Embed Size (px)
DESCRIPTION
drown
Citation preview

Drowning: an Update 2012
Gary WilliamsMini PAC Conference , Melbourne
16-17 November 2012
Plan
• Definitions• Guidelines• Epidemiology• Pathophysiology • Management• Outcome prediction
Definition
• 2002, World Congress on Drowning, Amsterdam: “respiratory embarrassment from submersion / immersion in a liquid medium”
“near drowning”“dry or wet drowning”“secondary drowning”“delayed onset respiratory distress”
Drowning: Aust Resus Council
• Victim rolled to side during initial checking, airway clearance and initial breathing check
• Begin EAR in water if immediate exit not possible
• If hypothermic, attempt resuscitation even after possibly prolonged immersion
Last updated Feb 2005
Drowning: ERC 2010 Update• More research comparing OHCA due to drowning with
primary cardiac OHCA needed• In-water EAR if victim unresponsive, 10-15 breaths in 1
minute then decide based on est time to shore• < 5 mins continue EAR while towing• > 5 mins give 1 more minute EAR then head off uninterrupted
• Early intubation with cuffed ETT, not LMA or Guedel• Use ECG, ET CO2 or echo to confirm arrest. Be wary to
discontinue resus efforts in the field• Core temp < 30C : limit defib to x3 and withold drugs till
core temp > 30C• Recommends rewarming hypothermic patient to 32-34C
and avoid temps >37C during subsequent intensive care course
Drowning: AHA / ILCOR 2010• Mouth to nose EAR by swimmer while retrieving• When ALS commenced traditional A-B-C sequence used• In hypothermic patient value of deferring subsequent defib
attempts or resuscitation drugs “controversial” and “reasonable to consider…. according to standard algorithm…concurrent with rewarming strategies”
• Use ETCO2 to monitor effectiveness, ROSC and avoid hyperventilation
• 32-34C “may be considered” for children who remain comatose after ROSC
• Avoid rewarming faster than 0.5C per 2 hours and treat fever (>38C) aggressively with antipyretics and cooling devices
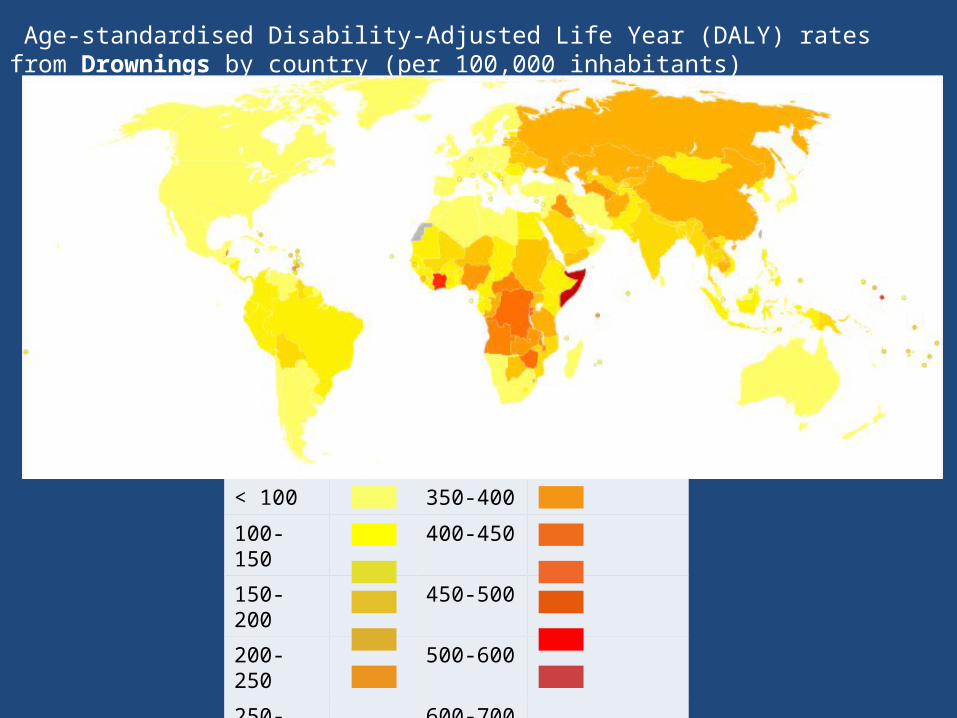
< 100 350-400
100-150 400-450
150-200 450-500
200-250 500-600
250-300 600-700
300-350 >700
Age-standardised Disability-Adjusted Life Year (DALY) rates from Drownings by country (per 100,000 inhabitants)
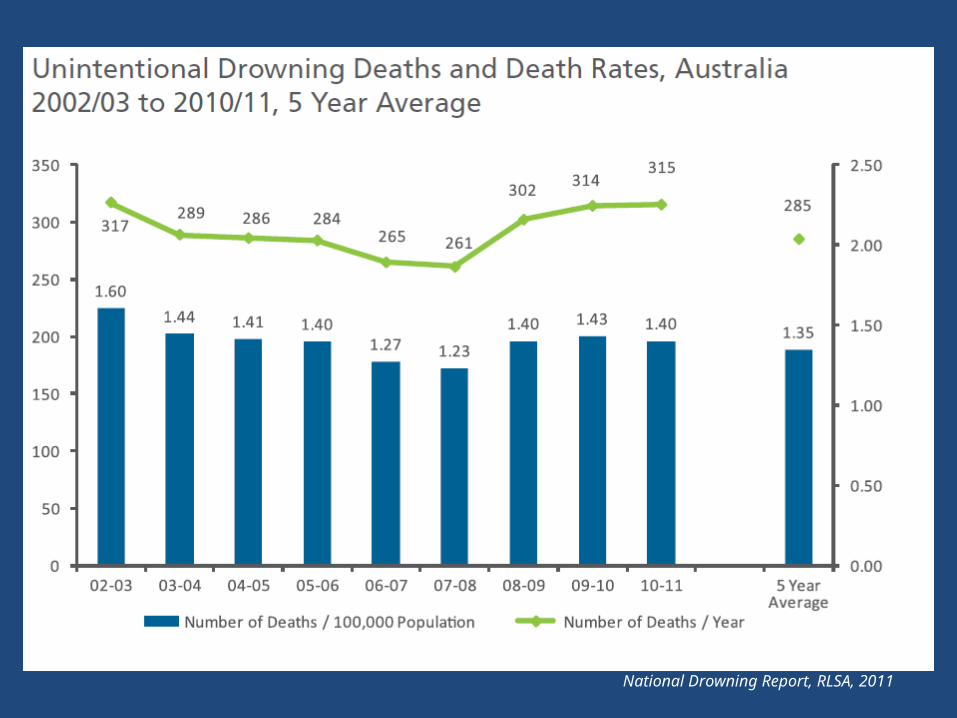
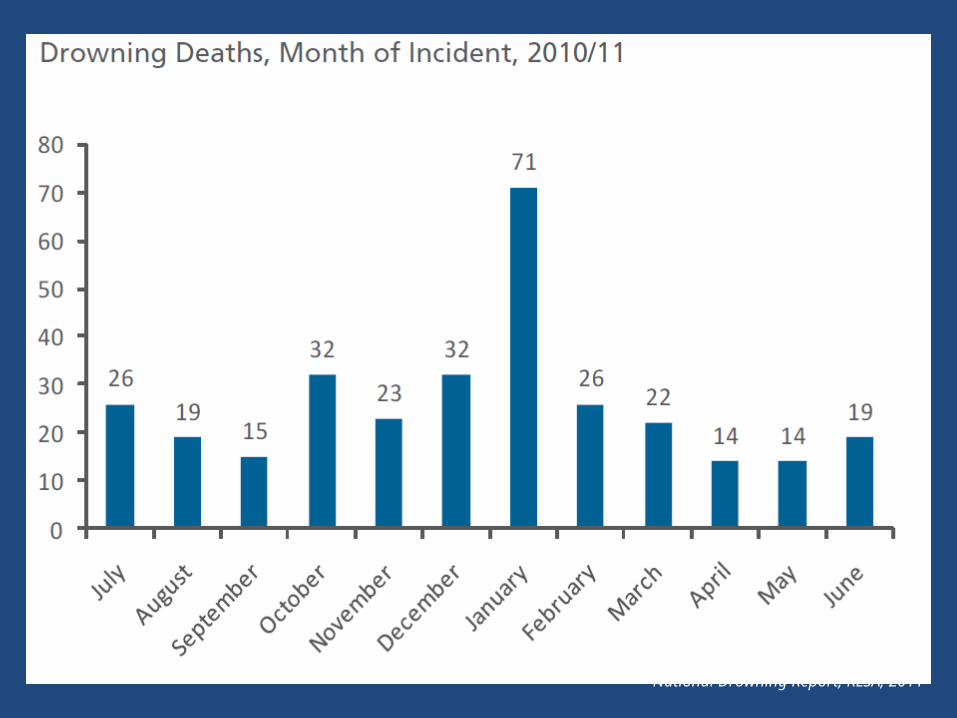
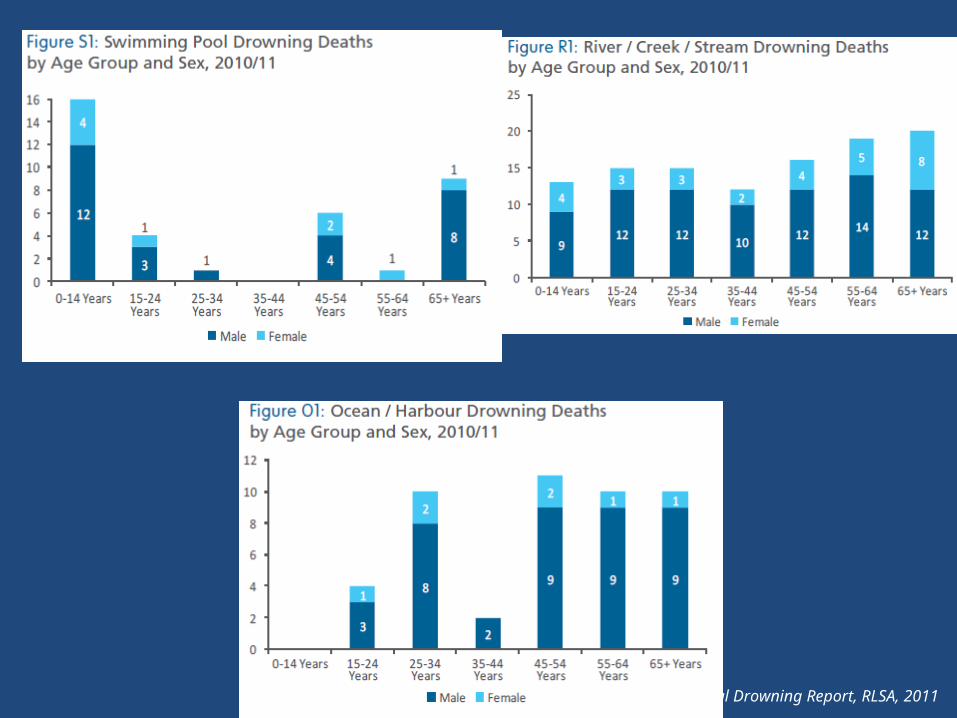
National Drowning Report, RLSA, 2011
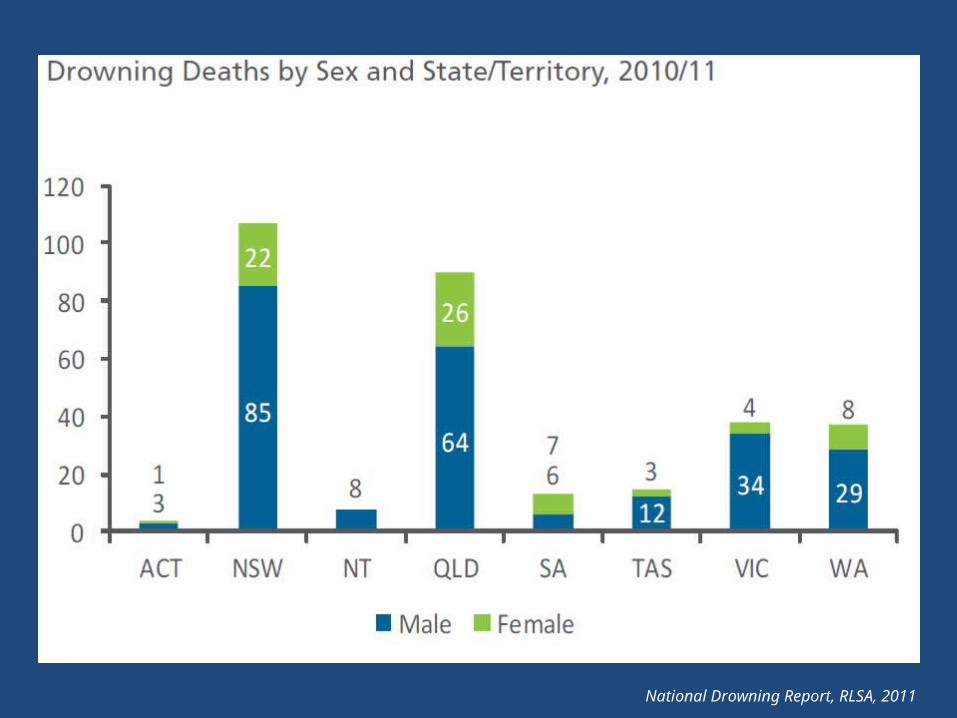
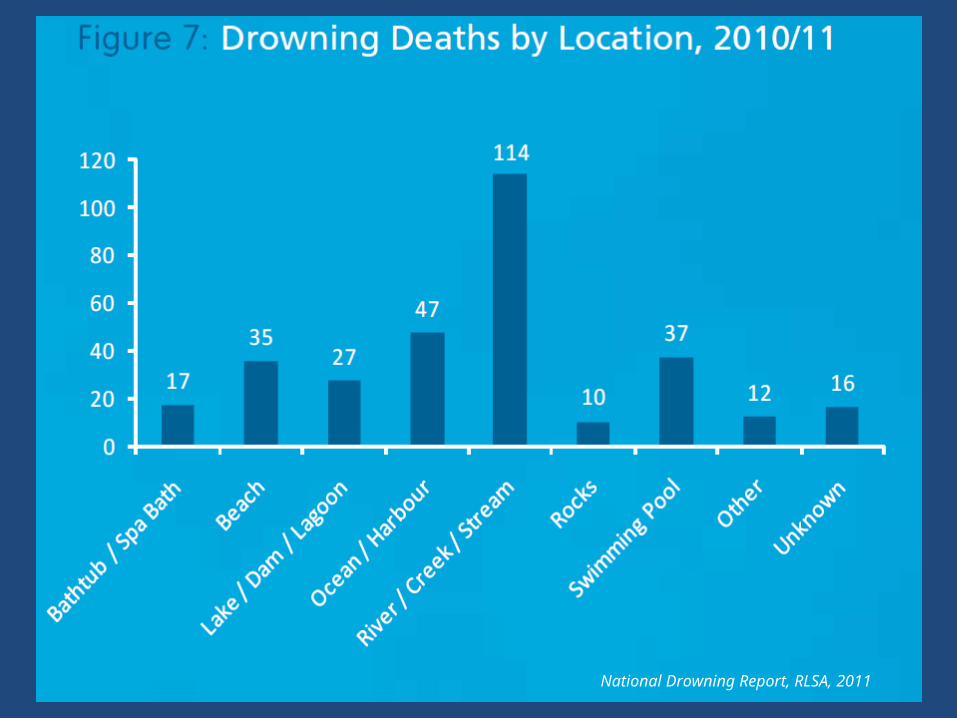
National Drowning Report, RLSA, 2011
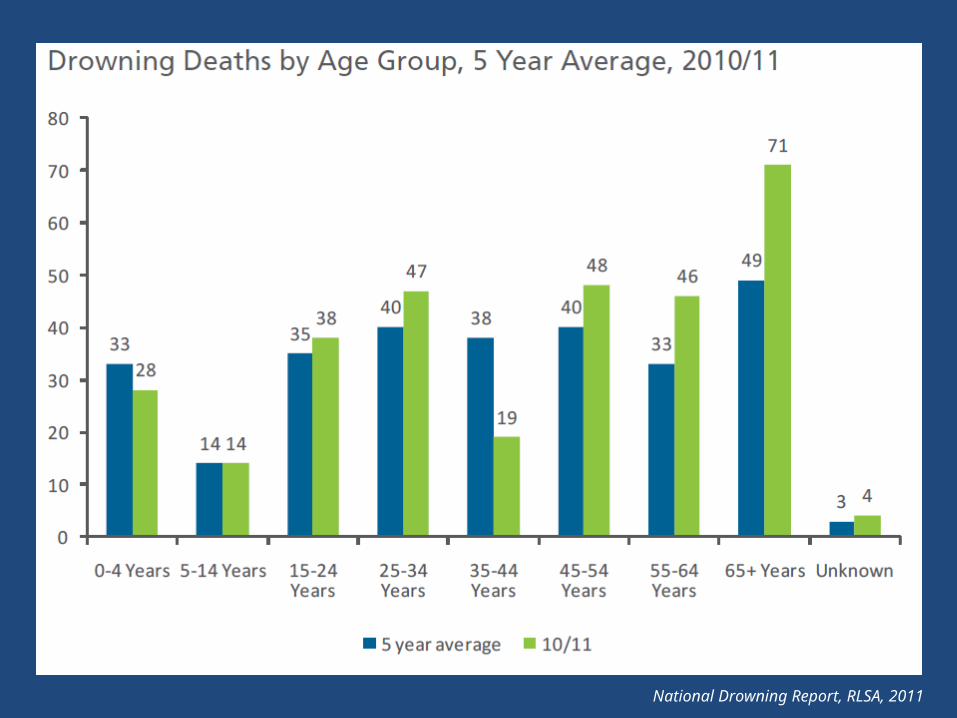
National Drowning Report, RLSA, 2011
ANZPIC Registry
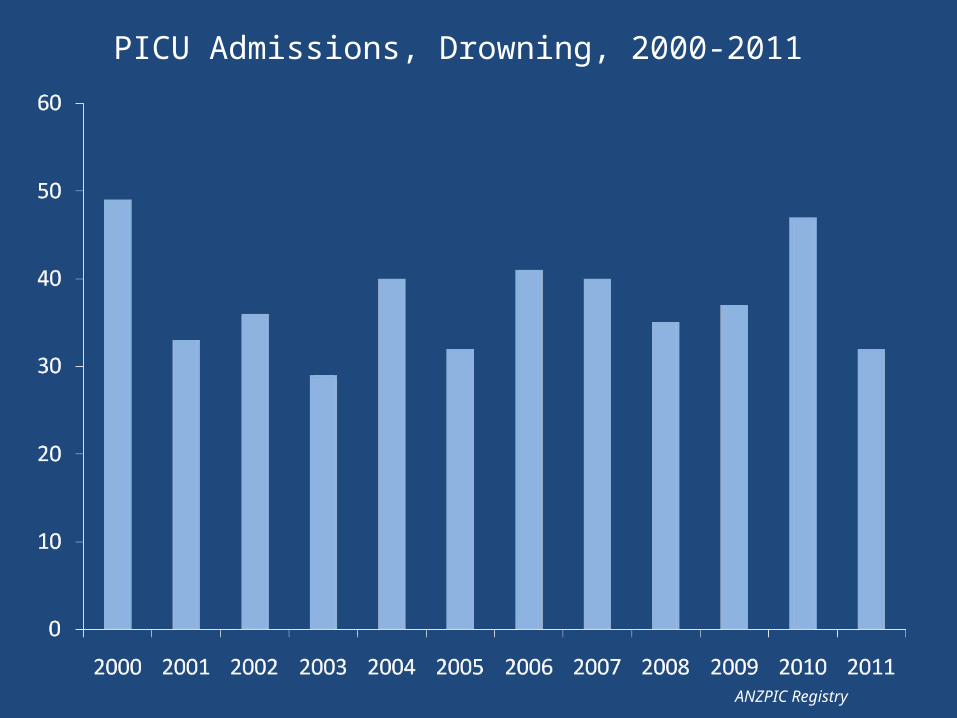
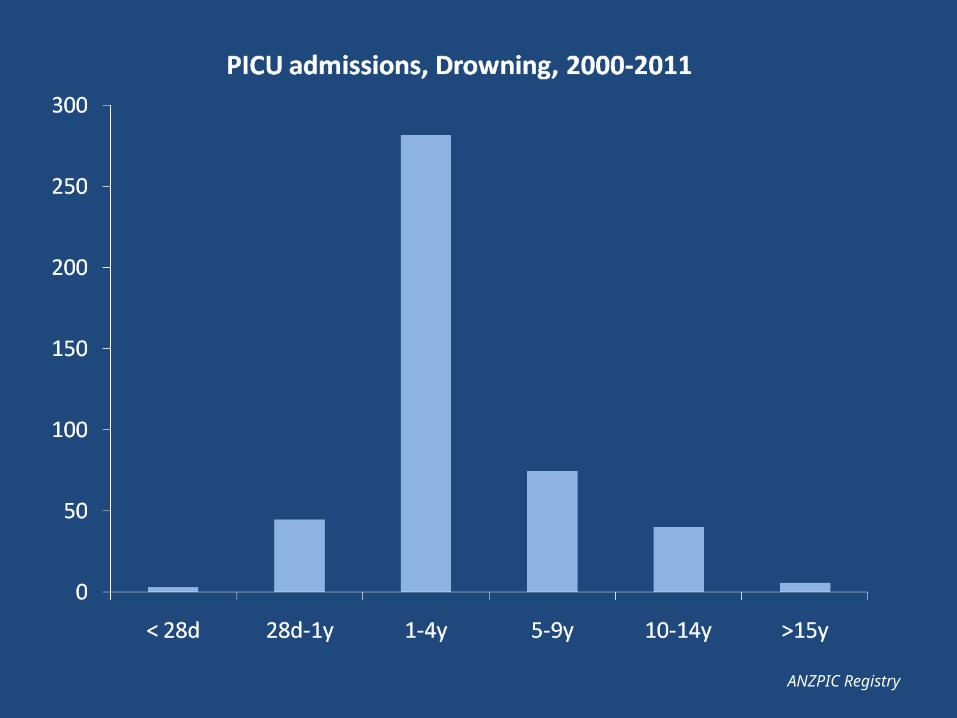
PICU Admissions, Drowning, 2000-2011
ANZPIC Registry
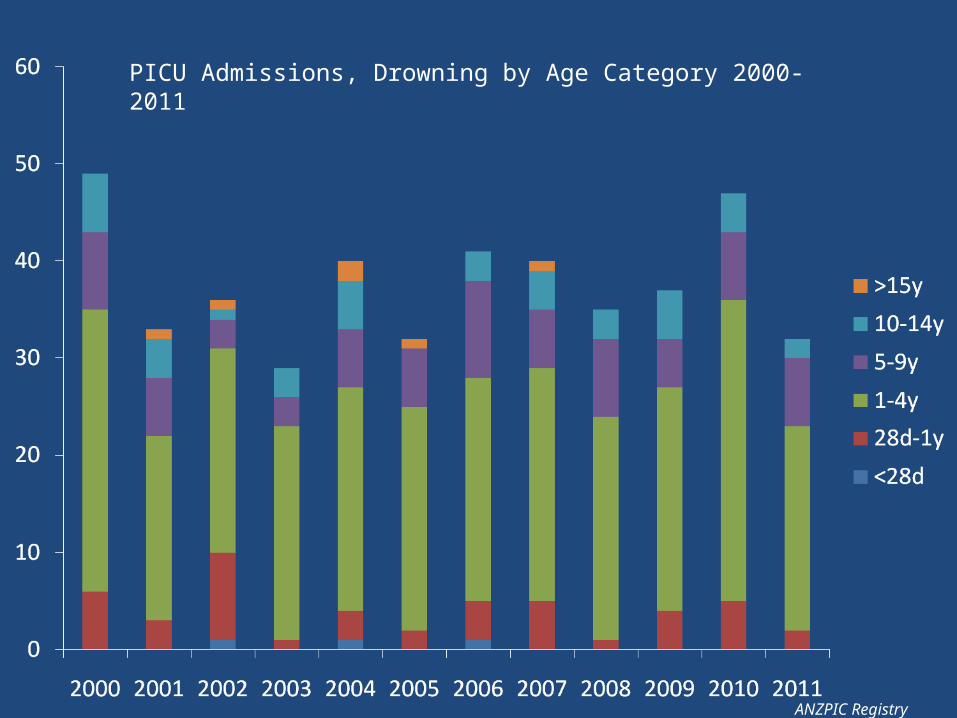
PICU Admissions, Drowning by Age Category 2000-2011
ANZPIC Registry
National Drowning Report, RLSA, 2011
National Drowning Report, RLSA, 2011
National Drowning Report, RLSA, 2011
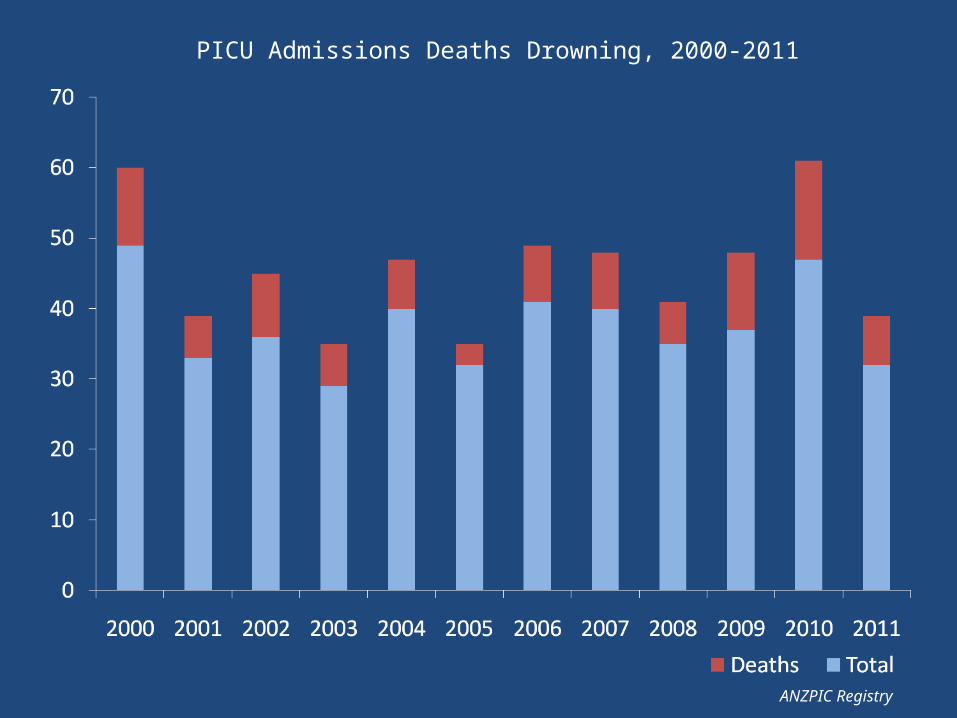
PICU Admissions Deaths Drowning, 2000-2011
ANZPIC Registry
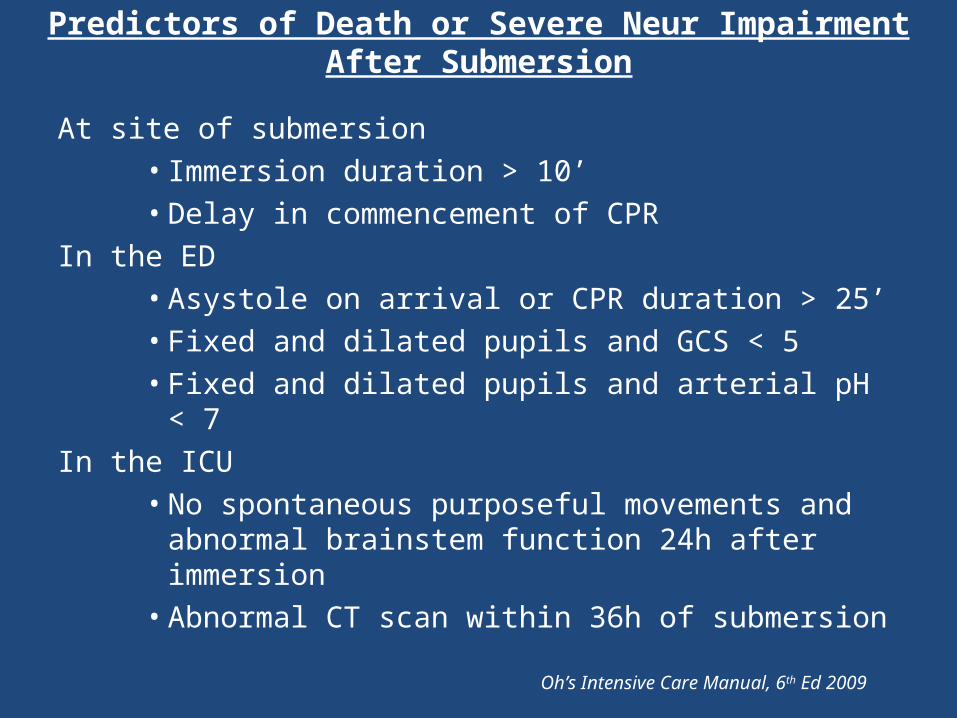
Predictors of Death or Severe Neur Impairment After Submersion
At site of submersion• Immersion duration > 10’• Delay in commencement of CPR
In the ED• Asystole on arrival or CPR duration > 25’• Fixed and dilated pupils and GCS < 5• Fixed and dilated pupils and arterial pH < 7
In the ICU• No spontaneous purposeful movements and abnormal
brainstem function 24h after immersion• Abnormal CT scan within 36h of submersion
Oh’s Intensive Care Manual, 6th Ed 2009
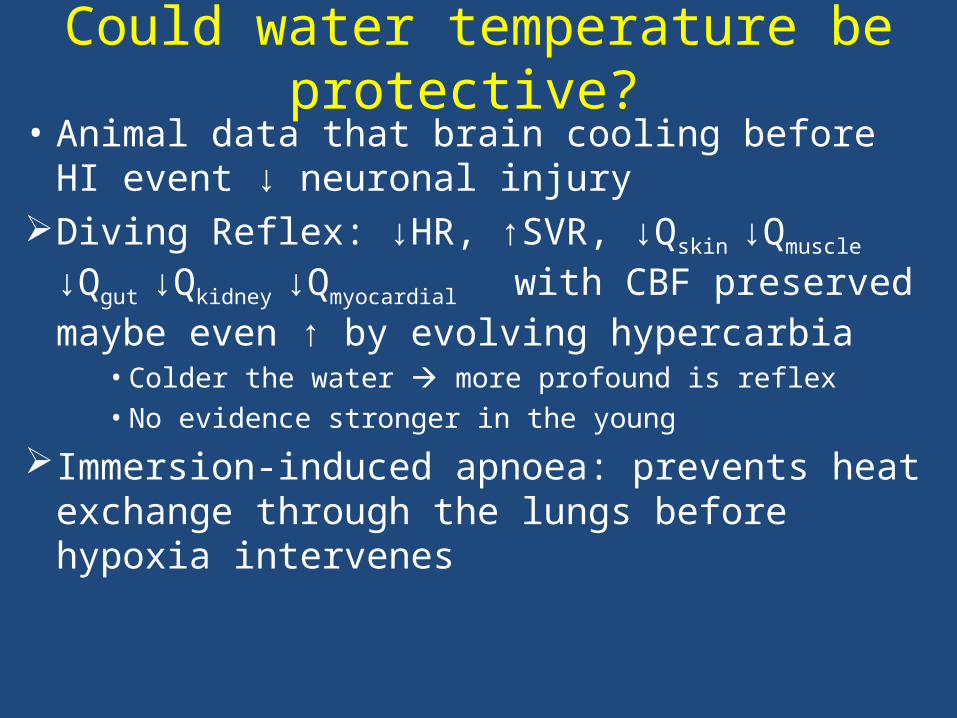
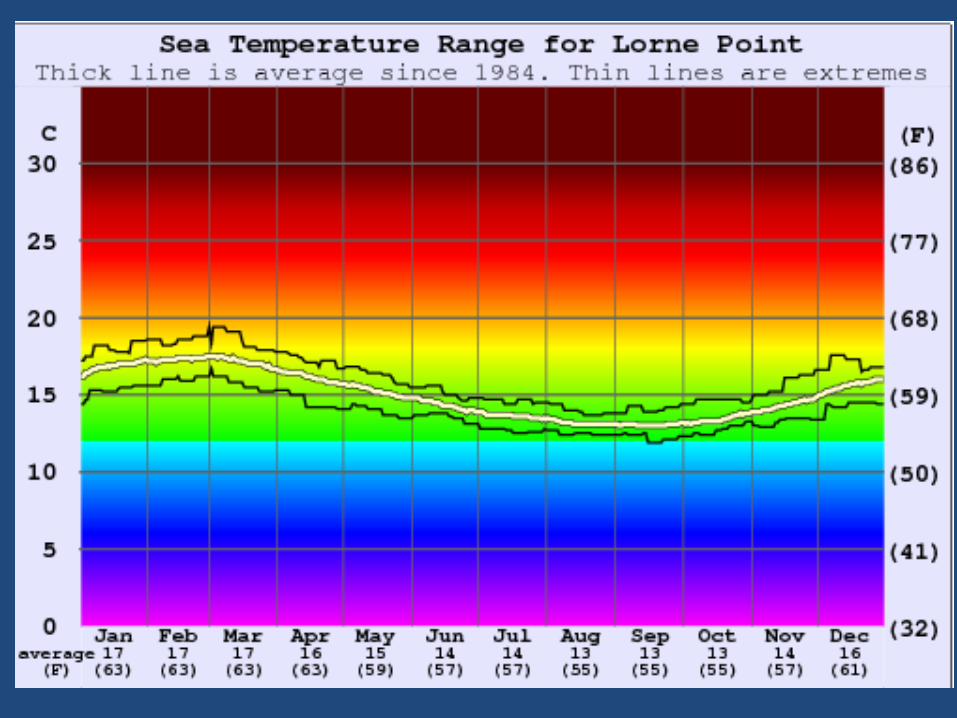
Could water temperature be protective? • Animal data that brain cooling before HI event ↓
neuronal injuryDiving Reflex: ↓HR, ↑SVR, ↓Qskin ↓Qmuscle ↓Qgut
↓Qkidney ↓Qmyocardial with CBF preserved maybe even ↑ by evolving hypercarbia
• Colder the water more profound is reflex• No evidence stronger in the young
Immersion-induced apnoea: prevents heat exchange through the lungs before hypoxia intervenes
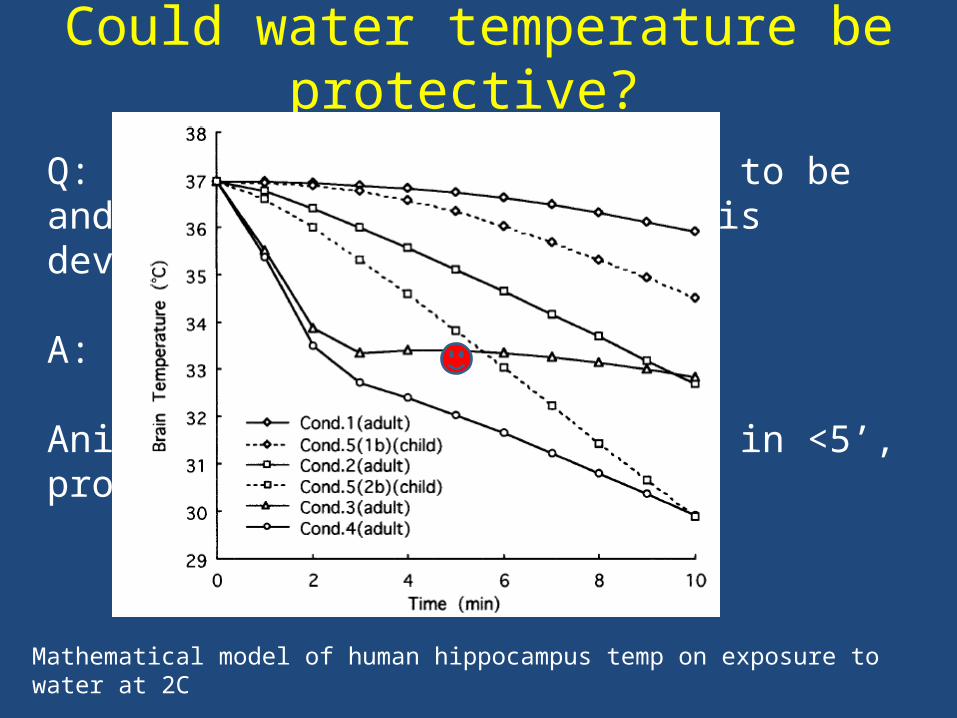
Could water temperature be protective?
Q: How cool has deep brain got to be and how quickly while hypoxia is developing?
A: Unknown
Animal data (rat) suggests 33C in <5’, probably 30C in <10’
Mathematical model of human hippocampus temp on exposure to water at 2C
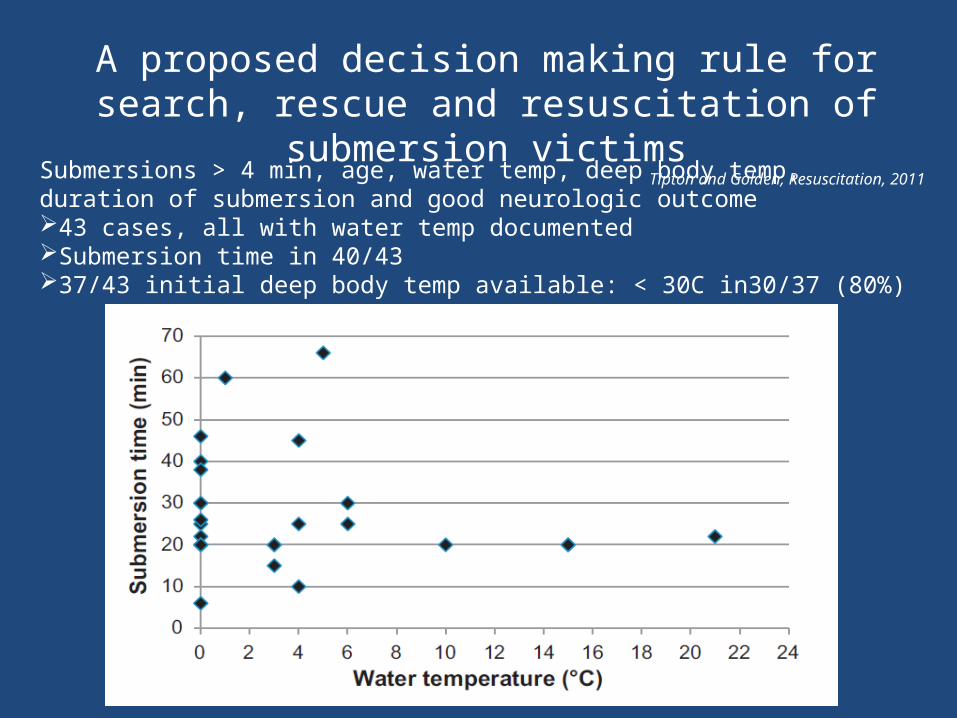
A proposed decision making rule for search, rescue and resuscitation of submersion victims
Tipton and Golden, Resuscitation, 2011
Submersions > 4 min, age, water temp, deep body temp, duration of submersion and good neurologic outcome43 cases, all with water temp documentedSubmersion time in 40/4337/43 initial deep body temp available: < 30C in30/37 (80%)
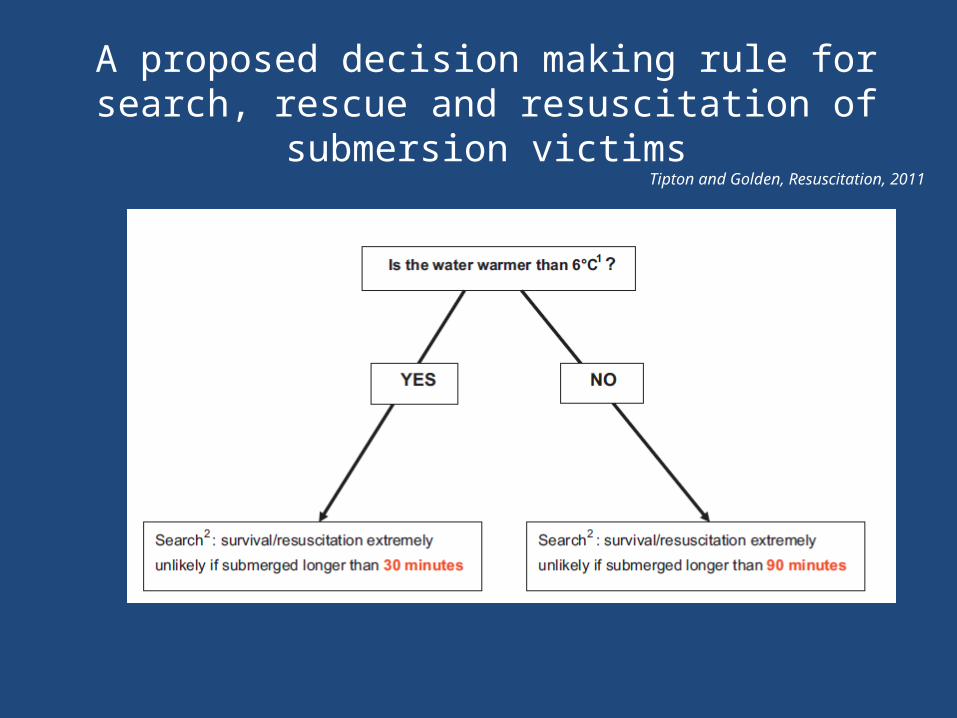
A proposed decision making rule for search, rescue and resuscitation of submersion victims
Tipton and Golden, Resuscitation, 2011
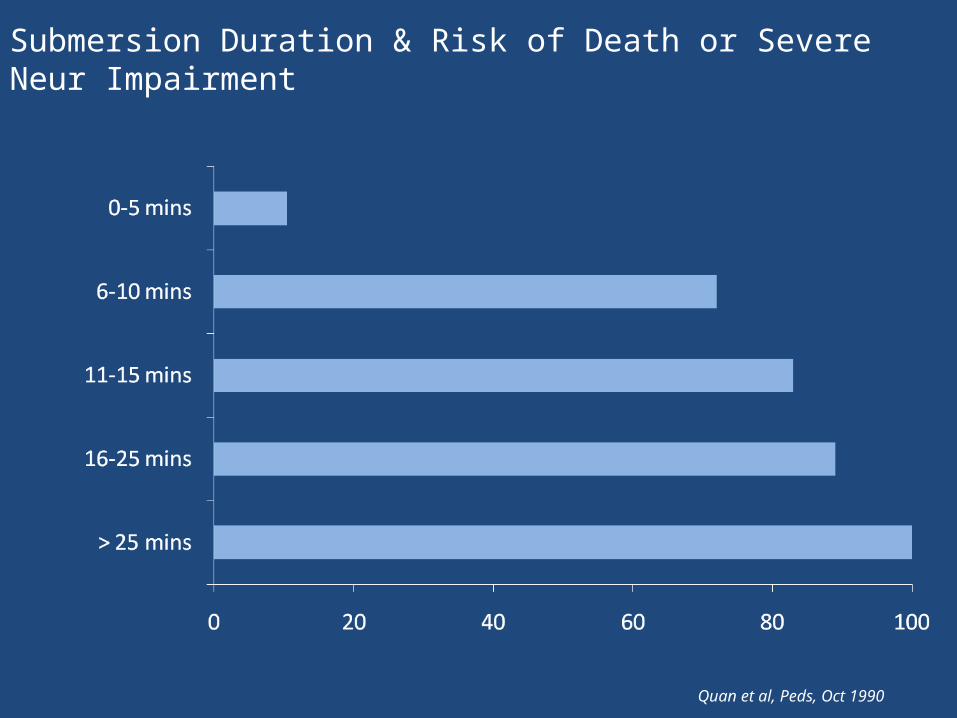
Submersion Duration & Risk of Death or Severe Neur Impairment
Quan et al, Peds, Oct 1990
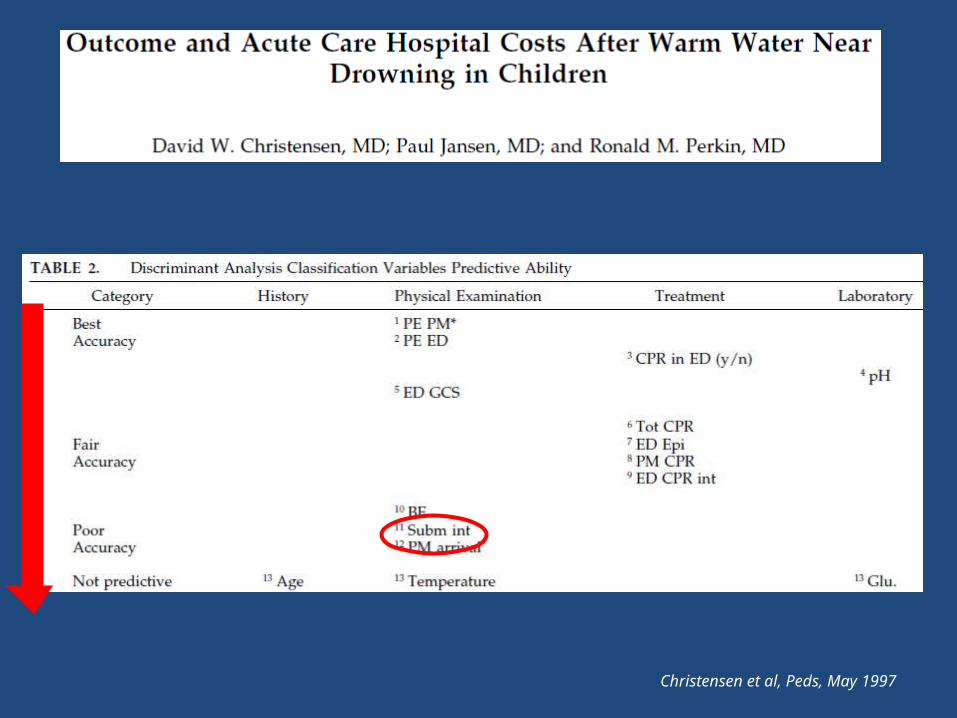
Christensen et al, Peds, May 1997
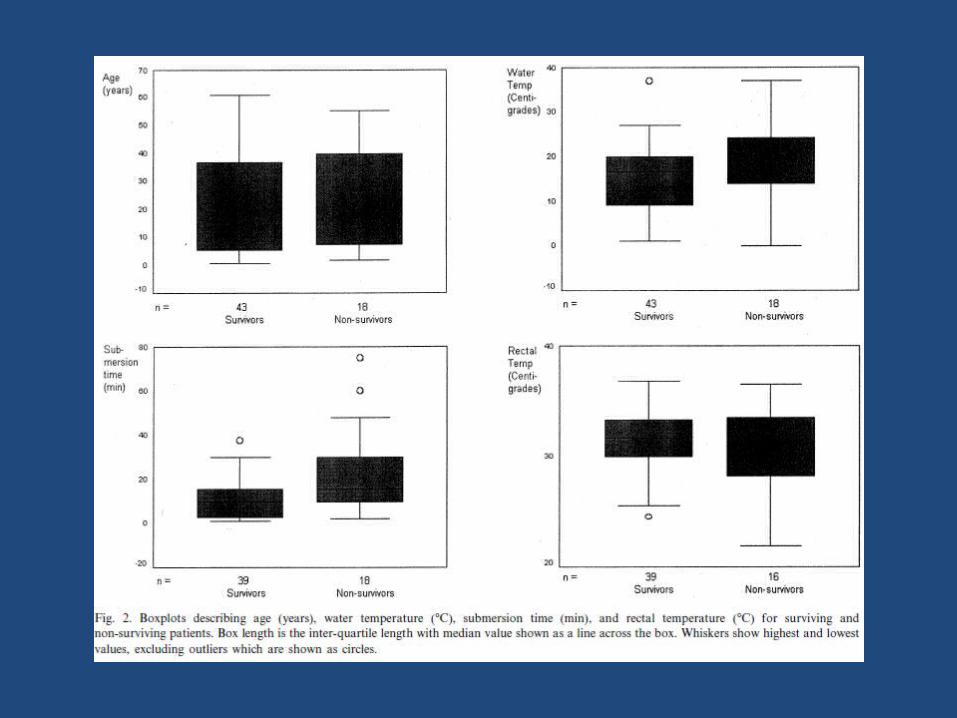
Impact of age, submersion time and water temp on outcome in near drowning Suominen et al, Resuscitation 2002
• Finland regional survey – most drownings occur in cold water
• 61 admissions to ICU Helsinki over 12 y: water temp, rectal temp, and estimated submersion time
• Median water temp 17C (range 0-33)…lower in survivors but much cross over
• 80% admission temp < 35C (no diff S & NS)• Est submersion time only independent predictor of
survival (5’ V 16’) but no clear cut off could be defined
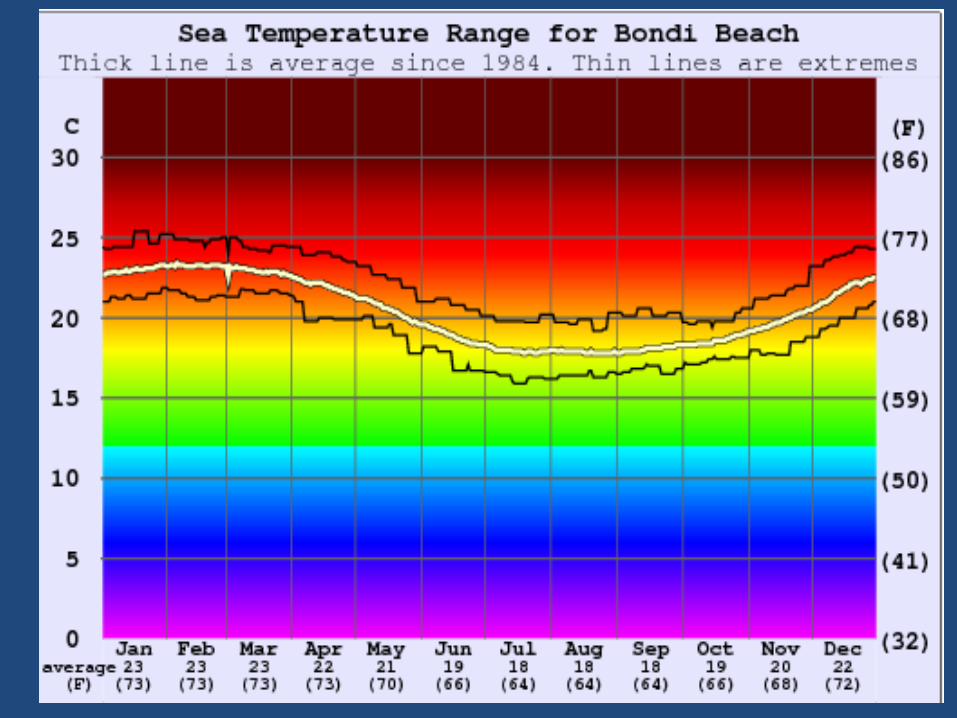
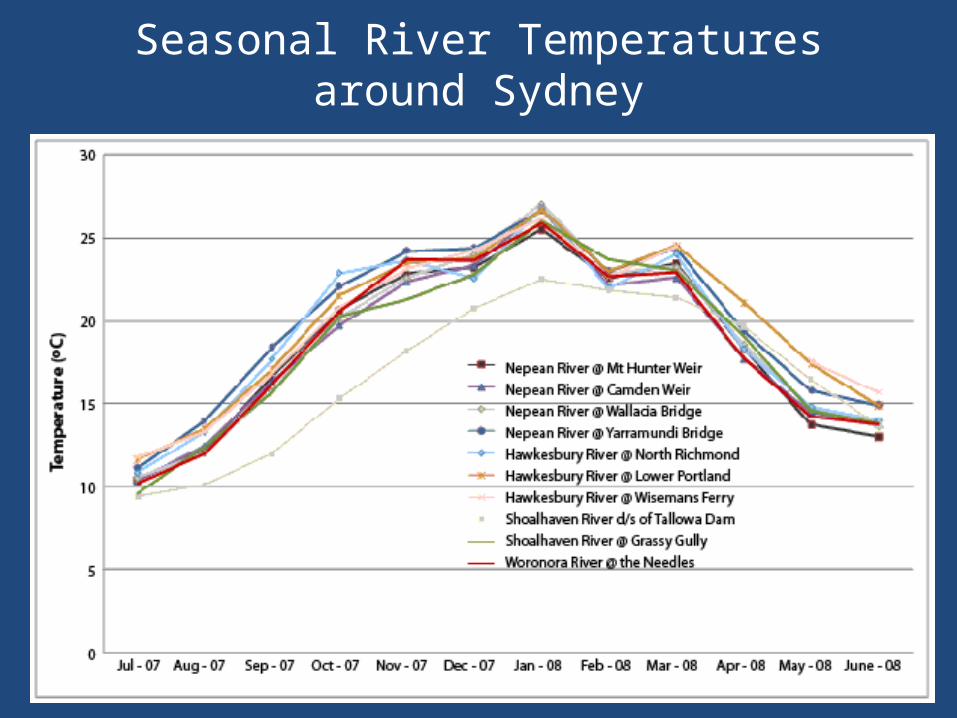
Seasonal River Temperatures around Sydney
ED Prediction of outcome ?
• Even fixed and dilated pupils, low GCS, need for CPR in ED have proven unreliable in individual cases
• Christensen et al (Peds, 1997): composite score based on ED physical exam (apnoea, coma) + need for CPR + lowest pH …..best available ……but even this 93% accurate in their hands
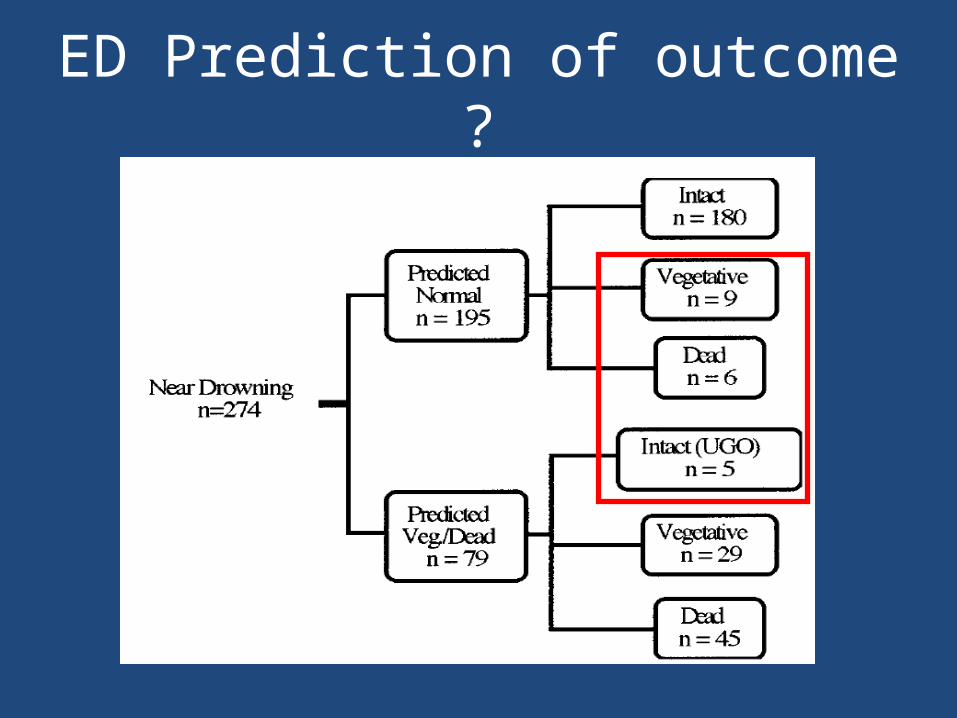
ED Prediction of outcome ?
ICU Prediction of Outcome ?• PE: GCS ≥ 6 or purposeful movement + intact
brainstem reflexes v likely good outcome• SEPS: absent SEPS 100% predictive of poor
outcome• Imaging:
Early (8h) abnormal CT strongly predictive for bad outcome; normal CT uninformative
MRI more specific but need 3-4 days to avoid inappropriate optimism
Drowning: PICU Management• Ventilation: normocapnia, optimise oxygenation,
minimise VILI• Circulation: fluids, inotropes, monitoring to optimise
haemodynamics, perfusion• Prophylactic anticonvulsants? No evidence• Continuous EEG monitoring of unconscious pt• Glucocorticoids? No evidence (Foex, ADC, 2002) ?
↑infection, ?? role later if ARDS• Prophylactic antibiotics? No evidence (Wood, ADC, 2010)
even with CXR changes…selects resistant bugs • Therapeutic Hypotherrmia “Cooling” ?
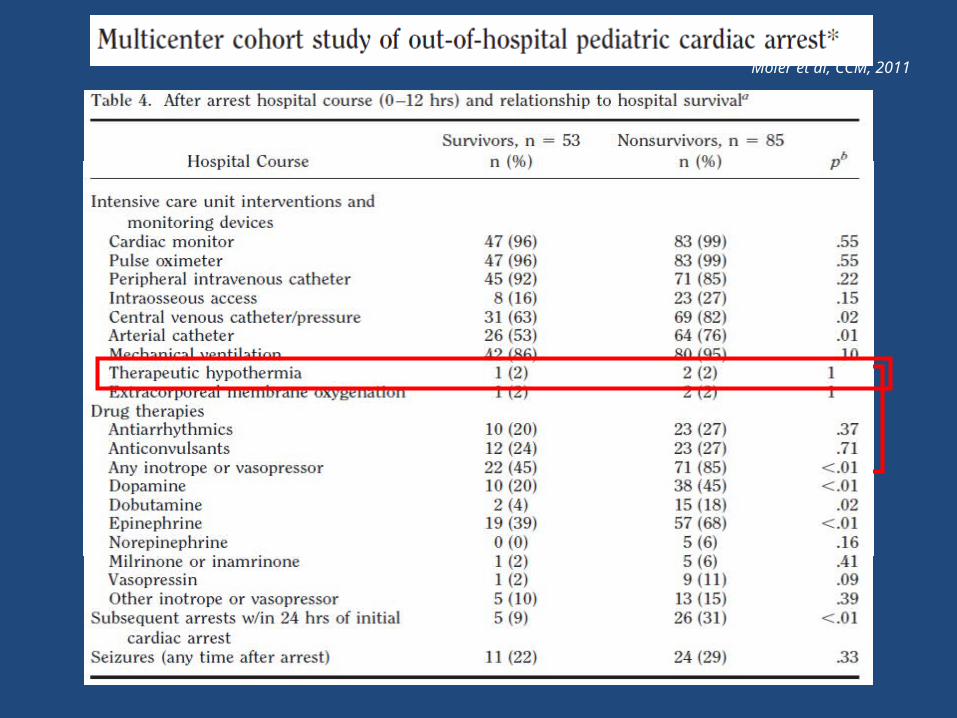
Moler et al, CCM, 2011
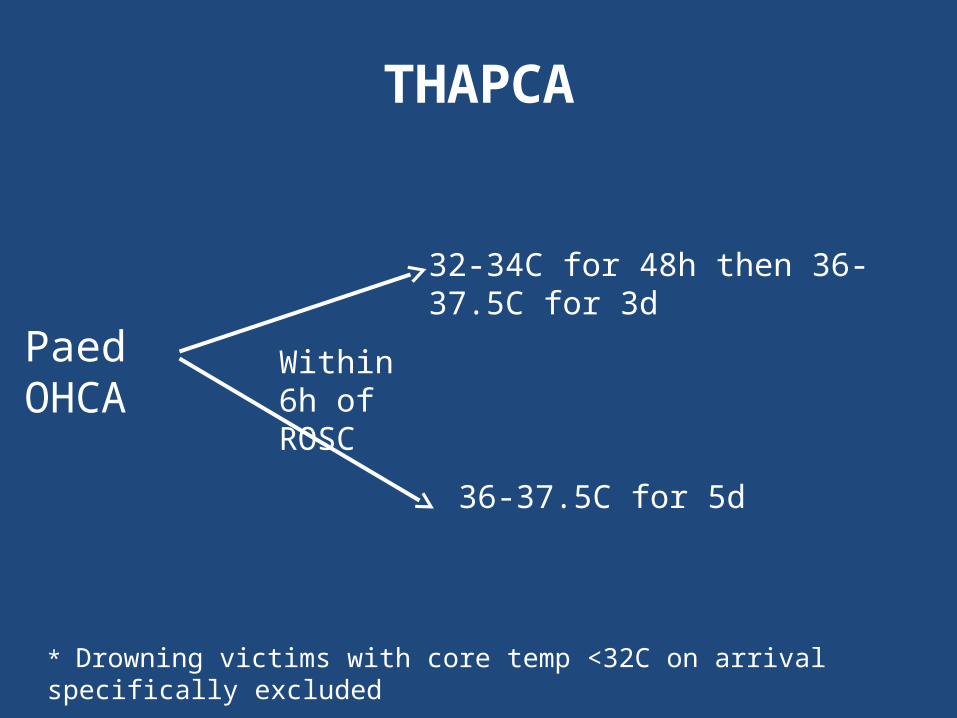
THAPCA
PaedOHCA
32-34C for 48h then 36-37.5C for 3d
36-37.5C for 5d
Within 6h of ROSC
* Drowning victims with core temp <32C on arrival specifically excluded
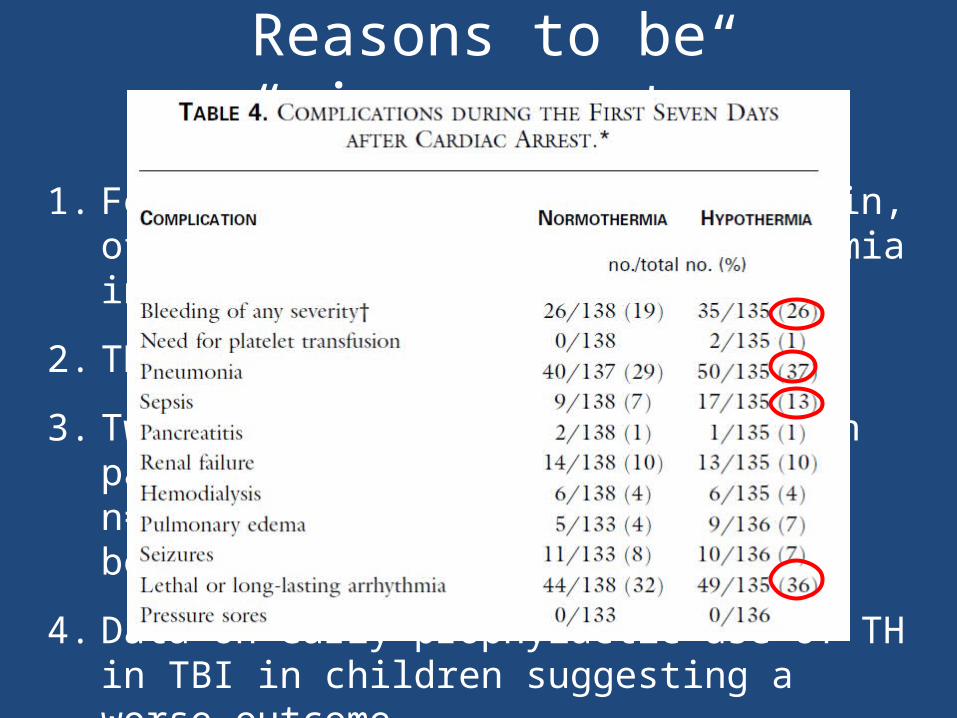
Reasons to be “circumspect”
1. Fever common, bad for injured brain, often not controlled to normothermia in control arms
2. TH does have risks
3. Two large retrospective studies in paed cardiac arrest (Pittsburgh n=181, CCTG n=222) have not shown benefit
4. Data on early prophylactic use of TH in TBI in children suggesting a worse outcome
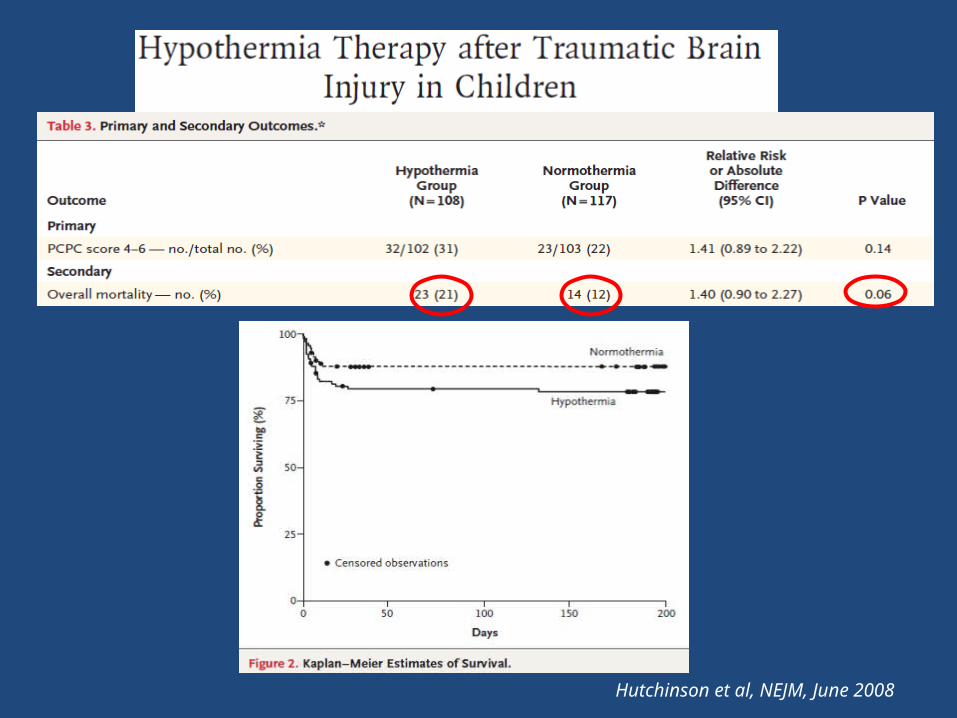
Hutchinson et al, NEJM, June 2008
Summary• Drowning remains a major cause death and
disability• Accurate outcome prediction in field and ED
problematic• Cold water protection theoretically feasible
but little evidence to support• Therapeutic hypothermia still waiting for good
evidence to support
Questions ?
“Drowning” by Ken Done
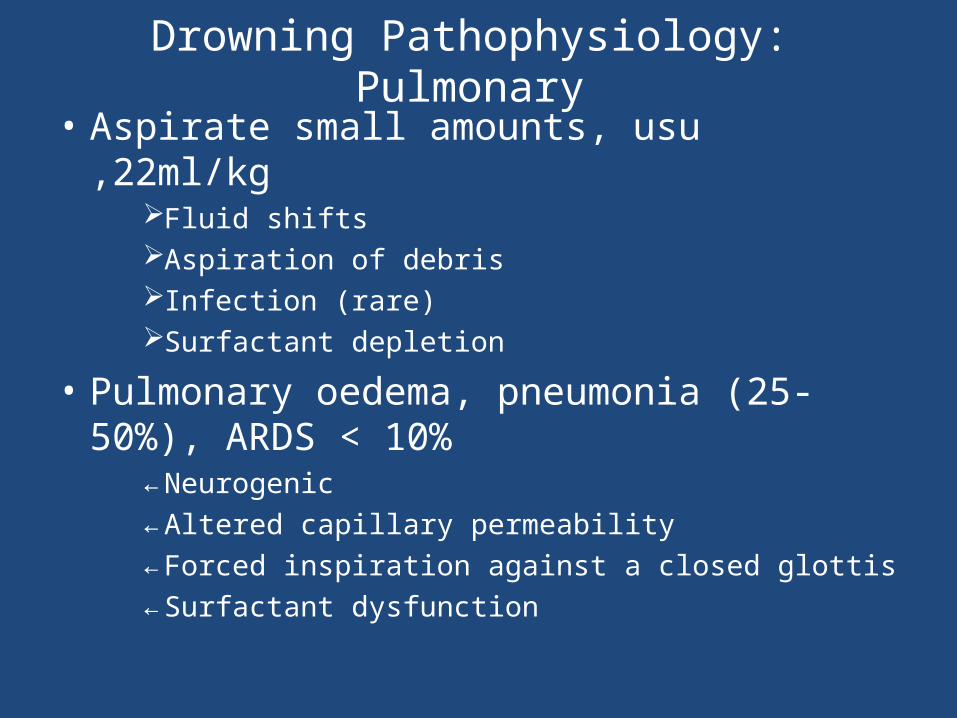
Drowning Pathophysiology: Pulmonary
• Aspirate small amounts, usu ,22ml/kgFluid shiftsAspiration of debrisInfection (rare)Surfactant depletion
• Pulmonary oedema, pneumonia (25-50%), ARDS < 10%
←Neurogenic←Altered capillary permeability←Forced inspiration against a closed glottis←Surfactant dysfunction
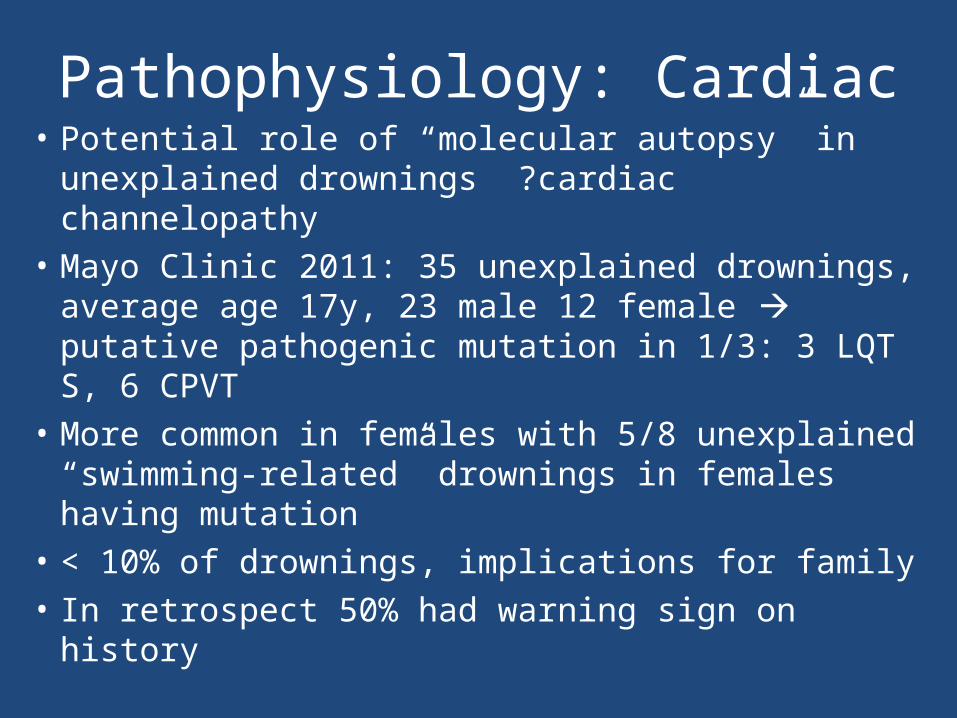
Pathophysiology: Cardiac• Potential role of “molecular autopsy” in
unexplained drownings ?cardiac channelopathy• Mayo Clinic 2011: 35 unexplained drownings,
average age 17y, 23 male 12 female putative pathogenic mutation in 1/3: 3 LQT S, 6 CPVT
• More common in females with 5/8 unexplained “swimming-related” drownings in females having mutation
• < 10% of drownings, implications for family• In retrospect 50% had warning sign on history
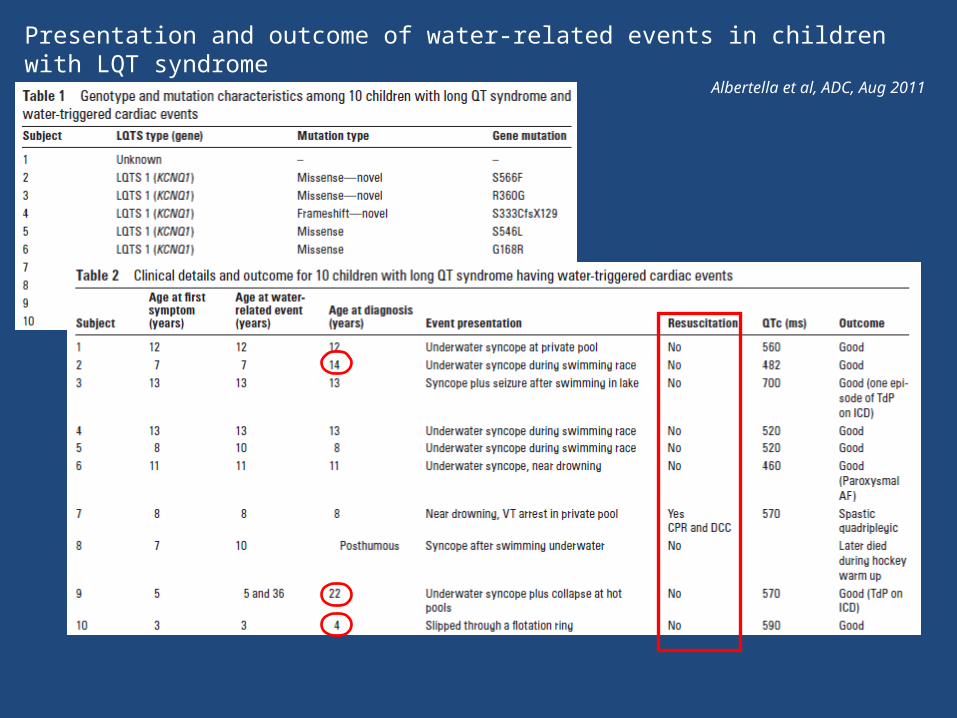
Presentation and outcome of water-related events in children with LQT syndromeAlbertella et al, ADC, Aug 2011
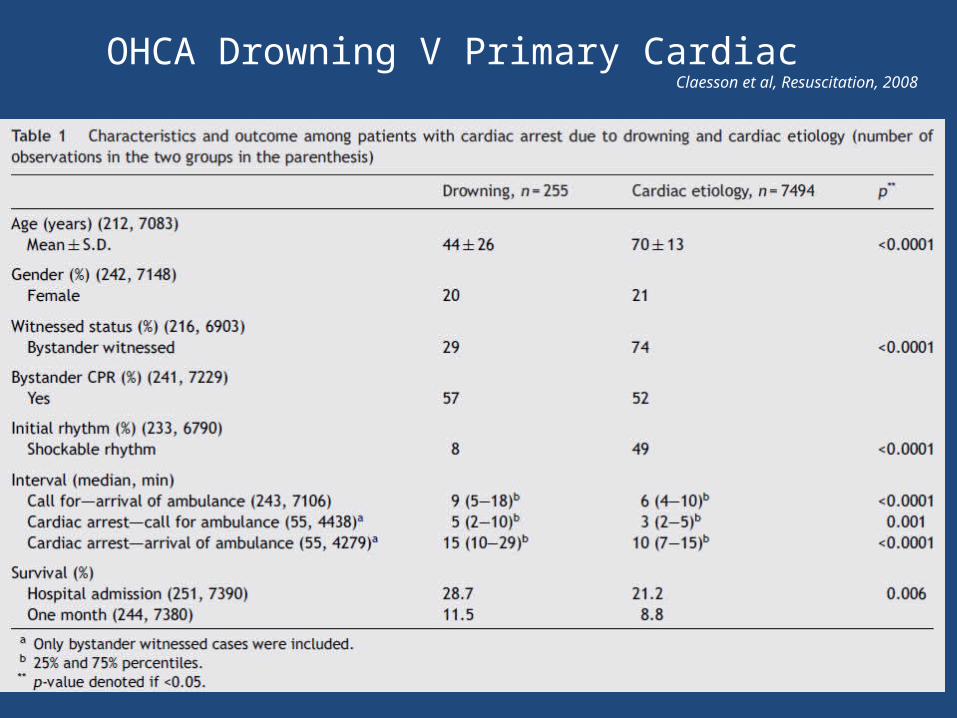
OHCA Drowning V Primary Cardiac Claesson et al, Resuscitation, 2008
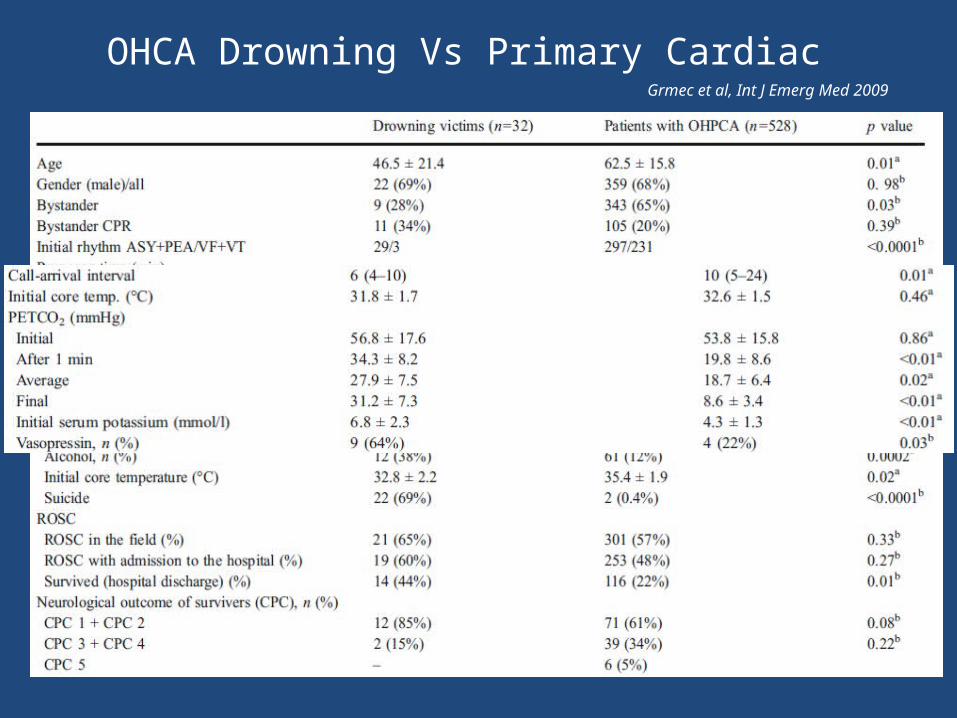
OHCA Drowning Vs Primary Cardiac Grmec et al, Int J Emerg Med 2009





























