Embed Size (px)
Citation preview
Dr Teresa Chalmers-WatsonConsultant Gastroenterologist and Hepatologist
Christchurch Hospital
Christchurch
16:30 - 17:30 WS #129: What's Up With Bowel Cancer Screening in 2018?
17:35 - 18:30 WS #139: What's Up With Bowel Cancer Screening in 2018?
(Repeated)
Colorectal Cancer Screening 2018
Dr Teresa Chalmers-Watson
Consultant Gastroenterologist & Clinical Senior Lecturer
Clinical Advisor – NZ Familial GI Cancer Service
August 2018
Colorectal Cancer Screening
What is the Problem? Do we need Bowel Screening?
What do we do currently?
Risk Stratify
What are the Screening Options for ‘Average Risk’ ?
The Bowel Screening Pilot & Results
Implications for Canterbury & Nationally
Does New Zealand Need Bowel Screening?
Colorectal Cancer:
One of New Zealand’s most Common Cancers
3000 new cases diagnosed each year
Second highest cause of cancer death
1200 die from it
Maori 30% more likely to die
New Zealand has highest incidence rates in world
Bowel Screening detects cancer at earlier stage & saves lives
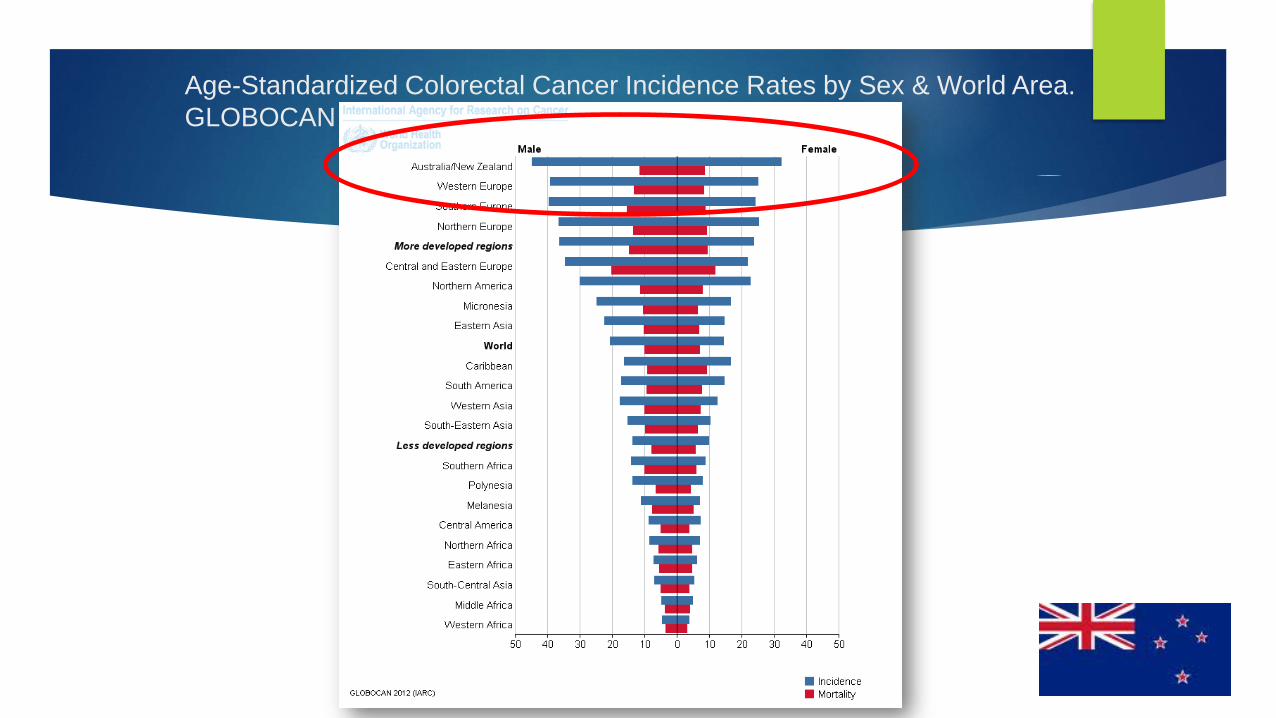
Age-Standardized Colorectal Cancer Incidence Rates by Sex & World Area.
GLOBOCAN 2008.
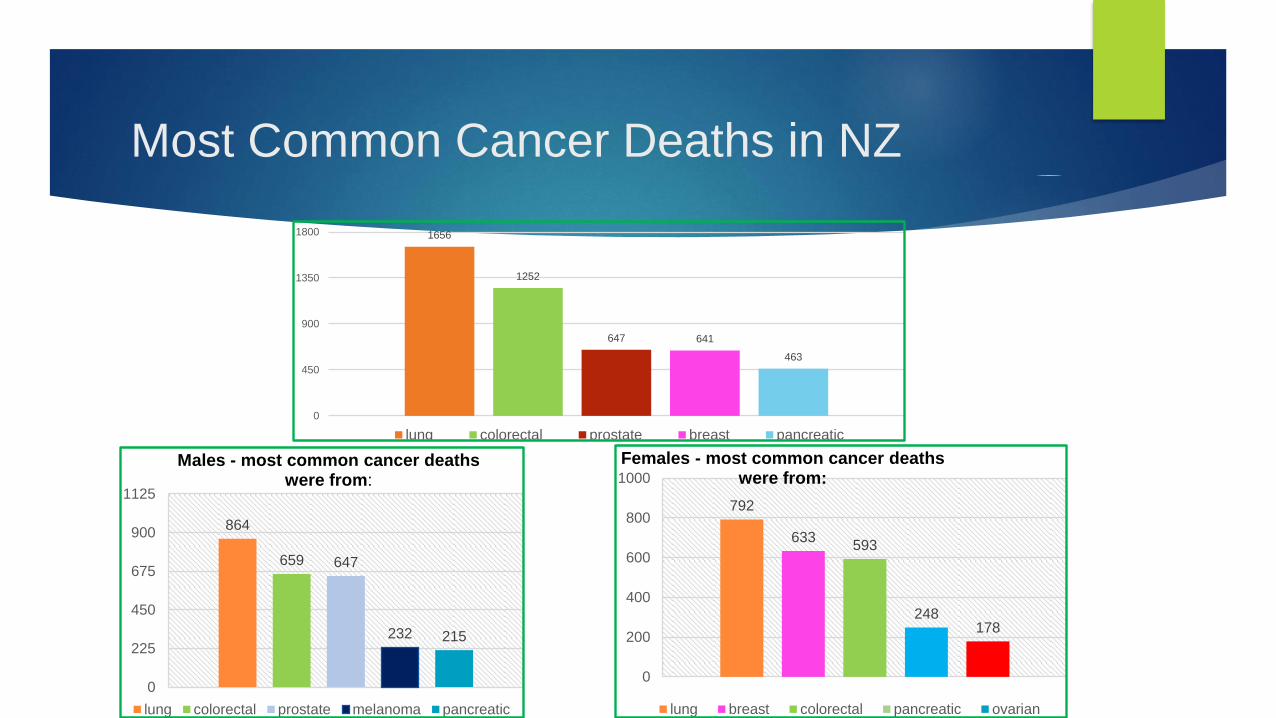
Most Common Cancer Deaths in NZ
1656
1252
647 641
463
0
450
900
1350
1800
lung colorectal prostate breast pancreatic
864
659 647
232 215
0
225
450
675
900
1125
Males - most common cancer deathswere from:
lung colorectal prostate melanoma pancreatic
792
633593
248178
0
200
400
600
800
1000
Females - most common cancer deaths were from:
lung breast colorectal pancreatic ovarian
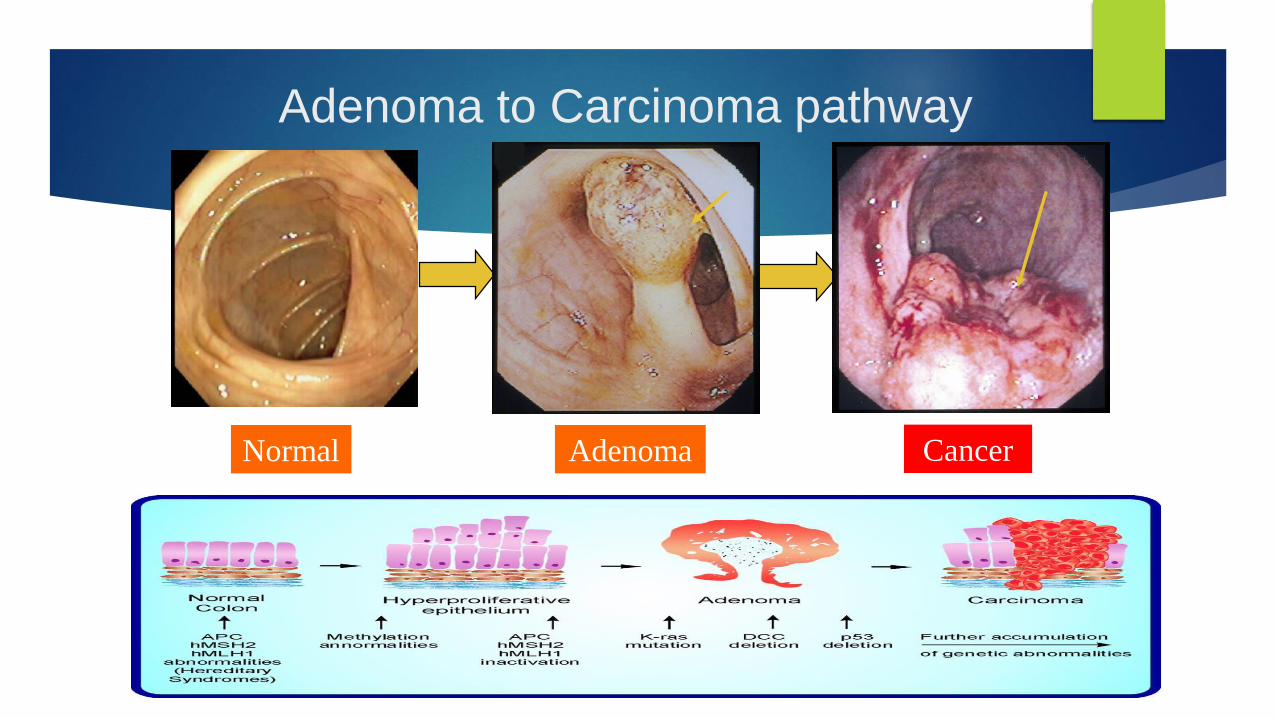
Adenoma to Carcinoma pathway
Normal CancerAdenoma
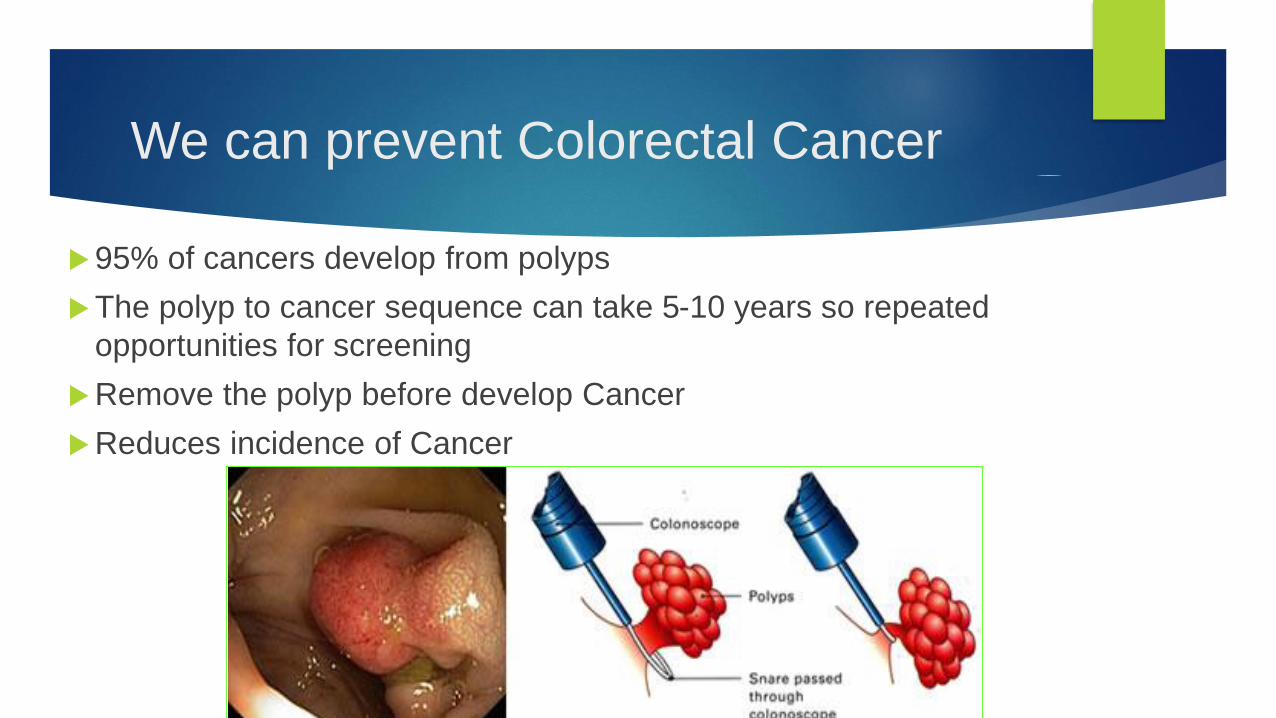
We can prevent Colorectal Cancer
95% of cancers develop from polyps
The polyp to cancer sequence can take 5-10 years so repeated
opportunities for screening
Remove the polyp before develop Cancer
Reduces incidence of Cancer
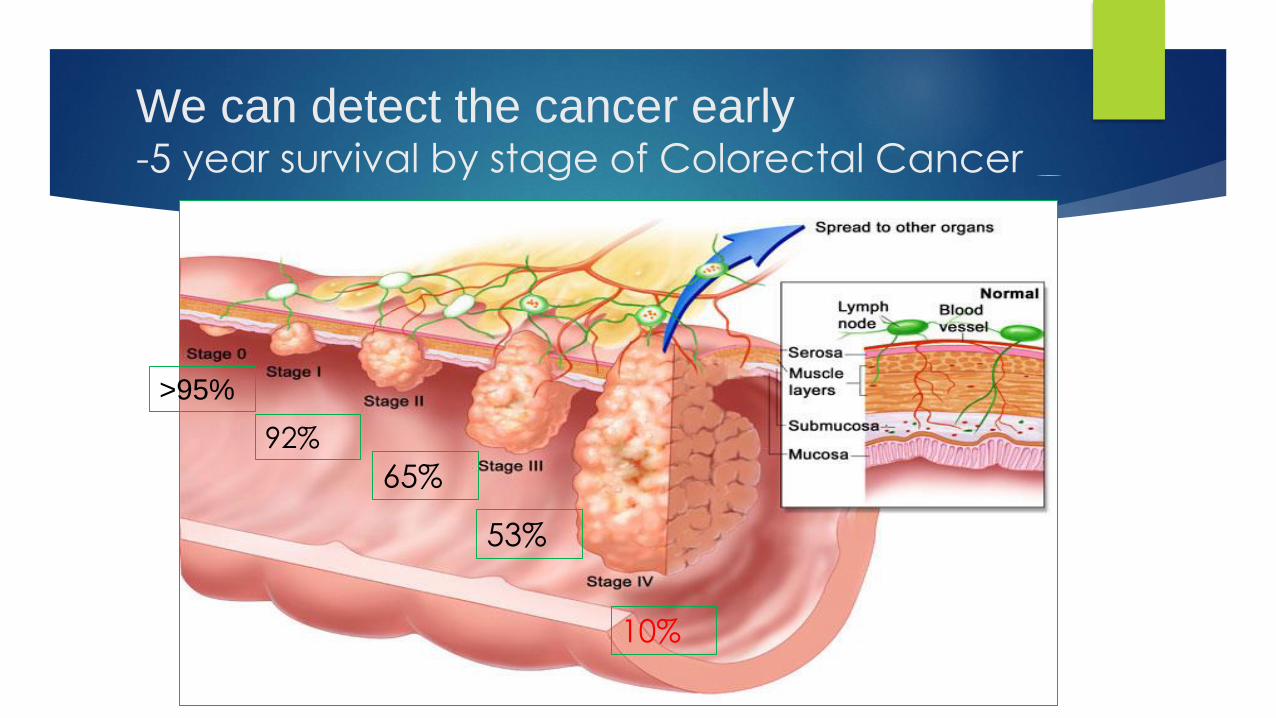
We can detect the cancer early -5 year survival by stage of Colorectal Cancer
92%
65%
53%
10%
>95%

What do we do now ?
- depends on ‘level of risk’
What is the Average Risk for individuals in NZ?
55 yrs:
Overall risk 0.6%
75 yrs
Overall risk 5.6%
Men: 1 in 18
Women 1 in 23
What increases your risk of bowel cancer?
Age:
Personal history:
Inflammatory Bowel Disease
Previous Cancer or polyps
Family history:
Other…
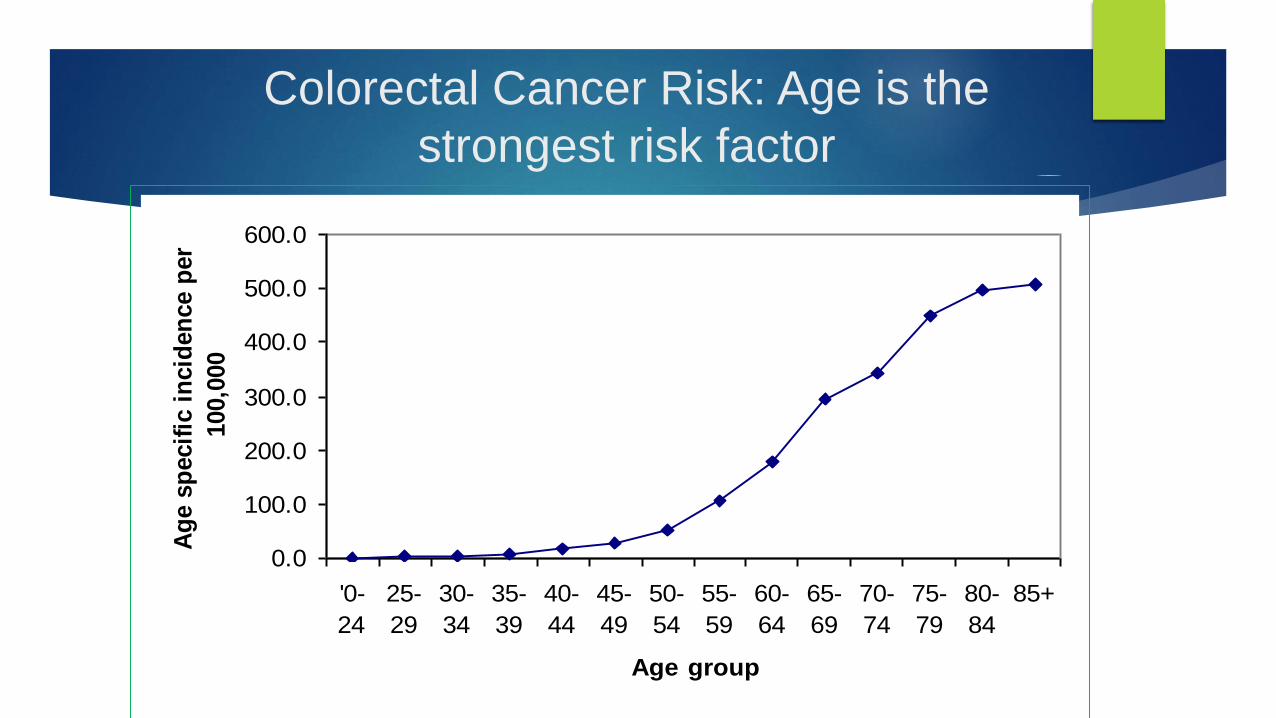
Colorectal Cancer Risk: Age is the
strongest risk factor
0.0
100.0
200.0
300.0
400.0
500.0
600.0
'0-
24
25-
29
30-
34
35-
39
40-
44
45-
49
50-
54
55-
59
60-
64
65-
69
70-
74
75-
79
80-
84
85+
Age group
Ag
e s
pecif
ic i
ncid
en
ce p
er
100,0
00
It’s in my genes…
70% of people with bowel cancer will have no family history -
Environmental factors dominant
Genetic factors are significant in 25% of cases
3 to 8% of bowel cancers are a consequence of recognized hereditary
conditions.
Lynch syndrome / HNPCC
Familial Adenomatous Polyposis - FAP
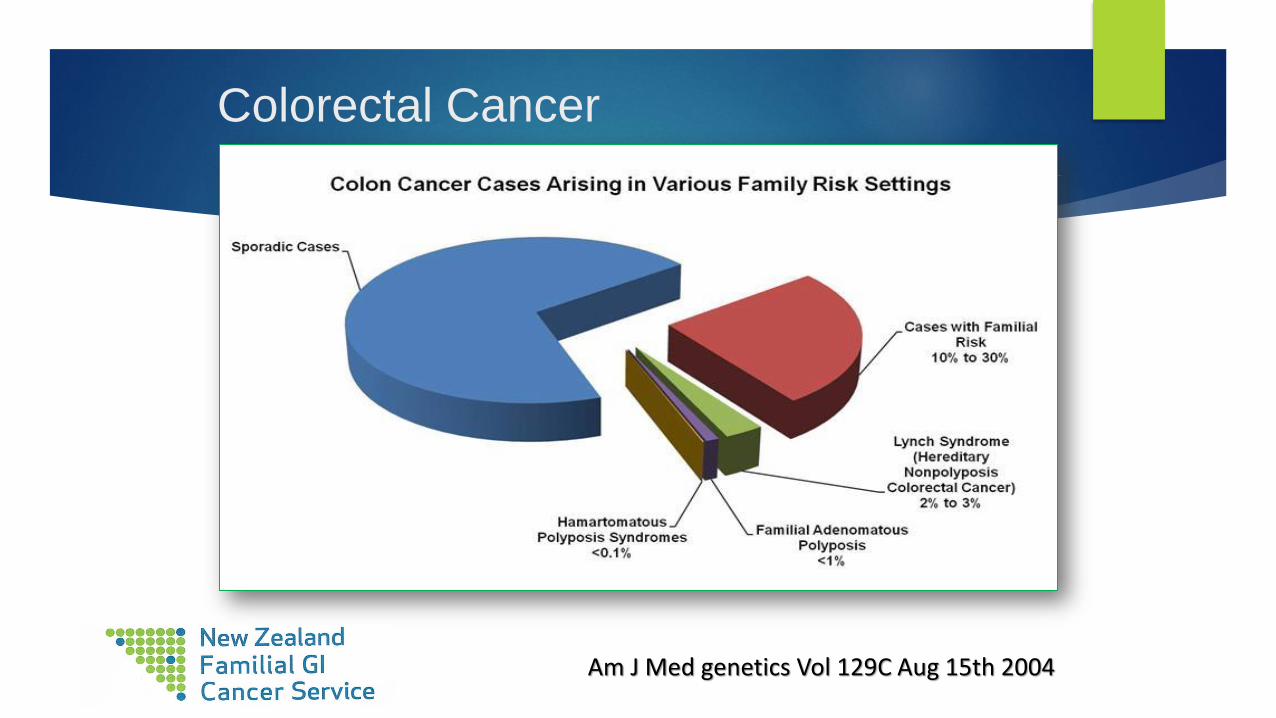
Colorectal Cancer
Am J Med genetics Vol 129C Aug 15th 2004
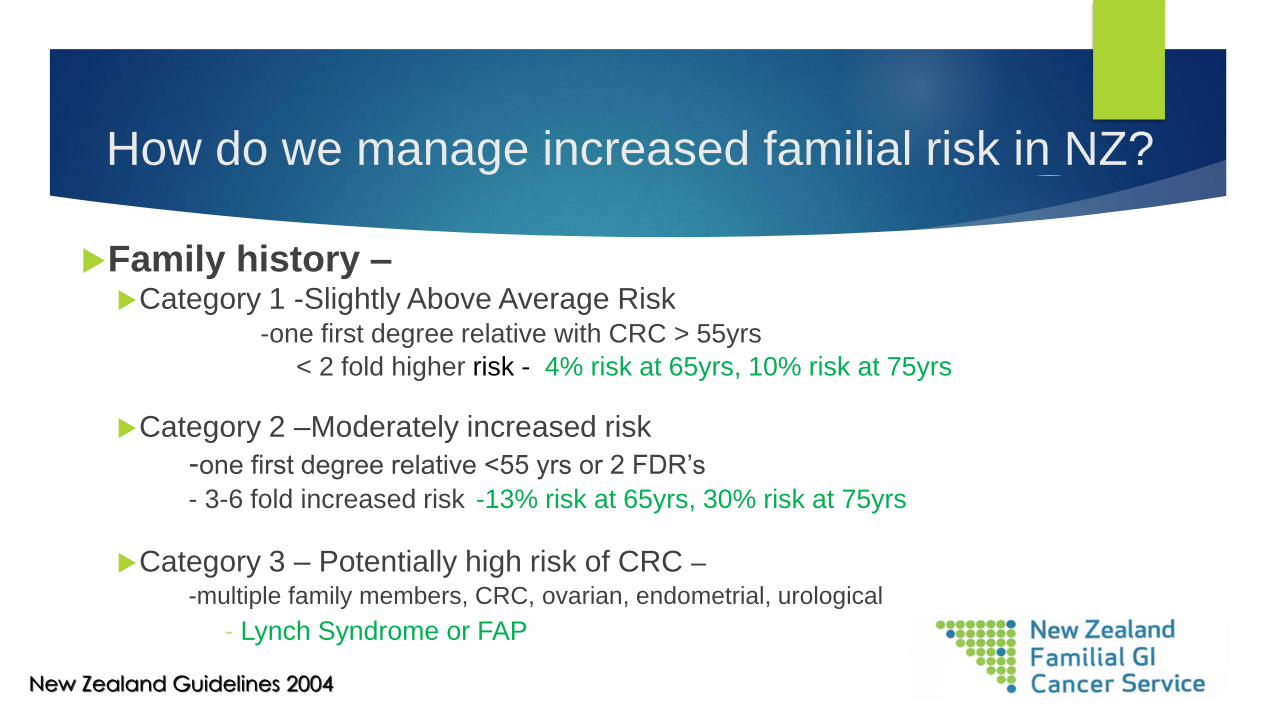
How do we manage increased familial risk in NZ?
Family history –Category 1 -Slightly Above Average Risk
-one first degree relative with CRC > 55yrs
< 2 fold higher risk - 4% risk at 65yrs, 10% risk at 75yrs
Category 2 –Moderately increased risk
-one first degree relative <55 yrs or 2 FDR’s
- 3-6 fold increased risk -13% risk at 65yrs, 30% risk at 75yrs
Category 3 – Potentially high risk of CRC –-multiple family members, CRC, ovarian, endometrial, urological
- Lynch Syndrome or FAP
New Zealand Guidelines 2004
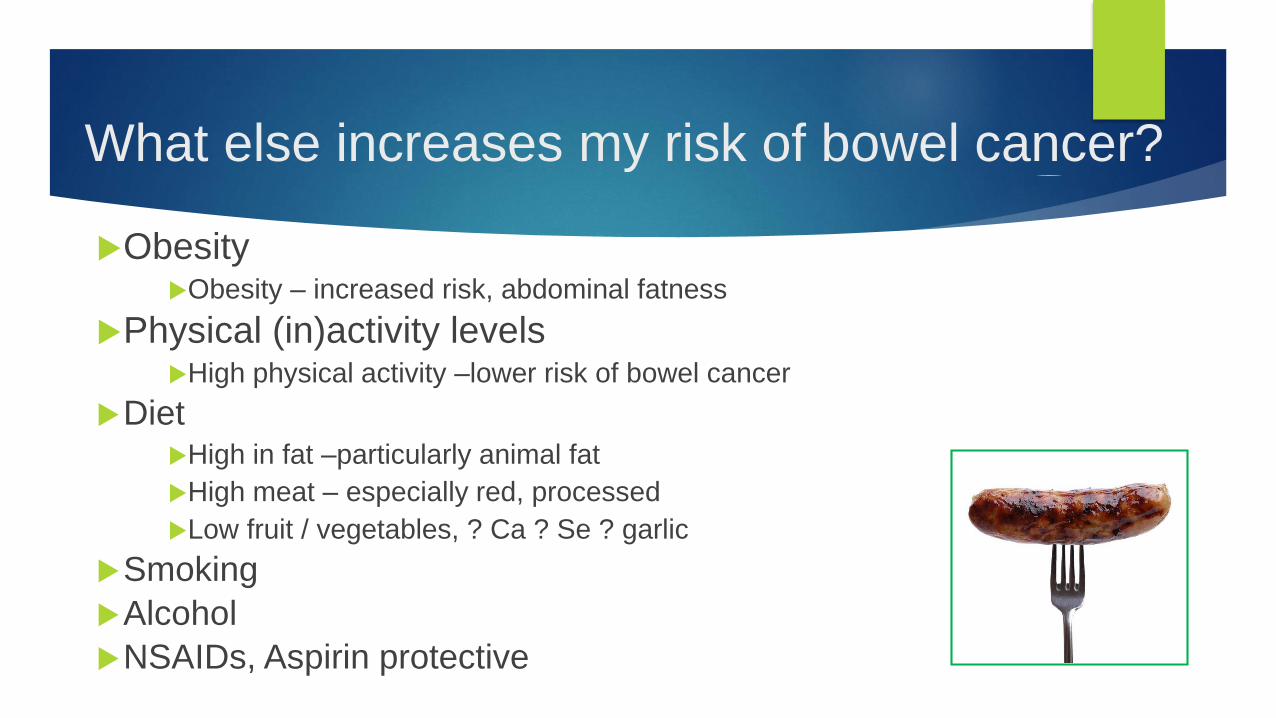
ObesityObesity – increased risk, abdominal fatness
Physical (in)activity levelsHigh physical activity –lower risk of bowel cancer
DietHigh in fat –particularly animal fat
High meat – especially red, processed
Low fruit / vegetables, ? Ca ? Se ? garlic
Smoking
Alcohol
NSAIDs, Aspirin protective
What else increases my risk of bowel cancer?

What do we do with ‘average’ & ‘slightly
increased risk’ individuals?
Should NZ do Bowel Screening?
The disease must be common & significant
Screening acceptable, safe and cost effective
Screening makes a difference to out come
- Screening reduces mortality from CRC by 16-90%
- Screening reduces incidence of CRC
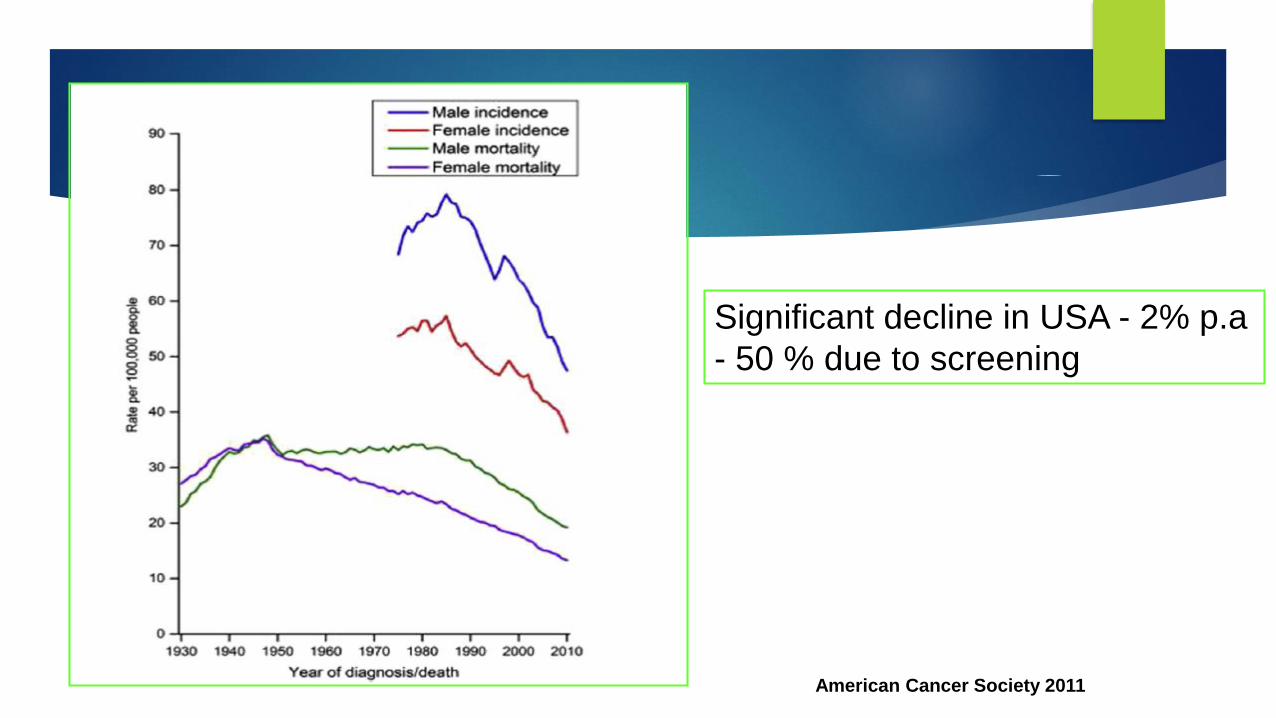
Significant decline in USA - 2% p.a
- 50 % due to screening
American Cancer Society 2011
Options for Bowel Screening
1. Detect Cancer
Stool tests
Most polyps never bleed
2. Detect Pre-cancerous lesions
CT colon
Colon capsule
Colonoscopy
Flexible Sigmoidoscopy
3. Others…
The Gastroenterologist’s view of
colonoscopy
• Safe
• Well-tolerated
• Sensitive
• Specific
• Safe
• Well Tolerated
• Sensitive
• Specific
The patient’s view of colonoscopy
• Invasive
• Expensive
• Dangerous
• Inconvenient
• Dangerous
• Inconvenient
• Invasive
• Expensive
Detecting Cancer – Stool samples
Faecal immunochemical test (iFOBT)
Detects the globin part of Hb
Requires only one sample
No time off work, discreet, in your own home
Are quantitative so sensitivity can be ‘set’
Less false positives
May detect advanced adenomas
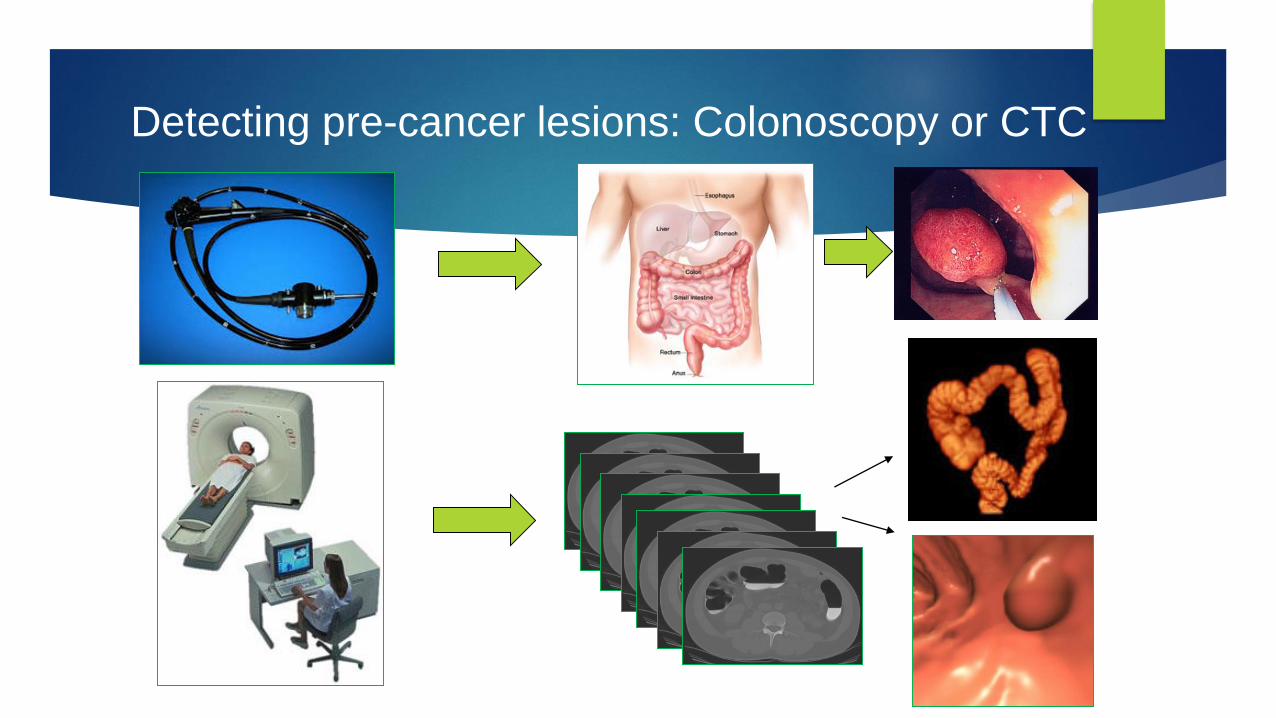
Detecting pre-cancer lesions: Colonoscopy or CTC
CT Colon
Potential advantages
Unsedated
Safe
no perforation with CO2
Good caecal visualization
Stricture fly-through
Extra-intestinal findings
Potential disadvantages
Radiation dose 2-3mSv
Bowel prep required
Only diagnostic
Less good at small polyps
Radiology also stretched
Colonoscopy
The gold standard
Requires bowel prep, day off
Safe but small risks (1/1000)
Diagnostic and therapeutic
If started by age 50 reduce CRC by 90%
Expensive on a population basis
Winawer et al N. Engl J Med 1993; 329:1977-1981
Flexible Sigmoidoscopy
Smaller amount of prep
Smaller amount of risk
Limited visualisation
Smaller benefit
‘No one likes them’
The future?
Bowel Screening Options in NZ
-Modelling
Single sigmoidoscopy is cheapest option and reduce CRC deaths by 16%
FIT followed by colonoscopy most cost effective and reduces CRC deaths by 27%
Internationally – favoured option
This is what the NZ pilot used
Sarafti et al NZMJ 2016
National Bowel Screening Pilot (BSP) in
Waitemata DHB
Four year Pilot – round 1 - 2012 to 2013, round 2 - 2014-2015,
Age range 50-74yrs men & women - approx 136,000 people
People invited every 2 years
Faecal immunochemical test for Haemoglobin (FIT)
Every 2 years
If positive invited for colonoscopy
Two screening rounds complete, 3rd ongoing
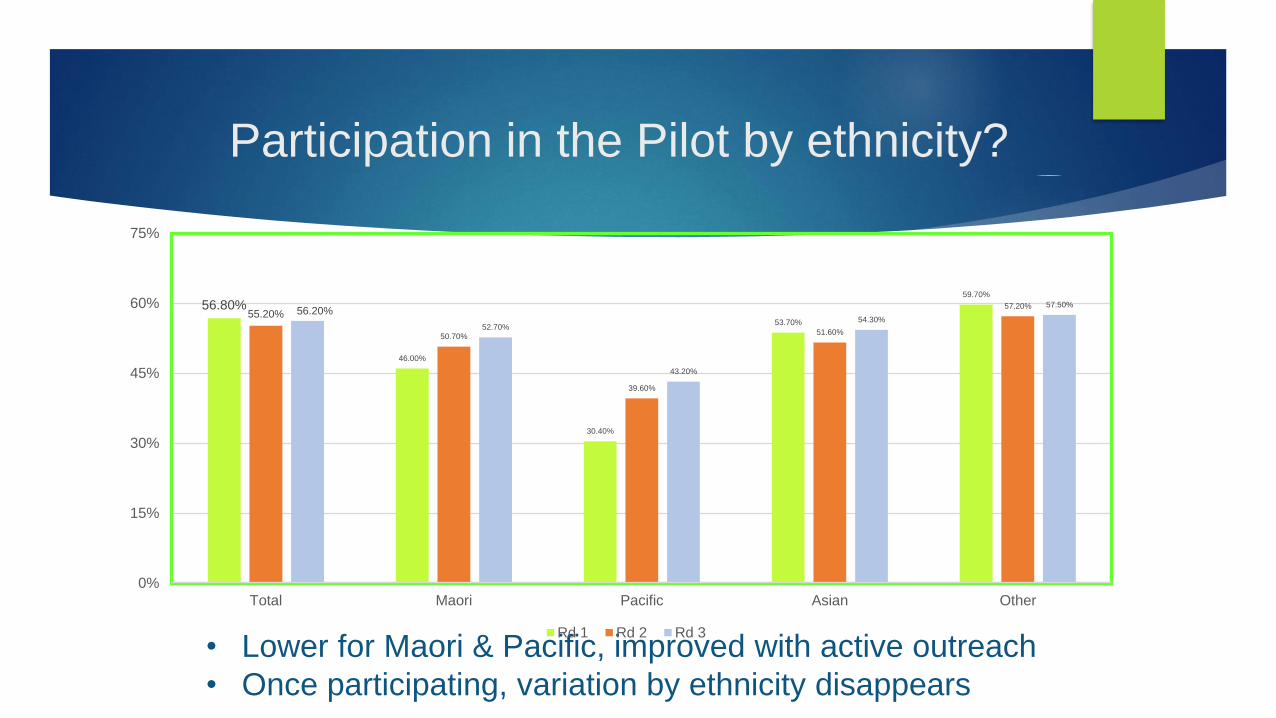
Participation in the Pilot by ethnicity?
• Lower for Maori & Pacific, improved with active outreach
• Once participating, variation by ethnicity disappears
56.80%
46.00%
30.40%
53.70%
59.70%
55.20%
50.70%
39.60%
51.60%
57.20%56.20%
52.70%
43.20%
54.30%
57.50%
0%
15%
30%
45%
60%
75%
Total Maori Pacific Asian Other
Rd 1 Rd 2 Rd 3
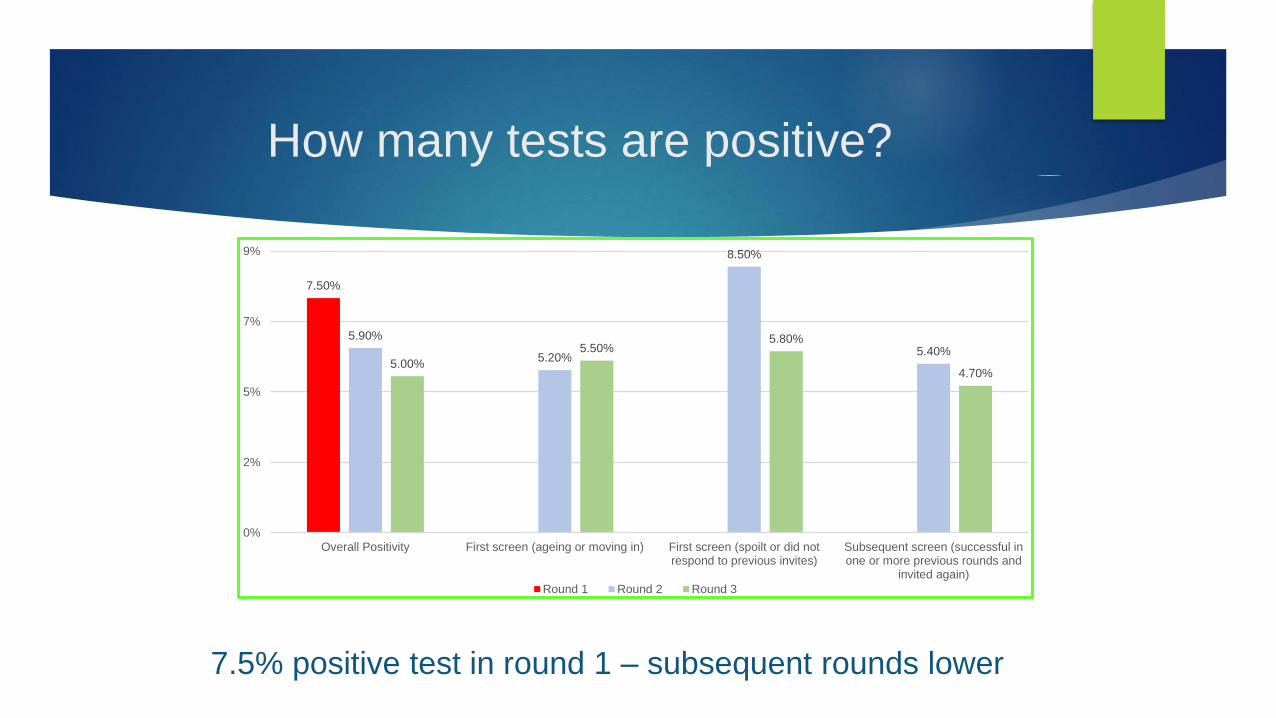
How many tests are positive?
7.50%
5.90%
5.20%
8.50%
5.40%5.00%
5.50%5.80%
4.70%
0%
2%
5%
7%
9%
Overall Positivity First screen (ageing or moving in) First screen (spoilt or did notrespond to previous invites)
Subsequent screen (successful inone or more previous rounds and
invited again)
Round 1 Round 2 Round 3
7.5% positive test in round 1 – subsequent rounds lower
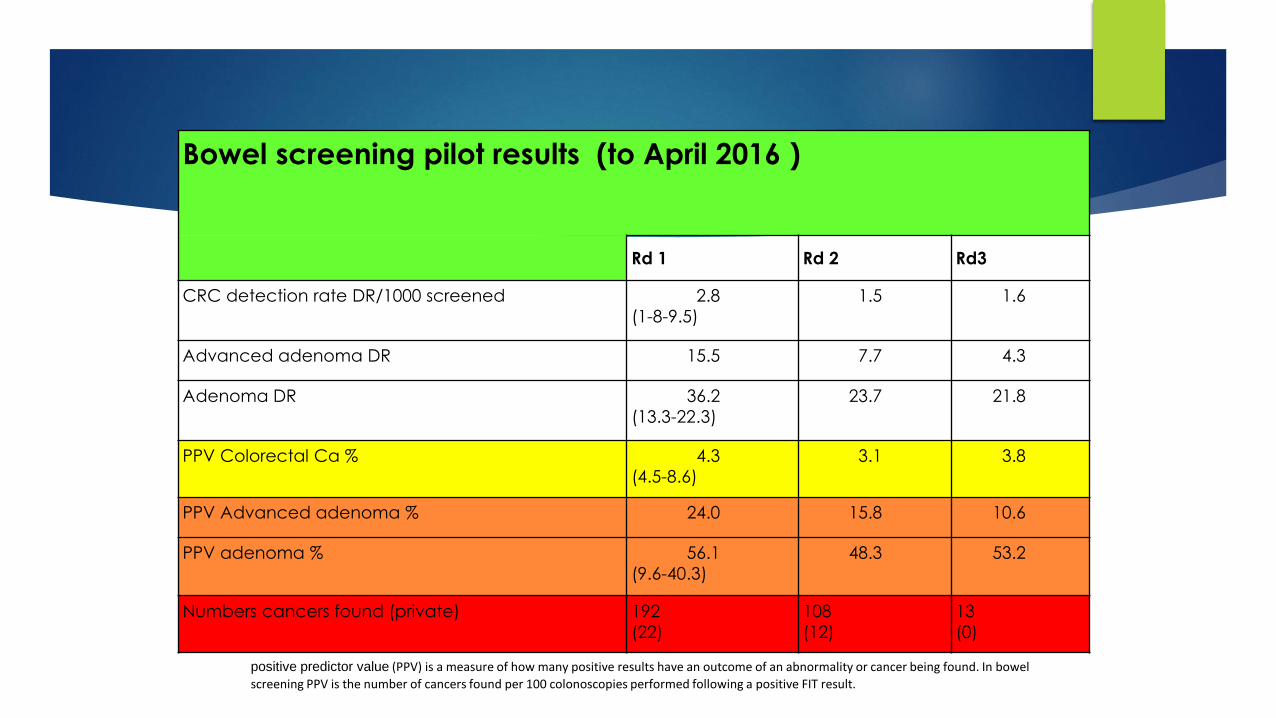
Bowel screening pilot results (to April 2016 )
Rd 1 Rd 2 Rd3
CRC detection rate DR/1000 screened 2.8
(1-8-9.5)
1.5 1.6
Advanced adenoma DR 15.5 7.7 4.3
Adenoma DR 36.2
(13.3-22.3)
23.7 21.8
PPV Colorectal Ca % 4.3
(4.5-8.6)
3.1 3.8
PPV Advanced adenoma % 24.0 15.8 10.6
PPV adenoma % 56.1
(9.6-40.3)
48.3 53.2
Numbers cancers found (private) 192
(22)
108
(12)
13
(0)
positive predictor value (PPV) is a measure of how many positive results have an outcome of an abnormality or cancer being found. In bowel
screening PPV is the number of cancers found per 100 colonoscopies performed following a positive FIT result.
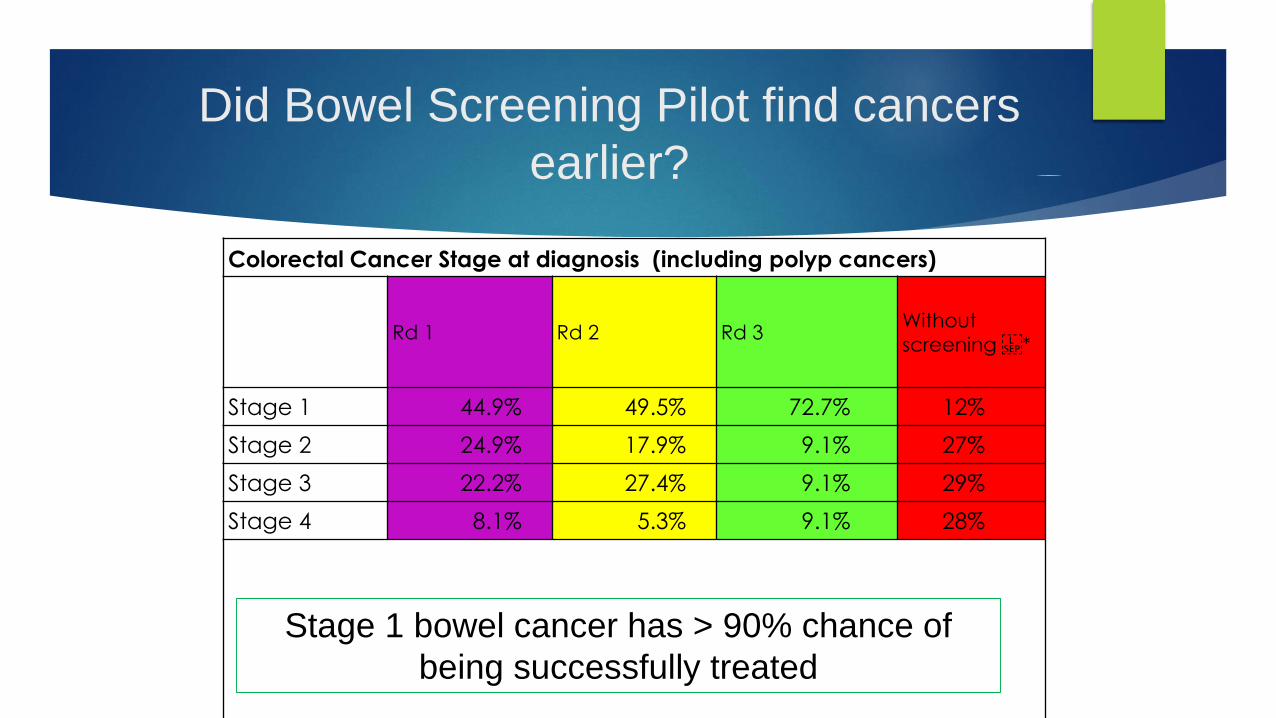
Did Bowel Screening Pilot find cancers
earlier?
Colorectal Cancer Stage at diagnosis (including polyp cancers)
Rd 1 Rd 2 Rd 3Without
screening *
Stage 1 44.9% 49.5% 72.7% 12%
Stage 2 24.9% 17.9% 9.1% 27%
Stage 3 22.2% 27.4% 9.1% 29%
Stage 4 8.1% 5.3% 9.1% 28%
Stage 1 bowel cancer has > 90% chance of
being successfully treated
Workforce & Resource implications… for CDHB
• There are currently not enough endoscopists to do the work –Gastroenterologists & surgeons
• Waitemata struggled
• Diagnostic work and waiting times affected
• Solutions? Increase trainees, Non specialist endoscopy - limited
• Need ½ a surgeon
• Need ½ a pathologist
• Endoscopy nurses
• GP’s
• Endoscopy physical capacity, administration, clerical
Budget 2016 Announcement
$39.3 million over 4 years for design, planning and set up of National Bowel
Screening Programme
Progressive roll out from mid 2017
Started with Lower Hutt and Wairarapa
Southern DHB – started June 2018
Canterbury DHB – starting when??
National Bowel Screening Programme
The Age Range has been raised to 60-74yrs
The threshold for a positive FIT test raised to 200ngHb/ ml buffer
Results from the New Zealand Bowel Screening Pilot
82 % of all cancers in BSP found in those aged 60-74yrs
80% of cancers were found following a FIT result > 200ng Hb/ml
47% positive FIT results were for Hb between 75 & 200ng
Therefore more likelihood of a cancer /advanced adenoma at colonoscopy, reduced colonoscopy requirements and so allows a National Screening Programme to start earlier...
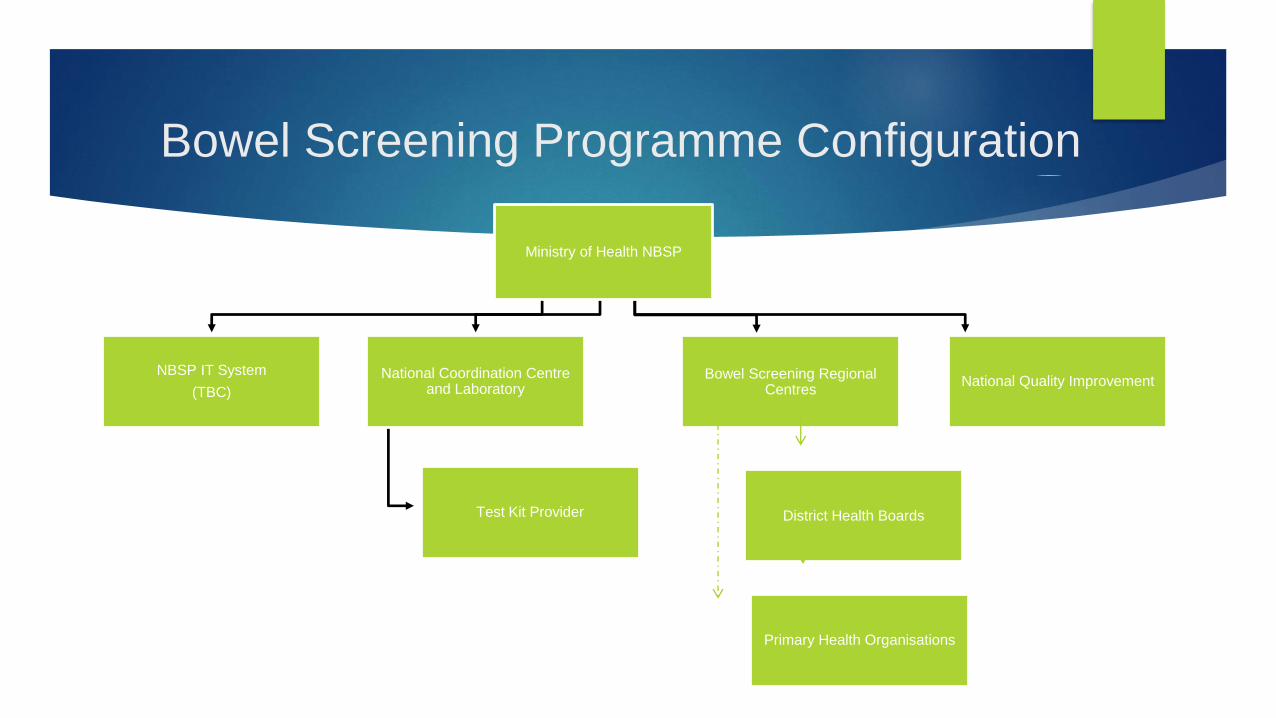
Bowel Screening Programme Configuration
Ministry of Health NBSP
NBSP IT System
(TBC)
National Coordination Centre and Laboratory
Test Kit Provider
Bowel Screening Regional Centres
District Health Boards
Primary Health Organisations
National Quality Improvement
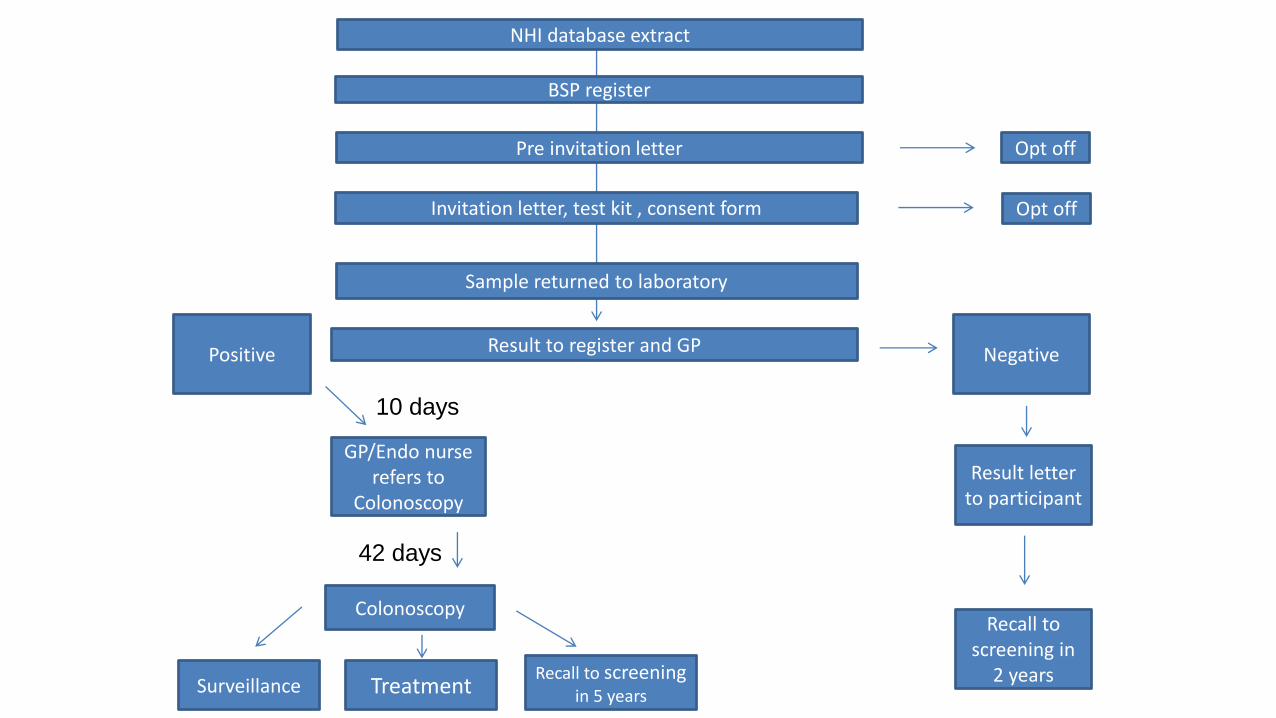
NHI database extract
BSP register
Pre invitation letter
Invitation letter, test kit , consent form
Sample returned to laboratory
Result to register and GP
10 days
GP/Endo nurse refers to
Colonoscopy
42 days
Result letter to participant
Recall to screening in
2 years
Colonoscopy
Recall to screeningin 5 yearsSurveillance
Opt off
Treatment
Opt off
NegativePositive
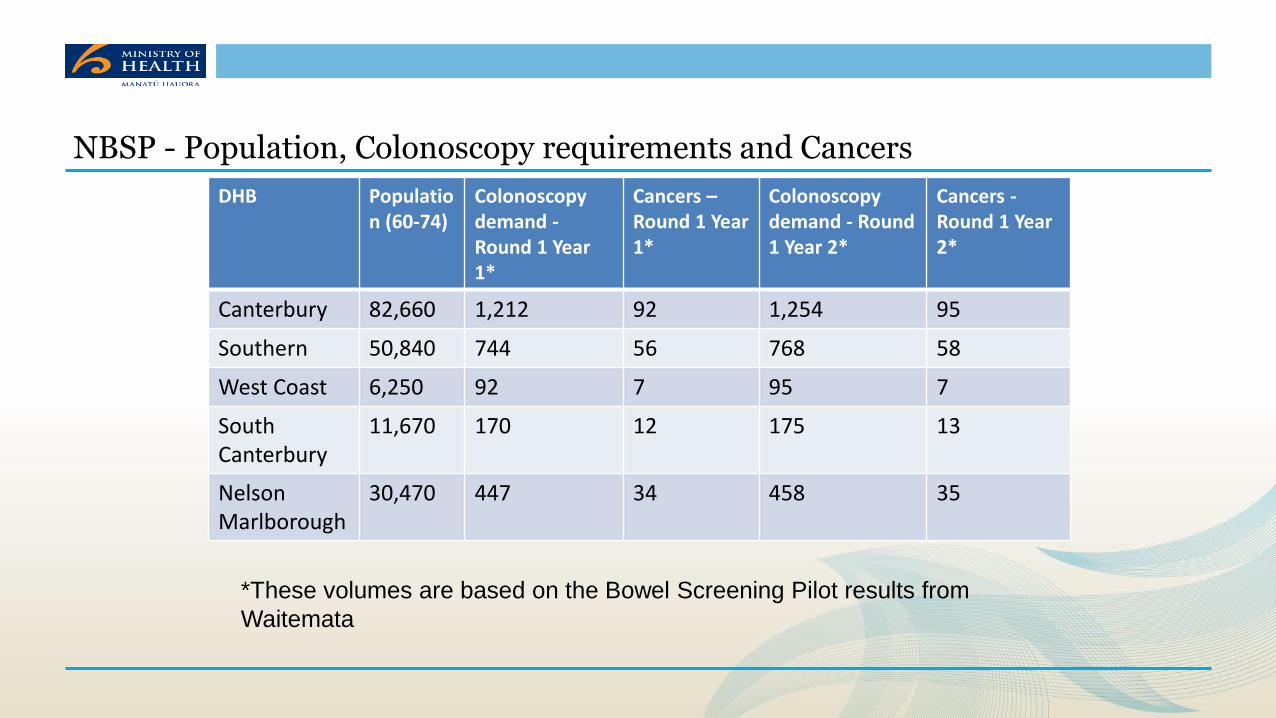
DHB Population (60-74)
Colonoscopydemand -Round 1 Year 1*
Cancers –Round 1 Year 1*
Colonoscopydemand - Round 1 Year 2*
Cancers -Round 1 Year 2*
Canterbury 82,660 1,212 92 1,254 95
Southern 50,840 744 56 768 58
West Coast 6,250 92 7 95 7
SouthCanterbury
11,670 170 12 175 13
NelsonMarlborough
30,470 447 34 458 35
NBSP - Population, Colonoscopy requirements and Cancers
*These volumes are based on the Bowel Screening Pilot results from
Waitemata
Conclusion - Colorectal Cancer Screening 2017
Colorectal Cancer:
One of New Zealand’s most Common Cancers & 2nd highest cause
of Ca death
New Zealand has highest incidence rates in world
Currently no screening for average risk or slightly increased risk
individuals
Bowel Screening detects cancer at earlier stage & saves lives.
Pilot successful – >300 cancers detected & at earlier stage
National Bowel Screening Programme rolling out …
v1

![Gillete Corner Invitation Letter[1] - WordPress.com · Microsoft Word - Gillete Corner Invitation Letter[1].doc Author: Lee Created Date: 20161010152046Z](https://img.pdfslide.us/doc/110x75/60346d67da560b7b185e38b1/gillete-corner-invitation-letter1-microsoft-word-gillete-corner-invitation.jpg)