Embed Size (px)
Citation preview

Drug-Drug interaction (Silent Epidemic)
By Mohie Aldien (MD)

Definitions and Terms • Side Effects: unintended, usually detrimental, consequences
• Adverse: untoward, unintended, possibly causing harm
• AE: Adverse Event, Effect or Experience
• ADE (AE associated with a Drug): an AE which happens in a patient taking a drug
• ADR (Adverse Drug Reaction): an ADE in which a causal association is suspected between the drug and the event
Unfortunately, these terms are frequently used interchangeably
•Drug Interactions:“ The pharmacologic or clinical response to the administration of a drug combination different from that anticipated from the known effects of the two agents when given alone ”
1Tatro DS (Ed.) Drug Interaction Facts. J.B. Lippincott Co. St. Louis 1992.

Why Are There So Many ADRs? • Two-thirds of patient visits result in Rx
• 3 BILLION outpatient Rx per year
• Specialists give 2.3 Rx per visit
• Medicare Patients (2003, before drug benefit)
– 89.2% take a prescription medicine daily
– 46.1% take ≥5 prescriptions chronically
– 53.6% take meds Rxed by 2 or more doctors
– 5% obtain an Rx from Canada/Mexico
• ADRs increase exponentially with ≥4 Rx

Leape LL et al. JAMA 1995;274(1):35–43.
Raschetti R et al. Eur J Clin Pharmacol 1999;54(12):959–963.
Contribution of Drug Interactions to the Overall Burden of Preventable ADRs
• Drug interactions represent 3–5% of preventable in-hospital ADRs
• Drug interactions are an important contributor to the number of ER visits and hospital admissions

0 10 20 30 40 50 60
Being Given the Wrong Drug
Being Given Drugs that Interact
Cost of Treatment
Complications of Treatment
Having Enough Information
Getting an Infection in the Office/Hospital
Side-Effects from a Medicine
Receiving too much Medicine
Suffering Pain
Cost of Prescriptions once discharged
% of Patients
Primary Worries in Primary Care: 1,008 Patients
Source: American Society of Health Systems Pharmacists.
ASHP Patient Concerns National Survey Research Report, 1999.

Prescriber’s Knowledge
Computer Screening
Pharmacist’s Knowledge
Patient Risk Factors
Patient Education
Monitoring
ADR
Drug Interaction Defenses
Hansten PD, Horn JR. Modified from: James Reason, Human Error, 1990
Drug Administration
Pharmacogenetics
Drug A + Drug B
Latent Failures
Defenses


Drug-Drug Interactions classification:
•According to effect:
A-Harmful Effects (potentiating/antagonism)
B- Beneficial Effects (Additive or Synergistic)

II) According to site of interaction:
A) In-vitro:
1-Drug-laboratory tests interaction:

Mixture Mixing into Result
•Thiopentone+ suxamethonium
•Heparin + hydrocortisone
•Kanamycin + hydrocortisone
•Kanamycin + pencillin
•Soluble insulin + PZ insulin.
•Penicillin + hydrocortisone
•B-lactam antibiotic + gentamycin
•Pz insulin +Heparin (Acid)
•Thiopentone (Alkaline) +
Succinylcholine (Acid)
•Same syringe •Precipitation(ppt)
•Inactivation of heparin
•Inactivation of kanamycin
•Inactivation of pencillin
•Ppt of soluble insulin.
•Inactivation of penicillin
•Mutual inactivation
•Neutralization
•Neutralization
•Na salt of barbiturate, phenytoin,
sulphonamide ,heparin ,peniciline,
Diazep. Amamphotricin,
Hydrocortisone .
•Ampicillin, Barbiturates &
Ascorbic acid (Vit C)
•IV adr.,erythrocin, cephalothin .
•Almost all drugs
•Iv fluid e.g 5%
dextrose.
•Dextran
•Aminophyline IV
solution
•In blood , plasma
aminoacid,manitol
or heparin IVI.
•Precipitation in acidic pH
of dextrose.
•Precipitation
•Decompose in alkaline
PH ofAminophyline .
•Precipitation or
inactivation
2) Mixing 2 drugs prior injection:

Drug-Drug interaction inside the body

Drug interaction Includes:
1.Drug-drug
2.Drug-allergy
3.Drug-nutrient
4.Drug-alternative medicine
5.Drug-food
Features:
1.Identify drug interactions and minimize adverse events
2.Ranked by severity
3.Description of each interaction
4.No redundant information
5.Customized alerts

•Onset of drug interaction It may be seconds up to weeks for example in case of enzyme induction, it needs weeks for protein synthesis , while enzyme inhibition occurs rapidly.
The onset of action of a drug may be affected by the half lives of the drugs e.g., cimitidine inhibits metabolism of theophylline. Cimitidine has a long half life, while, theophylline has a short one. When cimitidine is administered to a patient regimen for Theophylline, interaction takes place in one day.

Factors Influencing Drug Interaction Outcomes
PATIENT FACTORS
CLINICAL
OUTCOME
OF
DRUG
INTERACTIONS
DRUG ADMINISTRATION
•Genetics •Diseases(malignant cases, diabetic patients, patients with liver or kidney , disorders.)
•pregnant women •Diet/Nutrition
•Environment
•Smoking
•Alcohol
•Dose
•Duration
•Dosing Times
•Sequence
•Route
•Dosage Form
•lowTherapeutic index Phenytoin, Cyclosporine Theophylline
•Sharp response curve Phenytoin, Aminoglycoside Vancomycin
•Dose dependent , Michalis-Menten Kinetic.
Phenytoin
HIGH
VARIABILITY

Therapeutic Index : Ratio = LD50 / ED50 - LD50 = Lethal dose in 50% of animals - ED50 = Effective dose in 50% of animals *Theophylline *Quinine *Lithium *Digoxin *Anticoagulants (Warfarin) *Antibiotics (Aminoglycosid, rifampicin) *Anticonvulsants (carbamazepine, lithium, phenytoin, phenobarbital *Cytotoxic and Immunosuppresants *Oral Contraceptives, ciclosporin,

MTC
MEC
Time
Plas
ma d
rug
conc
entra
tion
Need to keep concentration of drug withinthe therapeutic range


Pharmacokinetic interactions
1) Altered GIT absorption.
•Altered pH • Altered bacterial flora • formation of drug chelates or complexes, • drug induced mucosal damage • altered GIT motility.

•Gastric acidity : -Infection Absorption of weak acid drugs eg Aspirin & Phenobarbitone. •Antiacids ,H2 antagonists , PPIs, atazanavir, itraconazole (gastric alkalinity) →↓absorbtion of weak acid (Aspirin,barbiturate,Ketoconazole
,quinolones and fluoroquinolones , tetracyclin) and ↑absorption weak base.
•Intestinal Alkalinity Absorption of weak base drugs e.g. Ephedrine
Therefore, these drugs must be separated by at least 2h in the time of administration of both .
a)Altered pH; The non-ionized form of a drug is more lipid soluble and more readily absorbed
from GIT than the ionized form does.

b)Interactions during absorption 1. Chelation chelating agent:1. a compound that combines with metal ions to form stable ring structures.
2. a substance used to ↓the concentration of free metal ion in solution by complexing it.
Usually separating administration of chelating drugs by 2+h decreases interaction effect
*Antacids (Ca2+, Mg2+, Al3+), iron salts (Fe2+) and
milk (Ca2+) inhibit the absorption of
tetracyclines through chelation
*Bile acid binding resins: cholestyramine,
cholestipol adsorps and inhibits the
absorption of thyroxine, cardiac glycosides
(digoxin, digitoxin), warfarin, corticosteroids,
thiazides and (Immunosuppressants?)
*Kaolin-pectin decrease the absorption of digoxin
*Tetracyclines and Quinolones chelate metals and
form an insoluble complex that reduces their
absorption.
* EDTA chelates toxic metals such as lead and
reduces toxicity..

b)Interactions during absorption(cont.)
Usually separating administration of chelating drugs by 2+h decreases interaction effect
2-Adsorption is the nonspecific binding
of a drug to another agent: •Cholestyramine adsorbs many drugs such as dicumarol, methotrexate and digitoxin and decreases their absorption. • Antacids decrease digoxin and iron absorption by adsorption

An enzyme inhibition interaction
The chloramphenicol inhibited the metabolism of the phenytoin in this patient so that the
serum levels climbed into the toxic range and intoxication developed (indicated by
nystagmus). The problem was solved by stopping the phenytoin and later re-starting at a
lower dosage (after Ballek RE et al., Lancet (1973) i, 150, with permission).

C) E p i t h e l i a l S t r u c t u r e o f G u t W a l l: •Phenytoin Absorption of Folic acid •Para-amino-salicylic acid (PASA) & Colchicine Absorption of Vit B-12 •Neomycin Absorption of digitalis & Penicillins . •Antineoplastic agents e.g., cyclophosphamide , vincristine, procarbazine mucosal damage Inhibit absorption of several drugs eg., digoxin

D) Altered motility;Gastric emptying time (GET) is the time required to
empty the stomach.
• GET is increased by food , morphine, Metoclopramide (antiemitic) →
Gastric emptying ↑ absorption of rapid dissolution drugs e.g
Paracetamol & Propranolol but ↓absorption of delay dissolution drugs e.g.
Digoxin.
GET is decreased by fasting ,antacids, opioid, antimuscarinic : (propantheline atropine), antidiarrhoeal →↓ Gastric emptying:
- ↓ absorption of paracetamol - Decreased bioavailability of drugs that
are degraded in the intestine (levodopa) - Increased bioavailability of lipid soluble drugs
•The Reverse.
•Laxatives will cause drugs to move through
The intestine so rapidly that they are poorly
absorbed

E)Interactions at the GIT may be indirect and complex: Antimicrobials: Chloramphenicol, tetracyclines alter gut flora.
• Causing decreased synthesis of vit K by bacteria, thus prolonged the effects of oral anticoagulants which compete with vit K.
• Inhibit the enterohepatic recycling of estrogens, thus decrease the efficacy of oral contraceptives
• Increase the absorption of drugs that are metabolized by gut bacteria e.g. digoxin

F) Altered intestinal bacterial flora ; - In 10% 0f patients receive digoxin….. 40% or more of the administered dose is metabolized by the intestinal flora
- Antibiotics (Chloramphenicol, tetracyclines) kill a large number of the normal flora of the intestine,
• Causing decreased synthesis of vit K by bacteria, thus prolonged the efects of oral anticoagulants which compete with vit K.
• Inhibit the enterohepatic recycling of estrogens, thus decrease the efficacy of oral contraceptives
• Increase the absorption of drugs that are metabolized by gut bacteria e.g. digoxin
Increase digoxin conc. and increase its toxicity

G) Increases in blood flow will increase drug absorption whereas a decrease in blood flow will decrease drug absorption. . Epinephrine reduces blood flow and is used in combination with local anesthetics [lidocaine and procaine] to decrease their absorption into the blood (rapidly hydrolyzed) and to prolong their duration of action.

Efflux (to intestinal lumen): • P-glycoprotein (P-gp, MDR1, ABCB1) • Breast Cancer Resistance Protein (BCRP, ABCG2)
G) Transport alteration

They Can Occur in the GI Tract • Sucralfate, some milk products,
antacids, and oral iron preparations
• Omeprazole, lansoprazole,
H2-antagonists
• Didanosine (given
as a buffered tablet)
• Cholestyramine
Block absorption of quinolones, tetracycline, and azithromycin
Reduce absorption of ketoconazole, delavirdine
Reduces ketoconazole absorption
Binds raloxifene, thyroid hormone, and digoxin

Drug affected Interacting drugs Effect of interaction
Digoxin
Metoclopramide Reduced digoxin absorption
Propantheline Increased digoxin absorption (due to changes in gutmotility)
Digoxin
Colestyramine Reduced absorption due to binding/complexation with colestyramine
Levothyroxine
Warfarin
Ketoconazole Antacids Reduced ketoconazole absorption due to
reduced dissolution H2-blockers
Penicillamine Antacids containing Al3+, Mg2+, iron preparations, food
Formation of less soluble penicillamine chelates resulting in reduced absorption of penicillamine
Penicillin Neomycin Neomycin-induced malabsorption state
Quinolone antibiotics
Antacidscontaining Al3+, Mg2+, milk, Zn2+ (?), Fe2+
Formation of poorly absorbed complexes
Tetracyclines Antacids containing Al3+, Ca2+, Mg2+, Bi2+, milk, Zn2+, Fe2+
Formation of poorly soluble chelates resulting in reduced antibiotic absorption
Some drug absorption interactions

Graphic depiction of a theoretical drug distribution interaction

PK interaction associated with Protein binding
• The major plasma proteins to which most drugs bind are albumin and a1-acid glycoprotein; the former typically binds acidic, anionic drugs whereas the latter typically favors basic drugs
• Competitive protein binding by another drug will result in increase concentration of free drug, and that will yield more drug response

f) Displaced protein binding
It depends on the affinity of the drug to plasma protein. The most likely bound drugs is capable to displace others. It is clinically important if displaced drug is highly PP binding , with LONG T ½, small Vd, narrow therapeutic range. The free drug is increased by displacement by another drug with higher affinity.
Aspirin, Phenylbutazone, Clofibrate & Sulfa Displace: a-Oral Anti-coagulants (Dicumarol, Warfarin) Bleeding b-Oral Hypoglycemics (Tolbutamide) Hypoglycemia c-Bilirubin in Neonate Jaundice & Kernictrus. D-phenytoin
Free drug
Bound drug

Transporters in Drug Distribution, Uptake and
excreation –important liver transporters

metabolism
Determinants of Drug Disposition and Interaction
Efflux
Enterocyte
Drug/Metabolite
Drug Systemic Circulation
Intestinal Lumen
Biliary and Renal Elimination
Uptake
Transport
Transport
Transport
Uptake
Transport
Hepatocyte,
Kidney tubule cells
metabolism
Efflux
Efflux

Examples of Clinically Significant Drug interactions Associated with Inhibition of Transporters Other Than PgP

Bauer B, Hartz AM, Fricker G, Miller D. Modulation of p-Glycoprotein Transport Function at the
Blood-Brain Barrier. Experimental Biology and Medicine Feb. 2005;230:118-27.
P-Glycoprotein (PGP) Substrates

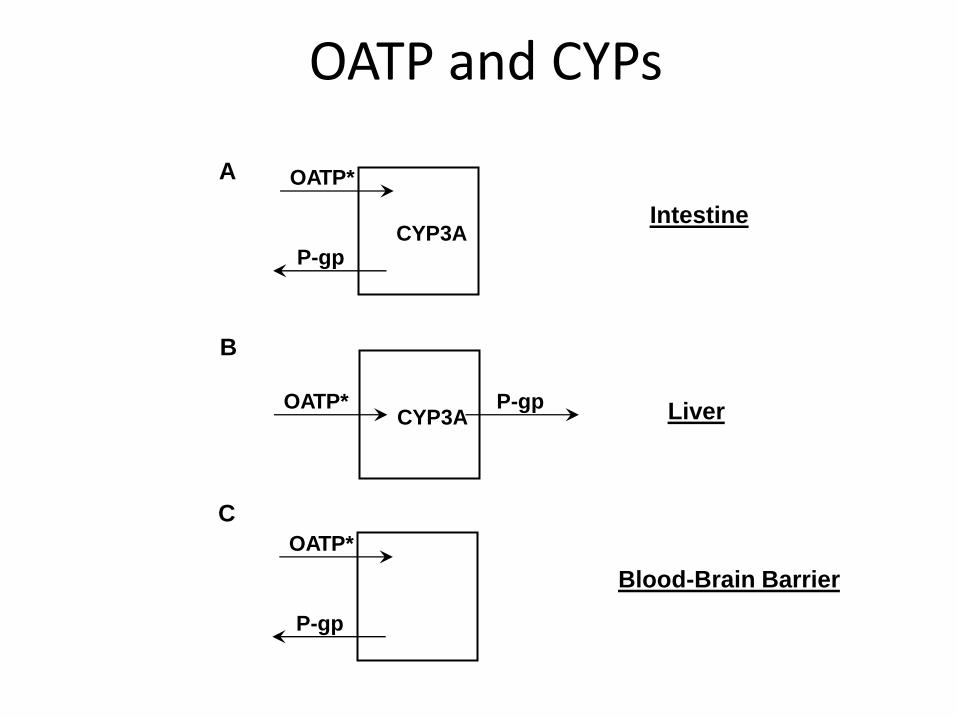
OATP and CYPs
CYP3A P-gp
OATP*
CYP3A P-gp OATP*
P-gp
OATP*
A
B
C
Intestine
Liver
Blood-Brain
Barrier

The effects of drug A on drug B through (A) direct induction/inhibition of enzymes; (B)
indirect induction/inhibition of transcription factors that regulate the drug-metabolizing
enzymes.
Tari L et al. Bioinformatics 2010;26:i547-i553



NEDMDG, March 2010 43
Ieiri et al. (2009) Expert Opinion in Drug Metabolism and Toxicology, 5: 703-729.
Transporter Interaction Redundancy:
Drugs that are shown to interact with one transporter typically interact with multiple transporters.
Thus, multiple pathways for clearance are possible for transporter substrates.
Slide courtesy of Dr. Mitchell Taub

Drug affected Interacting drugs Results of interaction
Clonidine Tricyclic antidepressants
Antihypertensive effects
opposed, possibly due to
interference in CNS with
clonidine uptake
Guanethidine-like
antihypertensives
(debrisoquine,
guanoclor, etc.)
Tricyclic antidepressants
Antihypertensive effects
opposed, due to
inhibition of uptake into
adrenergic neurones.
Chlorpromazine
Haloperidol
Tiotixene (Thiothixene)
Indirectly-acting
sympathomimetics
Noradrenaline
(norepinephrine) Tricyclic antidepressants
Pressor effects
increased due to
inhibition of
noradrenaline uptake
into adrenergic neurones
Interactions due to changes in drug transport mechanisms

OATP and CYPs
CYP3A P-gp
OATP*
CYP3A P-gp OATP*
P-gp
OATP*
A
B
C
Intestine
Liver
Blood-Brain Barrier

Transport Proteins in the liver
BCRP
canalicular
membrane
basalateral
membrane
MDR1
BSEP
MDR3
MRP2
NTCP
Na + Bile acids
OCT1 OAT2
OATP-C OATP-B OATP-8
Estrone-3-sulfate
BSP
pravastatin
E217G, Estrone-3-sulfate
LTC4, thyroid hormones
bile acids, pravastatin
digoxin
DPDPE, BSP
Estrone-3-sulfate
PGE2
AZT
MTX
phospholipids
Bile acids

Drug Efflux Transporters in the Liver
MDR1/ABCB1 MRP2/ABCC2 BCRP/ABCG2
Tissue
distribution
BBB, GI, liver, etc Liver, proximal part
of GI.
GI, liver, BBB,
placental, etc
MW (Kd) 170 190 70
Function Dramatic impact on
CNS exposure
Oral absorption
Maintain basal bile
flow
Biliary excretion
Oral absorption,
Biliary exretion
Typical
Substrates
Diverse
hydrophobic
xenobiotics:
vinblastine
GSH, GSH-
/glucuronide-
conjugates, organic
anions
mitoxantrone,
methotrexate
topotecan, E23-
sulfate

P-Glycoprotein (MDR1) Actively Transports Drugs Out of Cell Wall
Cell Wall
• Efflux pump: exposure to xenobiotics
• Found in numerous tissues: - Intestinal Epithelium - Biliary canaliculi
• -Renal proximal tubules - Blood-brain barrier - Tumor cells
• Promiscuous: interacts with wide variety of chemical structures
Inhibitors: cyclosporine, verapamil, erythromycin, Itraconazole,retoniver , ketocon-azole, verapamil ,itraconazole ,quinidine azrythromycin Inducers: phenobarbital, rifampin, phenytoin, St. John’s wort. Substrate:digoxin, fexofenadine, indinavir, vincristine, colchicine, topotecan, paclitaxel, talinolol, loperamide.
= Lipophilic Drug Inside Cell
Outside Cell
Entry via passive diffusion
PGP

Primary drug Interacting drug effect Result of interaction
•Digoxin
•Lignocaine
•Diuretics
•Tubocurarine
•Lithium
•Angiotensin-
converting
enzyme
inhibitor
•Diuretic-induced hypokalemia
•Diuretic-induced hypokalemia
•NSAID-induced salt and water
retention
•Diuretic-induced hypokalemia
•Thiazide-induced reduction in
renal clearance
•Potassium chloride and/or
patassium-retaining diuretic-
induced hyperkalemia
•Digoxin toxicity
•Antagonism of
antiarrhythmic effects
•Antagonism of diuretic
effects
•Prolonged paralysis
•Raised plasma lithium
•Severe hyperkalemia
Interactions secondary to drug-induced alterations of
fluid and electrolyte balance.

Drug affected Interacting drugs Results of interaction
Digitalis Potassium-depleting diuretics
Digitalis toxicity related to changes in ionic balance at the myocardium
Lithium chloride
Dietary salt restriction Increased serum lithium levels; intoxication possible
Increased salt intake Reduced serum lithium levels
Lithium chloride Thiazide and related diuretics
Increased serum lithium levels; intoxication possible
Guanethidine Chlorothiazide
Kebuzone Phenylbutazone
Antihypertensive effects opposed due to salt and water retention
Interactions due to disturbances in fluid and electrolyte balance



Liver
Induction
Drug A induces the body to produce more of an enzyme to metabolized Drug B
This reduces the amount of Drug B and may lead to loss of Drug B’s effectiveness
Inhibition
Drug A inhibits the production of enzymes to metabolize Drug B
This increases the amount of Drug B in the body and could lead to an overdose or toxic effects

a-HME Inducers: Phenytoin, Phenobarbitone, Rifampicin, Testosterone &
Tobacco smoking Their own metabolism & Other drugs.
b-HME Inhibitors: MAO-I, Cimetidine, Estrogen, Na Valproate & Chloramphenicol

Shimada T et al. J Pharmacol Exp Ther 1994;270(1):414.
CYP3A
CYP2D6
CYP2C
CYP1A2 CYP2E1
Relative Importance of
P450s in Drug Metabolism
CYP450 Activity in the Liver
CYP3A
CYP2C
CYP1A2
CYP2E1
?
CYP2D6
Relative Quantities
of P450s in Liver


Drug affected Inducing agent(s) Effect of interaction
Anticoagulants (oral)
Aminoglutethimide
Anticoagulant effects reduced
Barbiturates
Carbamazepine
Dichloralphenazone
Glutethimide
Phenazone
Rifampicin (rifampin)
Contraceptives (oral)
Barbiturates,Carbamazepine, Phenytoin, Primidone, Rifampicin
Contraceptive effects reduced. Break-through bleeding, contraceptive failures
Corticosteroids
Aminoglutethimide
Corticosteroid effects reduced
Barbiturates
Carbamazepine
Phenytoin
Primidone
Rifampicin (rifampin)
Haloperidol Tobacco smoke Haloperidol effects reduced
Pentazocine Tobacco smoke Pentazocine effects reduced
Phenytoin Rifampicin (rifampin) Phenytoin effects reduced. Seizure-risk increased
Theophylline Barbiturates
Theophylline effects reduced Rifampicin (rifampin) Tobacco smoke
Interactions due to enzyme induction

Drug affected Inducing agent(s) Effect of interaction
Anticoagulants (oral)
Aminoglutethimide
Anticoagulant effects reduced
Barbiturates
Carbamazepine
Dichloralphenazone
Glutethimide
Phenazone
Rifampicin (rifampin)
Contraceptives (oral) Barbiturates,Primidone,Carbamazepine, Phenytoin,Rifampicin
Contraceptive effects reduced. Break-through bleeding, contraceptive failures
Corticosteroids
Aminoglutethimide
Corticosteroid effects reduced
Barbiturates
Carbamazepine
Phenytoin
Primidone
Rifampicin (rifampin)
Haloperidol Tobacco smoke Haloperidol effects reduced
Pentazocine Tobacco smoke Pentazocine effects reduced
Phenytoin Rifampicin (rifampin) Phenytoin effects reduced. Seizure-risk increased
Theophylline Barbiturates
Theophylline effects reduced Rifampicin (rifampin) Tobacco smoke
Interactions due to enzyme induction
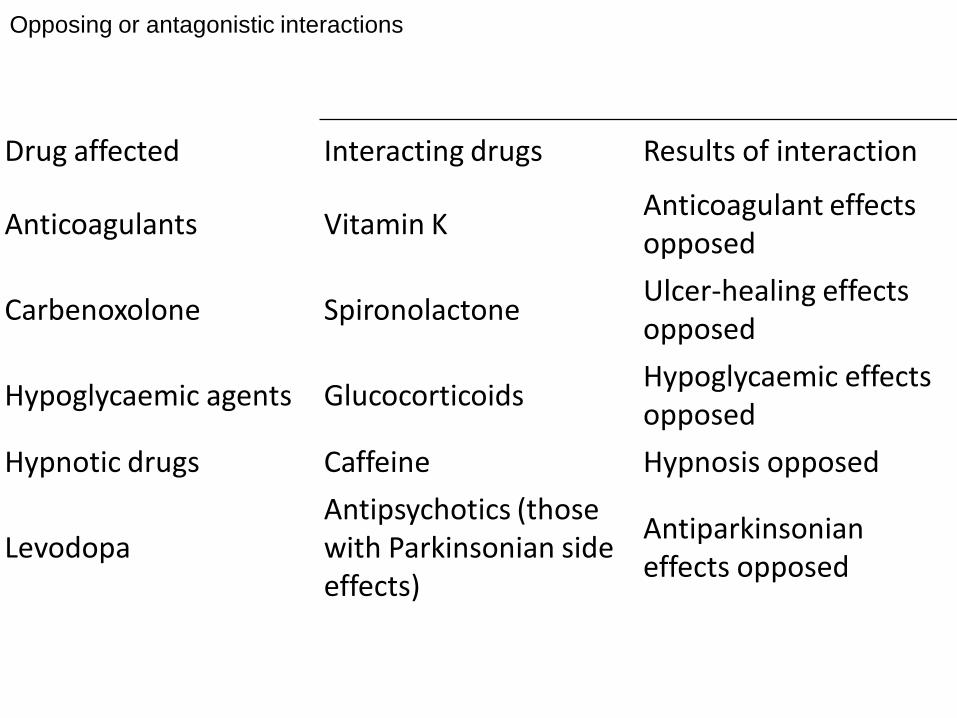
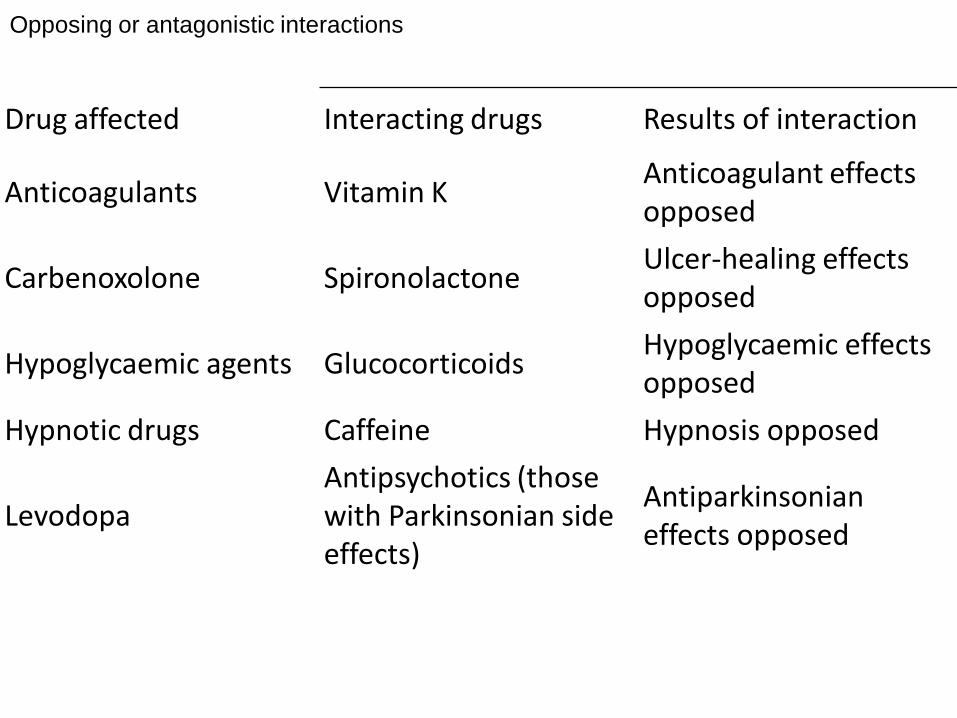
Drug affected Interacting drugs Results of interaction
Anticoagulants Vitamin K Anticoagulant effects opposed
Carbenoxolone Spironolactone Ulcer-healing effects opposed
Hypoglycaemic agents Glucocorticoids Hypoglycaemic effects opposed
Hypnotic drugs Caffeine Hypnosis opposed
Levodopa Antipsychotics (those with Parkinsonian side effects)
Antiparkinsonian effects opposed
Opposing or antagonistic interactions

a-Competition for A c t i v e Tubular Excretion: •Probenecid Excretion of penicillin Prolongs its duration of action •Probenecid Excretion of Frusemide Antagonize its diuretic effect •Quinidine Excretion of Digoxin Its plasma concentration
Competitive interaction between drugs for active tubular
secretion.Probenecid ( • ) is able successfully to compete with some
of the other drugs ( o ) for active secretory mechanisms in the
kidney tubules which reduces their loss in the urine and raises
serum levels. The probenecid is later passively reabsorbed
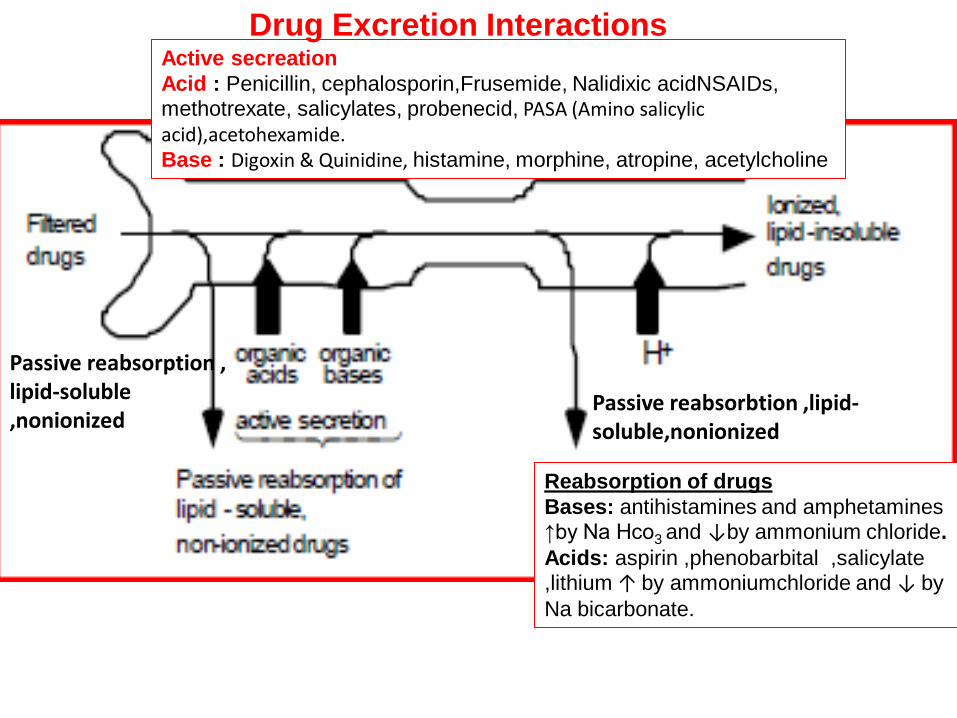
Reabsorption of drugs
Bases: antihistamines and amphetamines ↑by Na Hco3 and ↓by ammonium chloride.
Acids: aspirin ,phenobarbital ,salicylate ,lithium ↑ by ammoniumchloride and ↓ by
Na bicarbonate.
Active secreation
Acid : Penicillin, cephalosporin,Frusemide, Nalidixic acidNSAIDs, methotrexate, salicylates, probenecid, PASA (Amino salicylic acid),acetohexamide. Base : Digoxin & Quinidine, histamine, morphine, atropine, acetylcholine
Drug Excretion Interactions
Passive reabsorbtion ,lipid-soluble,nonionized
Passive reabsorption , lipid-soluble ,nonionized

b- p H C h a n g e s: Acidification of urine (NH4Cl) Excretion of Weak base drugs e.g. Ephedrine Alkalinization of urine (NaHCO3) Excretion of weak acid drugs e.g. Aspirin

Competitive interaction between drugs
for active tubular secretion
Probenecid ( • ) is able successfully to
compete with some of the other drugs ( o )
for active secretory mechanisms in the
kidney tubules which reduces their loss in
the urine and raises serum levels. The
probenecid is later passively reabsorbed


Common Inducers, Inhibitors, and Substrates of Select CYP450 Isozymes



Drugs Result of interaction
•Anticholinergics + anticholinergics (anti-parkinsonian agents, butyrophenones, phenothiazines, tricyclic antidepressants, etc.)
•Increased anticholinergic effects; heat stroke in hot and humid conditions; adynamic ileus; toxic psychoses
•Antihypertensives + drugs causing hypotension (anti-anginals, vasodilators, phenothiazines)
•Increased antihypertensive effects; orthostasis
•CNS depressants + CNS depressants (alcohol, anti-emetics, antihistamines, hypnosedatives, etc.)
•Impaired psychomotor skills, reduced alertness, drowsiness, stupor, respiratory depression, coma, death
•QT prolonging drugs + other QT prolonging drugs (Amiodarone + Disopyramide)
•Additive prolongation of QT interval, increased risk of torsade de pointes
•Methotrexate + co-trimoxazole •Bone marrow megaloblastosis due to folic acid antagonism
•Nephrotoxic drugs + nephrotoxic drugs (gentamicin or tobramycin with cefalotin (cephalothin)
•Increased nephrotoxicity
•Neuromuscular blockers + drugs with neuromuscular blocking effects (e.g. aminoglycoside antibacterials)
•Increased neuromuscular blockade; delayed recovery, prolonged apnoea
•Potassium supplements + potassium-sparing diuretics (triamterene)
•Marked hyperkalaemia
Additive, synergistic or summation interactions

Drugs Result of interaction
Anticholinergics + anticholinergics (anti-parkinsonian agents, butyrophenones, phenothiazines, tricyclic antidepressants, etc.)
Increased anticholinergic effects; heat stroke in hot and humid conditions; adynamic ileus; toxic psychoses
Antihypertensives + drugs causing hypotension (anti-anginals, vasodilators, phenothiazines)
Increased antihypertensive effects; orthostasis
CNS depressants + CNS depressants (alcohol, anti-emetics, antihistamines, hypnosedatives, etc.)
Impaired psychomotor skills, reduced alertness, drowsiness, stupor, respiratory depression, coma, death
QT prolonging drugs + other QT prolonging drugs (Amiodarone + Disopyramide)
Additive prolongation of QT interval, increased risk of torsade de pointes
Methotrexate + co-trimoxazole Bone marrow megaloblastosis due to folic acid antagonism
Nephrotoxic drugs + nephrotoxic drugs (genta-micin or tobramycin with cefalotin (cephalothin)
Increased nephrotoxicity
Neuromuscular blockers + drugs with neuromuscular blocking effects (e.g. aminoglycoside antibacterials)
Increased neuromuscular blockade; delayed recovery, prolonged apnoea
Potassium supplements + potassium-sparing diuretics (triamterene)
Marked hyperkalaemia
Additive, synergistic or summation interactions
Drug affected Interacting drugs Results of interaction
Anticoagulants Vitamin K Anticoagulant effects opposed
Carbenoxolone Spironolactone Ulcer-healing effects opposed
Hypoglycaemic agents Glucocorticoids Hypoglycaemic effects opposed
Hypnotic drugs Caffeine Hypnosis opposed
Levodopa Antipsychotics (those with Parkinsonian side effects)
Antiparkinsonian effects opposed
Opposing or antagonistic interactions

Interactions at adrenergic neurones

* Prevention of drug interaction
1) Monitoring therapy and making adjustments
2) Monitoring blood level of some drugs with narrow therapeutic index e.g., digoxin, anticancer agents…etc 3) Monitoring some parameters that may help to characterize the the early events of interaction or toxicity e.g., with warffarin administration, it is recommended to monitor the prothrombin time to detect any change in the drug activity. 4) Increase the interest of case report studies to report different possibilities of drug interaction

Drug–Drug Interaction Observed Adverse Outcome ACE inhibitors + K-sparing diuretics Hospitalization for hyperkalemia ACE inhibitors + co-trimoxazole Hospitalization for hyperkalemia Benzodiazepines + CYP3A4 inhibitors Hospitalization for hip fracture Calcium channel blockers + macrolides Hospitalization for hypotension or shock Digoxin + macrolides Hospitalization for digoxin toxicity Lithium + ACE inhibitors, loop diuretics Hospitalization for lithium toxicity Phenytoin + co-trimoxazole Hospitalization for phenytoin toxicity Glipizide or glyburide + CYP2C9 inhibitors Hospitalization for hypoglycemia Tamoxifen + paroxetine Death from breast cancer Theophylline + ciprofloxacin Hospitalization for theophylline toxicity Warfarin + co-trimoxazole or fluconazole Hospitalization for GI bleeding Warfarin + NSAIDs Hospitalization for GI bleeding .
ACE = angiotensin-converting enzyme; CYP = cytochrome P450; GI = gastrointestinal; K = potassium; NSAIDs =nonsteroidal anti-inflammatory drugs
Important Drug Interactions in the Elderly

Thank you

Drug–Drug Interaction Observed Adverse Outcome ACE inhibitors + K-sparing diuretics Hospitalization for hyperkalemia ACE inhibitors + co-trimoxazole Hospitalization for hyperkalemia Benzodiazepines + CYP3A4 inhibitors Hospitalization for hip fracture Calcium channel blockers + macrolides Hospitalization for hypotension or shock Digoxin + macrolides Hospitalization for digoxin toxicity Lithium + ACE inhibitors, loop diuretics Hospitalization for lithium toxicity Phenytoin + co-trimoxazole Hospitalization for phenytoin toxicity Glipizide or glyburide + CYP2C9 inhibitors Hospitalization for hypoglycemia Tamoxifen + paroxetine Death from breast cancer Theophylline + ciprofloxacin Hospitalization for theophylline toxicity Warfarin + co-trimoxazole or fluconazole Hospitalization for GI bleeding Warfarin + NSAIDs Hospitalization for GI bleeding .
ACE = angiotensin-converting enzyme; CYP = cytochrome P450; GI = gastrointestinal; K = potassium; NSAIDs =nonsteroidal anti-inflammatory drugs
Important Drug Interactions in the Elderly


Common Diabetes, Hypertension, and Lipid Drug Interactions



Common Inducers, Inhibitors, and Substrates of Select CYP450 Isozymes

Cytochrome P450 Nomenclature, e.g., for CYP2D6
• CYP = cytochrome P450
• 2 = genetic family
• D = genetic sub-family
• 6 = specific gene
• NOTE: This nomenclature is genetically based; it does not imply chemical specificity

Major Human CYP450 Isoforms
• CYP2D6
• CYP2E1
• CYP3A4
• CYP3A5
• CYP3A6
CYP1A2
CYP2B6
CYP2C8
CYP2C9
CYP2C19

Overactive metabolism can cause adverse events
“Normal” Activity
Morphine Enzyme
Pro-Drug (Codeine)
Morphine
Morphine
Morphine
Enzyme
Enzyme
Enzyme
“Ultra-rapid” Activity
Pro-Drug (Codeine)
Morphine
Morphine

Drug-Drug interaction (Silent Epidemic)
By Mohie Aldien (MD)
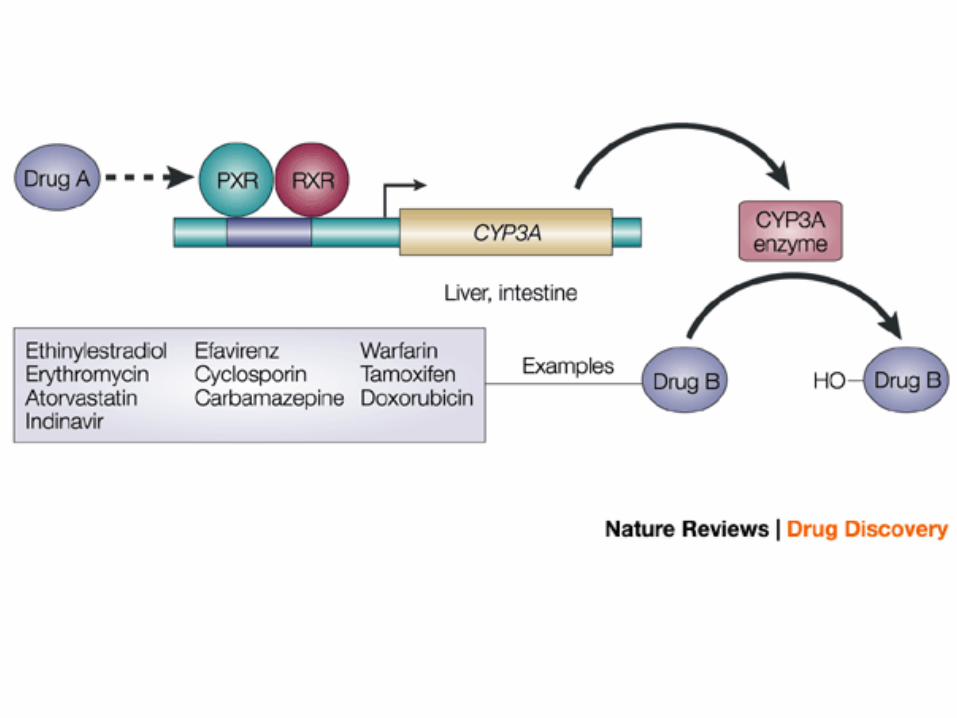

Drug Metabolism Interactions: Induction
Adapted from Urquhart et al J Clin Pharm 2007;47:566-78

First-pass metabolism: Oral administration increases the chance for liver and GIT metabolism of drugs leading to the loss of a part of the drug dose decreasing its action. This is more clear when such drug is an enzyme inducer or inhibitor.
EX., Rifampin lowers serum con. of verapamil level by increase its first pass . Also, Rifampin induces the hepatic metabolism of verapamil

Phase I - Drug Oxidation

Both PGP and CYP3A4
• Inhibitors
– Verapamil
– Clarithromycin
– Erythromycin
– Itraconazole
– Ritonavir
– Cyclosporine
• Inducers
– Rifampicin
– St. John’s Wort
– Phenobarbital
– Reserpine

*These programs are not endorsed by the FDA
Drug-Drug Interaction Prevention: A Stepwise Approach
1. Take a medication history
(AVOID Mistakes mnemonic)
2. Remember high-risk patients
• Any patient taking ≥ 2 medications
• Patients Rxed anticonvulsants, antibiotics, digoxin, warfarin, amiodarone, etc.
3. Check pocket reference or PDA
4. Consult pharmacists or drug info specialists
5. Check up-to-date computer program
• Medical Letter Drug Interaction Program*
• www.epocrates.com* and others

Marchietti S, et al. Clinical relevance of drug-drug and herb-drug interactions mediated by the
ABC transporter ABCB1 (MDR1, P-glycoprotein). The Oncologist 2007;12:927-41.
P - Glycoprotein Tissue Distribution

Bauer B, Hartz AM, Fricker G, Miller D. Modulation of p-Glycoprotein Transport Function at the Blood-Brain Barrier. Experimental
Biology and Medicine Feb. 2005;230:118-27.
P-Glycoprotein (PGP) Substrates

Uptake proteins: focus on OATP (also OCT, OAT) Transport numerous amphipathic compounds Some present only in the liver Many present at the BBB, lung, heart, intestine, kidney etc. Facilitate the influx of compounds Fexofenadine and digoxin are well-defined OATP substrates Fruit juices(grapefruit juice, apple juice, and orange juice) inhibit OATPs, along with
quinidine, nelfinavir, saquinavir, and ketoconazole


Recently, increased

NEDMDG, March 2010 97
Tables of Substrates and Inhibitors


NEDMDG, March 2010 99
Lack of selective inhibitors of drug transporters
1. Dantzig et al. (1999) JPET 290, 854-862 2. Hsiang et al. (1999) J Biol Chem 274, 37161-8 3. Abe et al. (1999) J Biol Chem 274, 17159-63 4. Konig et al. (2000) Am J Physiol Gastrointest Liver Physiol 278, G156-64 5. Hagenbuch. & Meier (2003) Biochim Biophys Acta 1609, 1-18 6. Oostendorp et al. (2009) DMD 37, 917-923
1999 1999 – 2003 2009
• LY 335979 (zosuquidar) is a potent inhibitor/modulator of P-gp, but does not inhibit MRP1 or MRP2. • Selectivity over inhibition of CYP3A4 is ~60-fold. [Reference 1]
• Discovery, cloning, and publication of OATP superfamily of uptake transporters [References 2-5]
• OATP1B1-mediated uptake of anticancer drugs gimatecan and BNP1350 were inhibited by zosuquidar. • The effect of modulators on the plasma pharmacokinetics of OATP1B1 substrate drugs may not be solely ascribed to inhibition of P-gp [Reference 6]
Slide courtesy of Dr. Mitchell Taub

Drug Interactions: Transport Proteins

Drugs metabolised by these cytochrome P450 isoenzymes
CYP450 isoenzyme
Drugs metabolised
CYP1A2 Caffeine, Clozapine, Imipramine, Maprotiline, Phenacetin, Propranolol, R-warfarin, Ropinirole, Theophylline
CYP2D6
Amitriptyline, Amfetamine (Amphetamine), Captopril, Clomipramine, Codeine, Desipramine, Dextromethorphan, Dihydrocodeine, Diphenhydramine, Flecainide, Fluoxetine, Haloperidol, Hydrocodone, Imipramine, Labetalol, Maprotiline, Metoprolol, Mexiletine, Nortriptyline, Ondensatron, Oxycodone, Papaverine, Paroxetine, Penbutolol, Perphenazine, Propafenone, Propranolol, Thioridazine, Timolol, Trimipramine, Venalfaxine, Yohimbine
CYP2C9 Diclofenac, Dofetilide, Fluvastatin, Ibuprofen, Mefenamic acid, Naproxen, Phenytoin, Piroxicam, S-warfarin, Tolbutamide
CYP2C19 Clomipramine, Diazepam, Hexobarbital (Hexobarbitone), Imipramine, Mephobarbital, Omeprazole, Phenytoin, Propranolol, Proguanil, S-mephenytoin
CYP3A4
Amiodarone, Amitriptyline, Alprazolam, Astemizole, Carbamazepine, Ciclosporin (Cyclosporin), Cisapride, Clindamycin, Clomipramine, Clonazepam, Dapsone, Dexamethasone, Dextromethorphan, Diazepam, Diltiazem, Erythromycin, Ethyl estradiol, Felodipine, Hydrocortisone (Cortisol), Imipramine, Indinavir, Lidocaine (Lignocaine), Lovastatin, Midazolam, Nefazodone, Nelfinavir, Nevirapine, Nifedipine, Nimodipine, Nisoldipine, Propafenone, Quinidine, R-warfarin, Ritonavir, Saquinavir, Sertraline, Simvastatin, Tamoxifen, Terfenadine, Testosterone, Triazolam, Venlafaxine, Verapamil, Zolpidem
This list is not exhaustive and is derived from several sources.

Cy P450 isoenzyme Inhibiting drugs
CYP1A2 Enoxacin, Cimetidine, Ciprofloxacin, Fluvoxamine, Furafylline, Grapefruit juice, Grepafloxacin
CYP2D6 Fluoxetine, Haloperidol, Paroxetine, Quinidine, Ritonavir, Sertraline, Thioridazine
CYP2C9 Fluconazole, Fluoxetine, Fluvoxamine, Ritonavir
CYP2C19 Fluoxetine, Fluvoxamine, Omeprazole
CYP3A4
Cimetidine, Clarithromycin, Erythromycin, Fluvoxamine, Grapefruit juice, Itraconazole, Ketoconazole, Miconazole, Nefazodone, Nelfinavir, Remacemide, Ritonavir
Drugs that inhibit these cytochrome P450 isoenzymes

Cytochrome P450 isoenzyme Inducing drugs
CYP1A2 Barbiturates, Omeprazole, Phenytoin, Tobacco smoke
CYP2D6 ?
CYP2C9 Barbiturates, Rifampicin (Rifampin)
CYP2C19 ?
CYP3A4 Barbiturates, Carbamazepine, Dexamethasone, Phenytoin, Rifabutin, Rifampicin (Rifampin)
Drugs that induce these cytochrome P450 isoenzymes


1 in 10 7
1 in 10 6
1 in 10 5
1 in 10 4
1 in 10 3 1 in 10 2
Lightning
Plane crash Murder
Auto-cash
Fatal, unexpected drug reaction
Increasing risk of death


Distribution
Harmful Effects (potentiation/antagonism)
Additive or Synergistic/ Beneficial Effects


Altered pH
Altered motility Chelation
Chelation

CYPP450 isoenzyme
Drugs metabolised
CYP1A2 Caffeine, Clozapine, Imipramine, Maprotiline, Phenacetin, Propranolol, R-warfarin, Ropinirole, Theophylline
CYP2D6
Amitriptyline, Amfetamine (Amphetamine), Captopril, Clomipramine, Codeine, Desipramine, Dextromethorphan, Dihydrocodeine, Diphenhydramine, Flecainide, Fluoxetine, Haloperidol, Hydrocodone, Imipramine, Labetalol, Maprotiline, Metoprolol, Mexiletine, Nortriptyline, Ondensatron, Oxycodone, Papaverine, Paroxetine, Penbutolol, Perphenazine, Propafenone, Propranolol, Thioridazine, Timolol, Trimipramine, Venalfaxine, Yohimbine
CYP2C9 Diclofenac, Dofetilide, Fluvastatin, Ibuprofen, Mefenamic acid, Naproxen, Phenytoin, Piroxicam, S-warfarin, Tolbutamide
CYP2C19 Clomipramine, Diazepam, Hexobarbital (Hexobarbitone), Imipramine, Mephobarbital, Omeprazole, Phenytoin, Propranolol, Proguanil, S-mephenytoin
CYP3A4
Amiodarone, Amitriptyline, Alprazolam, Astemizole, Carbamazepine, Ciclosporin (Cyclosporin), Cisapride, Clindamycin, Clomipramine, Clonazepam, Dapsone, Dexamethasone, Dextromethorphan, Diazepam, Diltiazem, Erythromycin, Ethyl estradiol, Felodipine, Hydrocortisone (Cortisol), Imipramine, Indinavir, Lidocaine (Lignocaine), Lovastatin, Midazolam, Nefazodone, Nelfinavir, Nevirapine, Nifedipine, Nimodipine, Nisoldipine, Propafenone, Quinidine, R-warfarin, Ritonavir, Saquinavir, Sertraline, Simvastatin, Tamoxifen, Terfenadine, Testosterone, Triazolam, Venlafaxine, Verapamil, Zolpidem
This list is not exhaustive and is derived from several sources.
1.6 Drugs metabolised by these cytochrome P450 isoenzymes





























