Embed Size (px)
Citation preview

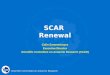
Translational Science
Drug Sensitivity Prediction Models Reveal a Linkbetween DNA Repair Defects and Poor Prognosisin HNSCCPaul B.M. Essers1, Martijn van der Heijden1,2, Caroline V.M. Verhagen1, Emily M. Ploeg1,Reinout H. de Roest3, C. Ren�e Leemans3, Ruud H. Brakenhoff3,Michiel W.M. van den Brekel2, Harry Bartelink4, Marcel Verheij1,4, and Conchita Vens1,4
Abstract
© 2019 American Association for Cancer Research
DNA damagingdrugs sensitivity
DNA repairdefect
identification
Primary tumor biopsies180 HNSCC patients
DNA repair deficient
High risk ofmetastasis
DNA repairdefect
prediction
Patient -derived HNSCC cell lines
In Vitro In Vivo
Geneexpression
DNA repair proficient
Link DNA repair defectsto metastasis
Machine learning classifiers developed to identify DNA repair defects in cells reveal associations withmetastasis in patients and link repair defects to migration and invasiveness.
viab
ility
?
Geneexpression
DNA repair deficient
DNA repair proficient
Migratoryinvasive
Train machinelearning classifiers
concentration
Head and neck squamous cell carcinoma (HNSCC) is charac-terized by the frequent manifestation of DNA crosslink repairdefects.We established novel expression-basedDNA repair defectmarkers to determine the clinical impact of such repair defects.Usinghypersensitivity to theDNAcrosslinking agents,mitomycinC and olaparib, as proxies for functional DNA repair defects in apanel of 25 HNSCC cell lines, we applied machine learning todefine gene expression models that predict repair defects. Theexpression profiles established predicted hypersensitivity toDNA-damaging agents and were associated with mutations incrosslink repair genes, as well as downregulation of DNA damageresponse and repair genes, in two independent datasets. Theprognostic value of the repair defect prediction profiles wasassessed in two retrospective cohorts with a total of 180 patientswith advanced HPV-negative HNSCC, who were treated withcisplatin-based chemoradiotherapy. DNA repair defects, as pre-dicted by the profiles, were associated with poor outcome in bothpatient cohorts. The poor prognosis association was particularlystrong in normoxic tumor samples andwas linked to an increasedrisk of distant metastasis. In vitro, only crosslink repair–defectiveHNSCC cell lines are highly migratory and invasive. This pheno-type could also be induced in cells by inhibiting rad51 in repaircompetent and reduced by DNA-PK inhibition. In conclusion,DNA crosslink repair prediction expression profiles reveal a poorprognosis association in HNSCC.
Significance: This study uses innovative machine learning-based approaches to derive models that predict the effect of DNArepair defects on treatment outcome in HNSCC.
Graphical Abstract: http://cancerres.aacrjournals.org/content/canres/79/21/5597/F1.large.jpg.
IntroductionDNA repair pathways, such as homologous recombination
(HR), Fanconi anemia (FA), and associated cellular repair path-ways govern genomic integrity and maintain chromosomal sta-
bility. Recent genetic studies highlight the identification of anincreasing number of DNA damage response (DDR) and DNArepair gene defects in cancer (1), but the role of these defects incancer outcome or treatment response is not yet fully understood.Early in vitro studies showed how defects in DDR and DNA repair
1Division of Cell Biology, The Netherlands Cancer Institute, Amsterdam, theNetherlands. 2Department of Head and Neck Oncology and Surgery, TheNetherlands Cancer Institute, Amsterdam, the Netherlands. 3Department ofOtolaryngology/Head and Neck Surgery, VUmc Cancer Center Amsterdam,Amsterdam, the Netherlands. 4Department of Radiation Oncology, TheNetherlands Cancer Institute, Amsterdam, the Netherlands.
Note: Supplementary data for this article are available at Cancer ResearchOnline (http://cancerres.aacrjournals.org/).
M. van der Heijden and C.V.M. Verhagen contributed equally to this article.
Corresponding Author: Conchita Vens, The Netherlands Cancer Institute, Ples-manlaan 121, 1066CX Amsterdam, The Netherlands. Phone: 31-20-512-2043;E-mail: [email protected]
Cancer Res 2019;79:5597–611
doi: 10.1158/0008-5472.CAN-18-3388
�2019 American Association for Cancer Research.
CancerResearch
www.aacrjournals.org 5597
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

pathways cause increased sensitivities to chemotherapeutic agentsor radiation. Thus, given the DNA-damaging nature of manycancer treatment agents, tumor repair defects are expected to bebeneficial for overall patient outcome.However, evidence,mostlyassessed in breast cancer, is inconclusive (2). Studies in othercancer types are less numerous and are greatly hampered by thelack of biomarkers that identify functional repair defects. Here weset out to develop DNA repair defect markers to determine theclinical impact of DNA repair defects in head and neck squamouscell carcinoma (HNSCC).
DNA repair gene variants may be used to depict DNA repairdefects, such as in the case of pathogenic BRCA1/2 variants inbreast or ovarian cancer (1, 3). Althoughmutations in such geneshave been shown to predict platinum (4) and olaparib (5)response, determining which mutations affect the function of agiven protein or pathway remains difficult (6). In addition,despite the high number of variants andmutations, the frequencyof specific variants is very low.Other attempts successfully appliedindirect repair defect measures such as "genomic scars" (7). Thegenomic scar biomarkers were developed in BRCA1/2-mutantbreast cancer and show promise for patient stratification forolaparib treatment in clinical trials in breast cancer (8). Suchscar-based biomarkers depict past repair defect events. Multipleresistance mechanisms have recently been described and someshow DNA repair restoration (9, 10).
The quest to assess the clinical impact of DDR and repairdefects in other cancer types faces many challenges. NumerousDDR genes have been shown to be mutated in human can-cer (11). However, the functional significance of most of thesemutations is largely unknown. Amultitude of genes are affectedand themutated genes or pathways vary largely among differentcancer types. The oncogenetic context in these cancers alsoimpacts DNA repair pathway engagement or performance.Detection of DNA repair defects therefore requires broadeningthe scope beyond breast- and ovarian cancer–specific BRCAmutations. A gene expression profile for mutations that phe-nocopy p53 inactivation was developed as a proxy for a defi-ciency in DNA damage response, and showed an associationwith poor prognosis in some cancers (12). However, an exclu-sive focus on TP53 mutations limits the prediction to alteredp53 response rather than DNA repair defect prediction. Func-tional analyses, such as the inability of cells to recover fromDNAcrosslinker exposure, reliably reveal DNA crosslink repairdefects, independent of the underlying genetic cause. Similarto genomic scars, functional repair endpoint studies aim toimprove the association with true yet undetected DNA repairdefects (13–15). Previous studies by us and others exposedfunctional DNA repair defects in the HR/FA pathway inHNSCC (16–18). These defects were identified by determiningsensitivity to the two DNA-damaging agents: mitomycin C(MMC) or olaparib in patient-derived HNSCC cell lines (16).MMC is a potent DNA crosslinking agent. Cellular survival afterexposure to DNA crosslinking agents requires the concertedaction of multiple repair pathways, including nucleotide exci-sion repair, FA andHR (19). MMChypersensitivity is therefore ahallmark of FA pathway defects and has been used in theidentification of many members of the FA and HR pathway,such as the BRCA1/2 genes (20). The PARP inhibitor olaparibinterferes in PARP-mediated DNA repair, primarily single-strand break repair and inhibitor-induced trapped PARP posesreplication blocks (21). Together with the increased load of
unresolved DNA damage, such blocks also contribute to theinduction of secondary DNA double-strand breaks (22). Cellswith HR/FA defects and with high levels of replication stressstruggle to survive PARP inhibition. As with MMC, hypersensi-tivity to PARP inhibition can therefore reveal functional HR andFA pathway defects, also of unknown genetic causes. Notably, ashift in the engagement from HR toward other DSB repairpathways can circumvent defects that cause PARP inhibitorsensitivity, while maintaining crosslinker sensitivity (9, 20, 23).Functional pathway defects were accompanied by genetic var-iants in multiple FA and HR genes in some of the HNSCC celllines, but not all, in our in vitro study, further arguing forfunctional endpoint-based assays (16).
HNSCC are in particular interesting in that they have beenshown to exhibit functional DNA repair defects that are caused bya multitude of genetic aberrations in different DNA repair path-ways. FA and HR gene variants were identified in larger HNSCCsequencing efforts (18) and found to be common in youngpatients withHNSCC (24), but the relation to treatment outcomeis less well explored. A small study compared HR pathwayengagement in biopsies of 13 patients with HNSCC before andafter the start of chemoradiotherapy by analyzing the ability toform Rad51 foci; this points to a poorer patient outcome ofcarriers of DNA repair–affected tumors (14). In line with suchan influence, a recent study highlights the association betweenchromosomal instability and lymph node status in HNSCC (25).Larger studies investigating the effect of functional DNA repairdefects on patient outcome in HNSCC are lacking.
In this study, we aimed to determine the impact of such DNArepair defects on outcome and treatment response inHNSCC.HRand FA repair defects provoke replication stress in proliferatingcells and a network of various compensatory DNA repair optionsare engaged to assure cellular survival. We therefore posit thatDNA repair–defective cells will show a distinct transcriptionalpattern that indirectly reflects the DNA damage response tounrepaired damage from endogenous sources. To embrace thevariety of repair defect types and genetic contexts, we employed alarge panel of patient-derivedHNSCCcell lines, ofwhich, a subsetshowed functional repair defects as determined by hypersensi-tivity to MMC and/or the PARP inhibitor olaparib and usedmachine learning models to predict a biological characteristic,DNA crosslink repair status. Independent in vitro datasets wereused to test the performance in identifying DNA repair defects.The impact ofDNA repair defects, as identifiedby these expressionmodels, in clinical outcome was determined in two independentHNSCC patient cohorts uniformly receiving standard-of-carecisplatin-based chemoradiotherapy.
Materials and MethodsCell culture
UT-SCC are primary tumor cell lines from patients withHNSCC and were established by Prof. Grenman (Universityof Turku, Turku, Finland) from whom we obtained the celllines. Cell lines were genotyped (Eurofins) and further charac-terized by photographs, cell doubling times, and assayed at lowpassage numbers. Cells were cultured in DMEM þ GlutaMAX(Gibco, Life Technologies), supplemented with 10% FBS(Gibco, Life Technologies), 1% penicillin–streptomycin(Gibco, Life Technologies) and 1� MEM non-essential aminoacids solution (NEAA; Gibco, Life Technologies) at 37�C, 5%
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5598
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

CO2, and 3% O2. Cell lines were routinely tested for Mycoplas-ma contamination.
Expression analysisRNA was isolated using the DNA AllPrep DNA/RNA Mini Kit
(Qiagen). Strand-specific libraries were generated using the Tru-Seq Stranded mRNA Sample Preparation Kit (Illumina Inc., RS-122-2101/2) according to the manufacturer's instructions. Readswere mapped against the GRCh38 human genome withTopHat2.1, using the options fr-firststrand, transcriptome-index,and prefilter multi-hits. Gene expression was determined usingHTSeq-count with options stranded and mode union. Differen-tial expression was performed using DESeq2. Genes with log2-fold change higher than one were classified as differentiallyexpressed, with a false discovery rate of 10%.
Data are available at the European Genome-phenome Archive(EGA).
Predictive modelingFor modelling, RPKM values were calculated from the read
counts and were scaled to have mean 0 and SD 1. Only geneswhose expression was measured in the CGP (26) and Peng (27)datasets (15,383 genes) were considered to allow model valida-tion in these datasets. In addition, expressions of 13,886 signa-tures from the Enrichr website (Supplementary Table S1) werecalculated using the GSVA BioConductor package. Variables wereselected as explained in Supplementary Fig. S1A. Models were fitusing the train function from the Caret R package. Options usedwere trainControl (boot ¼ 10), tuneLength ¼ 10, and preproces-sing (centre, scale). pROC package was used to calculate perfor-mance. Each of the best performing combinations of featureselection and classifier was trained on the whole dataset 20 times.For predictions, class probabilities were calculated as the averageof 20 model predictions. For the model ensemble predictions,class probabilities of the selectedmodels of each type (mmcOnly,olaOnly, or threeClass) were averaged to obtain the final predic-tion value. The mmcOnly model is available as an R package atbitbucket.org/paulessers/dna-repair-model-ensemble/.
Patient data and materialBiopsies and collection of fresh-frozen tumor material were
approved by the Institutional Review Board and all patientsgrantedwritten informed consent. The retrospective "NKI-CRAD"cohort provided pretreatment tumor biopsy material from 98patients with hypopharyngeal, laryngeal, or HPV-negative oro-pharyngeal HNSCC who were treated at the Netherlands CancerInstitute between 2001 and2014. Sampleswith tumor percentage<40%, as determined by hematoxylin and eosin (H&E) staining,were excluded. HPV status was determined using p16 and p53IHC and validated using PCR and RNA-sequencing. HPV-positivepatients were excluded. All patients were treated with cisplatin-based chemoradiotherapy. Radiotherapy was administeredaccording to a conventional (35 fractions of 2 Gy over 7 weeks)or DAHANCA scheme (35 fractions of 2 Gy over 6 weeks).Chemotherapy consisted of daily (25 times 6 mg/m2), weekly(6 � 40 mg/m2) or 3-weekly (3 � 100 mg/m2) intravenousadministration of cisplatin. Eight patients received intra-arterialcisplatin (4 � 150 mg/m2) according to the RADPLAT trial (28).Not all patients completed chemotherapy and the individual totalcumulative cisplatin dose was recorded. Overall survival wascalculated from the start of the treatment until the event or
censored at the time of the last follow-up. Metastasis and locor-egional recurrence-free survival were additionally censored at thetime of death. TheDESIGN cohort consisted of 82 advancedHPV-negative patients with HNSCC who were included in the Dutchmulticenter DESIGN study (KWF-A6C7072) and were treated attheVUmcCancerCenter Amsterdamor in theNetherlandsCancerInstitute (Amsterdam, the Netherlands). Patient selection criteriawere equal to those of the NKI-CRAD cohort; patients who werepreviously treated with radiotherapy in the head and neck area orchemotherapy were excluded.
Scratch assaysFor migration assays, cells were seeded in DMEMþGlutaMAX
in an IncuCyte ImageLock 96-wells Plate (Essen Bioscience) at100% confluence. After 24 hours, a homogeneous scratch wasmade with the use of the IncuCyte WoundMaker (Essen Biosci-ence) and washed twice with culture medium. Relative wounddensity was measured every 4 hours using the IncuCyte (EssenBioscience). For invasion assays, the same protocol was used withmodifications: 100 mg/mL growth factor reduced (GFR) Matrigel(Corning) was added to an IncuCyte ImageLock 96-well plate.After 24 hours, nonsolidified Matrigel was aspirated and cellsseeded. After 4 hours, the cells were scratched and washed twiceand 8 mg/mL GFR Matrigel was added. Thirty minutes later,culture medium was added and plates were placed in the Incu-Cyte. Rad51 experiments were performed by adding 500 nmol/LRad51 inhibitor (B02, SML0364, Sigma) after cell seeding andagain after the scratch was made. Inhibitors of DNA-PK NU7026,ATM Ku-55933, and WNT XAV-939 (all from SelleckChem) wereadded after the scratch was made.
Transwell assaysFor migration assays, multiple UT-SCC cell lines were seeded
(1.11 � 104 cells/insert) in culture medium with low serumconcentration (0.5% FBS) in the top of an 8-mm pore sizeTranswell insert (Falcon, Thermo Fisher Scientific). Culturemedium with 10% FBS was placed in the bottom of a 24-wellplate. After 24 hours, membranes were fixed for 2 minutes atroom temperature with 3.7% formaldehyde and washed twicewith PBS. Cells were permeabilized with 100%methanol for 20minutes at room temperature, washed twice with PBS, andstained with Hoechst (16 mg/mL; Thermo Fisher Scientific) for10 minutes at room temperature. The membrane was washedwith PBS and cells were removed from the bottom or top of themembrane with a cotton swab. Images were made (10� objec-tive) with the Axiovert 200M (Zeiss) microscope and analyzedusing ImageJ software. For invasion experiments, 125 mg/mLGFR Matrigel was added to the top of the insert and leftopen overnight, allowing the Matrigel to dry onto the mem-brane. The Matrigel was reconstituted with culture mediumfor 1 hour.
Statistical analysesAnalyses were performed in the R statistical computing envi-
ronment. Scripts used for visualizing patient survival are avail-able at https://github.com/PaulEssers/SurvivalPlots/. Spindleindex, scratch assays, and transwell assays were analyzed bylinear-mixed effects models using the nlme R package. Modelswere fit with "Group" as the fixed effect and the nested term"1|cellLine/Experiment" as the random effect. P values reportedare those for the fixed effects.
Predicting DNA Repair Defects in HNSCC
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5599
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

ResultsGeneration of DNA repair defect predictive expression modelsusing different functional endpoints
A dual drug sensitivity analysis in patient-derived HNSCC celllines revealed three classes of HNSCC: (i) MMC and olaparibsensitive, consistent with pronounced crosslink repair, i.e., HRandFA, pathwaydefects; (ii)MMCsensitive that lack concomitantolaparib sensitivity, likely due to compensatory repair mechan-isms and a shift in replication associated repair pathway prefer-ence and (iii) HNSCC that do not show strong repair defects asidentified by drug sensitivity (Fig. 1A; ref. 16). We will refer tothese groups as SensMO (i), SensM (ii), and Normal (iii), respec-tively. Upon further analysis, HR and FA gene mutations werefound in the MMC-sensitive HNSCC cell lines, providing thepotential genetic causes of the functional repair defects (Supple-mentary Fig. S1; refs. 16, 29).
We reasoned that changes in the transcriptome will reflectcellular DNA repair status via activation of the DNA damagestress response and downstream mediators. We therefore usedRNA-sequencing data from HNSCCs assigned to these threedifferent functional endpoint classes. By pairwise comparisons,82 genes were found to be differentially expressed between thegroups. However, expression levels of these genes varied consid-erably within groups, and therewere no genes that were expressedexclusively andubiquitously in each group (Fig. 1B).Consequent-ly, these traditional gene signatures, derived from these differen-tially expressed genes, performed poorly as predictors of drugsensitivity as determined by the AUC [area under the receiveroperating characteristic (ROC) curves; Fig. 1C)]. Therefore, weused machine learning algorithms to capture more complexrelationships between gene expression and the functional DNArepair endpoint.
Wegenerated apredictivemodel, exploiting the combineddrugsensitivity data, so as to be able to distinguish between the threegroups (threeClass). Alternatively, we generatedmodels that werebased on the sensitivity to each drug separately with the goal topredict olaparib or MMC sensitivity only (mmcOnly andolaOnly). Next to gene expression values, we also calculatedexpression values for established gene signatures (SupplementaryTable S1; ref. 30). Gene expression values, signature expressionvalues, or bothwere then used as input to train themodels. As ourultimate aim was to identify and investigate the effect of DNAcrosslink repair defects on patient outcome, we considered avariety of methods to minimize potential method–specific biasand repair-unrelated associations. Relevant genes and gene sig-natures were preselected using several techniques and were usedto trainmultiple predictivemodels (see Supplementary Fig. S2 forschematic representation and description). To assess the perfor-mance of all the different models derived from the individualcombinations of feature selection method and classifier, wecomputed the mean AUC values from 10 rounds of a 5-foldcross-validation, or 16 rounds of a 3-fold cross-validation of each(Fig. 1D andE; Supplementary Table S2).Nearly all combinationspredicting olaparib or MMC sensitivity (i.e., olaOnly andmmcOnly) performed well. We assessed whether the IC50 cutoffsthat were used to classify the cell lines were crucial for modelperformance and found that minor variations had little effect onthe AUC (Supplementary Fig. S3). The threeClass approachperformed less well in this analysis (Fig. 1E); however, this couldbe a result of low sample size when dividing the data into three
groups. This therefore does not necessarily preclude an ability toidentify repair defects. Consequently, the threeClass combina-tions were included in the subsequent validation studies.
For further external validation, we selected the best performingcombinations of feature selection and classifier, defined as thosewithin the top 25 of both the 3- and 5-fold cross-validations,resulting in 9mmcOnly, 13 olaOnly, and 13 threeClass combina-tions (Fig. 1F; Supplementary Table S2). We used these to trainmodels on the full HNSCC cell line expression dataset andcombined the resulting models into ensembles (Fig. 1F). Scoresof these ensembles that represent the probability of each cell lineto fall into any of the sensitivity groups (normal, SensM, SensMO)are shown in Fig. 1G.
Validation in external datasetsTo verify that our models can be used to predict DNA repair
defects, we next determinedwhether ourmodels are predictive forsensitivity ofDNA-damaging agents in other datasets.HNSCCcellline responses to a large number of compounds were determinedas part of the Cancer Genome Project (CGP; ref. 26). The predic-tions from both MMC sensitivity relevant ensembles, mmcOnly,and threeClass (SensM and SensMO combined), correlate withMMC IC50 in this dataset (Fig. 2A). This also translated into anability to identify DNA repair–defective cell lines, as classified bytheir MMC sensitivity (Fig. 2B). We did not observe a correlationbetween the olaOnly ensemble scores and MMC sensitivity. TheolaOnlymodel ensemblewas consequently unable to distinguishMMC-sensitive cells. For olaparib sensitivity, we did not observe acorrelation with model prediction scores for any ensemble, likelydue to uncertainty in the computationally inferred IC50 values inthe CGP HNSCC cell lines (Supplementary Fig. S4A–S4C).Importantly, all three model ensembles also predicted the pres-ence of mutations in DNA crosslink repair genes (SupplementaryFig. S4B; Supplementary Table S3), with the mmcOnly andthreeClass model ensembles showing the best performance(Fig. 2C).
As a complementary validation strategy that these modelspredict DNA repair defects beyond drug sensitivity, we deter-mined the capability of our models to detect alterations in DDRand repair. In a study by Peng and colleagues (27), components oftheDDRand repair pathwayswere knockeddownusing shRNA inbreast cancer cells and gene expression was measured usingmicroarrays. We tested whether the model ensembles can distin-guish cells treated with no or control shRNA from those treatedwith the tested shRNAs against DDR genes. We find that theensembles accurately predicted DDR defects caused by the loss ofATM, ATR, CHK1 CHK2, and 53BP1 (Fig. 2D). The performancefor BRCA1 and RAD51 knockdown was more heterogeneous(Fig. 2D), a characteristic that could be explained by the differ-ences in downstream signaling and transcriptomics that arecaused by the complete loss of the protein compared withdeleterious gene mutations. Interestingly, loss of the DNA dam-age response mediator MCPH1 (BRIT1) results in a consistentlyand greatly reduced signal for DNA repair defects, suggesting anessential role of the chromatin remodeling cyclin response inestablishing the distinctive gene expression patterns that aredetected by these models.
On the whole, we conclude that both the mmcOnly and thethreeClass model ensembles capture features of DDR and DNAcrosslink repair defects, i.e., drug sensitivity and DDR gene
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5600
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

mutations, and repair defects resulting from DDR geneknockdowns.
Predicted DNA repair defect association with poor clinicaloutcome
Using these two validated model ensembles, we determinedwhether survival is different in patients with tumors that showDNA repair defect–associated gene expression patterns. For thispurpose, we used pretreatment tumor biopsy gene expressiondata from our in-house HNSCC cohort (NKI-CRAD) of 98patients with advanced stage HPV-negative tumors (characteris-tics in Supplementary Table S4), who underwent radiotherapywith cisplatin-based treatment regimens. Consistent with previ-ous reports, tumor site (31) and cumulative cisplatin dose (32)are prognostic factors in ourNKI-CRAD cohort. DNA repair defectscores were established using the mmcOnly model ensemble forall tumor samples. These scores did not correlate with any of thepotentially prognostic clinical factors (NKI-CRAD data in Sup-plementary Fig. S5 and Supplementary Table S5). We then divid-ed the patient population into two equal-sized groups, based onthe ranking of the mmcOnly ensemble scores, and found a trendtoward poorer prognosis for the patients with the higher scores(Fig. 3A).
Hypoxia and cumulative cisplatin dose are independent prog-nostic factors in HNSCC (Supplementary Fig. S6A and S6B;ref. 33). To consider the hypoxia status, the average expressionof five published hypoxia signatures (34)was calculated and usedto divide the patient population into equally sized hypoxic andnormoxic subgroups. SubsequentDNA repair defect classificationby the mmcOnly models in these subgroups shows that the poorprognosis association is particularly strong in normoxic tumorsamples (Fig. 3B). This interaction is statistically significant (P ¼0.011) and was therefore included in subsequent multivariateanalyses. Upon closer inspection, we find that overall geneexpression changes from repair defects (high inDNA repair defectscore) under normoxia correlate highly with those from hypoxiaexposure (as determinedby thehypoxia score) in repair-proficienttumors in both cohorts, even though the actual patient classifi-cation does not (Supplementary Fig. S7A–S7D). Pathway enrich-ment analyses revealed that the downstream effects of hypoxiaand DNA repair defects are partially overlapping (SupplementaryFig. S7E–S7G). This may explain the lack of an endpoint associ-ation within the hypoxic tumor group and points to commonrepair defect sources or downstream signaling effects.
Tumors harboring DNA crosslink repair defects are expected tobe sensitive to cisplatin treatment. Variations in the cumulativecisplatin dose in our patients, as a result of discontinuation due tosystemic toxicities, gave us the opportunity to investigate thishypothesis. The patients were assigned to a high (>200mg/m2) orlow (�200mg/m2) cumulative cisplatin dose group according toprevious reports, resulting in a univariate HR of 2.3 for the low-dose patients (P¼ 0.0014). Overall, patients with predicted DNArepair–defective tumors benefitted most from the high cumula-tive cisplatin dose (Fig. 3C; Supplementary Fig. S8A and S8B).
To consider both the prognostic clinical factors and the hereinuncovered interaction with hypoxia, we combined predictedDNA repair status, hypoxia status, cisplatin dose, and tumor sitein a multivariate model (Fig. 4A). Our analysis shows thatexpression profiles associated with DNA repair defects werestrongly indicative of poor prognosis (HR ¼ 4.01, P ¼0.00091). The interactionbetweenDNA repair andhypoxia status
was also significant in this model (HR ¼ 0.19, P ¼ 0.0066),confirming that hypoxia and DNA repair defects are not additive(Fig. 4A, left). To independently test this poor patient prognosisassociation, we next computed DNA repair defect model scoresfor tumor samples from a second independent cohort with 82patients with advanced and HPV-negative HNSCC who werechemoradiotherapy treated and from which pretreatment mate-rial was collected within the multicenter DESIGN project(characteristics in Supplementary Table S4). This independentvalidation, shown in Fig. 4A (right), confirms that predicted DNArepair defects, as determined by our model ensemble, are signif-icantly associated with poor prognosis (HR ¼ 3.2, P ¼ 0.023).
By splitting the cohorts at their median scores into two equal-sized groups, as is common practice in biomarker studies, theabove analyses stipulate thatDNA repair defects are present inhalfof the HNSCC. Yet there is little support for this suggestion (50%DNA repair–defective tumors). Furthermore, prevalence can alsodiffer between cohorts. To verify that our findings are not biasedby certain cut-off points, we evaluated the multivariate HR at arange of cutoffs (Fig. 4B). The varied cutoffs for repair defect statusassignment are based on the proportion of patients in one or theother category as defined by their model score ranking, resultingin different score cutoffs for both cohorts in this analysis. Doingso, we find that DNA repair defects called by themmcOnlymodelensemble were significantly associated with poor prognosis at abroad range of cutoffs in both the NKI-CRAD cohort and thesecond independent DESIGN cohort.
We next assessed the DNA repair defect/poor prognosis asso-ciation by using the threeClass model ensemble. We find that thisthreeClass model ensemble showed highly similar results, con-firming a DNA repair defect/poor prognosis association and thatit also predicts poor survival in both advanced HNSCC patientcohorts largely independent of the chosen cutoffs (Fig. 4B; Sup-plementary Fig. S9A–S9D). As a comparison, clinical stage wasnot found to be significantly associated with poor survival ineither cohort (Supplementary Fig. S10).
Finally, to further reveal the origin of the poor prognosisassociation and cisplatin responsiveness, we analyzed the asso-ciation with different outcome endpoints. We find little evidencefor a role in locoregional control (Fig. 5A). However, we observedsignificantly increased HRs for the occurrence of distant metas-tasis, in particular in the NKI-CRAD cohort (Fig. 5A), whichsuggests that DNA repair–defective tumors may be more proneto metastasize. As for overall survival (Fig. 3C), this effect wasmost pronounced in normoxic tumors that also metastasize less,unless repair defective (Fig. 5B). Given the lack of endpointassociation in hypoxic tumors, we further investigated the effectof cumulative cisplatin dose in normoxic tumors only. HRs forDNA repair defects were higher in the patient group treated withlow-dose cisplatin at all cutoffs (Fig. 5C and D). Although onlystatistically significant at one cutoff, likely due to low patientnumbers, it points to the benefit of high-dose cisplatin to reducemetastasis occurrence in patients with DNA repair–defectivetumors.
DNA repair defect association with migratory and invasivebehavior
These findings prompted us to explore the link between DNArepair defects andmetastasis in in vitro studies with the confirmedcrosslink repair–impaired HNSCCs.We selected several represen-tative cell lines for each sensitivity class (Normal, SensM, and
Predicting DNA Repair Defects in HNSCC
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5601
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

A B
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Mea
n A
UC
per
mod
el
3f 5f 3f 5f 3f 5f
thre
eCla
ss
mm
cOnl
y
olaO
nly
0.65 0.74 0.78 0.77 0.83
0.7 0.71 0.79 0.79 0.81
0.74 0.81 0.82 0.77 0.75
0.73 0 0 0.83 0.81
0.69 0 0 0.73 0.83
0.7 0 0 0.82 0.83
0.62 0.74 0.75 0.76 0.77
0.68 0.77 0.79 0.78 0.76
0.67 0.77 0.79 0.77 0.78
0.72 0.74 0.8 0.8 0.75
0.69 0.75 0.85 0.84 0.84
0.74 0.76 0.82 0.81 0.81
0.72 0.83 0.9 0.89 0.9
0.64 0.78 0.81 0.8 0.82
0.65 0.79 0.72 0.82 0.82
0.62 0.82 0.76 0.78 0.79
Bor uta_bothBoruta_geneBor uta_sign
coeffVar_bothcoeffVar_genecoeffVar_sign
DESeq2mRMR_both
mRMR_genemRMR_sign
sSVM_IFR_bothsSVM_IFR_genesSVM_IFR_sign
VSURF_bothVSURF_geneVSURF_sign
knn nb
nnet rf
svm
Machine learning classification method
Mac
hine
lear
ning
feat
ure
sele
ctio
n m
etho
d
olaOnlymean(AUC) in 5-fold CV
−4
0
2
4
-2
Normal
SensM
SensMO
mmcOnlyensemble
olaOnlyensemble
Top 253-fold CV
Top 255-fold CV
Select overlap
threeClassensemble
sensM sensMO
mmcOnly9 models
olaOnly13 models
threeClass13 models
Performance ofmachine learning
D E F
sensMmmcOnly olaOnly
Cell lines
Pre
dict
ed p
roba
bilit
yof
DN
A re
pair
defe
ct
Normal
SensM
SensMO
Select bestcombinations
Combinemodels
0.00.10.20.30.40.50.60.70.80.91.0
mm
cOnl
yol
aOnl
yS
ensM
Sen
sMO
AU
C
Performance ofclassic signature
thre
e-C
lass
C
sensMOthreeClass
0.00
0.25
0.50
0.75
1.00
Train modelson full data
0.0
2.5
5.0
7.5
10.0
0 25 50 75 100
Mitomycin C IC50 (nmol/L)
Ola
parib
IC50
(μm
ol/L
)
Normal
SensM
SensMO
Control
Cell linesCell linesCell lines
Cell line group
G
Figure 1.
Generation of gene expression models to detect functional DNA repair defects using machine learning. A, Division of cell lines into three groups, based oncombined mitomycin C and olaparib sensitivity. Cells were grown for at least five doubling times (as determined for each cell line individually and to strengthensurvival and repair outcome data) in a range of concentrations of either compound, after which, the fraction of surviving cells was determined and IC50 valuescalculated (16). The MMC IC50 values of the control cell lines, i.e., normal fibroblast cell line GM388 (gray) and the crosslink DNA repair–defected FA patient-derived fibroblast cell lines EUFA636 and EUFA173 (light gray), were determined concomitantly and provide the reference values for sensitivity classification.These control cell lines were not included in the model generation or further analysis. Error bars, SEM on 3–5 independent experiments. B, Heatmap ofdifferentially expressed genes, combined from the three possible one-on-one comparisons. C, Cross-validation for the traditional signature approach. Cell lineswere randomly divided into three groups, two of which were combined to be the training set and one was used as the test set. Differentially expressed geneswere identified in the training set. For cell lines in the test set, a score was calculated by adding the normalized (center-scaled) expressions of overexpressedgenes and subtracting the expression of under-expressed genes. (Continued on the following page.)
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5602
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

SensMO; described in Fig. 1A). To investigate the link between theobserved metastatic behavior and DNA repair defects, we usedtwo assays to evaluate migratory behavior in these cell lines. Inscratch assays, a confluent layer of cells is scratched and the rate atwhich the remaining cells close the resulting gap is deter-mined (35). In transwell assays, the ability of cells to migratethrough a porousmembrane ismeasured (35).We found that cell
lines that show MMC sensitivity (SensM and SensMO) migratedsignificantly more often and faster than Normal classified celllines in both, the scratch assays (Fig. 6A and B) and transwellmigration assays (Fig. 6C). To evaluate invasive capacity in vitro,both assays were modified by depositing extracellular matrixproteins (Matrigel) in the scratch or on the membrane. Weobserved that in the scratch and transwell invasion assays, the
A
B
AU
C fo
r Mito
myc
in C
sen
sitiv
e
mmcOnlythreeClassSensM+MO
threeClassSensM+MO
threeClassSensMO
threeClassSensM
olaOnly
mmcOnly
Crosslink repairgene set
AUC for mutations AUC for shRNA knockdownC D
0.780.97 0.92 0.62 00.92 1 0.88
0.360.81 0.81 1 00.74 0.75 1
0.861 1 0.44 00.86 1 0.5
0.940.94 0.94 0.47 00.94 1 0.5
0.861 1 0.28 00.86 1 0.44sh
ATM
shA
TR
shC
HE
K1
shC
HE
K2
shB
RC
A1
shR
AD
51
shB
RIT
1
sh53
BP
1
shRNA
Canonical
Others
Crosslinkrepairmutation
None
0.79
0.58
0.79
0.61
0.8
0.72
0.63
0.85
0.6
0.81
cano
nica
l
all
0.00
0.25
0.50
0.75
1.00AUC
−4 −3 −2 −1 0
0.3
0.4
0.5
0.6
0.7
R²= −0.47P = 0.045
Mitomycin C ln(IC50) (μmol/L) Mitomycin C ln(IC50) (μmol/L) Mitomycin C ln(IC50) (μmol/L)
olaOnly
−4 −3 −2 −1 00.1
0.2
0.3
0.4
0.5
0.2
0.4
0.6
R²= −0.53P = 0.020
−4 −3 −2 −1 0
0.3
0.5
0.7 R²= −0.15P = 0.55
mm
cOnl
y
olaO
nly
thre
eCla
ssS
ensM
+MO
0.00.10.20.30.40.50.60.70.80.91.0
Mod
el s
core
Model ensemble
Figure 2.
External validation of model ensemble performance. A, Correlation between HNSCC cell line MMC IC50 values and their model scores in the CGP dataset. For thethreeClass model ensemble, the sum of predicted probabilities for the SensM and SensMO group to predict MMC sensitivity was used, as both these groups areMMC sensitive. Cell lines with reported mutations in crosslink repair pathway genes (Supplementary Table S3; 27 HR/FA genes for the canonical gene set) arehighlighted in red. B, AUC for DNA repair defect prediction of the indicated model ensembles as classified by MMC sensitivity. AUC are shown for a range of IC50
cutoffs (from 20% to 50% of the maximum tested dose; see Supplementary Fig. S4) to avoid reliance on a distinct arbitrary cutoff. C,AUC for detectingmutations in crosslink repair genes in the HNSCC CGP dataset (gene list in Supplementary Table S3).D, Performance of the model ensembles in the Peng andcolleagues dataset (27) to predict DNA damage response and repair defects. Samples treated with shRNA against the respective DNA repair genes wereconsidered defective (n¼ 4 for BRCA1, RAD51, andMCPH1 (BRIT1), n¼ 6 for ATM, ATR, CHEK1, CHEK2, and TP53BP1), while scrambled shRNA (n¼ 3–4) ornontreated samples (n¼ 3; not used in BRCA1, RAD51, and BRIT1 experiments) were considered proficient.
(Continued.) Area under the ROC (AUC) values were then calculated using these scores. This process was repeated with each of the three groups taking the roleof test set, a process known as k-fold cross-validation, with k¼ 3 in this case. Cross-validation was repeated 16 times, resulting in a total of 48 iterations. D,Multiple feature selection methods were combined with multiple machine learning methods to determine which combination performs optimally in predictingDNA repair defect classes in our cell lines. Either gene expression (_gene), signature expression (_sign), or both (_both) were used as input. Displayed AUCvalues are the average of 10 repeats of 5-fold cross-validation for olaOnly models. E,Mean performance values of all 80 possible combinations for the indicatedcross-validations (3-fold or 5-fold). Each box contains all the values for one cross-validation approach (i.e., olaOnly_5f contains all the values shown inD, whereeach combination is a single data point). For threeClass models, the mean AUC of each class versus the rest was reported. F,Overview of the strategy for buildingthe model ensembles. G, Performance in the training set to visualize the distinctive group identification of each model ensemble. Note that all AUCs are 1.
Predicting DNA Repair Defects in HNSCC
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5603
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

SensMOcell lineswere able to invade throughMatrigel, while thiswas not evident in the SensM or Normal cell lines (Fig. 6D–F). Tofurther test whether this is DNA repair defect related, we inhibitedHR/FADNA repair in the repair-proficient Normal cell lines usingthe RAD51 inhibitor B02 for 24 hours. This resulted in stronginduction of migratory (P ¼ 1.49 � 10�5) and invasive behavior(P ¼ 1.8 � 10�6 in ANOVA; Fig. 6G and H), further supporting apossible direct link between DNA repair defects and invasivenessin HNSCC. Interestingly, the quick induction also indicates a lackof a requirement for genetic adaptation. Treatment with equalconcentrations of RAD51 inhibitor was lethal for both SensM andSensMO cell lines (Supplementary Fig. S11), precluding furtherepistasis experiments. These in vitro data support the notionderived from the clinical data that functional FA/HR repairpathway defects are associated with a more aggressive, metasta-sis-prone nature.
Mechanistic links between DNA repair defect and migrationIn search for potential mechanistic links and prompted by the
high specificity in identifyingDNAdamage response deregulationbyATMknockdown (Fig. 2D; Supplementary Fig. S7),we hypoth-
esized that the activation of DNA damage response pathwaysinduces migration. This is in line with our initial position thatunrepaired damage from oxidative and endogenous sourceswould provoke a DNA damage response and accompanyingtranscriptional changes that allows us to identify repair defects.Indeed, ATM depletion was previously reported to reduce migra-tion and invasion. This was shown to occur through IL8 signalingregulated by ATM activation and induced by oxidative stress (36).We find that CXCL8 (IL8) is consistently upregulated in themigrating but not in the invading cell lines (Fig. 7A). Inhibitionof the DNA damage response protein ATM reduced migrationmildly in some cell lines, suggesting that this is not specific to aDNA repair–defective status (Fig. 7B; Supplementary Fig. S12). Asecond key player in the DNA damage response network is theDNA-dependent protein kinase, DNA-PK. DNA-PK has beenshown to promote migration and invasion in prostate cancer,possibly through DNA-PK–mediated gene expressionchanges (37). Others postulated DNA-PK influences invasionand migration through the control of the secretion of multiplemetastasis-associated proteins (38). When tested in our cell lines,DNA-PK inhibition reducedmigration in theBRCA1-mutatedUT-
Hypoxia gene signatures
Hypoxic
Years
Normoxic
Years
YearsYears
Cumulative cisplatin doseO
vera
ll su
rviv
alA C
B
ProficientDeficient
DNA Repair
mmcOnly model ensemble
ProficientDeficient
DNA RepairProficientDeficient
DNA RepairOve
rall
surv
ival
0 1 2 3 4 50.0
0.2
0.4
0.6
0.8
1.0 HR: 1.53 (0.93−2.52)P = 0.092
0 1 2 3 4 50.0
0.2
0.4
0.6
0.8
1.0 HR: 0.74 (0.36−1.5)P = 0.4
0 1 2 3 4 5
HR: 2.83 (1.36−5.86)P = 0.0052
0 1 2 3 4 5
> 200 mg/m²
≤ 200 mg/m²
Cumulative cisplatin dose
ProficientDeficient
DNA Repair
ProficientDeficient ≤ 200 mg/m²
> 200 mg/m²
Log test P = 0.0016
Figure 3.
DNA repair defects are prognostic for chemoradiotherapy-treated HNSCC patients. A,Overall survival of advanced patients with HPV-negative HNSCC (NKI-CRAD cohort) based on DNA repair defect prediction. The patient cohort was divided into two equal-sized groups based on the median mmcOnly modelensemble score. The high scoring group was classified as DNA repair deficient. B, The cumulative cisplatin dose of >200mg/m2 was used to discriminate patientswho received high cisplatin doses from those with less to evaluate the survival association with DNA repair defect prediction. C,mmcOnly model ensembleprediction association with overall survival in patients with hypoxic or normoxic tumors. Insets in A–C show univariate HR and associated P values.
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5604
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

SCC-60B (Fig. 7C; Supplementary Fig. S12A–S12D). Together,our data suggest that DNA-PK activation and IL8 expression–mediated processes may be responsible for the migration of cellswithin the migratory SensM group.
As the invasive SensMO group did not show such mechanisticlinks, we next evaluated the presence of known metastasis-promoting features. Metastasis is partly associated with epitheli-al-to-mesenchymal transition (EMT; ref. 39). DNA damage, suchas induced by radiation, has been reported to promote EMT andmigration in cell lines. We therefore tested whether DNA repair–defective cell lines show mesenchymal characteristics, elongatedcell body, and expression of key transcription factors (40). Inspec-tion by light microscopy revealed that both SensM and SensMOcell lines are more spindle-shaped than Normal cell lines, withSensMO cells showing the most elongated phenotype (P < 10�16
for both; Fig. 7D; Supplementary Fig. S13A). However, whilesome migratory and invasive cell lines exhibited mesenchymalcharacteristics, we did not find consistent differences between thecell line classes for expression of the classical EMT markers orEMT-related signatures (41) when using all cell lines. Assumingrepair-proficient cell linesmay also exhibit EMT (unrelated or notcaused byDNA repair defects), we performed gene set enrichmentanalysis using only the cell lines for whichmigration and invasiondatawere available. EMT-related geneswere significantly enriched(Fig. 7E), pointing to a possible mechanistic role for EMT. Whentesting EMT-related processes (41, 42), we found cell adhesionand migration genes to be enriched (Supplementary Fig. S13B)and most migrating cells to express mesenchymal markers(Supplementary Fig. S13C). EMT and cellular invasive behavioras mediated by TGFb requires SMAD4 (43, 44). SMAD4 loss,
that can cause spontaneous head and neck cancer in mice,however, promotes squamous cell carcinoma metastasis and wasshown to influence metastasis formation in cooperation withE-cadherin in othermodels (45, 46).UsingDNA capture sequenc-ing analysis (16), we find that UT-SCC-24B lacks SMAD4 expres-sion due to a genomic deletion of the first three exons (Fig. 7F andG). This finding links HR/FA repair defects with SMAD4 andinvasive behavior in one of the cell lines.
In conclusion, while we find evidence that repair defects can belinked tomigratory behavior through the engagement of keyDNAdamage response players and their links to migration as reportedby others, mechanisms in the invasive repair-defective class maydepend on genetic context and may be more multifaceted andcomplex.
DiscussionIn this study, we set out to investigate the effect of DNA repair
defects on clinical outcome in HNSCC. We defined DNA repairdefects by functional outcomes, hypersensitivity to DNA-damaging agents, which integrates the proficiency of all DNAdamage response and DNA repair pathways, including adapta-tions that have arisen to any defects in these pathways. Wereasoned that the transcriptome reflects the sum of all failed orsuccessful repair activities on endogenously generated damageand therefore encompasses defects and the activation of backuprepair pathways and other coping mechanisms. Reestablishmentof DNA repair, through compensatory repair activities, is a mech-anism for acquiring treatment resistance (9, 47), which does notrevert genomic scars or mutations, but is presumably reflected in
NKI-CRAD****
**
*
0.2 0.3 0.4 0.5 0.6 0.7 0.8
0
1
2
3
4
5
6
Cutoff used
HR
A
B
HR (95% CI)
mmcOnly
threeClassSensM+MO
P < 0.05 in Multi-variate analysis
0.2 0.3 0.4 0.5 0.6 0.7 0.8Cutoff used
0
1
2
3
4
5
6NKI-CRAD DESIGN
DNA Repair:hypoxia
TumorSite oropharynxTumorSite larynx
Cisplatin lowHypoxia high
DNA Repair deficient
Covariates
Interaction term
HR (95% CI)
****
**
***
1/7
1/6
1/5
1/4
1/3
1/2 1 2 3 4 5 6 7
1/7
1/6
1/5
1/4
1/3
1/2 1 2 3 4 5 6 7
DESIGN
Figure 4.
Independent validation of the prognostic value of the DNA repair defect models. A, Forest plots for multivariate Cox analysis in the NKI-CRAD and the DESIGNHNSCC patient cohorts, showing the DNA repair defect model (mmcOnly ensemble) association with survival in multivariate analyses that also include tumorsite, cumulative cisplatin dose, hypoxia status, and the interaction term between DNA repair defects and hypoxia as indicated. The HRs for patients with tumorsthat are both DNA repair deficient and hypoxic are 2.03 (HRDNA_repair_defect
�HRhypoxia� HRinteraction ¼ 4.01�2.64�0.19) in the NKI-CRAD cohort and
2.12 (¼ 3.24�4.36�0.15) in the DESIGN cohort. � , P < 0.05; �� , P < 0.01; ��� , P < 0.001. B, Repeated multivariate Cox HR analyses in unequally sized patient groupsas indicated on the x-axis. Used cutoffs for the "DNA repair–deficient" group comprised the 85% (left axis) to the 15% (right axis) top scoring patients.Multivariate Cox HR with the same variables as in Fig. 4A are shown on the y-axis for each of these splits andmodel ensemble as indicated. Note that the valuesshown in Fig. 3C correspond to the 0.5 cutoff (dotted gray line). Dots represent HR values with P value under 0.05.
Predicting DNA Repair Defects in HNSCC
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5605
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

the transcriptome. Together, we consider this an important addi-tion to the current arsenal of DNA repair biomarkers.
Our strategy allowed us to investigate the effect of DNA repairdefects in patients with HNSCC. This revealed that patients withtumors predicted to harbor DNA repair defects showed worseoverall survival in two independent patient cohorts. We concludethat they constitute a HNSCC group with a more aggressivebehavior. Hypoxia is known to alter cellular repair capacity andpathway choice and is a poor prognosis biomarker (48).Wefind anoticeable interaction with hypoxia that suggests that, in patientswith hypoxic tumors, prognosis is not further decreased by repairdefects. Hypoxia has been shown to promote metastasis and to
downregulate HR/FA repair processes (49–51). A considerableoverlap in gene expression changes to the tumors with DNArepair defects indicated common repair defect sources or down-stream signaling effects. Alternatively, the models may be unableto predict repair defects in hypoxic tumors, because the modelensembles were generated under nonhypoxic conditions.The RNA expression patterns in the DNA repair defective cellswere likely caused (in part) by oxidative stress. In contrast to ourfindings, in breast, ovarian, and lung cancer, DNA repair defectsin tumors were found to be associated with a favorable prog-nosis, possibly due to the treatment with DNA-damagingagents (52–55). Current treatments for HNSCC may hence not
0.2 0.3 0.4 0.5 0.6 0.7 0.8
02
46
8
Cutoff used
HR
NKI−CRADDESIGNP = 0.095
A
0.2 0.3 0.4 0.5 0.6 0.7 0.8
02
46
8
Cutoff used
HR
NKI−CRADDESIGN
P = 0.056
Dis
tant
met
asta
sis
free
Hypoxia gene signatures
Hypoxic Normoxic
0 1 2 3 4 50.0
0.2
0.4
0.6
0.8
1.0
Years
HR:1.43 (0.48−4.27)P = 0.52
0 1 2 3 4 5Years
HR:5.95 (1.23−28.69)P = 0.026
B
0 1 2 3 4 50.0
0.2
0.4
0.6
0.8
1.0
Years
HR:0.66 (0.12−3.63)P = 0.64
0 1 2 3 4 5Years
HR:6.01 (0.72−49.98)P = 0.097
Hypoxic Normoxic
Proficient (n = 22)Deficient (n = 27)
DNA Repair
Deficient (n = 22)Proficient (n = 27)
DNA Repair
Proficient (n = 11)Deficient (n = 30)
DNA RepairProficient (n = 15)Deficient (n = 26)
DNA Repair
NKI−CRAD
DESIGN
C
01
23
45
67
Normoxic only
Cutoff used
HR
0.2 0.3 0.4 0.5 0.6 0.7 0.8
≥200 mg/m² Cisplatin<200 mg/m² Cisplatin
D
0 1 2 3 4 50.0
0.2
0.4
0.6
0.8
1.0
Years0 1 2 3 4 5
Years
Normoxic≥200 mg/m² Cisplatin
Normoxic<200 mg/m² Cisplatin
Proficient (n = 19)Deficient (n = 14)
HR:5.88 (0.77−44.69)P = 0.087
Proficient (n = 26)Deficient (n = 30)
HR:1.65 (0.46−5.97)P = 0.44
DNA Repair
Dis
tant
met
asta
sis
free
Dis
tant
met
asta
sis
free
Multivariate analysis - distant metastasis
Multivariate analysis - locoregional control
Figure 5.
Association of DNA repair defects with metastasis and cisplatin response. A, Patients were repeatedly divided into two groups with the "DNA repair–deficient"group comprising the top scoring 85% (left) to 15% (right) of patients as based on their predicted probability of DNA repair defects by the mmcOnly modelensemble. Multivariate Cox HR with the same variables as in Fig. 4B are shown on the y-axis for each possible split, with distant metastasis or locoregionalrecurrence as clinical outcome. Dots represent splits where the associated P value was under 0.05. B, Kaplan–Meier plots at best splits (median in NKI-CRAD and0.31 in DESIGN) are shown for DNA repair defects (mmcOnly ensemble) within the hypoxic or normoxic classified tumor patient groups as indicated. Insets showunivariate HR and associated P values. C, HR plots for metastasis occurrence as in A in all patients (combining the NKI-CRAD and DESIGN cohort) according totheir received cumulative cisplatin dose. D, Kaplan–Meier plots showing distant metastasis-free survival in the high or low cumulative cisplatin patient group anddata according to DNA repair status based on the median in all patients with normoxic tumors. Insets show univariate HR and associated P values.
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5606
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

fully exploit the cellular sensitivities of tumors with DNA cross-link repair defects. The apparent increased benefit of high cumu-lative cisplatin dose in our clinical data supports this interpreta-tion. Given the risk, such patients could be candidates for addi-tional systemic treatment with crosslinkers, PARP inhibitors, orother novel therapies targeting such defects.
The in vitromigratory and invasive capacity thatwas exclusive tothe SensMO cell lines confirmed a proposed propensity of tumors
withDNA repair defects tometastasize. In addition,we found thatthe induction of DNA repair defects, in cell lines that wereotherwise repair proficient, results in rapid acquisition of thisinvasive phenotype. This suggests that a direct link and signalingmechanism underlies this effect, rather than genetic contextualadaptations to such repair defects. In line with these findings, arecent study showed that chromosomal instability induces inva-sive behavior through activation of NFkB signaling (25). Others
A*
*
*
**
Time (hours)0 12 24 36 48
0
20
40
60
80
100
Wou
ndde
nsity
(%)
16A1A79A60B1512A1424B20A45
0 12 24 36 480
20
40
60
80
100
Time (hours)
Wou
ndde
nsity
(%)
*
CB
D FE
16A1A79A60B1512A1424B20A45
Migration
Invasion
Normal SensM SensMO
16A 1A 79A
12A 15
60B 14
20A
24B 45
0
5
10
15
20
25
Mig
ratio
n A
UC
Normal SensM SensMO
16A 1A 79A
12A 15
60B 14
20A
24B
0
10
20
30
Mig
rate
d ce
lls (%
)
Normal SensM SensMO
16A 1A 79A
12A 15
60B 14
20A
24B 45
0
5
10In
vasi
on A
UC
Normal SensM SensMO
16A 1A 79A
12A 15
60B 14
20A
24B
0
10
20
30
Inva
ded
Cel
ls (%
)
0
20
40
80
100
0 12 24 36 48
Time (hours)
Wou
nd d
ensi
ty (%
)
Migration
0 12 24 36 48
Time (hours)
ConditionControl
Rad51i
Invasion
0
5
10
15
20
25A
UC
*** ***Control
Rad51 Inhibitor
Cell line16A1A79A
Cell line16A1A79A
60
Migration InvasionG H
Figure 6.
DNA repair–defective cell lines have a strong migratory and invasive phenotype. A,Migration as determined in scratch assays of SensMO (red), SensM (blue), andnormal (green) cell lines. After the scratch was made, cell density in the scratch area was monitored for 48 hours. Values shown are the average of multipleexperiments. B, AUCs over the first 12 hours were determined for the individual independent experiments from A that were performed on separate days and areshown as individual points, with error bars representing SD from the 5 technical replicates. Asterisks point to statistical significances between the groups, asdetermined by linear mixed-effects models. C, Proportion of migrated cells after 24 hours, as determined by transwell migration assays. Individual points
represent independent experiments. Error bars are the SDðsdratio ¼ ffiffiffiffiffiffiffiffiffiffiffiffiffiffiffiffi
s2 þ s2p Þ on the ratios of cell numbers on the bottom to the top of the membranes (n¼ 2–
3). D and E, As inA and B, with the modification that wells were covered with extracellular matrix after the scratch was made. AUCs were calculated over the first24 hours. F, As in C, with the modification that membranes were covered in Matrigel prior to the assay. G,Migration and invasion scratch assays for normal celllines treated with B02. Values shown are the average of multiple experiments. H,AUC for each experiment inG. ANOVAwas used to determine statisticalsignificance using the formula: "� Inhibitor�CellLineþ Experiment"; the interaction term is added to account for cell line–specific response. The P value for theinhibitor is reported.
Predicting DNA Repair Defects in HNSCC
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5607
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

have reported that knockdown of FA genes in HNSCC cell linesresults in increased invasion through activationof theNHEJ repairpathway and via DNA-PK and Rac1 signaling (56). Our DNA-PKinhibition data and differential pathway expression analysessupport the engagement of these migration-promoting mechan-
isms in DNA repair–deficient HNSCC cell lines and provides amechanistic link to a higher propensity to metastasize. DNA-PKactivation–mediated migration is also in line with an increasedengagement ofNHEJ as indicated by thePARP inhibitor resistanceand connects repair defects to the reports from others that show a
0
100
200
300
0100200300 UT-SCC-24B
SMAD4
UT-SCC-60B
Cov
erag
e (#
read
s)
G
B
5 10 5 10 5 10DNAPK Inhibitor NU7026 (μmol/L)
Hallmarks
0
200
400
600
CX
CL8
(IL8
) exp
ress
ion
(RP
KM
)
Normal
SensM
SensMO
12A
14
15
16A
1A
20A
24B
60B
79A
A
D
16A 1A 79A 15 12A 60B 14 24B 20A 45
0.00
0.25
0.50
0.75
1.00
Spi
ndle
inde
x
SensM SensMONormal
−Log10 (q.val)
0 5 10 15
il2_stat5_signalingfatty_acid_metabolism
uv_response_upcomplement
xenobiotic_metabolismuv_response_dn
estrogen_response_earlyadipogenesis
hypoxiapi3k_akt_mtor_signaling
epithelial_mesenchymal_transitiontnfa_signaling_via_nfkb
g2m_checkpointglycolysis
il6_jak_stat3_signalingmyc_targets_v2
unfolded_protein_responseallograft_rejectionmtorc1_signaling
inflammatory_responsee2f_targets
interferon_gamma_responseinterferon_alpha_response
oxidative_phosphorylationmyc_targets_v1
12A 15 60B 14 20A
24B
1.01.52.0
−Log10 (q.val)
UpregulatedDownregulated
E enrichment
SensM SensMOF
** * 79A 60B 14
−25
0
25
50
75
Inhi
bitio
n (%
)
16A 79A 60B 14
−25
0
25
50
75
Inhi
bitio
n (%
)
C
5 10 5 10 5 10ATM Inhibitor KU-55933 (μmol/L)
5 10
SensM SensMONormal SensM SensMONormal
0.0
2.5
5.0
7.5
10.0
SM
AD
4 ex
pres
sion
(RP
KM
)
24B
Figure 7.
Mechanisms linking DNA repair defects to increased migration. A, CXCL8 (IL8) expression levels in the three DNA repair classes (Normal, SensM, SensMO) withpairwise t test. � , P < 0.05; �� , P < 0.01. B,Migration inhibition values (%) from ATM inhibition by KU-55933 as determined in the scratch assay at 12 (triangles) and24 (filled circles) hours in the indicated HNSCC cell lines. Symbols showmean values of individual experiments. C,Migration inhibition values from DNA-PKinhibition by NU-7026 as determined in the scratch assay at 12 (triangles) and 24 (filled circles) hours in the indicated HNSCC cell lines. D, Distributions of spindleindex values in the HNSCC cell lines from the three different DNA repair classes. The spindle index is defined as 1�(width/length), such that a perfectly round cell(width¼ length) has index 0 and increases as cells are more elongated. Data from n¼ 3 independent experiments with 100 cells each are shown. E, Gene-setenrichment analysis using MSigDB hallmarks and comparing the migrating to the normal cell lines. F, SMAD4 expression levels in all analyzed cell lines. G, DNAsequencing read coverage plots in the UT-SCC-24B and UT-SCC-60B, indicating a loss of exons 1–3 in UT-SCC-24B.
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5608
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

role for these proteins in migration, invasion, and metastasis.Consistent with the notion that loss of FA/HR DNA repair mayinduce metastatic behavior, knockdown of BRCA1 and FANCD2was reported to causededifferentiation and induce EMT inhumanmammary epithelial cells in vitro (56). Cells that have undergoneEMT downregulate apoptosis (57) and show increased resistanceto DNA damage (58). At first glance, our data seem inconsistentwith such observations. Upon closer inspection, we find hints ofan increasedmesenchymal phenotype in the gene expression dataand cellular morphology of the invasive cell lines. In recent years,however, it has become clear that cancer cells tend not to be in asolely epithelial or mesenchymal state, but that many interme-diate states exists (59). Also, DNA repair–defective cell lines mayshow a partial EMT phenotype, this as part of a defense mech-anism against further DNA damage and the effects thereof.
In the cell line panel, we observed that invasive behavior andDNArepair defects overlap to a large degree.Considering the recentdata fromBakhoumand colleagues (25), ourdata further support acausal relationship between defective DNA repair that promoteschromosomal instability and migratory behavior. However, giventhis overlap in features, in patient material and based on ourtranscriptome analyses alone, a clear distinction between DNArepair deficiency and the sole and independent presentation ofinvasive features is therefore formally not possible. The associationwith cisplatin response and the inability topredict survival changesin hypoxic samples or to identify all metastasis-prone cases points,however, to repair-defect features in contrast to pure metastasisfeatures. For more accurate identification of tumor DNA repairdefects in individual patients, integration of transcriptomics, geno-mic rearrangements, pathogenic mutations, and phospho-proteomics is desirable. More cohorts of homogenously treatedHSNCC patients, for whom full transcriptomics, genomic data,and carefully recorded clinical data are available, are required tofurther optimize the identification of patients with tumors har-boring DNA repair defects with the purpose to provide alternativetreatment options to this poor prognosis group.
In summary, we find that DNA repair–defective cell lines aremore motile and invasive in vitro and we have developed geneexpression–basedmodels to detectDNA repair defects inHNSCC.Importantly, using these models, we find that these defects areassociated with poor overall survival in two independent patient
cohorts thereby confirming their prognostic value and the detri-mental role of tumor repair defects.
Disclosure of Potential Conflicts of InterestNo potential conflicts of interest were disclosed.
Authors' ContributionsConception and design: P.B.M. Essers, M.W.M. van den Brekel, H. Bartelink,C. VensDevelopment of methodology: P.B.M. Essers, C.V.M. Verhagen, M.W.M. vanden Brekel, C. VensAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): P.B.M. Essers, M. van der Heijden,C.V.M. Verhagen, E.M. Ploeg, R.H. de Roest, C.R. Leemans, R.H. Brakenhoff,H. Bartelink, M. Verheij, C. VensAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): P.B.M. Essers, M. van der Heijden, C.V.M. Verhagen,C.R. Leemans, R.H. Brakenhoff, M.W.M. van den Brekel, C. VensWriting, review, and/or revision of the manuscript: P.B.M. Essers, M. van derHeijden, C.V.M. Verhagen, R.H. de Roest, C.R. Leemans, R.H. Brakenhoff,M.W.M. van den Brekel, H. Bartelink, M. Verheij, C. VensAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): C.V.M. Verhagen, E.M. Ploeg, C. VensStudy supervision: P.B.M. Essers, M.W.M. van den Brekel, M. Verheij, C. Vens
AcknowledgmentsThis research was funded by the EU 7th framework program (257144
ARTFORCE), the Dutch Cancer Society (KWF-A6C7072, DESIGN consortium,to R.H. Brakenhoff, C. Vens, and M. van den Brekel) and the Brunel andVerwelius funds (to C. Vens and M. van den Brekel). We would like to thanktheNKI Genomics Core Facility for performing RNA sequencing, theNKI RHPCfacility for providing computational resources, and the Core Facility-MolecularPathology and Biobank (CFMPB) for collecting and preparing tissue samples.We are thankful for B. Floot's help and the kind gift of UT-SCC lines fromProfessor Reidar Gr�enman (Turku University Hospital, Turku, Finland). Wethank Robert W. Sobol (University South Alabama, Mobile, AL) for reviewingand providing editorial comments.
The costs of publicationof this articlewere defrayed inpart by the payment ofpage charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received November 7, 2018; revised May 16, 2019; accepted September 5,2019; published first September 12, 2019.
References1. Chae YK, Anker JF, Carneiro BA, Chandra S, Kaplan J, Kalyan A, et al.
Genomic landscape of DNA repair genes in cancer. Oncotarget 2016;7:23312–21.
2. Van Den Broek AJ, Schmidt MK, Van 't Veer LJ, Tollenaar RAEM, VanLeeuwen FE. Worse breast cancer prognosis of BRCA1/BRCA2 mutationcarriers: What's the evidence? A systematic review with meta-analysis.PLoS One 2015;10:1–29.
3. Mersch J, Jackson MA, Park M, Nebgen D, Peterson SK, Singletary C, et al.Cancers associated with BRCA1 and BRCA2 mutations other than breastand ovarian. Cancer 2015;121:269–75.
4. Pennington KP, Walsh T, Harrell MI, Lee MK, Pennil CC, Rendi MH,et al. Germline and somatic mutations in homologous recombina-tion genes predict platinum response and survival in ovarian, fal-lopian tube, and peritoneal carcinomas. Clin Cancer Res 2014;20:764–75.
5. RobsonM, ImS-A, Senkus E, XuB,Domchek SM,MasudaN, et al.Olaparibfor metastatic breast cancer in patients with a germline BRCA mutation.N Engl J Med 2017;377:523–33.
6. Lattimore V, Currie M, Lintott C, Sullivan J, Robinson BA, Walker LC.Meeting the challenges of interpreting variants of unknown clinical sig-nificance in BRCA testing. N Z Med J 2015;128:56–61.
7. Watkins JA, Irshad S, Grigoriadis A, Tutt ANJ. Genomic scars as biomarkersof homologous recombination deficiency and drug response in breast andovarian cancers. Breast Cancer Res 2014;16:211.
8. Telli ML, Jensen KC, Vinayak S, Kurian AW, Lipson JA, Flaherty PJ, et al.Phase II study of gemcitabine, carboplatin, and iniparib as neoadjuvanttherapy for triple-negative and BRCA1/2mutation-associated breast cancerwith assessment of a tumor-basedmeasure of genomic instability: PrECOG0105. J Clin Oncol 2015;33:1895–901.
9. Jaspers JE, Kersbergen A, Boon U, Sol W, Van Deemter L, Zander SA, et al.Loss of 53BP1 causes PARP inhibitor resistance in BRCA1-mutated mousemammary tumors. Cancer Discov 2013;3:68–81.
10. Henneman L, van Miltenburg MH, Michalak EM, Braumuller TM, JaspersJE, Drenth AP, et al. Selective resistance to the PARP inhibitor olaparib in amouse model for BRCA1-deficient metaplastic breast cancer. Proc NatlAcad Sci U S A 2015;112:8409–14.
Predicting DNA Repair Defects in HNSCC
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5609
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

11. Jeggo PA, Pearl LH, Carr AM. DNA repair, genome stability and cancer: ahistorical perspective. Nat Rev Cancer 2016;16:35–42.
12. Knijnenburg TA, Wang L, Zimmermann MT, Chambwe N, Gao GF,Cherniack AD, et al. Genomic and molecular landscape of DNA damagerepair deficiency across The Cancer Genome Atlas. Cell Rep 2018;23:239–54.
13. WillersH, Gheorghiu L, LiuQ, Efstathiou JA,Wirth LJ, KrauseM, et al. DNAdamage response assessments in human tumor samples provide function-al biomarkers of radiosensitivity. Semin Radiat Oncol 2015;25:237–50.
14. Bhide SA, Thway K, Lee J, Wong K, Clarke P, Newbold KL, et al. DelayedDNA double-strand break repair following platin-based chemotherapypredicts treatment response in head and neck squamous cell carcinoma.Br J Cancer 2016;115:825–30.
15. Naipal KAT, Verkaik NS, Ameziane N, van Deurzen CHM, Ter Brugge P,Meijers M, et al. Functional ex vivo assay to select homologous recombi-nation-deficient breast tumors for PARP inhibitor treatment. Clin CancerRes 2014;20:4816–26.
16. Verhagen CVM, Vossen DM, Borgmann K, Hageman F, Gr�enman R,Verwijs-JanssenM, et al. Fanconi anemia and homologous recombinationgene variants are associated with functional DNA repair defects in vitro andpoor outcome in patients with advanced head and neck squamous cellcarcinoma. Oncotarget 2018;9:18198–213.
17. Stoepker C, Ameziane N, Van Der Lelij P, Kooi IE, Oostra AB, RooimansMA, et al. Defects in the Fanconi anemia pathway and chromatid cohesionin head and neck cancer. Cancer Res 2015;75:3543–53.
18. Romick-Rosendale LE, Lui VWY, Grandis JR, Wells SI. The Fanconi anemiapathway: repairing the link between DNA damage and squamous cellcarcinoma. Mutat Res 2013;743:78–88.
19. Stingele J, Bellelli R, Boulton SJ. Mechanisms of DNA–protein crosslinkrepair. Nat Rev Mol Cell Biol 2017;18:563–73.
20. Lopez-Martinez D, Liang C-C, Cohn MA. Cellular response to DNAinterstrand crosslinks: the Fanconi anemia pathway. Cell Mol Life Sci2016;73:3097–114.
21. Pommier Y, O'Connor MJ, De Bono J. Laying a trap to kill cancer cells:PARP inhibitors and their mechanisms of action. Sci Transl Med 2016;8:1–8.
22. O'Connor MJ. Targeting the DNA damage response in cancer. Mol Cell2015;60:547–60.
23. Chaudhuri AR, Callen E, Ding X, Gogola E, Duarte AA, Lee JE, et al.Replication fork stability confers chemoresistance in BRCA-deficient cells.Nature 2016;535:382–7.
24. Chandrasekharappa SC, Chinn SB, Donovan FX, ChowdhuryNI, Kamat A,AdeyemoAA, et al. Assessing the spectrumof germline variation in Fanconianemia genes amongpatientswith head andneck carcinomabefore age 50.Cancer 2017;123:3943–54.
25. Bakhoum SF, Ngo B, Laughney AM, Cavallo J-A, Murphy CJ, Ly P, et al.Chromosomal instability drives metastasis through a cytosolic DNAresponse. Nature 2018;553:467–72.
26. Garnett MJ, Edelman EJ, Heidorn SJ, Greenman CD, Dastur A, Lau KW,et al. Systematic identification of genomic markers of drug sensitivity incancer cells. Nature 2012;483:570–5.
27. Peng G, Chun-Jen Lin C, Mo W, Dai H, Park Y-Y, Kim SM, et al. Genome-wide transcriptome profiling of homologous recombination DNA repair.Nat Commun 2014;5:3361.
28. BalmAJM, RaschCRN, Schornagel JH,Hilgers FJM, Keus RB, Schultze-KoolL, et al. High-dose superselective intra-arterial cisplatin and concomitantradiation (radplat) for advanced head and neck cancer. Head Neck 2004;26:485–93.
29. Vossen DM, Verhagen CVM, Gr�enman R, Kluin RJC, Verheij M, van denBrekel MWM, et al. Role of variant allele fraction and rare SNP filtering toimprove cellular DNA repair endpoint association. PLoS One 2018;13:e0206632.
30. Chen EY, Tan CM, Kou Y, Duan Q, Wang Z, Meirelles GV, et al. Enrichr:interactive and collaborative HTML5 gene list enrichment analysis tool.BMC Bioinformatics 2013;14:128.
31. Leemans CR, Braakhuis BJM, Brakenhoff RH. The molecular biology ofhead and neck cancer. Nat Rev Cancer 2011;11:9–22.
32. Al-Mamgani A, de RidderM,Navran A, KlopWM, de Boer JP, TesselaarME.The impact of cumulative dose of cisplatin on outcome of patients withhead andneck squamous cell carcinoma. EurArchOtorhinolaryngol 2017;274:3757–65.
33. Leemans CR, Snijders PJF, Brakenhoff RH. The molecular landscape ofhead and neck cancer. Nat Rev Cancer 2018;18:269–82.
34. van der HeijdenM, de JongMC, Verhagen CVM, de Roest RH, SanduleanuS,Hoebers F, et al. Acute hypoxia profile is a stronger prognostic factor thanchronic hypoxia in advanced stage head and neck cancer patients. Cancers2019;11:583.
35. Justus CR, LefflerN, Ruiz-EchevarriaM, Yang LV. In vitro cellmigration andinvasion assays. J Vis Exp 2014. doi: 10.3791/51046.
36. ChenW, Ebelt ND, Stracker TH, Xhemalce B, Van Den Berg CL, Miller KM.ATM regulation of IL-8 links oxidative stress to cancer cell migration andinvasion. Elife 2015;4:1–21.
37. Goodwin JF, KnudsenKE. BeyondDNA repair: DNA-PK function in cancer.Cancer Discov 2014;4:1126–39.
38. Kotula E, Berthault N, Agrario C, Lienafa M-C, Simon A, Dingli F, et al.DNA-PKcs plays role in cancer metastasis through regulation of secretedproteins involved in migration and invasion. Cell Cycle 2015;14:1961–72.
39. Lamouille S, Xu J, Derynck R. Molecular mechanisms of epithelial–mesenchymal transition. Nat Rev Mol Cell Biol 2014;15:178–96.
40. Koo V, El Mekabaty A, Hamilton P, Maxwell P, Sharaf O, Diamond J, et al.Novel in vitro assays for the characterization of EMT in tumourigenesis.Cell Oncol 2010;32:67–76.
41. Gr€oger CJ, Grubinger M, Waldh€or T, Vierlinger K, Mikulits W. Meta-analysis of gene expression signatures defining the epithelial to mesen-chymal transition during cancer progression. PLoS One 2012;7:1–10.
42. Byers LA, Diao L, Wang J, Saintigny P, Girard L, Peyton M, et al. Anepithelial-mesenchymal transition gene signature predicts resistance toEGFR and PI3K inhibitors and identifies Axl as a therapeutic target forovercoming EGFR inhibitor resistance. Clin Cancer Res 2013;19:279–90.
43. Zhao S, VenkatasubbaraoK, Lazor JW, Sperry J, JinC,CaoL, et al. Inhibitionof STAT3Tyr705 phosphorylation by Smad4 suppresses transforminggrowth factor b-mediated invasion and metastasis in pancreatic cancercells. Cancer Res 2008;68:4221–8.
44. Vincent T, Neve EPA, Johnson JR, Kukalev A, Rojo F, Albanell J, et al. ASNAIL1-SMAD3/4 transcriptional repressor complex promotes TGF-bmediated epithelial-mesenchymal transition. Nat Cell Biol 2009;11:943–50.
45. White RA, Neiman JM, Reddi A, Han G, Birlea S, Mitra D, et al. Epithelialstem cell mutations that promote squamous cell carcinoma metastasis.J Clin Invest 2013;123:4390–404.
46. Park JW, Jang SH, ParkDM, LimNJ,DengC, KimDY, et al. Cooperativity ofE-cadherin and Smad4 loss to promote diffuse-type gastric adenocarcino-ma and metastasis. Mol Cancer Res 2014;12:1088–99.
47. Sakai W, Swisher EM, Karlan BY, Agarwal MK, Higgins J, Friedman C, et al.Secondary mutations as a mechanism of cisplatin resistance in BRCA2-mutated cancers. Nature 2008;451:1116–20.
48. Bristow RG, Hill RP. Hypoxia and metabolism: hypoxia, DNA repair andgenetic instability. Nat Rev Cancer 2008;8:180–92.
49. Chan N, Pires IM, Bencokova Z, Coackley C, Luoto KR, Bhogal N, et al.Contextual synthetic lethality of cancer cell kill based on the tumormicroenvironment. Cancer Res 2010;70:8045–54.
50. Rankin EB, Giaccia AJ. Hypoxic control of metastasis. Science 2016;352:175–80.
51. Bindra RS, Schaffer PJ, Meng A, Woo J, Ma�seide K, Roth ME, et al. Down-
regulation of Rad51 and decreased homologous recombination inhypoxic cancer cells down-regulation of Rad51 and decreased homol-ogous recombination in hypoxic cancer cells. Mol Cell Biol 2004;24:8504–18.
52. Vollebergh MA, Lips EH, Nederlof PM, Wessels LFA, Wesseling J, vd VijverMJ, et al. Genomic patterns resembling BRCA1- and BRCA2-mutatedbreast cancers predict benefit of intensified carboplatin-based chemother-apy. Breast Cancer Res 2014;16:1–13.
53. Wang ZC, Birkbak NJ, Culhane AC, Drapkin R, Fatima A, Tian R, et al.Profiles of genomic instability in high-grade serous ovarian cancer predicttreatment outcome. Clin Cancer Res 2012;18:5806–15.
54. Kang J, D'Andrea AD, Kozono D. A DNA repair pathway-focused score forprediction of outcomes in ovarian cancer treated with platinum-basedchemotherapy. J Natl Cancer Inst 2012;104:670–81.
55. Pitroda SP, Pashtan IM, Logan HL, Budke B, Darga TE, Weichselbaum RR,et al. DNA repair pathway gene expression score correlates with repair
Essers et al.
Cancer Res; 79(21) November 1, 2019 Cancer Research5610
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

proficiency and tumor sensitivity to chemotherapy. Sci TranslMed 2014;6:229ra42.
56. Romick-Rosendale LE, Hoskins EE, Privette Vinnedge LM, Foglesong GD,Brusadelli MG, Potter SS, et al. Defects in the Fanconi anemia pathway inhead and neck cancer cells stimulate tumor cell invasion through DNA-PKand Rac1 signaling. Clin Cancer Res 2016;22:2062–73.
57. Kurrey NK, Jalgaonkar SP, Joglekar AV, Ghanate AD, Chaskar PD, Doi-phode RY, et al. Snail and slug mediate radioresistance and chemoresis-
tance by antagonizing p53-mediated apoptosis and acquiring a stem-likephenotype in ovarian cancer cells. Stem Cells 2009;27:2059–68.
58. De Jong MC, Ten Hoeve JJ, Gr�enman R, Wessels LF, Kerkhoven R, Te RieleH, et al. Pretreatment microRNA expression impacting on epithelial-to-mesenchymal transition predicts intrinsic radiosensitivity in head andneck cancer cell lines and patients. Clin Cancer Res 2015;21:5630–8.
59. Nieto MA, Huang RYYJ, Jackson RAA, Thiery JPP. Emt: 2016. Cell 2016;166:21–45.
www.aacrjournals.org Cancer Res; 79(21) November 1, 2019 5611
Predicting DNA Repair Defects in HNSCC
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388

2019;79:5597-5611. Published OnlineFirst September 12, 2019.Cancer Res Paul B.M. Essers, Martijn van der Heijden, Caroline V.M. Verhagen, et al. Repair Defects and Poor Prognosis in HNSCCDrug Sensitivity Prediction Models Reveal a Link between DNA
Updated version
10.1158/0008-5472.CAN-18-3388doi:
Access the most recent version of this article at:
Material
Supplementary
http://cancerres.aacrjournals.org/content/suppl/2019/09/12/0008-5472.CAN-18-3388.DC1
Access the most recent supplemental material at:
Overview
Visual
http://cancerres.aacrjournals.org/content/79/21/5597/F1.large.jpgA diagrammatic summary of the major findings and biological implications:
Cited articles
http://cancerres.aacrjournals.org/content/79/21/5597.full#ref-list-1
This article cites 58 articles, 17 of which you can access for free at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/79/21/5597To request permission to re-use all or part of this article, use this link
on June 1, 2020. © 2019 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 12, 2019; DOI: 10.1158/0008-5472.CAN-18-3388