Embed Size (px)
Citation preview
1
Unit 1 ©2014 Barkley & Associates
Advanced Pharmacology:
Thomas W. Barkley, Jr., PhD, ACNP‐BC, FAANPPresident, Barkley & Associates
www.NPcourses.comand
Professor of NursingDirector of Nurse Practitioner ProgramsCalifornia State University, Los Angeles
Advanced Introductory Principles
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Drug Information Resources
2
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Drug Information Resources & Literature Retrieval
60 million US adults use search engines daily
60% of adults search for health-related information
Patients rely on the internet for health and drug information
Skill of the researcher is essential in getting the best information
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Technology has brought drug information to health care providers as well as patients
Clinical decision should never be made from reading an abstract
Critical evaluation of the literature is a prerequisite of providing evidence based care
Many institutions and ambulatory care centers utilize clinical decision support to maximize patient care
Drug Information Resources & Literature Retrieval
3
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Search Engines
Do NOT rely on a single source of drug information
Wikipedia is NOT peer reviewed and does not always provide valid/reliable drug information
Search engines are “vastly” different and employ simple “logic” to search data
Google Scholar not designed to be comprehensive
More reliable databases (MEDLINE and PubMed) are preferred for researching drug information
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Resources for PractitionersPubMed
(www.ncbi.nlm.nih.gov)
Compilation of more than 21 million articles. Many articles are linked to full-text references.
Clinical Evidence
(www.clinicalevidence.com)
Evidence-based medicine database that provides grade levels to help put evidence into practice
US Food and Drug Administration (FDA)
(www.fda.gov)
Provides information on food, drugs, medical devices, vaccines, blood and biologics, animal and veterinary products, cosmetics, radiation-emitting products and tobacco products. Consumer and professional information. Safety recalls.
National Cancer Institute
(www.cancer.gov)
Provides unbiased information on the treatment of cancer including clinical trials, cancer statistics, research and funding and patient information
4
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Resources for ConsumersDailyMed(www.dailymed.nlm.nih.gov)
Provides high quality information about marketed drugs, including FDA-approved labeling. Provides easy-to-read product labeling
Drugs A to Z(www.drugs.com/drug_information.html)
Easily searched database to look up drugs, both generic and band name, to find consumer information that can help patients understand their medications including risks and benefits
Mayo Clinic(www.mayoclinic.com/)
High-quality health information written by professionals specifically for consumers. Provides a wealth of unbiased information
WebMD(www.webmd.com)
Provides consumer health-related information written and edited by health care professionals. Allows users to create programs like vaccine trackers and food & fitness planners
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Locating Clinical Practice GuidelinesGuideline.gov(www.guideline.gov)
National guideline clearinghouse of evidence-based guidelines. Large database of different guidelines form may professional organizations. Provides expert commentaries guideline synthesis, guideline resources, annotated bibliographies and comparative analysis of guidelines
American College of Physicians(www.acponline.org/clinical_information/guidelines/)
Provides current clinical guidelines as part of the American College of Physicians web site. Clearinghouse of clinically relevant guidelines
Open Clinical(www.openclinical.org/guidelines.html)
International organization that created a Web site to promote clinical decision support tools, clinical workflow and advanced knowledge management technologies within patient care as well as clinical research
5
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
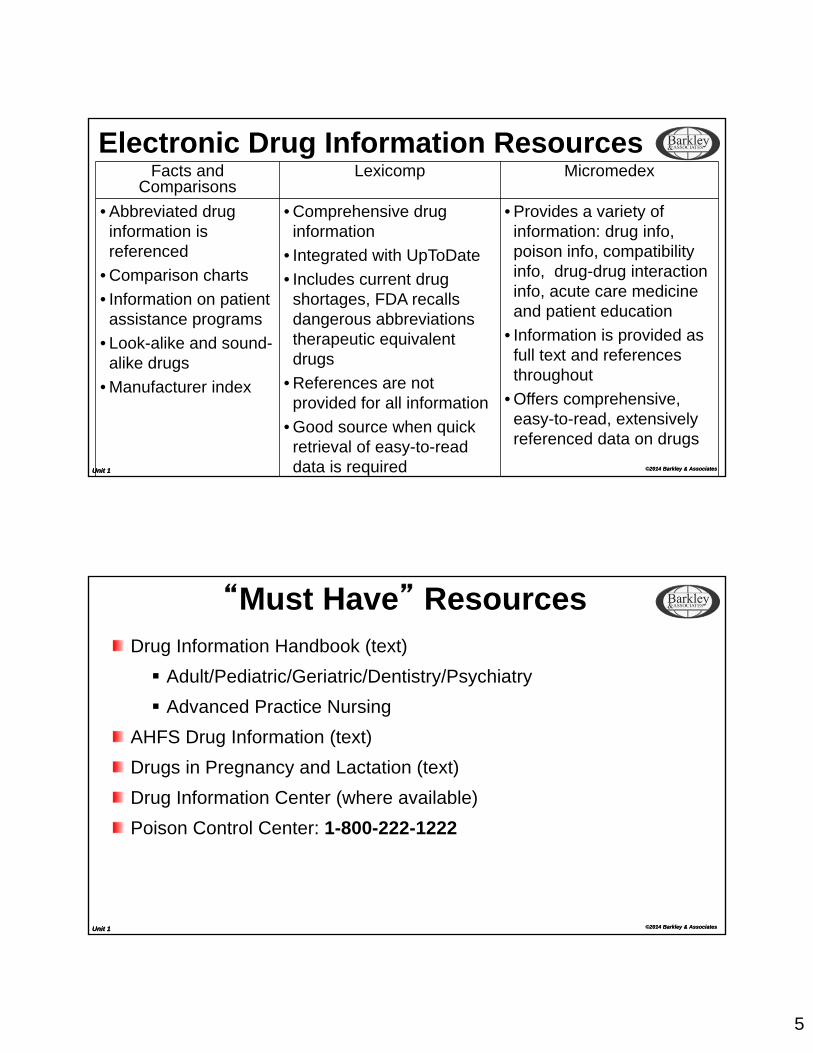
Electronic Drug Information ResourcesFacts and
ComparisonsLexicomp Micromedex
• Abbreviated drug information is referenced
• Comparison charts
• Information on patient assistance programs
• Look-alike and sound-alike drugs
• Manufacturer index
• Comprehensive drug information
• Integrated with UpToDate
• Includes current drug shortages, FDA recalls dangerous abbreviations therapeutic equivalent drugs
• References are not provided for all information
• Good source when quick retrieval of easy-to-read data is required
• Provides a variety of information: drug info, poison info, compatibility info, drug-drug interaction info, acute care medicine and patient education
• Information is provided as full text and references throughout
• Offers comprehensive, easy-to-read, extensively referenced data on drugs
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
“Must Have” ResourcesDrug Information Handbook (text)
Adult/Pediatric/Geriatric/Dentistry/Psychiatry
Advanced Practice Nursing
AHFS Drug Information (text)
Drugs in Pregnancy and Lactation (text)
Drug Information Center (where available)
Poison Control Center: 1-800-222-1222
6
Unit 1 ©2014 Barkley & Associates
Advanced Introductory Principles
http://pedseast.chsys.org/images/x8webtop_images/photos/prescription%20drugs.jpg
Unit 1 ©2014 Barkley & Associates
PharmacologyHistory can be traced to 3000 B.C., where the Babylonians recorded “prescriptions” on clay
Chinese recorded Pen Tsao (Great Herbal), a compilation of plant remedies ~2700 B.C.
PHARMACOLOGY is derived from two words: Pharmakon = “medicine” Logos = “study”
A. Paracelus: “All things are poisons, for there is nothing without poisonous qualities. It is only the dose which makes a thing a poison…a lot kills, a little cures.”
7
Unit 1 ©2014 Barkley & Associates
History in Drug Regulation
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Important History in Drug Regulation1906: Pure Food and Drug Act Government given the power to control the labeling
Prohibited mislabeling, as well as adding extraneous, improper or inferior ingredients to drugs
1914: Harrison Narcotic Act Regulated importing, manufacturing, the sale and use of opium,
cocaine and marijuana
Superceded by the Controlled Substances Act of 1970
8
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
1938: Food, Drug, and Cosmetic Act Passed by Congress; first law preventing marketing of drugs not
thoroughly tested Yet, did not require proof of effectiveness
1952: Durham-Humphrey Amendments Separated drugs into prescription (legend) and
nonprescription/over-the-counter (non-legend) categories. “Legend” must appear on every commercial container of legend
drugs: “ Caution Federal Law Prohibits Dispensing without Prescription”
Additional legend rules
Important History in Drug Regulation
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
1962: Kefauver-Harris Amendments Required proof of efficacy and safety before any new drug could
be placed on the market
Included guidelines for conducting clinical trials
1970: Comprehensive Drug Abuse Prevention and Control Act (Controlled Substances Act) Established rehabilitation programs for drug users
Established control (registration) and enforcement (DEA)
Regulates export/import of controlled substances
Important History in Drug Regulation
9
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
1970: Poison Prevention Packaging Act Regulated that certain household products must be packaged in a
manner to make it significantly difficult for children < 5 years of age to open
Child-resistant containers apply to:All controlled drugs
All legend drugs except:
SL nitroglycerin
Oral contraceptives in dispenser packs
Aspirin and most aspirin-containing preparations
Iron-containing drugs and most dietary supplements
http://www.guide4living.com/images/medication.jpg
Important History in Drug Regulation
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
1976: Medical Devices Act Required proof of both safety and efficacy before marketing of
medical devices for human use
1984: Drug Price Competition and Patent Restoration Act Allowed patent protection to be extended for five years, yet not to
exceed 14 years post-FDA approval
Established Abbreviated New Drug Application (ANDA) procedures for generic copies of drugs
Important History in Drug Regulation
10
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
1987: Prescription Drug Marketing Act Prohibited sale, purchase or trade of drug samples Intent was to curb drug diversion (i.e., use of prescription drugs for
recreational purposes)
1988: FDA officially established as an agency of the United States Department of Health and Human Services (USDHHS)
1990: Omnibus Budget Reconciliation Act New requirements/regulations:
States’ participation in the Medicaid programDrug utilization review (DUR) development Counseling of patients
Important History in Drug Regulation
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
1992: Prescription Drug User Fee Act
Required non-generic and biologic manufacturers to pay fees for improved drug review processes
1994: Dietary Supplement Health and Education Act
Required clear labeling of dietary supplements
FDA given power to remove supplements that cause significant risk
Important History in Drug Regulation

11
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Important Healthcare Regulation2010: Affordable Care Act Puts consumers back in charge of their health care
“Patient’s Bill of Rights”
Ends pre-existing condition exclusions for children
Ends arbitrary withdrawals of insurance coverage
Guarantees patient’s right to appeal
Ends lifetime limits on coverage
Insurance companies must now publicly justify any unreasonable rate hikes
Covers preventive care at no cost to the patient
Unit 1 ©2014 Barkley & Associates
Stages of Drug Development and Approval
12
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Stages of Drug Development and ApprovalDiscovery Chemical modification of known drugs Screening of natural products for activity Rational drug design based on known molecular mechanisms
Preclinical Investigation: Safety and Toxicity Testing Always done in animals – usually rodents – then data are extrapolated to
humans Range: 1-3 years Investigates:
Acute, subacute and chronic toxicityReproductive function effectsCarcinogenicityMutagenicityTeratogenicity
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Notice of Claim Investigational Exemption for New Drug (IND):Three phases of clinical trials
Requires informed consent Requires approval of FDA, organization sponsoring the IND and the
Institutional Review Board (IRB) of trial site
Phase 1 Healthy volunteers
Establish dose range limits
Observe for safety of tested doses
Preliminary pharmacokinetic data
Stages of Drug Development and Approval
13
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Phase 2 Tests patients with disease states Safety and efficacy are examined
Phase 1 and 2 testing are usually conducted in White men. Female differences? Pregnant women?
Phase 3 Evaluation in much larger numbers of patients Multi-center trials Actual use conditions Efficacy and broader range toxicity are explored
Stages of Drug Development and Approval
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
New Drug Application (NDA) Full reports of all preclinical and clinical data FDA review
Phase 4 Approval for marketing Monitor safety under actual conditions of usage
Post-marketing Surveillance Adverse affects Reactions Reports
Stages of Drug Development and Approval
14
Unit 1 ©2014 Barkley & Associates
What’s in a name?
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Drug NamesChemical Name: assigned by the International Union of Pure and Applied Chemistry (IUPAC) using standard nomenclature
Generic name: assigned by the U.S. Adopted Name Council Only one generic name for each drug! Learn THIS one!! Usually written lower case
Trade name: assigned by a company for marketing Usually, short and easy to remember Caution: Many similar names + sound alike, etc. Drug developers have 17 years of exclusive rights to name and market
after being submitted to the FDA After 17 years, a competing company may sale a generic equivalent
(after FDA approval)
15
Unit 1 ©2014 Barkley & Associates
Federal Drug Classification and Schedules
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Federal Drug Classificationand Schedules
Schedule IAbuse potential: HighestLimited or no accepted medical use in U.S.Investigational drugsExamples: Opiates: heroin, many synthetic derivatives Hallucinogens: lysergic acid diethylamide (LSD) Marijuana Methaqualone (Quaalude)
16
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
U.S. Drug Schedules - continuedSchedule IICurrently accepted medical use in U.S.Abuse potential: High Physical dependence Psychological dependence
Examples: Opiates/narcotics: opium, cocaine (topical anesthesia), codeine,
hydrocodone (alone), meperidine (Demerol), methadone (Dolophine), morphine (MS Contin, Duramorph), pentazocine (Talwin Injection), oxycodone (OxyContin, Percocet, Tylox), hydromorphone (Dilaudid), fentanyl, others
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Schedule II: Examples (continued) Stimulants: amphetamine (Benzedrine), dextroamphetamine
(Dexedrine), methamphetamine (Ritalin)
Note: Schedule II stimulants may not be used as anorexiants in many states.
Valid uses: narcolepsy, hyperkinesis, brain dysfunction, severe depression, etc.
Depressants: intermediate-acting barbiturates [e.g., amobarbital (Amytal), pentobarbital (Nembutal), secobarbital (Seconal)], others
U.S. Drug Schedules - continued
17
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Rules for prescribing Schedule II drugs: Written prescription required with prescriber’s actual (legal)
signature
Must be dated the same day as signed
*No refills allowed
In some states for emergency situations, a verbal order may be given for a limited quantity of drug to treat the emergency condition
Must be followed by a written prescription within 72 hours
U.S. Drug Schedules - continued
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Schedule IIIAbuse potential: ModerateRules for Schedule III prescriptions: Written or verbal prescriptions are allowed Valid for 6 months from the date written Refill limit: 5 times
Examples: Narcotic analgesics/antitussives: codeine and some derivatives in
combination with non-narcotic analgesicscodeine/acetaminophen (Tylenol #3)hydrocodone/acetaminophen (Lortab)pentazocine/acetaminophen (Talacen)Paregoric (camphorated opium tincture)
Anabolic steroids Some non-barbiturate sedative-hypnotics Some stimulants used as anorexiants for obesity
U.S. Drug Schedules - continued
18
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Schedule IVAbuse potential: LowSame prescription rules as Schedule III
Examples: Benzodiazepines
Diazepam (Valium)Lorazepam (Ativan)
Zolpidem (Ambien) Carisoprodol (Soma)
U.S. Drug Schedules - continued
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Schedule V
Abuse potential: Lowest
Examples:
Over-the-counter medications, including those with codeine
Purchase subject to state regulations – may differ
General Rule for Controlled Substances: Classifications determined by the State Board of Health, but may not be classified in lower schedules than federal law permits
U.S. Drug Schedules - continued
19
Unit 1 ©2014 Barkley & Associates
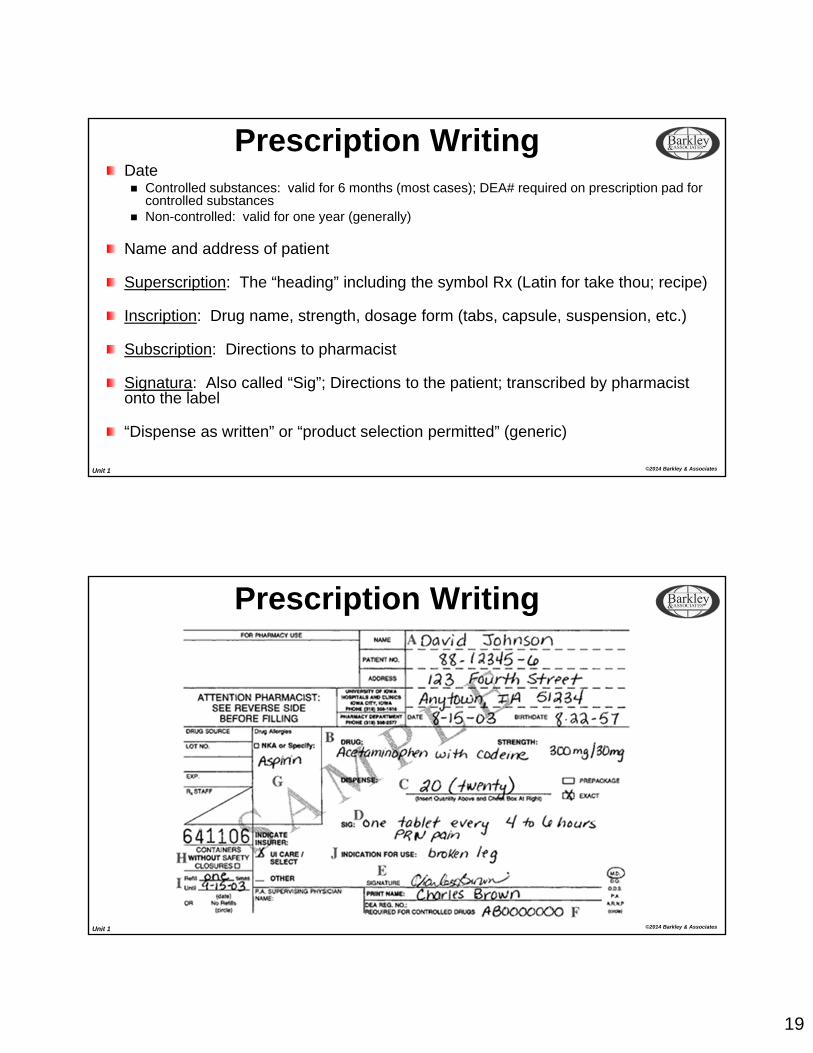
Prescription WritingDate Controlled substances: valid for 6 months (most cases); DEA# required on prescription pad for
controlled substances Non-controlled: valid for one year (generally)
Name and address of patient
Superscription: The “heading” including the symbol Rx (Latin for take thou; recipe)
Inscription: Drug name, strength, dosage form (tabs, capsule, suspension, etc.)
Subscription: Directions to pharmacist
Signatura: Also called “Sig”; Directions to the patient; transcribed by pharmacist onto the label
“Dispense as written” or “product selection permitted” (generic)
Unit 1 ©2014 Barkley & Associates
Prescription Writing
20
Unit 1 ©2014 Barkley & Associates
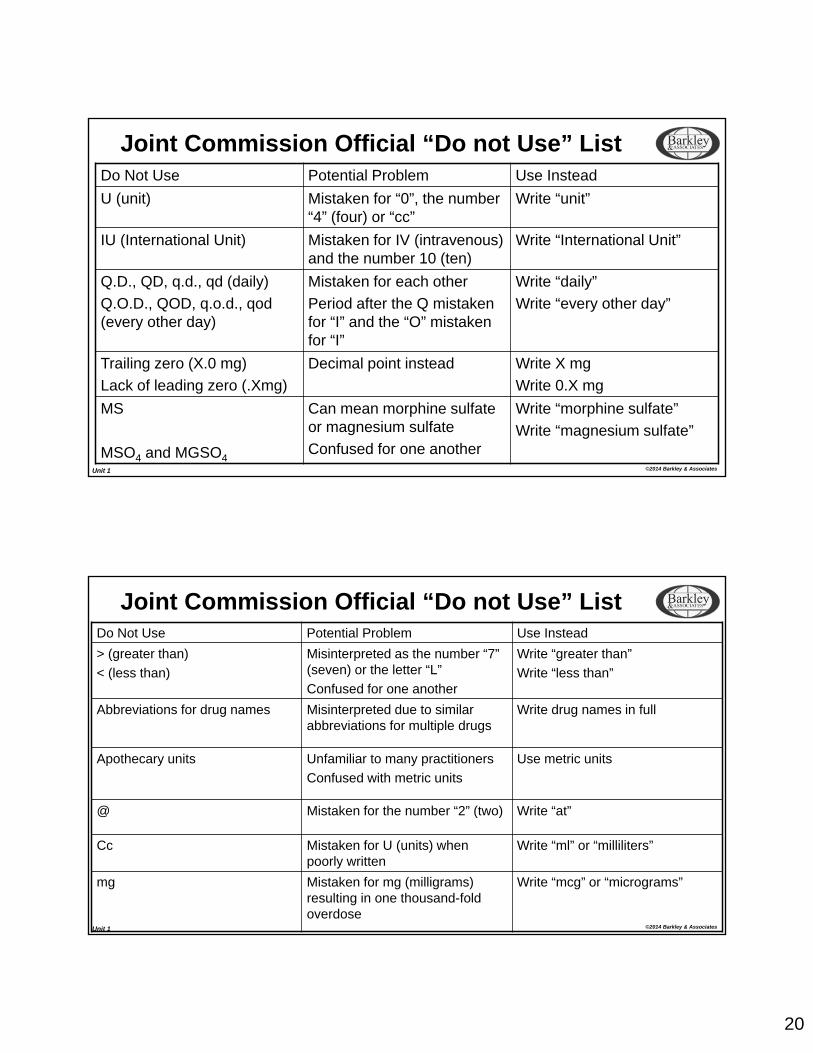
Joint Commission Official “Do not Use” ListDo Not Use Potential Problem Use Instead
U (unit) Mistaken for “0”, the number “4” (four) or “cc”
Write “unit”
IU (International Unit) Mistaken for IV (intravenous) and the number 10 (ten)
Write “International Unit”
Q.D., QD, q.d., qd (daily)
Q.O.D., QOD, q.o.d., qod (every other day)
Mistaken for each other
Period after the Q mistaken for “I” and the “O” mistaken for “I”
Write “daily”
Write “every other day”
Trailing zero (X.0 mg)
Lack of leading zero (.Xmg)
Decimal point instead Write X mg
Write 0.X mg
MS
MSO4 and MGSO4
Can mean morphine sulfate or magnesium sulfate
Confused for one another
Write “morphine sulfate”
Write “magnesium sulfate”
Unit 1 ©2014 Barkley & Associates
Do Not Use Potential Problem Use Instead
> (greater than)
< (less than)
Misinterpreted as the number “7” (seven) or the letter “L”
Confused for one another
Write “greater than”
Write “less than”
Abbreviations for drug names Misinterpreted due to similar abbreviations for multiple drugs
Write drug names in full
Apothecary units Unfamiliar to many practitioners
Confused with metric units
Use metric units
@ Mistaken for the number “2” (two) Write “at”
Cc Mistaken for U (units) when poorly written
Write “ml” or “milliliters”
mg Mistaken for mg (milligrams) resulting in one thousand-fold overdose
Write “mcg” or “micrograms”
Joint Commission Official “Do not Use” List
21
Unit 1 ©2014 Barkley & Associates
Phases of Drug Action
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Phases of Drug ActionA. Pharmaceutical Phase Pharmaceutics – physicochemical properties of drugs Design and manufacture of dosage formulations
B. Pharmacokinetic Phase Biopharmaceutics
LiberationAbsorptionDistributionMetabolism (biotransformation)Excretion
PharmacokineticsPhysiological modelsDesign and individualization of dosage regimens
22
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
C. Pharmacodynamic Phase
Pharmacology: interaction of drugs with tissue and cells Target sites of drugs: Receptors
D. Therapeutic Phase
Clinical pharmacology
Therapeutic and/or toxic effects of drugs
Phases of Drug Action
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
PharmacokineticsLiberation (of drug from dosage form) Extends from the time of drug administration to the time the drug is
dissolved in body fluids and ready for absorption
Immediate liberation: Parenteral
Exceptions: Long-acting, slow-release suspension formulas for IM or SQ
use (e.g., PCN G, insulins (except Regular), etc.Solutions that may precipitate [(e.g., phenytoin (Dilantin)]
Dosage-form dependent liberation: Topical Oral dosage forms (depend on the number of pharmaceutical
barriers to drug release)
23
Unit 1 ©2014 Barkley & Associates
Liberation: Oral Dosage Forms (continued)
Solution, elixir, syrup Already dissolved; no barriers to
release
Suspension Particles must completely dissolve
for release to occur Dissolution is the rate-limiting
(slowest) step in drug liberation from solid oral forms
Capsule Disruption – outer gelatin capsule
(rapid) Dispersion – of a powder Dissolution – of particles
Tablet Disintegration of granules to a
powder
Dispersion – of a powder
Dissolution – of particles
Coated tablet Dissolution of the coat
Others same as tablets
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacokinetics: AbsorptionAbsorption Process of drug movement from the absorption site across one or
more cell membrane barriers in the circulation
Mechanisms:Passive diffusionFacilitated diffusionActive transportPinocytosis
24
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Passive Diffusion The most common mechanism
Involves the movement of drug from its absorption site across a cell membrane barrier in the direction of the concentration gradient (driving force)
The drug moves from an area of higher concentration (e.g., GI lumen) to an area of lower concentration (e.g., the blood)
Movement of drug across lipid membranes is favored for the non-ionized form of the drug
The non-ionized form is the more lipid-soluble form and can more easily dissolve in and pass through biologic membranes
Ability of drug molecules to pass through biologic membranes depends on the drug’s partition coefficient (Kp), which is a measure of a drug’s ability to dissolve in a lipid phase compared to an aqueous phase
In general, the higher the Kp for a drug, the better will be its extent and rate of absorption.
Absorption Mechanism: Passive Diffusion
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Facilitated DiffusionSame principles as passive diffusion but, in addition…
A carrier molecule (usually a membrane protein) is required.
Drug at the absorption site combines with the carrier at the membrane surface, transported across the membrane, and then released. This process does not require energy.
Drug movement occurs only in the direction of the concentration gradient and for only as long as a concentration gradient exists.
Absorption Mechanism: Facilitated Diffusion
25
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Active Transport
Carrier-mediated transport process
Requires energy
Movement of drug occurs against the concentration gradient
The carrier system can become saturated so that the rate of drug transport reaches a maximum level.
The carrier has specificity for certain drugs with proper chemical structures
Absorption Mechanism: Active Transport
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pinocytosis
A portion of the cell membrane that surrounds the drug breaks off, and moves into the cell where drug is released
May be significant for extremely large drug molecules
Polypeptides, proteins, etc.
Absorption Mechanism: Pinocytosis
26
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Drug Absorption Sites
EnteralOralRectalSublingual
Parenteral Intravenous IntramuscularSubcutaneous
TopicalPercutaneousEyeLung
Unit 1 ©2014 Barkley & Associates
Drug Absorption: Oral/IntestinalGI epithelial cell membrane barrierSmall intestine – major site for drug absorption (huge surface area)Gastric emptying/intestinal motility (physiological factors) affecting drug absorption Rate-limiting step in oral
absorption
Increased emptying:Large fluid volumesCholinergicsGI pro-kineticsCathartics/laxatives
Decreased emptying:Solid foods – especially fatty, acidic or high in electrolytesAlcoholAntacidsAnticholinergicsNarcoticsDrugs with anticholinergic side effects (antidepressants, antihistamines)
http://www.integris-health.com/ih/layouts/digestive/smallIntestine2.jpg
27
Unit 1 ©2014 Barkley & Associates
Absorption Mechanism: First-pass EffectFirst-pass Effect
“Presystemic metabolism”During GI track drug absorption, there are two potential sites for metabolism to occur: Gut wall Liver
If the drug is chemically altered as it passes through either of these sites (metabolized), it is said to undergo first-pass metabolism.Effectively, the drug has been metabolized before it ever reaches the systemic circulation. Some drugs are so extensively metabolized when taken orally that therapeutic
effects cannot be obtained (e.g., lidocaine) Oral doses must be very large for some drugs compared to parenteral
http://www.boomer.org/c/p1/Ch07/Diag07.jpg
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Absorption Mechanisms (continued)Rectal Epithelial cell membrane Highly vascularized Lower and middle hemorrhoidal veins drain directly into the inferior
vena cava First-pass effects may be partially avoided if a drug can be
liberated and absorbed by the rectum
Sublingual Thin epithelial mucosal barrier Eliminates first-pass effects Requires rapid drug dissolution
28
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Intravenous No drug absorption barrier Immediate absorption and drug availability
Intramuscular/Subcutaneous Capillary endothelial cell membrane barrier Blood flow to the site: rate-limiting step
Percutaneous Thick epithelial barrier Outer layer of epidermis (stratum corneum) is the rate-limiting step
Absorption Mechanisms (continued)
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Eye Epithelial mucous membrane barrier
Absorption is greatly dependent on drop size
Lungs Thin epithelial mucous membrane barrier
Highly vascularized
Rapid absorption
Very large surface area
Aerosols/inhalers may not be used efficiently
As particle size decreases, absorption increases
Absorption Mechanisms (continued)
29
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacokinetics: DistributionDistribution Patterns: Plasma
Uniform into body water
Tissue concentrations
Non-uniform: depending on plasma, affinity of binding sites, lipid solubility and perfusion
Distribution Barriers: Blood-brain barrier (BBB)
Placental barrier
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacokinetics: MetabolismMetabolisms/Biotransformation:
Chemical alteration of a drug by enzymes in the body
Purposes of drug metabolism:
Detoxification mechanism (defense)
Termination of drug action
Major sites of drug metabolism:
Gut
Liver
Plasma
30
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacokinetics: ExcretionMajor routes:
Kidney
Bile (via enterohepatic circulation) fecal excretion
Pulmonary
Milk
Saliva
Renal excretion involves three processes:
Glomerular filtration (only free drug is filtered)
Active tubular secretion (proximal tubule)
Passive tubular reabsorption (from the proximal tubule)
Unit 1 ©2014 Barkley & Associates
Pharmacodynamics:
How drugs interact IN the body…within cells, tissues and organs
31
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
PharmacodynamicsReceptor Theory of Drug Action
Receptor: portion of tissue or cell capable of interacting with a drug with resulting pharmacologic effects
Chemical composition of receptors Membrane macromolecules (mostly proteins, lipids) Intracellular macromolecules ( proteins, nucleic acids) Enzymes
Receptors evolved for the purpose of reacting withendogenous compounds Drugs that resemble these endogenous compounds may also react with the
receptor
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Agonist (full agonist) Drug which interacts with a receptor to produce a pharmacologic response that is the same response produced by the endogenous compound Terbutaline (adrenergic agonist drug) reacts with adrenergic receptors in the
bronchioles to produce bronchodilation (same effect as produced by the endogenous agonist, epinephrine)
Partial Agonist Drug which can interact with a receptor but produces a much weaker
pharmacologic response than a full agonist
AntagonistDrug which interacts with a receptor to block the actions of the endogenous agonist Phenoxybenzamine (adrenergic receptor antagonist) reacts with adrenergic
receptors in blood vessels to block the actions of norepinephrine (endogenous agonist)
Drug-Receptor Interactions
32
Unit 1 ©2014 Barkley & Associates
Properties of Drug-Receptor Interactions:
AffinityEfficacyPotency
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Affinity
Measure of a drug’s ability to interact with a receptor
Drug + Receptor D-R complex
Agonist: high affinity
Antagonist: high affinity
Partial agonist: low affinity
Properties of Drug-Receptor Interactions
33
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Properties of Drug-Receptor Interactions
EfficacyMeasure of a drug’s ability to produce apharmacologic response after interactingwith a receptor
D-R complex Response
Agonist: high efficacy Antagonist: zero efficacy Partial agonist: low efficacy
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Potency
Measure of the dose of a full agonist
required to produce the maximum
pharmacologic response.
If drugs A and B are both agonists, and drug A produces the maximum response at a lower dose than drug B, then drug A is more potent than drug B.
Properties of Drug-Receptor Interactions
34
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Toxicology PrinciplesDefinitions:
Effective dose 50 (ED50) Dose which produces a desired therapeutic effect in 50% of test subjects
Lethal dose 50 (LD50) Dose which is lethal to 50% of test subject
Therapeutic index (TI) Ratio of the LD50 to the ED50
TI = LD50 / ED50A very low value of TI means that there is small difference between the doses of a drug which produce therapeutic vs. lethal effects
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Drug AllergiesGenerally not dose-relatedFour types of allergic responses Type I:
Allergic reactions to stings and drugsSymptoms range from mild rash to life-threatening anaphylaxisOnset is immediate
Type II:Autoimmune reactions to drugs
Type III:Serum sickness, vasculitis
Type IV: Contact dermatitis from topical application
Adverse Drug Reactions (ADRs)
35
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Side effects Unwanted effects of drugs that appear at normal doses required for
a therapeutic response
Toxicity Unwanted effects of drugs that appear as drug dosage is increased
beyond the dose required for a therapeutic response
Adverse Drug Reactions (ADRs)
Unit 1 ©2014 Barkley & Associates
Pharmacology: Practical Principles for Clinical Use
36
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacology: Practical Principlesfor Clinical Use
Pharmacokinetics The study of drug movements within an organism, particularly the
rate of such movements, as affected by absorption, distribution, metabolism, and excretion (ADME); “the art of pharmacotherapeutics”
“What the body does to the drug” Clinically, pharmacokinetics influences how much drug to give a
patient, and how often to dose.
Standard Parameters of Pharmacokinetics1. Clearance (CL)2. Volume of Distribution (Vd)3. Half-life
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Clearance (CL): The volume of fluid cleared of drug per unit of time. Total clearance is the sum of renal and non-renal (primarily hepatic) routes of
elimination.
Volume of Distribution (Vd): Fictitious proportionality constant between the total amount of drug in the body
and the concentration of the drug in the plasmaA low volume of distribution indicates that a drug remains mostly within the circulatory system.A high volume of distribution indicates that the drug is widely disseminated to various compartments, although it provides no information concerning the specific tissues in which a drug may be concentrated.
Vd is highly dependent on certain properties of the drug, particularly protein binding.
Pharmacology: Practical Principlesfor Clinical Use
37
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Half-life (t1/2):
If a drug follows so-called first order elimination processes, the half-life (t1/2) represents the time required for 50% of the drug dose to be removed from the body.
If the drug is being administered on a routine basis and steady state, a relatively constant plasma concentration occurs after approximately 4-5 half-lives have elapsed.
For most drugs, once administration is discontinued, the drug is eliminated in about 7 half-lives.
Pharmacology: Practical Principlesfor Clinical Use
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
The Plasma Concentration- Time Curve and AUCSingle Dosing Regimens: Typical plasma concentration-time curves after intravenous
administration of a single dose show that upon infusion, drug concentration in the serum increases rapidly to peak, then gradually declines as the drug is distributed to peripheral tissues and is removed from the body.
The area under the curve (AUC) is a pharmacodynamicparameter that represents the exposure of receptor to the drug.
The AUC is the single best predictor of clinical efficacy.This is particularly the case (and best documented) for the anti-infective drugs.
Pharmacology: Practical Principlesfor Clinical Use
38
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
For effective drug levels:
A larger dose of the drug could be given at the same dosing interval
The same dose could be administered more frequently or
A similar drug with longer half-life could be used
The second or third options are the most favorable as increasing dose may increase side effects.
If the second option is used, consideration should be given as to whether increasing dosing frequency may decrease compliance.
Pharmacology: Practical Principlesfor Clinical Use
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Multiple Dosing Regimens:
Used to maintain drug serum concentration levels at a steady state.
As the drug is distributed to tissues or is metabolized and excreted, its levels decrease in the serum.
To maintain efficacy, the drug must be dosed again in the appropriate time interval (determined by the half-life of the drug).
Pharmacology: Practical Principlesfor Clinical Use
39
Unit 1 ©2014 Barkley & Associates
Bioavailability and BioequivalenceBioequivalence:
Compares different dosage forms of the same drug to determine if these reach the same AUC.
Particularly important when comparing generic versus “trade name” drugs
Bioavailability describes how much of the drug is available to interact with it receptor after dosing.
With I.V. dosing, bioavailability is 100%.
Bioavailability shifts markedly in PO forms of drugs.
In this case, the drug is first absorbed via the portal circulation into the liver where a large fraction of it may be metabolized before it reaches the systemic circulation.
This “first-pass” effect determines the amount of drug per dose.
For several drugs, the first-pass effect is significant enough to markedly increase the oral dose versus the IV dose.
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacology:Practical Principles for Clinical Use
Protein Binding
A highly (90%) protein bound drug can have three different outcomes:
- decreased drug activity
- effects on tissue distribution
- effects on elimination
A highly bound drug is usually clinically ineffective, as only unbound drug can diffuse from the capillaries into the interstitial space of tissues where it works.
Only unbound drug can interact with receptors due to the “lock and key” fit drug molecules have with their specific receptors.
Protein binding also may affect elimination. Only unbound drug is filtered at the glomerulus, so protein binding slows elimination and prolongs half-life. Some protein bound drugs are actively secreted off of their plasma proteins into the proximal tubule. This effect usually negates the slowing of filtration of these drugs at the glomerulus.
40
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
PharmacodynamicsPharmacodynamics:
The study of drug action at the receptor level
“What the drug does to the body”
A drug needs to bind to receptor molecules on or in a cell with sufficient avidity to disrupt normal cellular functions.
Drug receptors on or in cells are linked to biochemical processes in that particular cell.
Four types:
Receptor-operated ion channels
G Protein-linked receptors
Enzyme receptors
DNA-linked receptors
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Pharmacodynamics: Drug ReceptorsReceptor-operated ion channels: Binding of an agonist opens these channels, and antagonists prevent opening. Receptors include those for ACH (nicotinic), GABA, Glycine, 5 Hydroxytryptamine (5-HT)
and Purine. Effects at these receptors are seen within milliseconds.
G Protein-linked receptors: At rest, these receptors exist, linked in a complex fashion, to guanosine diphosphate
(GDP). When an agonist binds to the receptor, GDP is converted to GTP, which activates the G
protein complex. The result is a change in enzyme systems, including those that make cyclic nucleotides
(including cAMP), inositol phosphate or diacylglycerol. Cyclic AMP formation results in increased lipolysis, decreased glycogen synthesis,
increased glycogen breakdown and increased calcium currents and release from the SR of cardiac cells.
Agonists at these receptors include autonomic agents such as epinephrine, norepinephrine, isoproterenol, etc.
Inositol phosphate and DAG formation result in a number of cellular processes. Effects at these receptors are seen within seconds.
41
Unit 1 ©2014 Barkley & AssociatesUnit 1 ©2014 Barkley & Associates
Enzyme receptors: One of the most common is tyrosine kinase. When an agent binds to this enzyme, growth and metabolism are
affected. Guanylyl cyclase is another enzyme receptor found in cardiac atria. Effects at these receptors are seen within minutes.
DNA-linked receptors: These are nuclear proteins that are intracellular. Agonists must be lipid soluble to get across the cell membrane to
interact with these receptors. Once in the nucleus, they may regulate protein expression. These agents take longer to work because of this mechanism –
effects are seen over a period of hours.
Pharmacodynamics: Drug Receptors
Unit 1 ©2014 Barkley & Associates
Homework: Important TriviaWhat are “red flag” drugs in relation to therapeutic index?
Provide examples.
Why specifically do some drugs potentially work differently based on one’s race/ethnicity?
What is the difference between a drug and a medication?
Do generic drugs work the same as all others? Discuss.
Describe the CYP450 system. Define polymorphisms, inhibition and induction.
Locate the Top 100 (Medicare) drug list and the Top 200 drug list. Identify specific agents, and note similarities of each list.
What is the Wal-Mart $4 drug list? How does it work? Give examples.
42
Unit 1 ©2014 Barkley & Associates
What is the difference between side effects and adverse effects? Give two examples.
Differentiate between the four types of Medicare benefits. Contrast differences in Medicare and Medicaid. Identify how much Medicare reimbursement a nurse practitioner may receive in collaboration with a supervising physician?
What does “highly protein bound” mean clinically? Give two examples.
What are the top prescribed drugs in the United States? How many are there? Name at least 10.
What is the difference between prescribing and furnishing medications?
In California, how does a nurse practitioner obtain the privilege to furnish medications? What are the requirements? Outline the procedure.
Homework: Important Trivia
Unit 1 ©2014 Barkley & Associates
The End

















![Therapeutic Class Overview Androgens (testosterone)testosterone)_2015-0812.pdf · Micromedex® Healthcare Series [database on the Internet]. Greenwood Village (CO): Thomson Micromedex;](https://img.pdfslide.us/doc/110x75/5dd141ddd6be591ccb64f9dc/therapeutic-class-overview-androgens-testosterone-testosterone2015-0812pdf.jpg)











