Embed Size (px)
Citation preview

IN THE NAME OF GOD

Electrocardiogram
Dr.Bayat,MDAssistant professor of cardiology
Echocardiologist


For more presentations www.medicalppt.blogspot.com
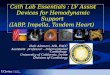
Normal Impulse Conduction
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers

For more presentations www.medicalppt.blogspot.com
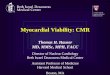
Impulse Conduction & the ECG
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers


For more presentations www.medicalppt.blogspot.com
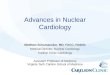
The “PQRST”
P wave - Atrial depolarization
• T wave - Ventricular repolarization
• QRS - Ventricular depolarization

For more presentations www.medicalppt.blogspot.com
The PR Interval
Atrial depolarization +
delay in AV junction (AV node/Bundle of
His)
(delay allows time for the atria to contract before the ventricles contract)

P wave:When th atria depolarize before atrial contraction begins
QRS COMPLEX:ventricular depolarization before contraction
T WAVE:ventricular repolarization wave,250 to 350 msec after depolarizatiuon
Characteristics of the normal ECG

No potential is recordrd in the ECG when the ventricular muscle is either completely polarized or completely depolarized
Only when the muscle is partly polarized and partly depolarized does current flow from one part of the ventricle to another part and therefore current also flows to the surface of the body to produce the ECG

P and QRS occurs at the begining of the atrial and ventricular contraction
Ventricles remain contracted until after repolarization has occurred that is until after the end of the T wave
Atrial repolarization,150-200 msec after termination of p wave(atrial T wave )Usually obscured by larger QRS complex
T wave :200 msec after QRS,and period 150 msec(350 msec),lower voltage due to prolonged length
Relationship of atrial and ventricular contraction to the waves of the ECG

Paper speed:25 mm/sec,each 1mm represents 40 msec(5:200 msec)
Voltage :each small box,0.1 mv Normal voltage: QRS=1-1.5 MV P WAVE=0.1-0.3 MV T WAVE=0.2-0.3 MV
Voltage and time calibration of the ECG

For more presentations www.medicalppt.blogspot.com
The ECG Paper Horizontally
◦ One small box - 0.04 s◦ One large box - 0.20 s
Vertically◦ One large box - 0.5 mV

For more presentations www.medicalppt.blogspot.com
The ECG Paper (cont)
Every 3 seconds (15 large boxes) is marked by a vertical line.
This helps when calculating the heart rate.NOTE: the following strips are not marked
but all are 6 seconds long.
3 sec
3 sec



Physiogical measurements
PR interval = 0.12-0.2 s (120-200 ms)QRS duration = 0.06-0.1 s (60-100 ms)QT interval = 0.30-0.46 s (300-460 ms)for heart rates varying between 45 to 115 beats per minute. The QT interval lengthens with bradycardia and shortens with tachycardia.

P-Q or P-R interval:atrial ,AV node and His-purkinje conduction,160 msec(120-200msec)
Q-T INTERVAL:contraction of the ventricles,350 msec
HEART RATE:60/RR INTERVAL(SEC)

THREE BIPOLAR LIMB LEADS LEAD I:Right arm(-) to left arm(+) LEAD II:Right arm(-) to left leg(+) LEAD III:left arm(-) to left leg(+)
EINTHOVEN’ S TRIANGLEEINTHOVEN’S LAW: SUM OF THE VLTAGES IN LEAD I+III=LEAD II
ECG LEADS






Neg electrode(indifferent electrode) is connected through equal electrical resistance to the rigth arm,left leg,left arm and positive electrode is connected to to anterior chest wall
V1,V2 are mainly negative(direction of electronegativity) and V4,V5,V6 ARE mainly positive
CHEST LEADS OR PRECORDIAL LEADS(V1-V6)


avR,avL,avF
avR recording is inverted
Augmented unipolar limb leads





In a normal heart the average direction of the vector during spread of the depolarization wave through the ventricle ,called the mean QRS vector,is about 59 degrees
Septal vector Ventricular Depolarization Ventricular repolarization
Principles of vectorial analysis of ECG

When the cardiac impulse enters the ventricular throuh the AV bundle the first part of ventricle to depolarized is left endocardial surface of the septum then depolarization spreads rapidly to involve both endocardial surfaces of the septum next spreads along the endocardial surface of 2 ventricles.finally spreads through the ventricle muscle to the outside of heart

The ventricular muscle had just begun to be depolarized representing an instant about 0.01 s after the onset of depola .at this time the vector is short because only small portion of the ventricular –septum- is depola.so all electrocardiographic voltages are low ,as recorded to the right of the ventricular muscle for each of the leads.the voltage in lead II is greater than the voltage in lead I and III because the heart vector extends mainly in the same direction as the axis of lead II.












When the vector in the heart is in a direction almost prependicular to the axis of the lead,the voltage recorded in the ECG of this lead is very low,conversly when the heart vector has almost exactly the same axis as the lead axis,essentially the entire voltage of the vector will be recorded.










ABNORMAL Q wave=>40 msec or >1/4 R WAVE
NORMAL Q WAVE IN LEAD III,aVR,V1,V2



Depolarization is much slower than ventricles
Due to no purkinje system
Repolarization from the site of first depolarization(SA node )therefore repolarization vector is opposite of depolarization vector)Atrial axis=0-75 degrees
Depolarization of the atria- p wave






P duration=0.08-0.1 msec
Voltage=0.1-0.2 mv RA enlargement-->2.5 mm LA enlargement--increased p duration



vectocardiogram



Determining the electrical axis from standard lead ECG


NORMAL AXIS=59 degrees(-30 to105) >40y-30->90 <40y0-105 TO THE LEFT:obesity,lie down,end of deep
expiration LVH,RVH LBBB,RBBB
AXIS DEVIATION

LAD

RAD



T &QRS angle


Normal pattern

In childhood

Sometimes in young paients(poor r progration)

Early repolarization

rSr’,r’<r(<5mm)

S1 S2 S3(S2>S3)


For voltage measuring:from the peak of the R wave to the bottom of S wave
When the sum of the voltages of all the QRS of complexs of three standard leads is greater than 4 millivolts,the patient is considered to have a high-voltage ECG
RVH,LVH
Abnormal voltages of the QRS complex


Old MI(decreased voltage and prolongation of QRS)
Pericardial effusion(short-circuits the electrical potentials)
Pleural effusion
Pulmonary emphysema(lungs act as an insulator)
DECREASED VOLTAGE OF THE ECG

Normal QRS lasts 0.06-0.08 second Prolonged QRS(0.09 to 0.12) due to
ventricular hyperthrophy or dilation
In purkinje system block (more than 0.12)
Bizarre QRS complex(in multiple scar tissue and block in muscles and purkinje system that leads to irregular impulse conduction and rapid shifts in voltages and axis deviationds
Prolonged and bizarre patterns of the QRS complex

Damaged heart muscle remains partially or totally depolarized all the time that introduced currents flows between the pathologically depolarized and the normally polarized areas even between heart beats,this is called a current of injury
The most common cause is ischemia caused by local coronary occlusion
Current of injury

At the end of the depolarization no current flow is seen but at the end of the repolarization injured area is depolaried and leads to current flow from this site to other parts and TP SEGMENT deviation is occurred
j-point:the exact point on ECG which the wave of depolarization just completes its passage through the heart,which occurs at the end of the QRS complex


T wave is normally positive in all standard bipolar limb leads
T wave becomes abnormal when the normal sequence of repolarization doesnot occur
Etiology:mild ischemia(shortening of depolarization),delayed conduction of depolarization impulse (LBBB)
Abnormalities in the T wave

Effect of digitalis on the T wave:In overdosage,depolarization duration in one part of the ventricles ,may be increased out of proportion to that of other parts(biphasic T wave or T wave inversion)