Embed Size (px)
Citation preview

LETTERS TO THE EDITOR
Drugs in liver disease To the Editor:
This letter is to augment your editorial describing the con- sensus achieved at the recent British Pharmacological Soci- ety meeting at Chester on the topic of regulatory requirements for drug development with respect to the use of a new drug in patients who have underlying liver disease. The objective of this letter is to provide a plea from one of the symposium participants to resurrect the concept of quantitative evalua- tion of hepatic function and suggest its application to drug development.
At the time of introduction of new drugs to the market place, regulatory authorities quite reasonably request drug company sponsors to provide written recommendations within the product label to advise the prescribing physician how to use the new drug in special patient populations. Liver disease is not common in the general population and is rarely the target for new drug development. However, patients who are targets for a new therapy may well have concomitant liver disease, so it is appropriate to routinely question whether the presence of the hepatic disease should provide justification for additional caution or dosage modification. This caution is particularly relevant for situations in which the dynamic response to the drug might be influenced in the presence of liver disease (eg, psychotropic drugs, diuretics, angiotensin- converting enzyme inhibitors, and angiotensin II receptor blockers), as well as when the liver contributes to the metab- olism and disposition of the drug. Thus a routine aspect of drug development incorporates an element of “what about liver disease?”
In considering the issue of “what about liver disease” from the perspective of drug development, 3 situations may be readily identified. The first is that the drug is being developed for use in patients with liver disease, in which case the pri- mary end point measures will be dynamic response and stud- ies in substantial numbers of patients with liver disease can be anticipated. At the opposite extreme are drugs that will rarely be given to patients with liver disease and whose dis- position is not influenced by the liver under normal condi- tions. It would seem to be reasonable to provide a disclaimer in the product label and not study the drug in patients with liver disease. The third and largest group is drugs that will only rarely be given to patients with liver disease but for which hepatic dysfunction can be expected to alter disposi- tion. It is this group for which current study design is often less than optimal.
Inherent problems in study design relate to the tensions of wanting to minimize sample size and study complexity for economic reasons, and the practical and ethical difficulty of studying patients with advanced liver disease with their atten-
462
dant potential complications. Compounding these difficulties is the complexity of the underlying disease process. It is well recognized that not only may different diseases have differ- ent effects on drug disposition but individual diseases can be expressed differently with respect to the extent of hepatocyte damage, new cell regeneration, biliary obstruction, and fibrous tissue formation. Furthermore, there may be difficulty in assessing the extent of hepatic dysfunction in an individ- ual patient for any given disease.
In renal disease, a pragmatic and useful concept has been the application of the intact nephron hypothesis. Despite the complexity and multiplicity of involved mechanisms, it is appreciated that the intact nephron acts as an integrated unit. A loss of the number of nephron units results in a propor- tional loss of any function related to this unit. Thus a reduc- tion in glomerular filtration rate results in a proportional reduction in renal clearance of a drug handled by renal tubule anionic secretion. This useful working model raises the question of whether there is a working analog model in liver disease.
Consideration of independent variables that contribute to hepatic clearance indicates that intrinsic hepatic clearance and liver blood flow are independent variables.‘,* The observed hepatic clearance of high intrinsic clearance drugs is limited by liver blood flow. In contrast, low intrinsic clearance drugs have hepatic clearance that is independent of flow. There are now a number of observations of close associations between high intrinsic clearance drugs, such as propranolol, galactose, lidocaine, and indocyanine green, with low intrinsic clear- ance drugs, such as antipyrine (INN, phenazone), that are con- sistent with an intact hepatocyte hypothesis.s,4 This hypothe- sis, which is supported by observations in animal models,5 states that chronic liver disease is associated with a reduced number of hepatocytes that function normally and are nor- mally perfused, as well as with the development of an intra- hepatic portosystemic shunt.
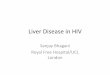
If valid, the analogous models of an intact nephron and intact hepatocyte model would permit the prediction of clear- ance in an individual patient with known renal and hepatic function (Figure 1). In the schematic illustrated, knowledge of the relative contribution of renal and hepatic clearances under normal circumstances to total clearance is prerequi- site. In the instance of a renally handled drug (drug A), clear- ance of drug in an individual patient would be a function of residual renal function in that patient and independent of hepatic function. In the instance of a hepatically handled drug (drug C), clearance would be a function of residual hepatic function and independent of renal function. In the example of a drug with both renal and hepatic clearance, clearance would be predictably modified by changes in renal and hepatic function.

<:I.INICAL PHAiWlACOLOGY s- THERAPEUTIC’S VOLUME 64. NCMKER 4 Letten to the Editor 463
Prediction of Modification of Drug Clearance by Renal and Hepatic Disease for Individual Patients
Rarnaining renal function (% normal)
‘- E 100 A /f
tj c 0 E ,5 7” #’
3 0 /’ 5 500 I
ki 2 ,A 0 ,’
5 / / 5 ,’ t- /
0 50 100
Remaining liver function (% normal)
Figure 1. Schematic representation of the changes in observed clearance to be expected with changes in renal function (left panel) or changes in hepatic function (right panel) with drugs that have renally determined elimination (drug A), renally and hepatically determined elimination (drug B), and hepat- ically determined elimination (drug C) in subjects with normal renal and hepatic function.
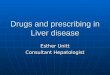
Differential Effect of Liver Disease on Individual Routes of Oxidative Metabolism
Percentage reduction in clearance in comparison
to same control group
0
25 ,
5o -
_-
28
Figure 2. The mean percentage change in clearance from the mean clearance of a control group (n = 6) for S-mephenytoin, dapsone, and debrisoquin (INN, debrisoquine) in the same group of patients with chronic liver disease (n = 6).
There is voluminous literature on drug disposition in liver disease that has been reviewed previously.6.7 Despite the observations that many drugs have impaired clearance in liver disease, the extent of impairment has infrequently been ade- quately described as the severity of the liver disease is rarely presented, and the validity of the intact hepatocyte hypothe- sis has been questioned.
The concept of the intact hepatocyte hypothesis was ques- tioned in early studies that compared drugs whose primary routes of elimination were by conjugation to a glucuronide in comparison to oxidation. One such example is a study in a
cohort of patients with chronic liver disease who had reduced clearance of antipyrine but normal clearances of 1orazepam.s Similar observations have been obtained with morphine in patients with compensated liver disease.9 However, a subse- quent study undertaken in patients with severe decompen- sated cirrhosis with hepatic encephalopathy showed reduced clearance of morphine.‘” A similar profile has been made with oxazepam.” Thus there appears to be a relative selective preservation of glucuronidation. More recently, the experi- mental paradigm of investigating multiple routes of metabo- lism in the same cohort has been extended to explore the rel-

464 Letters to the Editor CLINICAL PHARMA COLOGY & THERAPEUTICS
OCTOBER 1998
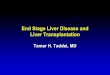
The Influence of Liver Disease On 100%
Drug Clearance
Hepatic Function
Figure 3. Schematic illustration of variations of drug clearance with deterioration in hepatic func- tion for drugs that undergo extensive metabolism. The example illustrated by a linear decrease indi- cates a major reduction in function before the development of clinical complications of chronic liver disease, and there is combined liver and renal dysfunction with further progression of disease. Some drugs are projected to have relative sparing of function until late in the disease. Other drugs are projected to have clearances that are sensitive to the presence of liver disease.
ative selectivity of chronic liver disease on oxidative drug metabolism undertaken by different cytochrome P450 enzymes (CYP). One study has used an approach to simulta- neously evaluate the activity of CYP2C19, CYP2D6, and pre- dominantly CYP3A4, with use of the probe drugs S-mepheny- toin, debrisoquin (INN, debrisoquine), and dapsone, respec- tively (Figure 2).12Js In the same cohort of patients with mild to moderate chronic liver disease, a previous observation that CYP2C19 was exquisitely sensitive to the presence of liver disease14 was confirmed. Dapsone N-hydroxylation was mod- estly but significantly reduced, whereas debrisoquin hydrox- ylation was unchanged. These data clearly indicate a selec- tive regulation of activity for different CYP enzymes in the presence of chronic liver disease, even though the mecha- nism(s) responsible for this differential effect remains unknown.
It therefore appears that for drugs that undergo hepatic metabolism, there are a range of sensitivities in modification of drug clearance in the presence of chronic liver disease; these are schematically presented in Figure 3. This range of variation makes it imperative to evaluate a new chemical entity in the context of (1) the full range of severity of liver disease and (2) comparison to a known entity. Based on con- siderations such as these, it therefore makes prudent sense to recommend that when pharmacokinetic studies are under- taken in patients with liver disease during the development of a new drug, a minimum requirement should be to include
a subset of patients with severe forms of liver disease. Fur- thermore, characterization of the status of hepatic function would benefit by being quantified on the basis of an indepen- dent measure of metabolism of a drug known to be influenced by liver disease in addition to clinical assessment, which has usually been semiquantitated as a Pugh score. This recom- mendation, although rational, has to be implemented with caution. The practical and ethical problems associated with giving investigational drugs that have no potential to confer benefit to patients with severe liver disease merits further dis- cussion in an open forum. This opportunity could be provided under the auspices of either this Journal or of the American Society for Clinical Pharmacology and Therapeutics.
In the future, it may be possible to predict the impact of chronic liver disease on the basis of knowledge of the major determinants of the disposition of a drug in healthy subjects, which may relate more to the enzymes involved in the metab- olism of the drug than the structure of the metabolite. How- ever, the state of knowledge is not yet sufficiently advanced to have confidence in this approach. Proof of predicted prin- ciple is still a prerequisite for smooth drug review, and appre- ciation of the need for functional characterization of the effect of the liver disease in each study subject deserves merit.
Robert A. Branch, MD Center for Clinical Pharmacology
University of Pittsburgh School of Medicine Pittsburgh, Pa

CLINICAL PHARMACOLOGY & THERAPEUTICS VOLUME 64, NUMRER 4 Letters to the Editor 465
References
I.
2.
3.
4.
5.
6.
7.
8.
9.
IO.
11
12
13
Wilkinson GR, Shaud DG. A physiological approach to hepatic drug clearance. Clin Pharmacol Ther 1975:18:377-90. Wilkinson GR, Wood AJJ, Branch RA, Shand DG. Intrinsic hepatic clearance in cirrhosis. Gastroenterology 1978;75:347-8. Shand DG, Branch RA, Wood AJJ, Villeneuve JP Drug metabolism in experimental cirrhosis: the intact hepatocyte theory. In: Preisig R, Birscher J, editors. The liver: quantitative aspects of structure and function. Proceedings of the Third International Gstaad Sym- posium. Aulendorf, Germany: Editio Cantor. 1978. p. 346-50. Wilkinson GR, Wood AJJ, Branch RA, Shand DG. Intrinsic hepatic clearance in cirrhosis. Gastroenterology 1978;75:347-8. Wood AJJ, Villeneuve JP, Branch RA, Rogers LW, Shand DG. Intact hepatocyte theory of impaired drug metabolism in experi- mental cirrhosis in the rat. Gastroenterology 1979;76: 1358-62. Kubisty CA, Arns PA. Wedlund PJ, Branch RA. Pharmacother- apy in liver failure. In: Chernow B, editor. Pocket book of criti- cal care pharmacotherapy. Baltimore: Williams and Wilkins; 1995. p. 91-138. Adedoyin A, Branch RA. Pharmacokinetics. In: Zakim D, Boyer TD, editors. Hepatology: a textbook of liver disease; vol 1. 3rd ed. Philadelphia: WB Saunders; 1996. p. 307-17. Kraus JW, Desmond PV, Marshall JP, Johnson RF, Schenker S, Wilkinson GR. Effects of aging and liver disease on disposition of lorazepam. Clin Pharmacol Ther 1978;24:41 l-9. Patwardhan RV, Johnson RF, Hoyumpa A, Sheehan JJ, Desmond PV, Wilkinson GR, et al. Normal metabolism of morphine in cir- rhosis. Gastroenterology 1981;81:1006-1 I. Hasselstrom J, Eriksson, S, Persson A, Rane A, Svensson JO, Sawe J. The metabolism and bioavailability of morphine in patients with severe liver cirrhosis. Br J Clin Pharmacol 1990; 29:289-97. Sonne J, Andreasen PB, Loft S, Dossing M, Andreasen F. Glu- curonidation of oxazepam is not spared in patients with hepatic encephalopathy. Hepatology 1990; II:95 1-6. May G, Ams PA, Richards WO, Porter J, Ryder D, Fleming CM, et al. The disposition of dapsone in cirrhosis. Clin Pharmacol Ther 1992;51:689-700. Adedoyin A, Arns PA, Richard WO, Wilkinson GR, Branch RA. Selective effect of liver disease on the activities of specific metabolizing enzymes: investigation of cytochromes P450 2Cl9 and 2D6. Clin Pharmacol Ther 1998;64:8- 17.
14. Arns P, Adedoyin A, DiBisceglie A, Waggoner J, Hoofnagle J, Wilkinson C. et al. Mephenytoin disposition and serum bile acids as indices of hepatic function in chronic viral hepatitis. Clin Pharmacol Ther 1997;62:527-37.
13/8/94004
should be enrolled in a study in which they receive an inter- vention from which they can derive no personal benefit is open to question. An alternative approach would be to measure drug
levels and clinical assessments when the drug is given to such patients for therapeutic purposes during “phase IV” shortly after marketing. This would require a consortium of institu- tions organized to do such phase IV special population stud- ies. (Such a consortium is one of the parts of the CERT pro- posal by Dr Woos1ey.t) It would also require the acceptance of the idea that much important information about drug effects in humans can best be learned after marketing when large het- erogeneous populations receive the drug.
Information about a drug is acquired incrementally. Our current practice suggests we think that a drug is risky and experimental, requiring institutional review and signed informed consent forms until the day it is approved for mar- keting. After that day, it is considered to be safe and effective. Yet it, the drug, does not change. As more is learned about drug effects during the premarketing period, the drug’s actions and dose-response relationships become more predictable. It is the predictability of a drug’s effects that is key. When the effects are predictable enough, approval for marketing is given. How much predictability is enough becomes the question. The idea that a drug is safe and effective upon registration exag- gerates the predictability of the responses in the general pop- ulation. Society must recognize that there are some special populations and some kinds of questions (eg, the effects of large overdose such as that which occurs in self or accidental poisoning) that cannot be studied before marketing. A proper program for addressing these issues after marketing with overt acceptance of the lack of this information before registration would improve therapeutics and align our concept of drug development with the realities of science.
Marcus M. Reidenberg, MD Division of Clinicul Pharmaco1og.y Cornell University Medical College
New York, NY
Reference I. Woosley RL. Centers for education and research in therapeutics.
Clin Pharmacol Ther 1994;56:693-7.
13/8/94068
Comment
Dr Branch’s suggestion, that a requirement for registration for drugs undergoing hepatic metabolism include at least a single-dose phatmacokinetic study in a group of patients with
severe forms of liver disease, may be very hard to implement. Severe forms of liver disease are often associated with encephalopathy. Whether patients with encephalopathy can really give informed consent for a drug study and whether they
Caffeine in tension headache
To the Editor: An article titled “Caffeine as an analgesic adjuvant in ten-
sion headache” was published in the November 1994 issue of Clinical Pharmacology & Therapeutics (Migliardi JR, Armellino JJ, Friedman M, Gilllings DB, Beaver WT. Caf- feine as an analgesic adjuvant in tension headache. Clin Pharmacol Ther 1994;56:576-86). Unfortunately, Dr Sey-