ progressors compared with autoAb+ nonprogres-sors. This trait was observed at time 1 (Fig. 2C), persistedto time 2 (data not shown), and was most prominentwithin the naive B-cell compartment (Supplementary Fig.3B). Taken together, we believe that these data suggestthat the BCR response is blunted as one progresses toclinical disease and that this phenotype is more prominentin mature naive B cells.
IL-21 Signaling Is Enhanced Selectively in Naive B Cellsof AutoAb+ SubjectsGiven the role of IL-21 signaling in promoting the mat-uration of B cells and antibody production (46,47), wehypothesized that enhanced B-cell responsiveness to IL-21may be associated with the development of autoantibodiesin T1D. To test this, we analyzed IL-21–mediated STAT3phosphorylation across all time points and stratified byprogressor status or number of autoAbs. We observeda significant increase in fold change pSTAT3 in naive Bcells from autoAb+ nonprogressors compared with autoAbneg
FDRs and in subjects with two autoAbs versus zero or oneautoAb (Fig. 3A–C and Supplementary Fig. 4A and B). Amultivariable mixed-effects model, controlled for age andsex, revealed a significant correlation between IL-21 re-sponse and progressor status, further confirming the en-hanced IL-21 response in at-risk autoAb+ nonprogressors(Fig. 3A). This enhancement did not extend to autoAb+
progressors or to subjects with three or more autoAbs,suggesting that this phenotype is a dynamic trait overthe course of disease development (Fig. 3B and C). Insupport of this, paired analysis of fold change pSTAT3 innaive B cells showed no differences between times 1 and2 in autoAb+ nonprogressors, whereas a significant declinewas observed in autoAb+ progressors between time points(Fig. 3C). In order to determine whether this decline wasdue to changes in IL-21R expression, we assessed IL-21/pSTAT3 and IL-21R surface expression levels in parallel ina separate cohort of autoAb+ progressors (SupplementaryTable 5), distinct from cohort 3. In this new cohort, thedecline in IL-21 response between times 1 and 2 was
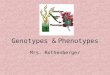
Figure 2—Naive B-cell homeostasis is altered in autoAb+ at-riskFDRs. A: Transitional B-cell frequency (as defined in SupplementaryFig. 2A) in autoAbneg FDR was compared with autoAb+ nonprogres-sors (Non-Prog) and autoAb+progressors (Prog) at time 1, ages #18years. Significance was determined using a Mann-Whitney two-tailedtest.B: BND B-cell frequency (as defined in Supplementary Fig. 2A) inyoung autoAb+ nonprogressors and autoAb+ progressors as com-pared with autoAbneg FDRs at time 2, ages #18 years. Significancewas determined using a two-tailed Mann-Whitney test and one-wayANOVA (Kruskal-Wallace test). C: Stratification of BCR response byautoAb status at time 1, ages #18 years. Signaling was quantifiedas in Supplementary Fig. 3A. Significance was determined usinga Mann-Whitney test. MFI, mean fluorescence intensity.
1244 B and T Helper Cells in T1D Progression Diabetes Volume 68, June 2019

replicated, but IL-21R expression levels were not signifi-cantly different between time points (Supplementary Fig.4C andD). This suggests that the dynamic response to IL-21in naive B cells from autoAb+ at-risk individuals is not solelydue to changes in IL-21R expression. Further, IL-21 re-sponse in naive B cells from a cohort of 100 subjects withestablished T1D was significantly decreased as comparedwith well-matched healthy individuals (Fig. 3D). This wasalso evident by a decreased frequency of pSTAT3-positivecells (data not shown). This result implies that decreasedresponse to IL-21 in naive B cells may be an acquired featurethat persists in established disease. Thus, these data revealenhanced naive B-cell responses to IL-21 that occur early inautoimmunity and decline near onset of clinical diabetes.
Recovery of BCR Signaling Differentiates Responses toRituximabGiven our data suggesting that blunted BCR signalingphenotype and Teff resistance are acquired traits, al-though IL-2–induced pSTAT5 was fixed, we examinedhow these traits were influenced by an interventionthat slowed the loss of C-peptide. We assessed samplesfrom new-onset T1D treated with rituximab (33). We didnot observe any changes in IL-2–induced pSTAT5, but didobserve a significant albeit modest decrease in the sup-pression of Teffs at week 12 in individuals treated withrituximab, the time at which the initial improvement inmean C-peptide levels from baseline was observed (Sup-plementary Fig. 5A).
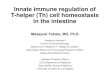
Figure 3—Enhanced IL-21 responsiveness in naive B cells from autoAb+ at-risk FDRs and diminished IL-21 signaling in autoAb+ FDRs whoprogress to T1D. Thawed PBMCs were rested in serum-free X-VIVO 15 medium for 1 h, washed with PBS, and stimulated with recombinanthuman IL-21 (0.1 ng/mL or 50 ng/mL) (Miltenyi Biotec) for 10 min. Cells were fixed, permeabilized, and stained with antibodies againstpSTAT3 (pY705), CD3, CD4, CD45RA, CD8, CD20, and CD27. A and B: Multivariable statistical analysis on combined time point data fornaive B-cell response to 0.1 ng/mL IL-21 was performed using a mixed-effects linear model of log2-transformed fold change meanfluorescence intensity (MFI) pSTAT3 log2(FC pSTAT3) with variables including cohort (autoAbneg FDR, autoAb+ non-progressor [Non-Prog],and autoAb+ progressor [Prog]), number of autoantibodies (numeric, 0–4), time point, age, glucose, and 2-h AUC C-peptide. A: Modeled bycohort. Statistical significance was determined by ANOVA: P = 0.0273; pairwise comparisons were done using a Mann-Whitney two-tailedtest. B: Modeled by number of autoantibodies. Statistical significance was determined by ANOVA with multiple comparisons testing: 0 vs.2 autoAbs, P = 0.030; 1 vs. 2 autoAbs, P = 0.052; 0 vs. 3 autoAbs, P = 0.123; and 0 vs. 4 autoAbs, P = 0.307. Time point, age, and metabolicparameters were not significant in this model. C: Paired analysis of fold change MFI pSTAT3 by time point for autoAb+ cohorts followingstimulation with 0.1 ng/mL IL-21. Significance was determined using two-tailed Mann-Whitney and Wilcoxon signed-rank tests. D: Analysisof IL-21/pSTAT3 response in adult healthy control subjects (N = 100) and subjects with T1D (n = 100) matched for sex, ethnicity, and age(control subjects, 18–49 years,mean 32.6 years; and T1D, 18–48 years, mean 32.5 years) from the BRI screened control and T1D repositories.Statistical significance was determined using a Mann-Whitney two-tailed test adjusted for multiple testing using the Benjamini-Hochbergmethod.
diabetes.diabetesjournals.org Habib and Associates 1245

As has been reported (33), rituximab treatment resultedin a decreased frequency of total, mature naive, andmemory B cells and increased frequency of transitionalB cells that did not differentiate responders from non-responders (Supplementary Fig. 5B and data not shown).BCR response at baseline did not determine clinical re-sponse to rituximab, as there was no significant differencein mean basal pPLCg2 at baseline or after treatmentbetween responders and nonresponders (SupplementaryFig. 5C). However, in rituximab-treated responders, theBCR response in total B cells at week 52 was significantlyincreased when compared with baseline (Fig. 4A), whichdid not correlate with IgM/IgD expression (data notshown). Together, these data suggest that BCR signaling“recovered” in responders to rituximab, whereas otherimmune features remained unchanged.
The source of the recovery of B-cell signaling may be dueto direct effects of rituximab on B cells or the result of analtered immune milieu in individuals who respond totreatment. At week 52, we did not observe significantdifferences in composition of the B-cell compartmentbetween responders and nonresponders (data not shown).To address whether improved BCR response is a functionof being a clinical responder per se, independent of thetherapeutic intervention, we assessed change in BCR re-sponse in the T1DAL trial, which demonstrated that alefacept-mediated depletion of pathogenic T cells could preserve mean4-h AUC C-peptide and improve glycemic control (32). Incontrast to our rituximab findings, BCR response was notsignificantly improved in B cells from alefacept-treated T1DALparticipants who had sustained 2-h AUC C-peptide at6 months (clinical responders, as defined by the rituximabtrial [33,48]) (Fig. 5B). These combined findings indicatethat alterations in BCR response in rituximab-treatedsubjects are likely due to a direct effect of the drug onB-cell depletion and that it may be therapeutically effec-tive in a subgroup of individuals for whom B-cell hyper-responsiveness is a driver of early disease.
DISCUSSION
The goal of this study was to provide the community witha broader understanding of the immune mechanisms in-volved in development of T1D. Using three independentlongitudinal at-risk cohorts, we provide new insight intohow these phenotypes evolve in the context of each other,thus providing a sequential model for better understand-ing the immune landscape of developing T1D (Fig. 5). Thefixed trait of reduced IL-2 response in autoAb+ FDRsprecedes homeostatic shifts in the immature and maturenaive B-cell subsets, and altered IL-21 and BCR signaling,with later acquisition of increased Teff resistance.
In at-risk T1D, it appears that certain B-cell phenotypesare consistent with those found in established T1D,whereas others are unique to the at-risk population. Forexample, the expanded transitional B-cell compartment inautoAb+ subjects as compared with autoAbneg FDRs mayreflect early B-cell selection defect(s) that result in anincrease in autoreactive B cells in the periphery, as describedin established T1D (28). Notably, our finding of reducedanergic BND B cells in autoAb+ subjects as compared withautoAbneg FDRs, together with the significant correlationbetween BND frequency and glucose levels, is consistent withthe results of Smith et al. (45,49), who reported tran-sient reduction of BND B cells among total B cells in theperiphery of subjects with prediabetes and new-onset T1D.More recently, this group found that insulin-binding B cellswere polyreactive and exhibited features associated withautoreactivity and autoantibodies (49). Interestingly, thisstudy also reported that high-risk HLA alleles and a subsetof non-HLA risk alleles were associated with loss of B-cellanergy. Given these associations, we explored these relation-ships in our at-risk cohort. The presence of high-risk HLA
Figure 4—BCR response is significantly increased in the rituximabtrial participants with sustained C-peptide at 1 year. A: Rituximabtrial participant samples from pretreatment (BL) and week 52 (Wk52) time points were assayed for BCR response as described inSupplementary Fig. 3A. Significantly increased fold change pPLCg2in total B cells from active treatment responders at 1-year post-therapy is shown (determined by a paired Wilcoxon signed-ranktest). B: T1DAL trial participant samples from pretreatment and week52 time points were assayed for BCR response as described inSupplementary Fig 3A. Statistical significance was determined bya paired Wilcoxon signed-rank test. Responder/nonresponder statusis defined using the rituximab trial definition based on 2-h mixed-mealtolerance test assay results at week 24 (48).
1246 B and T Helper Cells in T1D Progression Diabetes Volume 68, June 2019

class II alleles (DR3, DR4, or DR3/DR4) did not associate withtotal BND B cells in autoAbneg FDRs, autoAb+ nonprogres-sors, and autoAb+ progressors at either time point, includ-ing when glucose was included in the model. In addition,HLA class II genotype did not affect the difference infrequency of BND B cells between autoAbneg FDRs andautoAb+ progressors. For the non-HLA risk alleles, wefocused on PTPN22 but were limited by the small numberof subjects who carried the risk variant. However, whenrestricting our analysis to subjects who carry the nonriskallele of PTPT22, we found trends suggesting an associationwith increased transitional B cells and blunted BCR signal-ing in autoAb+ progressors (data not shown). Collectively,these findings implicate breach of anergy as a mechanismpredisposing at-risk individuals toward autoimmunity,a mechanism that is potentially influenced by extrinsicand/or genetic factors.
Previous human studies have suggested that BCR hypo-responsiveness leads to increased numbers of self-reactivetransitional B cells in the setting of T1D (29,50), thus ourobservation that blunted BCR response is an acquiredphenotype of at-risk subjects near clinical diagnosis wasunexpected. Early-stage BCR responsiveness in autoAb+
nonprogressors, together with enhanced IL-21 response,implies a cooperative mechanism to promote the matura-tion of autoreactive B cells and production of autoanti-bodies. Our findings further implicate T-cell–B-cellcooperative interactions in the development of disease.Reduced IL-2 response may impact the balance betweentolerance and immunity by impairing Treg fitness while
promoting expansion of Tfh and T helper 17 cells, all ofwhich have been described in subjects with long-standingT1D (12,18,51). In this study, the blunted IL-2 responsewas evident in autoAb+ FDRs, indicating that this may be afixed feature in T1D driven in part by early inflammatoryand genetic factors. This phenotype in the at-risk cohortwas most significant in CD4+ memory T cells and was notobserved in Tregs. In addition to its role in Treg develop-ment and stability, IL-2 has also been shown to inhibitTfh-cell differentiation (12,52,53). The presence of im-paired IL-2 responses in CD4 T cells at the time of autoAbdevelopment suggest that it may promote the develop-ment of Tfh and bidirectional B-cell–T-cell interactions inthe drive toward islet autoAb development. This is sup-ported by studies in T1D that demonstrate a correlationbetween IL-2 response and Tfh frequency and studiesthat have demonstrated increases in circulating Tfh in theat-risk population (12,15). Our study also revealed anenhanced B-cell response to IL-21 that is present in at-risk autoAb+ FDRs and attenuated as these individualsprogress toward clinical disease. This is consistent withan early priming of naive B cells for the generation ofpathogenic B-cell effectors, whereas the dampened responsemay reflect an exogenous effect of metabolic or inflamma-tory factors or a compensatory mechanism that influencesIL-21 responsiveness. As we found with BCR signaling,augmented IL-21 response is not seen in establishedT1D. An outstanding question is whether autoAbneg
FDRs display altered IL-21 response over time. Althoughthis was not specifically addressed in this study, we show
Figure 5—Sequential model of the evolution of T- and B-cell phenotypes. Our findings yield unique insight into whether specific traits are“fixed” (arise early and persist into later disease stages; e.g., IL-2/pSTAT5 and increased transitional B cells), potentially because of genetic/epigenetic programs or early inflammation, or “acquired” (develop near or at disease manifestation, e.g., increased Teff resistance to Tregsuppression and decreased BND B cells). These findings further reveal dynamic responses in B cells along the T1D continuum (BCR signaling andIL-21/pSTAT3 response), providing abetter understandingof howandwhen thesepotentially cooperativeB- andT- cell processesmaybeoptimallytargeted with combination therapies. Black font indicates findings published previously; red font indicates findings described in this study.
diabetes.diabetesjournals.org Habib and Associates 1247

that individuals with a single autoantibody across both timepoints did not display enhanced IL-21 response comparedwith autoAbneg FDRs. Further, previous studies demon-strate that positivity for two or more autoAbs, but notzero to one autoAbs, identifies a subgroup of patients withincreased Tfh activation and greater treatment efficacy withrituximab at disease onset (15). Based on these findings, wewould predict that interventions targeting IL-21 might bebest used in prevention in autoAb+ at risk, but not inestablished disease.
Tregs have a well-established role in protection fromT1D (8,54), and resistance of Teffs to Tregs has been welldescribed in established T1D (16,17). In this study, Tregfunction was not assessed due to limitations of samplequantities, but the response of Teff to Treg was measured.In addition, although we were unable to match our cohortsfor HLA due to the enrichment of HLA DR3 and DR4alleles in autoAb+ subjects as compared with autoAbneg
FDRs in the TrialNet cohort, we did examine the influenceof HLA class II genotype with respect to our findings. Usinga multivariable logistic model with HLA included in themodel, we found no significant association between IL-2/pSTAT5 and HLA DR3, DR4, or DQ0602. However, we didobserve that the presence of DQB1*0602 was negativelyassociated with Teff resistance. Although we were unableto address the role of HLA in disease progression in autoAb+
subjects because the majority of HLA DQB1*0602 sub-jects in our study were in the autoAbneg FDR cohort, thisfinding does suggest that the protective genetic role forDQB1*0602 may in part be due to responsiveness of Teffto Treg. Importantly, Teff resistance was still significantlyincreased in autoAb+ progressors when HLA was includedin our modeling. In the at-risk cohort, we found that Teffresistance was acquired in FDRs positive for two or moreautoAbs, consistent with the acquisition of Teff resistancewith age in the NOD mouse (42,43). This finding suggeststhat the mechanism(s) that drive Teff resistance may bedue to increased inflammatory signals, consistent with stud-ies showing that Teff resistance is often most pronouncedduring disease flares (55) or at sites of inflammation (56–58)in other autoimmune diseases. One factor not tested in ourstudy is a failure of Treg function itself, which, if aberrantearly in disease, could contribute to an inflammatory envi-ronment, which would promote Teff resistance.
Consistent with our finding that Teff resistance isacquired in T1D, a recent study by Ihantola et al. (44)of autoAb+ subjects with prediabetes versus newly diag-nosed and long-standing T1D confirmed the presence ofthe Teff resistance phenotype at later stages of autoim-munity and in established disease, but not in the at-riskpopulation. Importantly, the authors demonstrate that theresistance phenotype in T1D is mediated via STAT3 sig-nals, further linking Teff resistance to the proinflamma-tory cytokine milieu (20). Together with our findings, thesestudies suggest that interventions that target Teff resis-tance mechanisms may be most successful after the de-velopment of a single autoantibody, with the additional
goal of preventing epitope spreading and the acquisition ofadditional islet autoAb specificities. Importantly, a sourcefor the development of Teff resistance may be an earlierfailure of Treg themselves, which would support the use ofTreg therapy in T1D, either prior to the development ofTeff resistance or in combination with interventions thattarget Teff resistance directly.
We also addressed whether the observed B-cell pheno-types predicted response to an intervention targeting Bcells. Although we were unable to find a variable thatpredicted which individuals retained C-peptide, this anal-ysis yielded several important observations. We observedimprovement in BCR signaling among the individuals whoretained C-peptide with rituximab treatment; by contrast,this was not observed in alefacept-treated subjects, indicat-ing that the change was not due to the improved metabolicparameters, but was instead unique to individuals whoresponded to B-cell depletion with rituximab. This suggeststhat the enhanced BCR signaling that occurs after rituximabtherapy may promote a reset of the native BCR signalingas the B-cell compartment repopulates. The fact that wesee this only in individuals who respond favorably to thetherapy may indicate that these individuals have a diseasethat is more predominantly driven by B cells. Accordingly,the enhanced BCR signaling may not reflect an improve-ment in the B-cell response; rather, it may return the B cellsto a more potentially pathogenic, responsive state.
As a community, we have an ever-growing understand-ing of the genetic factors that predispose to T1D andfeatures of the immune response that are altered inindividuals with T1D. However, in order to develop effec-tive strategies to intervene and prevent disease, we mustunderstand these factors in the context of the trajectory ofdisease progression. In this study, we have used longitu-dinal samples from at-risk cohorts to demonstrate thatdistinct immune phenotypes arise at different times todiagnosis and, importantly, may be transient. Our novelfindings provide a more nuanced understanding of theimmune processes that precede disease and, importantly,complement the mechanistic insights gained to date fromprevention studies (59). For example, early stable changesin IL-2 responsiveness as reported in this study thatprecede or coincide with transiently altered B-cell responsesmay inform selection of subjects for sequential immunetherapies that first target B cells with rituximab, followed byspecific interventions that target enhanced B-cell and Teffresponses to promote a more sustained preservation ofC-peptide. More focused longitudinal studies of FDRs be-fore and after seroconversion will further distinguish un-derlying autoimmune mechanisms (genetic risk vs. earlyautoimmune inflammation), with implications that willinform optimal timing of interventions.
Acknowledgments. The authors thank Dr. Cate Speake (BRI, Seattle, WA)for helpful discussion about the manuscript and longitudinal studies in at-riskpopulations and Dr. Matt Dufort (BRI, Seattle, WA) for assistance with statistical
1248 B and T Helper Cells in T1D Progression Diabetes Volume 68, June 2019

modeling. The authors also thank the investigators and staff of the BRI TranslationalResearch Program and BRI Diabetes Research Program for recruitment of healthycontrol subjects and subjects with established T1D, respectively, as well as the BRITranslational Research Clinical Core for sample processing and handling. The authorsacknowledge the support of the Type 1 Diabetes TrialNet PTP Study Group, whichidentified study participants and provided samples and follow-up data for this study.Funding. This work was supported by National Institutes of Health (NIH) grantsRC4-DK-090796, U01-AI-101990-03, and DP3-DK-104466 to J.H.B. and a JDRFCareer Development Award (3-2012-205) to S.A.L. The Type 1 Diabetes TrialNetPTP Study Group is a clinical trials network funded by the NIH through the NationalInstitute of Diabetes and Digestive and Kidney Diseases, the National Institute ofAllergy and Infectious Diseases, and the Eunice Kennedy Shriver National Instituteof Child Health and Human Development through cooperative agreements U01-DK-061010, U01-DK-061034, U01-DK-061042, U01-DK-061058, U01-DK-085465, U01-DK-085453, U01-DK-085461, U01-DK-085466, U01-DK-085499,U01-DK-085504, U01-DK-085509, U01-DK-103180, U01-DK-103153, U01-DK-085476, U01-DK-103266, U01-DK-103282, U01-DK-106984, U01-DK-106994,U01-DK-107013, U01-DK-107014, and UC4-DK-106993 and JDRF. Research speci-mens from the ITN045AI T1DAL trial reported in this study were provided by theImmune Tolerance Network and supported by the National Institute of Allergyand Infectious Diseases of the NIH under award number UM1-AI-109565.
The contents of this article are solely the responsibility of the authors and do notnecessarily represent the official views of the NIH or JDRF.Duality of Interest. No potential conflicts of interest relevant to this articlewere reported.Author Contributions. T.H. designed and performed B-cell experiments,analyzed data, and wrote the manuscript. S.A.L. designed T-cell experiments,analyzed data, and wrote the manuscript. P.L.S. performed T-cell experiments andanalyzed data. A.B. and A.F. performed B-cell experiments and analyzed data. M.T.performed T- and B-cell experiments and analyzed data. A.M.H. contributed todata analysis and wrote the manuscript. K.C. and C.G. contributed to experimentaldesign and reviewed and edited the manuscript. M.T.M. and E.W. performed dataanalysis including statistical modeling. D.J.R. conceived the project and contrib-uted to experimental design. J.H.B. conceived the project, designed experiments,analyzed data, and wrote the manuscript. The Type 1 Diabetes TrialNet StudyGroup provided the samples and associated clinical data and contributed to thewriting of the manuscript. J.H.B. is the guarantor of this work and, as such, had fullaccess to all of the data in the study and takes responsibility for the integrity of thedata and the accuracy of the data analysis.Prior Presentation. Parts of this study were presented in poster form atthe Federation of Clinical Immunology Societies (FOCIS) 2018 Annual Meeting,San Francisco, CA, 20–23 June 2018.
References1. Atkinson MA. The pathogenesis and natural history of type 1 diabetes. ColdSpring Harb Perspect Med 2012;2:a0076412. Bonifacio E, Ziegler AG. Advances in the prediction and natural history of type1 diabetes. Endocrinol Metab Clin North Am 2010;39:513–5253. Sosenko JM, Skyler JS, DiMeglio LA, et al.; Type 1 Diabetes TrialNet StudyGroup; Diabetes Prevention Trial-Type 1 Study Group. A new approach for di-agnosing type 1 diabetes in autoantibody-positive individuals based on predictionand natural history. Diabetes Care 2015;38:271–2764. Gallagher MP, Goland RS, Greenbaum CJ. Making progress: preserving betacells in type 1 diabetes. Ann N Y Acad Sci 2011;1243:119–1345. Lord S, Greenbaum CJ. Disease modifying therapies in type 1 diabetes:where have we been, and where are we going? Pharmacol Res 2015;98:3–86. Ehlers MR. Strategies for clinical trials in type 1 diabetes. J Autoimmun 2016;71:88–967. Garyu JW, Meffre E, Cotsapas C, Herold KC. Progress and challenges fortreating Type 1 diabetes. J Autoimmun 2016;71:1–98. Bettini M, Vignali DA. T cell-driven initiation and propagation of autoimmunediabetes. Curr Opin Immunol 2011;23:754–760
9. Petersen LD, Duinkerken G, Bruining GJ, van Lier RA, de Vries RR, Roep BO.Increased numbers of in vivo activated T cells in patients with recent onset insulin-dependent diabetes mellitus. J Autoimmun 1996;9:731–73710. Matteucci E, Ghimenti M, Di Beo S, Giampietro O. Altered proportions ofnaïve, central memory and terminally differentiated central memory subsetsamong CD4+ and CD8 + T cells expressing CD26 in patients with type 1 diabetes.J Clin Immunol 2011;31:977–98411. Buckner JH, Nepom GT. Obstacles and opportunities for targeting the effectorT cell response in type 1 diabetes. J Autoimmun 2016;71:44–5012. Kenefeck R, Wang CJ, Kapadi T, et al. Follicular helper T cell signature in type1 diabetes. J Clin Invest 2015;125:292–30313. Xu X, Shi Y, Cai Y, et al. Inhibition of increased circulating Tfh cell by anti-CD20 monoclonal antibody in patients with type 1 diabetes. PLoS One 2013;8:e7985814. Ferreira RC, Simons HZ, Thompson WS, et al. IL-21 production by CD4+effector T cells and frequency of circulating follicular helper T cells are increased intype 1 diabetes patients. Diabetologia 2015;58:781–79015. Viisanen T, Ihantola EL, Näntö-Salonen K, et al. Circulating CXCR5+PD-1+ICOS+ follicular T helper cells are increased close to the diagnosis of type1 diabetes in children with multiple autoantibodies. Diabetes 2017;66:437–44716. Schneider A, Rieck M, Sanda S, Pihoker C, Greenbaum C, Buckner JH. Theeffector T cells of diabetic subjects are resistant to regulation via CD4+ FOXP3+regulatory T cells. J Immunol 2008;181:7350–735517. Lawson JM, Tremble J, Dayan C, et al. Increased resistance to CD4+CD25hiregulatory T cell-mediated suppression in patients with type 1 diabetes. Clin ExpImmunol 2008;154:353–35918. Long SA, Cerosaletti K, Bollyky PL, et al. Defects in IL-2R signaling contributeto diminished maintenance of FOXP3 expression in CD4(+)CD25(+) regulatoryT-cells of type 1 diabetic subjects. Diabetes 2010;59:407–41519. Schwedhelm K, Thorpe J, Murray SA, et al. Attenuated IL-2R signaling in CD4memory T cells of T1D subjects is intrinsic and dependent on activation state. ClinImmunol 2017;181:67–7420. Hundhausen C, Roth A, Whalen E, et al. Enhanced T cell responses to IL-6 intype 1 diabetes are associated with early clinical disease and increased IL-6receptor expression. Sci Transl Med 2016;8:356ra11921. Mariño E, Grey ST. B cells as effectors and regulators of autoimmunity.Autoimmunity 2012;45:377–38722. Khan WN, Wright JA, Kleiman E, Boucher JC, Castro I, Clark ES. B-lymphocytetolerance and effector function in immunity and autoimmunity. Immunol Res 2013;57:335–35323. Franks SE, Getahun A, Hogarth PM, Cambier JC. Targeting B cells intreatment of autoimmunity. Curr Opin Immunol 2016;43:39–4524. O’Neill SK, Liu E, Cambier JC. Change you can B(cell)eive in: recent progressconfirms a critical role for B cells in type 1 diabetes. Curr Opin Endocrinol DiabetesObes 2009;16:293–29825. Kochi Y, Myouzen K, Yamada R, et al. FCRL3, an autoimmune susceptibilitygene, has inhibitory potential on B-cell receptor-mediated signaling. J Immunol2009;183:5502–551026. Kozyrev SV, Abelson AK, Wojcik J, et al. Functional variants in the B-cell geneBANK1 are associated with systemic lupus erythematosus [published correctionappears in Nat Genet 2008;40:484]. Nat Genet 2008;40:211–21627. Li X, Ptacek TS, Brown EE, Edberg JC. Fcgamma receptors: structure,function and role as genetic risk factors in SLE. Genes Immun 2009;10:380–38928. Menard L, Saadoun D, Isnardi I, et al. The PTPN22 allele encoding an R620Wvariant interferes with the removal of developing autoreactive B cells in humans. JClin Invest 2011;121:3635–364429. Habib T, Funk A, Rieck M, et al. Altered B cell homeostasis is associated withtype I diabetes and carriers of the PTPN22 allelic variant. J Immunol 2012;188:487–49630. Manjarrez-Orduño N, Marasco E, Chung SA, et al. CSK regulatory poly-morphism is associated with systemic lupus erythematosus and influences B-cellsignaling and activation. Nat Genet 2012;44:1227–1230
diabetes.diabetesjournals.org Habib and Associates 1249

31. Dam EM, Habib T, Chen J, et al. The BANK1 SLE-risk variants are associatedwith alterations in peripheral B cell signaling and development in humans. ClinImmunol 2016;173:171–18032. Rigby MR, DiMeglio LA, Rendell MS, et al.; T1DAL Study Team. Targeting ofmemory T cells with alefacept in new-onset type 1 diabetes (T1DAL study):12 month results of a randomised, double-blind, placebo-controlled phase 2 trial.Lancet Diabetes Endocrinol 2013;1:284–29433. Pescovitz MD, Greenbaum CJ, Krause-Steinrauf H, et al.; Type 1 DiabetesTrialNet Anti-CD20 Study Group. Rituximab, B-lymphocyte depletion, and pres-ervation of beta-cell function. N Engl J Med 2009;361:2143–215234. Mahon JL, Sosenko JM, Rafkin-Mervis L, et al.; TrialNet Natural HistoryCommittee; Type 1 Diabetes TrialNet Study Group. The TrialNet Natural HistoryStudy of the Development of Type 1 Diabetes: objectives, design, and initialresults. Pediatr Diabetes 2009;10:97–10435. Herold KC, Usmani-Brown S, Ghazi T, et al.; Type 1 Diabetes TrialNet StudyGroup. b cell death and dysfunction during type 1 diabetes development in at-riskindividuals. J Clin Invest 2015;125:1163–117336. Schneider A, Buckner JH. Assessment of suppressive capacity by humanregulatory T cells using a reproducible, bi-directional CFSE-based in vitro assay.Methods Mol Biol 2011;707:233–24137. Putnam AL, Brusko TM, Lee MR, et al. Expansion of human regulatory T-cellsfrom patients with type 1 diabetes. Diabetes 2009;58:652–66238. Johnson SA, Cambier JC. Ageing, autoimmunity and arthritis: senescence ofthe B cell compartment - implications for humoral immunity. Arthritis Res Ther2004;6:131–13939. Morbach H, Eichhorn EM, Liese JG, Girschick HJ. Reference values for B cellsubpopulations from infancy to adulthood. Clin Exp Immunol 2010;162:271–27940. Garg G, Tyler JR, Yang JH, et al. Type 1 diabetes-associated IL2RA variationlowers IL-2 signaling and contributes to diminished CD4+CD25+ regulatory T cellfunction. J Immunol 2012;188:4644–465341. Downes K, Marcovecchio ML, Clarke P, et al. Plasma concentrations ofsoluble IL-2 receptor a (CD25) are increased in type 1 diabetes and associatedwith reduced C-peptide levels in young patients. Diabetologia 2014;57:366–37242. You S, Belghith M, Cobbold S, et al. Autoimmune diabetes onset results fromqualitative rather than quantitative age-dependent changes in pathogenic T-cells.Diabetes 2005;54:1415–142243. Wu G, Lu ZH, Gabius HJ, Ledeen RW, Bleich D. Ganglioside GM1 deficiency ineffector T cells from NODmice induces resistance to regulatory T-cell suppression.Diabetes 2011;60:2341–234944. Ihantola E-L, Viisanen T, Gazali AM, et al. Effector T cell resistance tosuppression and STAT3 signaling during the development of human type 1 di-abetes. J Immunol 2018;201:1144–1153
45. Smith MJ, Packard TA, O’Neill SK, et al. Loss of anergic B cells in prediabeticand new-onset type 1 diabetic patients. Diabetes 2015;64:1703–171246. Good KL, Bryant VL, Tangye SG. Kinetics of human B cell behavior andamplification of proliferative responses following stimulation with IL-21. J Immunol2006;177:5236–524747. Ettinger R, Sims GP, Fairhurst AM, et al. IL-21 induces differentiation ofhuman naive and memory B cells into antibody-secreting plasma cells. J Immunol2005;175:7867–787948. Herold KC, Pescovitz MD, McGee P, et al.; Type 1 Diabetes TrialNet Anti-CD20 Study Group. Increased T cell proliferative responses to islet antigensidentify clinical responders to anti-CD20 monoclonal antibody (rituximab) therapyin type 1 diabetes. J Immunol 2011;187:1998–200549. Smith MJ, Rihanek M, Wasserfall C, et al. Loss of B-cell anergy in type1 diabetes is associated with high-risk HLA and non-HLA disease susceptibilityalleles. Diabetes 2018;67:697–70350. Schickel JN, Kuhny M, Baldo A, et al. PTPN22 inhibition resets defectivehuman central B cell tolerance. Sci Immunol 2016;1:aaf715351. McClymont SA, Putnam AL, Lee MR, et al. Plasticity of human regulatoryT cells in healthy subjects and patients with type 1 diabetes. J Immunol 2011;186:3918–392652. Johnston RJ, Choi YS, Diamond JA, Yang JA, Crotty S. STAT5 is a potentnegative regulator of TFH cell differentiation. J Exp Med 2012;209:243–25053. Ballesteros-Tato A, León B, Graf BA, et al. Interleukin-2 inhibits germinalcenter formation by limiting T follicular helper cell differentiation. Immunity 2012;36:847–85654. Bussone G, Mouthon L. Autoimmune manifestations in primary immunedeficiencies. Autoimmun Rev 2009;8:332–33655. Vargas-Rojas MI, Crispín JC, Richaud-Patin Y, Alcocer-Varela J. Quantitativeand qualitative normal regulatory T cells are not capable of inducing suppression inSLE patients due to T-cell resistance. Lupus 2008;17:289–29456. Beavis PA, Gregory B, Green P, et al. Resistance to regulatory T cell-mediatedsuppression in rheumatoid arthritis can be bypassed by ectopic foxp3 expression inpathogenic synovial T cells. Proc Natl Acad Sci U S A 2011;108:16717–1672257. Goodman WA, Young AB, McCormick TS, Cooper KD, Levine AD. Stat3phosphorylation mediates resistance of primary human T cells to regulatory T cellsuppression. J Immunol 2011;186:3336–334558. Wehrens EJ, Mijnheer G, Duurland CL, et al. Functional human regulatoryT cells fail to control autoimmune inflammation due to PKB/c-akt hyperactivation ineffector cells. Blood 2011;118:3538–354859. Greenbaum CJ, Speake C, Krischer J, et al. Strength in numbers: oppor-tunities for enhancing the development of effective treatments for type 1 diabetes-the TrialNet experience. Diabetes 2018;67:1216–1225
1250 B and T Helper Cells in T1D Progression Diabetes Volume 68, June 2019






![Immune development and environment: lessons from Amish and ... · life [26,44–48], but not with allergic phenotypes [26,37,45,49,50] risk (withtwoexceptions[51,52]).Infact,the for](https://img.pdfslide.us/doc/110x75/5f90cf25bfc3d901fb36ac29/immune-development-and-environment-lessons-from-amish-and-life-2644a48.jpg)