Embed Size (px)
Citation preview

Dr Toby Talbot
Royal Cornwall Hospital

A busy year but some major trials now closed
Combi-I (Dab/Tram +/- PDL1 inhibitor/placebo)
Trilogy (Vem/Cobi +/- Atezolizumab/placebo)
ImSpire170 (BRAF wt – Pembro vs Atezo + Cobimet)
Keynote-693 Pembrolizumab 2nd line met cuSCC
Rational-MCC – surgery vs RT for MCC
Trials currently open and recruiting
NivoPASS – safety study for any patient on Nivolumab (including combination)

Trials in set up:
Interim – continuous vs intermittent Dab/Tram
Dante – 12 vs 24 months Pembrolizumab
PASIP – Pembrolizumab toxicity study
PASINI – Immunotherapy toxicity study
Keynote-630 – adjuvant Pembrolizumab in high risk cuSCC
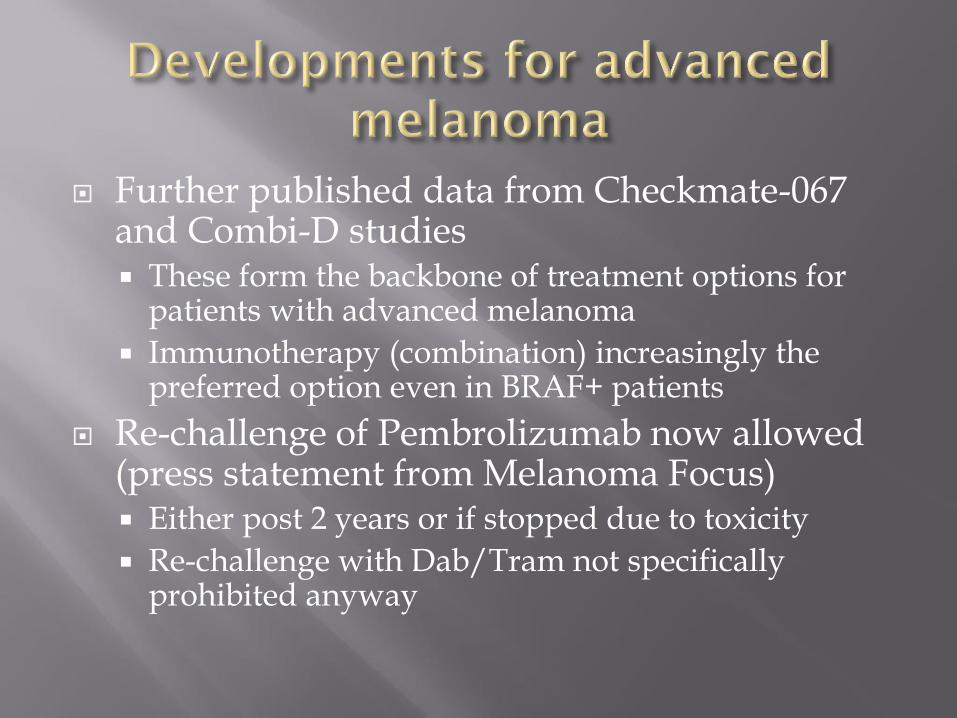
Further published data from Checkmate-067 and Combi-D studies These form the backbone of treatment options for
patients with advanced melanoma
Immunotherapy (combination) increasingly the preferred option even in BRAF+ patients
Re-challenge of Pembrolizumab now allowed (press statement from Melanoma Focus) Either post 2 years or if stopped due to toxicity
Re-challenge with Dab/Tram not specifically prohibited anyway
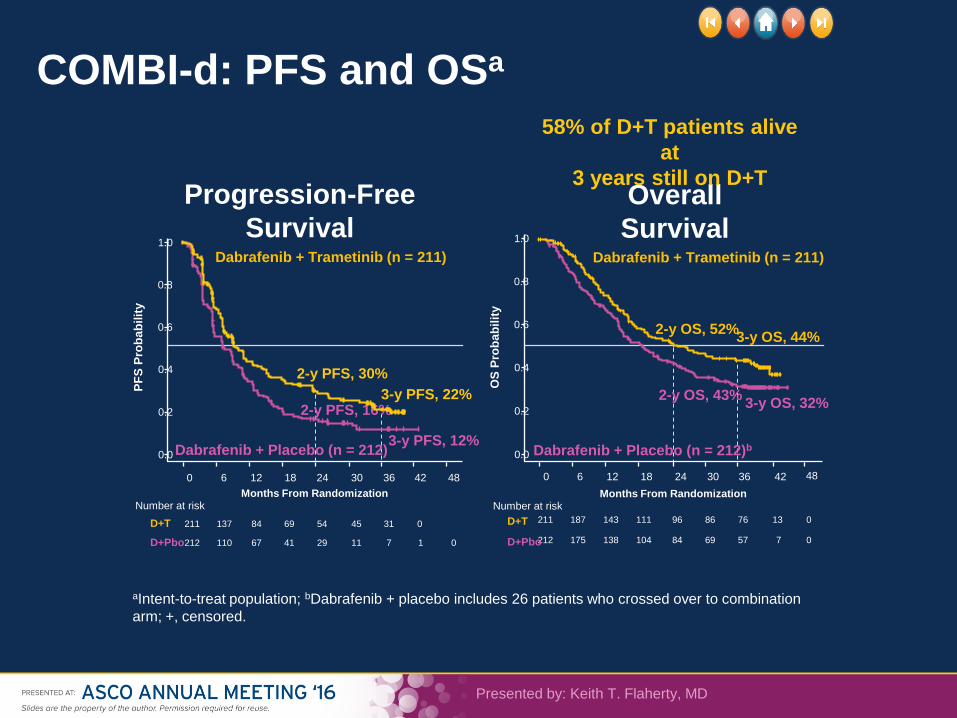
COMBI-d: PFS and OSa
Presented by: Keith T. Flaherty, MD
Overall
Survival
212 175 138 104 84 69 57 7 0
211 187 143 111 96 86 76 13 0
Dabrafenib + Trametinib (n = 211)
Dabrafenib + Placebo (n = 212)b
3-y OS, 44%
3-y OS, 32%
1.0
0.8
0.6
0.4
0.2
0.0
0 6 12 30 18
Months From Randomization O
S P
rob
ab
ilit
y
D+Pbo
D+T
Number at risk
2-y OS, 52%
2-y OS, 43%
24 36 42 48
Progression-Free
Survival
212 110 67 41 29 11 7 1 0
211 137 84 69 54 45 31 0
1.0
0.8
0.6
0.4
0.2
0.0
0
Months From Randomization
PF
S P
rob
ab
ilit
y
D+Pbo
D+T
Number at risk
6 12 30 18 24 36 42 48
3-y PFS, 22%
3-y PFS, 12%
2-y PFS, 30%
2-y PFS, 16%
Dabrafenib + Trametinib (n = 211)
Dabrafenib + Placebo (n = 212)
58% of D+T patients alive
at
3 years still on D+T
aIntent-to-treat population; bDabrafenib + placebo includes 26 patients who crossed over to combination
arm; +, censored.

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.
COMBI-v: Overall Survival (ITT population)
6
1.00
0.75
0.50
0.25
0.00
0 6 12 18 24 30 36 42
Months From Randomization
OS
Pro
bab
ility
Patients at
risk, n
D + T
Vem
3
5
2
3
5
2
3
1
1
2
8
9
2
4
5
2
0
3
2
0
1
1
5
4
1
7
1
1
1
9
1
5
0
1
0
3
1
2
7
8
1
3
3
2
2
3-y OS, 45%
3-y OS, 31%
2-y OS, 53%
2-y OS, 39% Vemurafenib (n = 352)a Median OS, 17.8 mo (95% CI,
15.6-20.7) • 128 censored pts, 89 (70%)
ongoing f/u, of which
10 (11%) are still on study tx HR, 0.68 (95% CI, 0.56-
0.83)
Dabrafenib + trametinib
(n = 352) Median OS, 26.1 mo (95% CI,
22.6-35.1) • 162 censored pts: 134 (83%)
ongoing f/u, of which 66 (49%)
are still on study tx
a Vemurafenib arm includes 34 patients (10%) who crossed over to the dabrafenib + trametinib arm.
D + T, dabrafenib + trametinib; f/u, follow-up; ITT, intent-to-treat; pts, patients; tx, treatment; Vem, vemurafenib.

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.
7

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.
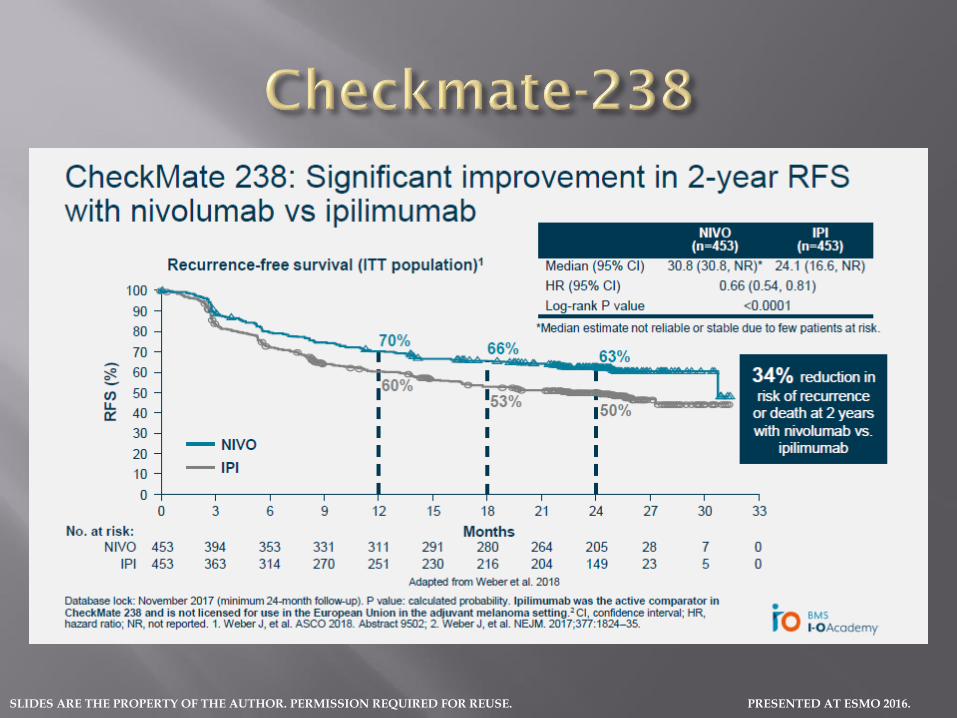
Positive trials for Nivolumab and Dabrafenib/Trametinib in Stage III melanoma
Dab/Tram Nice approved for BRAF+
Nivolumab declined by NICE initially but resubmitted – available through access scheme
Wording on licence for both treatments include “fully resected stage III disease”
No mention of minimal tumour burden
No mention of completion lymphadenectomy
Both studies required CLND…

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.
Strengthens the argument in favour of SNB
Less treatment overall (one year of treatment rather than ongoing)
Not clear if exposure to adjuvant Nivolumab influences funding for treatment upon relapse
Reduces the temptation for adjuvant radiotherapy

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.
PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.

SLIDES ARE THE PROPERTY OF THE AUTHOR.
PERMISSION REQUIRED FOR REUSE.
PRESENTED AT ESMO 2017.
14
BID, twice daily; DMFS, distant metastasis–free survival; ECOG, Eastern Cooperative Oncology Group; FFR, freedom from relapse; OS, overall survival; QD, once daily; RFS, relapse-free survival. a Or until disease recurrence, death, unacceptable toxicity, or withdrawal of consent; b Patients were followed for disease recurrence until the first recurrence and thereafter for survival; c The study will be considered complete and final OS analysis will occur when ≈ 70% of randomized patients have died or are lost to follow-up; d New primary melanoma considered as an event.
COMBI-AD: STUDY DESIGN
Key eligibility criteria
• Completely resected, high-risk stage IIIA
(lymph node metastasis > 1 mm), IIIB,
or IIIC cutaneous melanoma
• BRAF V600E/K mutation
• Surgically free of disease ≤ 12 weeks
before randomization
• ECOG performance status 0 or 1
• No prior radiotherapy or systemic
therapy
R
A
N
D
O
M
I
Z
A
T
I
O
N
Stratification
• BRAF mutation status (V600E, V600K)
• Disease stage (IIIA, IIIB, IIIC)
1:1
Dabrafenib 150 mg BID
+ trametinib 2 mg QD
(n = 438)
2 matched placebos
(n = 432)
Treatment: 12 monthsa
Follow-upb
until end of
studyc
•Primary endpoint: RFSd
•Secondary endpoints: OS, DMFS, FFR, safety N = 870

SLIDES ARE THE PROPERTY OF THE AUTHOR.
PERMISSION REQUIRED FOR REUSE.
PRESENTED AT ESMO 2017.
BASELINE DEMOGRAPHICS AND PATIENT CHARACTERISTICSa
Dabrafenib Plus Trametinib (n = 438)
Placebo (n = 432)
Total (N = 870)
Median age (range), years 50 (18-89) 51 (20-85) 50 (18-89)
Male, n (%) 195 (45) 193 (45) 388 (45)
BRAF mutation status, n (%) V600E V600Kb
397 (91)
41 (9)
395 (91)
37 (9)
792 (91)
78 (9)
ECOG performance status of 0, n (%)
402 (92) 390 (90) 792 (91)
Disease stage, n (%) IIIA IIIB IIIC III (unspecified)
83 (19) 169 (39) 181 (41)
5 (1)
71 (16) 187 (43) 166 (38)
8 (2)
154 (18) 356 (41) 347 (40)
13 (1)
a Reported for patients with available data; b One patient had both BRAF V600E and BRAF V600K mutations and was included in the V600K subset.

SLIDES ARE THE PROPERTY OF THE AUTHOR.
PERMISSION REQUIRED FOR REUSE.
PRESENTED AT ESMO 2017.
BASELINE DEMOGRAPHICS AND PATIENT CHARACTERISTICSa (CONT)
Dabrafenib Plus Trametinib (n = 438)
Placebo (n = 432)
Total (N = 870)
Number of positive lymph nodes, n (%) 1 2 or 3 ≥ 4
177 (40) 158 (36) 73 (17)
183 (42) 150 (35) 72 (17)
360 (41) 308 (35) 145 (17)
Type of lymph node involvement, n (%) Microscopic Macroscopic Not reported
152 (35) 158 (36) 128 (29)
157 (36) 161 (37) 114 (26)
309 (36) 319 (37) 242 (28)
Primary tumour ulceration, n (%) Yes No
179 (41) 253 (58)
177 (41) 249 (58)
356 (41) 502 (58)
In-transit disease, n (%) Yes No
51 (12) 387 (88)
36 (8)
395 (91)
87 (10) 782 (90)
a Reported for patients with available data.

SLIDES ARE THE PROPERTY OF THE AUTHOR.
PERMISSION REQUIRED FOR REUSE.
PRESENTED AT ESMO 2017.
17
RELAPSE-FREE SURVIVAL (PRIMARY ENDPOINT)
438 413 405 392 382 373 355 336 325 299 282 276 263 257 233 202 194 147 116 110 66 52 42 19 7 2 0
432 387 322 280 263 243 219 203 198 185 178 175 168 166 158 141 138 106 87 86 50 33 30 9 3 0 0
Months From Randomization
Dabrafenib plus trametinib
Placebo
No. at Risk
0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52
Pro
po
rtio
n A
live
and
Rel
apse
Fre
e
1 y, 88%
2 y, 67%
3 y, 58% 1 y, 56%
2 y, 44%
3 y, 39%
NR, not reached.
Group
Events, n (%)
Median (95% CI),
mo
HR (95% CI)
Dabrafenib plus trametinib
166 (38) NR
(44.5-NR) 0.47
(0.39-0.58);
P < .001 Placebo 248 (57) 16.6
(12.7-22.1)
P = .0000000000000153

SLIDES ARE THE PROPERTY OF THE AUTHOR.
PERMISSION REQUIRED FOR REUSE.
PRESENTED AT ESMO 2017.
18
OVERALL SURVIVAL (FIRST INTERIM ANALYSIS)
438 426 416 414 408 401 395 387 381 376 370 366 362 352 328 301 291 233 180 164 105 82 67 28 12 5 0
432 425 415 410 401 386 378 362 346 337 328 323 308 303 284 269 252 202 164 152 94 64 51 17 7 1 0
0
0
0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38 40 42 44 46 48 50 52 54
Pro
po
rtio
n A
live
1 y, 97%
2 y, 91%
3 y, 86%
1 y, 94%
2 y, 83%
3 y, 77%
a Prespecified significance boundary (P = .000019).
Months From Randomization
Group
Events, n (%)
Median (95% CI),
mo
HR (95% CI)
Dabrafenib plus trametinib
60 (14) NR
(NR-NR) 0.57
(0.42-0.79);
P = .0006a Placebo 93 (22) NR
(NR-NR)
Dabrafenib plus trametinib
Placebo
No. at Risk

PRESENTED AT ESMO 2016. SLIDES ARE THE PROPERTY OF THE AUTHOR. PERMISSION REQUIRED FOR REUSE.
No sign of slowing in survival gains in melanoma
Adjuvant options for high risk disease
?Extent of lymphatic surgery – debate
Surveillance protocol still not fixed – does adjuvant therapy influence this?
Still little change in non-melanoma skin cancers…