Embed Size (px)
Citation preview
DVT and PE
Pathophysiology, prophylaxis, treatment
Anton Sharapov
Cases to consider 38 yom for elective IHR 65 yom for elective IHR 65 yom, obesity/CHF/prev DVT for IHR 25 yof post severe head injury 25 yom post trauma/abdo/chest 75 yof post hip # 65 yom post THA, obese
Scope of the problem
PCommon postop complicationPAsymptomatic > symptomaticPDifficult to studyPMost studies evaluate asymptomatic pts
Epidemiology VTE 48:100,000 PE 69:100,000 Incidence – 20-70% surgery pts ½ begin in OR
Epidemiology DVT and PE – different stages of same
disease process 10% proximal DVTs progress to
symptomatic PE 25% distal DVTs become proximal
OutcomesP Most asymptomatic VTE recover
sans treatment and complicationsP Less then 1 in 8 confirmed clots
progress to symptomatic thromboembolic disease
P Important to observe clots over a period of time
Outcomes of PE Outcomes of PE are difficult to assess Registry estimates are always higher
then in clinical studies (7% vs 2%) Mortality is a function of RV function,
clot burden, and comorbidities Risk of fatal PE greatest 3-7 postop Asymptomatic PE are common
40% of asymptomatic prox DVTs
AssessmentP Assess risk of DVT and risk of
bleedingP Assess duration of prophylaxisP Assess Virchov triad
P Venous stasisP Endothelial injuryP hypercoagulability
Risk factors: venous stasis
PImmobility & tourniquet applicationPInstitutionalizationPCVAPParalysisPCHFPTravel >4 hoursPObesityPRespiratory failurePVaricose veinsPDuration/extent of postop immobilization
Risk factors: endothelial injury Trauma Atherosclerosis Perioperative Malignancy Post-phlebitic syndrome Prior DVT CV catheter Inflamatory condition Hyperhomocysteinemia
Risk factors: hypercoagulability, Acquired
Post op Malignancy Hormone replacement Estrogen therapy
Risk factors: hypercoagulability, Acquired: Antiphospholipid antibody Lupus anticoagulant – 5-10 fold risk Myeloproliferative d/o Paroxysmal nocturnal
hemoglobinuria Nephrotic syndrome Pn loosing enteropathy
Risk factors: hypercoagulability, Inherited:
Factor V leiden – APC resistanceB Absolute risk post op VTE is small - 1/100B Relative risk increased (3-5 fold)B Screening not recommended
Antithrombin, pn C/S deficiency Fibrinogen/TPA defects Prothrombin gene mutation
Risk factors: MiscelaneousP Use/nonuse of thrombopophylactic
measures Age - rises linearly after 40
P Ethnicity: Asian/South Pacific - threefold lower African American - slightly higher Latin - slightly lower
Site/extent traumatic injury Knee/spine=major trauma>hip>uro/gyny>
neuro>general/thoracic
Risk of DVT, miscellaneousP Surgical procedure - most important
Neurosurgery & ortho - 6% & 3%
Major vascular
Bowel, bladder, gastric bypass and kidney transplant
Radical neck, IHR, lap chole (0.3%),TURP, thyroid/parathyroid - lowest risk
Need for global integrative assessment American College of Chest
Physicians Risk stratification tool Problems:
What defines major vs minor surgeries?
No weighting of Risk Factors Why age 40 and 60 important?
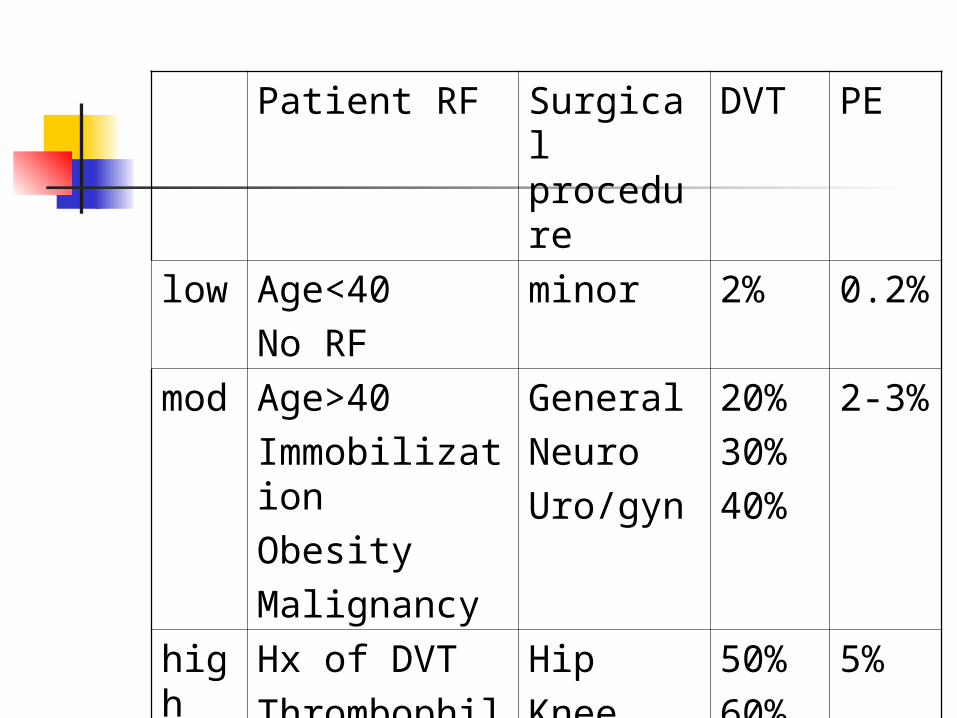
Patient RF Surgical procedure
DVT PE
low Age<40No RF
minor 2% 0.2%
mod
Age>40ImmobilizationObesityMalignancy
GeneralNeuroUro/gyn
20%30%40%
2-3%
high
Hx of DVTThrombophilia
HipKneeSpineTrauma
50%60%60%60%
5%
Risk of bleeding
PBleeding d/oPUse of antiplatelet medsPPrevious GI bleedPCancerPHepatic/renal insufficiencyP?age
VTE prophylaxis: what’s available? Intermittent compression devise Stockings ASA 80-325 mg UF heparin 5000 bid, tid LMW bid Warfarin Anti – Xa pentasaccharide
(fondaparinix)
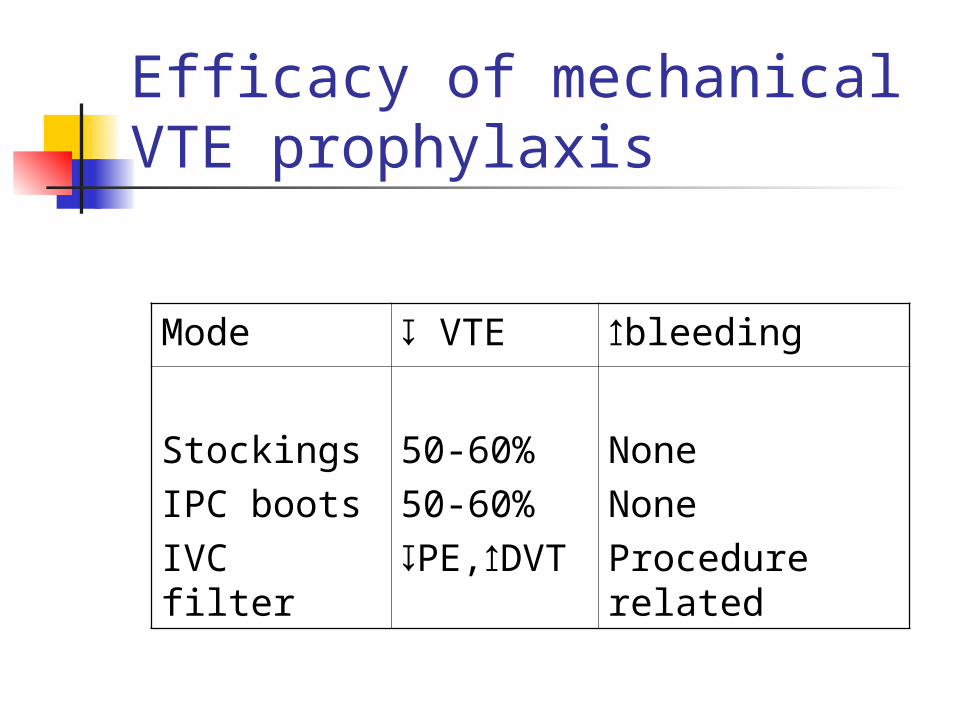
Efficacy of mechanical VTE prophylaxis
Mode ↧ VTE ↥bleeding
StockingsIPC bootsIVC filter
50-60%50-60%↧PE,↥DVT
NoneNoneProcedure related
Early ambulation Routine for all pts Acceptable as sole mode for low
risk Useful adjunct esp post knee/hip
surgery
Elastic stockings First shown to work in 1952 Decrease venous pooling Evidence of benefit for mod/high
risk, but used only as adjunct Harmful if not work correctly
ICD Work very well Not useful form BMI >25 Only effective if used correctly and
continuously when pt not ambulating Have potential to reduce ambulation Recommended in mod-high risk gyn
surgery as solo Not recommended as sole mode in
Highest risk – except neurosurgery High risk urological Hip and knee surgery
IVC For absolute contraindication of
anticoagulation For life-threatening hem on AC For failure of AC Used to prevent fatal PE Temporary filters preferred If left in place, cause DVTs
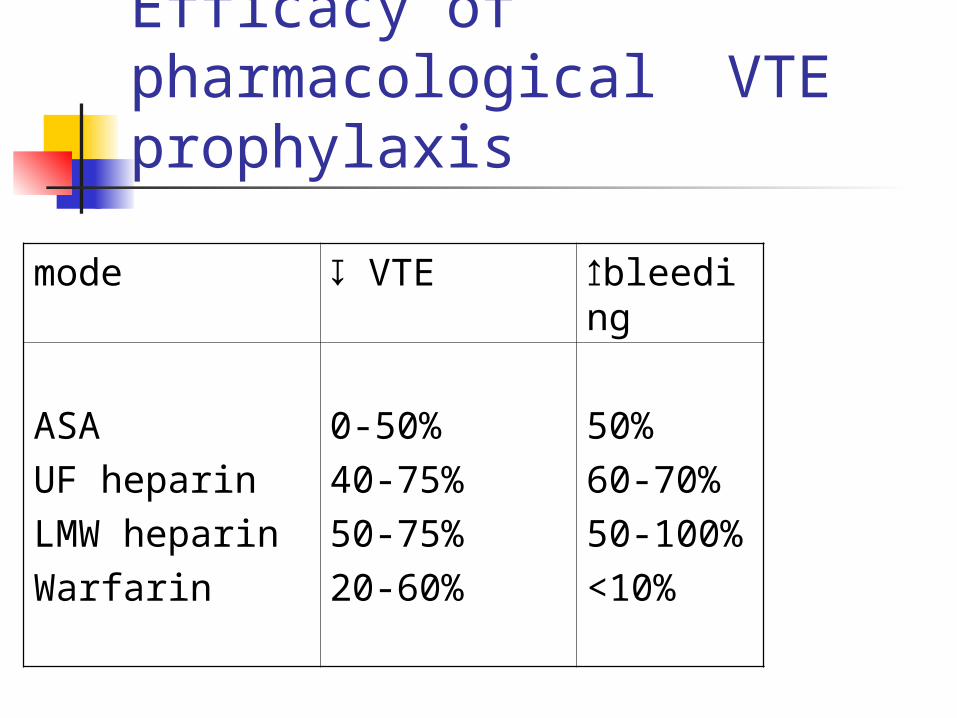
Efficacy of pharmacological VTE prophylaxis
mode ↧ VTE ↥bleeding
ASAUF heparinLMW heparinWarfarin
0-50%40-75%50-75%20-60%
50%60-70%50-100%<10%
Aspirin Not recommended as sole
prophylaxis Beneficial post hip-fracture
160 mg OD, 5/52, 13,000 pts Combined with routine prophylaxis PE – 0.7 vs 1.2 Fatal PE 18 vs 43
UF heparin Good for moderate risk gen
surgery Modest increase in bleeding
Compared to LMWH (2.65% vs 1.8%) Additive effect of stockings and
ICD] Risk of HIT
warfarin For very high risk with lower extremity
orthopedic and neuro surgery For gen surgery other methods work just
as well… Good for extended prophylaxis Delayed onset of action, may start
preop! Recommended for
Hip #, THA, TKA
LMW heparin and Pentasaccharideds Preferential inhibition of factor Xa FDA approved for DVT prophylaxis Not FDA approved as of yet for
DVT prophylaxis in pregnancy, spinal cord injury, trauma, neurosurgery… but are being used
LMW heparin and Pentasaccharideds cont’d Effective for mod risk general surgery Gyn/obs
second line to mechanical Trauma
Method of choice only if risk of bleeding is not significant. If it is – stocking+/-ICD
Recommended for ortho lower extremity surgery
Fondoparinix reduces asymptomatic DVTs only…
LMW heparin and Pentasaccharideds cont’d
Risk of epidural hematoma Strategies
Avoid regional anesth in those prone to bleed Needle in 12 h after onset of LMWH Single dose anesthetic better then infusion D/c cath in 12 h No dosing of LMWH within 2 h of cath d/c
Direct thrombin inhibitors Effective in initial studies Comparable to LMWH For HIT pts
Duration of prophylaxis Start immediately after or prior to
surgery 7-10 days post Warfarin may be started 10/7 prior but
INR should be less then 1.5 Argument for prolonged (30 day)
prophylaxis for high risk. DVT incidence sympt – 3% vs 1% on treatment Asympt – 19% vs 9% on treatment
Prolonged prophylaxis Orthopedics
Post THA for 4-6 weeks with LMWH or warfarin, especially with Risk Factors
Obesity, sedentary, prior DVT
General surgery Prolonged treatement with LMWH
prevents out-pt DVTs but at a marginal cost that was deemed inappropriate
Screening for DVT? Not in the asymptomatic pts….
Diagnostic strategy of DVT Suspect Dupplex For proximal or ANY symptomatic –
treat For distal AND asymptomatic –
follow with serial duplex US
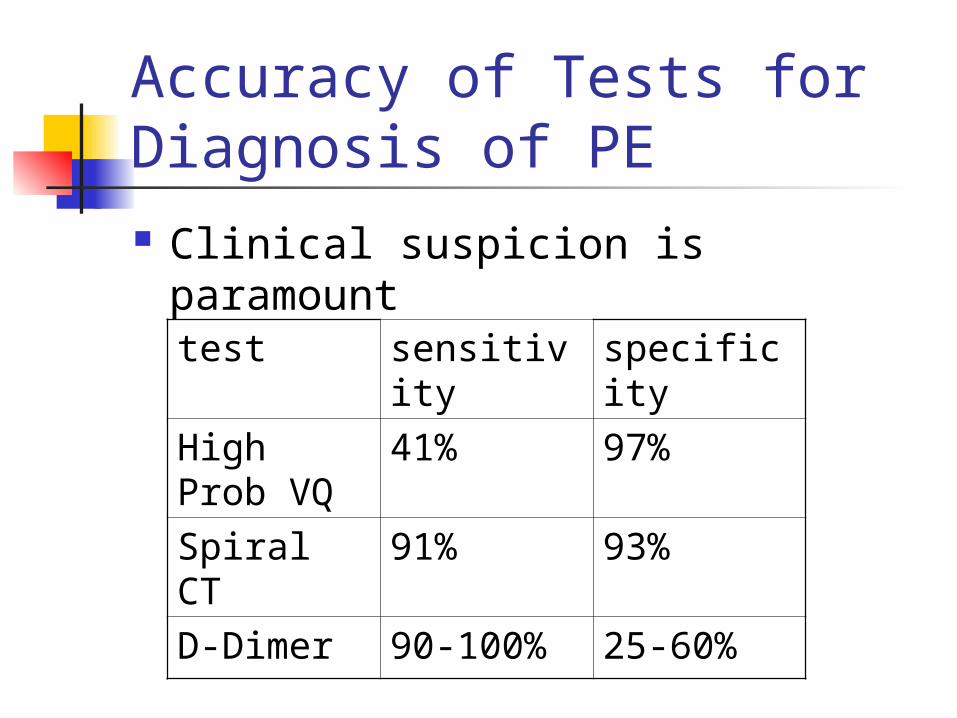
Accuracy of Tests for Diagnosis of PE Clinical suspicion is paramount
test sensitivity specificity
High Prob VQ
41% 97%
Spiral CT 91% 93%
D-Dimer 90-100% 25-60%
Diagnostic strategy for PE Suspect VQ If normal AND D-Dimer low – ruled
out If high probability – start treatment If indeterminate/nondiagnostic –
angio, angio CT
Treatment IV heparin, aPTT 1.5- 2.3 normal 5/7 May use LMW Coumadin INR 2-3 Overlap heparin and warfarin 4/7 On warfarin 3-6/12 Consider ECHO/trop to evaluate RVF
for PE to id High Risk pts.
Treatment Hemodynamically unstable PE may
require pressure support, fluid status monitoring, and/or thromolysis / surgery
Cases to consider
38 yom for elective IHR None, low risk
65 yom for elective IHR Moderate risk, Consider UN heparin pre-op,
ambulation, stockings post op
50 yom, obesity/CHF/prev DVT for IHR High risk, consider LMWH preop/post op. Conisder
warfarin
Cases concluded 25 yof post severe head injury
High risk, mechanical,
25 yom post trauma/abdo/chest High risk, mechanical initially, consider LMWH when
risk of bleeding is low
75 yof post hip # High, consider LMWH periop, warfarin or aspirin post
op
65 yom post THA, obese High, consider LMWH periop, warfarin or aspirin post
op