Embed Size (px)
Citation preview
Abnormal LFTs - a practical approach
Update on Liver Cancer GP Study Afternoon
Thursday 21st July 2016
Dr Shahid A Khan
Consultant Hepatologist
St Mary’s Hospital
Imperial College Healthcare NHS Trust

Do not interpret LFTs on their own
• History
• Clinical examination
• Laboratory findings
• Imaging
2
Liver function tests
• Interpretation must be performed within the context
of the patient’s risk factors, symptoms, concomitant
conditions, medications, and physical findings
• Rarely provide specific Dx, but rather suggest a
general category of liver disease
• Differing laboratories differing normal values
3
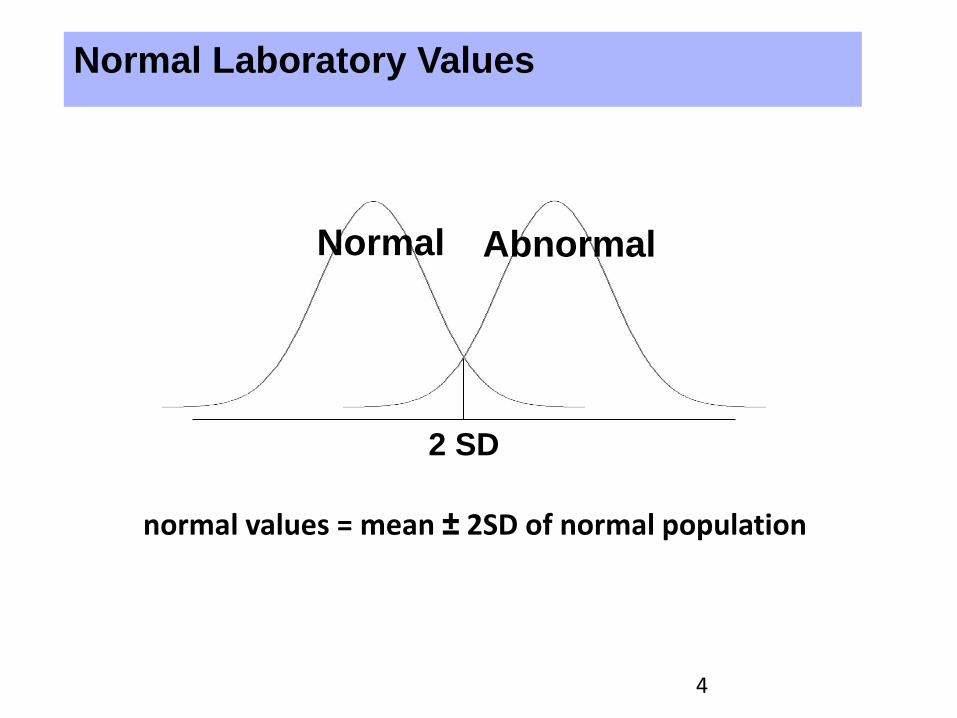
Normal Laboratory Values
2 SD
Abnormal Normal
normal values = mean ± 2SD of normal population
4
LFT abnormalities classification
• Hepatocellular injury (AST, ALT)
• Cholestatic injury (ALP, γGT, bilirubin)
• Infiltration (ALP, γGT, occasionally bilirubin)
• Synthetic function (albumin, INR)
Albumin, INR, bilirubin – also used as prognostic factors (Child-Pugh, MELD, UKELD)
5
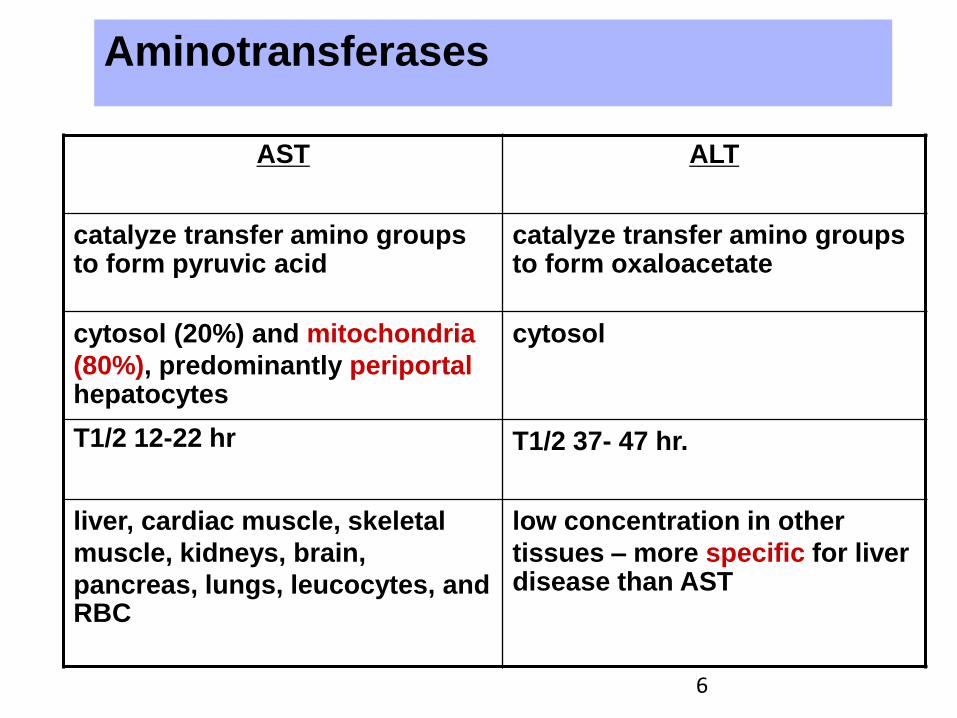
Aminotransferases
AST ALT
catalyze transfer amino groups to form pyruvic acid
catalyze transfer amino groups to form oxaloacetate
cytosol (20%) and mitochondria
(80%), predominantly periportal hepatocytes
cytosol
T1/2 12-22 hr T1/2 37- 47 hr.
liver, cardiac muscle, skeletal
muscle, kidneys, brain,
pancreas, lungs, leucocytes, and RBC
low concentration in other
tissues – more specific for liver disease than AST
6
Unexpected ALT elevation
• Muscle disease/injury (CPK, aldolase)
•Thyroid dysfunction (TSH)
•Coeliac disease (anti-endomysial antibody)
7
Alkaline phosphatase
• Of cytosolic origin in the liver
• Present in placenta, ileal mucosa, kidney, bone
• Half life = 3 days
• Elevated in 3d trimester of pregnancy
• Blood types O and B: can have elevated ALP
after fatty meal due to influx of intestinal ALP
• Liver origin: elevated GGT
Bone origin: normal GGT
8
Physiologic
• >60 yr.
• child and adolescent
• pregnancy
• blood group O
• post meal (fatty meal)
Pathologic
• intrahepatic
• extrahepatic
Alkaline phosphatase
9
γ-glutamyltransferase (GGT)
• catalyzed transfer of γ-glutamyl groups of peptides to
other amino acid
• abundant in liver, kidney, pancreas, intestine, and
prostate, spleen, heart, brain but not in bone
• T1/2
– 7-10 days
– 28 days in alcohol-associated liver injury
10
γ-glutamyltransferase (GGT)
• Increase
– alcohol (even without liver disease)
– drug
• anticonvulsant (CBZ, phenytoin, and barbiturate),
warfarin
– almost all type of liver diseases, inc fatty liver
– COPD, renal failure, DM, hyperthyroidism, RA,
AMI, pancreatic disease
11

BALLETS (Birmingham and Lambeth Liver
Evaluation Testing Strategies) study
• Prospective study in 11 GP practices Nov 2005 – Nov 2008
• Patients with no known liver disease and at least 1 abnormal liver function test
• Further assessment with:
– History
– Complete ‘liver panel’
– Ultrasound
• Follow up for 2 years
15
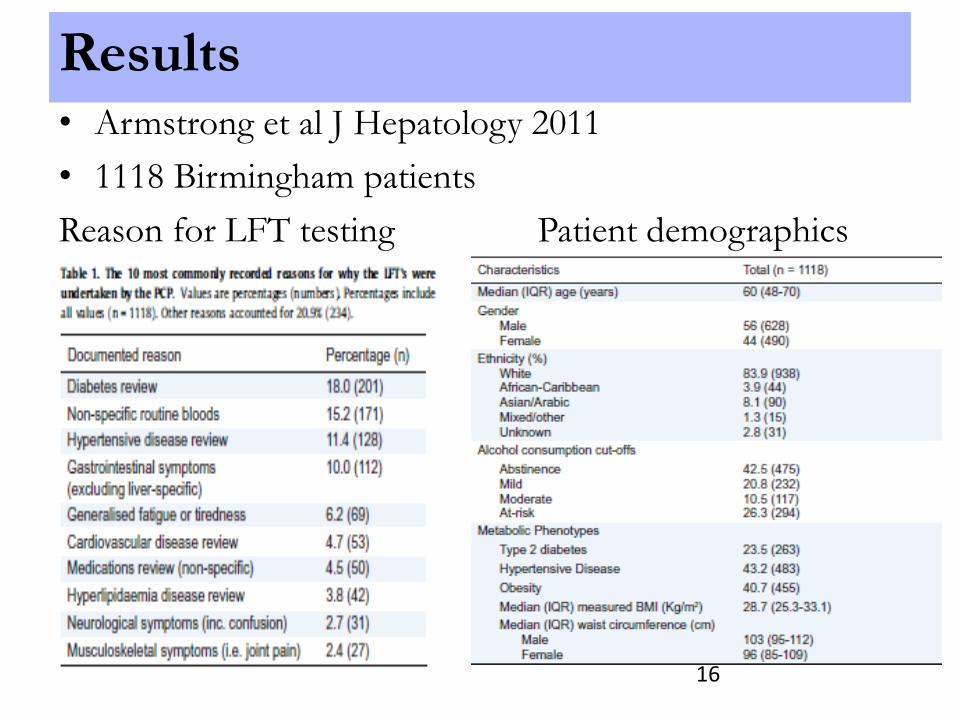
Results • Armstrong et al J Hepatology 2011
• 1118 Birmingham patients
Reason for LFT testing Patient demographics
16
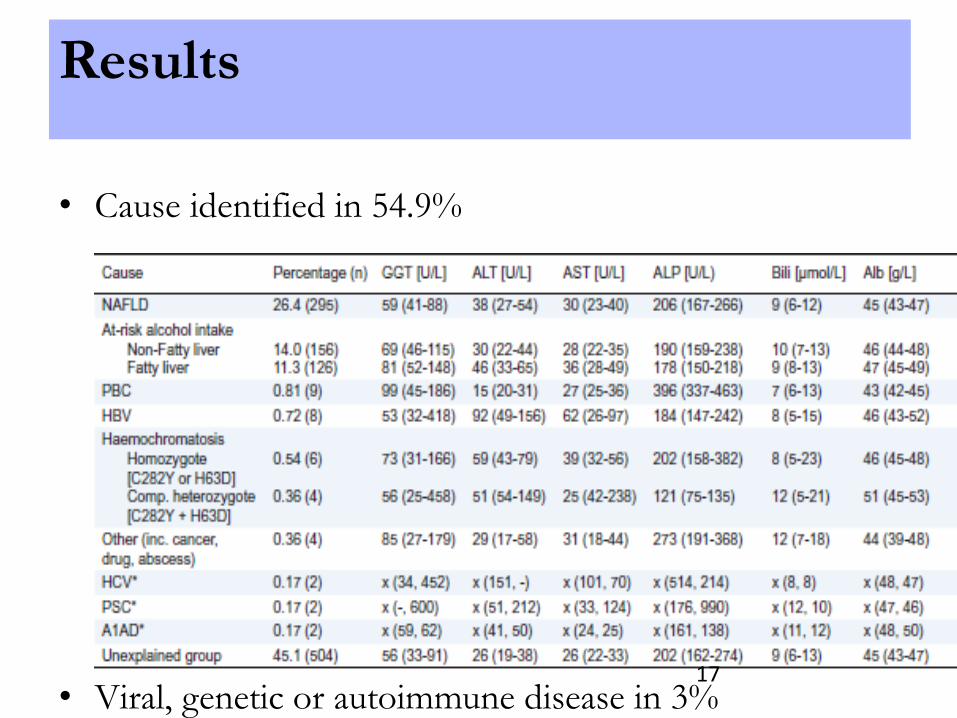
Results
• Cause identified in 54.9%
• Viral, genetic or autoimmune disease in 3%
17
Assessing Patients with Abnormal
LFTs • Do they have liver disease?
• What type of liver disease?
• How severe is it?
– ‘Stage of disease’
– How much liver fibrosis
18
• Chronic Alcohol Abuse
• Hepatitis B
• Hepatitis C
• Other Liver viruses
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis
• Non-alcoholic Fatty Liver Disease (NASH)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
• (Cystic fibrosis + other congenital diseases e.g. biliary atresia, LAL-Def, glycogen storage disease)
Screening Investigations for Liver Disease

• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B
• Hepatitis C
• Other Liver viruses
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis
• Non-alcoholic Fatty Liver Disease (NASH)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C
• Other Liver viruses
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis
• Non-alcoholic Fatty Liver Disease (NASH)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis
• Non-alcoholic Fatty Liver Disease (NASH)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis
• Non-alcoholic Fatty Liver Disease (NASH)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis (Liver Antibodies Anti-LKM, ANCA, ANA, ASMA, AMA)
• Non-alcoholic Fatty Liver Disease (NASH)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis (Liver Antibodies Anti-LKM, ANCA, ANA, ASMA, AMA)
• Non-alcoholic Fatty Liver Disease (NASH) (Lipids, Glucose/HbA1c)
• Haemochromatosis
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease

• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis (Liver Antibodies Anti-LKM, ANCA, ANA, ASMA, AMA)
• Non-alcoholic Fatty Liver Disease (NASH) (Lipids, Glucose/HbA1c)
• Haemochromatosis (Ferritin/Iron Studies, Transferrin satn)
• Wilson's disease (<40yo)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis (Liver Antibodies Anti-LKM, ANCA, ANA, ASMA, AMA)
• Non-alcoholic Fatty Liver Disease (NASH) (Lipids, Glucose/HbA1c)
• Haemochromatosis (Ferritin/Iron Studies, Transferrin satn)
• Wilson's disease (<40yo) (Serum Cu/caeruloplasmin, 24hr urine Cu)
• Alpha1-Antitrypsin Deficiency
• Liver Tumours
Screening Investigations for Liver Disease

• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis (Liver Antibodies Anti-LKM, ANCA, ANA, ASMA, AMA)
• Non-alcoholic Fatty Liver Disease (NASH) (Lipids, Glucose/HbA1c)
• Haemochromatosis (Ferritin/Iron Studies, Transferrin satn)
• Wilson's disease (<40yo) (Serum Cu/caeruloplasmin, 24hr urine Cu)
• Alpha1-Antitrypsin Deficiency (Alpha1-AT levels…then phenotyping)
• Liver Tumours
Screening Investigations for Liver Disease
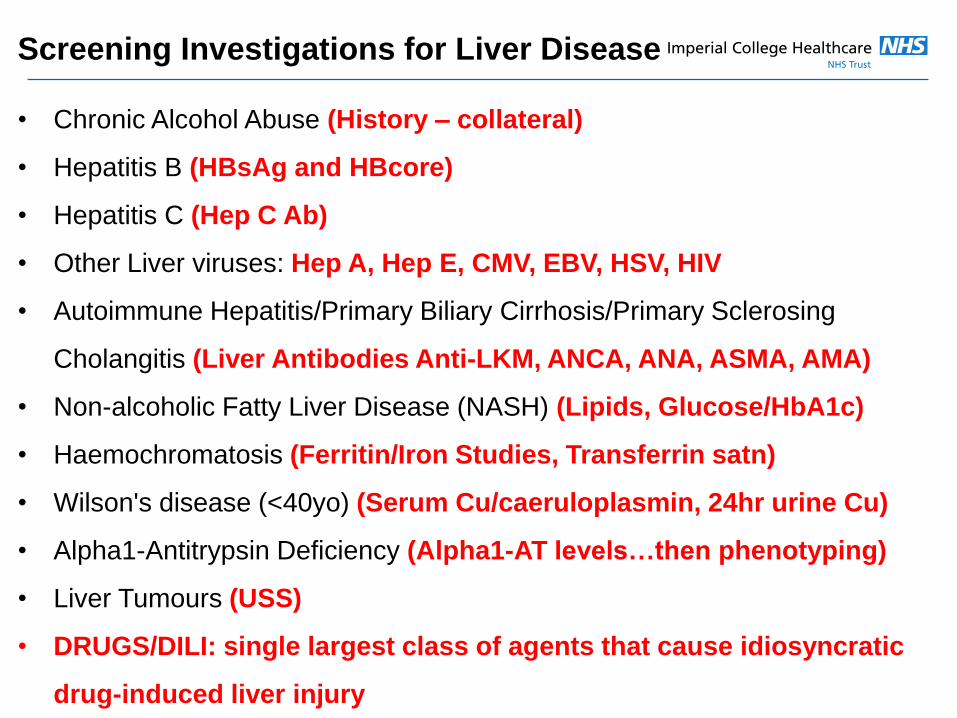
• Chronic Alcohol Abuse (History – collateral)
• Hepatitis B (HBsAg and HBcore)
• Hepatitis C (Hep C Ab)
• Other Liver viruses: Hep A, Hep E, CMV, EBV, HSV, HIV
• Autoimmune Hepatitis/Primary Biliary Cirrhosis/Primary Sclerosing
Cholangitis (Liver Antibodies Anti-LKM, ANCA, ANA, ASMA, AMA)
• Non-alcoholic Fatty Liver Disease (NASH) (Lipids, Glucose/HbA1c)
• Haemochromatosis (Ferritin/Iron Studies, Transferrin satn)
• Wilson's disease (<40yo) (Serum Cu/caeruloplasmin, 24hr urine Cu)
• Alpha1-Antitrypsin Deficiency (Alpha1-AT levels…then phenotyping)
• Liver Tumours (USS)
• DRUGS/DILI: single largest class of agents that cause idiosyncratic
drug-induced liver injury
Screening Investigations for Liver Disease
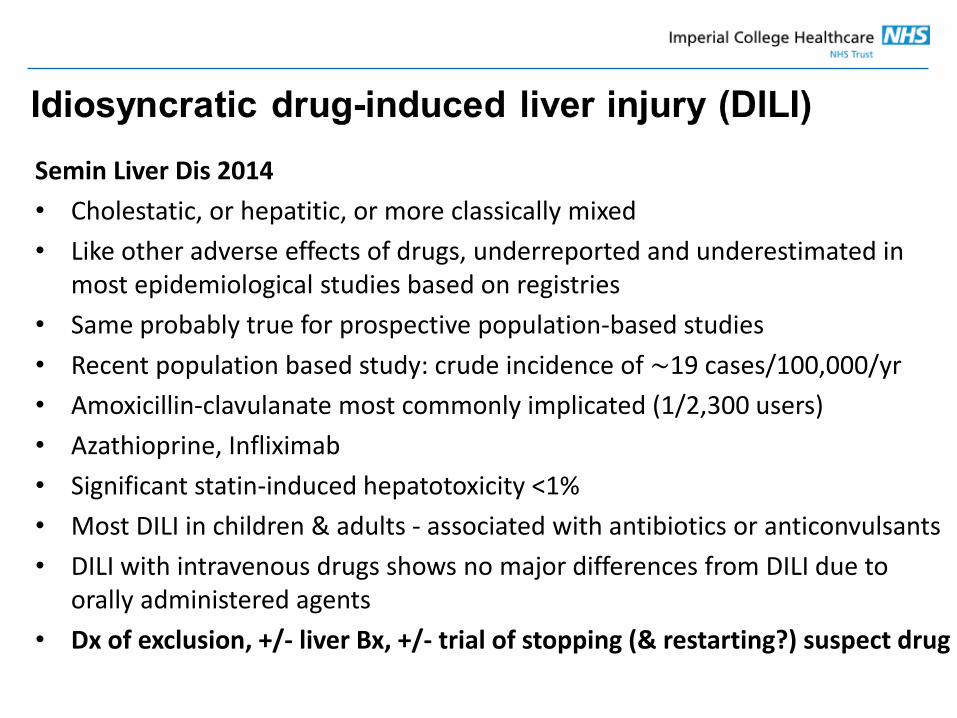
Semin Liver Dis 2014
• Cholestatic, or hepatitic, or more classically mixed
• Like other adverse effects of drugs, underreported and underestimated in most epidemiological studies based on registries
• Same probably true for prospective population-based studies
• Recent population based study: crude incidence of ∼19 cases/100,000/yr
• Amoxicillin-clavulanate most commonly implicated (1/2,300 users)
• Azathioprine, Infliximab
• Significant statin-induced hepatotoxicity <1%
• Most DILI in children & adults - associated with antibiotics or anticonvulsants
• DILI with intravenous drugs shows no major differences from DILI due to orally administered agents
• Dx of exclusion, +/- liver Bx, +/- trial of stopping (& restarting?) suspect drug
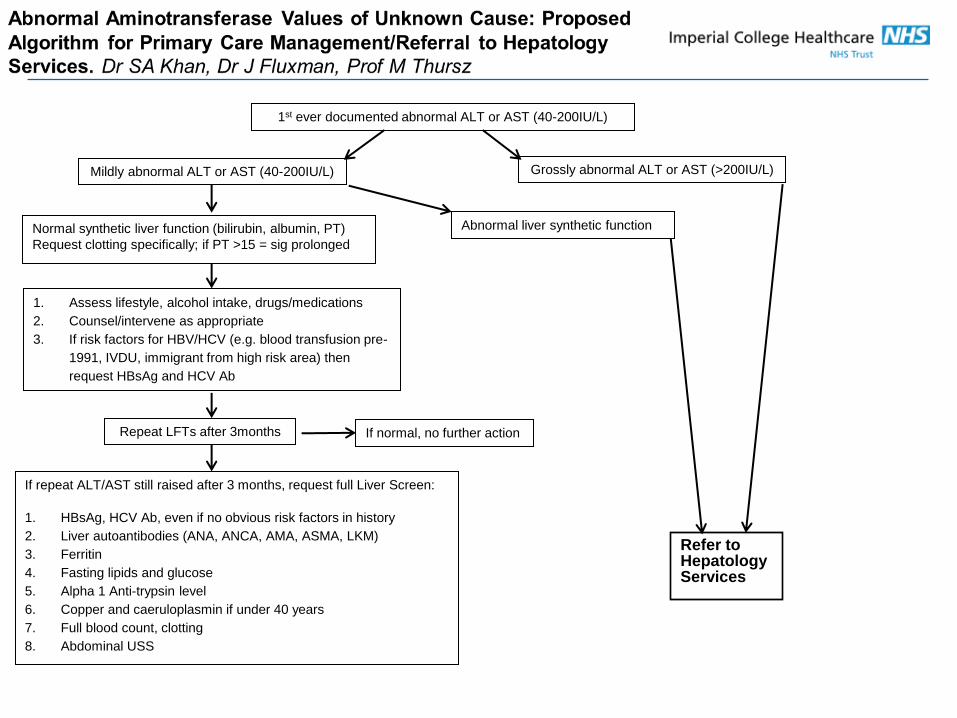
1st ever documented abnormal ALT or AST (40-200IU/L)
Mildly abnormal ALT or AST (40-200IU/L) Grossly abnormal ALT or AST (>200IU/L)
Normal synthetic liver function (bilirubin, albumin, PT)
Request clotting specifically; if PT >15 = sig prolonged
Abnormal liver synthetic function
1. Assess lifestyle, alcohol intake, drugs/medications
2. Counsel/intervene as appropriate
3. If risk factors for HBV/HCV (e.g. blood transfusion pre-
1991, IVDU, immigrant from high risk area) then
request HBsAg and HCV Ab
Repeat LFTs after 3months If normal, no further action
If repeat ALT/AST still raised after 3 months, request full Liver Screen:
1. HBsAg, HCV Ab, even if no obvious risk factors in history
2. Liver autoantibodies (ANA, ANCA, AMA, ASMA, LKM)
3. Ferritin
4. Fasting lipids and glucose
5. Alpha 1 Anti-trypsin level
6. Copper and caeruloplasmin if under 40 years
7. Full blood count, clotting
8. Abdominal USS
Refer to Hepatology Services
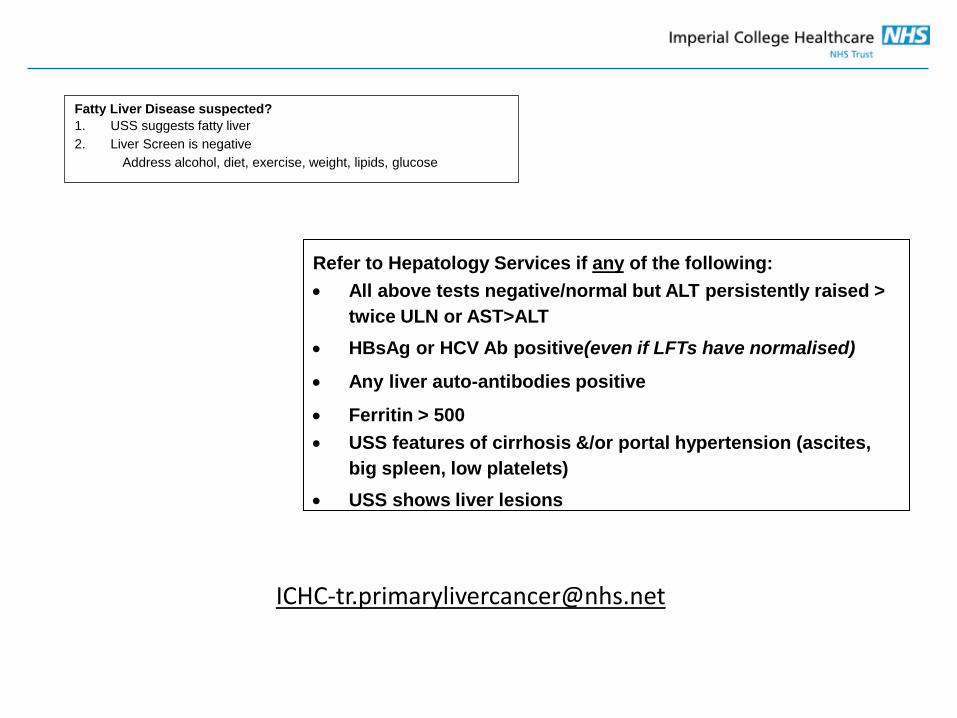
Fatty Liver Disease suspected?
1. USS suggests fatty liver
2. Liver Screen is negative
Address alcohol, diet, exercise, weight, lipids, glucose
Refer to Hepatology Services if any of the following:
All above tests negative/normal but ALT persistently raised >
twice ULN or AST>ALT
HBsAg or HCV Ab positive(even if LFTs have normalised)
Any liver auto-antibodies positive
Ferritin > 500
USS features of cirrhosis &/or portal hypertension (ascites,
big spleen, low platelets)
USS shows liver lesions
Abnormal LFTs - a practical approach
Update on Liver Cancer GP Study Afternoon
Thursday 21st July 2016
Dr Shahid A Khan
Consultant Hepatologist
St Mary’s Hospital
Imperial College Healthcare NHS Trust





























