Embed Size (px)
Citation preview

2011;17:406-415. Published OnlineFirst December 16, 2010.Clin Cancer Res Karel Eechoute, Alex Sparreboom, Herman Burger, et al. Clinical PracticeDrug Transporters and Imatinib Treatment: Implications for
Updated version
10.1158/1078-0432.CCR-10-2250doi:
Access the most recent version of this article at:
Cited Articles
http://clincancerres.aacrjournals.org/content/17/3/406.full.html#ref-list-1
This article cites by 78 articles, 37 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/3/406.full.html#related-urls
This article has been cited by 9 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
SubscriptionsReprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
To request permission to re-use all or part of this article, contact the AACR Publications
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

Review
Drug Transporters and Imatinib Treatment: Implications for Clinical Practice
Karel Eechoute1, Alex Sparreboom1,2, Herman Burger1, Ryan M. Franke2, Gaia Schiavon1, Jaap Verweij1,Walter J. Loos1, Erik A.C. Wiemer1, and Ron H.J. Mathijssen1
AbstractImatinib mesylate is approved for the treatment of chronic myeloid leukemia (CML) and advanced
gastrointestinal stromal tumors (GIST). Unfortunately, in the course of treatment, disease progression
occurs in the majority of patients with GIST. Lowered plasma trough levels of imatinib over time
potentially cause disease progression, a phenomenon known as "acquired pharmacokinetic drug resis-
tance." This outcome may be the result of an altered expression pattern or activity of drug transporters. To
date, the role of both efflux transporters (ATP-binding cassette transporters, such as ABCB1 and ABCG2)
and uptake transporters [solute carriers such as organic cation transporter 1 (OCT1) and organic anion
transporting polypeptide 1A2 (OATP1A2)] in imatinib pharmacokinetics and pharmacodynamics has
been studied. In vitro experiments show a significant role of ABCB1 and ABCG2 in cellular uptake and
retention of imatinib, although pharmacokinetic and pharmacogenetic data are still scarce and contra-
dictory. ABCB1 and ABCC1 expressionwas shown inGIST, whereas ABCB1, ABCG2, andOCT1were found
in mononuclear cells in CML patients. Several studies have reported a clinical relevance of tumor
expression or activity of OCT1 in CML patients. Further (clinical) studies are required to quantify drug
transporter expression over time in organs involved in imatinib metabolism, as well as in tumor tissue.
In addition, more pharmacogenetic studies will be needed to validate associations. Clin Cancer Res; 17(3);
406–15. �2010 AACR.
Introduction
Imatinib mesylate (Gleevec, Novartis International AG)is the first approved rationally designed inhibitor of specificprotein tyrosine kinases. The drug inhibits ABL and theBCR-ABL fusion protein [expressed in Philadelphia chro-mosome–positive chronicmyeloid leukemia (CML)], c-KIT[expressed in gastrointestinal stromal tumors (GIST)], andthe platelet-derived growth factor receptor (PDGF-R; i.e.,expressed in some sarcomas; refs. 1–4). Imatinib hasbecome the standard treatment for patients with chronicmyeloid leukemia (5, 6) and GIST (7–10).
Although response rates in imatinib-treated patients arehigh, ranging between 70 to 90% of patients with GIST aswell as CML (9, 11, 12), nonresponse or disease progres-sion after a certain period of time may occur. Geneticmutations or gene amplification of the drug targets areknown mechanisms for this observed (acquired) drugresistance (12–15). Accumulating data, however, indicate
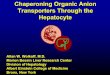
a contributing role of pharmacokinetics in imatinib effi-cacy, as well as for the initial therapeutic response, and forthe time to progression. Drug uptake and efflux trans-porters are likely to be involved in imatinib absorption,distribution, and excretion, thereby influencing pharma-cokinetics. Imatinib is almost completely absorbed (>97%;ref. 16) and is, then, extensively metabolized in the liverwith CGP74588 as its most active metabolite, predomi-nantly formed by cytochrome P450 isoform 3A4 and 3A5(CYP3A4, CYP3A5) as shown in Fig. 1 (17). This metabo-lite is equipotent to its parental compound in vitro. Othercytochrome P450 isoforms (CYP1A2, CYP2D6, CYP2C8,CYP2C9, and CYP2C19) also play a (minor) role in ima-tinib metabolism (17, 18). At clinically relevant concentra-tions, imatinib is bound to plasma proteins, mainlyalbumin and a1-acid glycoprotein (16, 19). Both imatiniband its activemetabolite are excreted in feces and, to a lesserextent, in urine.
Initial drug resistance could be correlated with drugexposure. For instance, imatinib trough levels, the lowestdrug concentration, right before administration of a newdose, in nonresponding patients are significantly lower (seeTable 1) than in responding patients (20–22). Moreover,imatinib pharmacokineticsmay also contribute to acquireddrug resistance. This finding was shown in a small-popula-tion pharmacokinetics study in patients with GIST (23).After long-term treatment (>1 year), imatinib clearanceincreased by �33% and systemic exposure decreasedby �42%, compared with the start of treatment, pos-sibly suggesting involvement of pharmacokinetics in the
Authors' Affiliations: 1Department of Medical Oncology, Daniel den HoedCancer Center, Erasmus University Medical Center, Rotterdam, the Neth-erlands; 2Department of Pharmaceutical Sciences, St. Jude Children'sResearch Hospital, Memphis, Tennessee
Corresponding Author: Ron H.J. Mathijssen, Dept. of Medical Oncology,Erasmus University Medical Center – Daniel den Hoed Cancer Center, ‘sGravendijkwal 230, 3015 CE, Rotterdam, the Netherlands. Phone: 31–10-7034897; Fax: 31–107034627; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-10-2250
�2010 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 17(3) February 1, 2011406
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

development of resistance. This change in pharmacoki-netics is likely also related to the reduced side effects overtime (14) and may also explain why dose escalation ofimatinib at first progression results in clinical benefit insubsets of patients with advanced CML and GIST (24–26).Despite a broad interpatient variability in imatinib
plasma exposure (27), more recent data suggest the clinicalsignificance of keeping imatinib plasma concentrationswithin a therapeutic range. That is, in GIST and CML, alower response rate and/or shorter time to progressionmayoccur when imatinib plasma levels drop below approxi-mately 1,000 ng/mL (21, 28–30). As reported in the studywith GIST patients, imatinib steady state trough levels werehigher than mentioned in literature (31). Therefore, anassociation with clinical benefit may be biased by theoverestimation of trough levels. Nonetheless, steady stateplasma concentrations above 1,000 ng/mL are often easilyreached with a daily dose of 400 mg imatinib (31–33). Yet,in a subset of patients, this plasma concentration is notreached with this standard dose. Understanding the causesfor this variability may be of clinical importance.One of the patient factors that is likely to be relevant for
the observed differences in imatinib pharmacokinetics isthe possible interpatient variability in drug transporterexpression and activity. In this review, we give a detailedoverview of the potential clinical relevance of recentlycharacterized drug transporters for imatinib therapy.
Interaction of Imatinib with Drug Transporters
Efflux transporters. Imatinib is a substrate of ATP-bind-ing cassette (ABC) transporters such as the ABC subfamily Bmember 1 (ABCB1; formerly known as P-glycoprotein orMDR1; refs. 32–38) and subfamily G member 2 [ABCG2;formerly known as breast cancer resistance protein (BCRP);refs. 37, 39, 40], which are involved in its excretion process.These drug transporters use the hydrolysis of ATP and
subsequent phosphorylation of the transporter as anenergy source, enabling active transport of substrates acrossvarious biomembranes (41, 42). Studies have reportedimatinib as an inhibitor of ABC transporters (35, 43,44), but there is growing consensus that ABC transporterinhibition by imatinib is dose dependent with inhibitiononly occurring at higher imatinib concentrations (Table 2;refs. 35, 37, 38). ABCB1 and ABCG2 are expressed in avariety of tissues, including liver (at the sinusoidal baso-lateral membrane, as well as the apical bile canalicularmembrane of hepatocytes; refs. 1, 37, 45, 46), intestine (atthe apical membrane; see Fig. 1; refs. 45–47), kidney,placenta (46, 48), and the blood-brain barrier (41, 49).The role of these efflux transporters in acquired drugresistance has been investigated more intensively thanthe role of uptake transporters because of the evidentphysiologic role of efflux transporters as a defense mechan-ism against penetration of xenobiotics.
Uptake transporters. Meanwhile, more than one fourthof the present-day anticancer drugs are oral formulations,stressing the possible relevance of intestinal absorptionthrough uptake transporters expressed on the apical mem-brane of enterocytes. These solute carriers (SLC) use elec-trochemical gradients of ions to transport substrates acrossa membrane. Mainly the role of organic cation transporter1 (OCT1 or the SLC22A1 gene product) and to a lesserextent organic anion transporting polypeptide 1A2(OATP1A2, the SLCO1A2 gene product) in imatinib uptakehas been described (50, 51). Furthermore, imatinib provedto be a good substrate for the solute carriers OATP1B3(SLCO1B3 gene product) and OCTN2 (SLC22A5 geneproduct), both expressed on the basolateral membraneof hepatocytes (Fig. 1; ref. 51).
Drug Transporters and ImatinibPharmacokinetics
AbsorptionThis knowledge raises the question whether altered
pharmacokinetics can be (in part) the result of (over)expression of drug transporters. At duodenal pH 5 to 6,imatinib is mainly charged (52), implying active intestinaltransport; this renders intestinally located solute carrierssuch as OATP1A2 and OCTN2 as good candidates forintestinal imatinib uptake (53, 54). However, to date, littleis known about the influence of these uptake transporterson imatinib pharmacokinetics. Another good candidate forsystemic imatinib uptake is ABCC4, expressed on thebasolateral membrane of hepatocytes (51). This effluxtransporter could pump imatinib from the liver to thesystemic circulation.
As mentioned above, imatinib is absorbed very effi-ciently, which is somewhat surprising, considering thehigh affinity of imatinib for ABC transporters, expressedon the canalicular membrane of hepatocytes and onenterocytes. A possible explanation for this apparentcontradiction could be local substrate inhibition ofefflux transporters by imatinib, bearing in mind its
Translational Relevance
Since the start of this millennium, imatinib hasbecome known as a very potent targeted agent for thetreatment of chronic myeloid leukemia (CML) andgastrointestinal stromal tumors (GIST). However, inpatients treated with imatinib, disease progression ulti-mately occurs because of resistance mechanisms. Toovercome drug resistance, it is essential to know moreabout the mechanisms behind this phenomenon. Inthis review, the role of influx and efflux transporters isdiscussed in depth to give clinical insight into pharma-cokinetic and pharmacodynamic pathways that arepossibly influenced by drug transporter expressionor activity. Finally, a better understanding of thesemechanisms should lead to strategies to prolong theefficacy of imatinib therapy in both of these diseases.
Drug Transporters and Imatinib Treatment
www.aacrjournals.org Clin Cancer Res; 17(3) February 1, 2011 407
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

dose-dependent interaction. Furthermore, absolute bioa-vailability could also be influenced by the balancebetween efflux and influx transport over the intestinalbarrier, favoring active imatinib uptake.
Tissue distributionLiver distribution. Imatinib is actively cleared from the
blood into the liver, where it is metabolized extensively.Possible candidates for this active transport are OATP1B3,OCTN2, and OCT1, predominantly located at the basolat-eral membrane of hepatocytes (Fig. 1; refs. 16, 51, 55, 56).
However, in vivo or clinical data, supporting the role ofsolute carriers in imatinib clearance, are not available.
Brain distribution. Systemic treatment of brain tumors(primary as well as metastases) is limited because of lowpenetration of drugs into the brain tissue. Distribution tothe brain is primarily prevented by the blood-brain barrierformed by the endothelial cells of brain capillaries. Theseendothelial cells also express ABCB1 and ABCG2 (41, 49),which actively prevent xenobiotics from diffusing into thebrain. This finding was illustrated in Bcrp and Mdr1a/1b(rodent analogs of ABCG2 and ABCB1, respectively)
© 2011 American Association for Cancer Research
Bilecanaliculus
Hepatocyte
CYP3A5CYP3A4
Imatinib
Uremictoxins
?
UremicUremictoxtttoxinsins
?
mmmmImmI
System circulation
ABCG2
ABCB1
ABCC4 OATP1B3
OCTN2
OCTN2
Smallintestine
ABCB1
ABCG2
OATP1A2
OCT1
Portal
vein
Figure 1. Scheme for theinvolvement of drug transportersin imatinib pharmacokinetics.Carriers and enzymes involved inimatinib absorption, metabolism,and excretion, respectively, intheir anatomical, tissue, and/orcellular localization.
Eechoute et al.
Clin Cancer Res; 17(3) February 1, 2011 Clinical Cancer Research408
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

Tab
le1.
Imatinib
trou
ghleve
ls(Cmin)in
imatinib-treated
chronicmye
loid
leuk
emia
andga
strointestinal
stromal
celltumor
patientswith
orwith
outclinical
resp
onse
Tum
or
type
Dose
rang
e(m
g)
No.of
patients
No.of
resp
ond
ers
Mea
nor
med
ianCmin
inresp
ond
ers(ng/m
L)
Med
ianfree
Cmin
inresp
ond
ers
(ng/m
L)
No.of
nonres
pond
ers
Mea
normed
ian
Cmin
inno
nres
pond
ers
(ng/m
L)
Med
ianfree
Cmin
inno
nres
pond
ers
(ng/m
L)
P-value
Referen
ce
CML
400–
800
351
297
1,00
9(�
544)
a,b
n.a.
c54
812(�
409)
an.a.
c0.01
20CML
50–80
025
421
81,05
7(�
585)
a,b
n.a.
c36
835(�
524)
an.a.
c0.03
330
CML
50–80
025
416
61,10
7(�
594)
a,d
n.a.
c88
873(�
528)
an.a.
c0.00
230
CML
400–
600
6856
1,12
3(�
617)
a,b
n.a.
c12
694(�
556)
an.a.
c0.03
21CML
400–
600
6834
1,45
2(�
649)
a,d
n.a.
c34
869(�
427)
an.a.
c0.00
121
CML
400
4020
2,34
0(�
520)
a,e
n.a.
c20
690(�
150)
an.a.
c0.00
229
GIST
400–
800
7357
1,44
6(414
–3,33
6)f,g
n.a.
c16
1,15
5(545
–4,18
2)f,h
n.a.
c0.25
28GISTi
Not
repo
rted
3314
n.a.
c25
.7(13.7–
27)j
19n.a.
c10
.1(6.1–17
.4)j,k
0.01
322
Abbreviations
:CML,
chronicmye
loid
leuk
emia;GIST,
gastrointestinal
stromal
tumors.
aMea
nCmin
(�SD).
bRes
pon
seis
defined
asco
mplete
cytoge
netic
resp
onse
.cNot
available.
dRes
pon
seis
defined
asmajor
molec
ular
resp
onse
.eRes
pon
seis
defined
asco
mplete
hematolog
icresp
onse
at3mon
thsor
major
cytoge
netic
resp
onse
at6mon
ths.
f Med
ianCmin
(and
rang
e).
gRes
pon
seis
defin
edbytheresp
onse
evalua
tioncrite
riain
solid
tumors(RECIST)
asstab
ledisea
se,partia
lres
pon
seor
complete
resp
onse
.hNon
resp
onse
isdefined
asdisea
seprogres
sion
byRECISTor
notas
sessab
le.
i Patientswith
exon
9mutated
orwtKIT
GIST.
j Med
ianfree
Cmin
(and
rang
e)de
duc
edfrom
imatinib
andAGPleve
ls.
k Non
resp
onse
isdefined
byRECISTas
disea
seprogres
sion
.
Drug Transporters and Imatinib Treatment
www.aacrjournals.org Clin Cancer Res; 17(3) February 1, 2011 409
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

knockout mouse models, showing that imatinib brainpenetration significantly increased in knockout mice com-pared with wild-type mice, with a greater difference inMdr1a/1b knockout (57). Another study with a rodentmodel showed that combined Bcrp and Mdr1a/1b knock-out proved to significantly increase brain penetration com-pared with individual Bcrp or Mdr1a/1b knockouts (33).These data suggest that inhibition of efflux transporters atthe blood-brain barrier may provide more tools in thetreatment of brain metastases in imatinib-treated patients.A few obstacles remain, however. For instance, Gardnerand colleagues showed that inhibition of ABCB1 andABCG2 in mice resulted in a proportional increase insystemic exposure to imatinib in plasma and brain, leavingthe brain-to-plasma concentration ratio unaltered (58).This finding suggests that reduced systemic eliminationof imatinib leads to the observed increase in imatinibexposure to the brain as a result of higher imatinib con-centrations at the blood-brain barrier, rather than a mod-ification of the barrier itself. Furthermore, it is still unclearif efflux inhibitors will increase imatinib levels in tumorcells located in the central nervous system, because theseinhibitors may be merely increasing brain uptake of sub-strates but not necessarily uptake into brain tumors (59).
ExcretionBiliary secretion. Up until now, in vivo experiments on
the importance of drug transporters for imatinib excretionhave shown only minor effects. Systemic clearance ofimatinib in Mdr1a/1b and Bcrp1 knockout mice was1.3-fold and 1.6-fold lower than wild-type mice (57). Acombined Mdr1a/1b/Bcrp1 knockout showed a 1.8-foldreduction in imatinib plasma clearance compared withwild-type mice when imatinib was administered intrave-nously (33). Interestingly, no differences in pharmacoki-netic parameters were found between Mdr1a/1b/Bcrpknockouts and wild-type mice after oral administrationof imatinib. Whether ABCB1 and ABCG2 contribute toimatinib clearance in humans to a similar degree and, moreimportantly, whether there is a possible upregulation ofthese efflux transporters in excretory organs during imati-nib treatment is unknown. These murine data, however,suggest a minor contribution of efflux transporters toimatinib clearance, compared with the hepatic metabo-lism. Indeed, an extensive first-pass metabolism of imati-nib could contribute more substantially to systemicclearance than Mdr1a/1b and Bcrp1 efflux.
Furthermore, protein expression of Abcb1 and Bcrp1 inmice did not differ after long-term treatment with orally
Table 2. Interaction between drug transporters and imatinib pharmacokinetics and pharmacodynamics
Drugtransporter
Study design Effects on imatinib PK Effects onimatinib PD
Transporterinteraction
Effect onimatinib IUR
Reference
ABCB1 In vitro IUR# 34–35,39In vitro Resistance " 35In vivo Systemic clearance " 33,57In vitro Inducer 32,40In vitro Inhibitor 32,35,37In vitro Substrate 37–38
ABCG2 In vitro IUR ¼ 44In vitro IUR# 39In vitro No resistance 44In vivo (mice) Systemic clearance " 33,57In vivo (mice) Plasma concentration ¼ 60In vivo (mice) Liver concentration ¼ 60In vitro Inhibitor 37,43–44In vitro Inducer 40In vivo (mice) No inducer 60In vitro Substrate 37–39
OCT1 In vitro IUR ¼ 51In vitro IUR" 50,62In vitro Resistance # 50Clinical (CML) Resistance # 63,65–66In vitro Substrate 50,62
OATP1A2 In vitro Substrate 51OATP1B3 In vitro Substrate 51OCTN2 In vitro Substrate 51
Abbreviations: PD, pharmacodynamics; PK, pharmacokinetics; IUR, intracellular uptake and retention.
Eechoute et al.
Clin Cancer Res; 17(3) February 1, 2011 Clinical Cancer Research410
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

administered imatinib (60). After daily administration for4 consecutive weeks, no upregulation of Abcb1 and Bcrp1in mouse liver and intestinal tissues was found. Also, nosignificant change in plasma and liver concentrations ofimatinib was seen. Theoretically, however, the length oftreatment required to induce upregulation of these drugtransporters in mice might be longer or the activity of bothefflux transporters over the course of time may changewithout a quantitative change in expression.Renal excretion. Although renal excretion accounts for
less than 10% of imatinib excretion (31, 61), increasedplasma exposure and decreased clearance in imatinib-trea-ted cancer patients with impaired renal function, were seen(61). This finding may be due to increased levels of circu-lating uremic toxins. One such toxin inhibits OATP1B3function in a rodent model (55), supporting the possibilitythat uremic toxins can directly reduce hepatic uptake ofimatinib by OATP1B3. Further elucidation of this mechan-ism is needed.
Drug Transporters and ImatinibPharmacodynamics
Role of OCT1 in chronic myeloid leukemia blasts. Thereis substantial evidence that tumor OCT1 expression oractivity determines therapeutic outcome in imatinib-treatedCML patients. Thomas and colleagues were the first to showthat inhibition of OCT1 in peripheral blood leukocytesfrom 6 CML patients, decreased intracellular imatinibuptake (62). This finding was confirmed in another study,showing that imatinibuptake in aCMLcell line significantlycorrelatedwithOCT1mRNA expression (63). Furthermore,White and colleagues showed that in vitro sensitivity forimatinib strongly correlated with the intracellular uptakeand retention of imatinib inmononuclear cells of untreatedCML patients (50).When prazosin, anOCT1 inhibitor, wasadded to these cells, the concentration needed to inhibitmolecular drug targets was significantly increased. Further-more, it was also shown that only the activity of OCT1 inmature CML blasts is associated with therapeutic outcomeand not the OCT1 activity in immature CD34þ cells (64).This could imply that effective tumoral uptake of imatinibby OCT1 may be decisive for therapeutic response in CMLpatients.On the other hand,Hu and colleagues showed thatintracellular uptake of imatinib in (nonleukemic) cellsoverexpressing OCT1 was only minimally higher than incontrol cells (51). In a gene expression analysis, theyshowed that SLC22A1 is significantly interrelated withABCB1, ABCG2, and SLCO1A2. Alternatively, SLC22A1gene expression could, therefore, be amarker for expressionand subsequent activity of other transporters involved inimatinib transport.SLC22A1 gene expression did prove to be a good pre-
dictor of clinical outcome in imatinib-treated CML patients(63, 65). Pretreatment OCT1 expression levels in 32 CMLpatients were 8 times higher in responders than in non-responding patients (65). This result was confirmed in 70CML patients, in which high baseline OCT1 RNA expres-
sion levels correlated with better cytogenetic response at6 months and prolonged progression-free and overallsurvival (63). White and colleagues showed that chronicphase CML patients with lowOCT1 activity showed clinicalbenefit from imatinib dose escalation, but they reported nocorrelation between clinical efficacy and OCT1 mRNAlevels (66).
ABC transporter expression in gastrointestinal stromaltumor and chronic myeloid leukemia. ABCB1 and ABCC1are expressed in approximately three quarters of GISTs,which is 2- to 3-fold more than the expression in leiomyo-sarcomas (67–69). On the other hand, Western blot ana-lysis of 21 GIST specimens showed no expression ofABCG2 (68). So, in contrast to the possible influence ofABCG2 on the intestinal uptake of imatinib (33, 40, 57),there seems to be no role for ABCG2 on a tumoral level inGIST patients. Little can be said of the impact of ABCB1 andABCC1 expression in stromal tumor cells on imatinibtherapy in these GIST patients because only a very limitednumber of patients in these studies were treated withimatinib.
Although preclinical data (34–36) show that cellular(over) expression of ABCB1 leads to a reduced intracellularaccumulation of imatinib, it is not clear whether long-termtreatment with imatinib induces overexpression of thistransporter in tumor cells. Mahon and colleagues examinedvarious cell lines and found no upregulation of the expres-sion of the ABCB1 gene by imatinib in time (70). Incontrast, bone marrow mononuclear cells in CML patientsresistant to imatinib showed an overexpression of ABCB1and ABCG2 (although not statistically significant; ref. 65).In addition, a gene expression analysis in CML patientsshowed that expression of ABCC3 in CML blasts wasunique to patients with disease recurrence (71). Morestudies with larger populations are needed to elucidatethe possible tumoral upregulation of efflux transportersduring imatinib therapy and its pharmacodynamic effects.
Integrating Knowledge of Transporters inImproving Imatinib Therapy: PharmacogeneticStudies
Pharmacokinetic impact of genetic variation in ABC trans-porters. To date, pharmacogenetic association studieswere predominantly done for ABCB1 andABCG2 (Table 3).Associations between 2 single nucleotide polymorphisms,known to reduce the activity of ABCB1 and ABCG2, respec-tively, and steady state imatinib pharmacokinetics in 82patients with mainly GIST, have been investigated (72).Sixteen patients had a heterozygous variant (421 C > A)genotype for ABCG2 and 20 patients expressed a homo-zygous variant for ABCB1 3435 C > T. No significantdifferences in imatinib pharmacokinetics were seen com-pared with the homozygous wild-type patients. On theother hand, Takahashi and colleagues recently showed thatimatinib trough levels were significantly higher in CMLpatients carrying an ABCG2 421A allele (in homozygous aswell as heterozygous variant genotypes; ref. 73).
Drug Transporters and Imatinib Treatment
www.aacrjournals.org Clin Cancer Res; 17(3) February 1, 2011 411
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

Gurney and colleagues found that patients with a TTThaplotype in ABCB1 1236C > T, 2677G > T/A, and 3435 C >T loci had significant higher estimated imatinib clearances(74). This finding is contradictory to reports showing lowermRNA and protein levels when a homozygous T allele forABCB1 3435C > T was present (75), and to the findings ofothers who observed a decreased hepatic 99mTC-MIBI elim-ination rate, a phenotypic marker for ABCB1-mediateddrug clearance, in patients with the TTT haplotype (76).In addition, in CML patients, a TTT-haplotype was asso-ciated with higher imatinib trough levels (77).
Clinical impact of genetic variation in ABC transporters.
Up until now, pharmacogenetic association studies asses-sing clinical efficacy were exclusively done in CML patients.A poor response was observed in CML patients who werehomozygous for the G allele in ABCG2 34G > A (78). As forABCB1, a 1236T allele was associated with better response,
whereas a 2677G allele or a CGC haplotype for the 1236,2,677, and 3,435 loci were associated with worse responsein CML patients (77). However, Kim and colleaguesobserved a reduced overall survival in CML patients carry-ing a TT genotype for 3435C > T locus, when analyzedunivariately (78). This finding was confirmed by anothergroup, who observed more resistance in CML patientscarrying T alleles at positions 1236 and 3,435 (79). Allin all, data on the role of pharmacogenetics in response andsurvival in CML patients receiving imatinib therapy arescarce and poorly validated or reproduced.
Pharmacokinetic and clinical impact of genetic variations
in solute carriers. To date, studies assessing the possiblerole of genetic polymorphisms in solute carriers in imatinibtherapy are limited to OCT1 and OATP1B3. Allelic variantsof the SLC22A1 gene (encoding for the OCT1 protein) withknown reduced function showed no effect on steady state
Table 3. Studied single-nucleotide polymorphisms in patients involved in imatinib pharmacokinetics andpharmacodynamics
Transporter gene Polymorphism Effects on imatinib PK Effects on imatinib PD No. of patients Reference
ABCB1 3435 T No 82 723435 T Cmin ¼ a Response ¼ b 67 73TTT haplotypec Cmin #a 90 77TTT haplotypec Clearance " 22 743435 T Overall survival #d 229 783435 T Resistance "e 52 791236 T Resistance "e 52 791236 T Response "b 90 771236 T Cmin ¼ a Response ¼ b 67 732677 T/A Cmin ¼ a Response ¼ b 67 732677 G Response #b 90 77CGC haplotypec Response #b 90 77
ABCG2 421 A No 82 72421 A Cmin "a Response ¼ b 67 7334 A Response #f 229 78
ABCC2 �24 T Cmin ¼ a Response ¼ b 67 73SLC22A1 181 T SS imatinib plasma level ¼ 74 51
1393 A SS imatinib plasma level ¼ 74 51181 T Response ¼ b 32 80480 G Response #g 229 78480 G Cmin ¼ a Response ¼ b 67 731022 T Cmin ¼ a Response ¼ b 67 731222 G Cmin ¼ a Response "b 67 73156 C Cmin ¼ a Response ¼ b 67 73
SLCO1B3 334 G Cmin ¼ a Response ¼ b 67 73
Abbreviations: PK, pharmacokinetics; PD, pharmacodynamics; SS, steady state.aImatinib plasma trough level.bMajor molecular response.cDescription haplotype: 1236C > T, 2677G > T/A, 3435C > T.dDefined as the period from initiation of imatinib therapy until the date of death from any cause or the date of last follow-up.eNonresponse defined as absence of cytogenetic response.fMajor or complete cytogenetic response.gHigher rate of loss of cytogenetic or molecular response.
Eechoute et al.
Clin Cancer Res; 17(3) February 1, 2011 Clinical Cancer Research412
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

imatinibplasma levels (181C>Tand1393G>A), in a groupof GIST and CML patients compared with the referencegenotype (51). Furthermore, Zach and colleagues found nosignificant differences in response in patients heterozygousfor the T allele in the SLC22A1 181C > T polymorphism(80). Also, no correlation between SLCO1B3 334T > Gpolymorphism and imatinib exposure or clinical responsewas seen in CML patients (73). On the other hand, CMLpatients carrying a homozygous GG genotype for theSLC22A1 480C > G polymorphism showed a lowerresponse rate (78). Furthermore, a higher response ratewas seen in CML patients carrying a GG genotype for the1222A>G locus (73).Unfortunately, imatinib trough levelsdid not significantly differ for these patients, carrying a1222GG genotype, as compared with the reference allele.
Future Perspectives
Although in vitro studies show that imatinib exposureleads to an upregulation of ABCB1 and ABCG2 in humancolon carcinoma cells (40), currently no data are availableon the expression of these drug transporters in humanintestinal cells under imatinib therapy. Future studiesshould assess the possible correlation between their expres-sion pattern in excretory organs over time with imatinibpharmacokinetics and clinical outcome. In order to studythe role of these transporters in the observed decline inimatinib clearance, a series of intestinal biopsies at differenttime points are needed.Current studies also show that the majority of GIST
expresses both ABCB1 and ABCC1, but its clinical impor-
tance is not yet elucidated. Although tumoral expression ofOCT1 in CML patients has already been correlated withtherapeutic outcome, more data are needed on the expres-sion pattern of drug transporters in tumor cells in bothCML and GIST patients and their possible pharmacody-namic impact. At least a quantification of these transportersover time should be made in GIST biopsies or mono-nuclear cells in CML patients in order to assess the possi-bility of an altered expression pattern of drug transportersas amechanistic explanation for an altered sensitivity to thedrug.
Finally, pharmacogenetic association data will need tobe validated or reproduced. At this point, no clear guide-lines exist on the design of pharmacogenetic studies.Preventing selection bias, adequate power analysis, clearendpoints, correction for genetic and nongenetic covari-ates, and other factors are often poorly implemented.Therefore, more pharmacogenetic studies assessing theassociation with imatinib pharmacokinetics and/or phar-macodynamics are desired, and study design will need tobe uniform. In the present context of rapidly emergingpromising compounds, the latter is of utmost importanceif we want to personalize dosing and treatment sequencesof rationally designed molecules to an individualpatient’s needs.
Disclosure of Potential Conflicts of Interest
No potential conflicts of interest were disclosed.
Received August 21, 2010; revised November 2, 2010; acceptedNovember 12, 2010; published OnlineFirst December 16, 2010.
References1. Buchdunger E, Zimmermann J, Mett H, Meyer T, M€uller M, Druker
BJ, et al. Inhibition of the Abl protein-tyrosine kinase in vitro and invivo by a 2-phenylaminopyrimidine derivative. Cancer Res 1996;56:100–4.
2. Lydon NB, Druker BJ. Lessons learned from the development ofimatinib. Leuk Res 2004;28[Suppl 1]:S29–38.
3. Verweij J, Judson I, van Oosterom A. STI571: a magic bullet? Eur JCancer 2001;37:1816–9.
4. de Jong FA, Verweij J. Role of imatinib mesylate (Gleevec/Glivec) ingastrointestinal stromal tumors. Expert Rev Anticancer Ther 2003;3:757–66.
5. O’Brien SG, Guilhot F, Larson RA, Gathmann I, Baccarani M, Cer-vantes F, et al. Imatinib compared with interferon and low-dosecytarabine for newly diagnosed chronic-phase chronic myeloid leu-kemia. N Engl J Med 2003;348:994–1004.
6. Druker BJ, Guilhot F, O’Brien SG, Gathmann I, Kantarjian H, Gatter-mann N, et al. Five-year follow-up of patients receiving imatinib forchronic myeloid leukemia. N Engl J Med 2006;355:2408–17.
7. van Oosterom AT, Judson I, Verweij J, Stroobants S, Donato di PaolaE, Dimitrijevic S, et al. Safety and efficacy of imatinib (STI571) inmetastatic gastrointestinal stromal tumours: a phase I study. Lancet2001;358:1421–3.
8. Demetri GD, von Mehren M, Blanke CD, Van Den Abbeele AD,Eisenberg B, Roberts PJ, et al. Efficacy and safety of imatinibmesylatein advanced gastrointestinal stromal tumors. N Engl J Med 2002;347:472–80.
9. Verweij J, Casali PG, Zalcberg J, LeCesne A, Reichardt P, Blay JY,et al. Progression-free survival in gastrointestinal stromal tumours
with high-dose imatinib: randomised trial. Lancet 2004;364:1127–34.
10. Joensuu H, Fletcher C, Dimitrijevic S, Silberman S, Roberts P, DemetriG. Management of malignant gastrointestinal stromal tumours. Lan-cet Oncol 2002;3:655–64.
11. Blanke CD, Rankin C, Demetri GD, Ryan CW, von Mehren M, Benja-min RS, et al. Phase III randomized, intergroup trial assessing imatinibmesylate at two dose levels in patients with unresectable or meta-static gastrointestinal stromal tumors expressing the kit receptortyrosine kinase: S0033. J Clin Oncol 2008;26:626–32.
12. Druker BJ. Translation of the Philadelphia chromosome into therapyfor CML. Blood 2008;112:4808–17.
13. Heinrich MC, Corless CL, Blanke CD, Demetri GD, Joensuu H,Roberts PJ, et al. Molecular correlates of imatinib resistancein gastrointestinal stromal tumors. J Clin Oncol 2006;24:4764–74.
14. Sleijfer S, Wiemer E, Seynaeve C, Verweij J. Improved insight intoresistance mechanisms to imatinib in gastrointestinal stromal tumors:a basis for novel approaches and individualization of treatment.Oncologist 2007;12:719–26.
15. Liegl B, Kepten I, Le C, Zhu M, Demetri GD, Heinrich MC, et al.Heterogeneity of kinase inhibitor resistance mechanisms in GIST.J Pathol 2008;216:64–74.
16. Peng B, Dutreix C, Mehring G, Hayes MJ, Ben-Am M, Seiberling M,et al. Absolute bioavailability of imatinib (Glivec) orally versus intra-venous infusion. J Clin Pharmacol 2004;44:158–62.
17. Gschwind HP, Pfaar U, Waldmeier F, Zollinger M, Sayer C, Zbinden P,et al. Metabolism and disposition of imatinib mesylate in healthyvolunteers. Drug Metab Dispos 2005;33:1503–12.
Drug Transporters and Imatinib Treatment
www.aacrjournals.org Clin Cancer Res; 17(3) February 1, 2011 413
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

18. Nebot N, Crettol S, D’Esposito F, Tattam B, Hibbs DE, Murray M.Participation of CYP2C8 and CYP3A4 in the N-demethylation ofimatinib in human hepatic microsomes. Br J Pharmacol 2010;161:1059–69.
19. Gambacorti-Passerini C, Zucchetti M, Russo D, Frapolli R, Verga M,Bungaro S, et al. Alpha1 acid glycoprotein binds to imatinib (STI571)and substantially alters its pharmacokinetics in chronic myeloid leu-kemia patients. Clin Cancer Res 2003;9:625–32.
20. Larson RA, Druker BJ, Guilhot F, O’Brien SG, Riviere GJ, Krahnke T,et al. Imatinib pharmacokinetics and its correlation with response andsafety in chronic-phase chronic myeloid leukemia: a subanalysis ofthe IRIS study. Blood 2008;111:4022–8.
21. Picard S, Titier K, Etienne G, Teilhet E, Ducint D, Bernard MA, et al.Trough imatinib plasma levels are associated with both cytogeneticand molecular responses to standard-dose imatinib in chronic mye-loid leukemia. Blood 2007;109:3496–9.
22. Widmer N, Decosterd LA, Csajka C, Montemurro M, Haouala A,Leyvraz S, et al. Imatinib plasma levels: correlation with clinical benefitin GIST patients. Br J Cancer 2010;102:1198–9.
23. Judson I, Ma P, Peng B, Verweij J, Racine A, di Paola ED, et al. Imatinibpharmacokinetics in patients with gastrointestinal stromal tumour: aretrospective population pharmacokinetic study over time. EORTCSoft Tissue and Bone Sarcoma Group. Cancer Chemother Pharmacol2005;55:379–86.
24. Kantarjian HM, Larson RA, Guilhot F, O’Brien SG,MoneM, Rudoltz M,et al. Efficacy of imatinib dose escalation in patients with chronicmyeloid leukemia in chronic phase. Cancer 2009;115:551–60.
25. Zalcberg JR, Verweij J, Casali PG, Le Cesne A, Reichardt P, Blay JY,et al. Outcome of patients with advanced gastro-intestinal stromaltumours crossing over to a daily imatinib dose of 800 mg afterprogression on 400 mg. Eur J Cancer 2005;41:1751–7.
26. Park I, Ryu MH, Sym SJ, Lee SS, Jang G, Kim TW, et al. Doseescalation of imatinib after failure of standard dose in Korean patientswith metastatic or unresectable gastrointestinal stromal tumor. Jpn JClin Oncol 2009;39:105–10.
27. Nikolova Z, Peng B, Hubert M, Sieberling M, Keller U, Ho YY, et al.Bioequivalence, safety, and tolerability of imatinib tablets comparedwith capsules. Cancer Chemother Pharmacol 2004;53:433–8.
28. Demetri GD,Wang Y,Wehrle E, Racine A, Nikolova Z, Blanke CD, et al.Imatinib plasma levels are correlated with clinical benefit in patientswith unresectable/metastatic gastrointestinal stromal tumors. J ClinOncol 2009;27:3141–7.
29. Singh N, Kumar L, Meena R, Velpandian T. Drugmonitoring of imatiniblevels in patients undergoing therapy for chronic myeloid leukaemia:comparing plasma levels of responders and non-responders. Eur JClin Pharmacol 2009;65:545–9.
30. Takahashi N, Wakita H, Miura M, Scott SA, Nishii K, Masuko M, et al.Correlation between imatinib pharmacokinetics and clinical responsein Japanese patients with chronic-phase chronic myeloid leukemia.Clin Pharmacol Ther 2010;88:809–13.
31. Peng B, Lloyd P, Schran H. Clinical pharmacokinetics of imatinib. ClinPharmacokinet 2005;44:879–94.
32. Hegedus T, Orfi L, Seprodi A, Varadi A, Sarkadi B, Keri G. Interaction oftyrosine kinase inhibitors with the human multidrug transporter pro-teins, MDR1 and MRP1. Biochim Biophys Acta 2002;1587:318–25.
33. Oostendorp RL, Buckle T, Beijnen JH, van Tellingen O, Schellens JH.The effect of P-gp (Mdr1a/1b), BCRP (Bcrp1) and P-gp/BCRP inhi-bitors on the in vivo absorption, distribution, metabolism and excre-tion of imatinib. Invest New Drugs 2009;27:31–40.
34. Widmer N, Colombo S, Buclin T, Decosterd LA. Functional conse-quence of MDR1 expression on imatinib intracellular concentrations.Blood 2003;102:1142.
35. Hamada A, Miyano H, Watanabe H, Saito H. Interaction of imatinibmesilate with human P-glycoprotein. J Pharmacol Exp Ther2003;307:824–8.
36. Zhang Y, Bachmeier C, Miller DW. In vitro and in vivo models forassessing drug efflux transporter activity. Adv Drug Deliv Rev2003;55:31–51.
37. Dohse M, Scharenberg C, Shukla S, Robey RW, Volkmann T, DeekenJF, et al. Comparison of ATP-binding cassette transporter interactions
with the tyrosine kinase inhibitors imatinib, nilotinib and dasatinib.Drug Metab Dispos 2010;38:1371–80.
38. Shukla S, Sauna ZE, Ambudkar SV. Evidence for the interaction ofimatinib at the transport-substrate site(s) of the multidrug-resistance-linked ABC drug transporters ABCB1 (P-glycoprotein) and ABCG2.Leukemia 2008;22:445–7.
39. Burger H, van Tol H, Boersma AW, Brok M,Wiemer EA, Stoter G, et al.Imatinib mesylate (STI571) is a substrate for the breast cancer resis-tance protein (BCRP)/ABCG2 drug pump. Blood 2004;104:2940–2.
40. BurgerH, van Tol H, BrokM,Wiemer EA, deBruijn EA,GuetensG, et al.Chronic imatinib mesylate exposure leads to reduced intracellulardrug accumulation by induction of the ABCG2 (BCRP) and ABCB1(MDR1) drug transport pumps. Cancer Biol Ther 2005;4:747–52.
41. Schinkel AH, Smit JJ, van Tellingen O, Beijnen JH, Wagenaar E, vanDeemter L, et al. Disruption of the mouse mdr1a P-glycoprotein geneleads to a deficiency in the blood-brain barrier and to increasedsensitivity to drugs. Cell 1994;77:491–502.
42. Giacomini KM, Sugiyama Y. Membrane transporters and drugresponse. Goodman & Gilman's The pharmacological basis of ther-apeutics. 11th ed. McGraw-Hill; 2005. p. 41–70.
43. Ozvegy-Laczka C, Hegedus T, Varady G, Ujhelly O, Schuetz JD, V¡radiA, et al. High-affinity interaction of tyrosine kinase inhibitors with theABCG2 multidrug transporter. Mol Pharmacol 2004;65:1485–95.
44. Houghton PJ, Germain GS, Harwood FC, Schuetz JD, Stewart CF,Buchdunger E, et al. Imatinib mesylate is a potent inhibitor of theABCG2 (BCRP) transporter and reverses resistance to topotecan andSN-38 in vitro. Cancer Res 2004;64:2333–7.
45. Thiebaut F, Tsuruo T, Hamada H, Gottesman MM, Pastan I, Will-ingham MC. Cellular localization of the multidrug-resistance geneproduct P-glycoprotein in normal human tissues. Proc Natl Acad Sci US A 1987;84:7735–8.
46. Maliepaard M, Scheffer GL, Faneyte IF, van Gastelen MA, PijnenborgAC, Schinkel AH, et al. Subcellular localization and distribution of thebreast cancer resistance protein transporter in normal human tissues.Cancer Res 2001;61:3458–64.
47. Behrens I, Kamm W, Dantzig AH, Kissel T. Variation of peptidetransporter (PepT1 andHPT1) expression in Caco-2 cells as a functionof cell origin. J Pharm Sci 2004;93:1743–54.
48. Nagashige M, Ushigome F, Koyabu N, Hirata K, Kawabuchi M,Hirakawa T, et al. Basal membrane localization of MRP1 in humanplacental trophoblast. Placenta 2003;24:951–8.
49. Cooray HC, Blackmore CG, Maskell L, Barrand MA. Localisation ofbreast cancer resistance protein inmicrovessel endothelium of humanbrain. Neuroreport 2002;13:2059–63.
50. White DL, Saunders VA, Dang P, Engler J, Zannettino AC, CambareriAC, et al. OCT-1-mediated influx is a key determinant of the intra-cellular uptake of imatinib but not nilotinib (AMN107): reduced OCT-1activity is the cause of low in vitro sensitivity to imatinib. Blood2006;108:697–704.
51. Hu S, Franke RM, Filipski KK, Hu C, Orwick SJ, de Bruijn EA, et al.Interaction of imatinib with human organic ion carriers. Clin CancerRes 2008;14:3141–8.
52. Szakacs Z, Beni S, Varga Z, Orfi L, Keri G, Noszal B. Acid-baseprofiling of imatinib (gleevec) and its fragments. J Med Chem2005;48:249–55.
53. Lee W, Glaeser H, Smith LH, Roberts RL, Moeckel GW, Gervasini G,et al. Polymorphisms in human organic anion-transporting polypep-tide 1A2 (OATP1A2): implications for altered drug disposition andcentral nervous system drug entry. J Biol Chem 2005;280:9610–7.
54. Koepsell H, Lips K, Volk C. Polyspecific organic cation transporters:structure, function, physiological roles, and biopharmaceutical impli-cations. Pharm Res 2007;24:1227–51.
55. Franke RM, Sparreboom A. Inhibition of imatinib transport by uremictoxins during renal failure. J Clin Oncol 2008;26:4226–7, author reply7–8.
56. Zhang L, Dresser MJ, Gray AT, Yost SC, Terashita S, Giacomini KM.Cloning and functional expression of a human liver organic cationtransporter. Mol Pharmacol 1997;51:913–21.
57. Breedveld P, Pluim D, Cipriani G,Wielinga P, van Tellingen O, SchinkelAH, et al. The effect of Bcrp1 (Abcg2) on the in vivo pharmacokinetics
Eechoute et al.
Clin Cancer Res; 17(3) February 1, 2011 Clinical Cancer Research414
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250

and brain penetration of imatinib mesylate (Gleevec): implications forthe use of breast cancer resistance protein and P-glycoprotein inhi-bitors to enable the brain penetration of imatinib in patients. CancerRes 2005;65:2577–82.
58. Gardner ER, Smith NF, Figg WD, Sparreboom A. Influence of the dualABCB1 and ABCG2 inhibitor tariquidar on the disposition of oralimatinib in mice. J Exp Clin Cancer Res 2009;28:99.
59. Shen J, Carcaboso AM, Hubbard KE, TagenM,Wynn HG, Panetta JC,et al. Compartment-specific roles of ATP-binding cassette transpor-ters define differential topotecan distribution in brain parenchyma andcerebrospinal fluid. Cancer Res 2009;69:5885–92.
60. Gardner ER, Sparreboom A, Verweij J, Figg WD. Lack of ABC trans-porter autoinduction in mice following long-term exposure to imatinib.Cancer Biol Ther 2008;7:412–5.
61. Gibbons J, Egorin MJ, Ramanathan RK, Fu P, Mulkerin DL, Shibata S,et al. Phase I and pharmacokinetic study of imatinib mesylate inpatients with advanced malignancies and varying degrees of renaldysfunction: a study by the National Cancer Institute Organ Dysfunc-tion Working Group. J Clin Oncol 2008;26:570–6.
62. Thomas J, Wang L, Clark RE, Pirmohamed M. Active transport ofimatinib into and out of cells: implications for drug resistance. Blood2004;104:3739–45.
63. Wang L, Giannoudis A, Lane S, Williamson P, Pirmohamed M, ClarkRE. Expression of the uptake drug transporter hOCT1 is an importantclinical determinant of the response to imatinib in chronic myeloidleukemia. Clin Pharmacol Ther 2008;83:258–64.
64. Engler JR, Frede A, Saunders V, Zannettino A, White DL, Hughes TP.The poor response to imatinib observed in CML patients with lowOCT-1 activity is not attributable to lower uptake of imatinib into theirCD34þ cells. Blood 2010;116:2776–8.
65. Crossman LC, Druker BJ, Deininger MW, Pirmohamed M, Wang L,Clark RE. hOCT 1 and resistance to imatinib. Blood 2005;106:1133–4,author reply 4.
66. White DL, Saunders VA, Dang P, Engler J, Venables A, Zrim S, et al.Most CML patients who have a suboptimal response to imatinib havelow OCT-1 activity: higher doses of imatinib may overcome thenegative impact of low OCT-1 activity. Blood 2007;110:4064–72.
67. Plaat BE, Hollema H, Molenaar WM, Torn Broers GH, Pijpe J, MastikMF, et al. Soft tissue leiomyosarcomas and malignant gastrointestinalstromal tumors: differences in clinical outcome and expression ofmultidrug resistance proteins. J Clin Oncol 2000;18:3211–20.
68. Theou N, Gil S, Devocelle A, Juli�e C, Lavergne-Slove A, Beauchet A,et al. Multidrug resistance proteins in gastrointestinal stromal tumors:site-dependent expression and initial response to imatinib. Clin Can-cer Res 2005;11:7593–8.
69. Perez-Gutierrez S, Gonzalez-Campora R, Amerigo-Navarro J, Beato-Moreno A, S�anchez-Le�on M, Pareja Megía JM, et al. Expression of
P-glycoprotein and metallothionein in gastrointestinal stromal tumorand leiomyosarcomas. Clinical implications. Pathol Oncol Res 2007;13:203–8.
70. Mahon FX, Deininger MW, Schultheis B, Chabrol J, Reiffers J, Gold-man JM, et al. Selection and characterization of BCR-ABL positive celllines with differential sensitivity to the tyrosine kinase inhibitor STI571:diverse mechanisms of resistance. Blood 2000;96:1070–9.
71. Radich JP, Dai H, Mao M, Oehler V, Schelter J, Druker B, et al. Geneexpression changes associated with progression and response inchronicmyeloid leukemia. Proc Natl Acad Sci U S A 2006;103:2794–9.
72. Gardner ER, Burger H, van Schaik RH, vanOosteromAT, de Bruijn EA,Guetens G, et al. Association of enzyme and transporter genotypeswith the pharmacokinetics of imatinib. Clin Pharmacol Ther2006;80:192–201.
73. Takahashi N, Miura M, Scott SA, Kagaya H, Kameoka Y, Tagawa H,et al. Influence of CYP3A5 and drug transporter polymorphisms onimatinib trough concentration and clinical response among patientswith chronic phase chronic myeloid leukemia. J Hum Genet2010;55:731–7.
74. Gurney H, Wong M, Balleine RL, Rivory LP, McLachlan AJ, HoskinsJM, et al. Imatinib disposition and ABCB1 (MDR1, P-glycoprotein)genotype. Clin Pharmacol Ther 2007;82:33–40.
75. Wang D, Johnson AD, Papp AC, Kroetz DL, Sadee W. Multidrugresistance polypeptide 1 (MDR1, ABCB1) variant 3435C>T affectsmRNA stability. Pharmacogenet Genomics 2005;15:693–704.
76. Wong M, Evans S, Rivory LP, Hoskins JM, Mann GJ, Farlow D,et al. Hepatic technetium Tc 99m-labeled sestamibi eliminationrate and ABCB1 (MDR1) genotype as indicators of ABCB1 (P-glycoprotein) activity in patients with cancer. Clin Pharmacol Ther2005;77:33–42.
77. Dulucq S, Bouchet S, Turcq B, Lippert E, Etienne G, Reiffers J, et al.Multidrug resistance gene (MDR1) polymorphisms are associatedwith major molecular responses to standard-dose imatinib in chronicmyeloid leukemia. Blood 2008;112:2024–7.
78. Kim DH, Sriharsha L, Xu W, Kamel-Reid S, Liu X, Siminovitch K, et al.Clinical relevance of a pharmacogenetic approach using multiplecandidate genes to predict response and resistance to imatinibtherapy in chronic myeloid leukemia. Clin Cancer Res 2009;15:4750–8.
79. Ni LN, Li JY, Miao KR, Qiao C, Zhang SJ, Qiu HR, et al. Multidrugresistance gene (MDR1) polymorphisms correlate with imatinibresponse in chronic myeloid leukemia. Med Oncol 2010. Epub2010 Mar 4.
80. Zach O, Krieger O, Foedermayr M, Zellhofer B, Lutz D. OCT1(SLC22A1) R61C polymorphism and response to imatinib treatmentin chronic myeloid leukemia patients. Leuk Lymphoma 2008;49:2222–3.
Drug Transporters and Imatinib Treatment
www.aacrjournals.org Clin Cancer Res; 17(3) February 1, 2011 415
Research. on April 13, 2014. © 2011 American Association for Cancerclincancerres.aacrjournals.org Downloaded from
Published OnlineFirst December 16, 2010; DOI: 10.1158/1078-0432.CCR-10-2250


![Ions channels/transporters and chloroplast regulation · transporters/pumps and secondary transporters (according to the Transport Classification system [1]). Channels transport](https://img.pdfslide.us/doc/110x75/601623c1d6936b1074546c48/ions-channelstransporters-and-chloroplast-transporterspumps-and-secondary-transporters.jpg)