Embed Size (px)
Citation preview
Draft Preliminary Recommendations
Precision Medicine Task Force
September 18, 2015Leslie Kelly Hall, Co-ChairJon White, Co-Chair
2
Agenda
• Opening Remarks, Work Plan Review• NIH ACD Update • HL7 Genomics Workgroup• Review and Finalize Recommendations• Next Steps

3
Precision Medicine Task Force Membership
Member OrganizationCo-ChairsLeslie Kelly Hall HealthwiseJon White ONC / Agency for Healthcare Research and Quality (AHRQ)MembersMary Barton National Committee for Quality Assurance (NCQA)Lisa Gallagher Healthcare Information and Management Systems Society (HIMSS)David McCallie, Jr. Cerner CorporationAndrey Ostrovsky Care at HandEric Rose Intelligent Medical ObjectsAndrew Wiesenthal Deloitte Consulting, LLPFederal Ex OfficioJames Breeling Veterans Health Administration (VHA)Josh Denny National Institutes of Health (NIH)Christina Heide HHS Office for Civil Rights (OCR)Betsy Humphreys National Library of Medicine (NLM)Mitra Rocca Food and Drug Administration (FDA)Invited GuestsMina Hsiang United States Digital Service (USDS) / Office of Management and Budget (OMB)Claudia Williams White House Office of Science & Technology Policy ONC StaffMaya Uppaluru ONC – Federal Staff LeadDebbie Bucci ONC - Technical Advisor

Precision Medicine Initiative
Mission Statement To enable a new era of medicine through research,
technology, and policies that empower patients, researchers, and providers to work together toward
development of individualized treatments.
4
5
Task Force Charge
• Identify opportunities for innovative collaboration around pilots and testing of standards that support health IT interoperability for precision medicine
• Recommend existing standards that are currently ready to support PMI
• Identify emerging standards and reference implementations that may require further pilot testing in order to support PMI
• Identify gaps in available data standards related to PMI
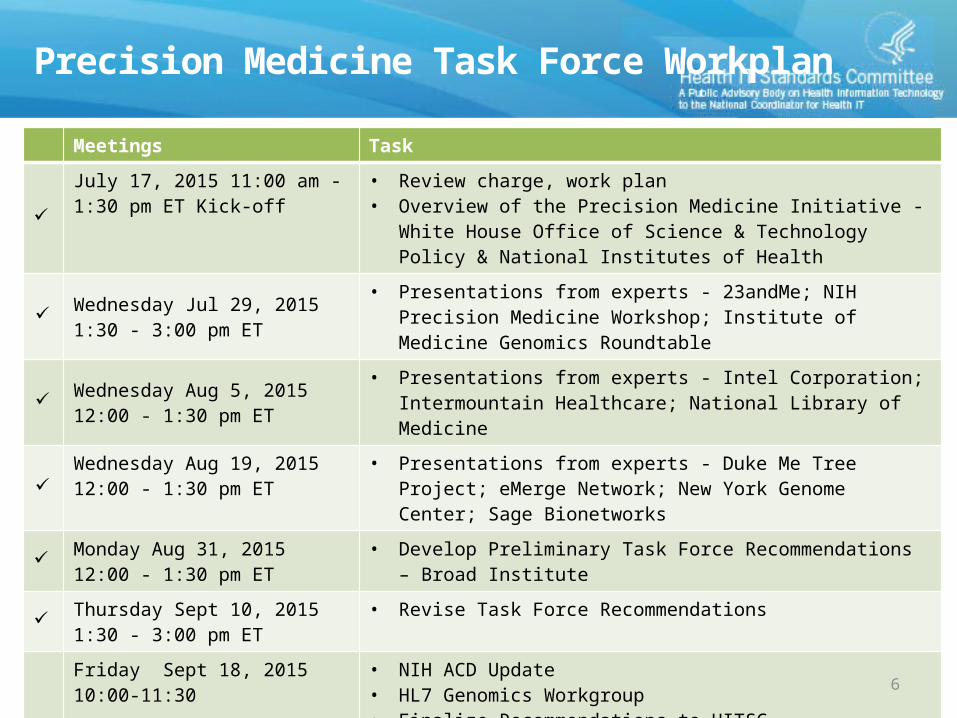
Meetings Task
July 17, 2015 11:00 am - 1:30 pm ET Kick-off
• Review charge, work plan• Overview of the Precision Medicine Initiative - White House Office of
Science & Technology Policy & National Institutes of Health
Wednesday Jul 29, 2015 1:30 - 3:00 pm ET
• Presentations from experts - 23andMe; NIH Precision Medicine Workshop; Institute of Medicine Genomics Roundtable
Wednesday Aug 5, 2015 12:00 - 1:30 pm ET
• Presentations from experts - Intel Corporation; Intermountain Healthcare; National Library of Medicine
Wednesday Aug 19, 2015 12:00 - 1:30 pm ET
• Presentations from experts - Duke Me Tree Project; eMerge Network; New York Genome Center; Sage Bionetworks
Monday Aug 31, 2015 12:00 - 1:30 pm ET
• Develop Preliminary Task Force Recommendations – Broad Institute
Thursday Sept 10, 2015 1:30 - 3:00 pm ET
• Revise Task Force Recommendations
Friday Sept 18, 2015 10:00-11:30 • NIH ACD Update • HL7 Genomics Workgroup• Finalize Recommendations to HITSC
September 22, 2015 – HITSC Meeting 10:00 am – 12:30 pm ET
• Present final recommendations
Precision Medicine Task Force Workplan
6
7
NIH ACD Update
8
NIH ACD Recommendations
• Hybrid model of centralized and federated data– Coordinating Center will centrally store a curated, analysis-ready, core
data set on all participants using common data models, and serve as a hub for accessing data and biospecimens.
– Hybrid data and analytics architecture will leverage both centralized data storage of a growing amount of core data, as well as federated access to additional data at the nodes across the network
• Common, growing core data set– Collection of diverse set of data types: EHRs, claims, surveys, baselines
health exams, mobile health, biologic investigations– Development of standardized and automated mechanisms to acquire
clinical data from healthcare provider organizations (HPOs)– Rigorous data curation for analysis-ready data sets

9
NIH ACD Recommendations:Acquiring research data for the PMI cohort
• From participating healthcare provider organizations (HPOs)– A longitudinal record of care (e.g., academic medical centers, Federally
Qualified Health Center (FQHCs), vertically integrated private health care organizations, and vertically integrated governmental organizations)
– Ability to consent volunteers to the PMI cohort, to share EHR data, and to collect new biospecimens
– [Those providers that] can contribute significantly to the size of the PMI cohort should be preferred.
• From individuals– Must be living in the U.S. or U.S. Territory and be able to visit a U.S. health
provider– Provide certain amount of core data, including baseline phenotype assessment
and data quality– Must be recontactable, provide a biospecimen, agree to share EHR data
10
NIH ACD Recommendations:Security & Privacy
• Ensure appropriate safeguards• Use of de-identified data whenever feasible, provide
appropriate data protections• Discourage data from being copied outside the secure
computing environment• Clearly articulated breach response and notification plan• NIH seeks to fill privacy gaps such as
– FOIA exemption for genomic data– Unauthorized re-identification– Require data users to secure a certificate of confidentiality

11
NIH ACD Recommendations
• Core data set– Standard self-report measures via direct patient assessment – Brief, standardized baseline health exam at enrollment – Structured clinical data
• ICD & CPT codes with dates• High value clinical lab results in structured format (e.g., eMERGE, PCORnet, Sentinel, MPOG). • Measure and reference ranges.• Medication data (e.g., start/stop date, inpatient or outpatient, dose, route, frequency, strength)• Vital measurements• Record of all encounters • Health plan data (enrollment and disenrollment dates, type of coverage)
– Biospecimen-derived data– Mobile health data
• Clinical data from direct volunteers– Ability to submit EHR data that to PMI cohort through existing data transfer protocols
(Blue Button, patient portals & VDT)
12
HL7 Clinical Genomics Workgroup

HL7 Clinical Genomics Work Group Mission
• Create and promote standards by enabling the communication between…parties of the clinical and personalized genomic data
• Focus: Personalization of the genomic data and the linking to relevant clinical information.
• Facilitate the development of common standards for clinical research information management across a variety of organizations, including:– National and international government agencies– Regulatory bodies, private research efforts, and sponsored research
• Facilitate availability of safe and effective therapies by improving the processes and efficiencies associated with regulated clinical research
13
14
HL7 Clinical Genomics Work GroupLeadership
• Co-Chairs– Gil Alterovitz , Boston Children's Hospital– Siew Lam MD MSc, Intermountain Healthcare– Bob Milius PhD, National Marrow Donor Program– Amnon Shabo PhD, Philips Healthcare– Mollie Ullman-Cullere, Partners HealthCare System, Inc.
• Facilitators– Amnon Shabo PhD, Philips Healthcare– Grant Wood, Intermountain Healthcare– Joyce Hernandez
http://www.hl7.org/Special/committees/clingenomics/leadership.cfm
15
Draft Recommendations

16
Recommendations
• Background - EHR likely to capture more phenotypic data from MDs and patient– Phenotypic data are collected already such as problems, medications, allergies, etc.– Core problem: Don't have a standard data model for EMR and categorical standard responses for
many basic types of information
• Recommendations - Advance filling gaps related to key missing components with a short term focus on supporting the PMI cohorts. Gaps include: – Transport mechanisms (for transmission among EHR, lab and individual)– Data structure– Value sets
• Standards and Recommendations were placed into four categories:1. Readily Applicable Standards for PMI (Green) – can be put to use to support the cohorts2. Promising Standards for PMI (Yellow) – may require additional effort to bring to use3. Standards Gaps for PMI (Red) – areas where considerable work is needed4. Accelerators (Blue) – opportunities to advance / improve standards
• Recommended Actions to Advance need to be assigned to each standard, emerging standard, recommendation, etc.– Short-term versus long-term priorities
17
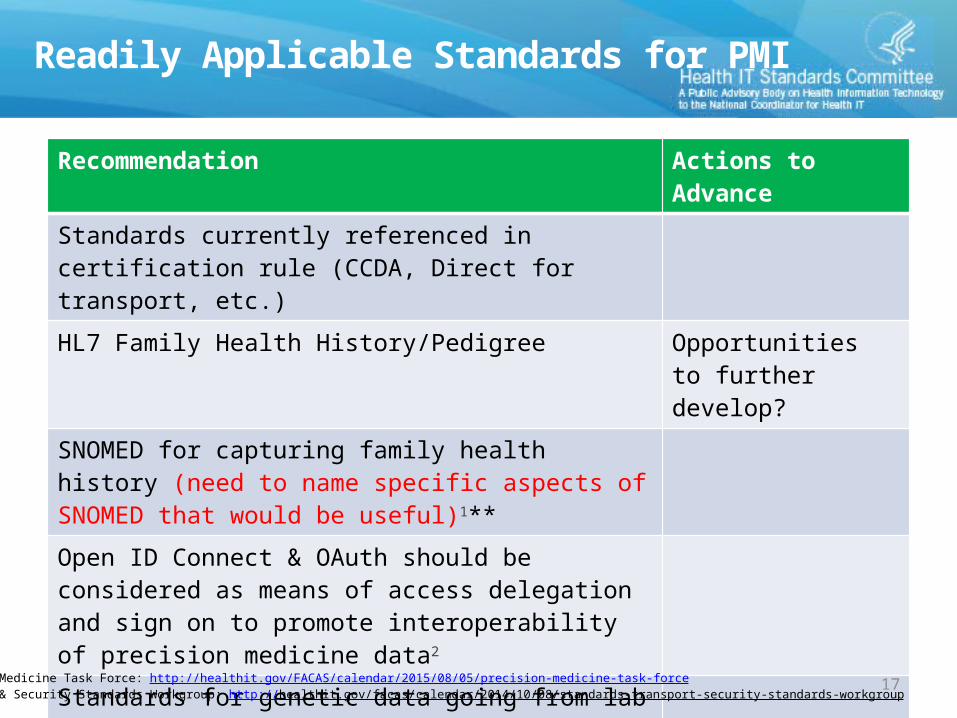
Readily Applicable Standards for PMI
Recommendation Actions to Advance
Standards currently referenced in certification rule (CCDA, Direct for transport, etc.)HL7 Family Health History/Pedigree Opportunities to
further develop?SNOMED for capturing family health history (need to name specific aspects of SNOMED that would be useful)1**Open ID Connect & OAuth should be considered as means of access delegation and sign on to promote interoperability of precision medicine data2
Standards for genetic data going from lab to EHR (need to name specific standards)Key: Actions to Advance1 – Form Task Force to advance2 - Apply accelerators (e.g., S&I Initiative, pilot project, policy guidance) to existing standards by ONC3 - Follow existing standards process
1) Precision Medicine Task Force: http://healthit.gov/FACAS/calendar/2015/08/05/precision-medicine-task-force2) Transport & Security Standards Workgroup: http://healthit.gov/facas/calendar/2014/10/08/standards-transport-security-standards-workgroup
18
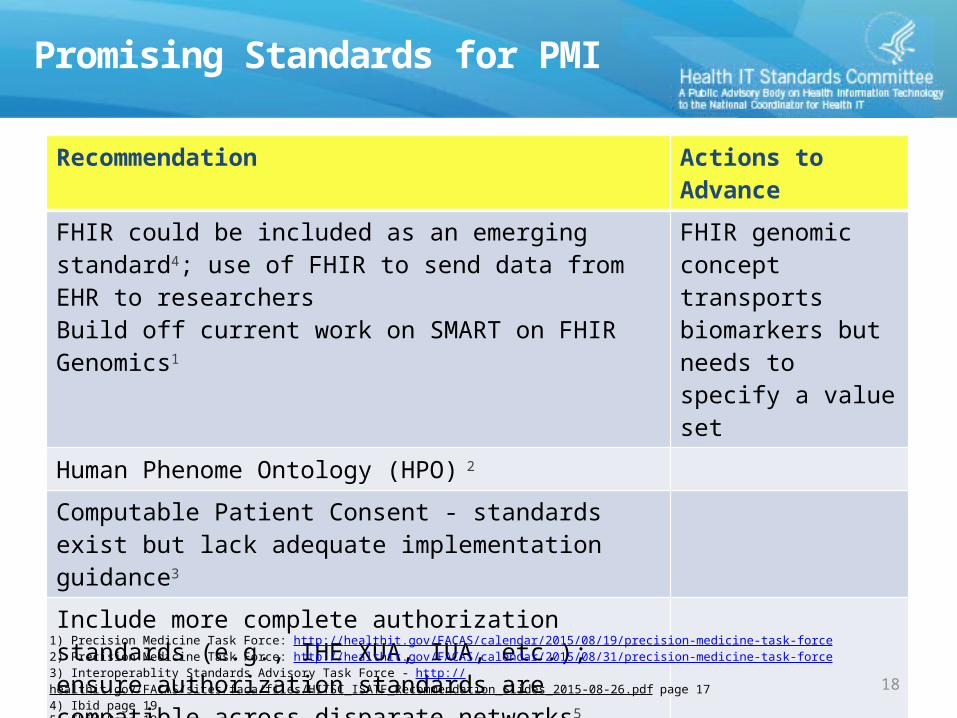
Promising Standards for PMI
Recommendation Actions to Advance
FHIR could be included as an emerging standard4; use of FHIR to send data from EHR to researchersBuild off current work on SMART on FHIR Genomics1
FHIR genomic concept transports biomarkers but needs to specify a value set
Human Phenome Ontology (HPO) 2
Computable Patient Consent - standards exist but lack adequate implementation guidance3
Include more complete authorization standards (e.g., IHE XUA, IUA, etc.); ensure authorization standards are compatible across disparate networks5
IOM Genomics Roundtable, GA4GH workKey: Actions to Advance1 – Form Task Force to advance2 - Apply accelerators (e.g., S&I Initiative, pilot project, policy guidance) to existing standards by ONC3 - Follow existing standards process
1) Precision Medicine Task Force: http://healthit.gov/FACAS/calendar/2015/08/19/precision-medicine-task-force2) Precision Medicine Task Force: http://healthit.gov/FACAS/calendar/2015/08/31/precision-medicine-task-force3) Interoperablity Standards Advisory Task Force - http://healthit.gov/FACAS/sites/faca/files/HITSC_ISATF_Recommendation_Slides_2015-08-26.pdf page 174) Ibid page 19 5) Ibid Page 19

19
Standards Gaps for PMI
Recommendation Actions to Advance
ONC should convene a stakeholder group to address computable patient consent; there exist standards but without clear implementation guidance1
Race and Ethnicity: OMB Standard may be suitable for some purposes but inadequate for precision medicine and directing therapy or clinical decisions2
1 – Form Task Force
ONC should work with stakeholders to define what is the minimum data set and/or means required to make precision medicine data useful in an EMR and in a clinical setting3
1 – Form Task Force
Microbiome data standards4
Key: Actions to Advance1 – Form Task Force to advance2 - Apply accelerators (e.g., S&I Initiative, pilot project, policy guidance) to existing standards by ONC3 - Follow existing standards process
1) Interoperablity Standards Advisory Task Force – Page 17 http://healthit.gov/FACAS/sites/faca/files/HITSC_ISATF_Recommendation_Slides_2015-08-26.pdf2) Ibid. page 153) Precision Medicine Task Force: http://healthit.gov/FACAS/calendar/2015/08/05/precision-medicine-task-force4) Precision Medicine Task Force: http://healthit.gov/FACAS/calendar/2015/08/31/precision-medicine-task-force

20
Accelerators
Recommendation Actions to Advance
Additional ONC investment in pilots of FHIR for research/individual data donation use case?Incorporation of HPO in the UMLS Metathesaurus and connections between HPO and SNOMED CT2
OMIM: Codes for phenotypes, genotypes and links between the twoHUGO: De facto standard for naming of genes
dpSNP and ClinVar: Opportunity to develop a service that would consumer data from these sources and synthesize so it’s digestible for a clinical information systemKey: Actions to Advance1 – Form Task Force to advance2 - Apply accelerators (e.g., S&I Initiative, pilot project, policy guidance) to existing standards by ONC3 - Follow existing standards process
1) Interoperability Standards Advisory Task Force – Page 19 http://healthit.gov/FACAS/sites/faca/files/HITSC_ISATF_Recommendation_Slides_2015-08-26.pdf2) http://ebooks.iospress.nl/publication/40319 , http://mor.nlm.nih.gov/pubs/pdf/2015-phenoday-fd.pdf
21
Next Steps

22
Appendix

23
Focus and Questions for Presenters
Focus• The exchange of genomic and phenomic data among:
– Patients/Participants– EHRs– Researchers – Testing labs (for both research and clinical care)
Questions for Presenters• What is the key problem or set of problems your organization is attempting
to solve? • What is the minimum interoperable data set of genome and phenome data
for these data exchanges?• Are there standards that can support this movement today? • What gaps are there and what is needed in the future?