Chalazion The meibomian glands are modified sebaceous glands
located in the tarsal plates which secrete the outer lipid layer of
the precorneal tear film. There are between 30 and 40 glands in the
upper tarsus and fewer (20-30) in the lower tarsus (. A chalazion
(meibomian cyst) is a chronic inflammatory lesion caused by
blockage of meibomian gland orifices and stagnation of sebaceous
secretions. Patients with acne rosacea and seborrhoeic dermatitis
are at increased risk of chalazion formation.
Slide 5
Slide 6
Examination shows a painless, roundish, firm lesion in the
tarsal plate Eversion of the lid may show an associated polypoid
mass (pyogenic granuloma) if the lesion has ruptured through the
tarsal conjunctiva. Occasionally, a cyst of the upper lid presses
on the cornea and causes blurred vision from induced
astigmatism.
Slide 7
Signs of chalazion (meibomian cyst) Painless, roundish, firm
lesion within tarsal plate May rupture through conjunctiva and
cause granuloma
Slide 8
Treatment is usually required for large, persistent lesions
although some small chalazia may disappear spontaneously. 1.
Surgery is by far the most common method of treatment. The eyelid
is everted with a special clamp and the cyst is incised and its
contents curetted through the tarsal plate. It is very important
that a meibomian gland carcinoma or a basal cell carcinoma is not
mistaken for 'recurrent chalazion'. In doubtful cases the lesion
should be biopsied and examined histologically.
Slide 9
Slide 10
2. Steroid injection into the lesion through the conjunctiva is
a good alternative to surgery. The success rate following one
injection is about 80%. In unresponsive cases a second injection
can be given 2 weeks later. 3. Systemic antibiotics may be required
as prophylaxis in patients with recurrent chalazia who have
associated acne rosacea or seborrhoeic dermatitis.
Slide 11
External hordeolum The glands of Zeis are modified sebaceous
glands that are associated with the lash follicles. The glands of
Moll are modified sweat glands whose ducts open either into a lash
follicle or directly onto the anterior lid margin between the
lashes. An external hordeolum (stye) is a small abscess caused by
an acute staphylococcal infection of a lash follicle and its
associated gland of Zeis or Moll. It may be associated with chronic
staphylococcal blepharitis.
Slide 12
Slide 13
External hordeolum Examination shows a tender inflamed swelling
in the lid margin which points anteriorly through the skin (. More
than one lesion may be present and occasionally minute abscesses
may involve the entire lid margin. In severe cases there may be a
preseptal cellulitis.
Slide 14
External hordeolum Treatment in most cases is unnecessary
because styes frequently resolve spontaneously or discharge
anteriorly, close to the lash roots. Resolution may be promoted by
the application of hot compresses and removal of the eyelash
associated with the infected follicle. Systemic antibiotics may be
necessary if there is severe preseptal cellulitis.
Slide 15
Internal hordeolum An internal hordeolum is a small abscess
caused by an acute staphylococcal infection of meibomian glands.
Examination shows a tender inflamed swelling within the tarsal
plate which is usually more painful than a stye. The lesion may
enlarge and then usually discharge either posteriorly through the
conjunctiva or anteriorly through the skin. Treatment by incision
may be required in some cases that do not discharge.
Slide 16
Acute hordeola Staph. abscess of meibomian glands Tender
swelling within tarsal plate May discharge through skin or
conjunctiva Staph. abscess of lash follicle and associated gland of
Zeis or Moll Tender swelling at lid margin May discharge through
skin Internal hordeolum ( acute chalazion ) External hordeolum
(stye)
Slide 17
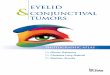
Molluscum contagiosum Molluscum contagiosum is an infection
caused by one of the pox viruses. Examination typically shows a
pale, waxy, umblicated nodule. Ocular irritation may occur as a
result of secondary chronic follicular conjunctivitis and
superficial keratitis.
Slide 18
Molluscum contagiosum Painless, waxy, umbilicated nodule
Chronic follicular conjunctivitis May be multiple in AIDS patients
Occasionally superficial keratitis SignsComplications
Slide 19
Treatment options include expression, shave excision,
cryotherapy or cauterization.
Slide 20
Strawberry naevus ( Capillary haemangioma) Presentation of this
rare tumour is typically within the first 6 months of birth.
Examination shows a raised red lesion. The tumour usually grows
until the age of about 12 months and then starts to involute
spontaneously. Complete resolution occurs in 75% of patients by the
age of 3 years.
Slide 21
The upper eyelid is most commonly involved and the tumour may
cause a mechanical ptosis. In some cases there is intraorbital
extension.
Slide 22
Capillary haemangioma Rare tumour which presents soon after
birth Starts as small, red lesion, most frequently on upper lid
Blanches with pressure and swells on crying Grows quickly during
first year May be associated with intraorbital extension Begins to
involute spontaneously during second year
Slide 23
Treatment is indicated if a large tumour threatens to produce
amblyopia by either obstructing the visual axis or inducing severe
corneal astigmatism. The most frequently used method of treatment
is steroid injection of a mixture, in equal parts, of triamcinolone
40 mg/ml and betamethasone 6mg/ml into the lesion using a 30-gauge
needle. The tumour usually begins to regress within 2 weeks and, if
necessary, second and third injections can be given after about 2
months. Reported but infrequent potential complications of steroid
injections include: skin depigmentation, fat atrophy, eyelid
necrosis and, very rarely, occlusion of the central retinal
artery.
Slide 24
Port wine stain Presentation is at birth. Examination shows a
sharply demarcated pink patch which darkens with age from red to
purple (naevus flammeus). The tumour is soft and subcutaneous, and
composed of large thin- walled vessels and capillaries.
Occasionally the involved skin is also swollen and coarse. The vast
majority of lesions occur in isolation, although more extensive
lesions involving the first and second divisions of the trigeminal
nerve are associated with a 45% incidence of glaucoma, and about 5%
are associated with multisystem disorders such as the Sturge-Weber
syndrome.
Slide 25
Treatment with an argon or yellow dye laser can reduce the
amount of skin discoloration.
Slide 26
Port-wine stain (naevus flammeus) Rare, congenital subcutaneous
lesion Segmental and usually unilateral Does not blanch with
pressure Ipsilateral glaucoma in 30% Sturge-Weber or
Klippel-Trenaunay-Weber syndrome in 5% Associations
Slide 27
Keratoacanthoma Presentation is typically in adult life with a
fast-growing skin lesion. Examination shows an erythematous papule
which turns into a firm, pinkish, indurated nodule with a
keratin-filled crater Spontaneous resolution is common but it may
take up to a year and leave a scar.
Slide 28
Treatment involves excision and histological examination
because squamous cell carcinoma may have a similar clinical
appearance; rarely, a keratoacanthoma may reveal histological
evidence of invasive squamous cell carcinoma at deeper levels of
sectioning.
Slide 29
Keratoacanthoma Uncommon, fast growing nodule Acquires rolled
edges and keratin-filled crater Involutes spontaneously within 1
year Lesion above surface epithelium Central keratin-filled crater
Chronic inflammatory cellular infiltration of dermis
Slide 30
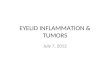
Pigmented naevi Naevi (moles) tend to become more pigmented at
puberty. Their appearance and classification are determined by
their location within the skin as indicated below. An intradermal
naevus is usually elevated and may be pigmented or non-pigmented.
It is the most common type and, when located on the eyelid margin,
lashes may be seen growing through the lesion. It has no malignant
potential. A junctional naevus is usually flat and well
circum-scribed with a uniform brown colour. The naevus cells
contained within the lesion are located at the junction of the
epidermis and dermis. It has a low potential for malignant
transformation. A compound naevus is characterized by both
intradermal and junctional components.
Slide 31
Intradermal naevus Junctional naevus
Slide 32
Naevi Appearance and classification determined by location
within skin Tend to become more pigmented at puberty Elevated
Intradermal May be non-pigmented No malignant potential Flat,
well-circumscribed Low malignant potential Junctional Has both
intradermal and junctional components Compound Pigmented
Slide 33
Miscellaneous lesions A cyst of Moll is a small, round,
non-tender, translucent fluid-filled lesion on the anterior lid
margin A cyst of Zeis is similar but, because it contains oily
secretions, it is less translucent. A sebaceous cyst arises from an
ordinary sebaceous gland and is characterized by a central punctum
with retained cheesy secretions. It is rarely found on the eyelid
although it may occur at the inner canthus.
Slide 34
Translucent On anterior lid margin Cyst of Moll Similar to cyst
of Moll Not confined to lid margin Eyelid cysts Opaque On anterior
lid margin Cyst of Zeis Eccrine sweat gland hidrocystoma Sebaceous
cyst Cheesy contents Frequently at inner canthus
Slide 35
Milia are small, white, round, superficial cysts which tend to
occur in crops. They are derived from hair follicles or sebaceous
glands. Squamous cell papilloma is the most common benign tumour of
the eyelids. It may be broad based (sessile) or pedunculated.
Seborrhoeic keratosis (basal cell papilloma) is a slow-growing,
discrete, greasy, brown, round or oval lesion with a friable
verrucous surface.
Slide 36
Seborrhoeic Common in elderly Discrete, greasy, brown lesion
Friable verrucous surface Flat stuck-on appearance Actinic Most
common pre-malignant skin lesion Rare on eyelids Affects elderly,
fair-skinned individuals Flat, scaly, hyperkeratotic lesion
Keratoses
Slide 37
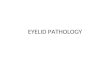
Xanthelasma Usually bilateral and located medially Common in
elderly or those with hypercholesterolaemia Yellowish, subcutaneous
plaques containing cholesterol and lipid
Slide 38
Viral wart (squamous cell papilloma) Most common benign lid
tumour Raspberry-like surface Pedunculate d Sessil e
Slide 39
Actinic keratosis is characterized by a rough, dry, scaly
lesion on an erythematous base. It typically affects elderly
fair-skinned individuals who have been exposed to excessive
sunlight. It is a pre-malignant lesion because it may occasionally
undergo transformation into a squamous cell carcinoma.
Xanthelasmata are yellowish subcutaneous plaques of cholesterol and
lipid which typically occur at the medial aspects of the eyelids in
elderly individuals. A cutaneous horn is frequently associated with
an underlying dysplastic (e.g. actinic keratosis) or neoplastic
(e.g. squamous cell carcinoma) lesion. The lesion should therefore
be biopsied and a portion of the base excised to determine the
underlying pathology.