Embed Size (px)
Citation preview
Drug Use, Prisons and Compulsory Drug Treatment
Centers
Sonia Bezziccheri, UNODC Regional Centre for East Asia and the PacificThai Satellite Meeting
19 April, 2009
2
Background
• In Thailand, drug offences account for the majority of people in prison
• An exponential increase in methamphetamine availability and use in the last ten years has placed further pressure on Thailand’s prison system
• In 2005, 65% of people in Thai prisons were on drugs related charges
• In 2006, 75% of the 68,000 drug-related arrests were methamphetamine related
3
Prisons are overcrowded
The large numbers of drug users in prison has led to severe overcrowding
The National Rehabilitation Act was established in 2002 to divert drug users from prison
Drug users considered “patients, not criminals”
4
Treatment Centers
Drug users increasingly sent to compulsory drug treatment centers (CDTC) “boot-camps” – there are currently 84 CDTCs in Thailand
75% of these centers are managed by the military or police
5
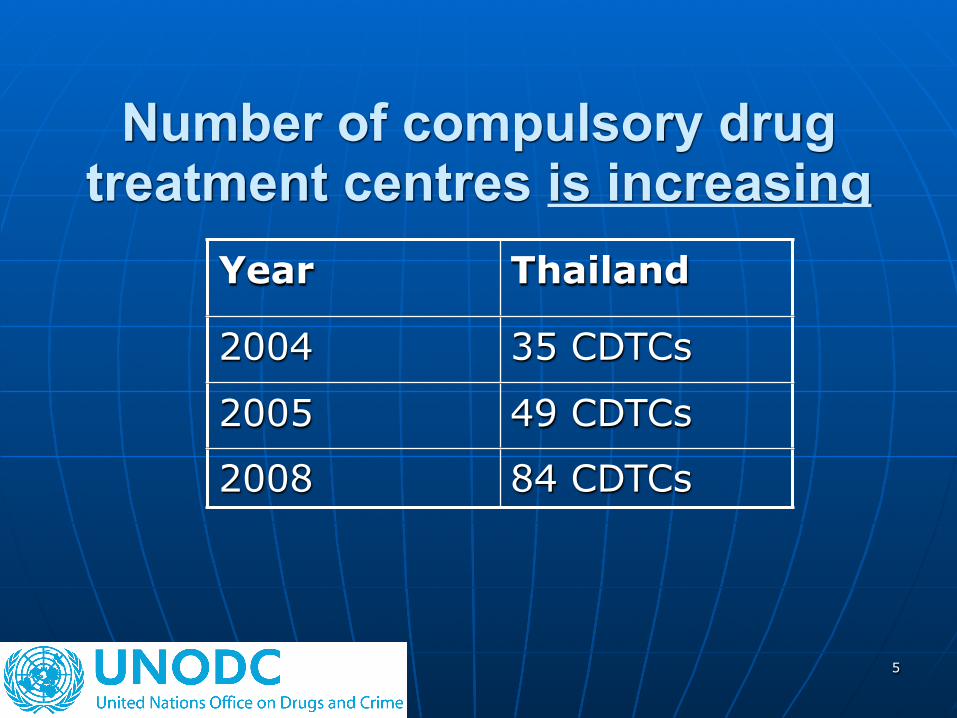
Number of compulsory drug treatment centres is increasing
Year Thailand
2004 35 CDTCs
2005 49 CDTCs
2008 84 CDTCs
6
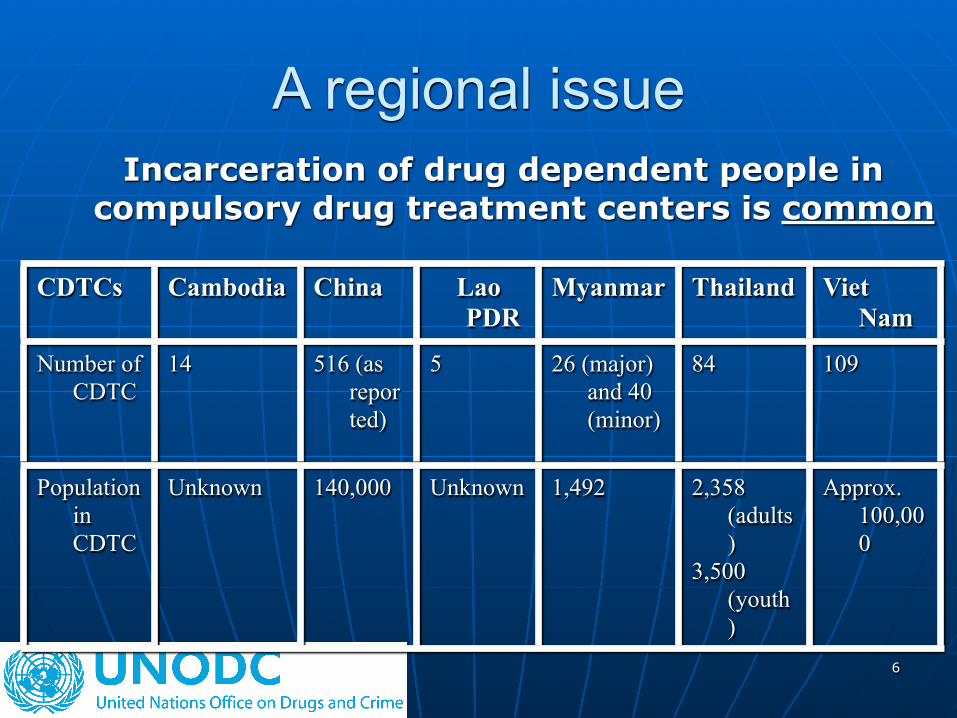
A regional issue Incarceration of drug dependent people in
compulsory drug treatment centers is common
CDTCs Cambodia China Lao PDR
Myanmar Thailand Viet Nam
Number of CDTC
14 516 (as reported)
5 26 (major) and 40 (minor)
84 109
Population in CDTC
Unknown 140,000 Unknown 1,492 2,358 (adults)
3,500 (youth)
Approx. 100,000
7
Implications for individual and public health
A history of incarceration has been associated with several negative health outcomes:
STIs including syphilis, herpes and HIV Mental health issues, skin infections TB Hepatitis B and C AIDS and TB are reportedly the major
cause of death
8
Why?
Risk behaviours in prisons and CDTCs are prevalent:
Unprotected sex Tattooing Injecting drug use Penile modification “Fung Muk”
9
The Facts
- Overcrowding - Limited availability of condoms- No availability of sterile needles/
syringes which leads to frequent sharing of equipment
- Under staffed and unqualified staff - Modest budget for HIV/AIDS services- Basic primary health needs are unmet
10
Discussion A policy of confinement of drug users in
either prison or a CDTC is common in South East Asia:
- CDTCs are present in every country in the SE Asia , and number is increasing in most countries
- Lack of research on effectiveness/consequences of this policy
- Relapse is high - when reported
11
Discussion cont’
No adequate provision of evidence based drug treatment for either opiate or methamphetamine dependence including harm reduction services
12
Human Rights and Principles of Drug Treatment
Current approaches of confinement of drug users contravene:
1. the UN Covenants on Human Rights: The Right to the Highest Attainable Standard of Physical and Mental Health
2. WHO/UNODC Principles of Drug Dependence Treatment
13
The concerns
No evidence that the drug treatment centers are in any way effective as relapse rates are very high
All necessary steps to prevent, treat and control epidemics (HIV particularly) are currently not being taken prisons and compulsory treatment centers
14
Universal Access or
Access: Denied?
What are the human, economic and social costs of the CDTCs approach for individual, the community, the state?
What are the public health risks for confined drug users and the wider society?
15
Recommendations
1. Research on health risks and vulnerability in both prisons and CDTCs is needed
2. Evaluation on effectiveness of CDTCs is necessary
3. Alternatives to imprisonment and confinement, including increased access to low threshold, voluntary, community and evidence based drug treatment options; and a comprehensive HIV/AIDS package of interventions for drug users
16
Recommendations
4.Protect human rights of drug users5. Cease long period of detention without
trial and without access to health care especially for drug dependent people
6. Involve NGOs/civil society/families/affected community in the research; design, and implementation of responses
17
Tools:
18
Thank you
www.unodc.un.or.th/drugsandhiv/





























