Embed Size (px)
Citation preview

590
once bone metastases occurred, cancer cure is no more possible and palliative therapy is the only viable approach. The commonest site of bone me-tastases is the vertebral bone marrow. The con-sequences are often significant morbidity and reduction in quality of life. In some cases, ver-tebral metastases do not cause symptoms. They often origin severe pain or reduction of mobility due to compression of the spinal cord by a direct mechanism or, indirectly, by causing a vertebral pathologic fracture.
In this scenario, the characterization of spinal bone marrow disorders is of vital importance for the management of oncological patients. Magne-tic resonance (MR) imaging plays a crucial role in differentiation. Different T1 and T2 relaxa-tion properties allow distinction of bone marrow lesion from normal bone marrow1,2. However, morphological MR sequences might fail in diffe-rentiating between malignant and benign lesion because signal characteristics may overlap. Fun-ctional MR imaging based on diffusion weighted imaging (DWI) and the derived apparent diffu-sion coefficient (ADC) maps may help define the nature of the lesion, offering both qualitative and quantitative information, respectively, on the stu-died tissue.
The basic principle of DWI is that water molecules in a tissue show a different Brow-nian motion depending on variations in micro-structure. Signal attenuation reflects the degree of water motion with a proportional relation-ship. ADC value allows the quantification of this Brownian motion, and is calculated from
Abstract. – Malignant spinal bone marrow disorders are one of the major causes of signifi-cant morbidity and reduction in quality of life in oncological patients. Thus, the characterization of these conditions is of crucial importance in the management of these patients.
Magnetic resonance (MR) imaging plays a vi-tal role in differentiation between benign and malignant spinal bone marrow disorders. How-ever, morphological imaging features, based on T1 and T2 relaxation properties, might fail in dif-ferentiating between these conditions because signal characteristics may overlap. Quantitative MR imaging based on diffusion weighted im-aging (DWI) and apparent diffusion coefficient (ADC) values has been proved to help in defin-ing the nature of the lesion. The aims of this pa-per were: to review basic principles of DWI tech-nique and ADC maps, to describe DWI and ADC maps appearances of normal vertebral bone marrow briefly, to discuss the DWI and ADC maps characteristics in vertebral malignant le-sions, to provide indications for differential di-agnosis between malignant and benign lesions.
Key Words: Bone marrow, Bone marrow disorders, Bone mar-
row, Magnetic resonance, Diffusion weighted imag-ing, Apparent diffusion coefficient.
Introduction
Metastatic bone disease is, unfortunately, a common event in the evolution of cancer. The development of metastases has a key impact on the management of oncological patients, because,
European Review for Medical and Pharmacological Sciences 2018; 22: 590-597
L. FILOGRANA1,2, N. MAGARELLI1, F. CELLINI1, S. MANFRIDA1, A. LEONE1, C. COLOSIMO1, V. VALENTINI1
1Department of Radiological Sciences, Catholic University of the Sacred Heart, Gemelli Foundation, School of Medicine, Rome, Italy2Department of Radiological Sciences, PhD Training Program in Oncological Sciences, Catholic University of the Sacred Heart, Gemelli Foundation, School of Medicine, Rome, Italy
Corresponding Author: Laura Filograna, MD; e-mail: [email protected]
Diffusion weighted imaging (DWI) and apparent diffusion coefficient (ADC) values for detection of malignant vertebral bone marrow lesions

DWI and ADC values for detection of malignant vertebral bone marrow lesions
591
maps derived by diffusional signal attenuation. Briefly, tissues with high free water compo-nent, like as those with lower content of mem-branes and intracellular organelles or high free extracellular water content show lower signal intensity on DWI and higher signal intensity on ADC maps in comparison to muscles. Conver-sely, tissues with restricted extracellular water content, like those with high cellularity, as tu-mors, show higher signal intensity on DWI and iso-hypointensity on ADC maps3.
DWI has a well-established role in the stu-dy of the central nervous system’s pathology4-6. Recently, this MRI technique has been em-ployed also in the musculoskeletal system for detection, characterization and monitoring of soft-tissue and osseous lesions in oncological patients7.
When a cancer spreads to new and different site, it very often locates in the axial skeleton, as metastases have a preferential tropism for red marrow contained in skeletal segments. For this reason, some authors8-11 have proposed the study of the whole spine for detection and fol-low-up of bone metastases, particularly those from prostatic cancer.
The aim of this paper was to illustrate the role of DWI imaging in the identification and characterization of malignant vertebral bone marrow lesions. In this study, after the intro-duction of basic principles of DWI and ADC maps, DWI appearances and ADC values of normal vertebral bone marrow will be descri-bed, and DWI and ADC maps characteristics in vertebral malignant lesions will be illustrated. Moreover, indications for differential diagnosis between vertebral malignant vs. benign lesions will be discussed.
DWI Basic Principles and TechniqueDWI technique finds its fundamentals in the
principles that regulate free water motion in the cellular environments. In all tissues, free and intra-cellular water molecules show a constant motion (Brownian motion) due to thermal kinetic energy. Whereas this motion is random for free extracel-lular water molecules, intracellular water’s motion is influenced by cell membranes and organelles12. This means that diffusion of water molecules de-pends strictly by the cellularity of the examined tissue, which influences the Brownian motion of both intracellular and extracellular water. The abi-lity of DWI to detect tumoral foci is explained by the fact that this technique provides visualization
and quantification of tissue water content. Tissues, like as cancerous tissue, hypercellular metastases and fibrosis, having increased cellularity, and thus, higher proportions of membranes, intracellular or-ganelles or restricted free extracellular space, show impeded water diffusibility compared with normal surrounding tissues. On the contrary, in tissues with less cellularity or also in necrotic regions of a tumour where disrupted cell membranes are preva-lent, diffusion is less restricted12,13.
DWI sequence is a spine-echo T2-weighted single shot sequence that derives from two sym-metric motion-probing gradient pulses about a 180° refocusing pulse. The first applied diffu-sion gradient causes a change of position of the phase shift; in a restricted environment the spins maintain their initial location along the gradient axis during the two pulses. Free water molecules, instead moving in the interval between the first and the second gradient when the second pulse arrive, will be subjected to a different field stren-gth, and will undergo a total phase shift, giving a decreased signal intensity on DWI image14. In other words, moving water molecules do not re-focus and show a signal loss on DWI. Conversely, water protons impeded by cellular membranes or intracellular organelles retain the signal and show hyperintensity on MR image.
The weighting to diffusion of DWI strictly de-pends on the b value. The b value is a parameter expressed in seconds per square millimeter that reflects the acquisition setup, i.e., the duration, amplitude, and temporal spacing of the two mo-tion-probing gradients. The b value determines the degree of the diffusion weighting with a di-rect proportion. The diffusion weighting incre-ases by increasing the b value. Lower b values, which mean higher T2 weighting, provide a high signal-to-noise ratio (SNR), but low definition in the diffusion. Generally, at least two different b values are used to extrapolate quantitative data. At our institution we use for the study of muscu-loskeletal system the b values of 0 and 800 s/mm.
The quantitative measurement of the Brownian motion is provided by the calculation of the ADC. Tissues with high cellularity and restricted diffu-sion of free extracellular water molecules exhibit low ADC values3. The ADC value is measured by tracing a region of interest (ROI) in the abnor-mal tissue. Thus, minimum, maximum, and mean ADC values are generated, representing the loga-rithmic decrease in signal intensity between two or more b values in the selected pixels, expressed in units of 10-3 × mm2/s.

L. Filograna, N. Magarelli, F. Cellini, S. Manfrida, A. Leone, C. Colosimo, V. Valentini
592
DWI of Normal Vertebral Bone MarrowThe behavior of normal bone marrow in DWI
and ADC maps pass through a deep understan-ding of the structural composition of this tissue. In adults, the bone marrow is constituted princi-pally by yellow bone barrow containing 80% of fat, 15% of water, and 5% of cellular components. In younger subjects, the prevalence of red bone marrow reflects in a different distribution of the same constituents: 40% of fat and water and 20% of cellular components16.
It has been demonstrated that normal yel-low bone marrow shows low signal intensity
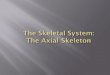
on DWI and low ADC values16,17 (Figure 1). This evidence has been explained as due to the prevalence of fat cells, that limits the presence of extracellular water, due to their hydropho-bic nature. Moreover, the yellow bone marrow, with its low cellular content, exhibits low perfu-sion18. Conversely, red marrow, with its higher cellularity and extracellular water content19,20, shows higher signal intensity on DWI and hi-gher ADC values than yellow bone marrow21-25. It has to be considered that vertebral metastases are more frequent in older subjects. Red bone marrow atrophy and trabecular bone loss are
Figure 1. 57-year-old man with normal vertebral bone morrow. Sagittal T1-weighted (a) and T2 fat saturated image (b), axial T1 weighted image at the level of D10 (c), show intermediate hyperintensity (a and c) and hypointensity (b) of the vertebral bodies in accordance with the prevalence of yellow bone marrow. Axial DWI image (d) and the corresponding ADC map in D10 at the same level (e) show low signal and high values (0.15 × 10-3 mm2/s), respectively

DWI and ADC values for detection of malignant vertebral bone marrow lesions
593
more evident after 40 years of age and in wo-man, probably due to estrogen deficiency and osteoporosis26,27. Both this evidence advantages the detection of hypercellular metastatic tissue.
Unlike other soft tissue cancer localizations, metastatic tissue colonizing yellow bone marrow displaces fat cells; the result is an increase of si-gnal intensity on DWI and an increment of ADC value (Figure 2).
DWI and ADC Maps in Vertebral Malignant Bone Marrow Disorders
MR imaging is the reference standard ima-ging modality for evaluating spinal lesions. The reason is mainly related to its excellent capacity of differentiating soft from bone tissue. Verte-bral metastases are generally classified as mo-stly destructive or osteolytic and mostly bone forming or osteoblastic (e.g., from prostatic carcinoma). Both types of vertebral metastasis appear on T1-weighted sequences as hypoin-tense lesions compared to fatty tissue, due to the replacement of adipose cells by tumor cells (Figure 2). On T2-weighted images the signal characteristics are more variable in relation to the water content of the metastases. However, they generally appear as more or less hyperin-tense lesions15 (Figure 2). In addition, around the lesion a hyperintense halo is visible, due to perilesional edema28,29. Nevertheless, morpho-logical sequences are often insufficient in di-stinguishing malignant from benign vertebral bone marrow lesions, due to overlapping fea-tures, or the coexistence of bone marrow ede-ma caused for example by fractures, infection, bone marrow hyperplasia related to therapy.
DWI and ADC maps have been proposed for the discrimination of malignant lesions, especial-ly in these particular conditions30-32.
Generally, bone marrow vertebral metastases appear on DWI as high signal intensity areas in an otherwise hypointense vertebral soma. These areas correspond to low signal intensities on ADC maps (Figure 2).
It is well known that bone metastases can be prevalently lytic or sclerotic. Although in both types of metastases the bone turnover is more pronounced than in normal bone marrow, in osteolytic metastases, the osteoclastic activity is prevalent as it is stimulated by the adjacent me-tastatic tumor cells. Conversely, the osteoblastic metastases origin from the prevalent stimulation of osteoblasts.
Osteolytic lesions are better detected on DWI imaging, due to the higher content of water and cells with respect to the sclerotic ones33.
It has to be considered, as mentioned above, that the behavior of vertebral malignant lesion on DWI and ADC map against normal tissue is different from that of other soft tissue malignant lesions. In fact, whereas in soft tissue malignant lesions show high signal intensity on DWI and lower ADC va-lues than the corresponding normal tissue, ma-lignant yellow bone marrow lesions show high signal intensity on DWI, but higher ADC values than normal yellow bone marrow22,23,33-35 (Figures 1, 2). As explained above, this is due to the fact that tumor cells infiltrating bone marrow displace fat cells, thus increasing cellular and water proton density, and augmenting blood perfusion19,24,36-38.
Padhani et al35 in 2013 and other previous stu-dies22,24,39 demonstrated statistically significant
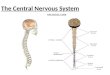
Figure 2. 45-year-old woman with breast carcinoma. T1 (a) and T2 fat saturated (b) images show the presence of two lumbar metastatic lesion respectively hypo- and hyperintense with respect to the surrounding tissue. The corresponding DWI image (c) demonstrates hyperhyntense lesions, that show on ADC map, values of 0.78-0.82 × 10-3 mm2/s.

L. Filograna, N. Magarelli, F. Cellini, S. Manfrida, A. Leone, C. Colosimo, V. Valentini
594
differences in signal intensity and ADC values of metastatic and normal yellow bone marrow. Parti-cularly, Padhani et al35 demonstrated that the 95th percentile and maximum values for mean tumor ADC distribution were 1.2 × 10-3 mm2/s and 1.4 × 10-3 mm2/s. The ADC cut-off value for distingui-shing between normal and malignant bone mar-row was settled at 0.774 × 10-3 mm2/s by Padhani et al35, and at 0.655 × 10-3 mm2/s by Messiou et al24. This means that when the presence of a verte-bral lesion is suspected in an oncological patient, the high signal intensity on DWI and ADC values above at least 0.655 × 10-3 mm2/s suggests the ma-lignant nature of the alteration. However, it has to be specified that this is truer for yellow bone mar-row. In younger patient, with an higher proportion of red bone marrow, or in patients treated with stimulating factors like G-CSF, because of higher signal intensity and ADC values of normal bone marrow related to higher cellular density and per-fusion, the differences in DWI signal intensity and ADC values between malignant and normal bone marrow are narrower.
Another major problem in oncological patien-ts is the differentiation between pathological vs. osteoporotic fracture. Also in this case, the use of DWI and ADC maps can be useful for diffe-rentiation. Bone marrow edema, that means the water proton density and interstitial space, is sup-posed to be superior in non-pathological fractures than in pathological ones. In fact, in pathological fractures, tumor cells infiltrating bone marrow cause restriction of interstitial space and a displa-cement of water molecules. The result is the evi-dence of higher DWI signal intensity and lower ADC values in pathological fractures with respect to what observed in osteoporotic fractures40,41.
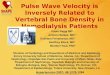
In a comprehensive review of the literature, Dietrich et al42 suggested the following differen-tiating ADC values: the ADC value of normal vertebral bone marrow is typically found to be between 0.2 and 0.6 × 10-3 mm2/s, ADC value in osteoporotic fractures are generally between 1.2 and 2.0 × 10-3 mm2/s, superior to that of malignant fractures or lesions, typically between 0.7 and 1.3 × 10-3 mm2/s (Figure 3).
About the differentiation between malignant and benign lesions, the literature offers some in-dications (Figure 4). Dietrich et al41 summarizing the results of some studies on the issue23,25,43-46 identified a mean value of 1.2 × 10-3 mm2/s for inflammatory vertebral lesions such as lesions caused by spondylitis or tuberculosis. Thus, in-termediate ADC values are identified for such le-sions, between those of osteoporotic fractures and malign vertebral lesions.
Conclusions
DWI and ADC maps are able to detect diffe-rences in cellularity of malignant bone marrow disorders with respect to the normal bone mar-row. This ability allows the diagnosis of vertebral metastases with a high level of confidence, so that DWI and its ADC maps could be effectively applied for the routine MR imaging analysis in oncological patients for the diagnosis of vertebral metastases. Some limitations for the daily appli-cation of DWI in the study of oncological patients are the presence of high cellularity lesions such as sclerotic vertebral metastases47 and the presen-ce of red bone marrow, for example in younger subjects or in those patients treated with bone marrow stimulating factors such as G-CSF. These
Figure 3. 44-year-old man with lung cancer. A vertebral collapse appears iso-hypointense on T1 weighted image (a), shows hyperintensity on DWI image (b), and ADC value on the related map (c) of 0.82 × 10-3 mm2/s.

DWI and ADC values for detection of malignant vertebral bone marrow lesions
595
last conditions, in fact, increase basal bone mar-row signal intensity on DWI imaging, thus ren-dering eventual malignant lesions less evident on the normal background.
Conflict of interestThe authors declare no conflicts of interest.
References
1) Vande Berg BC, LeCouVet Fe, MiChaux L, Ferrant a, MaLdague B, MaLgheM J. Magnetic resonance ima-ging of the bone marrow in hematological mali-gnancies. Eur Radiol 1998; 8: 1335-1344.
2) LeCouVet Fe, LarBi a, PasogLou V, oMouMi P, toMBaL B, MiChoux n, MaLgheM J, LhoMMeL r, Vande Berg BC. MRI for response assessment in metastatic bone disease. Eur Radiol 2013; 23: 1986-1997.
3) Le Bihan d, Breton e, LaLLeMand d, grenier P, CaBanis e, LaVaL-Jeantet M. MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neu-rologic disorders. Radiology 1986; 161: 401-407.
4) tsuruda Js, Chew wM, MoseLey Me, norMan d. Diffusion-weighted MR imaging of the brain: va-lue of differentiating between extraaxial cysts
and epidermoid tumors. AJNR Am J Neurora-diol 1990; 11: 925-931.
5) seViCk rJ, kuCharCzyk J, MintoroVitCh J, MoseLey Me, derugin n, norMan d. Diffusion-weighted MR imaging and T2-weighted MR imaging in acute cerebral ischaemia: comparison and cor-relation with histopathology. Acta Neurochir Suppl (Wien) 1990; 51: 210-212.
6) huisMan ta. Diffusion-weighted imaging: basic concepts and application in cerebral stroke and head trauma. Eur Radiol 2003; 13: 2283-2297.
7) suBhawong tk, JaCoBs Ma, Fayad LM. Diffusion-wei-ghted MR imaging for characterizing musculoske-letal lesions. Radiographics 2014; 34: 1163-1177.
8) LeCouVet Fe, geukens d, stainier a, JaMar F, JaMart J, d’othée BJ, therasse P, Vande Berg B, toMBaL B. Magnetic resonance imaging of the axial skele-ton for detecting bone metastases in patients with high-risk prostate cancer: diagnostic and costef-fectiveness and comparison with current detection strategies. J Clin Oncol 2007; 25: 3281-3287.
9) toMBaL B, rezazadeh a, therasse P, Van Cangh PJ, Vande Berg B, LeCouVet Fe. Magnetic resonance imaging of the axial skeleton enables objective measurement of tumor response on prostate can-cer bone metastases. Prostate 2005; 65: 178-187.
10) LeCouVet Fe, siMon M, toMBaL B, JaMart J, Vande Berg BC, siMoni P. Whole-body MRI (WB-MRI)
Figure 4. 48-year-old man with prostatic carcinoma. T1 (a) and T2 fat saturated (b) images show the presence in L2 of a lesion dishomogeneously hyperintense in (a) and hypointense in (b), suspected for metastases or atypical angioma. The corresponding DWI image (c) demonstrates hypointense lesion, that show hyperintensity on ADC map. Based on the characteristics on DWI and ADC map images the lesion was interpreted as atypical angioma.

L. Filograna, N. Magarelli, F. Cellini, S. Manfrida, A. Leone, C. Colosimo, V. Valentini
596
versus axial skeleton MRI (AS-MRI) to detect and measure bone metastases in prostate cancer (PCa). Eur Radiol 2010; 20: 2973-2982.
11) BarChetti F, stagnitti a, Megna V, aL ansari n, Marini a, Musio d, Monti ML, BarChetti g, toMBoLini V, Ca-taLano C, PaneBianCo V. Unenhanced whole-body MRI versus PET-CT for the detection of prostate cancer metastases after primary treatment. Eur Rev Med Pharmacol Sci 2016; 20: 3770-3776.
12) MaLayeri aa, eL khouLi rh, zaheer a, JaCoBs Ma, Corona-ViLLaLoBos CP, kaMeL ir, MaCura kJ. Princi-ples and applications of diffusion-weighted ima-ging in cancer detection, staging, and treatment follow-up. Radiographics 2011; 31: 1773-1791.
13) koh dM, CoLLins dJ. Diffusion-weighted MRI in the body: applications and challenges in oncology. AJR Am J Roentgenol 2007; 188: 1622-1635.
14) neiL JJ. Diffusion imaging concepts for clinicians. J Magn Reson Imaging 2008; 27: 1-7.
15) VaneL d, droMain C, tardiVon a. MRI of bone mar-row disorders. Eur Radiol 2000; 10: 224-229.
16) Padhani ar, koh dM, CoLLins dJ. Whole-body diffu-sion-weighted MR imaging in cancer: current sta-tus and research directions. Radiology 2011; 261: 700-718.
17) khoo MM, tyLer Pa, saiFuddin a, Padhani ar. Diffu-sion-weighted imaging (DWI) in musculoskeletal MRI: a critical review. Skeletal Radiol 2011; 40: 665-681.
18) Chen wt, shih tt, Chen rC, Lo sy, Chou Ct, Lee JM, tu hy. Vertebral bone marrow perfusion evalua-ted with dynamic contrast-enhanced MR imaging: significance of aging and sex. Radiology 2001; 220: 213-218.
19) goodsitt MM, hooVer P, VeLdee Ms, hsueh sL. The composition of bone marrow for a dual-energy quantitative computed tomography technique: a cadaver and computer simulation study. Invest Radiol 1994; 29: 695-704.
20) VogLer JB 3rd, MurPhy wa. Bone marrow imaging. Radiology 1988; 168: 679-693.
21) Chen wt1, shih tt, Chen rC, Lo hy, Chou Ct, Lee JM, tu hy. Blood perfusion of vertebral lesions eva-luated with gadolinium-enhanced dynamic MRI: in comparison with compression fracture and meta-stasis. J Magn Reson Imaging 2002; 15: 308-314.
22) hiLLengass J, BäuerLe t, BartL r, andruLis M, MC-CLanahan F, Laun FB, zeChMann CM, shah r, wa-gner-gund B, siMon d, heiss C, neBen k, ho ad, sChLeMMer hP, goLdsChMidt h, deLorMe s, stieLtJes B. Diffusion weighted imaging for non-invasive and quantitative monitoring of bone marrow infiltration in patients with monoclonal plasma cell disease: a comparative study with histology. Br J Haematol 2011; 153: 721-728.
23) Chan Jh, Peh wC, tsui ey, Chau LF, Cheung kk, Chan kB, yuen Mk, wong et, wong kP. Acute vertebral body compression fractures: discrimination betwe-en benign and malignant causes using apparent diffusion coefficients. Br J Radiol 2002; 75: 207-214.
24) Messiou C, CoLLins dJ, Morgan Va, desouza nM. Op-timising diffusion weighted MRI for imaging meta-
static and myeloma bone disease and assessing reproducibility. Eur Radiol 2011; 21: 1713-1718.
25) Pui Mh, Mitha a, rae wi, Corr P. Diffusion wei-ghted magnetic resonance imaging of spinal in-fection and malignancy. J Neuroimaging 2005; 15: 164-170.
26) sCheLLinger d, Lin Cs, Fertikh d, Lee Js, LauerMan wC, henderson F, daVis B. Normal lumbar verte-brae: anatomic, age, and sex variance in subjects at proton MR spectroscopy:initial experience. Ra-diology 2000; 215: 910-916.
27) syed Fa, oursLer MJ, heFFeranM te, Peterson JM, riggs BL, khosLa s. Effects of estrogen therapy on bone marrow adipocytes in postmenopausal osteoporotic women. Osteoporos Int 2008; 19: 1323-1330.
28) aLyas F, saiFuddin a, ConneLL d. MR imaging eva-luation of the bone marrow and marrow infiltrative disorders of the lumbar spine. Magn Reson Ima-ging Clin N Am 2007; 15: 199-219.
29) sChweitzer Me, LeVine C, MitCheLL dg, gannon Fh, goMeLLa Lg. Bull’s-eyes and halos: useful MR di-scriminators of osseous metastases. Radiology 1993; 188: 249-252.
30) wu LM1, gu hy, zheng J, xu x, Lin Lh, deng x, zhang w, xu Jr. Diagnostic value of whole-body magnetic resonance imaging for bone metasta-ses: a systematic review and meta-analysis. J Magn Reson Imaging 2011; 34: 128-135.
31) Padhani ar, gogBashian a. Bony metastases: asses-sing response to therapy with whole-body diffusion MRI. Cancer Imaging 2011; 11 Spec No A: S129-145.
32) LeCouVet Fe, eL Mouedden J, CoLLette L, CoChe e, danse e, JaMar F, MaChieLs JP, Vande Berg B, oMouMi P, toMBaL B. Can whole-body magnetic resonance imaging with diffusion-weighted imaging replace Tc 99m bone scanning and computed tomography for single-step detection of metastases in patients with high-risk prostate cancer? Eur Urol 2012; 62: 68-75.
33) eiBer M, hoLzaPFeL k, ganter C, ePPLe k, Metz s, geinitz h, küBLer h, gaa J, ruMMeny eJ, Beer aJ. Whole-bo-dy MRI including diffusion-weighted imaging (DWI) for patients with recurring prostate cancer: technical feasibility and assessment of lesion conspicuity in DWI. J Magn Reson Imaging 2011; 33: 1160-1170.
34) Messiou C, CoLLins dJ, giLes s, de Bono Js, BianChi-ni d, de souza nM. Assessing response in bone metastases in prostate cancer with diffusion wei-ghted MRI. Eur Radiol 2011; 10: 2169-2177.
35) Padhani ar, Van ree k, CoLLins dJ, d’sa s, Makris a. Assessing the relation between bone marrow signal intensity and apparent diffusion coefficient in diffusion-weighted MRI. AJR Am J Roentgenol 2013; 200: 163-170.
36) nonoMura y, yasuMoto M, yoshiMura r, haraguChi k, ito s, akashi t, ohashi i. Relationship between bone marrow cellularity and apparent diffusion coeffi-cient. J Magn Reson Imaging 2001; 13: 757-760.
37) hwang s, PaniCek dM. Magnetic resonance ima-ging of bone marrow in oncology. Part 1. Skeletal Radiol 2007; 36: 913-920.

DWI and ADC values for detection of malignant vertebral bone marrow lesions
597
38) Laor t, JaraMiLLo d. MR imaging insights into ske-letal maturation: what is normal? Radiology 2009; 250: 28-38.
39) BhugaLoo a, aBduLLah B, siow y, ng k. Diffusion weighted MR imaging in acute vertebral compres-sion fractures: differentiation between malignant and benign causes. Biomed Imaging Interv J 2006; 2: e12.
40) Baur a, stäBLer a, Brüning r, BartL r, krödeL a, rei-ser M, deiMLing M. Diffusion weighted MR imaging of bone marrow: differentiation of benign versus pathologic compression fractures. Radiology 1998; 207: 349-356.
41) karCheVsky M, BaBB Js, sChweitzer Me. Can diffu-sion-weighted imaging be used to differentiate benign from pathologic fractures? A meta-analy-sis. Skeletal Radiol 2008; 37: 791-795.
42) dietriCh o, geith t, reiser MF, Baur-MeLnyk a. Diffu-sion imaging of the vertebral bone marrow. NMR Biomed. 2015.
43) Fawzy F, tantawy hi, ragheB a, aBo hasheM s. Diagno-stic value of apparent diffusion coefficient to differen-
tiate benign from malignant vertebral bone marrow lesions. Egypt J Radiol Nucl Med 2013; 44: 265-271.
44) BaLLiu e, ViLanoVa JC, PeLáez i, Puig J, reMoLLo s, BarCeLó C, BarCeLó J, Pedraza s. Diagnostic value of apparent diffusion coefficients to differentiate benign from malignant vertebral bone marrow le-sions. Eur J Radiol 2009; 69: 560-566.
45) taşkin g, İnCesu k, asLan k. The value of apparent diffusion coefficient measurements in the dif-ferential diagnosis of vertebral bone marrow le-sions. Turk J Med Sci 2013; 43: 379-387.
46) aBo dewan kaw, saLaMa aa, eL haBashy hMs, kha-LiL aes. Evaluation of benign and malignant ver-tebral lesions with diffusion weighted magnetic resonance imaging and apparent diffusion coef-ficient measurements. Egypt J Radiol Nucl Med 2015; 46: 423-433.
47) oztekin o, ozan e, hiLaL adiBeLLi z, unaL g, aBaLi y. SSH-EPI diffusion-weighted MR imaging of the spi-ne with low b values: is it useful in differentiating malignant metastatic tumor infiltration from benign fracture edema? Skeletal Radiol 2009; 38: 651-658.