Embed Size (px)
DESCRIPTION
Dual Eligibles: The Basics. Barbara Lyons, Ph.D. Director, Kaiser Commission on Medicaid and the Uninsured Senior Vice President, Henry J. Kaiser Family Foundation For Alliance for Health Reform Washington, DC June 3, 2011. - PowerPoint PPT Presentation
Citation preview
Figure 1
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Dual Eligibles: The Basics
Barbara Lyons, Ph.D.
Director, Kaiser Commission on Medicaid and the Uninsured
Senior Vice President, Henry J. Kaiser Family Foundation
For
Alliance for Health Reform
Washington, DC
June 3, 2011
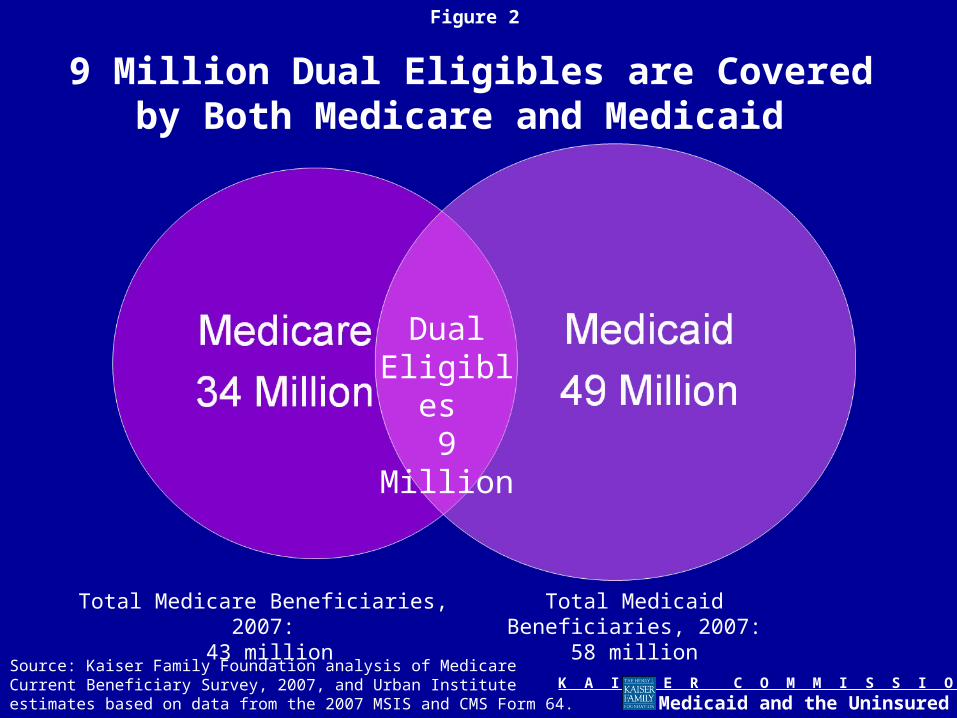
Figure 2
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
9 Million Dual Eligibles are Covered by Both Medicare and Medicaid
DualEligibles 9 Million
Total Medicare Beneficiaries, 2007: 43 million
Total Medicaid Beneficiaries, 2007:58 million
Source: Kaiser Family Foundation analysis of Medicare Current Beneficiary Survey, 2007, and Urban Institute estimates based on data from the 2007 MSIS and CMS Form 64.
Figure 3
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Medicaid Supplements Medicare for Dual Eligibles
• Nine million Medicare beneficiaries, including 5.5 million seniors and 3.4 million disabled, receive help from Medicaid
• Medicare is a national program that provides coverage of medical services, including hospital, physician, prescription drugs, and limited post-acute care, but requires premium payments and cost-sharing (ie, hospital deductible $1,132 annually; Part B premium $115/month in 2011)
• Medicaid is a joint federal-state program that supplements Medicare for low-income beneficiaries– Provides financial assistance with Medicare premiums and deductibles
and co-insurance for Medicare-covered services– Medicaid helps pay for services not covered by Medicare, such as
hearing, vision and long-term care
Figure 4
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
How Do Dual Eligibles Qualify for Medicaid?
• For the poor: States are generally required to cover individuals qualifying for SSI (income below 75% of poverty and $2,000 or less in assets for an individual); states have the option to cover individuals up to 100% of poverty
• For those with high medical or long-term care expenses, special eligibility and level of need rules apply- 38 states allow individuals who need nursing home care to qualify up to 300%
of the SSI level ($2,022 per month for an individual), but require them to contribute most of their income to the cost;
- 26 states have a medically needy program enabling individuals to spend-down; - Eligibility for home and community-based care is typically linked to nursing
home standards
• Most dual eligibles qualify for full Medicaid benefits, while some qualify for more limited Medicaid assistance to help with Medicare premiums and cost sharing through Medicare Savings Programs
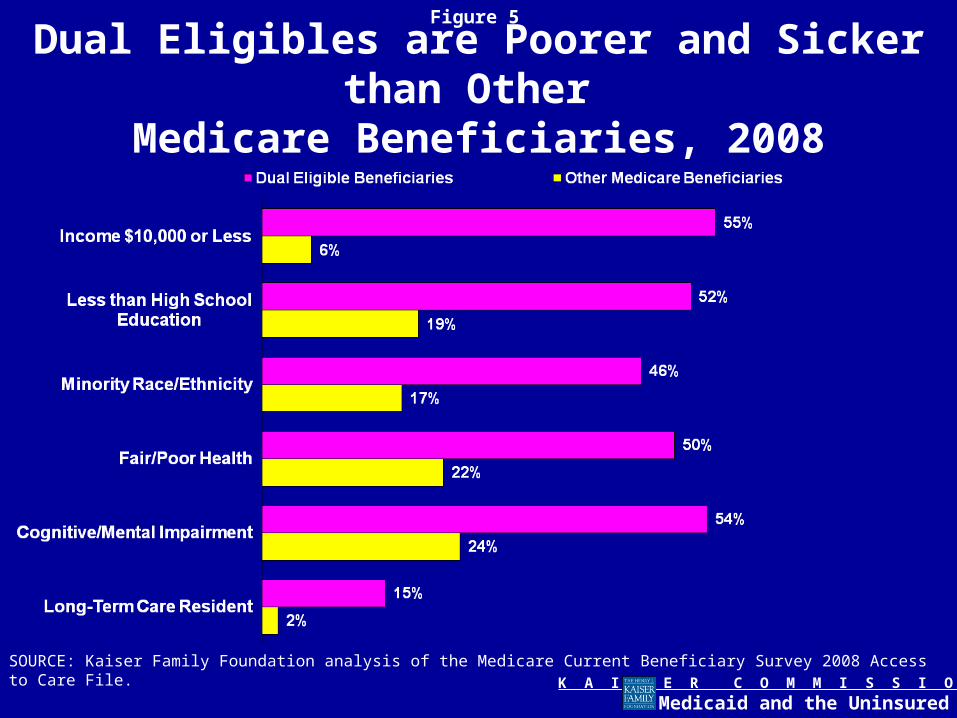
Figure 5
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Dual Eligibles are Poorer and Sicker than Other Medicare Beneficiaries, 2008
SOURCE: Kaiser Family Foundation analysis of the Medicare Current Beneficiary Survey 2008 Access to Care File.
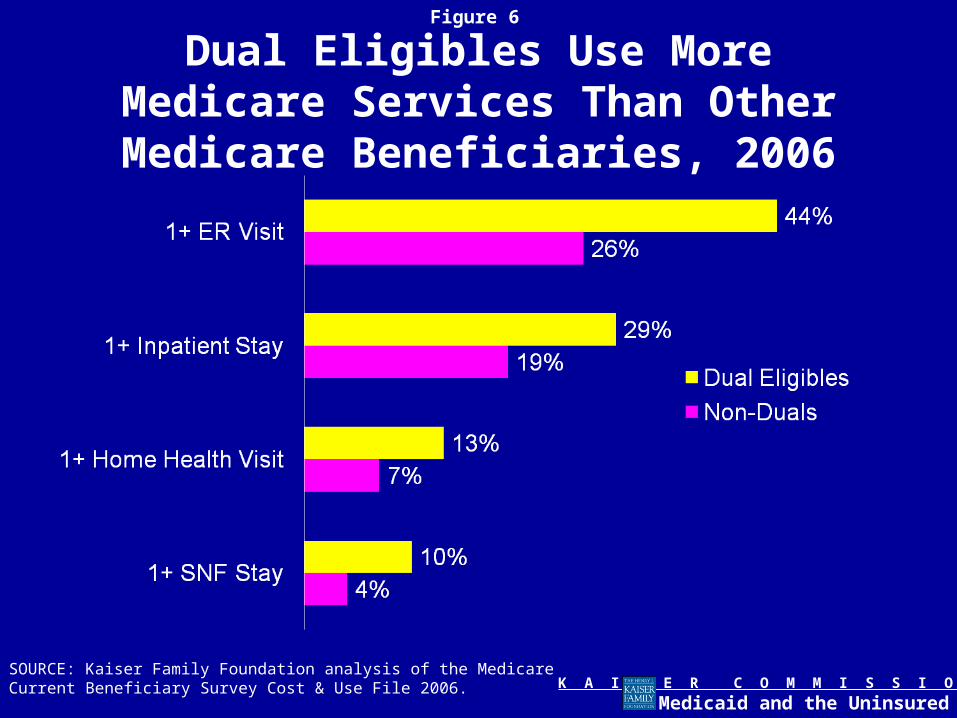
Figure 6
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Dual Eligibles Use More Medicare Services Than Other Medicare
Beneficiaries, 2006
SOURCE: Kaiser Family Foundation analysis of the Medicare Current Beneficiary Survey Cost & Use File 2006.
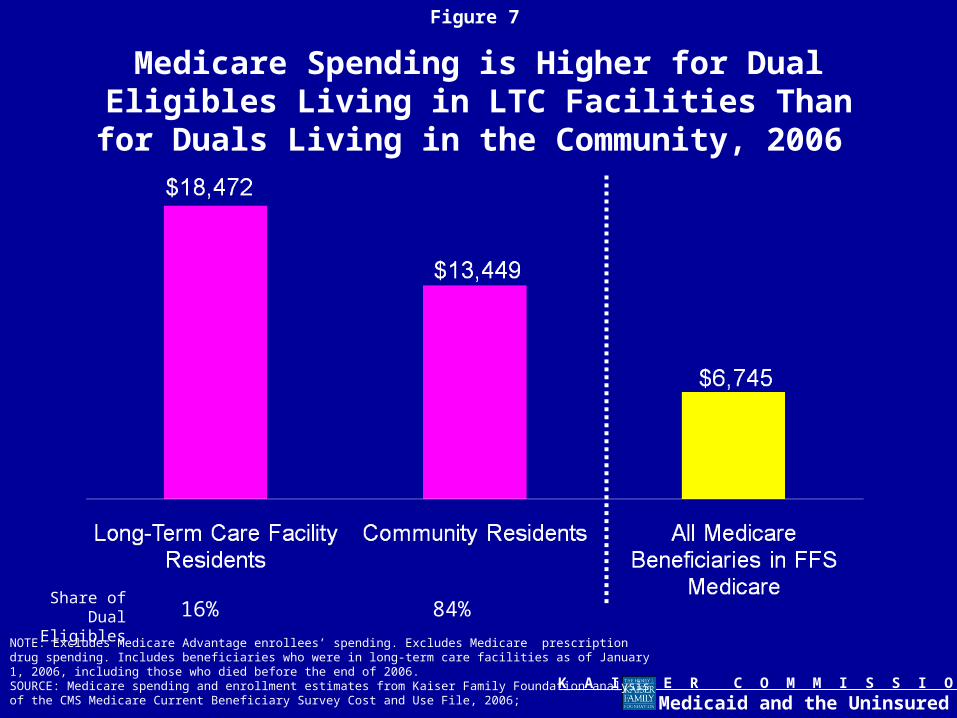
Figure 7
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Medicare Spending is Higher for Dual Eligibles Living in LTC Facilities Than for Duals Living in the
Community, 2006
NOTE: Excludes Medicare Advantage enrollees’ spending. Excludes Medicare prescription drug spending. Includes beneficiaries who were in long-term care facilities as of January 1, 2006, including those who died before the end of 2006.SOURCE: Medicare spending and enrollment estimates from Kaiser Family Foundation analysis of the CMS Medicare Current Beneficiary Survey Cost and Use File, 2006;
Share of Dual Eligibles 16% 84%
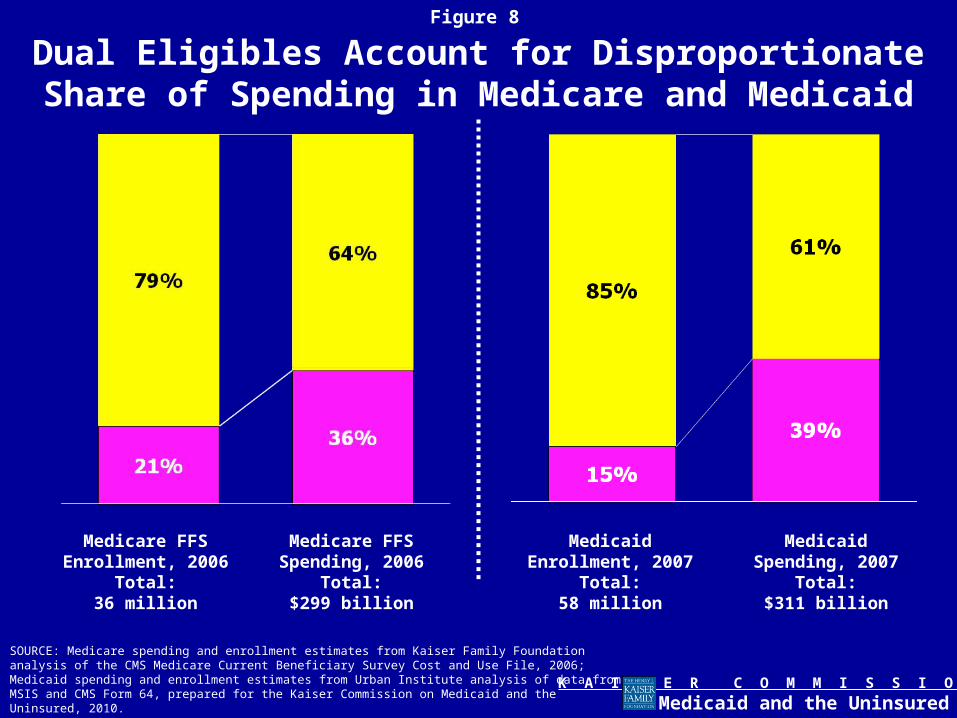
Figure 8
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Dual Eligibles Account for Disproportionate Share of Spending in Medicare and Medicaid
SOURCE: Medicare spending and enrollment estimates from Kaiser Family Foundation analysis of the CMS Medicare Current Beneficiary Survey Cost and Use File, 2006; Medicaid spending and enrollment estimates from Urban Institute analysis of data from MSIS and CMS Form 64, prepared for the Kaiser Commission on Medicaid and the Uninsured, 2010.
Medicare FFS Enrollment, 2006
Total:36 million
Medicare FFS Spending, 2006
Total:$299 billion
Medicaid Enrollment, 2007
Total:58 million
Medicaid Spending, 2007
Total:$311 billion
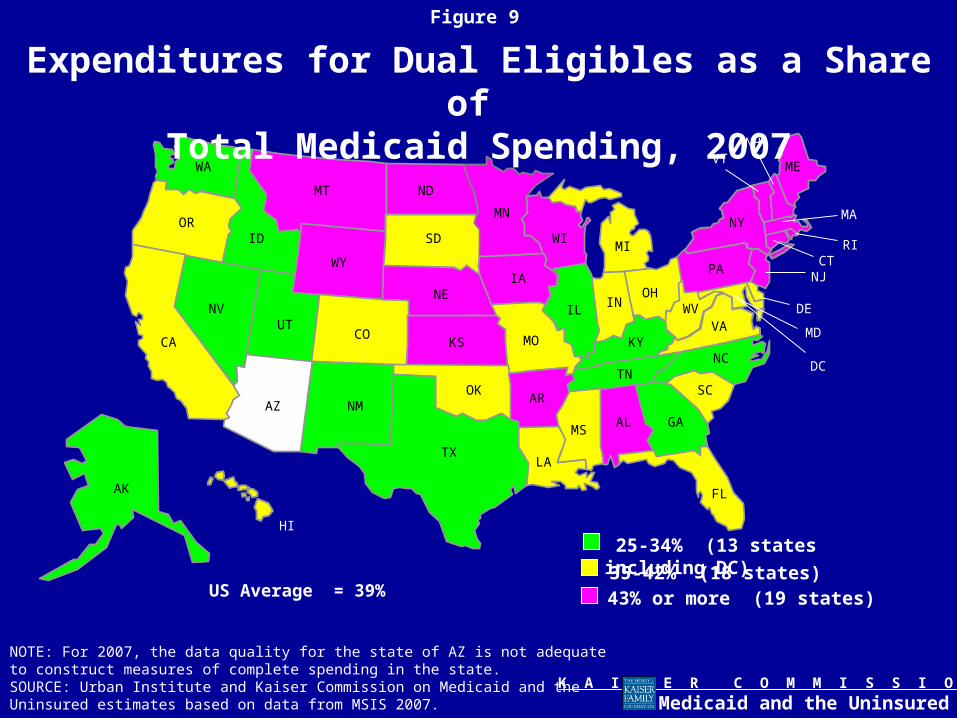
Figure 9
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
AZAR
MS
LA
WA
MN
ND
WY
ID
UTCO
OR
NV
CA
MT
IA
WIMI
NE
SD
ME
MOKS
OHIN
NY
IL
KY
TNNC
NH
MA
VT
PA
VAWV
CTNJ
DE
MD
RI
HI
DC
AK
SCNM
OK
GA
TX
IL
FL
AL
25-34% (13 states including DC)
35-42% (18 states)43% or more (19 states)
Expenditures for Dual Eligibles as a Share of Total Medicaid Spending, 2007
US Average = 39%
NOTE: For 2007, the data quality for the state of AZ is not adequate to construct measures of complete spending in the state. SOURCE: Urban Institute and Kaiser Commission on Medicaid and the Uninsured estimates based on data from MSIS 2007.
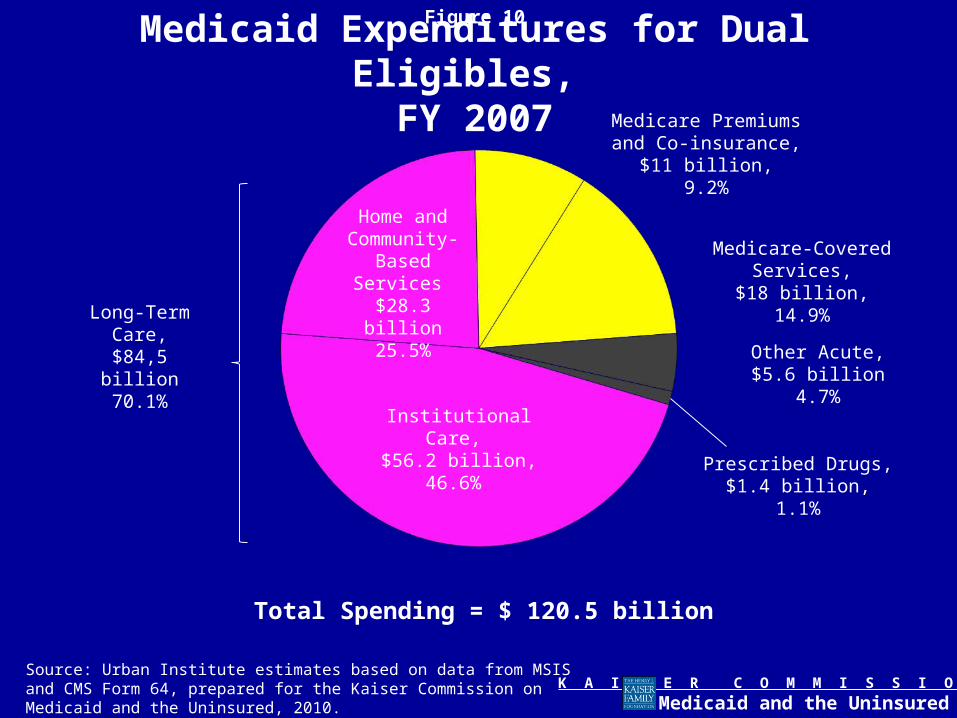
Figure 10
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Medicaid Expenditures for Dual Eligibles, FY 2007
Total Spending = $ 120.5 billion
Institutional Care, $56.2 billion,
46.6%
Home and Community-
Based Services $28.3 billion
25.5%
Medicare Premiums and Co-insurance,
$11 billion,9.2%
Medicare-Covered Services,$18 billion,
14.9%
Other Acute,$5.6 billion
4.7%
Prescribed Drugs,$1.4 billion,
1.1%
Long-Term Care,
$84,5 billion70.1%
Source: Urban Institute estimates based on data from MSIS and CMS Form 64, prepared for the Kaiser Commission on Medicaid and the Uninsured, 2010.

Figure 11
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
AZAR
MS
LA
WA
MN
ND
WY
ID
UTCO
OR
NV
CA
MT
IA
WIMI
NE
SD
ME
MOKS
OHIN
NY
IL
KY
TNNC
NH
MA
VT
PA
VAWV
CTNJ
DE
MD
RI
HI
DC
AK
SCNM
OK
GA
TX
IL
FL
AL
25% or more (10 states including DC)
11-18% (16 states)11-24% (10 states)
Home and Community Based Services as a Share of Total Medicaid LTC Spending on Elderly Duals, 2007
US Average = 23%
NOTE: For 2007, the data quality for the state of AZ is not adequate to construct measures of complete spending in the state. SOURCE: Urban Institute and Kaiser Commission on Medicaid and the Uninsured estimates based on data from MSIS 2007.
5-10% (13 states)
Figure 12
K A I S E R C O M M I S S I O N O N
Medicaid and the Uninsured
Looking Ahead• Medicaid is an important adjunct to Medicare for many low-income Medicare
beneficiaries providing financial protections and a fuller complement of medical and long-term care services.
• Because of their poorer health status and greater health needs, dual eligibles are an expensive population for both the Medicare and Medicaid programs.
• Fragmentation and lack of coordination between Medicare and Medicaid can be challenging for dual eligibles, their families, and providers and result in inefficient care.
• Federal and state budget pressures could impact Medicare and Medicaid’s role for dual eligibles.
• The ACA provides new opportunities to coordinate care delivery for dual eligibles through the Duals Office and Innovation Center and to promote community-based care for dual eligibles, but requires assuring beneficiary safeguards and accountability.





























