DVT Prophylaxis in Medical Patients. Rog Kyle, MD MUSC 6/5/12. Review risks for developing DVT and bleeding from DVT prophylaxis Review current recommendations for inpatient DVT prophylaxis (AT9) Review different pharmacologic and mechanical methods for DVT prophylaxis - PowerPoint PPT Presentation
DVT Prophylaxis in Medical Patients
DVT Prophylaxis in Medical PatientsRog Kyle, MDMUSC6/5/12Review
risks for developing DVT and bleeding from DVT prophylaxisReview
current recommendations for inpatient DVT prophylaxis (AT9)Review
different pharmacologic and mechanical methods for DVT
prophylaxisExamine recent controversies in DVT prophylaxis
Risk for DVTHistorical baseline0.8% DVT0.4% PENot used by ACCP
2012Hospitalization in general associated with 8X VTE risk and 25%
of all VTE50-75% of all in hospital VTE events are on medical
servicesRisk for DVTImportant to remember that most RCTs looking at
DVT prophylaxis used asymptomatic DVT detected by venography.Start
as calf DVTReduction in asymptomatic parallels reduction in
symptomatic DVTDoes not mean that the relative effects of
asymptomatic and symptomatic events will be similar (particularly
PE)Bleeding? - there are no published data addressing the
relationship between wound or joint bleeding and either wound
infection or long-term joint functionNet benefit (non-fatal) PE,
DVT, GI bleed, periop bleed)Prevention complication Fatal events
are rareRisk for DVTAT9Critically ill vs. non-criticalIn
non-criticalRAMs (risk assessment model) suffer from prospective
validation, among other problemsACCP 2012 guidelines utilize the
Padua Prediction Score
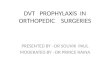
Risk for DVTCritically ill vs. non-criticalIn non-criticalRAMs
(risk assessment model) suffer from prospective validation, among
other problemsACCP 2012 guidelines utilize the Padua Prediction
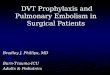
ScoreHigh Risk 4
Padua Prediction ScoreJournal of Thrombosis and Haemostasis
2010; 8: 24502457Prospective cohort study, 1180 pts. (medical)
followed to 90 days after d/cAssessedWhether pts could be assigned
to high or low risk by a RAMWhether prophylaxis worked (TID
heparin, LMWH, fondaparinux) in either groupRisk level was blinded
to the treating MDUse of prophylaxis left up to the treating
MDExcluded bleeding, plts < 100K, CrCl < 30Padua Prediction
Score40 % high risk, 60% low risk40% of the high risk received DVT
prophylaxis and 7.3% of the low riskOnly investigated symptomatic
pts for DVT/PE
Padua Prediction Score40 % high risk, 60% low risk40% of the
high risk received DVT prophylaxis and 7.3% of the low riskOnly
investigated symptomatic pts for DVT/PEHighly significant (P <
0.001, HR 0.13)Of the 4 in the high risk/treated 3 occurred after
d/c
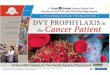
Bleeding Risk from ProphylaxisACCP 2012 choose 0.4% major
bleeding riskFrom the control arms of DVT prophylaxis trialsIMPROVE
trial
Chest. 2011; 139(1):69-79Bleeding Risk from ProphylaxisACCP 2012
choose 0.4% major bleeding riskFrom the control arms of DVT
prophylaxis trialsIMPROVE trial risk model too complex and not
validatedAT9AT92.3. For acutely ill hospitalized medical patients
at increased risk of thrombosis, we recommend anticoagulant
thromboprophylaxis with low molecular- weight heparin [LMWH],
low-dose unfractionated heparin (LDUH) bid, LDUH tid, or
fondaparinux (Grade 1B) .AT92.4. For acutely ill hospitalized
medical patients at low risk of thrombosis, we recommend against
the use of pharmacologic prophylaxis or mechanical prophylaxis
(Grade 1B) .DVT ProphylaxisLDUH vs. LMWHNo difference in DVT, PE,
overall mortality or HIT (one trial)No cost differenceMinimally
less major bleeds for LMWH (5/1000)BID vs. TID LDUHThe low quality
evidence from these indirect comparisons provides no compelling
evidence that LDUH TID dosing, compared with BID dosing, reduces
VTE or causes more bleeding
Chest 2007;131;507-516BID heparin dosing causes fewer major
bleeding episodes, while TID dosing appears to offer somewhat
better efficacy in preventing clinically relevant VTE events
Chest 2011;140;374-381Moderate-quality evidence suggests that
subcutaneous UFH bid and UFH tid do not differ in effect on DVT,
PE, major bleeding, and mortalityGCS vs. IPCs vs.
VFPsGCSConflicting data, thigh high probably better than knee high
(CLOTS I, II trials)Surgical, stroke ptsMost studies screened for
asymptomatic DVTIPC/VFPNo studies in hospitalized medical ptsLess
DVT (sxc) but no mortality or PE benefit in surgical pts
GCS vs. IPCs vs. VFPsthe compelling evidence of a decrease in
fatal PE that exists for anticoagulants and for aspirin does not
exist for mechanical methodsMechanical Compression vs. HeparinNo
studies in hospitalized medical ptsSurgical pts no difference in
DVT, PE (except subgroup of LMWH vs. compression less DVT); less
bleeding with compressionMechanical Compression + Heparinoids vs.
Heparinoids AloneSurgical ptsIPCs + pharm trended better than pharm
aloneGCS + pharm better than pharm alone but more skin
complications
ButSurgical studies looking at IPC functioning found them
working or applied properly in only 20 - 50% of pts.Extended
Duration DVT ProphylaxisApproximately 70% of DVTs in medical pts
occur in the out patient settingOver half of these pts had been
hospitalized within the past 3 months, and 2/3s of these within 1
monthMEDENOX RTC - N Engl J Med 1999;341: 793-800RTC40/20 lovenox
vs. placebo3 mos f/u
Extended Duration DVT ProphylaxisApproximately 70% of DVTs in
medical pts occur in the out patient settingOver half of these pts
had been hospitalized within the past 3 months, and 2/3s of these
within 1 monthMEDENOX RTC - N Engl J Med 1999;341: 793-800EXCLAIM -
Ann Intern Med. 2010;153:8-1840 lovenox for 28 days after initial
therapy in hosp
EXCLAIMOnly RTC of extended DVT prophylaxis (LMWH) in medical
pts (in-hospital and 28 days post-d/c)Reduced overall DVT (sym and
asym)Level 1 mobility (bed rest)> 75 y.o.femaleNo difference
fatal PENo difference in overall mortality and 4 ICBs (one fatal)
in LMWH group (none in placebo)Overall, 5/1000 fewer sxc DVTs,
4/1000 major bleedsAT9 not recommendedASAStudies in medical pts 9
trials, 555 pts all antiplatelet drugs Small number of events
(DVTs)Asymptomatic/symptomatic, proximal/distalUS/fibrinogen
labeling/venographyUp to 8 wks of drug, bleeding events not
reportedASAPooling 9 trials35% reduction in asymptomatic DVTNo
effect on PE rateBleeding not reportedASAPEP Trial - Lancet 2000;
355: 129530213,000 + ortho pts (hip fx)160 mg ASA vs. placebo (+
any other thromboprophylaxis thought necessary) for 35 days35 days
post hip fracture surg, THA, TKALess DVTs sym and asymLess PEs
fatal and non-fatalNo overall mortality benefitNo difference in
fatal bleeding (some increase in surg site bleeds)
ASAPEP Trial - Lancet 2000; 355: 129530213,000 + ortho pts (hip
fx)160 mg ASA vs. placebo (+ any other thromboprophylaxis thought
necessary) for 35 days35 days post hip fracture surg, THA, TKALess
DVTs sym and asymLess PEs fatal and non-fatalNo overall mortality
benefitNo difference in fatal bleeding (some increase in surg site
bleeds)there is now good evidence for considering aspirin routinely
in a wide range of surgical and medical groups at high risk of
venous thromboembolism
AT9Based on the low quality of available evidenceno
recommendation could be madeThere have been no studies of
antiplatelet therapy compared with antithrombotic therapy (pharm or
mech) to prevent VTE in acutely ill medical patients
Ann Intern Med. 2011;155:602-615Large meta-analysisRandomized
trials including medical patients or strokesHeparin, LMWH,
mechanical prophylaxis40 unique trials; 52,000 ptsMedical and
stroke pts, no surg/trauma/OB
TrialsHeparin vs no heparin (1)LMWH vs no LMWH (2)LMWH vs UFH
(3)Mechanical vs no mechanical (4)OutcomesDeath (primary); PE,
major bleeding (secondary) (1, 2, 3)Death (4) Resultsno significant
effect of prophylaxis on mortality (there was a trend in favor of
heparin prophylaxis (P=0.056)Heparin vs no heparin3 less PEs, 9
more bleeds (4 major)/1000 ptsLMWH vs heparinNo difference in
outcomesNo improved outcomes with mechanical prophylaxis in
strokeConclusionReduced PE, no change total mortality, increased
bleeding (heparin, LMWH) (stroke and medical pts)Therefore, no net
clinical benefit
Raised numerous questionsWhich are the preferred outcomes (PE vs
bleed)Use of surrogate outcomes asymptomatic DVT?Most PE not
preceded by symptomatic DVTAsymptomatic PEs? No studies screen with
CTEditorial commentsJCs recommendation for DVT proph only excludes
children and pts hospitalized < 2 days
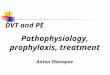
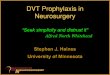
N Engl J Med 2011;365:2463-72N Engl J Med 2011;365:2463-72LMWH
in Medical PatientsDouble blind, randomized, placebo controlledLMWH
vs. placebo, all pts received elastic stockings with graduated
compressionChina, India, Korea, Malaysia, Mexico, the Philippines,
and Tunisia8300+ ptsPrimary outcome death at 30 daysSecondary
outcomes Death at 0-14 days, 0-90 days rate of cardiopulm death 14,
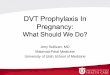
30, 90 days and sudden death or PE 14, 30, 90 days
Results
ConclusionNo reduction in the rate of death from any cause among
hospitalized, acutely ill medical patients with the addition of
lovenoxCounterintuitive?Pharm prophylaxis reduces DVT (including
asympt DVT) in acutely ill medical pts by > 45%Assumed that DVTs
in medical pts are the same as surgical distal to proximal
progression (we know that proximal DVT in medical pts has higher
risk of PE than distalReferencesKahn et al. Prevention of VTE in
Nonsurgical Patients : Antithrombotic Therapy and Prevention of
Thrombosis, 9th ed: American College of Chest Physicians
Evidence-Based Clinical Practice Guidelines. Chest
2012;141;e195S-e226SBarbar et al. A risk assessment model for the
identification of hospitalized medical patients at risk for venous
thromboembolism: the Padua Prediction Score. Journal of Thrombosis
and Haemostasis, 8: 24502457Decousus et al. Factors at Admission
Associated With Bleeding Risk in Medical Patients. Chest. 2011;
139(1):69-79King et al. Twice vs Three Times Daily Heparin Dosing
for Thromboembolism Prophylaxis in the General Medical Population.
Chest 2007;131;507-516Phung et al. Dosing Frequency of
Unfractionated Heparin Thromboprophylaxis. Chest
2011;140;374-381CLOTS Trial Collaboration. Thigh-Length Versus
Below-Knee Stockings for Deep Venous Thrombosis Prophylaxis After
Stroke. Ann Intern Med. 2010;153:553-562.Samama et al. A Comparison
of Enoxaparin with Placebo for the Prevention of Venous
Thromboembolism in Acutely Ill Medical Patients. N Engl J Med
1999;341:793-800.Hull et al. Extended-Duration Venous
Thromboembolism Prophylaxis in Acutely Ill Medical Patients With
Recently Reduced Mobility. Ann Intern Med. 2010;153:8-18.Pulmonary
Embolism Prevention (PEP) Trial Collaborative Group. Prevention of
pulmonary embolism and deep vein thrombosis with low dose aspirin:
Pulmonary Embolism Prevention (PEP) trial. Lancet 2000; 355:
1295302Lederle et al. Venous Thromboembolism Prophylaxis in
Hospitalized Medical Patients and Those With Stroke: A Background
Review for an American College of Physicians Clinical Practice
Guideline. Ann Intern Med. 2011;155:602-615Kakkar et al.
Low-Molecular-Weight Heparin and Mortality in Acutely Ill Medical
Patients. N Engl J Med 2011;365:2463-72.