DR RAKESH JAIN SR CARDIOLOGY MEDICAL COLLEGE, CALICUT
Slide 2
HEMOSTATIC SYSTEM In Brief.
Slide 3
WHEN DOES BLOOD COAGULATE ? Injury to blood vessel. Ex: Plaque
rupure Blood stasis. Ex: AF Procoagulants > Anticoagulants. Ex:
Coagulation disorders
Slide 4
OVERVIEW FROM ENDOTHELIAL DAMAGE TO THROMBOSIS
Slide 5
BLOOD COAGULATION PATHWAYS aPTT PT/ INR
Slide 6
CLASSIFICATION OF ANTICOAGULANTS Coumarin Derivatves e.g.
Warfarin, Acenocoumarol (Acitrom) Indandione Derivatves e.g.
Phenindione, Anisindione Newer anticaogulants Direct thrombin
inhibitors Dabigatran etexilate (Pradaxa) Direct factor Xa
inhibitors Rivaroxaban (Xarelto) Apixaban Edoxaban (DU-176b)
Betrixaban
Slide 7
WARFARIN almost 70 years old and still causing problems Still
we have to stick with it
Slide 8
HISTORY In the 1920s cattle in the Northern USA and Canada were
afflicted by an outbreak of an unusual disease characterized by
fatal bleeding, either spontaneously or from minor injuries. Mouldy
silage made from sweet clover ( Melilotus alba and M. officinalis )
was implicated, and L M Roderick in North Dakota showed that it
contained a haemorrhagic factor that reduced the activity of
prothrombin. However, it was not until 1940 that Karl Link and his
student Harold Campbell in Wisconsin discovered that the
anticoagulant in sweet clover was 3,3 methylenebis (4-hydroxy
coumarin). Further work by Link led in 1948 to the synthesis of
warfarin, which was initially approved as a rodenticide in the USA
in 1952, and then for human use in 1954. The name warfarin is
derived from WARF (Wisconsin Alumni Research Foundation) and arin
from coumarin.
Slide 9
WARFARIN Most widely used anticoagulant in the world Coumarin
derivative, water soluble vit K antagonist Low cost and highly
effective, if given in right way.
Slide 10
Vitamin K-dependent clotting factors (FII, FVII, FIX, FX,
Protein C/S/Z) Epoxide Reductase -Carboxylase (GGCX) MECHANISM OF
ACTION: Warfarin inhibits the vitamin K cycle Warfarin Inactivation
CYP2C9 Pharmacokinetic Post translational modification
Slide 11
PLASMA HALF-LIVES OF VITAMIN K-DEPENDENT PROTEINS Factor II72h
Factor VII6h Factor IX24h Factor X36h Peak anticoagulant effect may
be delayed by 72 to 96 hours
Slide 12
PHARMACOLOGY Recemic micture of R and S isomers (S more active)
Rapidly and completely absorbed from GI tract Blood level peaks
about 90 min of administration 90% of circulating warfarin is bound
to albumin Plasma t1/2 is 36-42 hrs Only small fraction of unbound
warfarin is biologically active Warfarin is accumulates in liver,
where it undergoes CYP2C9 mediated oxidative metabolism. Inactive
metabolites are excreted in urine and stools.
Slide 13
CYP2C9 SNPs alter warfarin metabolism: CYP2C9*1 (WT) normal
activity CYP2C9*2 (Arg144Cys) - low/intermediate activity CYP2C9*3
(Ile359Leu) - low activity Two relatively common variants, CYP2C9*2
and CYP2C9*3, encode an enzyme with reduced activity. requiring
lower maintenance doses of warfarin. Approximately 25% of whites
have at least one variant allele of CYP2C9*2 or CYP2C9*3, whereas
these variant alleles are less common in blacks and Asians Warfarin
dose reduction requires as follow: Heterozygosity for CYP2C9*2 or
CYP2C9*3 allele : 20%-30% Homozygosity for the CYP2C9*2 or CYP2C9*3
allele : 5 0%-70% Effect of CYP2C9 Genotype on Anticoagulation
Slide 14
Effect of CYP2C9 Genotype on Anticoagulation-Related Outcomes
(Higashi et al., JAMA 2002) N 127 28 4 18 3 5 mg warfarin/day
Slide 15
VKORC1: New Target Protein for Warfarin Epoxide Reductase
-Carboxylase (GGCX) Clotting Factors (FII, FVII, FIX, FX, Protein
C/S/Z) Rost et al. & Li, et al., Nature (2004) (VKORC1) 5 kb -
chr 16
Slide 16
Effect of VKORC1 Genotype on Anticoagulation Three polymorphic
variants of VKORC1 Non-A,Non-A : wild type Requiring more warfarin
dose Non-A/A : Heterozygous Requiring 25% dose reduction A/A :
Homozygous - Requiring 50% dose reduction Means wild type having
more resistance to warfarin while homozygous is more sensitive.
Asians have the highest prevalence of VKORC1 variants, followed by
whites and blacks Polymorphisms in VKORC1 likely explain 30% of the
variability in warfarin dose requirements. VKORC1 variants are more
prevalent than variants of CYP2C9 Genotype Freq in Asians (%) Dose
reduction Non-A,Non-A : wild type 7 -- Non-A/A : Heterozygous 30 26
A/A : Homozygous 63 50
Slide 17
These findings prompted the U.S. Food and Drug Administration
(FDA) to amend the prescribing information for warfarin to indicate
that lower initiation doses should be considered for patients with
CYP2C9 and VKORC1 genetic variants.
Slide 18
DOSING Usual dose is 5 mg/day (1-20 mg) Lower doses require in
Elderly Pt on increased risk of bleeding Ex. Pt on aspirin Heart
failure Liver disease Renal impairment Malnutrision Thyrotoxicosis
(Opposite in Myxedema) Asian patients: Explained by genetic
variation in hepatic enzymes (CYP3C9 & VKORC1 Polymorphism)
High intake dietary Vit-K (green vegetables e.g. broccoli) reduces
the efficacy of Warfarin. Practically best time to give warfarin is
~ 6 PM.
Slide 19
Why to add concomitant parenteral anticoagulation ? Because of
delayed onset of action, concomitant parenteral anticoagulant
should be given in pts with established thrombosis or high risk for
thrombosis until INR has been in therapeutic for at least 2 days.
Warfarin monotherapy decreases the levels of two endogenous
anticoagulants, proteins C and S, thus increasing thrombogenic
potential. Overlapping warfarin for at least 5 days with an
immediately effective parenteral anticoagulant counteracts the
procoagulant effect of unopposed warfarin. Usually a minimum 5 days
of concomitant parenteral anticoagulation is recommended.
Slide 20
Monitoring B/c of narrow therapeutic window of warfarin
Standard procedure is to check the PT-INR as follows: INR daily
until it is in therapeutic range 3 times weekly for 2 weeks Once
stable & warfarin dose is known INR every 3-4 weeks or more
frequently if introduction of any new medications
Slide 21
What is PT-INR Warfarin therapy is most often monitored using
the prothrombin time, a test sensitive to reductions in the levels
of prothrombin, factor VII, and factor X. This test involved
addition of thromboplastin (a reagent containing TF, phospholipid
& Ca ++ ) to citrated plasma and determining the time to clot
formation. Thromboplastins vary in their sensitivity to reductions
in the levels of the vitamin Kdependent clotting factors INR
represent the PT according to international reference
thromboplastin, as approved by WHO.
Slide 22
INTERNATIONAL NORMALISED RATIO (INR) INR = [PT pt ] ISI [PT Ref
] [PT Ref ] PT pt prothrombin time of patient PT Ref prothrombin
time of normal pooled sample ISI International Sensitivity Index
Highly sensitive thromboplastins have an ISI of 1.0 Most current
thromboplastins have ISI values that range from 1.0 to 1.4
Indications Atrial fibrillation Prosthetic heart valve Venous
thromboembolism Primary pulmonary hypertension Rarely after Acute
MI (If associated with high risk of thromboembolism e.g. AF, mobile
or pedunculated mural thrombus or prior venous
thromboembolism)
Slide 25
Warfarin in AF AF in the presence of heart disease is strongly
associated with thromboembolism and the benefits of warfarin far
exceed than risk of hemorrhage. Only clear indication for
withholding warfarin are: 1. Lone AF in younger pts 2. Bleeding
diathesis 3. Elderly pts with frequent falls
Slide 26
Warfarin in MS/MR Warfarin is indicated if associated with AF
(Persistent or paroxysmal) Previous embolic episodes (Even if in
sinus rhythm) May be considered if Marked LA enlargement (Diameter
> 55 mm) Spontaneous contrast on echocardiography Warfarin is
not indicated in pts with MS/MR with sinus rhythm.
Slide 27
Warfarin in Mechanical Prosthetic heart valve Class I
indication Warfarin should begin about 2 days after operation INR
should be in the range of 2.0 to 3.0 - bileaflet disc &
Medtronic-Hall valve in aortic position. 2.5 and 3.5 - higher risk
for thrombosis (e.g., AF, previous thromboembolism) or for other
mechanical valves in aortic position & for all valves in the
mitral position Aspirin 75 - 100 mg daily should be given to all
patients with prosthetic valves pts on warfarin for adequte
protection from thromboembolism (Class I indication)
Slide 28
Warfarin in Bio-Prosthetic heart valve Warfarin mandatory only
for first 6-12 weeks when risk of thromboembolism is highest.
Thereafter Aspirin alone is required.
Slide 29
Warfarin in Venous thromboembolism Warfarin should be initated
concurrently with parenteral heparin. For VTE patients, the usual
target INR range is between 2.0 and 3.0. After 5 days, warfarin
alone should be continued for at least 3 months Optimal duration of
anticoagulation depends on clinical settings
Slide 30
Optimal duration of anticoagulation CLINICAL
SETTINGRECOMMENDATION 1 st provoked PE/proximal leg DVT3 to 6
months 1 st provoked upper extremity DVT or isolated calf DVT 3
months 2 nd provoked VTEUncertain 3rd VTEIndefinite duration Cancer
and VTEConsider indefinite duration or until cancer is resolved
Unprovoked PE/proximal leg DVTConsider indefinite duration 1 st
unprovoked calf DVT3 months 2 nd unprovoked calf DVTUncertain
Slide 31
Warfarin in Idiopathic PAH Widely recommended & supported
by numerous studies implicating thrombus as contributing to disease
progression. Significant survival advantage in warfarin treated pts
Current recommendation is to use relatively low dose of warfarin to
maintain INR between 2-3.
Slide 32
Side effects of Warfarin Bleeding Skin necrosis Purple toe
syndrome Teratogenicity Osteoporosis Others: Agranulocytosis,
leukopenia, diarrhoea, nausea, anorexia. nausea, anorexia.
Slide 33
Bleeding Most common complication In form of Mild: epistaxis,
hematuria Severe: Retroperotoneal or gastrointestinal bleeding
Life-threatening : Intracranial bleed Rate of major bleeding
(defined as any visit to hospital for hemorrhage) is 1- 3% per
person-year [CMAJ on November 26, 2012] Half of the complications
occurs because INR exceeds therapeutic range Can be minimized by
keeping INR in therapeutic range
Slide 34
Interventions according to INR/symptoms Asymptomatic pts with
raised INR INR INTERVENTION > 3.5 4.5Withhold warfarin until in
therapeutic range > 4.5Low dose sublingual/oral Vit K 4.9 9.0Vit
k 1 mg > 9.0Vit k 2-3 mg Higher doses of vitamin K (up to 10 mg)
can be administered if more rapid reversal of the INR is required
Although vitamin K administration results in a more rapid reduction
in the INR, there is no evidence that it reduces the risk of
hemorrhage
Slide 35
Symptomatic pts with raised INR SYMPTOMS INTERVENTION Mild
bleedingWithhold warfarin Severe bleedingVit k 10 mg slow i/v
infusion FFP (15 ml/kg) Life threatening bleeding or pt cant
tolerate volume overload Prothrombin complex concentrate (II,IX
& X) Prosthetic valves ptsVit K should be strictly avoided,
unless there is life threatening intracranial bleed (Valve
thrombosis) Subcutaneous Vit K gives variable results and should be
avoided
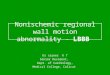
Slide 36
SKIN NECROSIS Rare but very serious complication of warfarin
(prevalence of 0.01-0.1 %) Br J Surg. 2000 Mar;87(3):266-72 Br J
Surg. Occurs 2 to 5 days after initiation of warfarin Usually
occurs after high dose of warfarin Typical presentation is :
Well-demarcated erythematous lesions form on the thighs, buttocks,
breasts, or toes. Typically, the center of the lesion becomes
progressively necrotic. Examination of skin biopsies taken from the
borders of these lesions reveals thrombi in the
microvasculature
Slide 37
Warfarin (Coumadin)induced skin necrosis on the lower abdomen
& breast
Slide 38
Mechanism : Not well understood but a precipitous fall in
plasma protein C or S levels (natural anticoagulants) before
warfarin exert anticoagulant effect, results in procoagulant state
triggering thrombosis of adipose tissue microvasculatures.
Treatment : Discontinuation of warfarin and reversal with vitamin
K, if needed An alternative anticoagulant, such as heparin or LMWH,
should be given to patients with thrombosis Protein C concentrates
or recombinant activated protein C may accelerate healing of the
skin lesions in protein C deficient patients Frozen plasma may be
useful for those with protein S deficiency Occasionally, skin
grafting is necessary when there is extensive skin loss. Prevention
: Start with low dose warfarin in pts with known Protein C or S
deficiency Overlapping with a parenteral anticoagulant when
initiating warfarin therapy
Slide 39
Purple toes syndrome Extremely uncommon cutaneous complication
Characterized by the sudden appearance of bilateral, painful,
purple nonhemorrhagic lesions on the toes and sides of the feet
that blanch with pressure Usually develops 3-8 weeks after the
start of warfarin therapy Mechanism: release of atheromatous plaque
emboli Discontinue COUMADIN therapy if such phenomena are observed.
Consider alternative drugs if continued anticoagulation therapy is
necessary. Pharmacotherapy. 2003 May;23(5):674-7
Pharmacotherapy.
Slide 40
Teratogenicity Occurs in 3.5 6 % Depends on time of gestation
and dose of warfarin given Usually in first trimester of pregnancy
It causes characteristic embryopathy consist of : Nasal hypoplasia
and Chondrodysplasia punctata (epiphyseal and vertebral bone
stippling) Cleft lip and (or) palate Choanal stenosis/atresia
Central nervous system abnormalities Coarctation of aorta (Rare
malformations described following first trimester exposure to
warfarin) Occurs especially if warfarin dose is > 5 mg/day J Am
Coll Cardiol 1999;33:1637 41
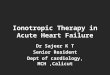
Slide 41
Lateral view X-ray showing calcifications and irregular
ossification of lumbar and sacral vertebrae, consistent with
warfarin embryopathy
Slide 42
OSTEOPOROSIS Long- term use of warfarin (> 1 yr) More common
in males 60% increased risk of osteoporosis-related fracture in men
Mechanism: combination of reduced intake of vitamin K, which is
necessary for bone health, and inhibition by warfarin of vitamin
K-mediated carboxylation of certain bone proteins, rendering them
nonfunctional Beta-adrenergic antagonists may protect against
osteoporotic fractures Arch Intern Med. 2006 Jan 23;166(2):241-6
Arch Intern Med.
Slide 43
Drug interaction- with Warfarin Drugs that Increase Warfarin
Activity Decrease binding to Albumin Inhibit Degradation Decrease
synthesis of Clotting Factors Aspirin, Sulfonamides Cimetidine,
Disulfiram Antibiotics (oral) Category Mechanism Representative
Drugs
Slide 44
Drug interaction with Warfarin Drugs that promote bleeding
Inhibition of plateletsAspirin Inhibition of clotting heparin
Factors antimetabolites Drugs that decrease Warfarin activity
Induction of metabolizingBarbiturates EnzymesPhenytoin Promote
clotting factorVitamin K Synthesis Reduced absorptioncholestyramine
colestipol
Slide 45
Warfarin in special conditions
Slide 46
Pregnancy It causes Fetal abnormalities (Teratogenic)- in first
trimister Chances of intracranial bleeding in baby while passage
through birth canal in third trimister Because of this, warfarin is
contraindicated in 1 st (first 12 weeks) & 3 rd trimsters (last
2 weeks) Warfarin does not passes in breast milk & is safe for
nursing mothers.
Slide 47
Anticoagulant approach in pregnancy Should be First 12 weeks12
to 38 weeks38 weeks to 12 hrs before delivery Postpartum period
UFH/LMWH WarfarinUFH or LMWHWarfarin+ UFH/LMWH (4-5 days) Warfarin
< 5 mg/day throughout pregnancy (Best, because of its good
antithrombotic effect)
Slide 48
Warfarin modification before surgery Pt on long term
anticoagulation with warfarin should stop it 5 days in prior to
elective surgery to allow INR to return to normal level Those at
high risk of thromboembolism can be bridged with once or twice
daily s/c LMWH once the INR fall below 2. The last dose of LMWH
should be given 12 or 24 hrs before depending on bd or od dose
respectively
Slide 49
ACENOCOUMAROL (acitrom) Same as warfarin with following
differences: Shoter half life 10-16 hrs More rapid onset of action
on PT Shorter duration of action (2 days) Causes GI disturbances,
oral ulcerations and dematitis 4 mg on day one, 4-8 mg on the day 2
nd then maintenance dose 1-8 mg according to response by PT
test
Slide 50
THE OVERALL ANTICOAGULATION QUALITY IS SIGNIFICANTLY BETTER
WITH WARFARIN AS COMPARED TO ACENOCOUMAROL 72% 67% 64% 66% 68% 70%
72% % Responders WarfarinAcenocoumarol Thrombosis And Haemostasis
1994; 71(2): 188-191
Slide 51
Newer Oral Anticoagulants
Slide 52
Why we need alternatives to warfarin ???
Slide 53
Whats wrong with warfarin? 1. Narrow therapeutic range 2. Slow
onset of action 3. Slow offset of action (long duration of action,
long elimination half life) 4. Multiple drug and dietary
interactions 5. Monitoring required to maintain in therapeutic
range 6. Difficult to manage for invasive procedures 7. Under-use
of therapy due to fear of adverse events and complexity of
management
Slide 54
8. Efficacy is dependent upon infrastructure Time in
therapeutic range (TTR) is associated with improved safety and
efficacy TTR is improved with AC management programs TTR is greater
in countries with more sophisticated health care
infrastructure
Slide 55
What are the attributes of the ideal anticoagulant? 1. Oral
administration 2. Rapid onset of action/rapid offset of action 3.
Wide therapeutic range 4. Predictable therapeutic effect with fixed
or weight-based dosing 5. No food or drug-drug interactions 6. No
monitoring required (but the ability to monitor if desired) 7. Well
defined pharmacokinetics in presence of renal or hepatic disease 8.
Easily reversible 9. Cost effective
Slide 56
Newer oral anticoagulants
Slide 57
Classification Direct thrombin (IIa) inhibitor Dabigatran
(Pradaxa) Factor Xa inhibitors Rivaroxaban (Xarelto) Apixaban
Slide 58
Dabigatran etexilate (Pradaxa) Oral Direct thrombin (factor
IIa) inhibitor It is a prodrug & does not exhibit any
pharmacological activity Initially recommended by FDA on October
19, 2010 for Non-valvular AF
Slide 59
Pharmacokinetics: After oral administration, dabigatran
etexilate is rapidly absorbed. It get rapidly & completely
converted to dabigatran (active form in plasma) Peak plasma
concentration reached in 0.5 2 hrs T1/2 is 15-17 hours 90% of
excreted unchanged in urine. So dose reduction required in moderate
renal impairment & is contraindicated in severe renal
impairment.
Slide 60
Minimal metabolism of dabigatran by CYP3A4 enzymes is
clinically insignificant No dose modification required in hepatic
impairment Dabigatran is also a substrate for P- glycoprotein ( a
trans-membrane pump expelling drugs out of cell). So P-
glycoprotein inhibitors (e.g. amiodarone, verapamil &
clarithromycin) can increase whereas inducers (e.g. rifampicin, st.
johns wart) may reduce dabigatran level in plasma.
Slide 61
Slide 62
Slide 63
Slide 64
Slide 65
Dabigatran hydrolyze over time when exposed to humidity,
causing a breakdown of active ingredient, and rendering the
medication less effective
Slide 66
So, Pradaxa is packaged in a 30-day supply bottle with a
desiccant cap or in unit-of-use blister packaging to minimize
product breakdown from moisture. (Use within 4 months of opening
and keep in original container)
Slide 67
RE-COVER Primary outcome (recurrent VTE or death due to VTE):
2.4% vs. 2.1% Mortality: 1.6% vs. 1.7% (p > 0.05) Major
bleeding: 1.6% vs. 1.9%; Major + clinically relevant bleeding: 5.6%
vs. 8.8.% (p = 0.002) Trial design: Evaluated the safety and
efficacy of dabigatran 150 mg twice daily (n 1274) vs. warfarin (n
1265) for the treatment of acute VTE. Patients were followed for 6
months. Results Dabigatran (n = 1,274) Dabigatran 150 mg twice
daily is noninferior to warfarin for the treatment of acute VTE,
with a slightly better bleeding profile Complements other studies
showing safety and efficacy of dabigatran, as compared with
warfarin in other settings, such as AF 2.4 2.1 % 0 4 (p <
0.001*) Conclusions Warfarin (n = 1,265) 1 2 3 Primary
endpointMajor bleeding % (p = 0.38) 1.6 1.9 Schulman S, et al. N
Engl J Med 2009;361:2342-52 5 * For noninferiority 0 4 1 2 3 5
Slide 68
Indications of dabigatran Useful alternative to warfarin- To
prevent stroke & blood clots in pts with either paroxysmal or
permanent AF in the absence of prosthetic heart valve, significant
heart valve disease or severe renal impairment (i.e. non valvular
AF) Treatment of DVT & Pulmonary embolism Prophylaxis of venous
thromboembolism after orthopedic surgery
Slide 69
Dose of Dabigatran Depends on renal function i.e. creatinine
clearance GFR (ml/min) Dabigatran dose > 30150 mg 1BD 30 - 1575
mg 1BD < 15 or dialysis not recommended Dabigtran should be
discontinued in pts who develop ARF while on dabigatran and
alternative anticoagulant should be considered.
Slide 70
Prophylaxis of venous thromboembolism after orthopedic surgery
is 220 mg once daily against venous thromboembolism in post
operative period Against stroke in AF pts Dose reduction by 50 % in
Moderate renal impairement Older than 75 years of age No dose
adjustment is required for pts weight Use without regard to meal
AJR:199,September 2012
Slide 71
Converting pts from or to Warfarin From warfarin to dabigatran
Stop warfarin & start dabigatran once INR fall below 2 From
dabigatran to warfarin Adjust the starting time of warfarin based
on creatinine clearance CrCL (ml/min)Days before stopping
dabigatran > 503 days 50 - 302 days 30 - 151 day < 15 or
dialysisnot recommended
Slide 72
Converting pts from or to parenteral anticoagulants From
parenteral anticoagulants to dabigatran Intermittent parenteral
anticoagulant Start dabigatran 0-2 hrs before next dose Continuous
parenteral anticoagulant (e.g. UFH) Start dabigatran at the time of
stopping parenteral anticoagulant From dabigatran to parenteral
anticoagulants Wait for 12 hrs (CrCl> 30 ml/min) or 24 hrs
(CrCl< 30 ml/min) after last dose of dabigatran before starting
parenteral anticoagulant
Slide 73
Dabigatran in pts planned for elective surgery If possible,
stop dabigatran 1-2 days before (CrCl> 50 ml/min) or 3-5 days
before (CrCl< 50 ml/min) invasive or surgical procedures. Longer
periods may be considered if pt undergoing 1. Major surgery 2.
Spinal puncture 3. Placement of spinal or epidural catheter or
port
Slide 74
Dabigatran in pts planned for emergency surgery Because
specific antidote is not available, options are Either have to wait
until the anticoagulant effect has spontaneously diminished Or
Undergo their procedure with the knowledge that they have a
increased risk of bleeding
Slide 75
Postoperative management It depends almost exclusively on the
postoperative risk of bleeding Procedures with with good hemostasis
shortly after the end of the procedure, resumption on same evening
can be done (i.e. minimum of 4 to 6 hours after surgery) starting
with a half dose (75 mg) for the rst dose, and thereafter the usual
maintenance dose. For major abdominal surgery or urologic surgery
with incomplete hemostasis, resumption should be delayed until
there is no drainage or other evidence of active bleeding
Slide 76
Monitoring anticoagulant effect of dabigatran Need not to
assess regularly (ex. In the setting of emergency surgery) In
emergency most accessible tests are 1. TCT 2. aPTT If the TCT is
normal, it is safe to assume that the level of dabigatran is very
low and that the patients risk of bleeding development is similar
to that of other patients undergoing the procedure
Slide 77
Antidote Specific agent not available Though limited data,
following agents may be used Activated prothrombin complex
concentrate Recombinant factor VIIa Concentrate of coagulant
factors II, IX and X Hemodialysis (because only 35% of dabigatran
is bound to plasma proteins) Protamine sulfate and Vit-K are not
helpful
Slide 78
Adverse effects Bleeding increases with age GI events Dyspepsia
(12%) Abdominal pain Gastritis including GERD, esophagitis, erosive
gastritis, gastric hemorrhage and GI ulcers Hypersensitivity
reaction (