Embed Size (px)
Citation preview
Prepared for the Auditor General for Scotland and the Accounts Commission March 2009
Drug and alcohol services in Scotland
Auditor General for Scotland The Auditor General for Scotland is the Parliament’s watchdog for ensuring propriety and value for money in the spending of public funds.
He is responsible for investigating whether public spending bodies achieve the best possible value for money and adhere to the highest standards of financial management.
He is independent and not subject to the control of any member of the Scottish Government or the Parliament.
The Auditor General is responsible for securing the audit of the Scottish Government and most other public sector bodies except local authorities and fire and police boards.
The following bodies fall within the remit of the Auditor General:
• directorates of the Scottish Government • government agencies, eg the Prison Service, Historic Scotland • NHS bodies • further education colleges • Scottish Water • NDPBs and others, eg Scottish Enterprise.
Note: Prior to September 2007, the Scottish Administration was generally referred to as the Scottish Executive. It is now called the Scottish Government. When dealing with the earlier period, this report refers to the Scottish Executive. Recommendations for the future refer to the Scottish Government.
The Accounts Commission The Accounts Commission is a statutory, independent body which, through the audit process, assists local authorities in Scotland to achieve the highest standards of financial stewardship and the economic, efficient and effective use of their resources. The Commission has four main responsibilities:
• securing the external audit, including the audit of Best Value and Community Planning
• following up issues of concern identified through the audit, to ensure satisfactory resolutions
• carrying out national performance studies to improve economy, efficiency and effectiveness in local government
• issuing an annual direction to local authorities which sets out the range of performance information they are required to publish.
The Commission secures the audit of 32 councils and 41 joint boards (including police and fire and rescue services). Local authorities spend over £19 billion of public funds a year.
Audit Scotland is a statutory body set up in April 2000 under the Public Finance and Accountability (Scotland) Act 2000. It provides services to the Auditor General for Scotland and the Accounts Commission. Together they ensure that the Scottish Government and public sector bodies in Scotland are held to account for the proper, efficient and effective use of public funds.
Acknowledgements:
Audit Scotland would like to thank the members of the project advisory group for their input and advice throughout the study (Appendix 2). We are also grateful to everyone who provided information and assisted us with this study.
Sally Thompson managed the project, with support from Mike McCarron (consultant), under the general direction of Claire Sweeney.
DrugandalcoholservicesinScotland1
Contents Summary page 2
Background
Aboutthestudy
Keymessages page 3
Keyrecommendations page 4
Part 1. The scale of drug and alcohol misuse page 5
Keymessages
Scotlandhasasignificantproblem withdrugsandalcoholcomparedto therestoftheUKandEurope page 6
Drugandalcoholmisuseaffectsall communitiesinScotlandbuthasa biggerimpactindeprivedareas page 8
Manypublicsectorbodies commissionorprovidedrugand alcoholservices page 9
Part 2. Direct expenditure on drug and alcohol services page 11
Keymessages
Thewidercostsofdrugandalcohol misuseareanestimated£5billion peryear
Thepublicsectorspent£173million ondrugandalcoholservicesin 2007/08 page 12
Spendingondrugandalcoholservices doesnotreflectlevelsofneed page 15
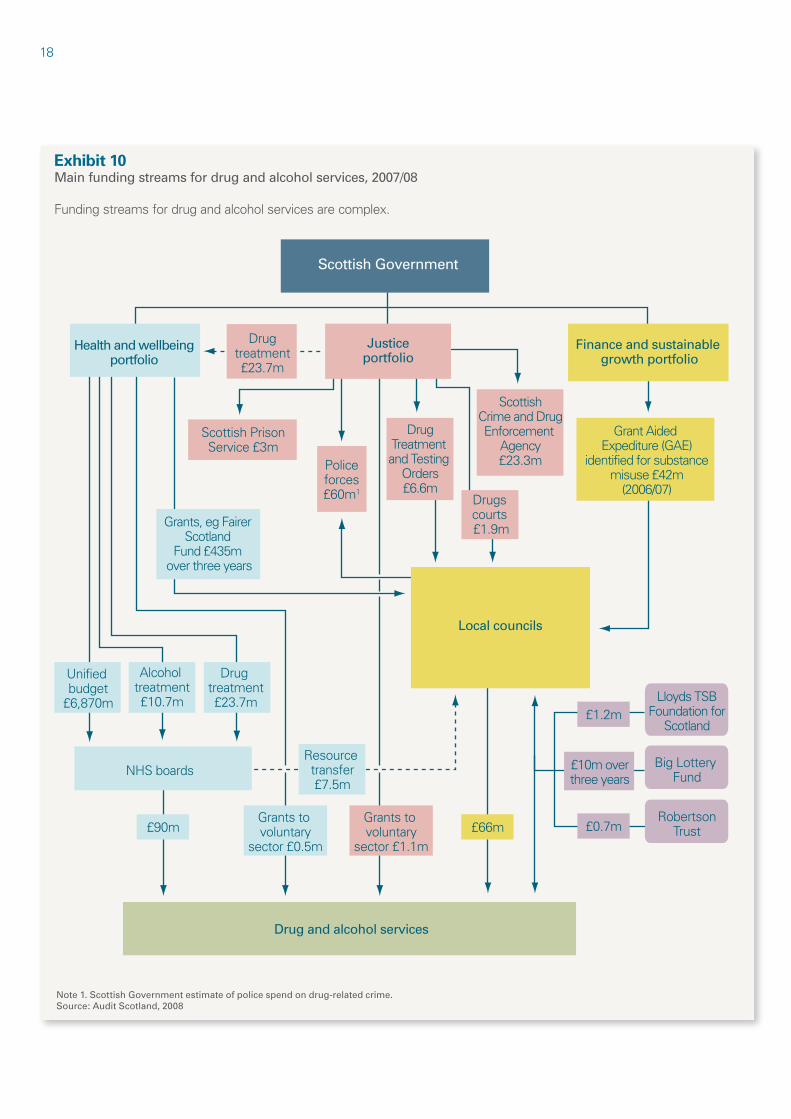
Fundingarrangementsfordrugand alcoholservicesarecomplexand makestrategicplanningdifficult page 16
Recommendations page 20
Part 3. Effectiveness of drug and alcohol services page 21
Keymessages
Drugandalcoholservicesvaryacross Scotland page 22
Nationalinformationonneedsandthe impactofservicesispoor page 24
Theimpactofdrugandalcohol servicesisnotknownatanational level page 25
Recommendations page 26
Part 4. Drug and alcohol partnerships page 27
Keymessages
Alackofcentralguidancehasledto variationinhowlocalpartnerships operate
Notalldrugandalcoholpartnerships haveachievedtheobjectivesset forthem
Therolesandresponsibilitiesofdrug andalcoholpartnershipsarestill unclear page 28
Recommendations page 30
Appendix 1. Notes to the text page 32
Appendix 2. Project advisory group membership page 34
Appendix 3. Drug and alcohol policy and guidance summary page 35
Appendix 4. Self-assessment checklist for partners page 37
2
Summary
Drugandalcoholmisusearemajorproblemsin Scotlandbutresourcestoaddressthemarenotalways usedeffectively.

Summary3
Background
1.Theimpactofdrugandalcohol misuseinScotlandiswidespread.Both individualsandsocietymorewidely areaffectedintermsofhealth,child protection,crime,communitysafety, housing,employmentandsocial exclusion.Drugandalcoholmisuseare problemsacrossthewholeofScotland butparticularlyaffectpeoplelivingin deprivedareas.1,2
2.Thelinksbetweendrugandalcohol misuseandeffortstoaddressthem arecomplexandinter-related,and manyservicesareaimedatbothdrug andalcoholmisuse.Numerouspublic sectororganisationsareinvolvedin providingservices,includingtheNHS, councils,thepoliceandtheprison service.Thevoluntarysectorisakey partnerindeliveringservicesfordrug andalcoholmisuse.
3.TheScottishGovernmenthas launchednewstrategiesfordrugs andalcoholinthelast12months:The Road to Recovery: A new approach for tackling Scotland’s drug problem inMay2008andChanging Scotland’s Relationship with Alcohol: A framework for actioninMarch2009.Themaindrug andalcoholpolicydocumentsissuedby theScottishExecutiveandtheScottish Governmentoverthelastdecadeare summarisedinAppendix3.3
4.Multi-agencypartnershipworking fordrugandalcoholproblemshas beeninplaceforaround20years. Partnershipworkingisacoreelement intherecentScottishGovernment strategiesfordrugsandalcohol.4,5
5.TheScottishGovernmentandother keypublicbodiesinvolvedinproviding servicesdonotholdcomparabledata onthecosts,activityorimpactof drugandalcoholservicesinScotland. Inthisreportwehaveusedavailable nationaldatasupplementedwithlocal informationwherenecessary.
About the study
6.Theaimofourstudywasto identifyhowmuchthepublicsector
spendson‘labelled’drugandalcohol services.6Wealsoassessedwhether evidenceofneedorwhatworks determineshowthismoneyisused andwhatimpactthemoneyhashad.
7.Inthisstudy,we:
• analysedpublishedinformation onservicesandreviewednational documents
• collectedandanalysedexpenditure datafromallNHSboardsand councils.Intheabsenceofcost informationfrompoliceservices, wecollectedactivitydatafromall policeforcesinScotlandtogivean indicationofexpenditure
• carriedoutfocusgroupswithpeople whohaveproblemswithdrugsand alcohol,familiesdirectlyaffectedby drugandalcoholmisuse,localdrug andalcoholpartnershipsupportstaff andvoluntaryandprivatesector serviceproviders
• interviewedstaffandreviewed documentsfromagencies commissioningorprovidingdrug andalcoholservices.
8.Wedidnotcollectinformation onthewidercostsassociatedwith drugandalcoholmisuseasexisting researchisavailableandreferred toinPart2.Thisresearchcovers costsrelatingtogenericservices suchasaccidentandemergency (A&E)departments,andwider economicandhumancostssuchas theestimatedcostoflostearnings anddeathsduetodrugandalcohol misuse.
9.Thisreportisinfourmainparts:
• Thescaleofdrugandalcohol misuse(Part1).
• Directexpenditureondrugand alcoholservices(Part2).
• Effectivenessofdrugandalcohol services(Part3).
• Drugandalcoholpartnerships(Part4).
Key messages
Scotlandhashighlevelsofdrug andalcoholmisusecompared totherestoftheUK.Drugand alcohol-relateddeathratesare amongthehighestinEurope andhavedoubledinthelast 15years.Drugandalcohol misusearefoundacrosssociety butpeoplewhoarelikelyto beexcludedfromsocietyand thoselivingindeprivedareas aremostaffected.
In2007/08,thepublicsector spent£173millionondrugand alcoholservicesinScotland, £84millionspecificallyondrug servicesand£30millionon alcoholservices.Theremainder wasspentonjointdrugand alcoholservices.Funding arrangementsarecomplexand projectscanhaveanumber ofseparatefundingstreams, eachwithdifferenttimescales andreportingcriteria.Thisis anaddeddifficultyforthose planningandprovidingservices.
Thereisvariationacross Scotlandintherangeand accessibilityofdrugand alcoholservices.TheScottish Governmenthasnotsetout minimumstandardsintermsof range,choiceandaccessibility thatserviceusersandtheir familiescanexpecttoreceive. Spendingdecisionsarenot alwaysbasedonevidence ofwhatworksoronafull assessmentoflocalneed.
Giventhescaleofdrugand alcoholproblemsinScotland andtherangeofagencies involved,clarityofrolesand accountabilityisessential.It isimportantfortheScottish Governmenttosetoutthe directionandtherolesand responsibilitiesofpartner agenciesandhowperformance willbeassessed.
•
•
•
•
4
Key recommendations
TheScottishGovernmentshould:
setclearnationalminimum standardsfordrugandalcohol servicesincludingtheirrange, qualityandaccessibility; receiveassurancethatthese standardsareimplementedin linewithsettimescales;and ensureperformanceisregularly monitoredandpubliclyreported
clarifyaccountabilityand governancearrangementsfor thedeliveryofdrugandalcohol servicesinScotlandandsetout clearlytheresponsibilitiesofall organisationsandpartnerships involvedinplanningordelivering theseservices.
Publicsectorbodiesshould:
ensurethatalldrugandalcohol servicesarebasedonan assessmentoflocalneedand thattheyareregularlyevaluated toensurevalueformoney.This informationshouldthenbe usedtoinformdecision-making inthelocalarea
ensurethatservice specificationsareinplaceforall drugandalcoholservicesand setoutrequirementsrelating toserviceactivityandquality. Whereservicesarecontracted, thisspecificationshouldbepart oftheformalcontract
setclearcriteriaofeffectiveness andexpectedoutcomesfor thedifferentservicesthatthey provideandundertakeregular auditstoensureservices adheretoexpectedstandards
usetheAuditScotlandchecklist detailedinAppendix4tohelp improvethedeliveryandimpact ofdrugandalcoholservices throughajoined-up,consistent approach.
•
•
•
•
•
•
5
Part 1. The scale of drug and alcohol misuse
Scotlandhasagreaterproblemwithdrugsand alcoholthantherestoftheUKandmostofEurope, withdeprivedcommunitiesmostaffected.
6
Key messages
Scotlandhashighlevelsofdrug andalcoholmisusecompared totherestoftheUK.The levelsofproblematicdrug misuseinScotlandaredouble thatofEnglandandthelevels ofalcoholdependencyarea thirdhigher.Alcoholmisuse isabiggerproblemthandrug misuse.
Drugandalcohol-relateddeath ratesareamongthehighest inEuropeandhavedoubledin thelast15years.Thisisata timewhenindicatorsofdrug andalcohol-relatedharmare reducinginothercountriesin Europe.
Drugandalcoholmisuseare foundacrosssocietybutpeople whoarelikelytobeexcluded fromsocietyandthoseliving indeprivedareasaremost affected.Peoplelivingin deprivedareasaremorelikelyto sufferserioushealthproblems asaresultoftheirdrugoralcohol misuse.
•
•
•
Scotland has a significant problem with drugs and alcohol compared to the rest of the UK and Europe
10.In1982,theMinisterialAdvisory CouncilontheMisuseofDrugs definedsomeonewithproblematic druguseas“any person who experiences social, psychological, physical or legal problems related to intoxication and/or regular excessive consumption and/or dependence as a consequence of his/her own use of drugs or chemical substances.” 7
11.TheWorldHealthOrganisation definesalcoholdependencyas“a cluster of psychological, behavioural and cognitive phenomena. A central characteristic is the desire (often strong, sometimes perceived as overpowering) to drink alcohol.” 8
Ourreportreferstoalcoholmisuse andincludesalcoholdependency, hazardous,harmfulandbinge
drinking,allofwhichhaveharmful consequencesintermsofhealth, violenceandcommunitysafety.
12.Thelinksbetweendrugand alcoholmisuseandeffortstoaddress themarecomplexandinter-related. Manyproblematicdruguserswilluse morethanonedrugandmayalso misusealcohol.
Therearehighandincreasinglevelsof drug-relatedharminScotland 13.Thereisahigherprevalence ofdrugmisuseinScotlandthan elsewhereintheUK.Theestimated numberofpeopleaged15to54 misusingopiates,suchasheroin, decreasedfrom55,800in2000to 51,582in2003.Thisequatesto 1.8percentofthepopulation.9This isdoublethelevelinEngland,where approximately0.9percentofthe populationaged15to64misuse opiates.10
14.Theuseofcocaineisincreasingin Scotland.Thenumberofnewpeople contactingservicesandlistingcocaine astheirmaindrugproblemdoubled from284in2003/04to625in 2007/08.11Thenumberofdrug-related deathsinvolvingcocainehasalso doubledoverthepastfiveyears.12
15.Scotlandalsohasthehighest rateofinjectingdrugusersinthe UKwitharateof5.6per1,000 populationcomparedto4.2forthe UKasawhole.13Scotlandhashigh levelsofdruguserssharinginjecting equipment.Thereareanestimated 50,000peopleinScotlandwith hepatitisCanddruguserswhoinject andshareinjectingequipmentarethe largestgroupofpeopleaffected.14,15 16.Thereisalackofnationaldataon thelevelsofdrugmisuserelatingto ethnicity.In2007/08,justover 99percentofnewpeoplecontacting servicesfordrugproblemsdescribed theirethnicityaswhiteandalmost 96percentaswhiteScottish.16
17.Drugsareusedbypeopleofall agesbutin2007/08themedianage ofnewpeoplecontactingservices
fordrugproblemswas30years.17 Sixteenpercentofnewcontacts wereover40yearsofageandeight percentwere19yearsoryounger.18
18.Therearelimiteddataonthe numberofchildrenaffectedby parentalsubstancemisusebutthere isinformationonpregnantwomen collectedinhospitals.In2006/07, 566pregnantwomeninhospitalwere recordedashavingdrugproblems inScotland,arateof10.4per1,000 maternities.Thisratehasincreased from6.7per1,000in2002/03.19
Youngpeopleanddrugs 19.Thelevelofdrugmisuseamong 13and15-year-oldshasreduced acrosstheUK,primarilyasaresultof adeclineintheuseofcannabis:20
• Nearlyaquarter(23percent)of 15-year-oldsinScotlandreported usingdrugsin2006,comparedto 31percentin2004.
• Sevenpercentof13-year-oldsin Scotlandreportedusingdrugsin 2006,comparedto11percent in2004.21
However,reporteduseofillegaldrugs amongschoolchildreninScotlandis stillhigh.
Drug-relatedhealthharmanddeaths 20.In2007/08,therewere 5,363dischargesfromacute generalhospitalswithadrug-related diagnosis,arateof108per100,000 population.Overthelastsixyears, therehasbeenlittlechangeintherate ofdrug-relateddischarges.22Ninety-five percentofpeopledischargedwitha drug-relateddiagnosiswereinitially admittedasanemergency.23 In2006/07,itisestimatedthat 148,050consultationswithGPs relatedtodrugmisuse.24
21.Drug-relateddeathsinScotland arethehighestrecordedintheUK andamongthehighestinEurope.In EnglandandWales,therateofdrugrelateddeathswas2.7per100,000 populationin2005comparedto 7.3per100,000inScotland.25

Part1.Thescaleofdrugandalcoholmisuse7
22.Drug-relateddeathsinScotland areattheirhighesteverlevelandare increasing.In2007,therewere455 drug-relateddeaths,a103percent increaseovertenyears.26,27Insome localareas,therehasbeenareduction inthenumberofdrug-relateddeaths inrecentyearsandsignificantvariation year-on-year.Forexample,inGlasgow therewere106drug-relateddeathsin 2004,thisfellto75in2005andthen increasedto113in2006.In2007, therewere90drug-relateddeathsin Glasgow.Mostdrug-relateddeathsin Scotlandinvolvemorethanonedrug andalcohol.28
Drugsandcrime 23.Seizuresofillegaldrugsby Scottishpoliceforcesincreasedby 27percent,from16,425in 1999/2000to20,938in2006/07.29 Seizuresofcocainehaveincreased atatimewhenfiguressuggest greatercocaineuseinsociety. Between2002/03and2006/07, cocaineseizuresbyScottishpolice forcesincreasedfrom17percent ofallseizuresofClassAdrugsto30 percent.Heroinaccountedforthe majorityofClassAseizures.30,31
24.Drugmisuseanddrugdealingin localcommunitiesleadstoincreases inboththefearofcrimeandactual crime.Seventy-sixpercentofpeople surveyedbytheScottishExecutivein 2006believedthatdrugmisusewasa ‘bigproblem’intheircommunity.32 25.In2007/08,theaveragespend onaheroinaddictionwas£245a weekand£624aweekonacocaine addiction.33Drugusersreportthata mixtureofsocialsecuritybenefitsand crimearemostcommonlyusedto fundtheirhabits.34Thishasobvious implicationsforcrimeratesandthe widercostsofdrugmisuse.
Therearehighandincreasinglevelsof alcohol-relatedharminScotland 26.Alcoholmisuseisabigger problemthandrugmisuseintermsof thenumberofpeoplemisusingand theharmcausedtohealth.Estimating
thesizeofScotland’salcohol problemisnoteasyduetoalackof nationaldataandunder-reportingof consumption.
27.InEngland,thefirstnational alcoholneedsassessmentwas carriedoutin2004.Itestimated that3.6percentofthepopulation agedbetween16and64was dependentonalcohol.35InScotland, itisestimatedthat4.9percentof thepopulationaged16andoverare dependentonalcohol.Thehigher prevalenceofalcoholdependency inScotlandwasfoundtobelargely duetothehigherratesofalcohol dependencyinScottishwomen.36
28.Overthelast45years,alcohol salesintheUKhavedoubled,rising from5.7litresofpurealcoholper personaged16andoverin1960to 11.3litresin2005.37
29.Therehavealsobeenchangesin thetypesofalcoholpurchasedover time.Salesofbeerhaveremained steadysince1980,buttherehave beenincreasesinthesaleofwine, cideranddrinkssuchasalcopops.38
30.MorealcoholissoldinScotland thaninEnglandandWalesperhead ofpopulation.In2007,anaverage of12.2litresofpurealcoholwas soldperpersonaged18andoverin Scotland,comparedto10.3litresin EnglandandWales.Thisdifference ispartlyduetopeopleinScotland buyingmorespiritscomparedtothe restoftheUK,anaverageof3.6 litresperpersonaged18andover inScotland,comparedto1.8litresin Englandin2007.39
31.Thenumberoffemalesreporting drinkingabovetherecommended weeklylimit(14unitsofalcohol)is increasing.40In1995,13percentof womenaged16to64yearsdrank morethan14unitsperweek,rising to17percentin2003.Thisislikelyto beanunder-estimate.40
Youngpeopleandalcohol 32.Levelsofunder-agedrinking arehigh.In2006,overathird (36percent)of15-year-oldsreported thattheyhadconsumedalcoholin thepreviousweek.Therehasbeena reductioninreporteddrinkingamong boys.Reporteddrinkingamong 15-year-oldgirlsincreasedfrom tenpercentin1990to23percentin 2002.Thishassincefallento 15percentof15-year-oldgirlsreporting theydrinkalcoholin2006,thisis 50percenthigherthanin1990.41
33.FiguresforhospitalA&E departmentshighlightthe consequencesofyoungpeople drinking.Overafive-weekperiodin 2006,nearly650childrenranging fromeightto15-years-oldwere treatedforalcohol-relatedproblemsin ScottishA&Edepartments.42
Alcohol-relatedhealthharmand deaths 34.In2007/08,therewere 42,430dischargesfromacutegeneral hospitalswithanalcohol-related diagnosis.Overthelastfiveyears, thedischargeratehasincreasedby ninepercent,from710per100,000 populationin2002/03to777per 100,000population.43
35.Alcoholisconsideredtobea contributoryfactorin11percentof allattendancesatA&E.Thebusiest timeforalcohol-relatedattendances isFridaynight/Saturdaymorning, betweenmidnightandfourinthe morning.44
36.In2006/07,itisestimatedthat around111,200consultationsfor alcoholmisusetookplacewithGPs andpracticenurses.45Theroleof GPsandpracticestaffinrelationto alcoholmisuseislikelytogrow,with specificfundingfromtheScottish Governmenttosupportscreeningand briefinterventionsinprimarycare.46
8
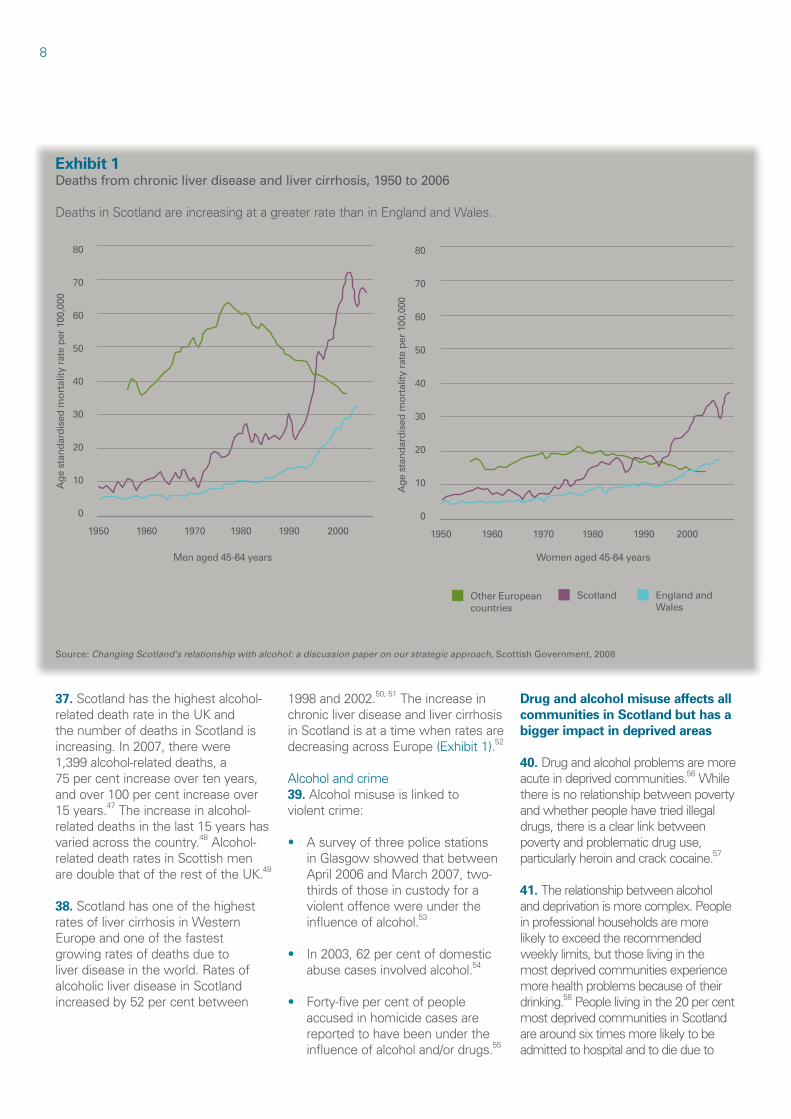
Exhibit 1 Deaths from chronic liver disease and liver cirrhosis, 1950 to 2006
DeathsinScotlandareincreasingatagreaterratethaninEnglandandWales.
Source: Changing Scotland’s relationship with alcohol: a discussion paper on our strategic approach, Scottish Government, 2008
Age
sta
ndar
dise
d m
orta
lity
rate
per
100
,000
80
70
60
50
40
30
20
10
0
1950 1960 1970 1980 1990 2000
Men aged 45-64 years
Age
sta
ndar
dise
d m
orta
lity
rate
per
100
,000
80
70
60
50
40
30
20
10
0
1950 1960 1970 1980 1990 2000
Women aged 45-64 years
Other European countries
Scotland England and Wales
37.Scotlandhasthehighestalcohol-relateddeathrateintheUKand thenumberofdeathsinScotlandis increasing.In2007,therewere 1,399alcohol-relateddeaths,a 75percentincreaseovertenyears, andover100percentincreaseover 15years.47Theincreaseinalcoholrelateddeathsinthelast15yearshas variedacrossthecountry.48AlcoholrelateddeathratesinScottishmen aredoublethatoftherestoftheUK.49
38.Scotlandhasoneofthehighest ratesoflivercirrhosisinWestern Europeandoneofthefastest growingratesofdeathsdueto liverdiseaseintheworld.Ratesof alcoholicliverdiseaseinScotland increasedby52percentbetween
1998and2002.50,51Theincreasein chronicliverdiseaseandlivercirrhosis inScotlandisatatimewhenratesare decreasingacrossEurope(Exhibit1).52
Alcoholandcrime 39.Alcoholmisuseislinkedto violentcrime:
• Asurveyofthreepolicestations inGlasgowshowedthatbetween April2006andMarch2007,twothirdsofthoseincustodyfora violentoffencewereunderthe influenceofalcohol.53
• In2003,62percentofdomestic abusecasesinvolvedalcohol.54
• Forty-fivepercentofpeople accusedinhomicidecasesare reportedtohavebeenunderthe influenceofalcoholand/ordrugs.55
Drug and alcohol misuse affects all communities in Scotland but has a bigger impact in deprived areas
40.Drugandalcoholproblemsaremore acuteindeprivedcommunities.56While thereisnorelationshipbetweenpoverty andwhetherpeoplehavetriedillegal drugs,thereisaclearlinkbetween povertyandproblematicdruguse, particularlyheroinandcrackcocaine.57
41.Therelationshipbetweenalcohol anddeprivationismorecomplex.People inprofessionalhouseholdsaremore likelytoexceedtherecommended weeklylimits,butthoselivinginthe mostdeprivedcommunitiesexperience morehealthproblemsbecauseoftheir drinking.58Peoplelivinginthe20percent mostdeprivedcommunitiesinScotland arearoundsixtimesmorelikelytobe admittedtohospitalandtodiedueto
Part1.Thescaleofdrugandalcoholmisuse9
alcoholmisusethanthosefromthemost affluentareas.59
Peoplewhoarelikelytobeexcluded fromsocietyhaveparticularproblems withdrugsandalcohol 42.Drugandalcoholmisuseare greaterproblemsforpeoplewho aresociallyexcluded,comparedto therestofsociety.Uptothreein fourpeopleusingdrugshavemental healthproblems,anduptooneintwo peoplewithalcoholproblemsmay haveamentalhealthproblem.60Audit Scotlandispublishinganoverview reportofmentalhealthservicesin ScotlandinMay2009.
43.Thereisalsoevidenceofhigh levelsofdrugmisuseamonghomeless people.Asampleof225homeless peopleinGlasgowshowedthat 56percentofthoseunder35years oldwereaddictedtodrugs,withheroin beingthemostcommon.Thesame sampleshowedthat54percentof homelesspeoplereportedhazardous drinkingbehaviour.61
44.Over40percentofprisoners arelikelytohaveanalcoholproblem, fourtimeshigherthanthegeneral population.62Two-thirdsofprisoners testpositiveforillegaldruguseon admissiontoprison.63
45.Drugandalcoholmisusedoes notjustaffecttheusersthemselves. Childrenofparentswhomisusedrugs andalcoholareoftenatincreasedrisk ofemotionalandphysicalabuse.In thelongterm,theymayexperience pooreducationalattainmentand limitedlifechoicesandaretherefore atriskofdevelopingsubstance problemsthemselves.64
46.Nationalinformationonchildren affectedbyparentalsubstancemisuse inScotlandispoor,butitisestimated thataquarterofchildrenontheChild ProtectionRegisteraretheredueto parentalalcoholordrugmisuse.65 Thereareanestimated60,000children affectedbyparentaldrugmisuse andapproximately65,000children affectedbyparentalalcoholmisuse inScotland.66,67
Many public sector bodies commission or provide drug and alcohol services
47.Drugandalcoholservicesare generallyclassedas:
• preventionservices,suchas educationinformalorinformal settings
• treatmentandcareservices, suchascounselling,needle exchange,detoxification,relapse prevention,prescribingofchemical substitutessuchasmethadone, residentialrehabilitation,trainingor employmentservices
• enforcementandregulation activities,suchastestpurchasing operationstorestrictthesaleof alcoholtounder-agepeople,arrests fordrugdealingorinternational policeeffortstotackledrug traffickingandseizeillegaldrugs.
48.Prevention,treatmentandcare servicestoaddressdrugandalcohol misuseareoftenjointandmanystaff addressbothdrugandalcoholproblems. Moredetailsaboutwiderpartnership workingaresetoutinPart4.
49.Arangeofdrugandalcohol servicesareprovidedeitherdirectlyby councils,theNHS,policeandprisons orcommissionedfromthevoluntary andprivatesectors(Exhibit2,overleaf). Thevoluntaryandprivatesectors alsoprovideavarietyofprevention, treatmentandrehabilitationservices thatarenotfundeddirectlybythe publicsector.
50.Therearemanygenericservices thattargetpeoplewhoaresocially excludedinsocietythatalsohelp peoplewhomisusedrugsandalcohol suchasservicesforhomelesspeople. TheScottishGovernment’snew initiativetoincreasetheroleofGPs, practicenursesandhospitalA&E departmentsinscreeningandbrief interventionsforalcoholproblemsis anotherexampleofageneralservice providingsomespecialistsupport.
10
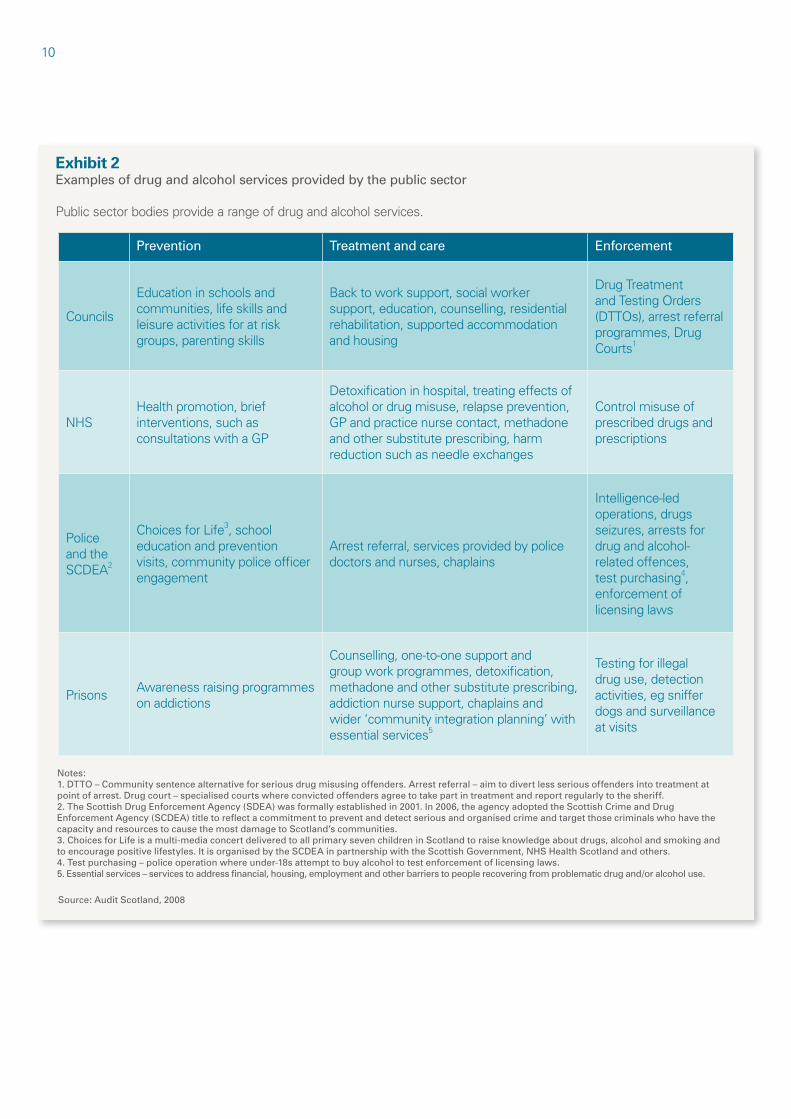
Exhibit 2 Examples of drug and alcohol services provided by the public sector
Publicsectorbodiesprovidearangeofdrugandalcoholservices.
Source: Audit Scotland, 2008
-
-
-
- -
-
Prevention Treatment and care Enforcement
Councils
Educationinschoolsand communities,lifeskillsand leisureactivitiesforat risk groups,parentingskills
Backtoworksupport,socialworker support,education,counselling,residential rehabilitation,supportedaccommodation andhousing
DrugTreatment andTestingOrders (DTTOs),arrestreferral programmes,Drug Courts1
NHS Healthpromotion,brief interventions,suchas consultationswithaGP
Detoxificationinhospital,treatingeffectsof alcoholordrugmisuse,relapseprevention, GPandpracticenursecontact,methadone andothersubstituteprescribing,harm reductionsuchasneedleexchanges
Controlmisuseof prescribeddrugsand prescriptions
Police andthe SCDEA2
ChoicesforLife3,school educationandprevention visits,communitypoliceofficer engagement
Arrestreferral,servicesprovidedbypolice doctorsandnurses,chaplains
Intelligence-led operations,drugs seizures,arrestsfor drugandalcohol- relatedoffences, testpurchasing4, enforcementof licensinglaws
Prisons Awarenessraisingprogrammes onaddictions
Counselling,one-to-onesupportand groupworkprogrammes,detoxification, methadoneandothersubstituteprescribing, addictionnursesupport,chaplainsand wider‘communityintegrationplanning’with essentialservices5
Testingforillegal druguse,detection activities,egsniffer dogsandsurveillance atvisits
Notes: 1. DTTO – Community sentence alternative for serious drug misusing offenders. Arrest referral – aim to divert less serious offenders into treatment at point of arrest. Drug court – specialised courts where convicted offenders agree to take part in treatment and report regularly to the sheriff. 2. The Scottish Drug Enforcement Agency (SDEA) was formally established in 2001. In 2006, the agency adopted the Scottish Crime and Drug Enforcement Agency (SCDEA) title to reflect a commitment to prevent and detect serious and organised crime and target those criminals who have the capacity and resources to cause the most damage to Scotland’s communities. 3. Choices for Life is a multi-media concert delivered to all primary seven children in Scotland to raise knowledge about drugs, alcohol and smoking and to encourage positive lifestyles. It is organised by the SCDEA in partnership with the Scottish Government, NHS Health Scotland and others. 4. Test purchasing – police operation where under-18s attempt to buy alcohol to test enforcement of licensing laws. 5. Essential services – services to address financial, housing, employment and other barriers to people recovering from problematic drug and/or alcohol use.
11
Part 2. Direct expenditure on drug and alcohol services
Spendingpatternsdonotreflectnationalprioritiesanddonot alwaysreflectindicatorsofneed.Fundingarrangementsare oftencomplexandfragmented.
12
Key messages
In2007/08,thepublicsector spent£173millionondrugand alcoholservicesinScotland, £84millionspecificallyondrugs servicesand£30millionon alcoholservices.Theremainder wasspentonjointdrugand alcoholservices.
Sixty-eightpercentofdrug andalcoholmoneyisspenton treatmentandcareservices. TheScottishGovernment’s recentstrategiesfordrugs andalcoholhaveafocuson preventionbutcurrentlyonly aroundsixpercentofdirect spendisonpreventative activities,includingservicesfor childrenaffectedbyparental substancemisuse.
TheamountthatNHSboards andcouncilsspendondrugand alcoholservicesvariesacross thecountry,fromalmost £14perheadofpopulationin theBorderstojustover £53inGreaterGlasgowand Clyde.Whilesomevariation wouldbeexpected,current patternsofspenddonotmatch nationalindicatorsofneedsuch aslevelsofmisuse.
Fundingarrangementsare complexandservicescanhave anumberofseparatefunding streams,eachwithdifferent timescalesandreportingcriteria. Thisisanaddeddifficultyfor thoseplanningandproviding services.
•
•
•
•
The wider costs of drug and alcohol misuse are an estimated £5 billion per year
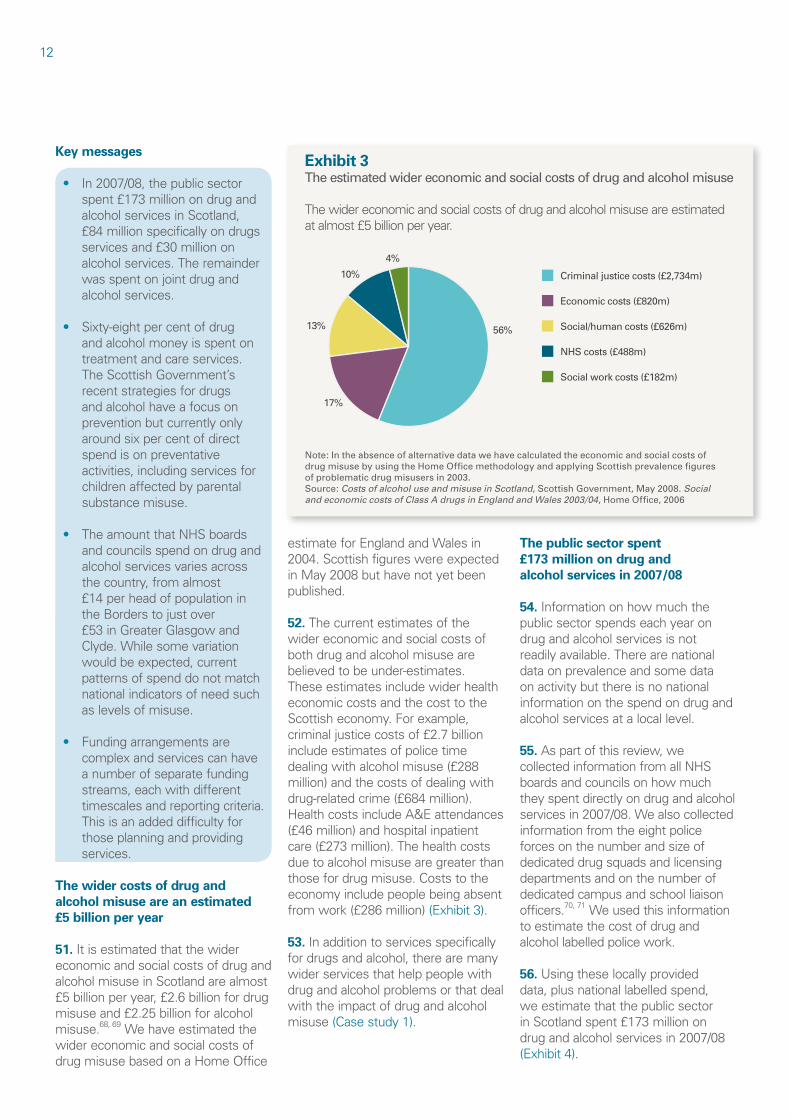
51.Itisestimatedthatthewider economicandsocialcostsofdrugand alcoholmisuseinScotlandarealmost £5billionperyear,£2.6billionfordrug misuseand£2.25billionforalcohol misuse.68,69Wehaveestimatedthe widereconomicandsocialcostsof drugmisusebasedonaHomeOffice
Exhibit 3 The estimated wider economic and social costs of drug and alcohol misuse
Thewidereconomicandsocialcostsofdrugandalcoholmisuseareestimated atalmost£5billionperyear.
Criminal justice costs (£2,734m)
Economic costs (£820m)
NHS costs (£488m)
Social/human costs (£626m)
Social work costs (£182m)
56%
17%
13%
10%
4%
Note: In the absence of alternative data we have calculated the economic and social costs of drug misuse by using the Home Office methodology and applying Scottish prevalence figures of problematic drug misusers in 2003. Source: Costs of alcohol use and misuse in Scotland, Scottish Government, May 2008. Social and economic costs of Class A drugs in England and Wales 2003/04, Home Office, 2006
estimateforEnglandandWalesin 2004.Scottishfigureswereexpected inMay2008buthavenotyetbeen published.
52. Thecurrentestimatesofthe widereconomicandsocialcostsof bothdrugandalcoholmisuseare believedtobeunder-estimates. Theseestimatesincludewiderhealth economiccostsandthecosttothe Scottisheconomy.Forexample, criminaljusticecostsof£2.7billion includeestimatesofpolicetime dealingwithalcoholmisuse(£288 million)andthecostsofdealingwith drug-relatedcrime(£684million). HealthcostsincludeA&Eattendances (£46million)andhospitalinpatient care(£273million).Thehealthcosts duetoalcoholmisusearegreaterthan thosefordrugmisuse.Coststothe economyincludepeoplebeingabsent fromwork(£286million)(Exhibit3).
53.Inadditiontoservicesspecifically fordrugsandalcohol,therearemany widerservicesthathelppeoplewith drugandalcoholproblemsorthatdeal withtheimpactofdrugandalcohol misuse(Casestudy1).
The public sector spent £173 million on drug and alcohol services in 2007/08
54.Informationonhowmuchthe publicsectorspendseachyearon drugandalcoholservicesisnot readilyavailable.Therearenational dataonprevalenceandsomedata onactivitybutthereisnonational informationonthespendondrugand alcoholservicesatalocallevel.
55.Aspartofthisreview,we collectedinformationfromallNHS boardsandcouncilsonhowmuch theyspentdirectlyondrugandalcohol servicesin2007/08.Wealsocollected informationfromtheeightpolice forcesonthenumberandsizeof dedicateddrugsquadsandlicensing departmentsandonthenumberof dedicatedcampusandschoolliaison officers.70,71Weusedthisinformation toestimatethecostofdrugand alcohollabelledpolicework.
56.Usingtheselocallyprovided data,plusnationallabelledspend, weestimatethatthepublicsector inScotlandspent£173millionon drugandalcoholservicesin2007/08 (Exhibit4).
Part2.Directexpenditureondrugandalcoholservices13
Case study 1 Examples of wider services for drugs and alcohol
Housingsupport–FabPadsupportsrecentlyhomelesspeopleandthose atriskoflosingtheirtenanciesinGlasgow.Itsupportspeopletodesignand decoratetheirhomestogivethemasenseofachievement,commitment totheirtenancyandultimatelycommitmenttomoveonintheirlives.Many oftheclientshaveproblemswithdrugsandalcoholandtheserviceoffers additionalsupporttothesepeople.In2007/08,approximately60percent ofpeopleattheservicehadaddictionproblems.Theannualcostofthe projectin2007/08inGlasgowwas£379,333.TheFabPadprojectisalso beingdeliveredinEdinburgh,Borders,NorthAyrshire,EastAyrshire,East Dunbartonshire,WestDunbartonshire,StirlingandSouthLanarkshire.
Antisocialpolicing–TheCommunityPreventionTrialinGlasgowCityCentre hasbeenrunningsince2003andaimstoreduceviolenceanddisorderinthe citycentre.Asitisestimatedthatapproximately70percentofviolentassaults inthecityarealcohol-related,thefocusoftheinitiativeisafter10pm.The projectcostsapproximately£80,000peryearandinvolvesStrathclydePolice, GlasgowCityCouncilandNHSGreaterGlasgowandClyde.
Source: Audit Scotland, 2008
Exhibit 4 Public sector spend on drug and alcohol services
Thepublicsectorspent£173millionondirectdrugandalcoholservices in2007/08.
Source: Audit Scotland, 2008
£ million
NHSboards 90
Councils 66
Policeforces 10
ScottishPrisonService 3
ScottishGovernmentdirectspend(eg,research) 4
Total 173
57.Thereare,however,differencesin thewaybudgetsarerecordedineach localareaandthewaythatservices areprovided.Manyservicesfor peoplemisusingdrugsandalcoholare deliveredaspartofgeneralservices
NHSboards 58.In2007/08,theScottish Governmentallocated£34million toNHSboardsfordrugandalcohol treatmentservices.Theseallocations haveincreasedinrecentyears:
andsofundingwillnotbelabelled asspecificallyfordrugoralcohol • Drugfundingincreasedfrom services.Thismakesitdifficulttogive almost£9millionin1998/99to comprehensivefiguresforwhatis around£24millionin2007/08. spentondrugsandalcohol.
• Alcoholfundingincreasedfrom £3millionin2004/05tojustover £10millionin2007/08.72
59.NHSboardsgenerallyaddto thismoneytoprovideservices,and in2007/08theyspentanadditional £56million(62percentoftheir totaldirectspendondrugand alcoholservices).
60.Theamountspentonalcoholand drugservicesshouldincreaseasthe ScottishGovernmenthasallocated anadditional£85.3millionforalcohol misuseoverthethreeyearsfrom 2008/09to2010/11;mostofthis moneywillgotoNHSboards (£24.8millionin2008/09).The ScottishGovernmentalsoplansto increaseallocationstoNHSboards fordrugservicesfrom£24.7millionin 2008/09to£28millionin2009/10.
Councils 61.TheScottishGovernment,in agreementwithCOSLA,allocates fundstocouncilsusinganagreed formulaknownastheGrantAided Expenditure(GAE).73TheGAEis notanallocationbutamethodfor calculatingeachcouncil’sindicative spendoneachofitsservices basedonitspopulation’sneeds.74In 2006/07,£42millionoftheGAEwas identifiedforservicesfor‘adultswith addictionandsubstancemisuse’, althoughitisacouncil’sdecisionhow tospenditsGAE.75,76
62.In2007/08,councilsspent £66millionondrugandalcohol services.Thisincludes£7.5million transferredtothemfromNHSboards.
NHSandcouncilspend 63.NHSboardsandcouncilsspent justunderonepercentoftheirtotal combinedrevenuebudgetsonlabelled drugandalcoholservicesin2007/08.
ComparisonswithEngland 64.In2005/06,governmentlabelled drug-relatedexpenditurewas estimatedat£2,695perproblematic druguserinEngland,comparedto £1,293perproblematicdruguserin Scotland.77InEngland,thereisno
14
ring-fencedfundingforalcoholservices, comparedtojustover£10millionto NHSboardsinScotlandin2007/08.
65.InEngland,significantresources havebeenallocatedtodrugservices overthelasttenyearsbyboththe DepartmentofHealthandtheHome Office.Someofthismoneywasused toestablishtheNationalTreatment Agency,aspecialhealthauthority createdtoincreasetheavailability, capacityandeffectivenessofdrug treatmentservices,andseveral intensivecriminaljusticeinterventions.
Voluntaryandprivatesectors 66.Thevoluntaryandprivate sectorsprovidemanydrugand alcoholservices.Threeofthemain independentfundersofthevoluntary sectoraretheBigLottery,LloydsTSB FoundationforScotland,Partnership DrugsInitiativeandtheRobertson Trust.TheBigLottery’sBetterOff Fundprovided£10millionover fiveyearsbetween2003and2007 tofundcommunityrehabilitation projectsforpeoplewhomisuse drugs.LloydsTSBFoundationfor Scotland,inpartnershipwiththe ScottishGovernment,provided approximately£1.2millionfordrug andalcoholservicesin2007/08and theRobertsonTrustcontributedan additional£730,000.
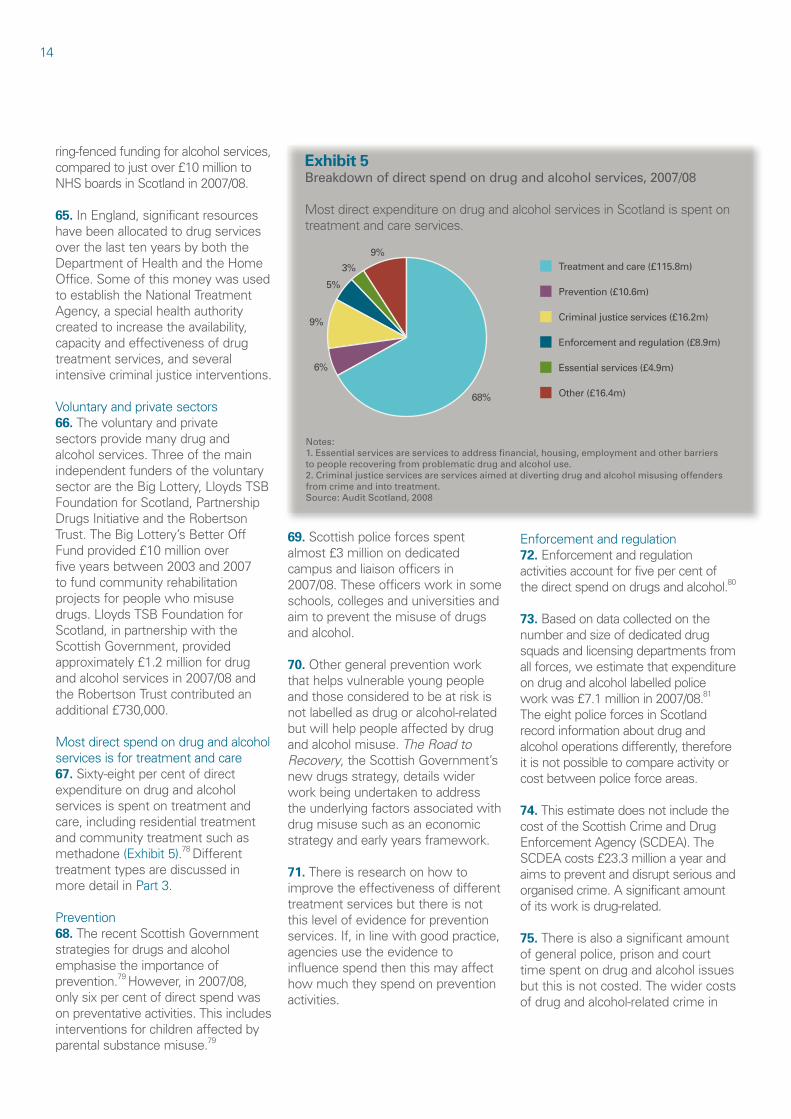
Mostdirectspendondrugandalcohol servicesisfortreatmentandcare 67.Sixty-eightpercentofdirect expenditureondrugandalcohol servicesisspentontreatmentand care,includingresidentialtreatment andcommunitytreatmentsuchas methadone(Exhibit5).78Different treatmenttypesarediscussedin moredetailinPart3.
Prevention 68.TherecentScottishGovernment strategiesfordrugsandalcohol emphasisetheimportanceof prevention.79However,in2007/08, onlysixpercentofdirectspendwas onpreventativeactivities.Thisincludes interventionsforchildrenaffectedby parentalsubstancemisuse.79
Exhibit 5 Breakdown of direct spend on drug and alcohol services, 2007/08
MostdirectexpenditureondrugandalcoholservicesinScotlandisspenton treatmentandcareservices.
Treatment and care (£115.8m)
68%
6%
9%
5%
3%
9%
Prevention (£10.6m)
Enforcement and regulation (£8.9m)
Criminal justice services (£16.2m)
Other (£16.4m)
Essential services (£4.9m)
Notes: 1. Essential services are services to address financial, housing, employment and other barriers to people recovering from problematic drug and alcohol use. 2. Criminal justice services are services aimed at diverting drug and alcohol misusing offenders from crime and into treatment. Source: Audit Scotland, 2008
69.Scottishpoliceforcesspent almost£3millionondedicated campusandliaisonofficersin 2007/08.Theseofficersworkinsome schools,collegesanduniversitiesand aimtopreventthemisuseofdrugs andalcohol.
70.Othergeneralpreventionwork thathelpsvulnerableyoungpeople andthoseconsideredtobeatriskis notlabelledasdrugoralcohol-related butwillhelppeopleaffectedbydrug andalcoholmisuse.The Road to Recovery,theScottishGovernment’s newdrugsstrategy,detailswider workbeingundertakentoaddress theunderlyingfactorsassociatedwith drugmisusesuchasaneconomic strategyandearlyyearsframework.
71.Thereisresearchonhowto improvetheeffectivenessofdifferent treatmentservicesbutthereisnot thislevelofevidenceforprevention services.If,inlinewithgoodpractice, agenciesusetheevidenceto influencespendthenthismayaffect howmuchtheyspendonprevention activities.
Enforcementandregulation 72.Enforcementandregulation activitiesaccountforfivepercentof thedirectspendondrugsandalcohol.80
73.Basedondatacollectedonthe numberandsizeofdedicateddrug squadsandlicensingdepartmentsfrom allforces,weestimatethatexpenditure ondrugandalcohollabelledpolice workwas£7.1millionin2007/08.81 TheeightpoliceforcesinScotland recordinformationaboutdrugand alcoholoperationsdifferently,therefore itisnotpossibletocompareactivityor costbetweenpoliceforceareas.
74.Thisestimatedoesnotincludethe costoftheScottishCrimeandDrug EnforcementAgency(SCDEA).The SCDEAcosts£23.3millionayearand aimstopreventanddisruptseriousand organisedcrime.Asignificantamount ofitsworkisdrug-related.
75.Thereisalsoasignificantamount ofgeneralpolice,prisonandcourt timespentondrugandalcoholissues butthisisnotcosted.Thewidercosts ofdrugandalcohol-relatedcrimein
Part2.Directexpenditureondrugandalcoholservices15
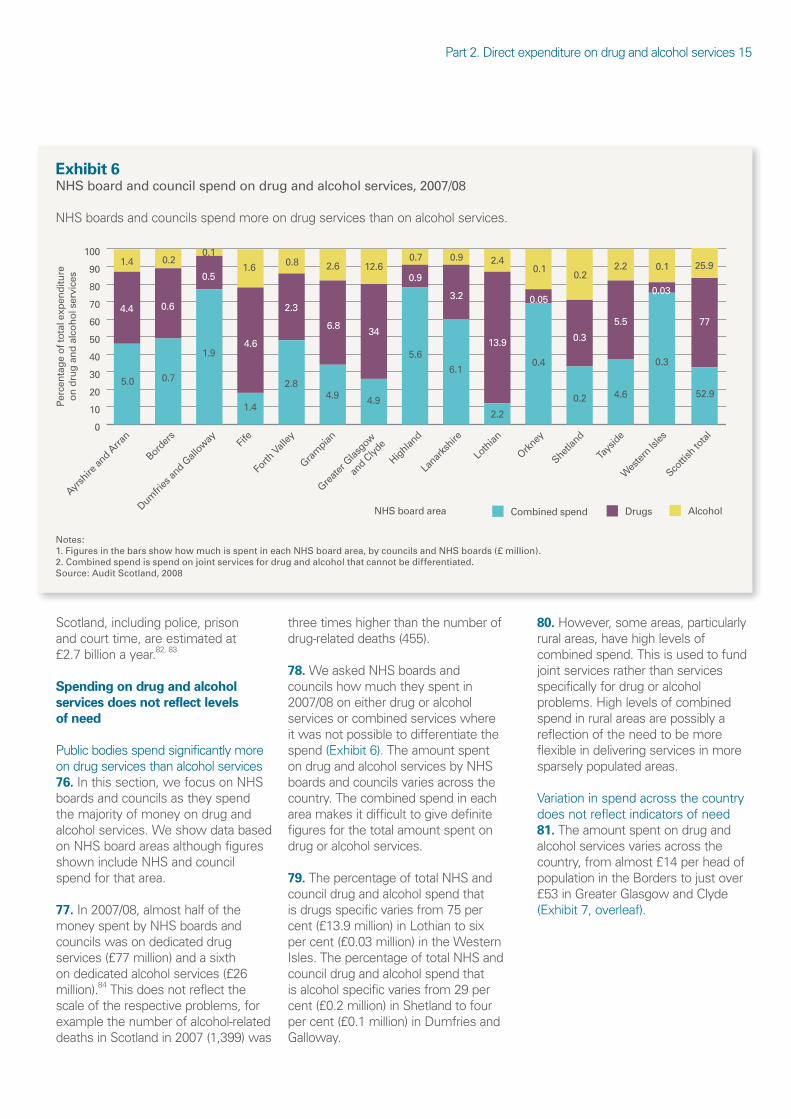
Exhibit 6 NHS board and council spend on drug and alcohol services, 2007/08
NHSboardsandcouncilsspendmoreondrugservicesthanonalcoholservices.
Notes: 1. Figures in the bars show how much is spent in each NHS board area, by councils and NHS boards (£ million). 2. Combined spend is spend on joint services for drug and alcohol that cannot be differentiated. Source: Audit Scotland, 2008
Perc
enta
ge o
f tot
al e
xpen
ditu
reon
dru
g a
nd a
lcoh
ol s
ervi
ces
NHS board area Combined spend Drugs Alcohol
0
10
20
30
40
50
60
70
80
90
100
Ayrsh
irean
d Arran
Borde
rs
Dumfri
esan
d Gallow
ay
Fife
Forth
Valle
y
Gram
pian
Greate
r Glasgo
w
and Clyd
e
Highlan
d
Lana
rkshir
e
Loth
ian
Orkney
Shetla
nd
Tays
ide
Wes
tern Isl
es
Scotti
shto
tal
1.4
5.0
0.2
0.7
0.1
1.9
1.6
1.4
0.8
2.8
2.6
4.9
12.6
4.9
0.7
5.6
0.9
6.1
2.4
2.2
0.1
0.4
0.2
0.2
2.2
4.6
0.1
0.3
25.9
52.9
4.4 0.6
0.5
4.6
2.3
6.8 34
0.9
3.2
13.9
0.05
0.3
5.5
0.03
77
Scotland,includingpolice,prison andcourttime,areestimatedat £2.7billionayear.82,83 Spending on drug and alcohol services does not reflect levels of need
Publicbodiesspendsignificantlymore ondrugservicesthanalcoholservices 76.Inthissection,wefocusonNHS boardsandcouncilsastheyspend themajorityofmoneyondrugand alcoholservices.Weshowdatabased onNHSboardareasalthoughfigures shownincludeNHSandcouncil spendforthatarea.
77.In2007/08,almosthalfofthe moneyspentbyNHSboardsand councilswasondedicateddrug services(£77million)andasixth ondedicatedalcoholservices(£26 million).84Thisdoesnotreflectthe scaleoftherespectiveproblems,for examplethenumberofalcohol-related deathsinScotlandin2007(1,399)was
threetimeshigherthanthenumberof drug-relateddeaths(455).
78.WeaskedNHSboardsand councilshowmuchtheyspentin 2007/08oneitherdrugoralcohol servicesorcombinedserviceswhere itwasnotpossibletodifferentiatethe spend(Exhibit6).Theamountspent ondrugandalcoholservicesbyNHS boardsandcouncilsvariesacrossthe country.Thecombinedspendineach areamakesitdifficulttogivedefinite figuresforthetotalamountspenton drugoralcoholservices.
79.ThepercentageoftotalNHSand councildrugandalcoholspendthat isdrugsspecificvariesfrom75per cent(£13.9million)inLothiantosix percent(£0.03million)intheWestern Isles.ThepercentageoftotalNHSand councildrugandalcoholspendthat isalcoholspecificvariesfrom29per cent(£0.2million)inShetlandtofour percent(£0.1million)inDumfriesand Galloway.
80.However,someareas,particularly ruralareas,havehighlevelsof combinedspend.Thisisusedtofund jointservicesratherthanservices specificallyfordrugoralcohol problems.Highlevelsofcombined spendinruralareasarepossiblya reflectionoftheneedtobemore flexibleindeliveringservicesinmore sparselypopulatedareas.
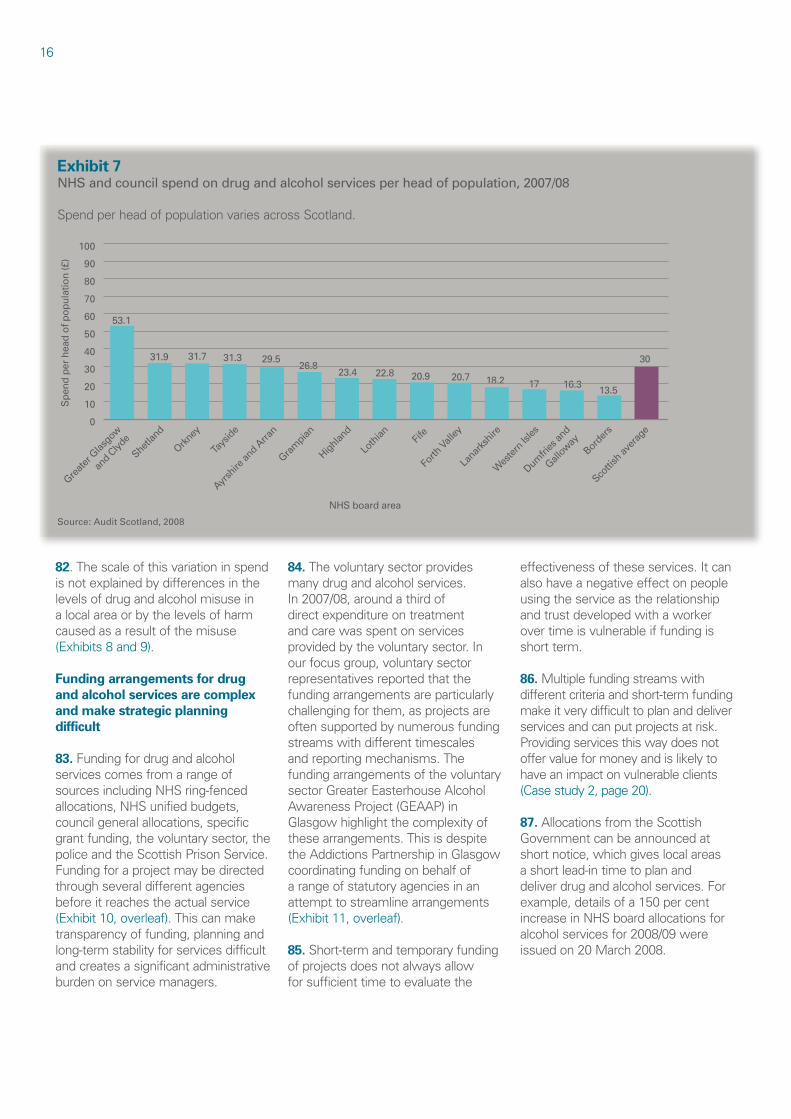
Variationinspendacrossthecountry doesnotreflectindicatorsofneed 81.Theamountspentondrugand alcoholservicesvariesacrossthe country,fromalmost£14perheadof populationintheBorderstojustover £53inGreaterGlasgowandClyde (Exhibit7,overleaf).
16
Exhibit 7 NHS and council spend on drug and alcohol services per head of population, 2007/08
SpendperheadofpopulationvariesacrossScotland.
Spe
nd p
er h
ead
of p
opul
atio
n (£
)
NHS board area
53.1
31.9 31.7 31.3 29.5 26.8
23.4 22.8 20.9 20.7 18.2 17 16.3 13.5
30
0
10
20
30
40
50
60
70
80
90
100
Greate
r Glasgo
w
and Clyd
e
Shetla
nd
Orkney
Tays
ide
Ayrsh
irean
d Arran
Gram
pian
Highlan
d
Loth
ian
Fife
Forth
Valle
y
Lana
rkshir
e
Wes
tern Isl
es
Dumfri
esan
d
Gallow
ayBor
ders
Scotti
shav
erag
e
Source: Audit Scotland, 2008
82.Thescaleofthisvariationinspend isnotexplainedbydifferencesinthe levelsofdrugandalcoholmisusein alocalareaorbythelevelsofharm causedasaresultofthemisuse (Exhibits8and9).
Funding arrangements for drug and alcohol services are complex and make strategic planning difficult
83.Fundingfordrugandalcohol servicescomesfromarangeof sourcesincludingNHSring-fenced allocations,NHSunifiedbudgets, councilgeneralallocations,specific grantfunding,thevoluntarysector,the policeandtheScottishPrisonService. Fundingforaprojectmaybedirected throughseveraldifferentagencies beforeitreachestheactualservice (Exhibit10,overleaf).Thiscanmake transparencyoffunding,planningand long-termstabilityforservicesdifficult andcreatesasignificantadministrative burdenonservicemanagers.
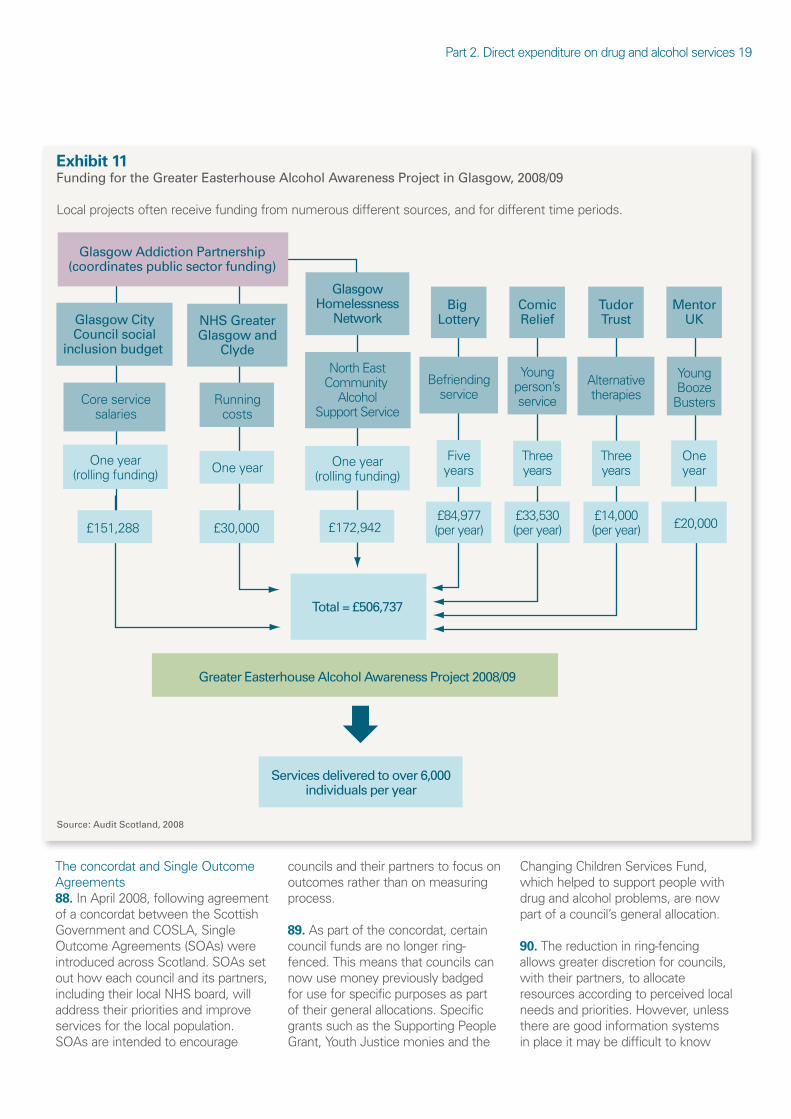
84.Thevoluntarysectorprovides manydrugandalcoholservices. In2007/08,aroundathirdof directexpenditureontreatment andcarewasspentonservices providedbythevoluntarysector.In ourfocusgroup,voluntarysector representativesreportedthatthe fundingarrangementsareparticularly challengingforthem,asprojectsare oftensupportedbynumerousfunding streamswithdifferenttimescales andreportingmechanisms.The fundingarrangementsofthevoluntary sectorGreaterEasterhouseAlcohol AwarenessProject(GEAAP)in Glasgowhighlightthecomplexityof thesearrangements.Thisisdespite theAddictionsPartnershipinGlasgow coordinatingfundingonbehalfof arangeofstatutoryagenciesinan attempttostreamlinearrangements (Exhibit11,overleaf). 85.Short-termandtemporaryfunding ofprojectsdoesnotalwaysallow forsufficienttimetoevaluatethe
effectivenessoftheseservices.Itcan alsohaveanegativeeffectonpeople usingtheserviceastherelationship andtrustdevelopedwithaworker overtimeisvulnerableiffundingis shortterm.
86.Multiplefundingstreamswith differentcriteriaandshort-termfunding makeitverydifficulttoplananddeliver servicesandcanputprojectsatrisk. Providingservicesthiswaydoesnot offervalueformoneyandislikelyto haveanimpactonvulnerableclients (Casestudy2,page20).
87.AllocationsfromtheScottish Governmentcanbeannouncedat shortnotice,whichgiveslocalareas ashortlead-intimetoplanand deliverdrugandalcoholservices.For example,detailsofa150percent increaseinNHSboardallocationsfor alcoholservicesfor2008/09were issuedon20March2008.

Part2.Directexpenditureondrugandalcoholservices17
Exhibit 8 NHS and council spend on drug and combined drug and alcohol services per 1,000 population, 2007/08
Spendondrugspecificandcombineddrugandalcoholservicesdoesnotreflectdrugmisuseprevalencerates.
Drug spend Combined drug and alcohol spend
Drug prevalance
45,000
40,000
35,000
30,000
25,000
20,000
15,000
10,000
5,000
0
30
25
20
15
10
5
0
Dru
g a
nd c
ombi
ned
dru
g a
nd a
lcoh
olla
belle
d s
pend
per
1,0
00 p
opul
atio
n (£
)
NHS board area
Drug
misuse prevalence per 1,000
population aged
15-54 years
Greate
rGlas
gow
andClyd
e
Ayrsh
irean
dArran
Tays
ide
Orkney
Shetla
nd
Gram
pian
Highlan
d
Loth
ian
Forth
Valle
y
Lana
rkshir
e
Fife
Dumfri
esan
d
Gallow
ay
Wes
tern Isl
es
Borde
rs
Note: Combined drug and alcohol spend is spend on joint services that cannot be differentiated. Source: Audit Scotland, 2008
Exhibit 9 NHS and council spend on alcohol and combined drug and alcohol services per 1,000 population, 2007/08
Spendonalcoholspecificandcombineddrugandalcoholservicesdoesnotreflectalcohol-relateddischargerates.
Alcohol spend Combined drug and alcohol spend
Alcohol-related hospital discharge rates
35,000
30,000
25,000
20,000
15,000
10,000
5,000
0
20 18 16 14 12 10 8 6 4 2 0A
lcoh
ol a
nd c
ombi
ned
dru
gs a
ndal
coho
l lab
elle
d s
pend
07/
08 p
er1,
000
popu
latio
n (£
)
NHS board area
Alcohol-related
hospital discharges 2006/07 per
1,000 population
Orkney
Greate
rGlas
gow
andClyd
e
Highlan
d
Shetla
nd
Ayrsh
irean
dArran
Tays
ide
Wes
tern Isl
es
Gram
pian
Dumfri
esan
d
Gallow
ay
Forth
Valle
y
Lana
rkshir
e Fif
e
Borde
rs
Loth
ian
Note 1. Combined drug and alcohol spend is spend on joint services that cannot be differentiated. Note 2. We have used alcohol-related hospital discharge rates as the prevalence of alcohol dependency is not available at NHS board level. Source: Audit Scotland, 2008
18
Exhibit 10 Main funding streams for drug and alcohol services, 2007/08
Fundingstreamsfordrugandalcoholservicesarecomplex.
Scottish Government
Drug and alcohol services
Unified budget
£6,870m
Resource transfer £7.5m
Alcohol treatment £10.7m
Drug treatment £23.7m
Drug treatment £23.7m
Scottish Prison Service £3m
Police forces £60m1
£1.2m
Grants, eg Fairer Scotland
Fund £435m over three years
Lloyds TSB Foundation for
Scotland
Big Lottery Fund
Robertson Trust
£10m over three years
£0.7m £66m £90m
Local councils
NHS boards
Grants to voluntary
sector £1.1m
Grants to voluntary
sector £0.5m
Drug Treatment and Testing
Orders £6.6m
Scottish Crime and Drug Enforcement
Agency £23.3m
Grant Aided Expediture (GAE)
identified for substance misuse £42m
(2006/07)
Finance and sustainable growth portfolio
Health and wellbeing portfolio
Drugs courts £1.9m
Justice portfolio
Note 1. Scottish Government estimate of police spend on drug-related crime. Source: Audit Scotland, 2008
Part2.Directexpenditureondrugandalcoholservices19
Exhibit 11 Funding for the Greater Easterhouse Alcohol Awareness Project in Glasgow, 2008/09
Localprojectsoftenreceivefundingfromnumerousdifferentsources,andfordifferenttimeperiods.
Greater Easterhouse Alcohol Awareness Project 2008/09
Total = £506,737
Services delivered to over 6,000 individuals per year
North East Community
Alcohol Support Service
One year (rolling funding)
£172,942
NHS Greater Glasgow and
Clyde
Running costs
One year
Glasgow City Council social
inclusion budget
Core service salaries
One year (rolling funding)
£151,288 £30,000
Glasgow Addiction Partnership (coordinates public sector funding)
£84,977 (per year)
Five years
Big Lottery
Befriending service
£33,530 (per year)
Three years
Comic Relief
Young person’s service
£14,000 (per year)
Three years
Tudor Trust
Alternative therapies
£20,000
One year
Mentor UK
Young Booze
Busters
Glasgow Homelessness
Network
Source: Audit Scotland, 2008
TheconcordatandSingleOutcome Agreements 88.InApril2008,followingagreement ofaconcordatbetweentheScottish GovernmentandCOSLA,Single OutcomeAgreements(SOAs)were introducedacrossScotland.SOAsset outhoweachcouncilanditspartners, includingtheirlocalNHSboard,will addresstheirprioritiesandimprove servicesforthelocalpopulation. SOAsareintendedtoencourage
councilsandtheirpartnerstofocuson outcomesratherthanonmeasuring process.
89.Aspartoftheconcordat,certain councilfundsarenolongerringfenced.Thismeansthatcouncilscan nowusemoneypreviouslybadged foruseforspecificpurposesaspart oftheirgeneralallocations.Specific grantssuchastheSupportingPeople Grant,YouthJusticemoniesandthe
ChangingChildrenServicesFund, whichhelpedtosupportpeoplewith drugandalcoholproblems,arenow partofacouncil’sgeneralallocation.
90.Thereductioninring-fencing allowsgreaterdiscretionforcouncils, withtheirpartners,toallocate resourcesaccordingtoperceivedlocal needsandpriorities.However,unless therearegoodinformationsystems inplaceitmaybedifficulttoknow
20
Case study 2 Short-term funding can have an impact on services
Aberlourisachildren’scharityprovidingservicesandadvicetovulnerable children,youngpeopleandfamiliesinScotland.
In1999,ScottishEnterprisegrantfunding(theNewFuturesFund)paid AberlourtoprovideanemploymentandtrainingservicetosubstancemisusingmotherswithdependentchildreninGlasgow.Themajorityofthese serviceusershavenotbeeninpaidemploymentandhavenotcompleted basiceducation.Inasix-monthperiod,theserviceworkedwitharound 25clients,helpingthemtoengageinfurthereducation,trainingand/or employment.
In2006,fundingforAberlourmovedtoCommunityPlanningPartnerships (CPPs).Theservicereceivedayear’sfundingfromtheCPPsin2007/08 andafterthistimealternativefundinghadtobesought.Inanyoneyear, theremaynotbeserviceusersfromeveryCPPandthisthereforemade negotiationsdifficult.Theprojectdidnotsecurefundingandhadtoclose.
Source: Audit Scotland, 2008
whetherdrugandalcoholprojects securethenecessaryfunding.
91.Drugsandalcoholarenot includedintheconcordatasaspecific commitmentandalthoughseveralof the15nationaloutcomescouldrelate todrugandalcoholmisuse,thereis nodirectlink.Allofthe32firstSOAs domentiondrugandalcoholmisuse. However,somereferencestodrugs andalcoholareverybriefandthe expectedimpactondrugandalcohol servicesisoftenunclear.
Recommendations
Thepublicsectorshould:
regularlyreviewfunding arrangementsfordrugand alcoholservicestoensurethat theymaximisevalueformoney andreflectlevelsoflocalneed
workwithprovider organisationstoreducethe impactofcomplexandshorttermfundingonprojects.
•
•
21 21
Part 3. Effectiveness of drug and alcohol services
Thereisnoconsistencyintheservicesavailable andinformationtoassesscost-effectiveness nationallyislimited.
22
Key messages
Thereisvariationacross Scotlandintherangeand accessibilityofdrugand alcoholservices.TheScottish Governmenthasnotsetout minimumstandardsinterms ofrange,choiceoraccessibility thatserviceusersandtheir familiescanexpecttoreceive.
Spendingdecisionsarenot alwaysbasedonevidence ofwhatworksoronafull assessmentoflocalneed.The majorityofdrugandalcohol servicesdonothaveclear aimsandthereisverylittle informationonwhethertheyare achievingspecificoutcomesor measuresofsuccess.
Somelocalareashave informationontheactivity,cost andimpactofdrugandalcohol servicesbutthisisnotavailable nationally.Itisnotpossibleto comparethecost-effectiveness ofdifferentservices.
•
•
•
Drug and alcohol services vary across Scotland
92.Thedrugandalcoholservicesthat peoplereceivevarydependingon wheretheylive(Casestudy3).
93.CurrentScottishGovernment policyhighlightstheneedtohavea rangeofservicesinplacetomeet individualneedsbutthereissome evidenceofalackofchoice.Drug serviceuserswhoparticipatedinour focusgrouphighlightedthattheyfeel theyhavelittlechoice:“one size fits all – you have to fit with the service, not it with you.” 85
94.Thereisnodirectionfromthe ScottishGovernmentonwhatmoney fordrugtreatmentandcareservices shoulddeliver.AlthoughtheScottish ExecutivedevelopedNational Quality Standards for Substance Misuse Servicesin2006thereisnonational monitoringofwhethertheyhave beenimplemented.86Adifferent
Case study 3 Examples of alcohol services in Tayside and Forth Valley
NHSTaysiderunstheTaysideAlcoholProblemService(TAPS).Peoplecan contacttheservicedirectlyorthroughaGPorsocialworker.
Theserviceoffersassessmentandtreatmentoptionsinsatelliteclinics acrosstheregionandhasawell-establishedresidentialfacilityinalocal hospital,whichpeoplecanalsoaccess.
NHSForthValleyrunstheCommunityAlcoholService.Peoplecancontact theservicethroughaGPorthroughSignpostForthValley,whichisadirect accessserviceforpeoplewithsubstancemisuseproblemsacrosstheForth Valleyarea.
Theserviceoffersarangeofcommunity-basedtreatmentincludinghome detoxificationthatprovidespeoplewithtreatmentintheirhomeratherthan inahospitalorotherresidentialsetting.
Source: Audit Scotland, 2008
approachistakeninEnglandwhere thegovernmenthassetoutand monitorsarequiredrangeofdrug serviceswhichshouldbeinplaceand minimumstandardsofaccess.
95.ThereisdirectionfromtheScottish Governmentonwhatadditionalmoney foralcoholservicesshoulddeliver.The ScottishGovernment’sadditional allocationof£24.8milliononalcohol servicestotheNHSin2008/09has comewithaclearinstructionto usesomeofthemoneytoprovide screeningsandbriefinterventions topreventpeoplefromdeveloping seriousproblemswithalcoholandthe remainderonsupportingadditional treatmentandpreventionservices. TheScottishGovernmenthasasked everyNHSboardtocompletea progressreportsettingouthowmuch oftheadditionalmoneytheyhave spentin2008/09andwhatservicesit hasfunded.
96.Inaddition,aspartofthenew alcoholstrategy,aMonitoringand EvaluationReferenceGroupfor Alcoholhasbeenestablishedtotrack implementationofthealcoholstrategy andrelatedoutcomes.Thisgroupis chairedbyNHSHealthScotlandand aimstoidentifytheimpactofthe additional£85.3millionoverthree yearsforalcoholmisuse.
97.Despitetheincreasedpresence ofcocaineinScotland,drugservices remainfocusedonheroinmisuse andmaynotbesetuptosufficiently meettheneedsofpeoplewho misusecocaine.TheScottishAdvisory CommitteeonDrugMisuseestimated thatonlyninepercentofdrug treatmentservicesprovidetreatment specificallyforpeoplewhomisuse drugsthathaveanti-depressantor moodelevatingproperties,suchas cocaine.Thefewspecialistservicesfor cocainemisuseareallinurbanareas, suchasAberdeenandEdinburgh.87
Prevention 98.Therearenationalinitiativesaimed atpreventingdrugandalcoholmisuse. Forexample,theKnowtheScore campaignaimstoincreaseknowledge andpromoteavoidanceofdrug misuseandhasabudgetof£580,000 for2008/09.Therearealsonational preventioninitiativesforalcohol,for exampleAlcoholAwarenessWeeks, thataimtoraiseawarenessabout alcoholconsumptionandhavea budgetof£190,000for2008/09.There isnonationalinformationcollectedon preventionactivityatalocalleveland thereisnoevaluationoftheimpactof thispreventionwork.
99.Oftenpreventionformspartof theworkoftreatmentandcare

Case study 3Examples of alcohol services in Tayside and Forth Valley
NHSTaysiderunstheTaysideAlcoholProblemService(TAPS).PeoplecancontacttheservicedirectlyorthroughaGPorsocialworker.
Theserviceoffersassessmentandtreatmentoptionsinsatelliteclinicsacrosstheregionandhasawell-establishedresidentialfacilityinalocalhospital,whichpeoplecanalsoaccess.
NHSForthValleyrunstheCommunityAlcoholService.PeoplecancontacttheservicethroughaGPorthroughSignpostForthValley,whichisadirectaccessserviceforpeoplewithsubstancemisuseproblemsacrosstheForthValleyarea.
Theserviceoffersarangeofcommunity-basedtreatmentincludinghomedetoxificationthatprovidespeoplewithtreatmentintheirhomeratherthaninahospitalorotherresidentialsetting.
Source: Audit Scotland, 2008
Part3.Effectivenessofdrugandalcoholservices23
Exhibit 12 NHS board and council spend on community and residential treatment, by NHS board area, 2007/08
ThespendoncommunitytreatmentcomparedtoresidentialtreatmentvariesacrossScotland.
Perc
enta
ge o
f tre
atm
ent s
pend
(res
iden
tial a
nd c
omm
unity
trea
tmen
t)
NHS board area Community treatment
Residential treatment
0
10
20
30
40
50
60
70
80
90
100
Ayrsh
irean
d Arran
Borde
rs
Dumfri
esan
d Gallow
ay
Fife
Forth
Valle
y
Gram
pian
Greate
r Glasgo
w
and Clyd
e
Highlan
d
Lana
rkshir
e
Loth
ian
Orkney
Shetla
nd
Tays
ide
Wes
tern Isl
es
Scotti
shav
erag
e
9% 11% 7% 10% 2% 25% 23% 18% 11% 15% 1% 14% 22% 18%
Source: Audit Scotland, 2008
91% 89% 93% 90% 98%
75% 77% 82% 89% 85%
99% 86%
78%
100% 82%
servicesandcanbedifficultto separateout.Forexample,inGreater GlasgowandClydeitisestimated thatathirdofthe£47million treatmentandcarespendwillhave animpactonchildrenaffectedby substancemisusethroughsupporting parentingandtreatingparents.
Residentialandcommunitytreatment 100.Itisimportantthatarangeof servicesisavailabletomeettheneeds ofpeoplewhomisusedrugsand alcohol,asitisunlikelythatasingle serviceortypeoftreatmentwillsuit everyone.Serviceusersshouldbe activelyinvolvedinthesedecisions.
101.Residentialtreatment, prescribingofsubstitutes(suchas methadone)andothercommunity treatment(forexamplecounselling) haveaplaceinhelpingtotreatpeople whomisusedrugsandalcohol.88
102.Theuseofresidentialdrugand alcoholservicesvariesacrossthecountry andhighlightstheissueofchoiceand accessibility.Theamountspenton communitytreatmentcomparedto residentialtreatmentvaries(Exhibit12). InsomeareasofScotland,peoplewho
misusedrugsandalcoholcanbereferred toresidentialtreatment,whileinother areasthisserviceisrarelyoffered.89 Supportinthecommunityaftera residentialplacementisimportanttolongtermpositiveoutcomesfortheindividual.
103.Thereisnocentralmonitoring ofthenumberofpeopleinresidential treatmentbuttherearesome limiteddatafrom2005/06onservice activityandentrycriteria.AScottish Governmentreportestimatedthatin 2005/06therewere352bedsavailable forresidentialtreatmentfordrugand alcoholmisuse,providedby22separate servicesacrossScotland.Thenumber ofbedsperservicerangedfromtwo to104andthecapacityofresidential servicesinScotlandwasestimated as1,670peopleperyear.In2005/06, residentialtreatmentoccupancyrates inthese22servicesvariedfrom 36percentto96percent.90Almost athirdofthebedsandserviceswere locatedinGlasgow.Thereportnoted thatareaofresidenceandagewere themainlimitingfactorsinaccessing residentialservices.Onlyoneservice acceptedpeopleunder16andathird ofthebedswereonlyavailableto Glasgowresidents.91
104.Residentialtreatmentis moreexpensiveperserviceuser thanotherformsoftreatment.In 2007/08,£19.4millionwasspent onresidentialtreatmentbyNHS boardsandlocalcouncils.In2006 inAberdeenCity,itwasestimated thattheaveragepackageofcarefor residentialrehabilitationperperson cost£20,000peryearcomparedto £3,000forcommunityrehabilitation.92 Oftenapersonaccessingresidential treatmentwillhavealreadytriedother programmestohelpthemmanage orrecoverfromtheiruseofdrugsor alcohol.
105.Methadoneprescribingisa commontreatmentinScotland,with around20,000peopleestimatedto bereceivingthesubstitutedrugin 2004.93Methadoneonitsownisa lessexpensiveoptionthanresidential treatmentandcanbeusedtohelp manageaddictiontoopiates.In 2007/08,£24.9millionwasspenton methadonetreatmentinScotland.94 Thereisnonationalestimateofthe unitcostsofmethadonetreatment butinEnglandtheaveragecostper personforayearhasbeenestimated at£1,970.95
24
106.Formethadoneprogrammesto beeffective,cliniciansneedtoregularly reviewmethadoneprescriptions withtheserviceuserandensure otherservicesareinplacetosupport them.However,theScottishAdvisory CommitteeonDrugMisusepublished areviewofmethadoneprescribingin 2007whichhighlightedthatalthough methadonewasthedrugtreatment withthemosteffectivetrackrecord, informationontheperformance ofserviceswassparseandthere wereconcernsaboutmethadone prescribinginScotland.Thereview notedproblemsrelatingto“prescribing philosophy; limited availability of treatment options in some areas; inconsistency in practice and quality of service across Scotland; effectiveness of services – in particular relating to the delivery of acceptable harm reduction and recovery outcomes, crime reduction and the safety of children.” 96
107.DrugTreatmentandTesting Orders(DTTOs)arealternativesto custodyandofferprescribedsubstitute drugtreatment,suchasmethadone, foroffendersinthecommunitywith compulsorydrugtesting.Peoplewho havemisuseddrugswhoattendedour focusgroupfeltthatakeybenefitof DTTOsisthattheyareabletokeepthe samekeyworkerandbuildtrust.The averagecostofaDTTOisestimated atjustover£18,000perserviceuser
97peryear.
108.Itisdifficulttoofferarangeof servicesforaddictioninruraland remoteareas.Theseareasoften needtotakeadifferentapproachto deliveringservicesthanmoreurban areas.Forexample,inLochaberin Highlandtherewerelimitedsocial workorsupportworkerservicesfor peoplemisusingdrugsandalcohol. StafffromNHSHighlandandHighland Councilworkasoneserviceoffering integratedsubstancemisuseservices aspartofthewidercommunity mentalhealthservice.Thisapproach hasassistedcommunicationacross theserviceandhasenabledaccess toawiderrangeofprofessional andsupportstaffforserviceusers, includingthosewithdualdiagnoses.
Servicesforfamilies 109.TheScottishGovernment highlightstheimportantrolefamilies affectedbydrugandalcoholmisuse playinhelpingpeopletorecoverin theirrecentdrugsandalcoholpolicies. TheScottishExecutiveestablished theScottishNetworkforFamilies AffectedbyDrugs(SNFAD)in2003, andtheScottishGovernmentprovided £70,000toSNFADin2007/08.SNFAD isanumbrellagroupthatsupports localfamilygroupsacrossScotland. However,ourfocusgrouphighlighted thatfamiliesinneedareoftennot awareofthesupportavailable.Thereis noequivalentorganisationforfamilies affectedbyalcoholmisuse.
Joined-upservices 110.TheScottishExecutiveprovided aseriesofoperationalguidance onintegratingtreatmentandcare services.98Despitethis,therearestill problemsinthewaythatsomeservices worktogether.Thislackofjoined-up workingaffectsspecificgroupsof peopleincludingthosewithadiagnosis ofaddictionandmentalillnessand recentlyreleasedprisoners.99
111.Generalservices,suchas housingsupportandemployment andtrainingservices,alsohave animportantroletoplaybutthe availabilityoftheseservicesfordrug andalcoholmisusersvariesacross Scotland.100
National information on needs and the impact of services is poor
112.Nationaldrugandalcohol informationexistsonprevalence, indicatorsofharmsuchashospital dischargesanddeathsandpolice informationonarrests,seizuresofillegal drugsandalcohol-relatedoffences.
113.TheScottishGovernmentfunds anationaldatabaseofdrugtreatment servicesthatrecordspeopleentering specialistdrugservices.Thisdatabase isbeingdevelopedtoprovidefollowupinformationonindividualsafter asettimeintreatment.Thereis noequivalentdatabaseforalcohol servicesandnationalinformationon
alcoholservicesisweak.However, theScottishGovernmenthasfunded researchtoestimatethecapacityof alcoholservicesinScotland.Thisisdue tobepublishedinApril2009. 114.Informationontheactivity,cost orimpactofservicesdesignedto reducedrugandalcoholproblems existsinsomelocalareasbutthe typeandqualityofdatacollectedvary acrossScotland.Nationalinformation onthecost,activityandqualityof servicesisnotavailable.
115.Thelackofconsistent, comparableandsharedinformation makesitdifficulttoplanand commissionprevention,treatmentand careservicesandtoinfluencehow servicesdevelopbasedonevidence.
116.Serviceplannersandproviders assesslocaldrugandalcoholservice needs,buttheseassessmentsareoften notdoneinanycoordinatedwayacross alocalarea.Whereneedsassessments areundertakentoinformthe developmentofservices,thisisusually onlyinrelationtoadditionalresources andoftendoneasaone-offexercise.
117.Currently,localmonitoring ofservicesgenerallyfocuseson numbersofpeopleinaserviceand activityratherthanonthequalityof theservicedeliveredortheoutcomes achieved.
118.Publicbodiesdonotroutinely evaluatetheeffectivenessofdrug andalcoholservices.Lessthan onepercentoftotalspendbyNHS boardsandcouncilsondrugand alcoholservicesisusedforresearch andevaluationpurposes.Thereare, however,someexamplesofgood practicewheretherehasbeena comprehensivereviewofalldrug andalcoholservicesinanarea (Casestudy4).Agenciesplanning andprovidingservicesinGlasgow, Edinburgh,AberdeenandAyrshire establishedaworkinggroupin2008 tobenchmarkdrugandalcohol servicesinScotland.Thisworkisstill atanearlystage.
Part3.Effectivenessofdrugandalcoholservices25
Localcost-effectiveness 119.Therearenocomparableunit costsfordrugandalcoholservices inScotland(withtheexception ofcriminaljusticeinterventions) tohelplocalareasevaluatecost- effectivenessofservices.InEngland, thegovernmentisconsultingon guidancesettingoutunitcostsfor varioustreatments.
The impact of drug and alcohol services is not known at a national level
120.Thereisnoconsistent understandingofwhatthemoney spentondrugandalcoholservices hasbought.TheScottishGovernment hasnotdefinedwhatconstitutesa ‘service’,an‘intervention’,orany measuresofsuccessforservices.
121.Fundingfordrugandalcohol servicesgenerallydoesnothaveclear aimsorexplicitoutcomesattached. Aspartofourfieldwork,wefound thatmanyservicesdidnothavea servicelevelagreement,contract orservicespecificationthatstated theexpectedactivityoroutcomeof thefunding.Theuseofservicelevel agreementsandcontractsvaried acrossthecountry.
Outcomes 122.Althoughdemonstratingbenefits fromthespendingondrugand alcoholservicesiscomplex,there aresomeexamplesofgoodpractice wherepublicsectorbodieshave changedthewayinwhichtheywork tofocusonoutcomes(Casestudy5).
123.TheScottishGovernmentchairs theDeliveryReformGroup,which itestablishedin2008toadvise ministersonhowtoimprovedelivery arrangementsfordrugandalcohol servicesandensurebetteroutcomes forserviceusers.Asubgroupofthe DeliveryReformGroupdeveloped anoutcomestoolkitfordrugand alcoholservicesinJanuary2009 (Exhibit13,overleaf).Basedonthe proposalsoftheDeliveryReform Grouptheseoutcomemeasureswill notbemandatorybutmaybeusedby
Case study 4 Comprehensive review of addiction services in Greater Glasgow
Before the review:In2003,addictionservicesinGreaterGlasgowwererun acrossthreeagencies:NHSDrugProblemService,NHSAlcoholandDrug DirectorateandSocialWorkAddictionservices.Theservicepeoplereceived dependedonwheretheylived.
The review:Aseriesofstrategicreviewsfocusedondifferentservicessuch ascouncilservices,homelessservicesandservicespaidforbytheNHS andcouncilbutdeliveredbyothers(eg,residentialservices).Eachstrategic reviewincludedneedsassessments,ananalysisoflevelsofcurrentuse andserviceuserviewsandaliteraturereviewofeffectiveness.Allthis informationwassharedacrossagencies.
After the review:Thereisnowasinglepartnershipwithresponsibilityfor theplanningandperformanceofdrugandalcoholservicesacrossGreater Glasgow.Thereare13CommunityAddictionTeamsacrossGreaterGlasgow withasinglemanagementstructure,forbothNHSandcouncil,andsingle accountability.Theservicehas580staffandabudgetof£42millionperyear, whichismanagedthroughajointfinancialframework.
Source: Audit Scotland, 2008
Case study 5 Outcome-based service development in West Lothian
WestLothianAlcoholandDrugActionTeam(ADAT)hasdevelopedaseries ofstagestohelptocommissionservicesbasedonoutcomemeasures.
Stage 1 analysis – building the evidence base.Regularneedsassessment andresearchintowhatworkstoprovideevidencetoinformfundingdecisions.
Stage 2 planning – specifying the outcomes.Alocaloutcomeframework isagreedbasedonneedsassessments.Thefocusisontheoutcomesthat providersmustachieveandhowtheywillachievetheseoutcomesisnotset outinadvance.Potentialserviceproviderssubmitanoutcomespecification andanoutcomedeliveryplanrecordshowtheproviderwillachievethe outcomesandwhatfundingisneededtodelivertheproject.Anoutcome milestonechartisusedtoidentifykeyclientstagesandcapacityinthe service.Alltendersareevaluatedagainstspecificcriteria.
Stage 3 doing – outcome contracting.Successfulproviderssubmit quarterlymonitoringtemplateswhicharefocusedonoutcomes.All successfulprovidersarealsorequiredtocompleteequalityimpact assessments,whicharereviewedonanongoingbasis. Source: Audit Scotland, 2008
servicesandrecordedthroughSOAs. 124.Giventhelackofconsistenthigh- Itwillbeimportantforlocalareasto qualityperformancemanagementdata havebaselineinformationagainst andthatnewoutcomemeasuresare whichtomeasuretheirperformance. proposedasoptional,comprehensive Theproposalsdonotincludeanyplans andcomparableoutcomeinformation tomonitorwhichareasimplement willnotbeavailableacrossScotland theseoutcomes. inthenearfuture.Thiscontrastswith
thedevelopmentinEnglandover
26
recentyearsofasystemfornational perfomancemanagementand accountability,whichcombinesservice datawithunitcosts. 125.Theimpactofenforcementactivity iscomplex.Arrestsanddrugseizures areincreasingovertimebuttheimpact thatthishasontheavailabilityofillegal drugsorScotland’sdrugproblemisnot known.RecentresearchbytheUnited KingdomDrugPolicyCommission highlightsthelackofevidenceof effectivenessofenforcementactivity.101
126.Whiletherearesomeexamples ofgoodpracticeintermsofreviewing servicesandprovidingintegrated services,thisisnotroutinelysharedto helpimproveservicesacrossScotland.
127.ThepublicsectorinScotland shoulduseaconsistentperformance frameworktohelpthemtobenchmark servicesandperformance.Aselfassessmentchecklistissetoutat Appendix4,whichaimstohelppartners improvethedeliveryandimpactofdrug andalcoholservicesintheirlocalareain aconsistentwayacrossScotland.
Recommendations
Exhibit 13 Scottish Government example outcomes for drug and alcohol services
Drug specific:
Reductionindrug-relatedmorbidity,mortalityanddeaths.
Lessdrug-relatedcrime–acquisitive,violent,organised.
Alcohol specific:
Reducealcohol-relatedinjuries,physicalandpsychological morbidityandmortality.
Lessalcohol-relatedviolence/abuse/offencesandantisocialbehaviour.
Drug and alcohol:
Saferandhappierfamiliesandcommunities.
Reducednumberofchildrenlookedafterandaccommodated/separated fromparents.
Increasesinyoungpeoplecompletingschool,collegeortraining.
Reductioninchildren’sexposuretosubstancemisuse.
Increasedproductivityintheworkplace.
Reductioninadultsonbenefitsduetodrug/alcohol-relatedincapacity.
Lessabsenteeism/lostproductivitycausedbydruguse/alcohol consumptionintheworkplaceandeducationalestablishments.
•
•
•
•
•
•
•
•
•
•
•
Source: Scottish Government, 2009
TheScottishGovernmentand publicsectorbodiesshould:
workcloselytogetherto developaperformance frameworkincorporating,but notlimitedto,existingtargets. Furtherworkisrequiredto identifyinformationonspend, activityandoutcomes
ensurethatthereisa comprehensiverangeofservices availableineachlocalarea
developunitcostinformation fordifferentdrugandalcohol servicestohelppublicbodies measureandcomparethecost- effectivenessofvariousservices.
•
•
•
TheScottishGovernmentshould:
setclearnationalminimum standardsfordrugandalcohol servicesincludingtheirrange, qualityandaccessibility; receiveassurancethatthese standardsareimplementedin linewithsettimescales;and ensureperformanceisregularly monitoredandpubliclyreported.
Publicsectorbodiesshould:
ensurethatalldrugandalcohol servicesarebasedonan assessmentoflocalneedand thattheyareregularlyevaluated toensurevalueformoney.This informationshouldthenbe usedtoinformdecision-making inthelocalarea
•
•
ensurethatservice specificationsareinplaceforall drugandalcoholservicesand setoutrequirementsrelating toserviceactivityandquality. Whereservicesarecontracted thisspecificationshouldbepart ofaformalcontract
setclearcriteriaofeffectiveness andexpectedoutcomesfor thedifferentservicesthatthey provide,andundertakeregular auditstoensureservices adheretoexpectedstandards
usetheAuditScotlandchecklist detailedinAppendix4tohelp improvethedeliveryandimpact ofdrugandalcoholservices throughajoined-up,consistent approach.
•
•
•

27
Part 4. Drug and alcohol partnerships
Drugandalcoholpartnershipshavebeeninplace sincethelate1980sbuttheyhavenotallachievedthe objectivessetforthem.
28
Key messages
Partnershipsfordrugsand alcoholhavebeeninplacesince thelate1980s.Limitednational guidancehasbeenissuedto partners,despitethecreation ofnewpartnershipbodiesand advancesinunderstandingthe problemsofdrugandalcohol misuse.
Giventhelimitedguidance,drug andalcoholpartnershipshave evolvedtoworkindifferent waysacrossScotland.Some partnershipshaveoperated strategicallywhileothershavehad amoredetailedfocusonspecific services.Notalldrugandalcohol partnershipshaveachievedthe objectivessetforthem.
Therearemanypublicsector bodiesinvolvedindelivering drugandalcoholservices,each withdifferentaccountabilityand governancearrangements.A clearerstructurefororganising resourcesfordrugandalcohol servicesinScotlandisneeded, alongsideclarityabouttheroles ofservicesandpartnersand howtheyshouldlinktogether.
•
•
•
A lack of central guidance has led to variation in how local partnerships operate
128.Manypublicsectorbodies contributetoaddressingdrugand alcoholproblemsinsomeway.NHS boards,councils,thepoliceandthe prisonserviceallplayapart.Although theseagenciesaddressdrugandalcohol problemsthroughtheroutinework theydo,suchascitycentrepolicingat weekends,thesepartnersshouldalso cometogethertojointlyplanservices andshareresourcestotackledrugand alcoholproblemswithinalocalarea.
129.Sincethelate1980s,partnership bodieshavebeentaskedwith developingcross-cuttinglocal responsestonationalgovernment strategiesfordrugsandalcohol.These partnershipbodieshavebeenknown
asAlcoholMisuseCoordinating Committees,DrugActionTeams, AlcoholActionTeamsandAlcoholand DrugActionTeams(ADATs).
130.TheScottishExecutivepublished adetailedremitforDrugAction Teamsin1995.Thisguidancewas updatedin2002whenAlcohol ActionTeamsandjointAlcoholand DrugActionTeamswerebeing formedlocally.Theaimsforthese partnershipssetin1995wereto:
• collectandshareinformationto assessthelocaldrugproblem
• ensureeffectiveprevention measuresaredeveloped
• assessiftherangeandqualityof servicesmeetsneeds,andplanand initiateimprovementswhereneeded
• ensurecommunityviewsare takenonboard
• ensureregularevaluationand reviewsareundertakenofservices andactivitieswithaviewto improvingefficiency.
131.Eachlocalpartnershiphas developedadifferentfocus: performancemonitoringhasbeen poorinsomeareas,involvementof localcommunitieshasbeenvariable andpartnershipswereoftenable toinfluenceonlyasmallproportion ofmoneyspentinanareaondrug andalcoholservices.Insomeareas, ADATshaveactedascommissioning bodies,whileinotherstheyhavehad astrategicplanningrole.
132.Despitesignificantchanges inthewaydrugandalcohol servicesoperateandadvancesin understandingtheproblemsofdrug andalcoholmisuse(includingthe impactonchildprotection),theremit ofdrugandalcoholpartnershipshas notbeenrevisedsince2002.The ScottishGovernmentplanstoissue revisedguidanceondrugandalcohol partnershipsinspring2009,based onproposalsmadetheDelivery ReformGroup.
Not all drug and alcohol partnerships have achieved the objectives set for them
133.Althoughitisnotpossibleto assesstheperformanceofdrug andalcoholpartnershipsagainstthe revisedguidance,itispossibletolook atwhetherpreviousexpectations havebeenmet,andtocompare theoriginalexpectationswiththe proposedexpectations(Exhibit14).
134.Ingeneral,ADATshavenot achievedwhatwasexpectedof thembutthereareexamplesofgood practice.Forexample,inMoray, OperationAvonaimstoreducethe amountofstreetdrinkingamong underageyouthsandofferssupport andadviceatanearlystagetothose whomayalreadybesufferingthe adverseaffectsofalcoholmisuse. ThisinitiativeinvolvesGrampian Police,NHSGrampian,Moray Council,MoraySocialandHealth CarePartnerships,MorayDrug andAlcoholService,MorayYouth JusticeandCommunityLearningand Development.
The roles and responsibilities of drug and alcohol partnerships are still unclear
135.TheScottishGovernmentplans toissuerevisedguidanceondrugand alcoholpartnershipsinspring2009. Theguidancewasoriginallyplanned tobepublishedinNovember2008.
136.Thisrevisedguidancewillbethe resultoffouryears’workatanational leveltoreviewlocalAlcoholandDrug ActionTeams.In2005,thethen JusticeMinisteraskedforareview oftheeffectivenessandperformance ofADATsinrelationtodrugservices. Thiswasfollowedin2007withthe ScottishExecutive’sReport of the Stocktake of Alcohol and Drug Action Teams.
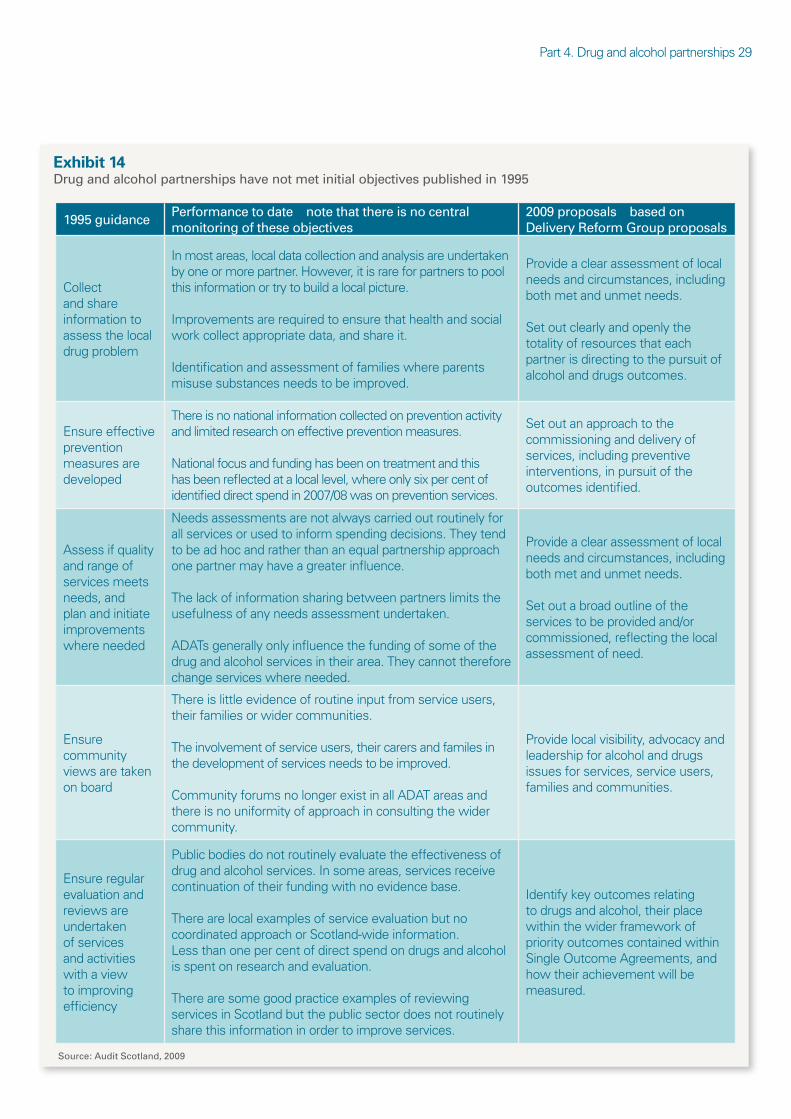
Part4.Drugandalcoholpartnerships29
Exhibit 14 Drug and alcohol partnerships have not met initial objectives published in 1995
1995 guidance Performance to date note that there is no central monitoring of these objectives
2009 proposals based on Delivery Reform Group proposals
Collect andshare informationto assessthelocal drugproblem
Inmostareas,localdatacollectionandanalysisareundertaken byoneormorepartner.However,itisrareforpartnerstopool thisinformationortrytobuildalocalpicture.
Improvementsarerequiredtoensurethathealthandsocial workcollectappropriatedata,andshareit.
Identificationandassessmentoffamilieswhereparents misusesubstancesneedstobeimproved.
Provideaclearassessmentoflocal needsandcircumstances,including bothmetandunmetneeds.
Setoutclearlyandopenlythe totalityofresourcesthateach partnerisdirectingtothepursuitof alcoholanddrugsoutcomes.
Ensureeffective prevention measuresare developed
Thereisnonationalinformationcollectedonpreventionactivity andlimitedresearchoneffectivepreventionmeasures.
Nationalfocusandfundinghasbeenontreatmentandthis hasbeenreflectedatalocallevel,whereonlysixpercentof identifieddirectspendin2007/08wasonpreventionservices.
Setoutanapproachtothe commissioninganddeliveryof services,includingpreventive interventions,inpursuitofthe outcomesidentified.
Assessifquality andrangeof servicesmeets needs,and planandinitiate improvements whereneeded
Needsassessmentsarenotalwayscarriedoutroutinelyfor allservicesorusedtoinformspendingdecisions.Theytend tobeadhocandratherthananequalpartnershipapproach onepartnermayhaveagreaterinfluence.
Thelackofinformationsharingbetweenpartnerslimitsthe usefulnessofanyneedsassessmentundertaken.
ADATsgenerallyonlyinfluencethefundingofsomeofthe drugandalcoholservicesintheirarea.Theycannottherefore changeserviceswhereneeded.
Provideaclearassessmentoflocal needsandcircumstances,including bothmetandunmetneeds.
Setoutabroadoutlineofthe servicestobeprovidedand/or commissioned,reflectingthelocal assessmentofneed.
Ensure community viewsaretaken onboard
Thereislittleevidenceofroutineinputfromserviceusers, theirfamiliesorwidercommunities.
Theinvolvementofserviceusers,theircarersandfamilesin thedevelopmentofservicesneedstobeimproved.
CommunityforumsnolongerexistinallADATareasand thereisnouniformityofapproachinconsultingthewider community.
Providelocalvisibility,advocacyand leadershipforalcoholanddrugs issuesforservices,serviceusers, familiesandcommunities.
Ensureregular evaluationand reviewsare undertaken ofservices andactivities withaview toimproving efficiency
Publicbodiesdonotroutinelyevaluatetheeffectivenessof drugandalcoholservices.Insomeareas,servicesreceive continuationoftheirfundingwithnoevidencebase.
Therearelocalexamplesofserviceevaluationbutno coordinatedapproachorScotland-wideinformation. Lessthanonepercentofdirectspendondrugsandalcohol isspentonresearchandevaluation.
Therearesomegoodpracticeexamplesofreviewing servicesinScotlandbutthepublicsectordoesnotroutinely sharethisinformationinordertoimproveservices.
Identifykeyoutcomesrelating todrugsandalcohol,theirplace withinthewiderframeworkof priorityoutcomescontainedwithin SingleOutcomeAgreements,and howtheirachievementwillbe measured.
Source: Audit Scotland, 2009
30
137.TheDeliveryReformGroup’s proposalshavesetoutgeneral principlesforpartnersand partnerships,whichareinlinewith previousguidance(Exhibit14).These havestilltobeapprovedbyministers. Ifapproved,furtherworkisneeded toclarifyhowtheseproposalswill beimplementedconsistentlyacross Scotlandandwhatrolevoluntary sectorpartnerswillplay.
138.Underthenewproposals,drug andalcoholpartnershipswillsitwithin CommunityPlanningPartnerships (CPPs).Ifthereismorethanone drugandalcoholpartnershipina NHSboardareathepartnershipswill beexpectedtocoordinateactivity. Thelocalpartnershipswillbeheld accountableforSingleOutcome Agreementcommitmentsthrough CPPsandforhealthtargetsthrough NHSpartners.Ahealthtargetfor alcoholwasintroducedin2008to provideanagreednumberofbrief interventionsthataimtoprevent peopledevelopingalcohol-related problems.Ahealthtargetfordrug misusewillbeintroducedin2009/10 andwillfocusonwaitingtimesfor services.Thedetailsofthistargetare stillunclear.
139.Thereare32councils,14NHS boards,eightpoliceforcesandeight CommunityJusticeAuthorities,each withdifferentboundaries.102The 22ADATsinScotlandhavetowork witheachofthesebodies.Todate, theyhavefounditdifficulttoensure thatdrugsandalcoholarepriorities ineachlocalarea,notleastbecause ofthevarietyofagenciestheymust workwith(Exhibit15).Newguidance needstohelptoclarifyaccountability andgovernancearrangementsand prioritysetting.
140.IntheGreaterGlasgowand Clydearea,localNHSboardand councilpartnershaveworkedto streamlinetheirapproachtothe planning,deliveryandperformance managementofdrugandalcohol services.Thishasfocusedonthe creationofasingleAddictions Partnershipprovidingasingleplanning
structureacrossallareasandincludes CPPsandCommunityHealthand CarePartnerships(CHCPs).
141.Thenewproposalsforlocal drugandalcoholpartnershipsinclude thedevelopmentofanational supportfunctionwithintheScottish Governmenttohelplocalpartnerships achieveimprovementsforpeople whomisusedrugsandalcohol.Itis envisagedthatsupportcoordinators willworkinlocalareastosupport amovetoanoutcomes-based approach,tocaptureandsharebest practiceandtofacilitatediscussions betweenpartners.Therewouldbeno scrutinyroleforsupport coordinatorsbuttheywillworkin areasthataskfortheirhelp.The ScottishGovernmenthopesthat theoutcomestoolkitfordrugand alcoholserviceswillalsohelplocal areasmovetoanoutcomes-based approach.
Recommendations
TheScottishGovernmentshould:
clarifyaccountabilityand governancearrangementsfor thedeliveryofdrugandalcohol servicesinScotlandandsetout clearlytheresponsibilitiesofall organisationsandpartnerships involvedinplanningordelivering theseservices
systematicallyidentifyand disseminategoodpractice –includingthedetailsof localdrugandalcohol-related interventionsandtreatments.
Publicsectorbodiesshould:
ensurethatdrugandalcohol partnersareclearabouttheir roleindeliveringeffectiveand joined-updrugandalcohol servicesinScotland
•
•
•
putsystemsinplaceto routinelyengagewithservice usersandtheirfamiliesto ensurethattheirviewsinform thedevelopmentofdrugand alcoholservicestoaddress localneeds.
•
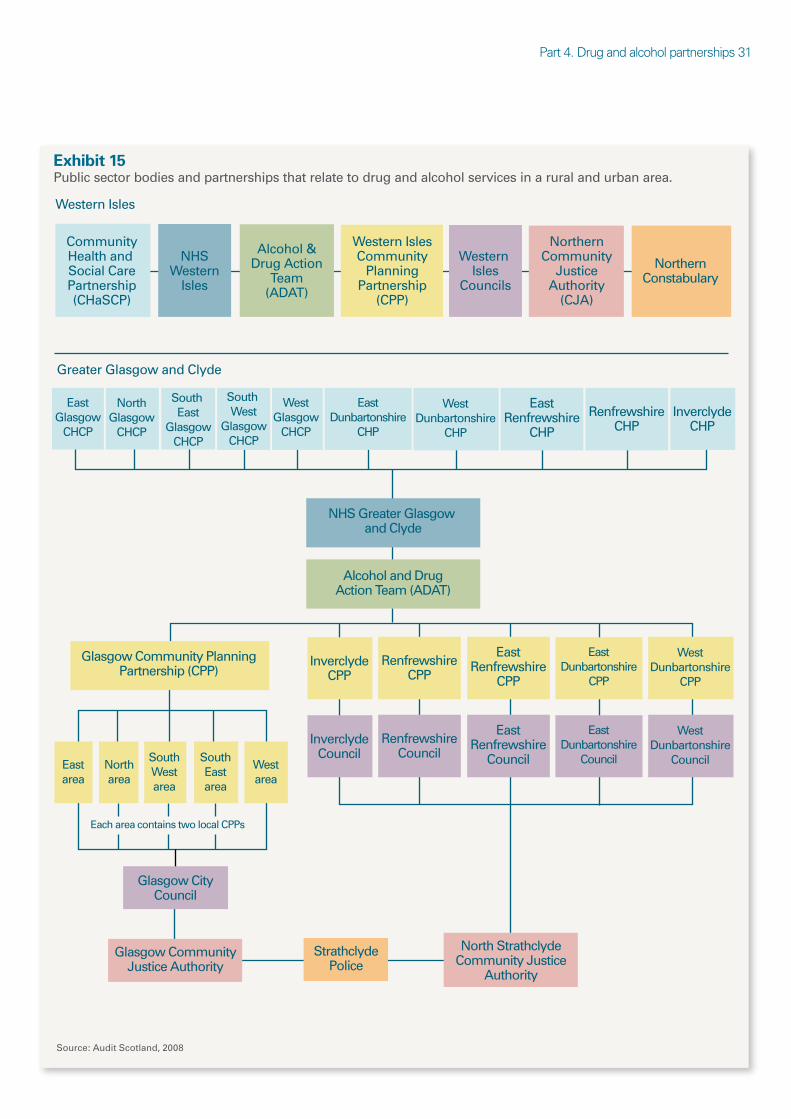
Part4.Drugandalcoholpartnerships31
Exhibit 15 Public sector bodies and partnerships that relate to drug and alcohol services in a rural and urban area.
Community Health and Social Care Partnership (CHaSCP)
NHS Western
Isles
Western Isles
Greater Glasgow and Clyde
Alcohol & Drug Action
Team (ADAT)
Western Isles Community
Planning Partnership
(CPP)
Western Isles
Councils
Northern Community
Justice Authority
(CJA)
Northern Constabulary
East Glasgow
CHCP
North Glasgow
CHCP
South East
Glasgow CHCP
South West
Glasgow CHCP
West Glasgow
CHCP
East Dunbartonshire
CHP
East Dunbartonshire
CPP
West Dunbartonshire
CHP
East Renfrewshire
CHP
East Renfrewshire
CPP
Renfrewshire CHP
Renfrewshire CPP
Inverclyde CHP
NHS Greater Glasgow and Clyde
Alcohol and Drug Action Team (ADAT)
North area
South West area
South East area
Glasgow City Council
Glasgow Community Justice Authority
North Strathclyde Community Justice
Authority
Strathclyde Police
East Dunbartonshire
Council
West Dunbartonshire
Council
East Renfrewshire
Council
Renfrewshire Council
Inverclyde Council
Inverclyde CPP
West Dunbartonshire
CPP
East area
Glasgow Community Planning Partnership (CPP)
West area
Each area contains two local CPPs
Source: Audit Scotland, 2008
332 2
Appendix 1. Notes to the text
Notes to Summary
1 Drug misuse and the environment,TheAdvisoryCouncilfortheMisuse ofDrugs,1998.
2 Alcohol Statistics Scotland 2008,InformationServicesDivision(ISD) Scotland,2009.
3 PriortoSeptember2007,theScottishAdministrationwasgenerally referredtoastheScottishExecutive.Sincethechangeinadministration itisnowcalledtheScottishGovernment.Whendealingwiththeearlier periodthisdocumentreferstotheScottishExecutive.
4 The Road to Recovery: a new approach for tackling Scotland’s drug problem,ScottishGovernment,2008.
5 Changing Scotland’s Relationship with Alcohol: A framework for action, ScottishGovernment,2009.
6 Wehavedefinedlabelledexpenditureasdirectidentifiableexpenditure fordrugand/oralcoholspecificservicesorspecificdrugand/oralcohol- relatedcontributionsforuseinotherservices,forexample,adedicated addictionsworkerinahousingproject.
Notes to Part 1
7 MinisterialAdvisoryCouncilontheMisuseofDrugs,1982. 8 International statistical classification of diseases and related health
problems,10threvision,WorldHealthOrganisation,2007. 9 Estimating the National and Local Prevalence of Problem Drug Misuse
in Scotland,GordonHay,MariaGannon,NeilMcKeganey,Sharon HutchinsonandDavidGoldbery,2004.
10 Local and national estimates of the prevalence of opiate use and/or crack cocaine use (2004/05),GordonHay,MariaGannon,JaneMacDougall, TimMillar,CatherineEastwood,NeilMcKeganey,2006.
11 ScottishDrugMisuseDatabase,ISDScotland. 12 Psychostimulant Project Group Report,ScottishGovernment,2008. 13 2007 National Report to the EMCDDA,UKFocalPointonDrugs,
October2007. 14 HepatitisCisablood-borneinfection.Mostcasesoccurinpeoplewho
shareneedlescontaminatedwithtracesofbloodtoinjectillegaldrugs. Aftermanyyearsofinfectionsomepeopledevelopcirrhosis,andafew developlivercancer.
15 http://www.hps.scot.nhs.uk/bbvsti/Hepatitisc.aspx?subjectid=93 16 Drug Misuse Statistics Scotland 2008,ISDScotland,2008. 17 Themedianisthemiddlevalueofanorderedsetofdata. 18 Drug Misuse Statistics Scotland 2008,ISDScotland,2008. 19 Ibid. 20 2007 National Report to the EMCDDA,UKFocalPointonDrugs,
October2007. 21 Scottish Schools Adolescent Lifestyle and Substance Use Survey
(SALSUS),BMRBSocialResearch,2006. 22 Drug Misuse Statistics Scotland 2008,ISDScotland,2008. 23 Ibid. 24 Ibid. 25 2007 National Report to the EMCDDA,UKFocalPointonDrugs,
October2007. 26 Drug related deaths in Scotland in 2007,GeneralRegisterOfficefor
Scotland,2008. 27 Althoughnationallydrug-relateddeathsareincreasingthereislocalvariation. 28 Drug related deaths in Scotland in 2007,GeneralRegisterOfficefor
Scotland,2008. 29 Drug seizures by Scottish police forces,ScottishExecutive,2007. 30 Drug seizures by Scottish police forces 2005/06 and 2006/07,Scottish
Government,June2008. 31 Therearethreecategoriesofillegaldrugseachwithdifferentpenalties
forpossessingordealing.ClassA,BandCdrugsaredetailedunderthe MisuseofDrugsAct1971,withClassAconsideredthemostharmful.
32 Scottish Crime and Victimisation Survey,ScottishExecutive,2006. 33 ScottishDrugMisuseDatabase,ISDScotland. 34 The Road to Recovery: a new approach for tackling Scotland’s drug
problem,ScottishGovernment,2008. 35 Alcohol needs assessment research project (ANARP): the 2004
national alcohol needs assessment for England,DepartmentofHealth, November2005.
36 Psychiatric morbidity among adults living in private households 2000, OfficeofNationalStatistics,2002.
37 Alcohol: price, policy and public health,ScottishHealthActiononAlcohol Problems,2008.
38 Ibid. 39 NeilsenRetailTracking,2008. 40 ScottishHealthSurvey,ScottishExecutive,2003. 41 Scottish Schools Adolescent Lifestyle and Substance Use Survey
(SALSUS),BMRBSocialResearch,2006. 42 Harmful Drinking,NHSQualityImprovementScotland,2006. 43 Alcohol Statistics Scotland 2008,ISDScotland,2009. 44 Findingsfromrandomlyselectedtendayperiodin2005intenA&E
departmentsinHarmful drinking: The size of the problem,NHSQuality ImprovementScotland,2006.
45 Alcohol Statistics Scotland 2008,ISDScotland,2009. 46 Abriefinterventionisadiscussionaimedatmotivatingorsupporting
someonetotrytochangetheirbehaviour.Itisoftenadiscussion betweenaGPandtheirpatient.
47 http://www.gro-scotland.gov.uk/statistics/deaths 48 Ibid. 49 Health Statistics Quarterly,OfficeofNationalStatistics,spring2007. 50 Health in Scotland 2007, AnnualreporttotheChiefMedicalOfficer,2008. 51 Alcohol: price, policy and public health,ScottishHealthActiononAlcohol
Problems,2008. 52 Changing Scotland’s Relationship with Alcohol: a discussion paper on our
strategic approach,ScottishGovernment,2008. 53 UnpublisheddatasuppliedtotheScottishGovernmentbyStrathclyde
Police,2007. 54 Alcohol and intimate partner violence:keyfindingsfromtheresearch,
HomeOffice,2004. 55 Homicide in Scotland 2007-2008,ScottishGovernment,2007. 56 Deprivedcommunitiesareidentifiedbylookingatindicatorsthatshow
disadvantageinthepopulation,suchasincome,employment,education, housing,healthandgeographicalaccess.
57 Drug Misuse and the Environment,TheAdvisoryCouncilfortheMisuse ofDrugs,1998.
58 http://www.drugscope.org.uk/resources/faqs 59 Alcohol Statistics Scotland 2008,ISDScotland,2009. 60 Mind the Gaps: Meeting the needs of people with co-occurring
substance misuse and mental health problems,ScottishExecutive,2003. 61 Survey of the health and well-being of homeless people in Glasgow,A
Kershaw,NSingletonandHMeltzer,2000. 62 Prison Health in Scotland: A health care needs assessment,Scottish
PrisonService,2007. 63 Ibid. 64 Hidden Harm: Responding to the needs of children of problem drug
users,AdvisoryCouncilontheMisuseofDrugs,2003. 65 Ibid. 66 Have we got our priorities right?Aberlour,2007. 67 Changing Scotland’s Relationship with Alcohol: A discussion paper on
our strategic approach,ScottishGovernment,2008.
Appendix1.33
Notes to Part 2 68 DuetotheabsenceofScottishestimatesofthewidereconomicand
socialcostsofdrugmisusewehaveusedthemethodologyfromSocial and economic costs ofClass A drugs in England and Wales 2003/04, HomeOffice,2006,andappliedScottishprevalencefigures.
69 Costs of alcohol use and misuse in Scotland,ScottishGovernment, May2008.
70 TheAssociationofChiefPoliceOfficersinScotland(ACPOS)highlight thatthisislikelytobeasignificantunder-estimateasitdoesnotinclude workundertakenbyoperationaluniformedofficersorplainclothes divisionalunitswhowilldealwithdrugoffendersormakeroutine licensedpremisesvisitsaspartoftheirroutineactivities.
71 Campus/liaisonofficersandpoliceofficerswhoworkwithschools, collegesanduniversitiestoraiseawarenessofsubstancemisuseand preventproblematicbehaviour.
72 NationalNHSring-fencedallocationsfordrugsexistedfrom1998before dedicatedmoneyforalcoholwasintroducedin2004.
73 TheConventionofScottishLocalAuthorities(COSLA)isthe representativevoiceofScottishlocalgovernmentandalsoactsasthe employers’associationonbehalfofallScottishcouncils.
74 TheGAEformulaisbasedonfactorssuchasdemographics,deprivation andhealthindicators.Theactualfundingallocationismadethrougha blockrevenuesupportgrant.Councilshavethediscretiontosettheirlocal servicebudgetsatdifferentlevelstotheindicativelevelsintheGAE.
75 Scottish local government financial statistics,2006/07(webonly publication–http://www.scotland.gov.uk/publications)
76 Publisheddatacurrentlyonlyavailablefor2006/07. 77 2007 National Report to the EMCDDA,UKFocalPointonDrugs,2007. 78 FigureincludesNHS,councilandScottishPrisonServicelabelled
expenditure. 79 FigureincludesNHSandcouncilspend,thecostofpolicecampusand
liaisonofficersandScottishGovernmentlabelledexpenditure(eg,Know theScoreandChoicesforLife).
80 Figureincludespolice,ScottishPrisonServiceandsomeScottish Governmentlabelledexpenditure.
81 Thisispoliceenforcementandregulationworkanddoesnotincludethe preventionworkofcampusandliaisonofficers.
82 Costs of alcohol use and misuse in Scotland,ScottishGovernment,May 2008.
83 DuetodelaysinScottishGovernmentestimatesofthewidereconomic andsocialcostsofdrugmisusewehaveusedmethodologyfromSocial andeconomiccostsofClass A drugs in England and Wales 2003/04, HomeOffice,2006,andappliedScottishprevalencefigures.
84 Theremaining£53millionwasspentoncombineddrugandalcohol services.
Notes to Part 3
85 AuditScotlandfieldwork,2008. 86 National Quality Standards for Substance Misuse Services,Scottish
Executive,2006. 87 Psychostimulant Project Group Report,ScottishAdvisoryCommitteeon
DrugMisuse,2008. 88 The Road to Recovery: a new approach for tackling Scotland’s drug
problem,ScottishGovernment,2008. 89 Review of Residential Drug Detoxification and Rehabilitation Services in
Scotland,ScottishGovernment,2007. 90 Ibid. 91 Ibid. 92 Ibid. 93 Review of methadone in drug treatment: prescribing information and
practice,ScottishGovernment,2007.
94 Thisincludes£10.8milliononthecostsofthemethadoneand £14.1milliononpharmacydispensingcosts.
95 Unit Costs for Drug Misuse,NationalTreatmentAgency,2006. 96 Reducing harm and promoting recovery: a report on methadone
treatment for substance misuse in Scotland,ScottishAdvisory CommitteeonDrugMisuse,2007.
97 Costs and equalities and the Scottish criminal justice system 2005/06, ScottishGovernment,2008.
98 TheEffectiveInterventionsUnitoftheScottishExecutiveprovideda seriesofdocumentsonIntegratedCare.
99 Approaches to alcohol and drugs in Scotland,Scotland’sFuturesForum, 2008.
100 Essential Care,ScottishGovernment,2008. 101 Reducing drug use, reducing reoffending,UnitedKingdomDrugPolicy
Commission,2008.
Notes to Part 4 102 CommunityJusticeAuthorities(CJAs)wereestablishedbyThe
ManagementofOffenders,etc.(Scotland)Act2005.TheeightCJAsare: FifeandForthValley,Glasgow,Lanarkshire,LothianandBorders,North Strathclyde,Northern,SouthWestScotlandandTayside.
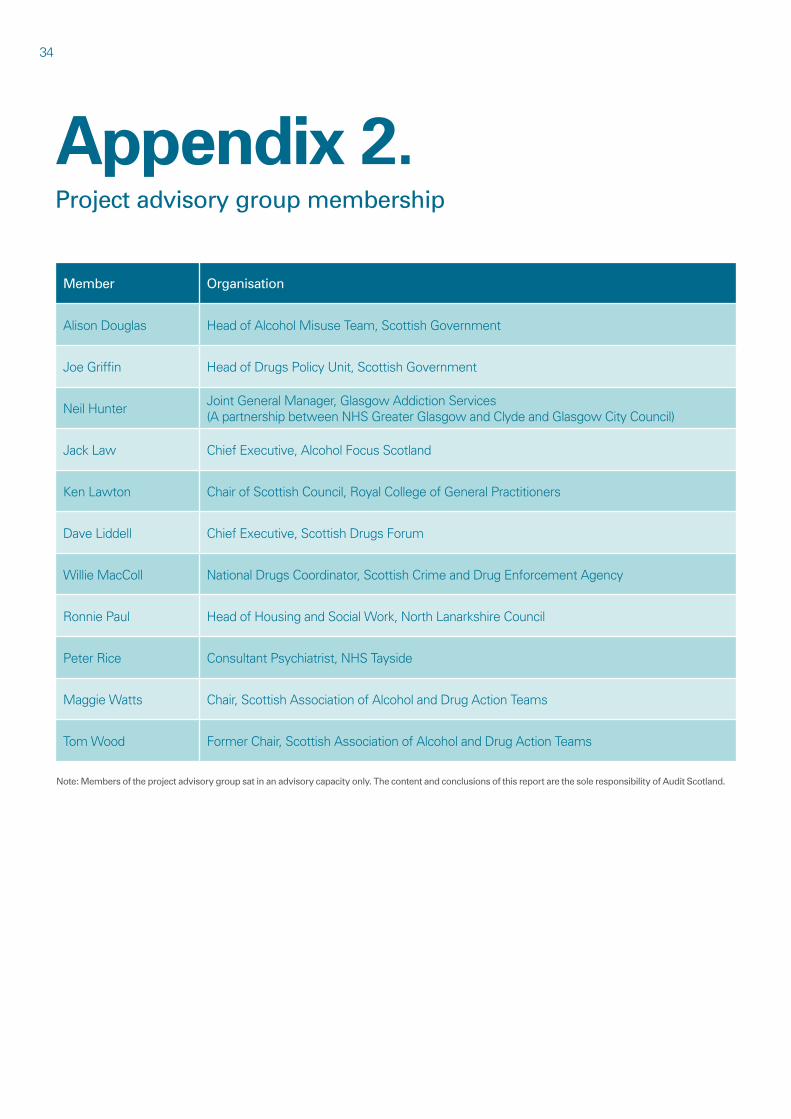
34
Appendix 2. Project advisory group membership
Member Organisation
AlisonDouglas HeadofAlcoholMisuseTeam,ScottishGovernment
JoeGriffin HeadofDrugsPolicyUnit,ScottishGovernment
NeilHunter JointGeneralManager,GlasgowAddictionServices (ApartnershipbetweenNHSGreaterGlasgowandClydeandGlasgowCityCouncil)
JackLaw ChiefExecutive,AlcoholFocusScotland
KenLawton ChairofScottishCouncil,RoyalCollegeofGeneralPractitioners
DaveLiddell ChiefExecutive,ScottishDrugsForum
WillieMacColl NationalDrugsCoordinator,ScottishCrimeandDrugEnforcementAgency
RonniePaul HeadofHousingandSocialWork,NorthLanarkshireCouncil
PeterRice ConsultantPsychiatrist,NHSTayside
MaggieWatts Chair,ScottishAssociationofAlcoholandDrugActionTeams
TomWood FormerChair,ScottishAssociationofAlcoholandDrugActionTeams
Note: Members of the project advisory group sat in an advisory capacity only. The content and conclusions of this report are the sole responsibility of Audit Scotland.
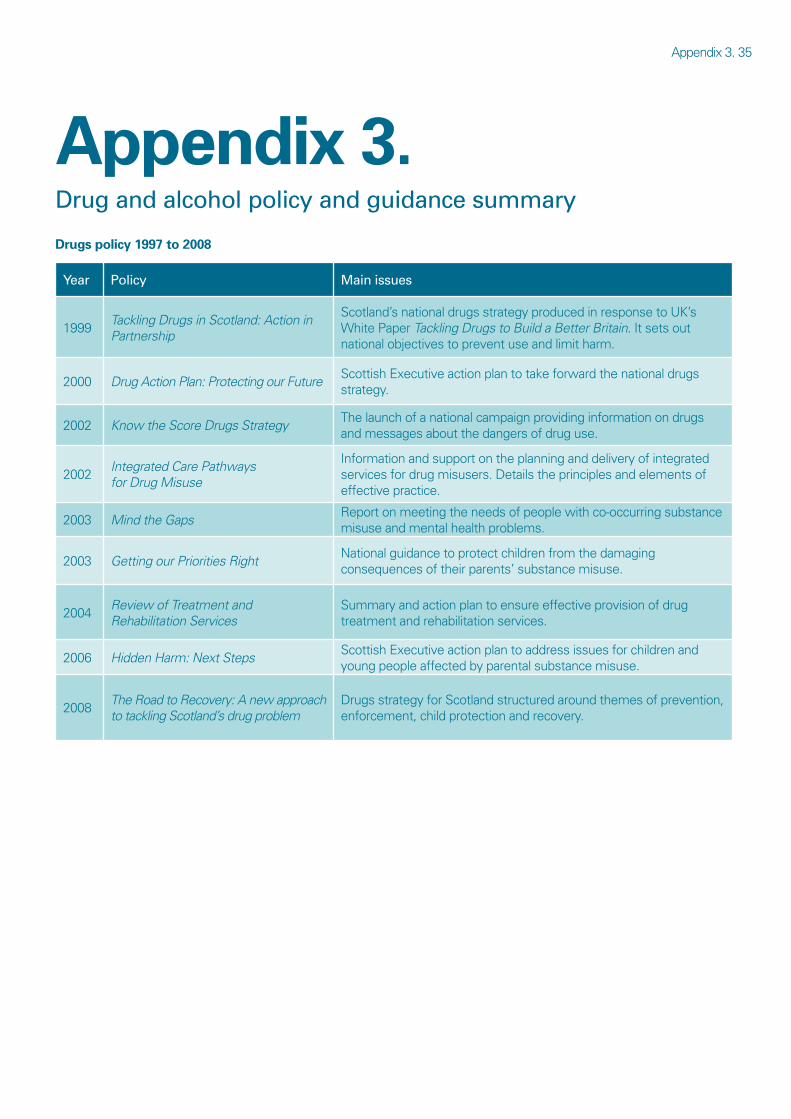
Appendix3.35
Appendix 3. Drug and alcohol policy and guidance summary
Drugs policy 1997 to 2008
Year Policy Main issues
1999 Tackling Drugs in Scotland: Action in Partnership
Scotland’snationaldrugsstrategyproducedinresponsetoUK’s WhitePaperTackling Drugs to Build a Better Britain.Itsetsout nationalobjectivestopreventuseandlimitharm.
2000 Drug Action Plan: Protecting our Future ScottishExecutiveactionplantotakeforwardthenationaldrugs strategy.
2002
2002
2003
2003
Know the Score Drugs Strategy
Integrated Care Pathways for Drug Misuse
Mind the Gaps
Getting our Priorities Right
Thelaunchofanationalcampaignprovidinginformationondrugs andmessagesaboutthedangersofdruguse.
Informationandsupportontheplanninganddeliveryofintegrated servicesfordrugmisusers.Detailstheprinciplesandelementsof effectivepractice.
Reportonmeetingtheneedsofpeoplewithco-occurringsubstance misuseandmentalhealthproblems.
Nationalguidancetoprotectchildrenfromthedamaging consequencesoftheirparents’substancemisuse.
2004 Review of Treatment and Rehabilitation Services
Summaryandactionplantoensureeffectiveprovisionofdrug treatmentandrehabilitationservices.
2006 Hidden Harm: Next Steps ScottishExecutiveactionplantoaddressissuesforchildrenand youngpeopleaffectedbyparentalsubstancemisuse.
2008 The Road to Recovery: A new approach to tackling Scotland’s drug problem
DrugsstrategyforScotlandstructuredaroundthemesofprevention, enforcement,childprotectionandrecovery.
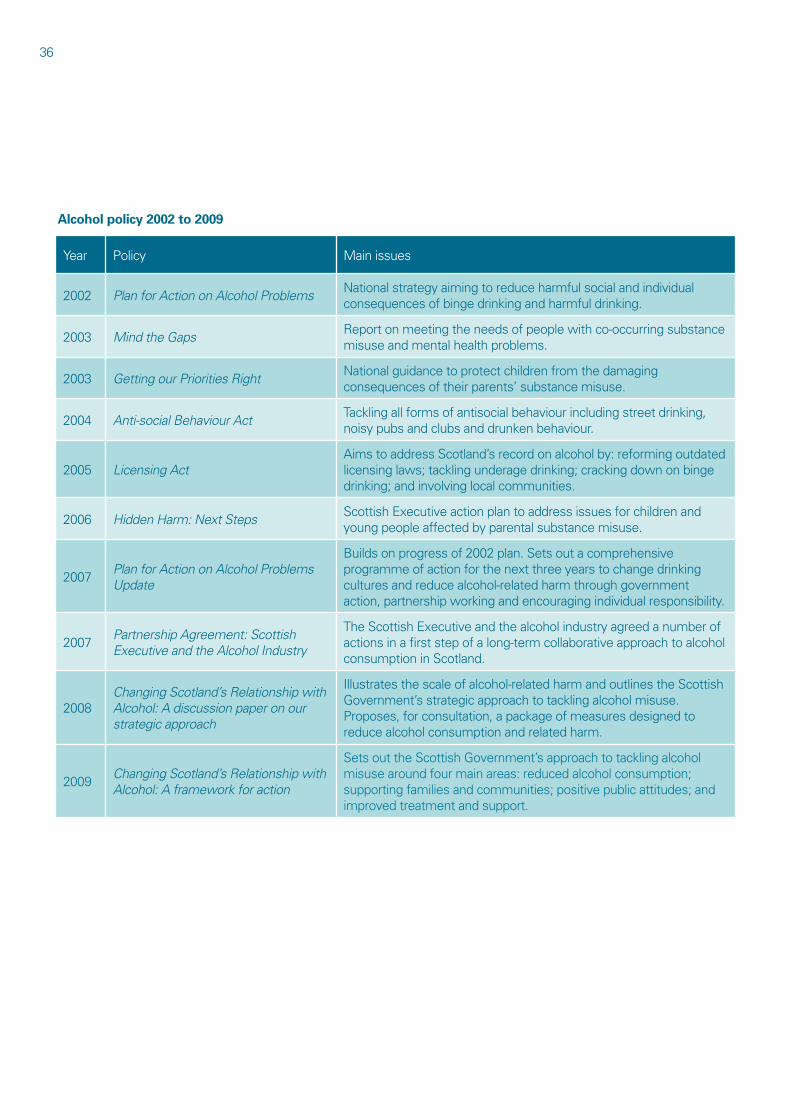
36
Alcohol policy 2002 to 2009
Year Policy Mainissues
2002 Plan for Action on Alcohol Problems Nationalstrategyaimingtoreduceharmfulsocialandindividual consequencesofbingedrinkingandharmfuldrinking.
2003 Mind the Gaps Reportonmeetingtheneedsofpeoplewithco-occurringsubstance misuseandmentalhealthproblems.
2003 Getting our Priorities Right Nationalguidancetoprotectchildrenfromthedamaging consequencesoftheirparents’substancemisuse.
2004 Anti-social Behaviour Act Tacklingallformsofantisocialbehaviourincludingstreetdrinking, noisypubsandclubsanddrunkenbehaviour.
2005 Licensing Act AimstoaddressScotland’srecordonalcoholby:reformingoutdated licensinglaws;tacklingunderagedrinking;crackingdownonbinge drinking;andinvolvinglocalcommunities.
2006 Hidden Harm: Next Steps ScottishExecutiveactionplantoaddressissuesforchildrenand youngpeopleaffectedbyparentalsubstancemisuse.
2007 Plan for Action on Alcohol Problems Update
Buildsonprogressof2002plan.Setsoutacomprehensive programmeofactionforthenextthreeyearstochangedrinking culturesandreducealcohol-relatedharmthroughgovernment action,partnershipworkingandencouragingindividualresponsibility.
2007 Partnership Agreement: Scottish Executive and the Alcohol Industry
TheScottishExecutiveandthealcoholindustryagreedanumberof actionsinafirststepofalong-termcollaborativeapproachtoalcohol consumptioninScotland.
2008 Changing Scotland’s Relationship with Alcohol: A discussion paper on our strategic approach
Illustratesthescaleofalcohol-relatedharmandoutlinestheScottish Government’sstrategicapproachtotacklingalcoholmisuse. Proposes,forconsultation,apackageofmeasuresdesignedto reducealcoholconsumptionandrelatedharm.
2009 Changing Scotland’s Relationship with Alcohol: A framework for action
SetsouttheScottishGovernment’sapproachtotacklingalcohol misusearoundfourmainareas:reducedalcoholconsumption; supportingfamiliesandcommunities;positivepublicattitudes;and improvedtreatmentandsupport.
Appendix4.37
Appendix 4. Self-assessment checklist for partners
Thechecklistonthenextfewpagessetsoutsomeofthehigh-levelpractical issuesarounddrugandalcoholservicesraisedinthisreport.NHSboards, councils,policeforces,prisonsandthevoluntaryandprivatesectorsshoulduse thechecklisttoassessthemselvesagainsteachstatementasappropriateand assessthestrengthofallrelevantpartnershiparrangements.
Thischecklistisbasedonstatementsfromavarietyofsourcesincluding previousAuditScotlandreports,AuditCommissionreportsandNationalAudit Officereports.
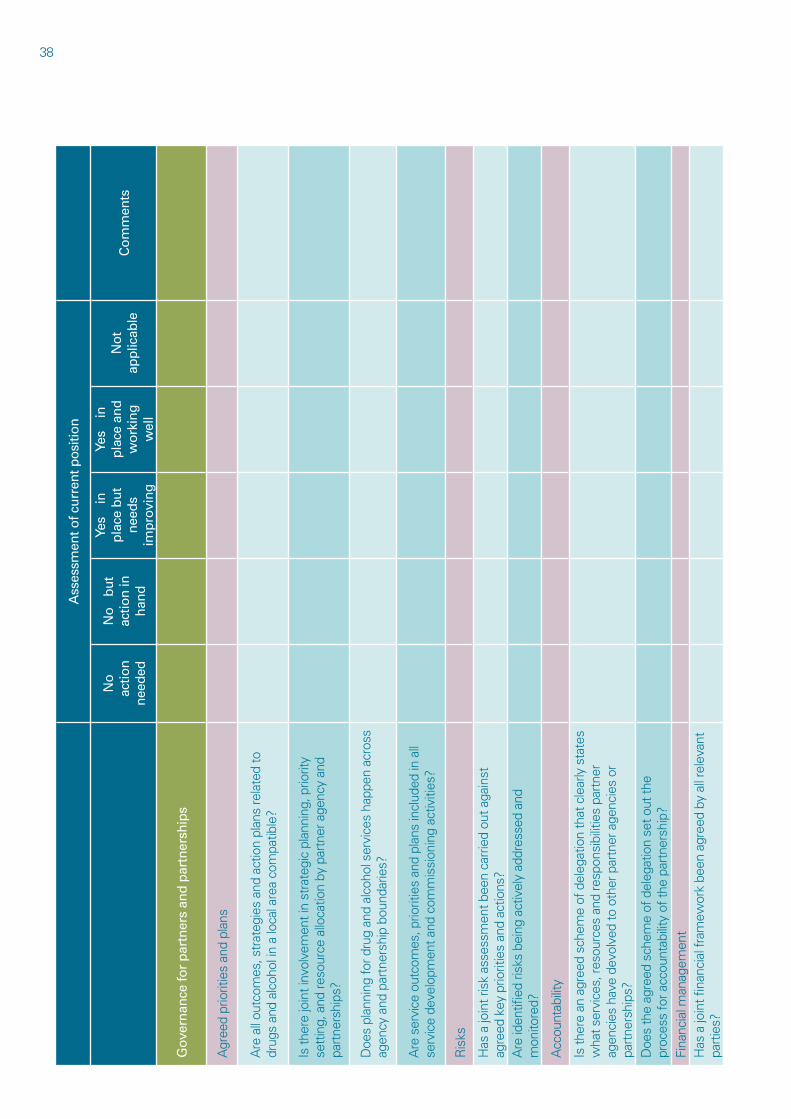
38 A
sses
smen
t of c
urre
nt p
ositi
on
No
ac
tion
ne
eded
No
bu
t ac
tion
in
hand
Yes
in
plac
e bu
t ne
eds
impr
ovin
g
Yes
in
plac
e an
d
wor
king
w
ell
Not
ap
plic
able
C
omm
ents
Gov
erna
nce
for
part
ners
and
par
tner
ship
s
A g r
e e d
p r i o
r i t i e
s a n
d p l
a n s
A r e
a l l
o u t c
o m e s
, s t r
a t e g
i e s
a n d
a c t i o
n p l
a n s
r e l a
t e d
t o
d r u g
s a n
d a l
c o h o
l i n
a l o
c a l a
r e a
c o m
p a t i b
l e ?
I s t h
e r e
j o i n
t i n v
o l v e
m e n
t i n
s t r a
t e g i
c p l
a n n i
n g , p
r i o r i t
y s e
t t i n
g , a
n d r e
s o u r
c e a
l l o c a
t i o n
b y p
a r t n
e r a
g e n c
y a n
d p a
r t n e
r s h i
p s ?
D o e
s p l
a n n i
n g f o
r d r u
g a n
d a l
c o h o
l s e r
v i c e
s h a
p p e n
a c r
o s s
a g e n
c y a
n d p
a r t n
e r s h
i p b
o u n d
a r i e
s ?
A r e
s e r
v i c e
o u t
c o m
e s , p
r i o r i t
i e s
a n d
p l a n
s i n
c l u d
e d i n
a l l
s e r v
i c e
d e v e
l o p m
e n t a
n d c
o m m
i s s i
o n i n
g a c
t i v i t i
e s ?
R i s
k s
H a s
a j o
i n t r
i s k
a s s e
s s m
e n t b
e e n
c a r r
i e d
o u t a
g a i n
s t
a g r e
e d k
e y p
r i o r i t
i e s
a n d
a c t i o
n s ?
A r e
i d e n
t i fi e d
r i s k
s b e
i n g
a c t i v
e l y
a d d r
e s s e
d a n
d m
o n i t o
r e d ?
A c c
o u n t
a b i l i
t y
I s t h
e r e
a n a
g r e e
d s c
h e m
e o f
d e l
e g a t
i o n
t h a t
c l e
a r l y
s t a
t e s
w h a
t s e r
v i c e
s , r e
s o u r
c e s
a n d
r e s p
o n s i
b i l i t
i e s
p a r t
n e r
a g e n
c i e s
h a v
e d e
v o l v
e d t o
o t h
e r p
a r t n
e r a
g e n c
i e s
o r
p a r t
n e r s
h i p s
? D
o e s
t h e
a g r e
e d s
c h e m
e o f
d e l
e g a t
i o n
s e t o
u t t h
e p r
o c e s
s f o
r a c c
o u n t
a b i l i
t y o
f t h e
p a r
t n e r
s h i p
?F i
n a n c
i a l m
a n a g
e m e n
tH
a s a
j o i n
t fi n a
n c i a
l f r a
m e w
o r k
b e e n
a g r
e e d
b y a
l l r e
l e v a
n t
p a r t
i e s ?
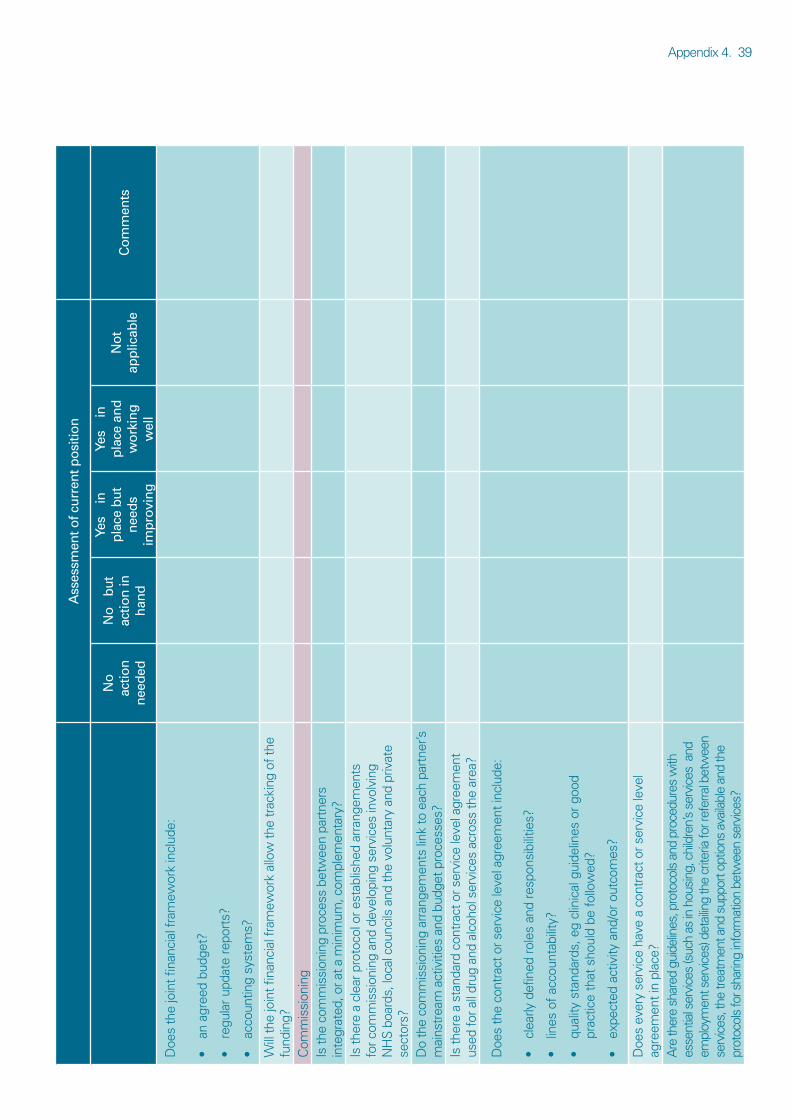
Appendix4 .39 A
sses
smen
t of c
urre
nt p
ositi
on
No
ac
tion
ne
eded
No
bu
t ac
tion
in
hand
Yes
in
plac
e bu
t ne
eds
impr
ovin
g
Yes
in
plac
e an
d
wor
king
w
ell
Not
ap
plic
able
C
omm
ents
D o e
s t h
e j o
i n t fi
n a n c
i a l f
r a m
e w o r
k i n
c l u d
e :
a n a
g r e e
d b u
d g e t
?
r e g u
l a r u
p d a t
e r e
p o r t
s ?
a c c o
u n t i n
g s y
s t e m
s ?
• • • W i l l
t h e
j o i n
t fi n a
n c i a
l f r a
m e w
o r k
a l l o
w t h
e t r
a c k i
n g o
f t h e
f u
n d i n
g ?C
o m m
i s s i
o n i n
g I s
t h e
c o m
m i s
s i o n
i n g
p r o c
e s s
b e t w
e e n
p a r t
n e r s
i n
t e g r
a t e d
, o r a
t a m
i n i m
u m , c
o m p l
e m e n
t a r y
?I s
t h e r
e a
c l e a
r p r o
t o c o
l o r e
s t a b
l i s h e
d a r
r a n g
e m e n
t s
f o r c
o m m
i s s i
o n i n
g a n
d d e
v e l o
p i n g
s e r
v i c e
s i n
v o l v
i n g
N H
S b
o a r d
s , l o
c a l c
o u n c
i l s a
n d t h
e v o
l u n t
a r y
a n d
p r i v
a t e
s e c t
o r s ?
D o
t h e
c o m
m i s
s i o n
i n g
a r r a
n g e m
e n t s
l i n k
t o e
a c h
p a r t
n e r ’ s
m
a i n s
t r e a
m a
c t i v
i t i e s
a n d
b u d
g e t p
r o c e
s s e s
?I s
t h e r
e a
s t a n
d a r d
c o n
t r a c
t o r s
e r v i
c e l e
v e l a
g r e e
m e n
t u s
e d f o
r a l l
d r u g
a n d
a l c
o h o l
s e r
v i c e
s a c
r o s s
t h e
a r e a
?
D o e
s t h
e c o
n t r a
c t o
r s e r
v i c e
l e v e
l a g r
e e m
e n t i
n c l u
d e :
c l e a
r l y d
e f i n
e d r
o l e s
a n d
r e s
p o n s
i b i l i
t i e s ?
l i n e s
o f a
c c o u
n t a b
i l i t y
?
q u a l
i t y s
t a n d
a r d s
, e g
c l i n
i c a l
g u i
d e l i n
e s o
r g o o
d
p r a c
t i c e
t h a t
s h o
u l d
b e f
o l l o
w e d
?
e x p e
c t e d
a c t
i v i t y
a n d
/ o r o
u t c o
m e s
?
• • • • D o e
s e v
e r y
s e r v
i c e
h a v e
a c
o n t r
a c t o
r s e r
v i c e
l e v e
l a g
r e e m
e n t i
n p l
a c e ?
A r e
t h e r
e s h
a r e d
g u i
d e l i n
e s , p
r o t o
c o l s
a n d
p r o
c e d u
r e s
w i t h
e s
s e n t
i a l s
e r v i
c e s
( s u c
h a s
i n h
o u s i
n g , c
h i l d
r e n ’
s s e
r v i c
e s a
n d
e m p l
o y m
e n t s
e r v i
c e s )
d e t
a i l i n
g t h
e c r
i t e r i a
f o r r
e f e r
r a l b
e t w
e e n
s e r v
i c e s
, t h e
t r e a
t m e n
t a n d
s u p
p o r t o
p t i o
n s a
v a i l a
b l e
a n d
t h e
p r o t
o c o l
s f o
r s h a
r i n g
i n f o
r m a t
i o n
b e t w
e e n
s e r v
i c e s
?
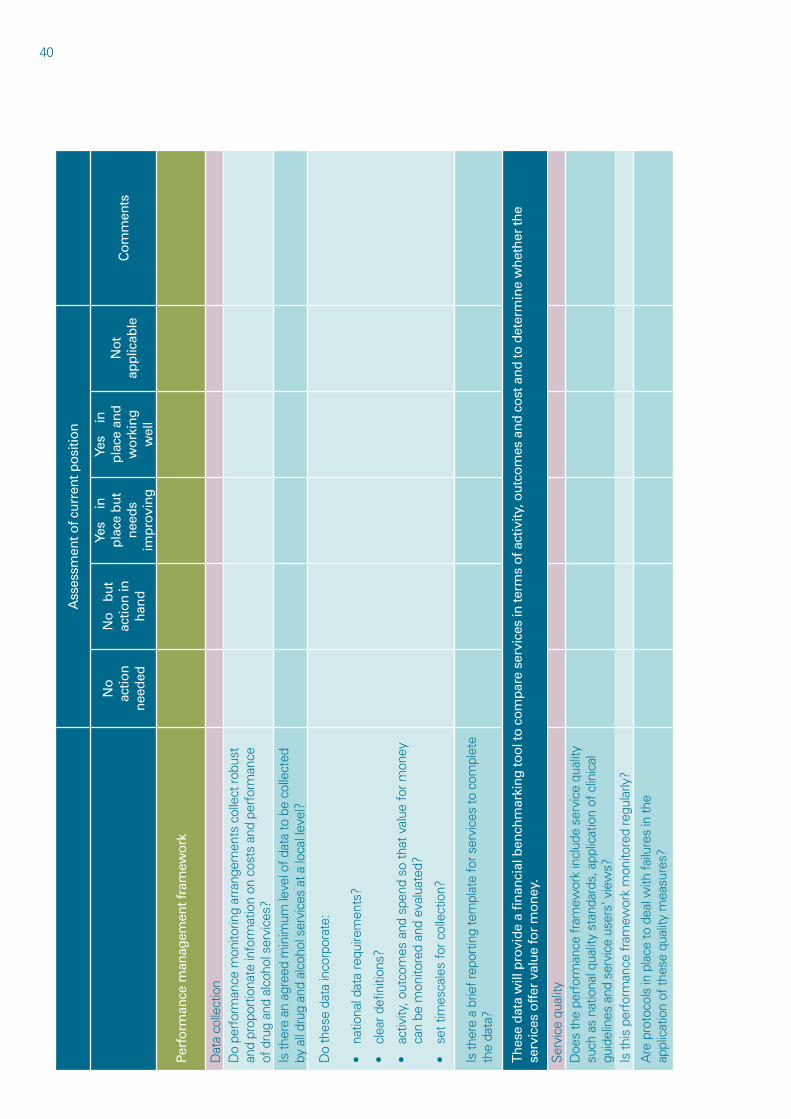
40 A
s s e s
s m e n
t o f c
u r r
e n t p
o s i
t i o n
Y e s
i n
Y
e s
i n
N o
N
o
b u
t p
l a c e
b u
t p
l a c e
a n
d
N o
t a c
t i o n
a c
t i o n
i n
C o
m m
e n t s
n
e e d
s w
o r k
i n g
a p
p l i c
a b l e
n
e e d
e d
h a n
d
i m p
r o v i
n g
w
e l l
P e r
f o r m
a n c e
m a n
a g e m
e n t f
r a m
e w o
r k
Dat
aco
llect
ion
Do
perf
orm
ance
mon
itorin
gar
rang
emen
tsc
olle
ctro
bust
an
dpr
opor
tiona
tein
form
atio
non
cos
tsa
ndp
erfo
rman
ce
ofd
rug
and
alco
hols
ervi
ces?
Isth
ere
ana
gree
dm
inim
umle
velo
fdat
ato
be
colle
cted
by
all
drug
and
alc
ohol
ser
vice
sat
alo
call
evel
?
Do
thes
eda
tain
corp
orat
e:
•na
tiona
ldat
are
quire
men
ts?
•cl
eard
efin
ition
s?
•ac
tivity
,out
com
esa
nds
pend
so
that
val
uefo
rmon
ey
can
bem
onito
red
and
eval
uate
d?
•se
ttim
esca
les
forc
olle
ctio
n?
Isth
ere
abr
iefr
epor
ting
tem
plat
efo
rser
vice
sto
com
plet
eth
eda
ta?
T h
e s e
d a t
a w
i l l p
r o v i
d e
a fi
n a n
c i a l
b e n
c h m
a r k i
n g
t o o
l t o
c o
m p
a r e
s e r v
i c e s
i n t e
r m s
o f a
c t i v
i t y , o
u t c
o m
e s a
n d
c o
s t a
n d
t o d
e t e r
m i n
e w
h e t
h e r
t h e
s e r v
i c e s
o f f
e r v
a l u
e f o
r m
o n
e y .
Isth
isp
erfo
rman
cefr
amew
ork
mon
itore
dre
gula
rly?
Are
pro
toco
lsin
pla
ceto
dea
lwith
failu
res
inth
eap
plic
atio
nof
thes
equ
ality
mea
sure
s?
Serv
ice
qual
ityD
oes
the
perf
orm
ance
fram
ewor
kin
clud
ese
rvic
equ
ality
su
cha
sna
tiona
lqua
lity
stan
dard
s,a
pplic
atio
nof
clin
ical
gu
idel
ines
and
ser
vice
use
rs’v
iew
s?
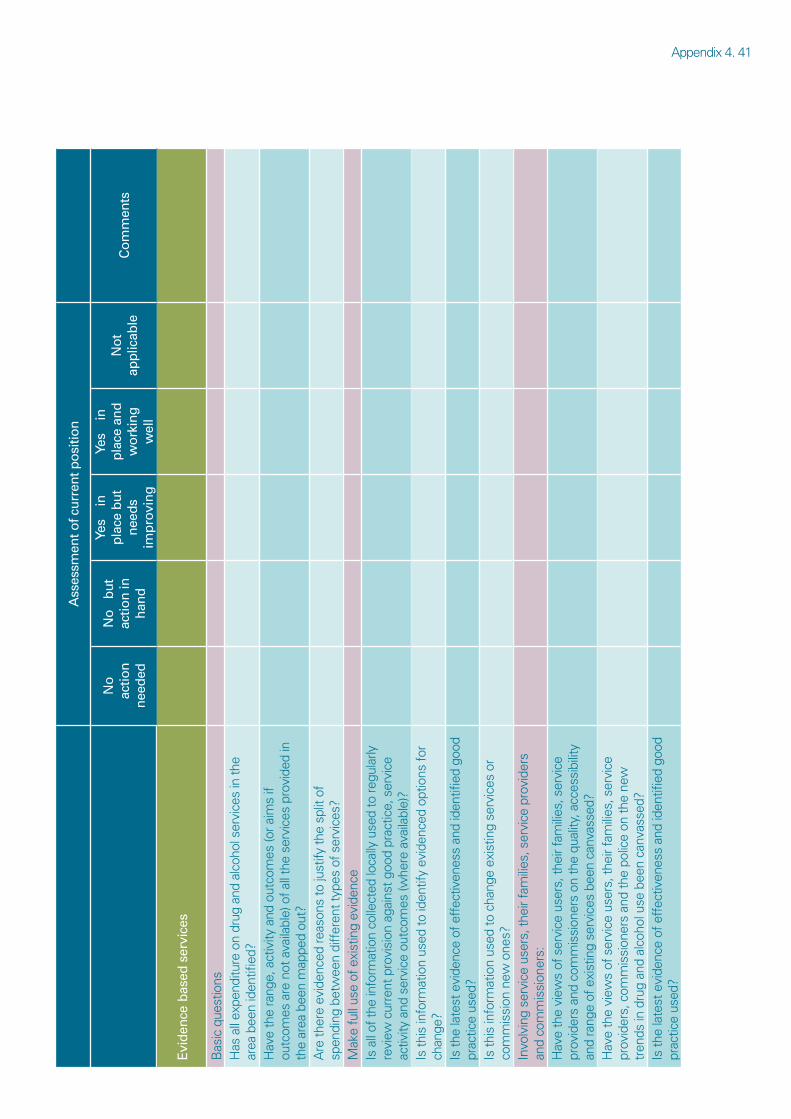
Appendix4 .41 A
sses
smen
t of c
urre
nt p
ositi
on
Yes
in
Yes
in
No
N
o
but
plac
e bu
t pl
ace
and
N
ot
actio
n
actio
n in
C
omm
ents
ne
eds
wor
king
ap
plic
able
ne
eded
ha
nd
impr
ovin
g
wel
l
Evid
ence
bas
ed s
ervi
ces
B a s
i c q
u e s t
i o n s
H a s
a l l
e x p e
n d i t u
r e o
n d r
u g a
n d a
l c o h
o l s
e r v i
c e s
i n t h
e a r
e a b
e e n
i d e n
t fi
i e d
?H
a v e
t h e
r a n g
e , a
c t i v
i t y a
n d o
u t c o
m e s
( o r a
i m s
i f o u
t c o m
e s a
r e n
o t a
v a i l a
b l e )
o f a
l l t h
e s e
r v i c
e s p
r o v i
d e d
i n
t h e
a r e a
b e e
n m
a p p e
d o u
t ?A
r e t h
e r e
e v i d
e n c e
d r e
a s o n
s t o
j u s t
i f y t h
e s p
l i t o
f s p
e n d i
n g b
e t w
e e n
d i f f
e r e n
t t y p
e s o
f s e r
v i c e
s ?
I s t h
i s i n
f o r m
a t i o
n u s
e d t o
i d e n
t i f y
e v i d
e n c e
d o p
t i o n s
f o r
c h a n
g e ?
I s t h
e l a
t e s t
e v i
d e n c
e o f
e f f
e c t i v
e n e s
s a n
d i d
e n t fi
i
e d g
o o d
p r
a c t i c
e u s
e d ?
I s t h
i s i n
f o r m
a t i o
n u s
e d t o
c h a
n g e
e x i s
t i n g
s e r v
i c e s
o r
c o m
m i s
s i o n
n e w
o n e
s ?
H a v
e t h
e v i
e w s
o f s
e r v i
c e u
s e r s
, t h e
i r f a
m i l i
e s , s
e r v i
c e
p r o v
i d e r
s , c
o m m
i s s i
o n e r
s a n
d t h
e p o
l i c e
o n t h
e n e
w
t r e n
d s i n
d r u
g a n
d a l
c o h o
l u s e
b e e
n c a
n v a s
s e d ?
I s t h
e l a
t e s t
e v i
d e n c
e o f
e f f
e c t i v
e n e s
s a n
d i d
e n t fi
i
e d g
o o d
p r
a c t i c
e u s
e d ?
M a k
e f u
l l u s
e o f
e x i
s t i n
g e v
i d e n
c eI s
a l l
o f t h
e i n
f o r m
a t i o
n c o
l l e c t
e d l o
c a l l y
u s e
d t o
r e g u
l a r l y
r e
v i e w
c u r
r e n t
p r o
v i s i
o n a
g a i n
s t g
o o d
p r a c
t i c e ,
s e r
v i c e
a c
t i v i t y
a n d
s e r
v i c e
o u t
c o m
e s ( w
h e r e
a v a
i l a b l
e ) ?
I n v o
l v i n
g s e
r v i c
e u s
e r s ,
t h e i
r f a m
i l i e s
, s e r
v i c e
p r o
v i d e
r s
a n d
c o m
m i s
s i o n
e r s :
H a v
e t h
e v i
e w s
o f s
e r v i
c e u
s e r s
, t h e
i r f a
m i l i
e s , s
e r v i
c e
p r o v
i d e r
s a n
d c o
m m
i s s i
o n e r
s o n
t h e
q u a l
i t y , a
c c e s
s i b i
l i t y
a n d
r a n g
e o f
e x i
s t i n
g s e
r v i c
e s b
e e n
c a n v
a s s e
d ?
Drug and alcohol services in Scotland If you require this publication in an alternative format and/or language, please contact us to discuss your needs.
You can also download this document at: www.audit scotland.gov.uk
Audit Scotland, 110 George Street, Edinburgh EH2 4LH T: 0845 146 1010 F: 0845 146 1009 www.audit scotland.gov.uk
ISBN 978 1 906752 36 1 AGS/2009/3
Printed on Revive 100 Uncoated, a recycled grade, containing 100% post consumer waste and manufactured at a mill accredited with ISO 14001 environmental management standard. The pulp used in this product is bleached using an Elemental Chlorine Free process (ECF).





























