Embed Size (px)
Citation preview
Dr. Brian Perri Dr. Khawar Siddique Dr. Edward Nomoto Dr. Albert Wong
Gender:
First Name:
XXX-XX-
Last 4 of Social:Female Male
Dr. Patrick Hill
State: Zip Code:
Home Phone: Cell Phone: Work Phone:
Last Name:
Date of Birth:
Address:
City:
Last Name: First Name:
Specialty:
Address:
City: State: Zip Code:
Office Phone: Fax:
Last Name: First Name:
Address:
City: State: Zip Code:
Office Phone: Fax:
Upd. 10/11/2018 AD
Email Address:
5 6 7 8 9 10
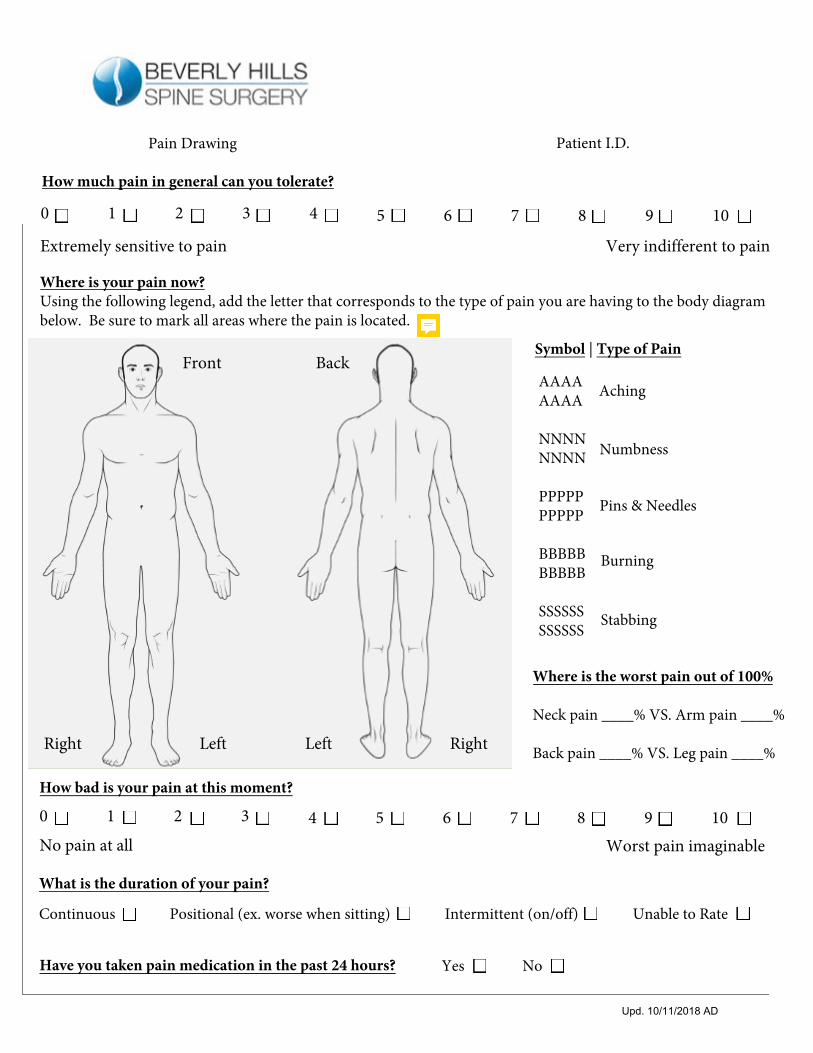
Where is your pain now?Using the following legend, add the letter that corresponds to the type of pain you are having to the body diagram below. Be sure to mark all areas where the pain is located.
AAAAAAAA
NNNNNNNN
PPPPPPPPPP
BBBBBBBBBB
SSSSSSSSSSSS
Aching
Numbness
Pins & Needles
Burning
Stabbing
Symbol | Type of Pain
Where is the worst pain out of 100%
Neck pain ____% VS. Arm pain ____%
Back pain ____% VS. Leg pain ____%
Upd. 10/11/2018 AD
Patient I.D. Pain Drawing
How much pain in general can you tolerate?
0 1 2 3 4
Extremely sensitive to pain Very indifferent to pain
4 5 6 7 8 9 10
How bad is your pain at this moment?
0 1 2 3
No pain at all Worst pain imaginable
Right Left Left Right
Front Back
What is the duration of your pain?
Have you taken pain medication in the past 24 hours? Yes No
Continuous Positional (ex. worse when sitting) Intermittent (on/off) Unable to Rate
Patient I.D. Personal Information
Last Name: _________________________________ First Name: ________________________ Middle: ______ Age: __________ Occupation: ____________________________________ Right-Handed Left-Handed
Duration of symptoms:
Date of surgeries:
What are your symptoms?
Previous operations:
Other past and current medical problems (i.e. hypertension, stroke, diabetes, cancer, etc.):
Family medical history (if deceased, list cause of death):
Current medications and frequency (including over-the-counter medicines):
Yes No What & how often? ____________________________ per weekYes No What & how often? ____________________________ per week
List any and all allergies (ex. latex, ibuprofen, etc.):
Smoker? Alochol? Recreational drug use? Yes No What & how often? ____________________________ per week
Radiology: What type of radiology have you had recently? Please list dates and location:
Regarding MRIs, are you claustrophobic? Yes No Do you have metal implants? Yes No
Upd. 10/11/2018 AD
Patient I.D.General Review of your Sypmtoms
Upd. 10/11/2018 AD
Please mark any medical condition that applies to you
CardiovascularChest painIrregular heart beatHigh/low blood pressurePoor circulationRapid heart rateSwelling of anklesVaricose VeinsHeart attack
ConstitutionalChills/sweats/feverFaintingForgetfulnessLoss of sleepNervousnessWeight loss
Ear/Nose/ThroatBleeding gumsDifficulty swallowingEarache Ear dischargeHearing lossHoarsenessNosebleedsPersistent coughRinging in earsSinus problems
EndocrineRapid weight loss/gainIntolerance to warm roomMultiple broken bonesCessation of Menstrual periodsExcessive hunger/thirstLoss of libidoSpontaneous nipple discharge
I do not have any of the listed medical conditions
EyesBlurred visionCrossed eyesDouble visionVision flashes or halos
GenitourinaryBlood in urineLack of bladder controlPainful urinationFrequent urination
GastrointestinalBloatingBowel changesConstipationDiarrheaGasHemorrhoidsIndigestionNauseaPoor appetiteRectal bleedingStomach painUlcersLiver problems
Hematologic/LymphaticSwollen lymph nodesEasy skin bruisingProlonged bleeding cuts tooth extractionLow blood countFrequent infections
IntegumentarySkin rashes or eruptionsChronic skin itching
MusculoskeletalPain, weakness numbness, or swelling in hands, wrist, hips, knees or jointsPain in arms or legs
NeurologicalFaintingHeadachesNumbness of arm or legSeizuresTingling in hands or feet
PsychiatricAnxietyDepressionPanic attacksRestlessness
RespiratoryBloodCoughDizzinessShortness of breath
Women Abnormal pap smear Bleeding between periods Breast lumpExtreme menstrual pain Hot flashesPainful intercourseAre you pregnant? No Yes
MenBreast lumpLump in testiclePenis dischargeSore on penis
08/24/2018 ME
PATRICK HILL, MD
EDWARD NOMOTO, MD BRIAN PERRI, DO
KHAWAR SIDDIQUE, MD ALBERT WONG, MD
AUTHORIZATION TO COMMUNICATE VIA ELECTRONIC MEANS Our office prefers the efficiency and convenience of electronic communication. We may send you office reminders, test results, appointment summaries and surgery instructions via the electronic method you prefer. If you agree to communicate with us electronically, please fill out your information below. We will never sell your information to any third party. Per California law, certain test results such as HIV, cancer, pathology, and STD will not be sent via electronic means. Email Address________________________________________________________________________________ Secure phone number for messages________________________________________________________ Additional person(s)/email(s)/phone number(s) authorized to receive information outlined above on my behalf: _______________________________________________________________ Name (Printed)______________________________________________________________________________________ Signature______________________________________________________________________________________ Date___________________________________________________________________________________________
DISCLOSURE OF INFORMATION AND FINANCIAL AGREEMENT
PATIENT CONSENT FOR SERVICES: I hereby consent to and authorize the performance of all treatments, surgery, and medical services by the staff of the Beverly Hills Spine Surgery network. These may include but are not limited to: emergency treatment or services, laboratory procedures, x-ray examinations, medical or surgical treatment or procedures, or anesthesia provided to me under the general and special instructions of my physician or surgeon. PATIENT PHOTOGRAPH: I understand that Beverly Hills Spine Surgery is deeply committed to my safety and identity protection. I agree to have my picture taken at check-in for inclusion in my medical record. I understand that my photograph will be used to protect me from identity theft, to ensure patient safety and to further personalize the services I will receive. My picture helps to confirm that all members of the Beverly Hills Spine Surgery Network care team are accessing the correct medical record. REFERRALS/AUTHORIZATION: I understand that depending on my insurance, I may need a referral from my provider to see a specialist. If so, and my provider decides it is medically necessary, I will allow 7-10 working days for this process. I will be promptly advised of any requests that are determined not to be appropriate or necessary. I understand that if I choose to access specialty services without prior authorization from my provider, or I elect to use a Point of Service option or fail to notify Beverly Hills Spine Surgery if my insurance plan requires specific outside vendors such as laboratories to perform referred services, I may be financially responsible for the services rendered and insurance may not cover the relevant services. RELEASE OF INFORMATION: I authorize the release of my medical records or other information necessary to provide health care, to process my medical claims, and for other purposes relating to the health care operations. Additional information is provided in our HIPAA Privacy Policy. MEDICATION REFILLS: I understand that refills may take 24-48 hours to complete and that the most efficient way to get a refill is to contact my pharmacy directly. In order to ensure timely medication refills, I agree to notify my physician’s office regarding my preferred pharmacy. ANCILLARY SERVICES: I understand that depending on my insurance, I may receive a separate bill for laboratory, x-ray, anesthesia, or other ancillary services. INSURANCE COVERAGE: I acknowledge that it is my responsibility to understand the benefits and limitations on benefits under my insurance or health plan and to contact my insurance carrier/health plan if I have questions. COPAYMENT POLICY: If applicable, at the time of check-in, I will be required to pay a co-payment. If I do not pay my co-payment, I understand that my visit may be cancelled. FINANCIAL RESPONSBILITY FOR SERVICES AND CONSENT OF PAYMENT: I hereby authorize payment of medical benefits billed to my insurance to Beverly Hills Spine Surgery. I have listed all health insurance plans from which I may receive benefits. I hereby accept responsibility for payment for any service(s) provided to me that is not covered by my insurance. I agree to pay all copayments, coinsurance, and deductibles at the time services are rendered. I also accept responsibility for fees that exceed the payment made by my insurance, if Beverly Hills Spine Surgery does not participate with my insurance. I hereby authorize Beverly Hills Spine Surgery to use and/or disclose my health information which specifically identities me or which can reasonably to be used to identify me to carry out my treatment, payment, and healthcare operations. I understand that if my insurance company issues a check to me for the services provided, it is my responsibility to forward the check to Beverly Hills Spine Surgery for deposit. I understand that while this consent is voluntary, if I refuse to sign this consent, Beverly Hills Spine Surgery can refuse to treat me. I understand this authorization can only be revoked in writing, if I revoke my consent, such revocation will not affect any actions that Beverly Hills Spine Surgery took before receiving my revocation. I certify that I have read and fully understand the above. Anything that I did not understand was explained to me. I have no additional questions. Signature of Patient or Patient’s Representative: _______________________________________ Date: _______________________ Printed Name of Patient: _________________________________ Relationship of representative to patient: _________________________
HIPAA PRIVACY POLICY PATIENT CONSENT FORM
The Health Insurance Portability and Accountability Act (HIPAA) provides safeguards to protect your privacy. Implementation of HIPAA requirements officially began on April 14, 2003. Many of the policies have been our practice for years. This form is a “friendly” version. What this is all about: Specifically, there are rules and restrictions on who may see or be notified of your Protected Health Information (PHI). These restrictions do not include the normal interchange of information necessary to provide you with office services. HIPAA provides certain rights and protections to you as the patient. We balance these needs with our goal of providing you with quality professional service and care. Additional information is available from the U.S. Department of Health and Human Services. www.hhs.gov We have adopted the following policies: 1. Patient information will be kept confidential except as is necessary to provide services or to ensure that all administrative matters related to your care are handled appropriately. This specifically includes the sharing of information with other healthcare providers, laboratories, health insurance payers as is necessary and appropriate for your care. The normal course of providing care means that such records may be left, at least temporarily, in administrative areas such as the front office, examination room, etc. Those records will not be available to persons other than office staff. You agree to the normal procedures utilized within the office for the handling of charts, patient records, PHI and other documents or information. 2. It is the policy of this office to remind patients of their appointments. We may do this by telephone, e-mail, U.S mail, or by any means convenient for the practice and/or as requested by you. We may send you other communications informing you of changes to office policy and new technology that you might find valuable or informative. 3.The practice utilizes a number of vendors in the conduct of business. These vendors may have access to PHI but must agree to abide by the confidentiality rules of HIPAA. 4. You understand and agree to inspections of the office and review of documents which may include PHI by government agencies or insurance payers in normal performance of their duties. 5. You agree to bring any concerns or complaints regarding privacy to the attention of the office manager or the doctor. 6. Your confidential information will not be used for the purposes of marketing or advertising of products, goods, or services. 7. We agree to provide patients with access to their records in accordance with state and federal laws. 8. We may change, add, delete, or modify any of these provisions to better serve the needs of the both the practice and the patient. 9. You have the right to request restrictions in the use of your protected health information and to request change in certain policies used within the office concerning your PHI. However, we are not obligated to alter internal policies to conform to your request. I, ________________________________________, do hereby consent and acknowledge my agreement to the terms set forth in the HIPAA INFORMATION FORM and any subsequent changes in office policy. I understand that this consent shall remain in force from this time forward. SIGNATURE: _____________________________________________ DATE: ______________________ IF A MINOR, signature, name, and date of parent/guardian: Printed name: _________________________________ Date: _____________________ Signature: _________________________________
Patient Name (Last Name, First Name): _____________________________________________________
Address: _____________________________________________
Phone: _________________________ City: _________________ State: ________ Zip: _____________
I authorize Beverly Hills Spine Surgery to Release or Receive my Medical Information: To From Person / Organization: _________________________________________________
By Mail, to Address: _______________________________________________________________ By Fax, to Number: ______________________________ Phone: ___________________________ By Email, to Email Address: _________________________________________________________ By Pickup in our office.
I authorize the release of the following information. The date range of documents is __________________ Op. Report Office Visit Notes Billing Records Radiology Reports Labs Other________
8436 W. 3rd Street Suite 800Los Angeles, CA 90048
phone 310-746-5918 fax 323-433-7016 Rev 12/13/2018 AD
AUTHORIZATION FOR USE OR DISCLOSURE OF HEALTH INFORMATIONFailure to provide all information may invalidate this authorization
Date of Birth: ____________________
Signature (Patient or Legal Representative): __________________________________Print Name: _____________________________________________ Date: _________Legal Representative Relationship: _________________________________________
I understand that:1. I have a right to receive a copy of this authorization. I may inspect or obtain a copy
of the health information that I am being asked to allow the use or disclosure of. If Irefuse to sign this authorization my refusal will not affect my ability to obtaintreatment.
2. I may revoke this authorization at any time in writing, signed by me or on my behalfand delivered to Beverly Hills Spine Surgery, Inc 8436 W. 3rd Street Suite 800,Los Angeles, CA 90048. If I revoke this authorization, the revocation will not haveany effect on any actions taken prior to receiving the revocation.
3. Information disclosed pursuant to this authorization could be re-disclosed by therecipient and may no longer be protected by federal confidentiality law (HIPAA).However, California law prohibits the person receiving my health information frommaking further disclosure of it unless another authorization for such disclosure isobtained from me or unless such disclosure is specifically required or permitted bylaw.





























