Embed Size (px)
Citation preview
EmergencyDRUGS
Epinephrine
• Indication
▫ VF, pulseless VT, PEA, or asystole
1 mg I.V push every 3-5 min
Intermediate dosing: 2-5 mg IV push over 3-5 min
Escalating dosing: 1mg, 3mg, 5 mg IV push 3 min apart
High dosing: ,1 mg/kg IV push every 3 – 5 min
Symptomatic Bradycardia: continous infusion at 2-10 mcg/min
Nsg. consideration
• Each dose is followed by 20 mL iv fluid flush.
• Can be given via ET tube 2-2.5 x the IV dose, followed with 10 mL Flush PNSS
• IC when no other route is available
• It increases systemic vascular resistance, BP, Cardiac elec. Activity, strenth of contraction, automaticity, and myocardial O2 requirement
Lidocaine
Indication
• VF or Pulseless VT: Initially 1-1.5 mg/kg IV push: every 3-5 mins, max of 3mg/kg
• Stable VT or Stable wide-complex tachycardia: repeat doses are half the original dose.
• If lidocaine succesfully converts the VF/VT: begin continous infusion at 2-4 mg/min
Nsg consideration
• Toxicity( Slurred speech, altertered LOC, Muscle twitching, and seizures), stop the drug/reduce dose
• Via ET: 2-2.5 times the iv dose, flush with 10 ml PNSS
• Don’t give if PVC occurs with bradycardia or escape rhythm.
• No longer recommended for VT/VF prophylaxis in acute MI
Atropine
• Symptomatic Bradycardia
▫ .5-1 mg iv push q 3-5 min, not to exceed .04 mg/kg
• Asystole/PEA
▫ 1 mg iv push q 3-5 min, not to exceed a total dose of .04mg/kg
Nsg consideration
• Don’t give less than .5 mg dose – may further slow heart rate
• Via ET: dilute 1-2 mg in 10 mL sterile water of PNSS, flush with 10 mL PNSS
Adenosine
• PSVT or wide-complex tachycardia:
▫ Initially 6 mg rapid iv push; if no response in 1-2 min, give 12 mg iv push; may be followed by a third 12 mg dose given in 1-2 min.
Nsg consideration
• Given rapidly over 1-3 sec ( half life is 5 sec)
• Follow dose with a 20 ml PNSS flush
• If methylxanthines, dipyridamole and carbamazepine are present higher dose may be needed
• A brief period of Asystole is common after administration
Bretylium
• VF/ of pulseless VT unresponsive to defibrilation, epi and lido
▫ 5mg/kg iv push; is arhythmia persists, increase to 10 mg/kg q 5-10 min, to a max dose of 35 mg/kg
• Stable VT or Stable wide-complex tachycardia:
▫ 5-10 mg/kg over 8-10 min, to max 35 mg/kg over 24 hrs, if loading dose converts arhythmia start infusion of 2 mg/min.
Dobutamine
• Heart Failure
▫ 2-20 mcg/kg/min
Nsg considerations
• May cause tachycardia and other arhythmias, BP fluctuations, nausea and hypokalemia
• Monitor heart closely; increases in heart heartrate more than 10% may induce or exacernateMyocardial Ischemia
Dopamine
• Hypotension c symptomatic bradycardia, heart failure or after spontaneous return of circulation
▫ Initially, 1-5 mcg/kg/min; max is 20 mcg/kg/min
Enhances renal blood flow – 1-2 mcg/kg/min
Nsg consideration
• May induce tachycardia, - dose reduction/withdrawal
• Extravasation may cause severe tissue sloughing and necrosis
• Norepinephrine should be added is more than max dose is needed to maintain BP
• Use slowest infusion first• Can exacerbate pulmonary congestion and
compromise cardiac output• Eliminate hypovolemia as a cause of hypotension
before treating
Magnesium
• VF/VT with hypomagnesemia
▫ 1-2 grams diluted in 10 mL D5W given IV push over 1-2 min
• Torsades de pointes: 5-10 grams iv
• Acute MI with hypomagnesemia
▫ Intermitent of continous infusions
Nsg consideration
• Flushing, sweating, mild bradycardia, and hypotension may develop from rapid administration in non arrest situations
Procainamide
• PVCs or recurrent VT with pulse
▫ Initially, 20 mg/min until
Hypotension occurs
QRS complex
PR interval
QT interval is widened by 50 %
Total of 17mg/kg of the drug was administered
▫ Maintenance infusion 1-4 mg/min
Nsg consideration
• Monitor BP closely during administration; may cause precipitous hypotension, infuse cautiously in patients with acute MI
• Contraindicated in patients with preexisting long QT intervals and torsades de pointes
• Torsades de pointes, or simply torsades is a French term that literally means "twisting of the points". It was first described by Dessertenne in 1966[1] and refers to a specific, rare variety of ventricular tachycardia that exhibits distinct characteristics on the electrocardiogram (ECG).
• CharacteristicsRotation of the heart's electrical axis by at least 180ºProlonged QT interval (LQTS)Preceded by long and short RR-intervalsTriggered by an early premature ventricular contraction (R-on-T PVC)
ToxicologyPoisoning
Occurrence of Poisoning
• Unintentional
• Intentional
Most common poisons
• Unintentional
• Intentional
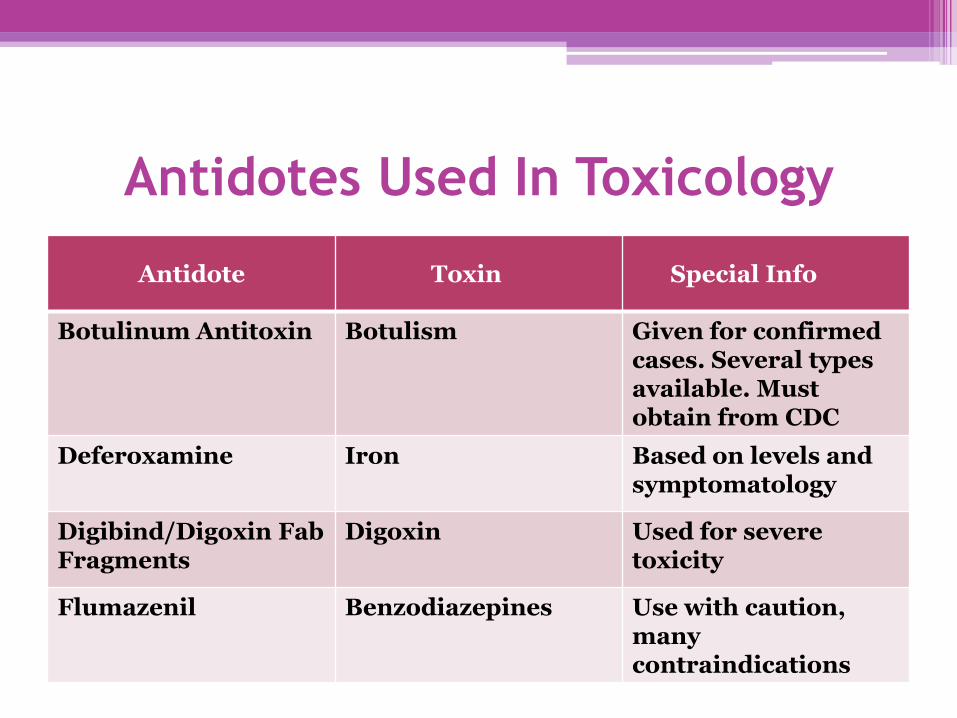
Antidotes Used In Toxicology
Antidote Toxin Special Info
Botulinum Antitoxin Botulism Given for confirmed cases. Several types available. Must obtain from CDC
Deferoxamine Iron Based on levels and symptomatology
Digibind/Digoxin Fab Fragments
Digoxin Used for severe toxicity
Flumazenil Benzodiazepines Use with caution, many contraindications
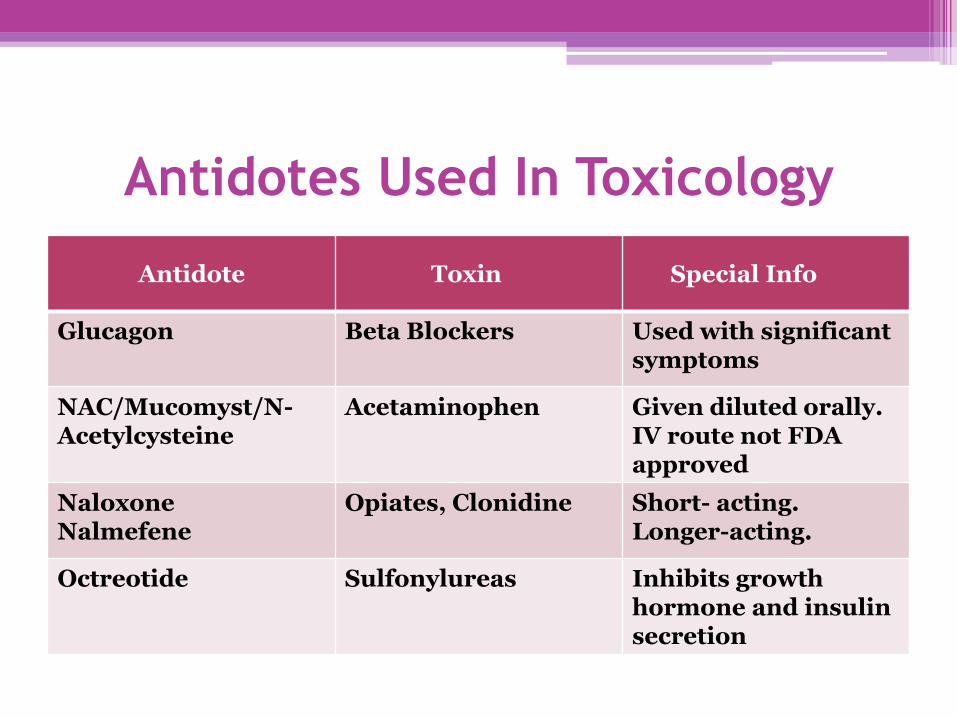
Antidotes Used In Toxicology
Antidote Toxin Special Info
Glucagon Beta Blockers Used with significant symptoms
NAC/Mucomyst/N-Acetylcysteine
Acetaminophen Given diluted orally. IV route not FDA approved
Naloxone Nalmefene
Opiates, Clonidine Short- acting. Longer-acting.
Octreotide Sulfonylureas Inhibits growth hormone and insulin secretion
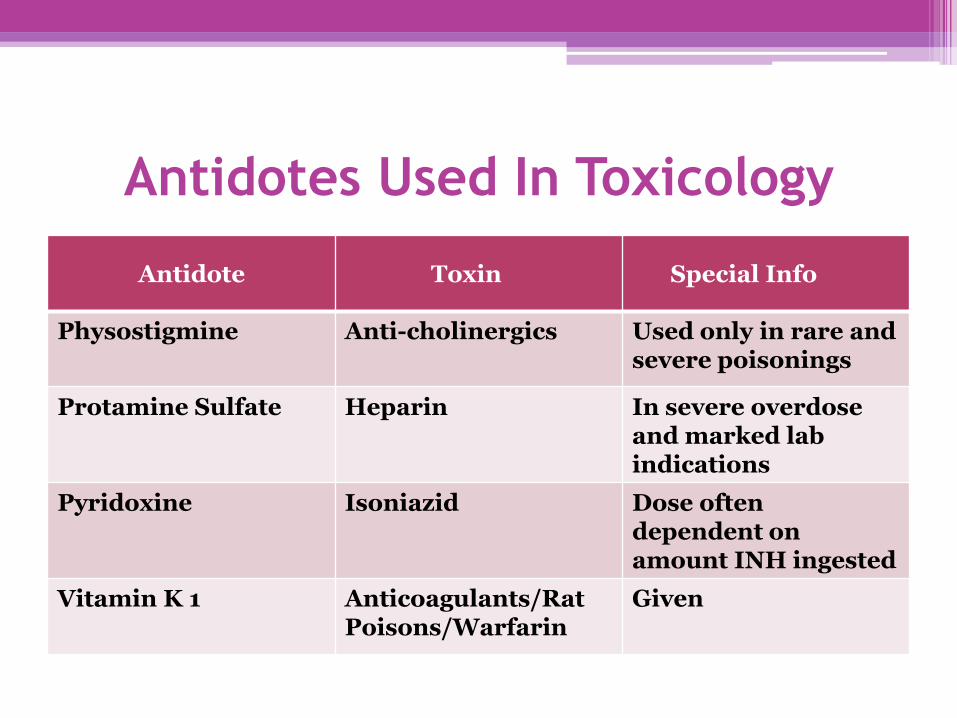
Antidotes Used In Toxicology
Antidote Toxin Special Info
Physostigmine Anti-cholinergics Used only in rare and severe poisonings
Protamine Sulfate Heparin In severe overdose and marked lab indications
Pyridoxine Isoniazid Dose often dependent on amount INH ingested
Vitamin K 1 Anticoagulants/Rat Poisons/Warfarin
Given
EmergencyDRUGS