Embed Size (px)
Citation preview

Dr Steve RitchieInfectious Diseases Physician
Auckland
8:55 - 9:20 A Modern Approach to Treating Cellulitis

An (modern) approach to treating cellulitis in primary and secondary care
Dr Stephen Ritchie

Acknowledgments
• Tim Cutfield & Eamon Duffy
• The ADHB cellulitis pathway development team
– improvement specialists, nurses, pharmacists, doctors
– medicine, surgery, ID, primary care, POAC, orthopaedics, ED, dermatology …..

Cellulitis
https://creativecommons.org/licenses/by-nc-nd/3.0/nz/legalcode,
www.dermnetnz.org www.medscape.com

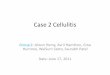
Cellulitis pathology
Boil/furuncleHigh number of bacteria
High number of neutrophils responding to bacteria
Localised tissue destruction
CellulitisLower number of bacteria
Moderate number of neutrophils responding to bacterial toxins
Generalised tissue inflammation
www.wikimedia.orgwww.cdc.gov

Diagnosis is primarily clinical
• In Harvard, approx. 30% of cases of cellulitis were “pseudo-cellulitis”– 25% of these
stasis dermatitis
– 18% of these Lyme disease skin lesions

Not cellulitis
• inflamed skin
• can be unilateral, non symmetrical
• less rapid onset
• no systemic symptoms (low fever)
• no response to antibiotics
https://creativecommons.org/licenses/by-nc-nd/3.0/nz/legalcode,
acute lipodermatosclerosis

Aetiology of cellulitis
• Streptococci* – 90%• S. pyogenes (Gp A strep), Gp C and Gp G streptococci
• Staphylococcus aureus – 10% • Others
*Estimated from blood culture isolates and efficacy rates from studies of benzylpenicillin

Don’t try too hard to culture anything
• maybe swab purulent material
• blood cultures if systemically unwell

Antibiotic treatment of cellulitis

• Pre-antibiotic era 145 cases of cellulitis
– 105 limb cellulitis
• 55 (52%) resolved, 43 (41%) resolved after abscess drained, 7 (7%) sepsis
• 3 (3%) died

• Pain relief achieved rapidly via bandaging
• all going well, bandage left for approximately 14 days
• “frequently, …., a man may return to work in four to seven days still wearing his bandage”

Although 90%* of cellulitis cases are caused by penicillin susceptible streptococci, anti-staphylococcal antibiotics
are required
• For adults:– FLUCLOXACILLIN 500mg QID P.O.
– CEFAZOLIN is of NO ADVANTAGE apart from a (slightly) longer half-life

Combinations of antibiotics are NOT useful

Cellulitis - so simple…
• an "easy" condition to diagnose
• only caused by two bacteria
• local and international guidelines indicate that (for almost all) there is only one treatment
– FLUCLOXACILLIN

Cellulitis, so simple…so why is management so variable at ADHB?
• high use of unnecessary IV antibiotics
• >100 different SMOs looking after cases
• frequent ID team referral
• “change to oral antibiotics and discharge”

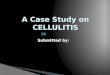
Most patients at ADHB received IV antibiotics
94.1%90.8%
98.9% 100.0%
0%
25%
50%
75%
100%
Class 1 Class 2 Class 3 Class 4
Pro
po
rtio
n o
f ce
llulit
is c
ases
(n
=14
62
)
Severity Class
these people have “mild” disease

Also a primary care problem
• 45% of patients with cellulitis at ADHB were referred by their GP
• many who weren’t systemically unwell were then admitted for several days solely for IV antibiotics
• Ditto for the 55% who self-present

SCRIPT – ADHB antibiotic guideline app
• google play/app store: “ADHB SCRIPT”


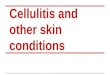
Cellulitis severity
55.4%
18.5%
23.9%
2.2%
0%
15%
30%
45%
60%
1 2 3 4
Pro
po
rtio
n o
f ce
llulit
is c
ase
s (n
=14
62
)
Dundee Severity Class
unwell

Most patients at ADHB received IV antibiotics
94.1%90.8%
98.9% 100.0%
0%
25%
50%
75%
100%
Class 1 Class 2 Class 3 Class 4
Pro
po
rtio
n o
f ce
llulit
is c
ases
(n
=14
62
)
Severity Class
these people have “mild” disease

The problems
1. over reliance on admission for IV antibiotics
2. antibiotic guideline subjective
3. unnecessary referrals
resulting in:
1. high bed-day utilization/length of stay

ADHB cellulitis pathway to improve patient care
• simple, tangible parameters to define management
• consistent between primary care and secondary care
• single point of contact in secondary care

1. is the patient systemically unwell?
2. are there risk factors for failure of oral antibiotic
treatment
Decisions about admission and treatment
can be based on two questions:

The ADHB pathway
• Class 1 patients– well, no risk for failure of oral antibiotics
– home, take away pack of oral FLUCLOXACILLIN for 5 days

The ADHB pathway
• Class 2 patients– well, risk for failure of oral antibiotics
– home, IV treatment via POAC

The ADHB pathway
• Class 3 patients– unwell
– admit, IV FLUCLOX, discharge once systemically stable

The ADHB pathway
• Class 4 patients– very unwell
– surgical review, ICU review, antibiotic cocktail

Impact of the pathway

Length of stay reduced from 2 days to 0.6 dayswith no change in mortality and no change in
readmission
2%
8%
1%
9%
0%
3%
6%
9%
12%
30 day Mortality 30 day Readmission
Pre-pathway Post-pathway

IV vs. oral treatment
• No increase in POAC funded IV cefazolin*
• 903 Class 1 patients– 285 (31%) received oral treatment
– oral LOS 0.1 days vs. 2 days for IV treatment
– 30 day readmission 19/285 (7%) vs. 42/618 (7%)
– 30 day mortality 1/285 (0.4%) vs. 4/618 (0.06%)
*Deanna Williams, Helen Liley, Sarah Hyder

Other pathway improvement highlights
• takeaway pack of oral antibiotics
• funded GP follow-up for people treated with oral antibiotics
• single point of contact (direct line to nurse specialist) for GPs

Summary
• cellulitis is simple
• use oral FLUCLOXACILLIN for systemically well people who do not have other significant co-morbidities
• patients who are systemically unwell should be admitted
• you have won once the systemic symptoms have resolved OR the redness has started to regress
• “relapses” are due to gravity

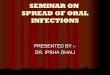
Comorbidities of 1462 people with cellulitis at ADHB
24%
21%18%
13%12%
4% 4% 3%
0%
8%
15%
23%
30%
Prio
r Ce
llulitis
Dia
bete
s
Mo
rbid
Ob
esity
Ch
ron
ic V
en
ou
s…
He
art F
ailu
re
Pre
vio
us D
VT
PA
D
Imm
un
e s
up
pre
ssio
n
Co-morbidities associated with failure of oral antibiotic treatment and with increased length of stay
Co-morbidities associated with length of stay