Embed Size (px)
Citation preview

Dual-time point 18F-FDG PET/CT scan: is it always working?
Dr. Hussein R. S. Farghaly Prince Sultan Military Medical City

• The utility of 18F-fluorodeoxyglucose (FDG) PET/CT is widely used for the management of patients with cancer including several aspects including diagnosis, staging, restaging, monitoring therapeutic intervention and radiotherapy planning.
• However, FDG is not a tumor specific and accumulates also in the inflammatory lesions. So recently F-18 FDG PET/CT is also used for detection, characterization, and monitoring of patients with infectious and non-infectious inflammatory processes.
• Because of this non-specific uptake of FDG in benign processes such as inflammation and infection, distinguishing malignant lesions from benign ones can be difficult in some cases.
• Dual time point (DTP) and delayed FDG-PET imaging protocols were developed to enhance the ability of FDG PET/CT for distinction between malignant and benign lesions.
• The rational for DTP is that pattern and rate of FDG uptake over time vary considerably between malignant and benign processes.
Rational of Dual Time Point FDG PET/CT


FDG Uptake in Malignant cell vs. inflammatory cell
Malignant Cell Inflammatory Cell
FDG FDG FDG-6P
High levels of hexokinase
low levels of glucose-6-phosphatase G
LUT
FDG
Low levels of hexokinase
High levels of glucose-6-phosphatase,
FDG FDG-6P
FDG

• There is evidence in the recent literature of the clinical usefulness of dual-time-point FDG-PET imaging in a wide variety of malignancies, including those of head and neck, lung, breast, gallbladder, cervix, liver, and in brain tumors.
• A lesion is likely to be malignant if the standard uptake value increases over time, whereas it is likely to be benign if the standard uptake value is stable or decreases.
• However; there is also evidence in the literature of limited value of DTP FDG –PET such as in characterization of lung nodules, mediastinal lymph nodes (TB endemic areas), primary esophageal car

Studies showed added value of DTP

Studies showed limited value of DTP

In our center we reviewed 60 consecutive patients with cancer (19 women, 41 men) with mean age of 63±10.4 years. All patients suspected to have malignant lesions and investigated by performing whole body PET/CT at 60 minutes and delayed limited PET/CT on areas of interest at 120 minutes after the tracer injection. Visual and semiquantitative analysis was performed on both the early and delayed images. All findings were confirmed by histopathology and/or at least 3 months imaging follow-up (clinical, PET/CT, CT or/and MRI).
The result consider true positive (TP) in lesions with increased SUV in delayed image and confirmed to be malignant, false positive (FP) in lesions with increased SUV and confirmed to be benign, true negative (TN) in lesions showed decreased or unchanged SUV and confirmed to be benign and false negative (FN) in lesion showed decreased or unchanged SUV and confirmed to be malignant.
DTP FDG-PET/CT preliminary research in PSMMC

Preliminary Results:
• The total number of suspicious lesions was 82 (the common lesions were 10 presacral soft tissue lesions in rectal car., 9 lung nodules, 7 hepatic lesions, 8 rectal lesion, , 9 Hodgkin’s disease (HD) lesions, 8 head and neck (H&N) lesions, 7 Non-Hodgkin’s lymphoma (NHL) lesions).
• 32 lesions were histopathologically confirmed and 50 lesions confirmed based on 3 months imaging follow-up.
• There were 33 TP lesions, 27 FP, 22 NT and no FN results.
• The overall sensitivity was 98.5% of DTP FDG PET/CT in detecting suspicious lesions.
• The specificity was 44.9% in differentiating benign from malignant lesions and the accuracy was 67%. PPV was 55%, NPV 100%.

• Preliminary Result cont.
• All hepatic lesions were TP.
• Lung nodules showed 5 TP, 2 FP and 2 TN with accuracy 78%.
• Rectal lesions showed 1 TP, 3 FP and 4 TN with accuracy of 62%.
• Presacral soft tissue lesions showed 2 TP, 2 FP and 6 TN with accuracy 80%.
• Mediastinal LN showed accuracy of 33.3%.
• HD lesions showed accuracy of 78% and NHL lesions showed accuracy of 71%.
• H&N lesions (LN and suspicious recurrent lesions) showed accuracy 75%
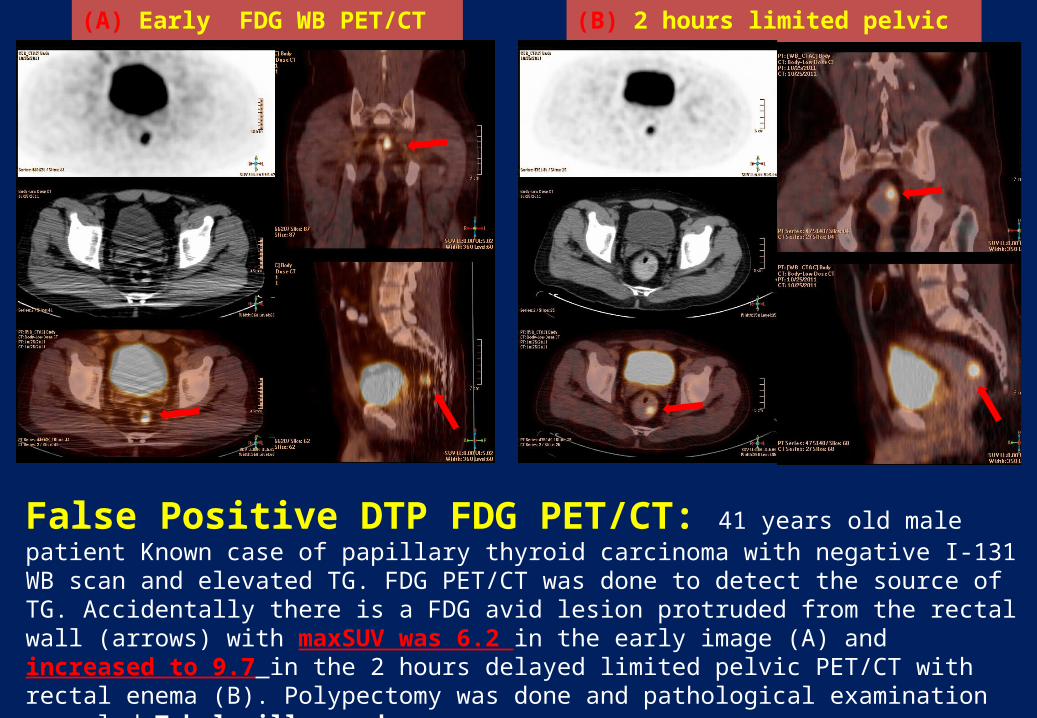
False Positive DTP FDG PET/CT: 41 years old male patient Known case of papillary thyroid carcinoma with negative I-131 WB scan and elevated TG. FDG PET/CT was done to detect the source of TG. Accidentally there is a FDG avid lesion protruded from the rectal wall (arrows) with maxSUV was 6.2 in the early image (A) and increased to 9.7 in the 2 hours delayed limited pelvic PET/CT with rectal enema (B). Polypectomy was done and pathological examination revealed Tubulovillous adenoma.
(A) Early FDG WB PET/CT scan (B) 2 hours limited pelvic PET/CT

(A) Early WB FDG PET/CT Fusion ( sagital. Coronal and axial)
(B) 2 hours Delayed limited Chest FDG PET/CT Fusion ( sagital. Coronal and axial)
True Positive DTP FDG PET/CT: 46-yr-old female patient known case of breast Ca with pulmonary nodule. FDG PET/CT was done for characterization of the lung nodule. (A) early WB FDG PET/CT showed FDG avid right lung apical density (white arrow) with maxSUV of 3.6 and a left supraclavicular brown fat FDG uptake (red arrow) with maxSUV of 8. (B) 2 hours delayed chest FDG PET/CT showed increased of the maxSUV of the lung lesion to 5.6 and left supraclavicular brown to 9.8. CT guided biopsy and pathological examination from the right apical lesion revealed metastases from breast cancer.

(B) 2 hours delayed pelvic FDG PET/CT(A) Early WB FDG PET/CT images
True Negative DTP FDG PET/CT: 56 yrs male patient with cancer rectum, post surgery and chemotherapy, CT showed perirectal soft tissue density, FDG PET/CT done to rule out recurrence. (A) Early WB FDG PET/CT fusion images showed heterogeneous FDG uptake in the perirectal soft tissue density with maxSUV of 4. (B) 2 hours delayed pelvic FDG PET/CT images showed decreased in maxSUV to be 2.3 in the perirectal soft tissue density. Biopsy showed minimal non-specific inflammation with no evidence of malignancy.

CONCULSION:
DTP 18F-FDG-PET/CT protocol is not always working.
However; promising results was noted in hepatic lesions and
presacral soft tissue lesions and to less extent in lung nodules
and lymphomatous lesions which need further studies with
large patient number to emphasize these results. Also
concluded that decrease SUV in delayed image has high NPV.


![QUANTIFICATION OF DYNAMIC [18F]FDG PET …10.1007/s11307...QUANTIFICATION OF DYNAMIC [18F]FDG PET STUDIES IN ACUTE LUNG INJURY Journal: Molecular Imaging and Biology Elisabetta Grecchi1,6,](https://img.pdfslide.us/doc/110x75/5aa9f1017f8b9a6c188d9646/quantification-of-dynamic-18ffdg-pet-101007s11307quantification-of-dynamic.jpg)






![Radiomics analysis of pre-treatment [18F]FDG PET/CT for patients … · 2018. 10. 26. · ORIGINAL ARTICLE Radiomics analysis of pre-treatment [18F]FDG PET/CT for patientswith metastatic](https://img.pdfslide.us/doc/110x75/5fcdb0e68fed49190433314d/radiomics-analysis-of-pre-treatment-18ffdg-petct-for-patients-2018-10-26.jpg)







![[18F]FDG uptake of bone marrow on PET/CT for predicting ......BLR ≥ 0.91 had a distant recurrence rate of 40.7%. Conclusions: BLR on pretreatment [18F]FDG PET/CT were significant](https://img.pdfslide.us/doc/110x75/60de3dd8893f706a1901a451/18ffdg-uptake-of-bone-marrow-on-petct-for-predicting-blr-a-091-had.jpg)
![Regional, kinetic [18F]FDG PET imaging of a unilateral Parkinsonian animal model](https://img.pdfslide.us/doc/110x75/56d6c0051a28ab3016989e06/regional-kinetic-18ffdg-pet-imaging-of-a-unilateral-parkinsonian-animal.jpg)



![Pharmacokinetic modeling of [18F]fluorodeoxyglucose (FDG](https://img.pdfslide.us/doc/110x75/61886b54df681277ae16a602/pharmacokinetic-modeling-of-18ffluorodeoxyglucose-fdg-.jpg)





