Embed Size (px)
Citation preview

Pediatric Pulmonology 36:43–48 (2003)
Duration of Effect of Intravenous Antibioticson Spirometry and Sputum Cytokines in Children
With Cystic Fibrosis
Steven Cunningham, MRCP, PhD,1* Janet R. McColm, PhD,1 Aileen Mallinson, RSCN,2
Ingrid Boyd, RSCN,2 and Tom G. Marshall, FRCP2
Summary. Intravenous (IV) antibiotics are amainstayof therapy in childrenwith cystic fibrosis. It is
unclear, however, over what period associated improvements in pulmonary function are maint-
ained, and towhat extent the underlying inflammatory process is impeded in children admitted for a
course of IV antibiotics. This was a prospective, interventional study of 14 children (median age,
14 years; interquartile range, 10–14) with cystic fibrosis who were regular sputum producers and
who required admission for a 2-week course of IV antibiotics. Children performed spirometry and
provided a sputum sample prior to starting IV antibiotics and then weekly for 6 weeks, the first
2 weeks of which IV antibiotics were given. Sputum IL-8, TNF-a, IL-6, IL-10, MIP1-a, and elastase
weremeasured. Seven children were asked to repeat the protocol in a subsequent exacerbation to
assess similarities in response to therapy. Significant improvements were seen in forced expired
volume in 1 sec (FEV1) in association with IV antibiotics (27% relative improvement in predicted
from baseline to end of week 1, median FEV1 41.3% increasing to 52.2%), but this continued
only 1 week following cessation of antibiotics. Although IL-8 demonstrated a trend for reduction
in association with antibiotics, no significant profile was demonstrated for any of the cytokines
assessed. IL-10 was detectable in 64% of samples (all<100 pg/ml). In children with two episodes
assessed, although there was a close correlation of FEV1 and FVC between exacerbations
(before antibiotics), no significant correlation was seen for IL-8, TNF-a, or IL-10 measured in both
sets of samples at any sample point (indeed, a discordant response was seen between sample
points in the two exacerbations). AlthoughFEV1 temporarily improves in response to admission for
IV antibiotics, no such response is seen in sputum cytokine values. In addition, assessment of
cytokines in subsequent exacerbations does not show a similar pattern of response to treatment.
Pediatr Pulmonol. 2003; 36:43–48. � 2003 Wiley-Liss, Inc.
Key words: cystic fibrosis; sputum; children; exacerbation; IL-8.
INTRODUCTION
Cystic fibrosis (CF) lung disease is characterized by anearly, sustained, and progressive inflammatory process,which occurs in response to infection and possibly as anintrinsic component of the disease.1–3 The use of intra-venous (IV) antibiotic courses has become a mainstay oftherapy in an attempt to keep inflammation under control.Studies clearly documented an improvement in pulmon-ary function in association with hospital admission for IVantibiotics,4 though the duration of effect has not beendocumented. In addition, the effects of antibiotics on theunderlying inflammatory process and the duration of thateffect have not been clearly demonstrated, as there are anumber of conflicting reports. Studies assessing the serumcytokine response to a 2-week course of IV antibioticsdemonstrated a reduction in TNF-a4–6 in some, but not allstudies.7 Cytokines are elevated in those with pulmonaryexacerbations, compared with stable patients in cross-sectional studies of sputum,8,9 but not bronchoalveolarlavage fluid.10 One paper assessing IL-6 and TNF-a in
sputum and serum demonstrated no response in sputum,but a reduction in serum IL-6 in response to 14 days of IVantibiotics.11
We hypothesized that 2-week courses of intravenousantibiotics would be able to sustain improvements in lungfunction longer than sputum inflammatory markers. We
1Department of Child Life and Health, University of Edinburgh, Edinburgh,
UK.
2Department of Respiratory and Sleep Medicine, Royal Hospital for Sick
Children, Edinburgh, UK.
*Correspondence to: Dr. Steven Cunningham, Department of Respiratory
and Sleep Medicine, Royal Hospital for Sick Children, Sciennes Road,
Edinburgh EH9 1LF, United Kingdom.
E-mail: [email protected]
Received 15 August 2000; Accepted 13 February 2003.
DOI 10.1002/ppul.10311
Published online in Wiley InterScience (www.interscience.wiley.com).
� 2003 Wiley-Liss, Inc.

also hypothesized that even if children did not have signi-ficant improvements in sputum inflammatory responseduring treatment (as demonstrated by previous conflictingreports), they would still follow the same pattern ofresponse in subsequent treatments.
The aim of this study was twofold: first, to identify in agroup of children the duration of improvement in pul-monary function afforded by a course of IVantibiotics fora pulmonary exacerbation, and whether a profile could bedetermined in sputum cytokine response over the sameperiod; and secondly, given previous conflicting reports inidentifying cytokine response to antibiotics, whether inthe same group of patients, the direction of change ofcytokines in response to antibiotic courses would beconsistent from one exacerbation to another.
MATERIALS AND METHODS
The study assessed children at our regional pediatric CFclinic whowere regular sputum producers andwere due tocommence a course of IV antibiotics for a pulmonaryexacerbation. Our policy was to treat pulmonary exacer-bations and not to give regular IVantibiotics (study criteriaof pulmonary exacerbation defined in accordance withpreviously reported criteria, i.e., any 4 of the following 12signs or symptoms: change in sputum; new or increasedhemoptysis; increased cough; increased dyspnea;malaise,fatigue, or lethargy; temperature above 388C; anorexia orweight loss; sinus pain or tenderness; change in sinusdischarge; change in physical examination of the chest;decrease in pulmonary function by 10% or more from apreviously recorded value; or radiographic changes indic-ative of pulmonary infection12). Two weeks of combinedIV antibiotics were given based on in vitro bacterialsensitivity testing: ceftazidime and tobramycinwere givenin 17 exacerbations, meropenem and tobramycin in 3, andceftazidime and colistin in 1.
Each child provided a sputum sample prior to startingIV antibiotics (sample 0). A further sample was thenobtained on the same day each week for 6 weeks (sevensamples in total). Spirometry forced expired volume in1 sec (FEV1) and forced vital capacity (FVC); Micro PlusSpirometer, Micro Medical) was measured at the sametime that each sputum sample was collected.
Further data on children were obtained from theirhospital notes or our cystic fibrosis database (age, recentChrispinNorman score, time since previous IVantibiotics,IgE level, Aspergillus RAST level, use of inhaled steroids,and oral antibiotics given before IVantibiotics).
Within the study period, we asked children to providea second set of samples during subsequent pulmonaryexacerbations, in order to assess the relation of cytokinemarkers between exacerbations.
Two groups of patients will therefore be described.Group 1 contains children providing one series of seven
spirometry and sputum samples during a single exacerba-tion. Group 2 consists of those children who provided twoseries of samples during two exacerbations. In the case ofthose children with two series of samples, the secondseries of samples onlywas included in group 1 analyses, asthese included IL-6 and elastase measurements. Inchildren with two series of measurements, values for IL-8, IL-10, and TNF-a were compared between first andsecond monitored exacerbations.
Sputum Processing
Sputum samples were held in a ‘‘coolbag’’ followingcollection and transferred to the laboratory within 3 hr ofcollection (mean time to processing, 1.9 hr). Samplevolume was measured, and samples were mixed with 1 Mphosphate-buffered saline (ratio, 1:1). Samples were thenhomogenized by vortexing for at least 30 sec and thencentrifuged for 30 min at 2,000g at 48C.9,13 The resultingsupernatant was aliquoted and kept at �708C until analy-sis. Assessment of untreated sputum samples is recom-mended for the assessment of cytokines in sputum.14
Cytokine Assays
Interleukin 10 (IL-10), interleukin 6 (IL-6), and tumornecrosis factor alpha (TNF-a) were measured by ELISAkit (R&D Systems Europe, Ltd., Abingdon, Oxon,UK).15,16 Interleukin 8 (IL-8) was measured by in-houseradioimmunoassay. Elastase was measured by spectro-photometric assay: briefly, equal volumes of sputumsample and substrate (N-methoxysuccinyl A-A-P-Vp-nitroanilide 0.1 mg/ml, Sigma) were incubated at 378Cfor at least 15 min. The resulting color development wasread at 405 nm and compared to a standard of elastase(Elastine Products, Owensville, MO) of 7.8–2,000 ng/ml.Elastase (7.8–2,000 ng/ml: intra-assay, 6.2%; interassay,13.8%). IL-8 (19.5–2,500 pg/ml: intra-assay, <5%;interassay, 13.8%). Because of sample quantity restric-tions, elastase and IL-6 were measured in samples fromthe final 15 treatment episodes.
Interleukin 8 was measured, as it is considered one ofthe main chemoattractants in CF airways, being inducedby both TNF-a and elastase.3 IL-6 is also a proinflamma-tory cytokine found in CF airways.3 Interleukin-10 is animportant anti-inflammatory cytokine, able to down-regulate production of IL-8, TNF-a, and many otherproinflammatory cytokines.3
Statistics
Descriptive statistics are generally provided as median(interquartile range) unless otherwise indicated. Correla-tion was by Spearman rank. Differences were determinedbyStudent’s t-test orMann-WhitneyU test, as appropriate.
44 Cunningham et al.
Consent
Informed consent was obtained from both parents andchildren. Ethical approval was given to the study by thePaediatric/Reproductive Medicine Research Ethics Sub-Committee of the Lothian Research Ethics Committee.
RESULTS
Group 1: Effect of IV Antibiotics on Spirometryand Sputum Cytokines and Elastase Duringand After a Single Exacerbation
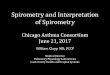
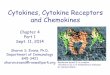
Fourteen children (3 female, 11 male) with a medianage of 14 years (interquartile range (iqr), 10–14 years)received a median 14 days of IV antibiotics (iqr, 14–16.5 days); 5 children received inhaled steroidmedication;5 receivedDNase therapy. All but one of the children (whohad Stenotrophomonas maltophilia) were chronicallycolonized with Pseudomonas aeruginosa. Children inthis group had a median Chrispin Norman score of 14 (iqr,10–18), IgE 60 ng/l (iqr, 26–96), and a median of 5months (iqr, 3–9) since receiving their last IV antibioticcourse. Children provided amedian of 7 samples (iqr, 5.5–7) from a maximum 7 samples requested.
Spirometry and sputum cytokine/elastase measure-ments obtained in the seven weekly samples are shownin Table 1.
There was a significant improvement in FEV1 inassociation with 2 weeks of IVantibiotics (Table 1). Thisimprovementwas short-lived, however, as FEV1 remainedsignificantly higher than baseline for only 1 week afterstopping antibiotics, and returned to baseline by 4 weekspostantibiotics. Although a trend was observed for animprovement in FVC during antibiotic therapy, no signi-ficant difference was found compared with pretreatmentvalues (Table 1).
Sputum cytokines demonstrated a trend for a reductionin IL-8 and (paradoxically) IL-10 values in associationwith IV antibiotic courses, but the range of values waswide, and consequently there were no significant differ-ences between values measured at sample 0 with samples1–6 for any cytokines/elastase measured. The time tominimumvalues17 assayedwas broadly spread throughoutthe period of study and was not concentrated during orafter antibiotics courses (Table 1).
Therewas no consistent significant correlation betweenIL-8, IL-6, IL-10, TNF-a, and elastase concentrations insputum and lung function measurements (FEV1 and FVC)taken simultaneously.
Of the other factors assessed, there was no consistentcorrelation between cytokine/elastase concentrations andthe child’s age, recent Chrispin Norman score, number ofdays of IV antibiotics, time since previous antibiotics, orrecent IgE level. There was also no significant differencein cytokine/elastase values found in those using inhaled T
AB
LE
1—
Sp
iro
metr
yan
dS
pu
tum
Cyto
kin
eM
easu
rem
en
tsB
efo
re,
Du
rin
g,
an
dA
fter
IVA
nti
bio
tics
1
Sam
ple
Pre-treatment0
1(Ivs)
2(IVs)
34
56
IL-8
(ng/m
l)27.5
(17.9–39.0)
26.4
(22.3–34.8)
21.8
(2.9–37.0)
21.4
(14.5–31.9)
22.3
(15.9–46.5)
26.7
(16.5–40.8)
26.3
(22.5–54.5)
TNF-a
(pg/m
l)1,089(324–1,265)
195(81–1,304)
729(128–952)
572(110–1,849)
323(112–1,219)
600(401–1,264)
612(313–1,255)
IL-6
(pg/m
l)33.7
(9.9–165.1)
42.1
(24.0–146.9)
38.5
(16.6–300.7)
87.9
(3.6–179.1)
39.4
(13.3–206.1)
32.5
(7.5–554.6)
22.3
(12.7–2,428.9)
IL-10(pg/m
l)12.9
(0.0–31.5)
0.0
(0.0–31.0)
8.2
(0.0–12.4)
12.8
(1.4–30.5)
2.8
(0.0–15.4)
11.2
(0–34.1)
18.2
(6.7–37.8)
Elastase(mg/m
l)257.0
(33.1–454.0)
48.8
(0–204.9)
148.4
(0–268.0)
119.5
(4.3–207.6)
284(60.5–352.5)
114.5
(49.4–196.5)
260.0(182.0–431.3)
FVC(%
predicted)
62.0
(37.8–74.7)
68.5
(39.1–80.9)
70.6
(35.7–84.2)
67.4
(36.9–76.9)
58.8
(40.3–82.5)
63.3
(36.6–74.1)
57.8
(35.7–77.8)
FEV1(%
predicted)
41.3
(29.1–58.2)
52.2*(35.3–73.4)
49.6*(31.7–60.9)
49.9*(28.5–71.6)
43.7
(27.6–65.5)
42.9
(27.2–63.1)
40.7
(32.6–60.9)
1Values
aremedian(interquartilerange).
*P<0.05compared
withbaseline(sam
ple0).
Duration of Effect of Antibiotics in CF 45

steroids, nebulized colistin, or acute antibiotic coursesgiven prior to IV courses. There was a significant differ-ence seen in elastase levels between those groups receiv-ing and not receiving prophylactic antibiotics (samples 0and 2; P< 0.05).
Group 2: Comparison of Sputum Cytokine/ElastaseMeasurements Made at the Same Time PointsDuring Two Treatment Episodes
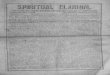
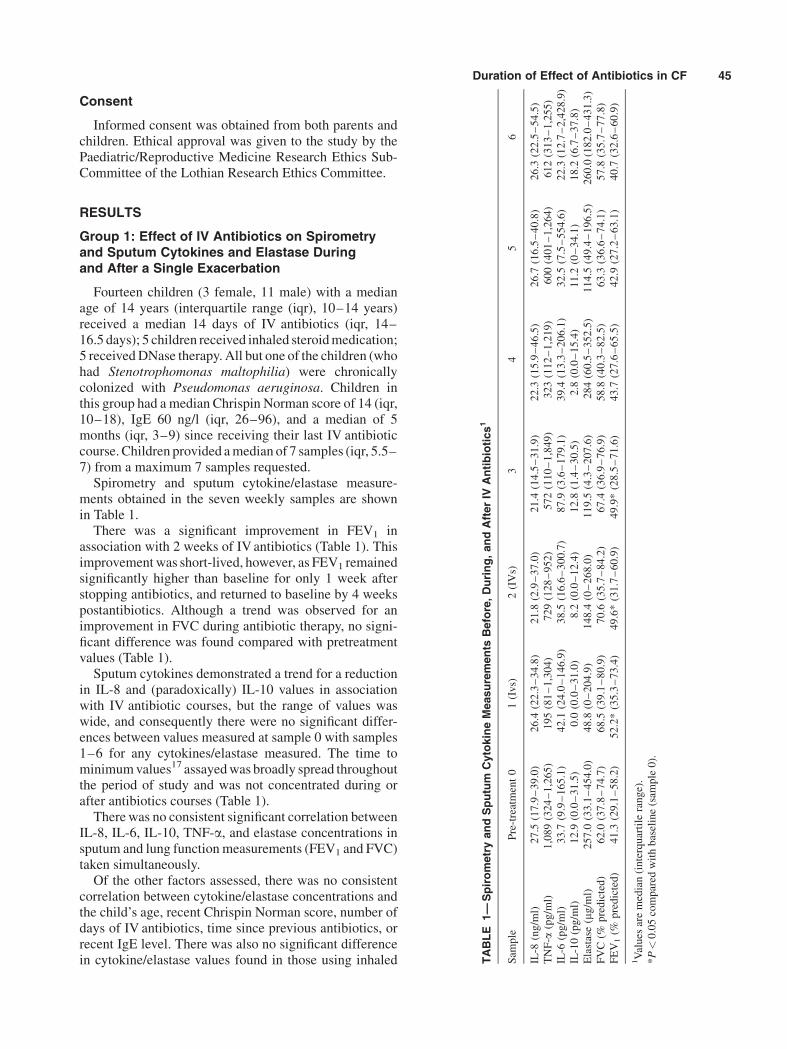
Seven children provided two sets of samples: 3 femalesand 4 males, median age 14.7 years (iqr, 9.3–15.8). Themedian time difference between start of sample collectionfor first and second IV antibiotic courses was 431 days(iqr, 400–436). Children were given a year betweensampling to encourage participation and to minimize‘‘study fatigue.’’
Table 2 shows the data for the children providing twosets of data. There was a significant and strong correlationbetween the two episodes at sample 0 for both FEV1
(r¼ 0.96, P¼ 0.037) and FVC (r¼ 0.99, P¼ 0.004).However, sputum cytokine values did not significantlycorrelate at this sample point (Table 2). In addition, thedirection of change in sputum cytokines in response to IVantibioticswas not consistent fromweek toweek for eitherIL-8, TNF-a, or IL-10. In many instances there was adiscordant change of direction between sample points inthe first and second episodes assessed (data not shown).
DISCUSSION
Our first hypothesis (that improvements in lungfunction would be sustained longer than changes insputum inflammatory markers) was confirmed, thoughthe duration of this effect was shorter than was expected(1 week), and the effects of treatment on sputum inflam-matory markers was limited to a nonsignificant trend. Wealso hypothesized, however, that even if sputum inflam-matory markers appeared a poor indicator of response totreatment, then the trend in subsequent exacerbationswould be similar. This hypothesis was incorrect, and noconsistent trend in response was seen.
Although it is always encouraging to note improve-ments in lung function in patients admitted for courses ofIVantibiotics, it is disappointing that the duration of effectwas so short (1 week). Other groups demonstrated animprovement in FEV1 in association with IV antibioticstherapy for a pulmonary exacerbation, without identifyinglength of treatment effect.4,18,19 As clinicians, we oftenconsider that IV antibiotic courses confer significant im-provement to our patients, though our results would sug-gest that in reality the effect is short-lived, and far less thanthe 3 monthly antibiotic regimen used by many centers.
The assessment of the inflammatory profile in our child-ren did not demonstrate a consistent pattern of cytokine/elastase response to a course of IV antibiotics. Although T
AB
LE
2—
Co
mp
ari
so
no
fS
pir
om
etr
yan
dS
pu
tum
Cyto
kin
es
inT
wo
IVT
reatm
en
tE
pis
od
es
1
Sam
ple
Group
0(pretreatm
ent)
1(IVs)
2(IVs)
34
56
12
12
12
12
12
12
12
IL-8
(ng/m
l)35.2
(21.7–51.6)
28.5
(25.5–33.2)
29.7
(23.4–71.6)
28.0
(25.7–33.5)
25.2
(14.6–53.3)
28.3
(18.5–42.4)
22.3
(16.4–52.1)
22.3
(17.1–30.9)
64.2
(27.3–81.1)
24.8
(15.9–44.1)
49.7
(38.5–50.4)
24.1
(19.9–36.5)
43.2
(36.2–48.1)
35.4
(31.7–73.5)
TNF-a
(pg/m
l)716.0(413–861)1,089.0
(629–1,179)
803.0
(144–1,398)
1,322.0
(705–2,221)
372.0
(168–589)
806.0
(457–1,083)
360.0
(81–396)
1,708.0
(1,091–2,605)995.0
(122–1,714)
911.0
(475–1,219)
500.0(121–1,626)
1,307.0
(1134–2,383)
382.0
(226–981)
911.0
(404–1,295)
IL-10(pg/m
l)9.6
(8.3–32.7)
16.2
(0.0–28.3)
24.1
(17.4–31.0)
4.0
(0.0–29.9)
18.0
(6.7–20.6)
5.0
(0.0–10.2)
26.4
(17.0–50.2)
18.5
(13.8–30.5)
16.8
(11.8–22.2)
5.9
(0.0–14.5)
40.1
(19.3–42.9)
0.0
(0.0–9.8)
31.2
(24.0–47.9)
15.0
(7.2–41.5)
FEV1%
predicted
27.2
(25.5–31.9)
32.3
(21.5–41.7)
39.4
(28.8–42.3)
35.8
(23.8–52.2)
38.1
(26.0–50.1)
41.1
(31.7–56.6)
35.9
(25.5–43.7)
45.1
(31.9–51.5)
29.0
(24.6–40.2)
39.8
(31.9–51.7)
25.8
(22.7–37.1)
39.7
(30.4–49.8)
33.4
(28.1–37.1)
40.2
(34.5–53.0)
FVC%
predicted
39.1
(35.5–49.9)
36.8
(32.3–57.6)
46.2
(38.5–58.4)
39.1
(30.6–65.1)
42.3
(37.7–65.4)
54.1
(35.8–74.4)
44.4
(36.1–57.7)
58.3
(36.9–74.7)
42.8
(40.5–56.2)
42.2
(36.1–65.7)
37.9
(31.5–41.7)
52.4
(36.6–71.1)
41.2
(38.3–44.8)
40.2
(35.7–68.6)
1Values
aremedian(interquartilerange).
46 Cunningham et al.

onemight expect that improved airway clearance, reducedbacterial load, and improved nutrition might reduce thecytokines present in sputum, it is possible that suchtherapy, having so short a duration of effect on airwayobstruction, does not satisfactorily alter the degree ofinflammation in the lower airways. Other groups alsonoted little variability in sputum inflammatory markersbetween periods of exacerbation and stability.20–22
However, our systematic sampling before, during, andafter an exacerbation treatment enabled us to provide anoptimal opportunity for assessing both effect and possibleduration of effect and a broad range of inflammatorymarkers and lung function.
The reasons for the apparent limited improvement ininflammatory markers during treatment are unclear. Atrend for improvement was demonstrated in IL-8 andTNF-a, but not other markers. There are conflictingreports with regard to the effects of bacterial load on levelsof inflammatory mediators: some reports conclude thatbacterial load is important in determining IL-8 levels inCFairways,23 while others do not find such an association.24
Many clinicians would expect a course of IVantibiotics toreduce bacterial load, improve airway clearance, and havean influence on sputum levels of inflammatory mediators.Sputum processing can have important effects on themeasurement of cytokines, as can assay techniques.Attempts at standardization are now being addressed,but great variability persists.25We assessed samples usingan ‘‘untreated’’ processing method. The use of untreatedprocessing has been confirmed as useful in the assessmentof cytokines within sputum samples.14 Additional varia-tion in results may occur when sputum derives fromdifferent areas of the lung, with variable levels of inflam-mation; as such, cytokine assays may not represent apicture consistent with inflammation within the lung.26 Itis also possible that antibiotics, particularly those used incystic fibrosis, could be responsible for upregulation ofcytokine production,27 and that ceftazidime in thepresence of organisms can lead to higher concentrationsof IL-6 and TNF-a than other antibiotics.28,29 This up-regulation of cytokines by antibiotics, associated withendotoxin-induced cytokine release from bacterial killing,might mask any potential benefit to measured sputumcytokines afforded by courses of IVantibiotics.
We chose to assess inflammatory markers in sputum asopposed to blood or bronchoalveolar lavage, as repeatedsputum samples may be obtained frequently with thewilling consent of the patient, and this consequentlyallows for a more intensive longitudinal assessment of theinflammatory profile in response to an intervention. Inaddition, sputum (when compared with serum) isconsidered to better represent the local cytokine reactionin the lung, and hence to be of more relevance to lunginjury in CF.7 Cross-sectional studies demonstrated thatsputum contains significant quantities of inflammatory
markers, the levels of which correlate well with simulta-neous measurements made by bronchoalveolar lavage.30
With variability in sputum cytokine values, large numbersof patients would be required to ensure that type 2 erroris limited. The intensive nature of sample collection in thisstudy limited our study numbers, and studies of this naturemay be limited by the significant logistic difficulties ofobtaining such regular samples at school and home duringthe follow-up period.Manymarkers have been explored to help determine the
concentration of lung fluids, though none have beenwidely accepted. Albumin, urea, total protein, and sur-factant proteins have been investigated without success.Noah et al. recently demonstrated that adjusting foralbumin, urea, or body weight does not improve thereliability ofmeasurements in lung fluids.10 In the absenceof other evidence,31 we chose to assess concentrationswith reference to volume of supernatant obtained.Although therewere no significant changes in cytokines
during the courses of antibiotics, the trend for a reductionin both IL-8 and also TNF-a should be noted. It is possiblethat larger numbers of children, or a more prolongedcourse of therapy, could begin to demonstrate a clearerpattern of cytokine suppression. Interleukin 10 suppressesmany cytokines and so is regarded as potentially importantin restraining proinflammatory cytokines in CF lungdisease.32 Interleukin 10 was detectable in 64% of oursamples, though we required a high-sensitivity assay fordetection, with all values<100 pg/ml. Balfour-Lynn et al.could not demonstrate IL-10 in sputum samples,33 andBonfield et al. demonstrated IL-10 in 59% of 22 CF bron-choalveolar lavage samples at a median of 869 pg/ml.32
The reasons for such low levels of IL-10 in cystic fibro-sis are unclear, though this may have important implica-tions for the proinflammatory cytokine profile in CFpatients. Other inflammatory conditions also demon-strated a raised IL-8, with a marked reduction in IL-10.34
The trend for improvement in sputum inflammatorymarkers in our study and those previously discussedsuggests that similar inflammatory profiles may be seen inthe same patient during subsequent exacerbations. We didnot demonstrate any correlation of note between the firstand second treatment episodes; indeed, at certain timepoints in some individuals, there seemed to be an oppositeresponse by individual cytokines. This contrasts withpulmonary function, where a significant association wasdemonstrated between exacerbations. This discordantcytokine response in the same patient to what clinicallyappears to be the same degree of pulmonary infection, interms of symptoms and lung function, is disappointing.In conclusion, while FEV1 improves during admission
for IV antibiotic courses, it may not reflect an improve-ment in underlying pulmonary inflammation. Sputumcytokines do not demonstrate predictable changes duringadmission and follow-up of pulmonary exacerbations, and
Duration of Effect of Antibiotics in CF 47
do not demonstrate repeatable patterns of response withtreatment of subsequent exacerbations.
REFERENCES
1. Armstrong DS, Grimwood K, Carzino R, Carlin JB, Olinsky A.
Lower respiratory infection and inflammation in infants with
newly diagnosed cystic fibrosis. Br Med J [Clin Res] 1995;310:
1571–1572.
2. Khan TZ, Wagener JS, Bost T, Martinez J, Accurso FJ, Riches
DWH. Early pulmonary inflammation in infants with cystic
fibrosis. Am J Respir Crit Care Med 1995;151:1075–1082.
3. Konstan MW, Berger M. Current understanding of the inflamma-
tory process in cystic fibrosis: onset and etiology. Pediatr Pulmonol
1997;24:137–142.
4. Norman D, Elborn JS, Cordon SM, Raynor RJ, Wiseman MS,
Hiller EJ, Shale DJ. Plasma tumour necrosis factor alpha in cystic
fibrosis. Thorax 1991;46:91–95.
5. Peckham D, Crouch S, Humphreys H, Lobo B, Tse A, Knox JA.
Effect of antibiotic treatment on inflammatory markers and lung
function in cystic fibrosis patients with Pseudomnonas cepacia.
Thorax 1994;49:803–807.
6. Rayner RJ, Wiseman WS, Cordon SM, Norman D, Hiller EJ.
Inflammatory markers in cystic fibrosis. Respir Med 1991;85:
139–145.
7. Wilmott RW, Frenzke M, Kociela V, Peng L. Plasma interleukin-1
alpha and beta, tumor necrosis factor-alpha, and lipopolysacchar-
ide concentrations during pulmonary exacerbations of cystic
fibrosis. Pediatr Pulmonol 1994;18:21–27.
8. Schuster A, Haarmann A, Wahn V. Cytokines in neutrophil-
dominated airway inflammation in patients with cystic fibrosis.
Eur Arch Otorhinolaryngol 1995;252:59–60.
9. Francoeur C, Denis M. Nitric oxide and interleukin-8 as inflam-
matory components of cystic fibrosis. Inflammation 1995;19:
587–598.
10. Noah TL, Black HR, Cheng PW, Wood RE, Leigh MW. Nasal and
bronchoalveolar lavage fluid cytokines in early cystic fibrosis.
J Infect Dis 1997;175:638–647.
11. Nixon LS, Yung B, Bell SC, Elborn JS, Shale DJ. Circulating
Immunoreactive Interleukin-6 in cystic fibrosis. Am J Respir Crit
Care Med 1998;157:1764–1769.
12. Fuchs HJ, Borowitz DS, Christiansen DH, Morris EM, Nash ML,
Ramsey BW, Rosenstein BJ, Smith AL, Wohl ME. Effect of
aerosolized recombinant human DNase on exacerbations of
respiratory symptoms and on pulmonary function in patients
with cystic fibrosis. N Engl J Med 1994;331:637–642.
13. Koller DY, Nething I, Otto J, Urbanek R, Eichler I. Cytokine
concentrations in sputum from patients with cystic fibrosis and
their relation to eosinophil activity. Am J Respir Crit Care Med
1997;155:1050–1054.
14. Woolhouse IS, Bayley DL, Stockley RA. Effect of sputum
processing with dithiothreitol on the detection of inflammatory
mediators in chronic bronchitis and bronchiectasis. Thorax 2002;
57:667–671.
15. Stockley RA, Bayley DL. Validation of assays for inflammatory
mediators in sputum. Eur Respir J 2000;15:778–781.
16. Takanashi S, Hasegawa Y, Kanehira Y, Yamamoto K, Fujimoto K,
Satoh K, et al. Interleukin-10 levels in sputum is reduced in
bronchial asthma, COPD and in smokers. Eur Respir J 1999;14:
309–314.
17. Matthews JNS, Altman DG, Campbell MJ, Royston P. Analysis of
serial measurements in medical research. Br Med J [Clin Res]
1990;300:230–235.
18. Niggemann B, Stiller T, Magdorf K, Wahn U. Myeloperoxidase
and eosinophil cationic protein in serum and sputum during
antibiotic treatment in cystic fibrosis patients with Pseudomonas
aeruginosa infection. Mediators Inflammation 1995;4:282–288.
19. Smith AL, Redding G, Doershuk C, et al. Sputum changes
associated with therapy for endobronchial exacerbation in cystic
fibrosis. J Pediatr 1988;112:547–554.
20. Salva PS, Doyle NA, Graham L, Eigen H, Doerschuk CM. TNF-a,IL-8, soluble ICAM-1 and neutrophils in sputum of cystic fibrosis
patients. Pediatr Pulmonol 1996;21:11–19.
21. Wolter JM, Rodwell RL, Bowler SD, McCormack JG. Cytokines
and inflammatory mediators do not indicate acute infection in
cystic fibrosis. Clin Diagn Lab Immunol 1999;6:260–265.
22. Karpati F, Hjelte FL, Wretlind B. TNF-a and IL-8 in consecutive
sputum samples from cystic fibrosis patients during antibiotic
treatment. Scand J Infect Dis 2000;32:75–79.
23. Muhlebach MS, Stewart PW, Leigh MW, Noah TL. Quantitation
of inflammatory responses to bacteria in young cystic fibrosis and
control patients. Am J Respir Crit Care Med 1999;160:186–191.
24. Sagal SD, Sontag MK, Wagener JS, Kapsner RK, Osberg I,
Accurso FJ. Induced sputum inflammatory markers correlate with
lung function in children with cystic fibrosis. J Pediatr 2002;141:
811–817.
25. Djukanovic R, Sterk PJ, Fahy JV, Hargreave FE. Standardised
methodology of sputum induction and processing. Eur Respir J
[Suppl] 2002;20:15–25.
26. Dakin CJ, Pereira JK, Henry RL, Wang H, Morton JR.
Relationship between sputum inflammatory markers, lung func-
tion, and lung pathology on high-resolution computed tomogra-
phy in children with cystic fibrosis. Pediatr Pulmonol 2002;33:
475–482.
27. Riesbeck K, Sigvardsson M, Leanderson T, Forsgren A. Super-
induction of cytokine gene transcription by ciprofloxacin. J
Immunol 1994;153:343–352.
28. Prins JM, Kuijper EJ, Mevissen ML, Speelman P, van Deventer
SJ. Release of tumor necrosis factor alpha and interleukin 6
during antibiotic killing of Escherichia coli in whole blood:
influence of antibiotic class, antibiotic concentration, and pre-
sence of septic serum. Infect Immununol 1995;63:2236–2242.
29. Schneider CM, Huzly D, Vetter C, von Specht BU, Daschner FD.
Tumor necrosis factor alpha and interleukin 6 release induced by
antibiotic killing of Pseudomonas aeruginosa and Staphylococcus
aureus. Eur J Clin Microbiol Infect Dis 1997;16:467–471.
30. Dean TP, Dai Y, Shute JK, Church MK, Warner JO. Interleukin-8
concentrations are elevated in bronchoalveolar lavage, sputum,
and sera of children with cystic fibrosis. Pediatr Res 1993;34:
159–161.
31. de Blic J, Midulla F, Barbato A, Clement I, Dab I, Eber E,
Green C, Grigg J, Kotecha S, Kurland G, Pohunek P, Ratjen F,
Rossi G, for ERS Task Force on Bronchoalveolar Lavage in
Children. Bronchoalveolar lavage in children. Eur Respir J 2000;
15:217–231.
32. Bonfield TL, Panuska JR, Konstan MW, et al. Inflammatory
cytokines in cystic fibrosis lungs. Am J Respir Crit Care Med
1995;152:2111–2118.
33. Balfour-Lynn IM, Klein NJ, Dinwiddie R. Randomised controlled
trial of inhaled corticosteroids (fluticasone propionate) in cystic
fibrosis. Arch Dis Child 1997;77:124–130.
34. Jones CA, Cayabyab RG, Kwong KC, et al. Undetectable
interleukin (IL)-10 and persistent IL-8 expression early in hyaline
membrane disease: a possible developmental basis for the
predisposition to chronic lung inflammation in preterm newborns.
Pediatr Res 1996;39:966–975.
48 Cunningham et al.