Embed Size (px)
Citation preview
International Journal of Law and Psychiatry
27 (2004) 361–374
Duty, burden, and ambivalence: Families of forensic psychiatric
patients in Hong Kong
Veronica Pearson (Professor)a,*, Hector W.H. Tsang (Associate Professor)b
aDepartment of Social Work and Social Administration, The University of Hong Kong, Pokfulam Road, Hong KongbDepartment of Rehabilitation Sciences, Hong Kong Polytechnic University, Hong Kong
1. Introduction
The last three decades in psychiatric research have been typified by an increasing awareness of the
effect of having a mentally ill family member on other family members. Despite this, very little work has
been done to examine the specific problems and experiences of those families who have the misfortune
to have a close relative with severe mental disorder who has also been involved with the criminal justice
system. We are now in a position to appreciate that first, most people with severe mental disorder live
with family members (Gibbons, Horn, & Powell, 1984; McMillan, Gold, & Crow, 1986; McNeil,
Rosales, & Binder, 1992; Phillips, 1993; Salokangas, Daarinen & Ojanen, 1992); second, that family
members experience this as stressful (Clark, 1994; Kuipers, 1991; Pearson & Ning, 1997; Stengard &
Salokangas, 1997; Vaddadi, 1996; Vaddadi, Gilleard, & Adlard, 1997; Winefield & Harvey, 1994); third,
that their emotions and behavior towards the patient have a highly correlated effect on relapse (Butzlaff
& Hooley, 1998; Lam, Chan & Leff, 1995; Leff & Vaughn, 1985; Mari & Streiner, 1994; Penn &
Mueser, 1996; Phillips & Xiong, 1995); and fourth, it is only recently that attention has been paid to the
needs of caregivers in performing their task of caring. Obviously, helping relatives meet their needs
strengthens their capacity to cope and therefore directly benefits the patient. (Pollio, North, & Foster,
1998). Perring, Twigg, and Aitken (1990), reviewing English and American studies, list relatives’ needs
as information and involvement from and with caring professionals, support in a crisis, respite and day
care, advice on how to manage difficult behavior, advice on welfare benefits, and help with transport. To
this list, Kuipers (1991) adds continuity, trust, and understanding from the involved professionals. Most
authors agree that services for caregivers still fall short of even basic standards.
In addition, the sense of familism and responsibility to care for family members is particularly deep
and significant in Chinese societies (Kung, 2003; Pearson & Ning, 1997; Phillips, 1993; Phillips &
Xiong, 1995). Adult children frequently live with parents until marriage and many of them stay with
their parents after marriage. If a family member is ill or has a disability, then, wherever possible, that
0160-2527/$ - see front matter D 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.ijlp.2003.08.001
* Corresponding author. Tel.: +852-28592288; fax: +852-2587604.
E-mail address: [email protected] (V. Pearson).
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374362
person will be cared for within the family. These expectations are taken seriously and many families
would consider it shameful to do anything less. Having said that, it is as likely as in Western countries
that the major burden of caregiving will fall on a female, frequently the mother. Extended families are
not usually involved in the daily care tasks and the same problems arise as in Western cultures as to what
will become of the patient when the elderly mother/father dies.
1.1. Additional difficulties associated with patients with a forensic background
How much more must these issues affect relatives with patients who have committed an offence
and as a consequence are admitted to a high-security hospital or psychiatric prison? Yet, there is
almost nothing in the literature about the experiences of family members who find themselves in
this position. Their loved ones are doubly disadvantaged in the eyes of the public because they are
perceived as both mad and bad, as well as profoundly unpredictable. This further exacerbates the
existing stigma (Gray, 2002; Phillips, Pearson, Li, Xu, & Yang, 2002; Trute, Tefft, & Segall, 1989).
There is no doubt that families find the violent behaviors of their relatives and the stigmatization of
people with a mental illness by the public and media very burdensome. Relatives of murderers and
rapists are often deemed guilty by association, suffering ostracism, abuse, and sometimes, physical
violence. Additional stress may arise from the needs of the parents and other relatives to cope with
the police, courts, lawyers, and the judicial system in general, following on as a consequence of the
offence. James (1996) suggests that at least two factors, namely, violence and stigma, may add
further to the problems and stress faced by families of forensic psychiatric patients. His study
reported that the burden borne by families of forensic psychiatric patients is greater than that
experienced by families of nonforensic psychiatric patients. The additional burdens are the
following:
1. Sensationalized media coverage of the criminal acts committed by the patients and the consequent
public shaming of both the patient and the family.
2. The fact that many of the families are victims of their own relatives’ violence, thus causing
ambivalence among family members towards the perpetrator.
3. Disintegration of the whole family when the crime is a homicide, the victim is a spouse or a parent,
and the perpetrator is imprisoned.
Despite all this, efforts to assess the burdens and needs of families of offenders with mental illness
have been surprisingly limited. Only five recent studies (James, 1996; McCann, 1993; McCann &
McKeown, 1995; McCann, McKeown, & Porter, 1995; McKeown & McCann, 1995) were found in a
review of the literature and most of these were of a preliminary nature. The most systematic effort was
McCann (1993) who sent questionnaires to participants in relatives’ support groups in a special hospital
(Ashworth) in the United Kingdom. Questionnaires returned by 17 relatives gave 40 stress-related
comments associated with the patients. These comments suggest that stress is not short-lived and had
long-standing effects on the relatives and that the most stressful events involved the offence and its
consequences. Most of the worries centered round a lack of information and adverse publicity about the
admission to the special hospital. They were ignorant of the ward routines and procedures, about mental
illness and treatment. They were anxious about such treatment as medication, its use to control patients,
the use of seclusion, length of incarceration, punishment, and feelings of injustice.
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374 363
2. The current research
Tsang, Pearson, and Yuen (2002) developed a model of the interrelationship between families’ sense
of stress and burden and the forensic psychiatric experience of the patient that is reproduced here as Fig.
1. This figure model builds on the traditional concept of dividing family burden into objective (referring
to finance, health, and recreation) and subjective (the affective response of family members to the
situation of caring). Based on the specific issues that affect families whose patients commit a crime, it is
likely that there is an additional and cumulative effect on the sense of burden that family members
experience from dealing with police, court proceedings, facing the media, and admission to a special
hospital or prison (Tsang et al., 2002).
No work to explore the stresses, burdens, experiences, and needs of relatives of forensic psychiatric
patients has been done in a Chinese society. Bearing this in mind, it was decided to carry out an
exploratory, qualitative study that would give relatives a voice that they so far have lacked and that
would permit a greater level of understanding of professional interventions that would be both relevant
and feasible. In-depth interviews are a viable means to explore participants’ experiences, concerns, and
needs and minimize the risk of the research team projecting their ideas and priorities onto this little-
studied client group. This, of course, imposes limitations on the generalizability of any results, but at this
initial stage that is not seen as an impediment.
2.1. The participants
Forensic psychiatric patients in Hong Kong are confined either in Siu Lam Psychiatric Center (run
by the government’s Correctional Services Department and part of the prison service) or in the more
secure wards of Castle Peak Psychiatric Hospital, the oldest (opened in 1961) and largest with at least
1000 beds in Hong Kong. Many forensic patients are transferred from Siu Lam Psychiatric Center to
Castle Peak Hospital to be treated in less restrictive conditions after a period of time, usually when
their hospital order expires. By interviewing family members with forensic patients in Castle Peak
Hospital, we were also able to include their experience of Siu Lam Psychiatric Center. Thus, all
interviews (23 in all) were conducted with family members visiting their relatives at Castle Peak
Hospital. The purpose of the interviews was explained to the relatives and their verbal consent gained
for participation. Nurses made the initial approach and the refusal rate was approximately 40%. The
interviews generally lasted for about an hour with a little variation in either direction. This was a
convenience sample because, due to institutional constraints, no other alternatives were available. Bias
may be present, but it is impossible to know why some relatives refused to participate and others
agreed because we were not allowed access to those who refused. Discussing family matters of a
shameful nature is an intensely sensitive issue particularly in a research context in Hong Kong. This in
itself would have disbarred some relatives. For others, it could have been a time constraint. However,
within exploratory research using a qualitative methodology the issue of bias does not threaten the
validity of the results.
2.2. Instrument development
Development and validation of measuring instruments abound in the literature. However, instruments
that assess family burden applicable to Chinese communities are limited. A search in the literature

V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374364
suggested that the Relative Assessment Interview (RAI) is widely used among clinicians and researchers
in the field, especially in Europe. The RAI was developed by Barrowclough and Tarrier (1992) based on
the Camberwell Family Interview, with some modifications for use in clinical settings. The RAI is a
semistructured interview used to obtain information regarding problems and needs of the caregivers in
coping with clients with schizophrenia. The information is then used to guide family intervention. The
only limitation of this scale (for our purposes) is that it ignores the additional family burdens that may
occur in offenders with schizophrenia. So the section on ‘‘psychiatric history’’ was deleted as
nonmedical professionals used the version in this study and 23 items regarding the forensic nature of
the illness and offence history were added. This expanded version was then translated into Chinese and
back-translated by two independent qualified translators who did not confer with each other. The
Chinese version was then produced after minor revisions of the first draft. Content validity and cultural
relevance were then established by a panel of 10 psychiatric professionals. The interview schedule is
reproduced in Appendix A.
2.3. Data analysis
Interviewees were asked for their permission to audiotape the interviews for later transcription and
analysis. Each interview was translated into English from the original Cantonese. Another independent
specialist reviewed the equivalence of the English and Cantonese versions. The English version was then
used as the basis for content analysis by the first author.
3. Results
3.1. The patients’ profile
The patients were primarily male (20/23) and most had been previously admitted to a psychiatric
hospital (14/23). Nine of them had a previous history of physical violence (9/23), much of which
was directed towards family members, and rarely went to court. In terms of their relationship to the
family members visiting them, 14 were sons, 2 were husbands, and 4 were younger brothers. The
three female patients consisted of a wife, a sister, and a daughter. The visiting relatives consisted of
nine mothers, five fathers, four brothers, two wives, one husband, one sister, and one set of
parents.
Almost all offences for which the patients were being detained involved physical violence (or serious
threat of it) to another person (18/23). If three cases of indecent assault are also included in the violent
category, the figure then becomes 21 of 23. The remaining two crimes are child abduction and drug
addiction. A detailed breakdown of the crimes is as follows:
Manslaughter—3
Assault/wounding—14
Arson—1
Indecent assault—3
Child abduction—1
Possession of an illegal drug (‘‘ice’’)—1.
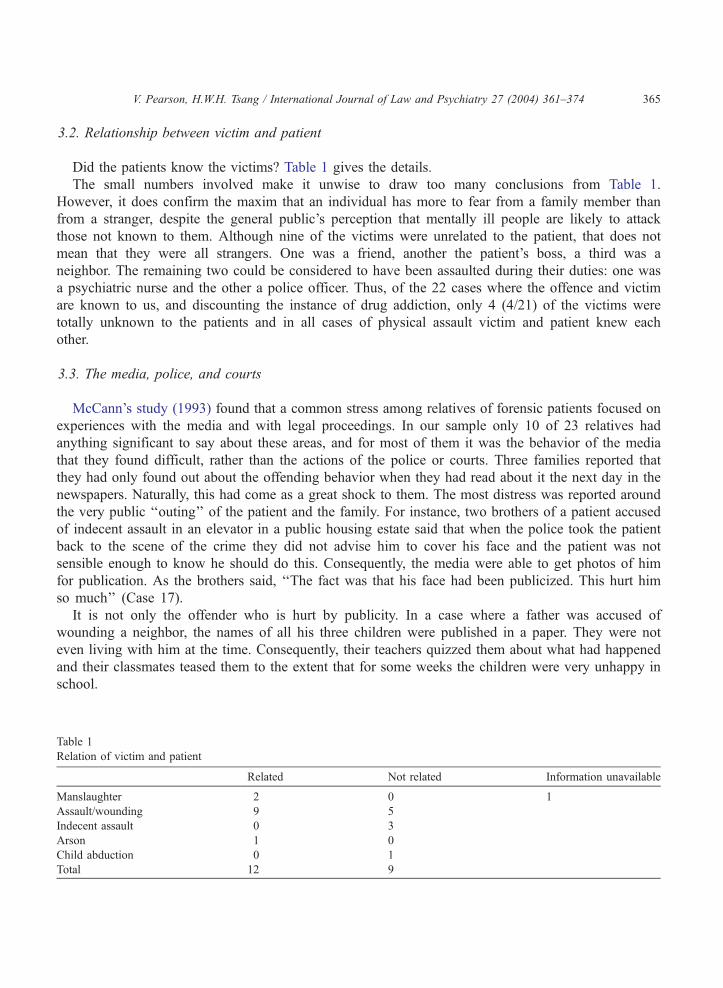
3.2. Relationship between victim and patient
Did the patients know the victims? Table 1 gives the details.
The small numbers involved make it unwise to draw too many conclusions from Table 1.
However, it does confirm the maxim that an individual has more to fear from a family member than
from a stranger, despite the general public’s perception that mentally ill people are likely to attack
those not known to them. Although nine of the victims were unrelated to the patient, that does not
mean that they were all strangers. One was a friend, another the patient’s boss, a third was a
neighbor. The remaining two could be considered to have been assaulted during their duties: one was
a psychiatric nurse and the other a police officer. Thus, of the 22 cases where the offence and victim
are known to us, and discounting the instance of drug addiction, only 4 (4/21) of the victims were
totally unknown to the patients and in all cases of physical assault victim and patient knew each
other.
3.3. The media, police, and courts
McCann’s study (1993) found that a common stress among relatives of forensic patients focused on
experiences with the media and with legal proceedings. In our sample only 10 of 23 relatives had
anything significant to say about these areas, and for most of them it was the behavior of the media
that they found difficult, rather than the actions of the police or courts. Three families reported that
they had only found out about the offending behavior when they had read about it the next day in the
newspapers. Naturally, this had come as a great shock to them. The most distress was reported around
the very public ‘‘outing’’ of the patient and the family. For instance, two brothers of a patient accused
of indecent assault in an elevator in a public housing estate said that when the police took the patient
back to the scene of the crime they did not advise him to cover his face and the patient was not
sensible enough to know he should do this. Consequently, the media were able to get photos of him
for publication. As the brothers said, ‘‘The fact was that his face had been publicized. This hurt him
so much’’ (Case 17).
It is not only the offender who is hurt by publicity. In a case where a father was accused of
wounding a neighbor, the names of all his three children were published in a paper. They were not
even living with him at the time. Consequently, their teachers quizzed them about what had happened
and their classmates teased them to the extent that for some weeks the children were very unhappy in
school.
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374 365
Table 1
Relation of victim and patient
Related Not related Information unavailable
Manslaughter 2 0 1
Assault/wounding 9 5
Indecent assault 0 3
Arson 1 0
Child abduction 0 1
Total 12 9
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374366
In more sensational cases, media reporters could be unbelievably intrusive. The father of this patient
had been stabbed by his son. According to him,
When the ambulance came [to take him to hospital] two reporters were waiting downstairs. I
was naı̈ve and didn’t think of covering myself with a blanket. So they took full pictures of me
that were in the newspapers the next day. When I arrived at the hospital 6 or 7 reporters were
already there to take photos. Then after surgery, when I was wheeled out of the operation
theatre, I was tired and the wound ached, but these reporters still followed me for an
interview. I was very upset and very unhappy. They even came into my ward at the
hospital.. . . All my colleagues knew about it. But I didn’t talk about it and they didn’t ask.
(Case 4)
Another major issue for families is the attitude of the neighbors. A crime of violence committed by
a close family member is not the sort of thing that anyone would wish others to know about. In the
Chinese context, where privacy about family matters and the good reputation of the whole family are
so important, publicity is an especially painful issue. In many situations, it was impossible for the
neighbors not to know what was going on. For instance, ‘‘There was an ambulance, a police car and
policemen came up [to the flat] so the neighbors knew . . . but they didn’t ask too many questions’’
(Case 4).
In another case of a son who attacked his father (who required 10 stitches in the wound) the
mother was out of the house when the incident took place. When she returned it was to find
police, reporters, and neighbors all milling round. The police refused her entrance to her home so
she perforce had to deal with all of those around her. When asked how she had managed she
said:
I didn’t really manage it. I just let them ask. They didn’t let me enter my flat when I came back.
It is very troublesome but what could I do? No one helped me even though I was so troubled.
All those people just wanted to look, like watching lanterns during the mid-autumn festival.
(Case 2)
Pictures of both her husband and son appeared in the papers the next day.
It is hardly surprising that death generates the greatest effects and an incident of matricide perhaps the
greatest shock of all. The wife of the patient who had killed his mother had been out shopping in the
market when the incident took place. When she returned she found the whole floor packed with reporters
who badgered her with questions.
My daughters told me to shield myself with a shirt. There were a whole bunch of reporters pressing
me for answers. I didn’t want to talk to them. I was in misery already but they still demanded that I
say something, but I didn’t . . . they followed hard after me . . . kept asking me to tell them this and tell
them that. Asked me to say why it happened. (Case 1)
Needless to say, the neighbors and relatives were scared. Some neighbors refused to talk to her; others
bombarded her with questions. Initially she was so shocked that she could not cry, but later, especially
when the neighbors ‘‘cut her dead,’’ she wept.
3.4. The future
Respondents were asked questions in two areas that appertained to the future. One was where the
patients would live if they were discharged and the other was what health and social services would
be available, useful, or both. This was followed up by a prompt that listed doctors, occupational
therapists, and social workers as possibilities. It has to be said that overall respondents were
unaware of community-based rehabilitation possibilities. Despite many of their relatives having a
long history of chronic psychiatric illness, they had had very little contact with health and social
services other than outpatient departments and hospital admission. It was also clear that despite most
being regular visitors to the hospital, they had little contact with hospital staff. Three complained
openly about the difficulty of seeing a doctor familiar with their relative and knowledgeable about
the treatment plan.
The necessity of having a job, or vocational training, on discharge was mentioned by seven relatives,
but the most frequently mentioned service (8/23) was a halfway house or hostel where it was thought
patients could be more closely supervised. There were also an additional two relatives who were
negative about the possibility of halfway house residence, one saying that ‘‘you don’t know who they
will meet’’ and the other that ‘‘he won’t be able to get along with the other residents.’’
However, the issue that brought forth the richest responses was whether the patient should live with
family members after discharge. There were seven respondents who were clear that they were willing to
have the patient back home and another seven who were equally clear that they were unwilling, but nine
showed an ambivalence that was obviously very painful for some. The mother of the patient who was
addicted to ice said at one point in the interview, ‘‘I really don’t want him to come out any time soon. I’m
afraid that he will hack at me.’’ Then about half a page further on in the transcript she claims that ‘‘I
would want him to come home and live with us if he was discharged’’ (Case 5). Another elderly mother
began to tremble violently as she contemplated the prospect of her son’s discharge and said that although
she would have him to live with her she is afraid that he will beat her again. His temper, she explains, is
unpredictable and when he loses it, it frightens even her (Case 3).
It is not unusual for family members to use the word ‘‘unpredictable’’ to describe the patient, but this
does not mean that they are not alert to changes in the patients’ moods and behavior. Many of them are
intimately familiar with the patient’s signs and symptoms and sensitive to their quirks. Their problem lies
with being able to persuade the patient to seek treatment or admission when they are clearly relapsing
because services in Hong Kong offer no medical support in the home. If the patient refuses to attend a
clinic, then an elderly mother is confined in a small flat with an actively psychotic male with a
propensity to violence. Her only choice is to call the police and have him admitted via the Accident and
Emergency Department of her local government hospital. This strategy has drawbacks that make many
family members hesitant to use it. It creates disturbance and alerts the neighbors to the problem, and it
causes bitter resentment on the part of the patients who may choose to take their revenge later.
An elder brother visiting his younger brother who is the patient states his opinion very clearly.
Because there are not enough beds in hospitals, the doctors very often just shove their responsibility
onto patients’ families . . . if there is someone to take the patient home . . . the doctors would be very
happy. But I have a family. I can’t have my brother to live with me. My mother is over 60. How can
the society be so cruel as to let someone over 60 take care of someone so strong.. . . There’s a 70 per
cent chance that he will relapse. It’s really quite dreadful. (Case 11)
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374 367
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374368
A mother of a young man, who had launched an unprovoked attack on a young girl selling
newspapers in the street and broken her nose, put it thus:
Alas, he scares me . . . he may suddenly turn very unpredictable. Would you let him go down to the
street? I am his mother but I cannot take care of him. He is tall and big. It is impossible for me to take
care of him by myself. (Case 14)
The family members who visit these patients talk in a way that suggests that many of them, despite
what they have suffered directly at the hands of the patient, are dutiful, sad, affectionate, and supportive.
For some, especially the older wives and mothers, there is a sense that the weekly or even daily visit gives
a welcome structure to their lives even when the financial costs of visiting cause hardship. It emphasizes
that they still have the honorable status of wife or mother. The ex-wife of one patient who visits every day,
despite being verbally abused by her husband most of the time she is there, expresses this by talking about
them living together when her husband is discharged, whereas later in the interview saying that she would
rather he stayed in hospital ‘‘where he is safe and doesn’t cause me trouble’’ (Case 8). A son or husband in
a psychiatric hospital is nothing to boast about, but it may be better than no son or husband at all.
3.5. An informal caring network?
It is a fallacy to assume that because Hong Kong is a Chinese society it is dominated by traditional
large, extended families available as a source of mutual aid during times of difficulty. Most Hong Kong’s
families are of the nuclear type, parents and children living under one roof. Of course, close relatives
may live nearby, and it cannot be said that anywhere in Hong Kong is truly far from anywhere else. But
which family members are sought out when psychiatric illness strikes? And are other people included in
a network of support—friends, neighbors, colleagues, residents of the home village in China.
Respondents differentiated between ‘‘family’’ and ‘‘relatives,’’ family being used to include those to
whom they were closer. Who, exactly, was included tended to vary from respondent to respondent. For
instance, one father visiting his son said that they had not told the patient’s wife, who lives in China; ‘‘of
course’’ they had not told the neighbors and ‘‘even the home village residents have not been told.’’ Thus,
for him, ‘‘family’’ meant his wife and two unmarried sons who live at home (Case 1). Another father had
never let relatives and friends know about the son’s offence (indecent assault) and incarceration. Only
recently, when his wife died, did her relatives find out that anything was wrong. In his view, ‘‘a family
disgrace should not be made public,’’ an opinion that most of our respondents would share. However, he
does confide in his younger brother not only because he works in a hospital and can provide his older
brother with useful information about circumnavigating hospital systems, but also because the father
believes that the uncle genuinely is fond of his nephew and shows sincere concern for him. Parents,
especially mothers, are frequently blamed when their children do not turn out well and relatives are not
necessarily supportive. One mother reported that she had heard ‘‘relatives’’ criticizing her for not
teaching her son how to behave properly.
The mother whose daughter (a well-educated nurse) assaulted a stranger in the street had certainly not
told neighbors and relatives, only her other adult children. The sister of the patient accompanied her at
the court hearing to relieve the mother of the stress of doing so, and it is this daughter the mother turns to
when she is unhappy and wishes to talk. There is also an adult son but she says that she does not dare to
talk to him because he is married and she does not want to put him in a ‘‘cleft stick.’’ ‘‘Sons cannot help

V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374 369
their mothers.’’ And what about her husband with whom she lives. ‘‘We’ve been husband and wife for so
many years; we don’t have much to say to each other’’ (Case 4).
Husbands and wives are by no means supportive of each other. One mother of a son who had
assaulted his father (necessitating 10 stitches in the wound) when asked whether her husband could offer
her any emotional support retorted, ‘‘I would be happy enough if he stopped swearing’’ (Case 2). A
father, when asked if his wife shared her feelings about their son with him, answered ‘‘Of course. But I
am already very troubled and sometimes I tell her to be quiet.’’ Does he talk to her about his feelings of
unhappiness? ‘‘No’’ (Case 4). Many of them are not convinced that talking does any good. The husband
of one participant is currently living with his 90-year-old mother in his home village in China. Was she
in the habit of talking to her husband about her son? ‘‘Talk is no use.’’ Did she talk to friends? ‘‘No. If I
tell others, they will laugh at me. Sometimes when I go out with him, his arms and legs shake and people
would call out after him ‘‘stupid oaf, stupid oaf.’’ At this point, she began to weep (Case 5).
The events associated with the offence are often so traumatic for relatives that they seem to retire from
social life. The wife of one respondent abducted a child. The offence generated so much publicity that
there was no possibility of ensuring that family, friends, and neighbors did not know. Since then ‘‘I don’t
talk to my family and friends. I’ve become very low key.’’ Would he like to have someone to talk to?
‘‘Yes, of course. There are so many practical problems’’ (Case 9). Even when there is little publicity and
the family manages to sustain their secret, they may still withdraw from social contact. This is a mother
talking about a son who assaulted his boss unprovoked.
He cares a lot about his face. Not only does he want to save his face, I want to save mine, too. Though
I don’t feel his illness is a sin, sometimes when we go out, I could see his body trembling. Even I feel
uncomfortable, not to say other people. We have become distant from relatives and friends. I don’t
want to see them. I don’t go to visit even the closest ones because of my son, so that they won’t come
over to visit us. We don’t have anything to chat about. I have a son who is like this, alas. It is not a sin
but I feel very downhearted. (Case 3)
4. Discussion
We need to reiterate that the number of our participants is relatively small (23) and their experiences
are unlikely to reflect those of the entire population of relatives of forensic psychiatric patients. Even so,
there is still much that can be learned from them. The greatest stress for relatives came not from the
police or courts but seemed to be caused by the behavior of the media. Exposure of themselves and the
patient in the newspapers, particularly when accompanied by a picture, was a source of shame and
suffering, and the sense of stigma was acute. Such negative reporting has been well documented to
adversely affect the process of recovery and community reintegration of individuals with a mental illness
(Corrigan, 1998). Dealing constructively with the media is simply not in most people’s skill repertoire
and most would not predict that they would ever need such knowledge.
Hong Kong people are avid newspaper readers and a population of 6.8 million supports 14 general
daily papers—not counting those of a specialist nature (School of Journalism and Communication,
2001).) The irony is that the three with the largest circulation (The Sun, Apple Daily, and Oriental Daily
News), accounting for 70% of all papers sold in this category, are also rated by the general public (who
are buying them) to be the closest to works of pure fiction (Hutcheon, 1998). Research on credibility

V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374370
found that the public rated these three papers as the eleventh, thirteenth and 14th least credible of the
daily papers (School of Journalism and Communication, 2001). The Mingpao Daily is rated by the
public as the most credible of the daily papers in Hong Kong but it has a low circulation. As one of its
editorials comments, rather wistfully, ‘‘In Hong Kong a newspaper’s circulation does not increase with
its credibility’’ (November 16, 2001).
Public concern is constantly expressed about the lack of ethical behavior by reporters and photo-
journalists working for these papers. After a public outcry concerning particularly gross invasions of
privacy, the Hong Kong Press Council was established by Hong Kong journalists in 2000, supported by
voluntary financial contributions. The Council has set standards for ethical behavior in journalism, but
adhering to them is voluntary and the most notorious papers have not signed the necessary agreement,
nor are they members of the Press Council (http://www.presscouncil.org.hk). In light of the Hong Kong
government’s preference for the minimum of regulatory action on its part, it is most unlikely that stricter
standards would be proposed or policed, and certainly not legislated.
Another issue that emerges strongly from the interviews is the apparent lack of social and medical
services offered to either patient or family. Many of these families had been trying for many years to
cope with extraordinarily difficult behavior on the part of the patient and, other than access to medication
and periods of hospitalization, had received very little support in their efforts. Participants were not
knowledgeable about available services, and if they knew about them, they were uncertain how to access
them. Their impression was that once the patient was deemed recovered, it was then their job to provide
care. As we can see from the interviews, ambivalence characterized their attitudes towards the patients.
They were glad that they were out of harm’s way. However, they still felt the vestiges of affection for the
patients and thought that it was their duty to care for them at home. As mentioned in the Introduction,
this sense of the need to keep the family intact and to care for its vulnerable members is entirely typical
of Chinese families. However, based on our sample, there is no sense in which the large extended family
is involved in direct care. Indeed, the opposite seems to be the case: that severe psychiatric illness,
particularly with forensic involvement, actually causes the effective size of the family to shrink.
Their situation is exacerbated by what they perceive to be (and probably are) high levels of
discrimination and stigma associated with mental illness. One of our findings is the ostensibly
excessive lengths relatives go to keep the patient’s illness and offence a secret. Yet this may be for
a reason and they obviously feel it necessary to do so. It could be argued that in a ‘‘face’’-sensitive
society people will go to greater lengths to keep negative matters under wraps. On the other hand,
as was seen in the literature review, research in non-‘‘face’’-sensitive societies has found relatives
prone to experiencing similar reactions. Thus, what we have is not a difference in kind but, at most,
one of degree. Another explanation is that the level of negative feeling and stigma felt towards
people with a mental illness, combined with the tendency to blame the parents for the patient’s poor
behavior, is just so much greater in Hong Kong. This is by no means an unlikely explanation
(Cheung, 1990; Pearson & Yiu, 1993; Tam, 1986).
The findings of this research demonstrate that there is a lack of coordination between hospital- and
community-based rehabilitation services in Hong Kong. Huber (1996) described case management as
the process of linking, managing, and organizing services to meet client needs. Such client-focussed
coordination is lacking in Hong Kong although many social workers and other paraprofessionals have
been advocating true multidisciplinary team management and holistic care for at least two decades.
Service coordination and continuity of care remain largely unexplored areas. Patients with a forensic
history suffer a further difficulty in that many community-based facilities, for instance halfway houses,
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374 371
refuse to take those with a history of violence, however remote in time or person specific. This creates a
vacuum for those who no longer require hospitalization and yet where it would be clearly inadvisable to
discharge a patient to live with an elderly relative.
Overall our participants were not reluctant to be involved with patients and their treatment but it was
difficult for them to know how to be constructively involved. Some spoke vividly of the difficulty they
experienced in liaising with the hospital, finding a doctor who knew their relative and was knowledge-
able about the treatment plan, which led them to believe that there might not be one. Others were afraid
that if they became too ‘‘visible’’ to the hospital, this might encourage an unwelcome discharge. There is
no sense in these narratives of the relatives being treated as partners in care. Nor do they feel that their
legitimate needs (for instance, the need to feel safe in their own homes) are taken into account by those
caring for the patient. Of course, this is only one side of the story and hasty judgments should not be
drawn, but it does suggest that there is considerable room for improvement in communication between
relatives and health workers.
Relatives are also hampered by their lack of knowledge about mental illness (particularly
schizophrenia), services, formal legal procedures, and their rights. They would undoubtedly benefit
from access to information about these issues and even more so from a formal psychoeducation
program (Kuipers et al., 1992). These are not well established in Hong Kong, partly because the
practical problems in establishing them are formidable. These include the major targets being older,
illiterate women and the punishing working schedules of those in the work force that leave little time
for extra activities.
5. Conclusions
The sources of burden that the participants in this study experienced may be said to come from the
patient’s behavior and symptomatology, the nature of the offence, the response of family, workmates,
and others, and high levels of stigma against mentally ill people and especially those with an offending
background in Hong Kong society, the intrusive nature of the media, the lack of service provision, the
lack of service coordination, and the noncaring attitude that a number of service providers display. At
first sight, this list seems overwhelming, but there are areas in which changes could be made that would
bring about improvements without adding markedly to costs. For instance, it would be feasible to
nominate a minimum number of formal feedback sessions between ward staff and relatives over the
space of a year, with a brief written record of what was discussed to be kept by both parties.
Recognizing that relatives of forensic patients have needs of their own that are separate from those of
the patients would lead to greater resources being made available to them. One of the issues may be that
families do not approach service providers for assistance. They may not know the services are available,
or who to approach. Perhaps they are too ashamed to ask. Rather than waiting for a request for service
there is a strong argument to be made for proactive responses on behalf of service providers. A family
where a murder or other violent crime has taken place is almost certainly going to be in need of
counseling. It would be helpful if policies could be formulated so that in the face of a particular
circumstance (e.g., violence within the family, elderly mother living alone with male patient) services
were automatically offered/implemented. The conclusion regarding the current situation can only be that
the relatives of forensic psychiatric patients are in a most unenviable position, or in the words of one
mother, ‘‘I look at the sun and it has turned gray’’ (Case 15).
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374372
Acknowledgements
The research on which this article was based was supported by a grant from the Hong Kong Health
Services Research Committee.
The authors thank Ms. Zoeki Chan who carried out the interviews, transcription, and translation, and
Ms. Jan Tsang and Ms. Gladys Au Yeung who provided assistance in searching for local material in
Chinese-language data bases.
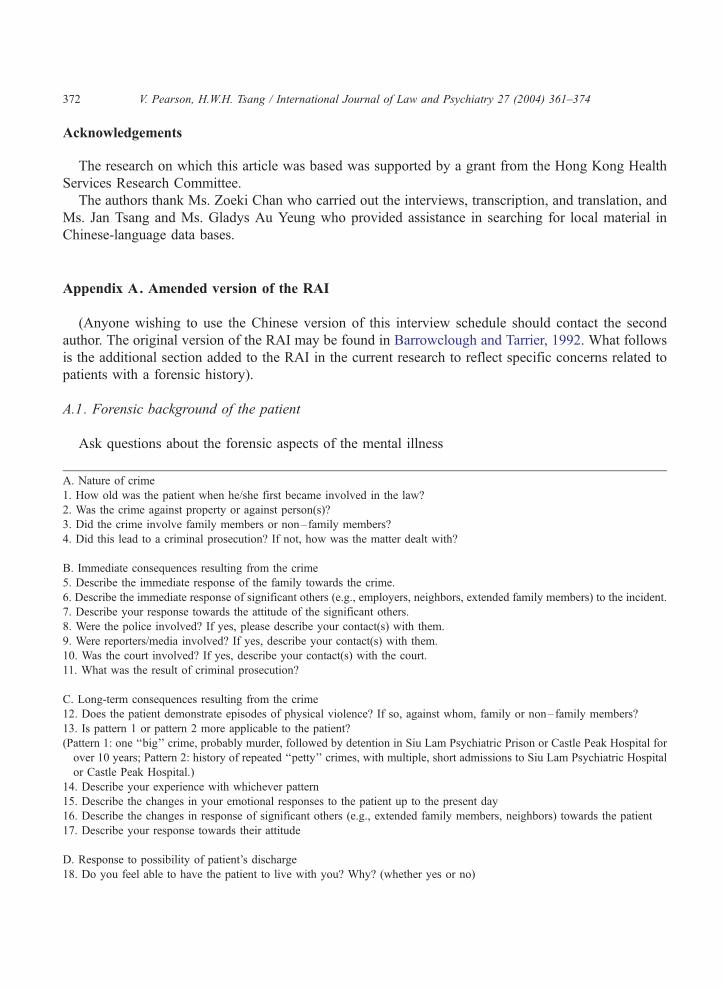
Appendix A. Amended version of the RAI
(Anyone wishing to use the Chinese version of this interview schedule should contact the second
author. The original version of the RAI may be found in Barrowclough and Tarrier, 1992. What follows
is the additional section added to the RAI in the current research to reflect specific concerns related to
patients with a forensic history).
A.1. Forensic background of the patient
Ask questions about the forensic aspects of the mental illness
A. Nature of crime
1. How old was the patient when he/she first became involved in the law?
2. Was the crime against property or against person(s)?
3. Did the crime involve family members or non–family members?
4. Did this lead to a criminal prosecution? If not, how was the matter dealt with?
B. Immediate consequences resulting from the crime
5. Describe the immediate response of the family towards the crime.
6. Describe the immediate response of significant others (e.g., employers, neighbors, extended family members) to the incident.
7. Describe your response towards the attitude of the significant others.
8. Were the police involved? If yes, please describe your contact(s) with them.
9. Were reporters/media involved? If yes, describe your contact(s) with them.
10. Was the court involved? If yes, describe your contact(s) with the court.
11. What was the result of criminal prosecution?
C. Long-term consequences resulting from the crime
12. Does the patient demonstrate episodes of physical violence? If so, against whom, family or non–family members?
13. Is pattern 1 or pattern 2 more applicable to the patient?
(Pattern 1: one ‘‘big’’ crime, probably murder, followed by detention in Siu Lam Psychiatric Prison or Castle Peak Hospital for
over 10 years; Pattern 2: history of repeated ‘‘petty’’ crimes, with multiple, short admissions to Siu Lam Psychiatric Hospital
or Castle Peak Hospital.)
14. Describe your experience with whichever pattern
15. Describe the changes in your emotional responses to the patient up to the present day
16. Describe the changes in response of significant others (e.g., extended family members, neighbors) towards the patient
17. Describe your response towards their attitude
D. Response to possibility of patient’s discharge
18. Do you feel able to have the patient to live with you? Why? (whether yes or no)

19. What help do you think you need from the doctors, nurses, social workers, and occupational therapists once the patient is
discharged?
20. Are you fearful that the patient will commit a crime again?
21. How would you help to prevent the patient from committing a crime again?
22. Are you concerned about the response of a) family and b) neighbors?
23. What problems do you think you might face?
E. Final question
24. Is there anything else I have not covered or you would like to tell me?
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374 373
Thank the relative for his/her cooperation.
References
Barrowclough, C., & Tarrier, N. (1992). Families of schizophrenic patients: Cognitive behavioral interventions. London:
Chapman and Hall.
Butzlaff, R. L., & Hooley, J. M. (1998). Expressed emotion and psychiatric relapse: A meta analysis. Archives of General
Psychiatry, 55, 547–552.
Cheung, F. M. (1990). People against the mentally ill; community opposition to residential treatment facilities. Community
Mental Health Journal, 26(2), 205–211.
Clark, R. E. (1994). Family costs associated with severe mental illness and substance use. Hospital and Community
Psychiatry, 45, 808–813.
Corrigan, P. W. (1998). The impact of stigma on severe mental illness. Cognitive and Behavioral Practice, 5, 201–222.
Gibbons, J. S., Horn, S. H., & Powell, J. M. (1984). Schizophrenic patients and their families; a survey in a psychiatric service
based on a district general hospital. British Journal of Psychiatry, 144, 70–77.
Gray, A. J. (2002). Stigma and psychiatry. Journal of the Royal Society of Medicine, 95(2), 72–77.
Huber, D. (1996). Leadership and nursing care management. Philadelphia: W.B. Saunders.
Hutcheon, S. J. (1998). Pressing Concerns: Hong Kong’s Media in an Era of Transition (Discussion Paper). The Joan
Shorenstein Center for Press, Politics and Public Policy, Harvard University, John F. Kennedy School of Government,
Boston, USA.
James, L. (1996). Family centered outreach for forensic psychiatric clients. Australian and New Zealand Journal of Mental
Health Nursing, 5, 63–68.
Kuipers, L. (1991). Schizophrenia and the family. International Review of Psychiatry, 3, 105–117.
Kuipers, L., Leff, J., & Lam, D. (1992). Family work for schizophrenia: A practical guide. London: Gaskell.
Kung, W. W. (2003). The illness, stigma, culture or immigration? Burdens on Chinese American caregivers of patients with
schizophrenia. Families in Society, p. 547.
Lam, D. H., Chan, C. K., & Leff, J. (1995). Family work for schizophrenia; some lessons for Chinese immigrant families.
Journal of Family Therapy, 17, 281–297.
Leff, J., & Vaughn, C. (1985). Expressed emotion in families: Its significance for mental illness. New York: Guilford Press.
Mari, J. D., & Streiner, D. L. (1994). An overview of family interventions and relapse on schizophrenia: Meta-analysis of
research findings. Psychological Medicine, 24, 565–578.
McCann, G. (1993). Relatives’ support groups in a special hospital: An evaluative study. Journal of Advanced Nursing, 18,
1883–1888.
McCann, G., & McKeown, M. (1995). Identifying the needs of relatives of forensic patients. Nursing Times, 91(24),
35–37.
McCann, G., McKeown, M., & Porter, I. (1995). Identifying the needs of relatives of forensic patients. Nursing Times, 9(24),
35–37.
McKeown, M., & McCann, G. (1995). A schedule for assessing relatives. The relative assessment interview for schizophrenia
in a secure environment (RAISSE). Psychiatric Care, 2(3), 84–88.
V. Pearson, H.W.H. Tsang / International Journal of Law and Psychiatry 27 (2004) 361–374374
McMillan, J. F., Gold, A., & Crow, T. J. (1986). The Northwick Park study of first episodes of schizophrenia: IV. Expressed
motion and relapse. British Journal of Psychiatry, 148, 133–143.
McNeil, D. E., Rosales, I. R., & Binder, R. L. (1992). Family attitudes that predict home placement of hospitalized
psychiatric patients. Hospital and Community Psychiatry, 43, 1035–1037.
Pearson, V., & Ning, S. P. (1997). Family care in schizophrenia. In N. Rhind, & C. Chan (Eds.), Social work in health care: The
Hong Kong scene. Hong Kong: Hong Kong University Press.
Pearson, V., & Yiu, M. Y. (1993). Public attitudes towards mental health facilities: A study in Hong Kong. Social Work and
Social Services Review, 4(1), 59–82.
Penn, D. L., & Mueser, K. T. (1996). Research update on the psychosocial treatment of schizophrenia. American Journal of
Psychiatry, 153(5), 607–661.
Perring, C., Twigg, J., & Aitken, K. (1990). Families caring for people diagnosed as mentally ill; the literature re-examined.
London: Her Majesty’s Stationery Office.
Phillips, M. R. (1993). Strategies used by Chinese families coping with schizophrenia. In D. Davis, & S. Harrell (Eds.), Chinese
families in the post-Mao era. Berkeley: University of California Press
Phillips, M. R., & Xiong, W. (1995). Expressed emotion in Mainland China: Chinese families with schizophrenic patients.
International Journal of Mental Health, 24, 54–75.
Phillips, M. R., Pearson, V., Li, F. F., Xu, M. J., & Yang, L. (2002). Stigma and expressed emotion: A study of people with
schizophrenia and their family members in China. British Journal of Psychiatry, 181, 488–493.
Pollio, D. E., North, C., & Foster, D. A. (1998). Content and curriculum in psychoeducational groups for families of persons
with severe mental illness. Psychiatric Services, 49(6), 816–826.
Salokangas, R. K. R., Daarinen, S., & Ojanen, M. (1992). Sairaalasta kotiutetut skitsofreniapotilaat I (Reports of Psychiatria
Fennica no. 97). Helsinki.
School of Journalism and Communication. (2001). Highlights of the surveys, November 14, 2001 (Press release). Hong Kong:
Chinese University of Hong Kong, School of Journalism and Communication.
Stengard, E., & Salokangas, R. K. R. (1997). Well-being of the caregivers of the mentally ill. Nordic Journal of
Psychiatry, 51(3), 159–164.
Tam, V. C. W. (1986). Community Response to a Mental Health Facility: A Study of the Objections to the Setting Up of a Half-
way House in Sun Tsui Estate, Sha Tin. Unpublished Master of Social Work dissertation, University of Hong Kong.
Trute, B., Tefft, B., & Segall, A. (1989). Social rejection of the mentally ill: A replication study of public attitudes. Social
Psychiatry and Psychiatric Epidemiology, 24, 69–76.
Tsang, H. W. H., Pearson, V., & Yuen, C. H. (2002). Family needs and burdens of psychiatric patients with a forensic history.
International Journal of Rehabilitation Research, 25, 25–32.
Vaddadi, K. S. (1996). Stress of caregiving for the chronically mentally ill. Psychiatric Annals, 26(12), 766–771.
Vaddadi, K. S., Gilleard, C. J., & Adlard, S. (1997). Mental illness, physical abuse and burden of care on relatives: A study of
acute psychiatric admission patients. Acta Psychiatrica Scandinavica, 95, 313–317.
Winefield, H. R., & Harvey, E. J. (1994). Needs of family caregivers in chronic schizophrenia. Schizophrenia Bulletin, 20(3),
557–566.