Embed Size (px)
Citation preview
at the university skin clinic of Heidelberg.]J Dtsch Dermatol Ges 2006;4:308–18. InGerman.
19 Mahmud E, Brocato M, Palakodeti V,Tsimikas S. Fibromuscular dysplasia ofrenal arteries: percutaneousrevascularization based on hemodynamicassessment with a pressure measurementguidewire. Catheter Cardiovasc Interv2006;67:434–7.
20 Laforet P, Eymard B. [Exercise-intoleranceand exercise-induced rhabdomyolysis:etiology and diagnosis.] Review. RevNeurol (Paris) 2004;160:217–23. In French.
21 Mora Palma FJ, Ellis HA, Cook DB et al.Osteomalacia in patients with chronicrenal failure before dialysis ortransplantation. Q J Med 1983;52:332–48.
170 Clinical Medicine Vol 7 No 2 April 2007
CME Neurology
Drug-induced neurological disorders(DINDs) are important because earlyrecognition and drug withdrawal canprevent irreversible damage. This reviewdeals specifically with the recognisedneurological complications of prescrip-tion-only, single-agent therapy, either atrecommended doses or in excess(including overdose and abuse of pre-scription drugs), and summarises themore important DINDs. Some of thedrugs described may also exacerbate neu-rological disorders that are oftensubclinical and undiagnosed. Druginteractions can increase the toxicity of
single agents; these are well documentedelsewhere.1
DINDs can occur at initiation, duringsudden withdrawal of therapy (eg tram-adol withdrawal seizures) and after manymonths or years of therapy (eg valproateencephalopathy). Treatment is primarilyconcerned with controlled withdrawal,but toxic levels may necessitate haemo-dialysis or haemofiltration (eg lithium),specific neutralising therapies (eg Fabfragments in digoxin toxicity) or sympto-matic treatments.
Recent detailed and comprehensivereviews of DINDs can be foundelsewhere.2,3
Seizures
Seizures may be caused by antipsychotics,antidepressants, antineoplastic agents(alkylators, antimetabolites, vinca alka-loids, ifosfamide and cisplatin), peni-cillins, cephalosporins, quinolones,antimalarials, aminophylline and allop-urinol. They are frequently observed indrug-induced encephalopathy (seebelow). Other less frequently reporteddrugs which may induce seizures include
Mark R Baker MA MB BChir PhD MRCP,
Specialist Registrar, Department of
Neurology, Royal Victoria Infirmary,
Newcastle upon Tyne
Don J Mahad MB ChB PhD MRCP, Specialist
Registrar and Wellcome Trust Intermediate
Fellow, Mitochondrial Research Group,
School of Neurology, Neurobiology and
Psychiatry, Medical School, Newcastle upon
Tyne
Clin Med 2007;7:170–6
Drug-induced disorders of the
nervous system
Prescription drugs are an important reversible cause of common neurologicaldisorders
Mitochondrial toxicity is an important mechanism in a number of drug-inducedneurological disorders (DINDs)
Early recognition of DINDs and drug withdrawal can prevent irreversible damage
Some DINDs require urgent symptomatic treatment to avoid serious complications
Vitamins and essential trace elements may help to reverse some DINDs
Statin-induced neurological disorders are likely to become more prevalent
Increasing use of novel humanised monoclonal antibodies may cause previouslyunrecognised DINDs
Key Points
KEY WORDS: antiretrovirals, drug-induced disorders, mitochondrion, monoclonalantibodies, nervous system, statins
Clinical Medicine Vol 7 No 2 April 2007 171
CME Neurology
opioids, baclofen, digoxin, dopaminergicagents, thyroxine and ondansetron.4
Drug-induced cerebrovasculardisease
Mechanisms of drug-induced cere-brovascular disease are outlinedschematically, with examples, in Fig 1.Antihypertensives and arrhythmogenicagents can cause focal ischaemia, partic-ularly in the elderly, with right shiftedautoregulation and underlying athero-sclerotic arterial stenoses.2 Cancerchemotherapy may cause thrombo-embolism, haemorrhage, vasopasm orvasculitis; probably because of the synergistic actions of factors secreted bythe tumour or products of tumour lysis.In contrast to primary vasculitis, drug-induced cerebral vasculitis (Fig 2)involves small arteries and is charac-terised by polymorphonuclear leucocyticinfiltrates without giant cells or granulo-mata, marked necrosis and markedintimal involvement.
Headache
Drugs that cause headache usually do soby exacerbating pre-existing migraine,tension headache or chronic daily
headache. Analgesics, including thoseused to treat headache, may also causethe analgesic overuse syndrome seenmost commonly in frequent use ofopiate-based analgesia. Drugs used in thetreatment of other medical conditionswhich can cause headache include anti-depressants, H1- and H2-antagonists,antifungals, antihypertensives, beta-blockers, sulphonamides, intravenousimmunoglobulin (IVIg) and oral con-traceptive pills (OCPs).
One special cause of headache, usuallyassociated with visual disturbance andpapilloedema, is idiopathic intracranialhypertension (IIH). Tetracyclines,retinoids, corticosteroids, oestrogenreceptor agonists and antagonists, non-steroidal anti-inflammatory drugs,growth hormone, cimetidine, nalidixicacid, trimethoprim-sulfamethoxazole,amiodarone and lithium are all associatedwith IIH.
Fig 1. Mechanisms of drug-induced cerebrovascular disease. APA = drug-inducedantiphospholipid antibodies; COCP = combined oral contraceptive pill; HIT = heparin-induced thrombocytopenia.
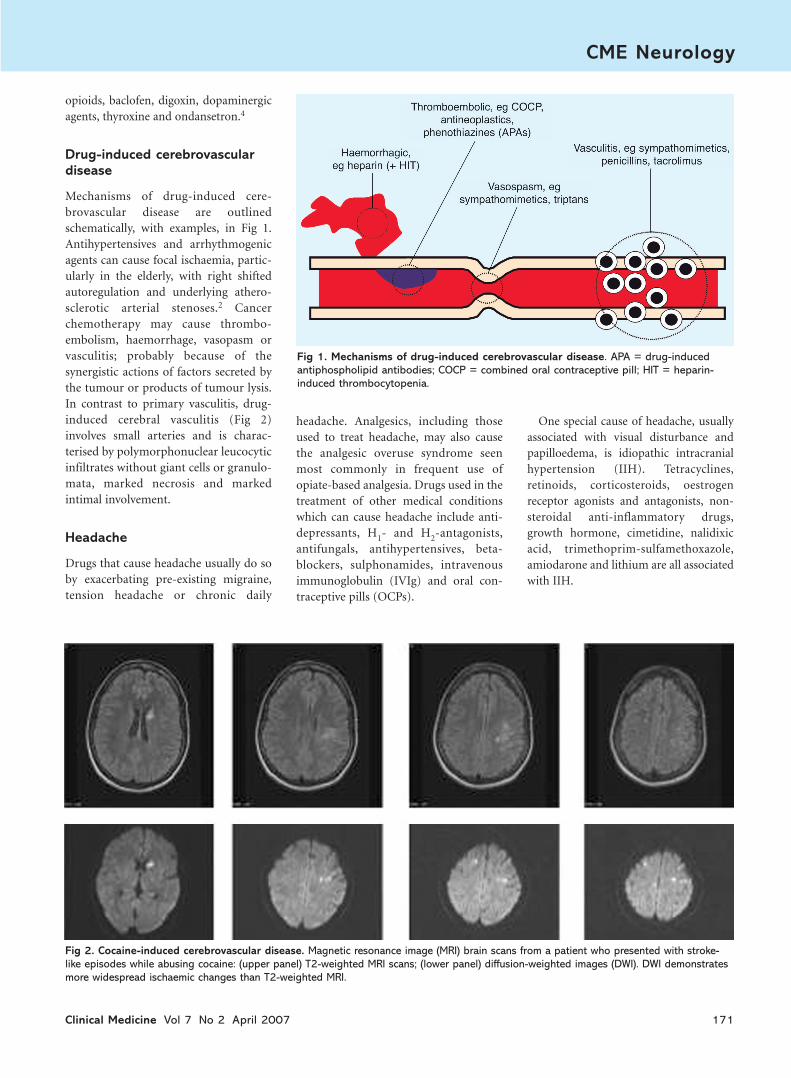
Fig 2. Cocaine-induced cerebrovascular disease. Magnetic resonance image (MRI) brain scans from a patient who presented with stroke-like episodes while abusing cocaine: (upper panel) T2-weighted MRI scans; (lower panel) diffusion-weighted images (DWI). DWI demonstratesmore widespread ischaemic changes than T2-weighted MRI.

Encephalopathy
Drugs that cause encephalopathy andcoma do so either by inducing metabolicdisturbances (eg hepatic, hypoglycaemic,hyponatraemic or uraemic encephalo-pathy) or by direct central nervoussystem (CNS) toxicity (eg anti-epilepticdrugs (AEDs), cephalosporins, peni-cillins, IVIg). Drug-induced coma mostcommonly occurs at toxic serum concen-trations of drug, typically after overdose(eg tricyclic antidepressants (TCAs),opiates, benzodiazepines, AEDs).
Posterior reversible leukoencephalopathy(PRLE) (Fig 3) is associated with seizuresand hypertension and commonly occursin transplant patients treated withciclosporin or tacrolimus. Other drugsknown to cause PRLE include aciclovir,amphotericin B, cisplatin, cytarabine,ifosfamide, and methotrexate.
Dementia
Anticholinergics, antihypertensives (egcalcium channel blockers, adrenergicagents), AEDs (sodium valproate,
phenytoin, lamotrigine), antipsychotics,benzodiazepines, corticosteroids,cytokines (eg interleukins, interferon(IFN)-α) and desferrioxamine can allcause a reversible condition resemblingdementia.
Extrapyramidal disorders
Drug-induced symmetrical akinetic rigidsyndromes are thought to result frommonoamine oxidase dysregulation andchronic dopamine depletion after pro-longed treatment with phenothiazines,haloperidol, TCAs, metoclopramide,lithium and cinnarizine. Hyperkineticsyndromes may be the result of druginteractions with dopamine transporterproteins. Acute dystonia-dyskinesia(including oculogyric crisis) iscommonly caused by antipsychotics,TCAs, AEDs and metoclopramide.Choreo-athetosis is sometimes seen withbenzhexol, neuroleptics and OCPs. TCAsand antipsychotics can both cause rest-less leg syndrome, while dextroampheta-mine, methylphenidate and haloperidolcan cause motor tics.
Drug withdrawal is the first step butacute symptomatic treatment is also oftenrequired (eg iv procyclidine, benztropineor diphenhydramine and iv benzo-diazepines in oculogyric crisis). Tardivedyskinesia, which develops after pro-longed treatment with phenothiazines,thioxanthines, butyrophenones, diben-zepines, diphenylbutylpiperidines andmetoclopramide, can be irreversible. Itmay be prevented by concomitant treat-ment with vitamin E, but the evidence isweak.5 Patients in whom tardive dyski-nesia develops should be converted toalternative antipsychotic medication(eg sulpiride). Symptomatic treatmentscan also be used (eg tetrabenazine).Patients may complain of akathisia whentreated with phenothiazines, butyrophe-nones, TCAs, L-dopa and monoamineoxidase inhibitors (MAOIs); if severe andpersistent, it can be treated with anti-cholinergics, amantadine or propranolol.6
Cerebellar disorders and tremor
Drug-induced cerebellar syndromes areoccasionally irreversible and can be
172 Clinical Medicine Vol 7 No 2 April 2007
CME Neurology
Fig 3. Posterior reversible leukoencephalopathy (PRLE). Fluid attenuatedinversion recovery (FLAIR) magnetic resonance image (MRI) sequences obtainedfrom a patient treated with intravenous aciclovir who developed PRLE: (a) and (b)the extent of white matter change during treatment with aciclovir; (c) and (d) similarMRI sections obtained during the recovery phase after stopping aciclovir. Classically,MRI changes observed in PRLE are limited to the distribution of the posteriorcirculation and resemble the MRI appearance of hypertensive encephalopathy. PRLEis usually, but not always, associated with hypertension and seizures.
(a) (c)
(b) (d)

caused by AEDs, phenothiazines,MAOIs, thioxanthines, lithium andciclosporin. Treatment with theo-phylline, thyroxine, phenothiazines,butyrophenones, amiodarone, adri-amycin, cimetidine, terfenadine, lithium,ciclosporin or tacrolimus can sometimescause postural and kinetic tremor.Resting tremor is occasionally caused bysodium valproate.
Myoclonus
TCAs, lithium, antipsychotics, dopamineand dopaminergic agonists can all causemyoclonus. Myoclonus persisting afterdrug withdrawal or reduction can betreated with clonazepam, sodiumvalproate, piracetam or levetiracetam,but an alternative diagnosis should beconsidered.7
Eye movement disorders
The most common DIND of eyemovements is nystagmus. Horizontalphasic nystagmus can be caused bybenzodiazepines, AEDs, MAOIs, salicy-lates, fenfluramine, TCAs and ototoxicantimicrobials, while downbeatnystagmus is caused by lithium. Externalophthalmoplegia (with absent vestibulo-ocular reflex) is sometimes seen withTCAs, barbiturates, carbamazepine(overdose) and phenytoin. Occasionally,benzodiazepines, fenfluramine, lithiumand fluorouracil can cause internuclearophthalmoplegia.
Cranial neuropathies
Cytosine arabinoside, ciclosporin andganciclovir can all induce abducenspalsies, but the last two have beendescribed only following allogeneic bonemarrow transplantation. Immunologicalreactions are likely to explain the occur-rence of sulfasalazine, insulin-likegrowth factor-1, didanosine, and HBVvaccine-induced facial palsies. There areseveral reports of recurrent laryngealpalsy with vincristine chemotherapy,usually in association with peripheralneuropathy; if severe, it can requiretracheal intubation. Early withdrawal oftherapy is essential to ensure recovery.
Special senses
Vision
Blurred vision is a common side effect ofmedication. Examples of the morecommon, more serious and occasionallyirreversible causes of visual impairmentare given in Fig 4(a). Note that agentsknown to cause PRLE can also causecortical blindness.
Ototoxicity
Ototoxic agents are categorised accordingto vestibular or cochlear toxicity. Putativemechanisms of hair cell toxicity areidentified (Fig 4(b)) by abbreviations inparenthesis (mechano-electrical trans-
duction (MET), mitochondria (mt) andmembrane potential (V)).
Smell and taste
DINDs of smell and taste can often becorrected by administering zinc andmagnesium supplements and phospho-diesterase inhibitors (PDIs) (eg theo-phylline, caffeine). Both zinc andmagnesium are essential to olfactory andgustatory receptor function; many drugsthat cause disorders of smell and tastemay act by depleting such trace metals.PDIs increase intracellular cyclic adeno-sine monophosphate levels which areimportant for intracellular signal trans-duction in both smell and taste.2
Clinical Medicine Vol 7 No 2 April 2007 173
CME Neurology
Fig 4. Drug-induced neurological disorders affecting (a) vision and (b) hearing.Possible mechanisms include mechano-electrical transduction (MET), mitochondria (mt)and membrane potential (V). LGN = lateral geniculate nucleus; OCP = oral contraceptivepill; TCA = tricyclic antidepressant.

Drug-induced disorders ofspinal cord and peripheralnervous system
Figure 5 provides examples of drugs thatcan be toxic to the peripheral nervoussystem and spinal cord, and indicatestheir sites of toxicity. Drugs that inducesubacute myelo-optico-neuropathy arethought to do so by depleting vitamins(particularly B vitamins and vitamin E)or by inhibiting their intracellular co-factors (copper and zinc dependent).Drug-induced neuropathies can bedemyelinating (D), axonal (A) or mixed(M) with elements of axonal loss anddemyelination. There is little evidence tosupport specific treatments for drug-induced neuropathies (except drug with-drawal), but B vitamins, glutathione andzinc supplements should be considered.2
Drug-induced neurologicaldisorders associated with threeincreasingly commonly usedtherapies
Three commonly used therapies associ-ated with DINDs are:
• statins
• antiretroviral agents, and
• humanised monoclonal antibodies(MAb).
Statins
The frequency of statin-induced neuro-logical disorders is likely to increase inthe UK because of their availability off-prescription. The major statin-inducedneurological disorders are myopathy andsmall fibre neuropathy.
Mild myopathic symptoms (eg myalgia)
have been reported by 5–7% of patientstaking statins. The incidence of severemyotoxicity is 0.44–0.54 per 10,000patient-years.7 Fortunately, myopathyusually resolves once the statin is with-drawn. Severe myotoxicity typicallypresents as a necrotising myopathy withproximal weakness and myalgia. In moresevere situations there is rhabdomyolysiswith the concomitant risks of renal failure.
The incidence of statin-inducedneuropathy is approximately 0.3 per10,000 patient-years.8 It can present upto two years after starting treatment.Clinical features include distal lowerlimb dysaesthesia and anaesthesia, prox-imal and distal weakness, and fascicula-tions. In one case series, the neuropathyresolved in 58% of cases after stoppingstatin therapy.9
Mitochondrial toxicity has been impli-cated in the pathogenesis of both statin-induced myopathy and neuropathy (seebelow). Statins increase the ratio oflactate to pyruvate, an indirect indicationof mitochondrial dysfunction. Cyto-chrome oxidase-negative fibres andragged red fibres, hallmarks of mito-chondrial myopathy, are seen in musclebiopsy specimens from patients withstatin-induced myopathy.10 Statins blockthe synthesis of ubiquinone (coenzymeQ10), an electron-transfer carrier essen-tial to mitochondrial function, whichmight suggest one putative mechanism.
Antiretrovirals
The estimated adult HIV prevalence inthe UK is approximately 53,00011 with asignificant proportion of HIV-positiveindividuals treated with highly activeantiretroviral therapy (HAART). Nucleo-side analogue reverse transcriptaseinhibitors (NRTIs) are an essential com-ponent of HAART in HIV. NRTIs causedeath and dysfunction of highly energydependent cells in the nervous systemand muscle, manifesting as peripheralneuropathy (eg zalcitabine) or myopathy(zidovudine), by inhibiting mito-chondrial polymerase gamma andmitochondrial DNA replication (Fig 6).This causes mitochondrial DNAdepletion and mutations, oxidative stressand programmed cell death.12
174 Clinical Medicine Vol 7 No 2 April 2007
CME Neurology
Fig 5. Drug-induced disorders of spinal cord and peripheral nervous system. Theymay be axonal (A), demyelinating (D) or mixed (M). Abs = antibodies; SMON = subacutemyelo-optico-neuropathy; TNF = tumour necrosis factor.

Clinical Medicine Vol 7 No 2 April 2007 175
CME Neurology
Immune reconstitution inflammatorysyndrome (IRIS) is a recognised compli-cation of HAART in HIV. In IRIS there isa paradoxical deterioration of clinicalstatus (eg appearance of progressivemultifocal leukoencephalopathy) as theimmune system recovers.13
Monoclonal antibodies
MAbs have received considerable mediaattention in the UK recently, particularlyin the context of cancer therapies.Neurological adverse events are wellrecognised with MABs that target twospecific immune molecules:
Tumour necrosis factor. Anti-tumournecrosis factor (TNF) MAbs, adali-mumab (hMAb) and infliximab(chimeric antibody against recombinantTNF) are used to treat rheumatoidarthritis, juvenile chronic arthritis, adultpsoriatic arthritis, ankylosing spondylitisand Crohn’s disease.
Inflammatory demyelinating diseasesof the CNS (MS and transverse myelitis)and peripheral nervous system (chronicinflammatory demyelinating polyradicu-loneuropathy), aseptic meningitis, bilat-
eral anterior toxic optic neuropathy,mononeuritis multiplex, orbitalmyositis, polymyositis, CNS lupus andvasculitis are recognised events associ-ated with anti-TNF treatment. Theinflammatory disorders caused or aggra-vated by anti-TNF agents may be due toattenuation of organ specific T cell apop-tosis and T cell signalling.14 Multiplesclerosis (MS) patients who respond toIFN-α have increased levels of TNF-related apoptosis-inducing ligand, amember of the TNF superfamily.
Very late adhesion molecule. Humanisedanti-very late adhesion molecule(VLA)-4 MAb (natalizumab) is used inMS and Crohn’s disease. Progressivemultifocal leukoencephalopathy, anoften fatal disease due to infection ofCNS glia by Jamestown Canyon virus(JCV), is a rare (0.1%) event related toanti-VLA-4 MAb (natalizumab). JCviraemia with natalizumab may be dueto effects on bone marrow (release ofJCV infected B cells into the circulation)or lack of immune surveillance due tosuppression of CD4+ T cell entry intothe CNS.15
Other MAbs can cause neurological
disorders, but those are less frequent andthe mechanisms unclear. For example,OKT3 (muromonab) may causeencephalopathy and seizures but themechanisms remain speculative.
Mitochondria and drug-inducedneurological disorders
As is apparent from the preceding discus-sion, the mitochondrion is the site of toxicity common to many DINDs. Theschematic diagram in Fig 6 summarisessome of the important metabolic loci ofsusceptibility within the mitochondrion(examples in red text boxes).
Carnitine is necessary for the transportof long chain fatty acids across the innermitochondrial membrane and isimported into cells by the carnitinetransporter, organic cation transporter(OCTN2), located in the plasmamembrane. It is then conjugated withfatty-acyl-coenzyme A (CoA) to formfatty-acyl-carnitine by carnitine palmi-toyl transferases (CPT) and transferredacross inner mitochondrial membraneby carnitine acylcarnitine translocase(CACT). CPT2 then converts fatty-acyl-carnitine back to fatty-acyl-CoA for beta
Fig 6. The role ofmitochondria in drug-inducedneurological disorders. ADP = adenosine diphosphate;ATP = adenosine triphosphate;CACT = carnitine acylcarnitinetranslocase; CoA = coenzyme A; CoQ =coenzyme Q; CPT = carnitinepalmitoyl transferase;MPT = mitochondrialpermeability transition; NADH =nicotinamide adeninedinucleotide dehydrogenase;NRTI = nucleoside analoguereverse transcriptase inhibitor;OCTN = organic cationtransporter; TCA = tri-carboxylicacid.
mitoDNA
mitoDNA
mitoDNA

oxidation within the mitochondrion.Primary carnitine deficiency or dysfunc-tion of OCTN2, CPT1, CACT or CPT2may cause myopathy, rhabdomyolysis,hepatic encephalopathy or hypoketotic,hypoglycaemic coma. Drugs which causesecondary carnitine deficiency canpresent with a similar clinical picture.Sodium valproate toxicity is associatedwith carnitine deficiency by inhibitingeither carnitine biosynthesis or transportof carnitine into cells, causing encephalo-pathy with extrapyramidal rigidity, some-times associated with hyperammonaemia.Valproate encephalopathy can appearyears after initiating treatment.
Propofol infusion syndrome due toprolonged exposure to propofol is oftenfatal and characterised by rhabdomyol-ysis, bradyarrythmias, renal failure,metabolic acidosis and lipaemic plasma.Propofol inhibits complex II and IVactivity as well as CPT1 activity, reducingthe entry of fatty-acylcarnitine intomitochondria.16
Reye’s syndrome, the incidence ofwhich dramatically reduced in the 1980s,presents with acute encephalopathy,raised intracranial pressure and fattydegeneration of the liver; it is associatedwith the use of aspirin during acute viralillnesses and thought to be caused bysalicylate-induced mitochondrial perme-ability transition.17 This process leads tocell death through mitochondrialswelling and uncoupling of oxidativephosphorylation. It is thought to be aconsequence of linking of native mito-chondrial proteins in outer and innermitochondrial membranes to form aprotein pore, causing loss of adenosinetriphosphate production.
Aminoglycoside ototoxicity is associ-ated with a mitochondrial DNA pointmutation in the 12S ribosome RNA gene(1555A to G, which makes rRNA similarto bacterial rRNA), accounting for15–30% of aminoglycoside induceddeafness. A maternal family history ofdeafness is an important indicator ofsusceptibility to aminoglycosides.18
Paclitaxol and linezolid are alsoreported to cause a painful peripheralneuropathy. Paclitaxol is an anti-proliferative and pro-apoptotic agentincreasingly used to treat cancer. Swollen
mitochondria in c-fibres are reported inpaclitaxol-associated peripheral neuro-pathy but the mechanisms are not wellknown. Linezolid-associated peripheralneuropathy is purportedly due to theinhibition of respiratory chain complexIV activity.
References
1 Joint Formulary Committee. British nationalformulary 52. London: BMA and RoyalPharmaceutical Society of Great Britain,2005.
2 Jain KK. Drug-induced neurologicaldisorders, 2nd edn. Seattle, WA: Hogrefe &Huber, 2001.
3 Mastaglia FL. Iatrogenic (drug-induced)disorders of the nervous system. In:Aminoff MJ (ed). Neurology and generalmedicine: the neurological aspects of medicaldisorders, 2nd edn. Philadelphia: Churchill-Livingstone, 1995:587–614.
4 Garcia PA, Alldredge BK. Drug-inducedseizures. Neurol Clin 1994;12:85–99.
5 Soares KVS, McGrath JJ. Vitamin E forneuroleptic-induced tardive dyskinesia.Cachrane Database of Systematic Reviews2001(4): CD000209.
6 Jimenez-Jimenez FJ, Garcia-Ruiz PJ, MolinaJA. Drug-induced movement disorders.Review. Drug Saf 1997;16:180–204.
7 Jimenez-Jimenez FJ, Puertas I, de Toledo-Heras M. Drug-induced myoclonus:frequency, mechanisms and management.Review. CNS Drugs 2004;18:93–104.
8 Arora R, Liebo M, Maldonado F. Statin-induced myopathy: the two faces of Janus.J Cardiovasc Pharmacol Ther 2006;11:105–12.
9 Gaist D, Garcia Rodriguez LA, Huerta C,Hallas J, Sindrup SH. Are users of lipid-lowering drugs at increased risk ofperipheral neuropathy. Eur J ClinPharmacol 2001;56:931–3.
10 Phan T, McLeod JG, Pollard JD et al.Peripheral neuropathy associated withsimvastatin. J Neurol Neurosurg Psychiatry1995;58:625–8.
11 Phillips PS, Haas RH, Bannykh S et al.Statin-induced myopathy with normalcreatine kinase levels. Ann Intern Med2002;137:581–5.
12 McGarrigle CA, Cliffe S, Copas AJ et al.Estimating adult HIV prevalence in the UKin 2003: the direct method of estimation.Review. Sex Transm Infect 2006;82(Suppl 3):iii78–86.
13 Lewis W, Kohler JJ, Hosseini SH et al.Antiretroviral nucleosides, deoxynucleotidecarrier and mitochondrial DNA: evidencesupporting the DNA pol gammahypothesis. AIDS 2006;20:675–84.
14 Battegay M, Nuesch R, Hirschel B,
Kaufmann GR. Immunological recoveryand anti-retroviral therapy in HIV-1infection. Review. Lancet Infect Dis 2006;6:280–7.
15 Sicotte NL, Voskuhl RR. Onset of multiplesclerosis associated with anti-TNF therapy.Neurology 2001;57:1885–8.
16 Ransohoff RM. Natalizumab and PML. NatNeurosci 2005;8:1275.
17 Wolf A, Weir P, Segar P, Stone J, Shield J.Impaired fatty acid oxidation in propofolinfusion syndrome. Lancet 2001;357:606–7.
18 Lemasters JJ, Nieminen AL, Qian T,Trost LC, Heman B. The mitochondrialpermeability transition in toxic, hypoxicand reperfusion injury. Review. Mol CellBiochem 1997;174:159–65.
19 Fischel-Ghodsian N. Mitochondrialmutations and hearing loss: paradigm formitochondrial genetics. Review. Am J HumGenet 1998;62:15–9.
176 Clinical Medicine Vol 7 No 2 April 2007
CME Neurology