Embed Size (px)
DESCRIPTION
Dr mahnaz sadeghian Pediatric gastroentrologist. How Common Is Encopresis ?. Encopresis is fairly common, even though many cases are not reported due to the child's and/or the parents' embarrassment. - PowerPoint PPT Presentation
Citation preview
Dr mahnaz sadeghian
Pediatric gastroentrologist
HOW COMMON IS ENCOPRESIS?
Encopresis is fairly common, even though many cases are not reported due to the child's and/or the parents' embarrassment.
It is estimated that anywhere from 1.5%
to 10% of children have encopresis. It is more common in boys than in girls.
DEFINITIONEncopresis Refers to the passage of feces
into inappropriate places after a chronologic age of 4 yr (or equivalent developmental level). Subtypes include:
1. Retentive encopresis: Encopresis with constipation and overflow incontinence
2. Nonretentive encopresis: Encopresis without constipation and overflow incontinence
About two thirds of encopresis cases are of the retentive type and associated with chronic constipation
ENCOPRESIS MAY BE:
1.Primary: persist from infancy onward 2.Secondary : may appear after successful toilet training .
typically begins after stool continence has been achieved for a period of 1 or more years (secondary encopresis).

a chart review study suggests that Primary encopresis in boys is associated with global developmental delays and enuresis, Secondary encopresis is associated with high levels of psychosocial stressors and conduct disorder


OVERFLOW INCONTINENCE
IT MAY NOT BE FUNCTIONAL…..Organic incontinence can occur in:
Children who have damaged corticospinal pathways such as lumbosacral myelomeningocele.
Anorectal dysfunction after operative pullthrough surgery for high imperforate anus or colectomy.
Prolonged diarrhea (pelvic floor muscles fatigue)
Psychological counseling may be equally valuable in all forms of encopresis because the stress of soiling is independent of etiology.
WHAT ARE THE SYMPTOMS OF ENCOPRESIS? In addition to the behavior of releasing waste in
improper places, a child with encopresis may have other symptoms, including:
Loss of appetite Abdominal pan Loose, watery stools (bowel movements) Scratching or rubbing the anal area due to
irritation from watery stools Decreased interest in physical activity Withdrawal from friends and family Secretive behavior associated with bowel
movements.

DIAGNOSTIC APPROACH HISTORY birth history of gestational complications,
birthweight, timing of passage of meconium, and tolerance of early feedings.
introduction of cow milk is the most constipating component of the young child’s diet.
Transitions to child care, all-day school, diaper to toilet training
Family history is reviewed for evidence of genetic factors, as aganglionosis, cystic fibrosis, hypothyroidism, neurofibromatosis, or myopathies

HISTORY The character of the stools is reviewed
from birth, especially for the first 24 hours, for consistency, caliber, volume, and frequency.
The age and circumstances at onset of encopresis should be documented.
Encopresis in the absence of constipation suggests an organic or behavioral origin.
A history of possible sexual or rectal abuse should be elicited

DEFINITIONS: (ROME III) FUNCTIONAL DISORDERS OF DEFECATION CATEGORIES
• Functional constipation:
1. - In infants and preschool children
2. - In children 4 to 18 years old3. - Infant dyschezia4. - Nonretentive fecal
incontinence

ROME III CRITERIA FOR THE DIAGNOSIS OF FUNCTIONAL CONSTIPATION IN CHILDREN
Infants and toddlers :At least two of the following present for at least one month: 1. Two or fewer defecations per week 2. At least one episode of incontinence after the acquisition of
toileting skills 3. History of excessive stool retention 4. History of painful or hard bowel movements 5. Presence of a large fecal mass in the rectum 6. History of large-diameter stools that may obstruct the toilet
Children with developmental age 4 to 18 years :At least two of the following present for at least two months: 7. Two or fewer defecations per week 8. At least one episode of fecal incontinence per week 9. History of retentive posturing or excessive volitional stool
retention 10. History of painful or hard bowel movements 11. Presence of a large fecal mass in the rectum 12. History of large-diameter stools that may obstruct the toilet

ROME III CRITERIA FOR THE DIAGNOSIS OF FUNCTIONAL CONSTIPATION IN CHILDREN
infant dyschezia : at least 10 minutes of straining and crying before
successful passage of soft stool in an otherwise healthy infant younger than 6 months of age .The symptom is caused by failure to relax the pelvic floor during the defecation effort, and generally resolves
spontaneously.
fecal incontinence : functional constipation ("retentive incontinence" 80
percent) without constipation ("nonretentive incontinence",
20 percent)

HISTORY prior surgery neonatal complications (NEC) courses of medications that may
contribute to constipation

PHYSICAL EXAMINATION(1) Documentation of growth and weight
gain Signs of systemic diseases include a
thorough neurologic evaluation. The abdomen is examined for degree of
distension Bowel sounds are documented,
perineum is inspected for evidence of encopresis, streptococcal or monilial infection, fissures, and trauma (abuse)
The anal opening is observed, watch for perirectal manifestations of Crohn‘s disease

PHYSICAL EXAMINATION (2) A dilated ampulla filled with retained
firm stool is a feature of functional retention.
The abdominal examination may demonstrate palpable dilated loops of sigmoid and distal colon.
The back should be examined for sacral skin clues to lower spine deformity.
Tendon reflexes should also be assessed to rule out neurological problem.
CLINICAL MANIFESTATIONSThe first consideration in managing
encopresis is assessment of fecal retention.
Rectal examination * A positive rectal examination is
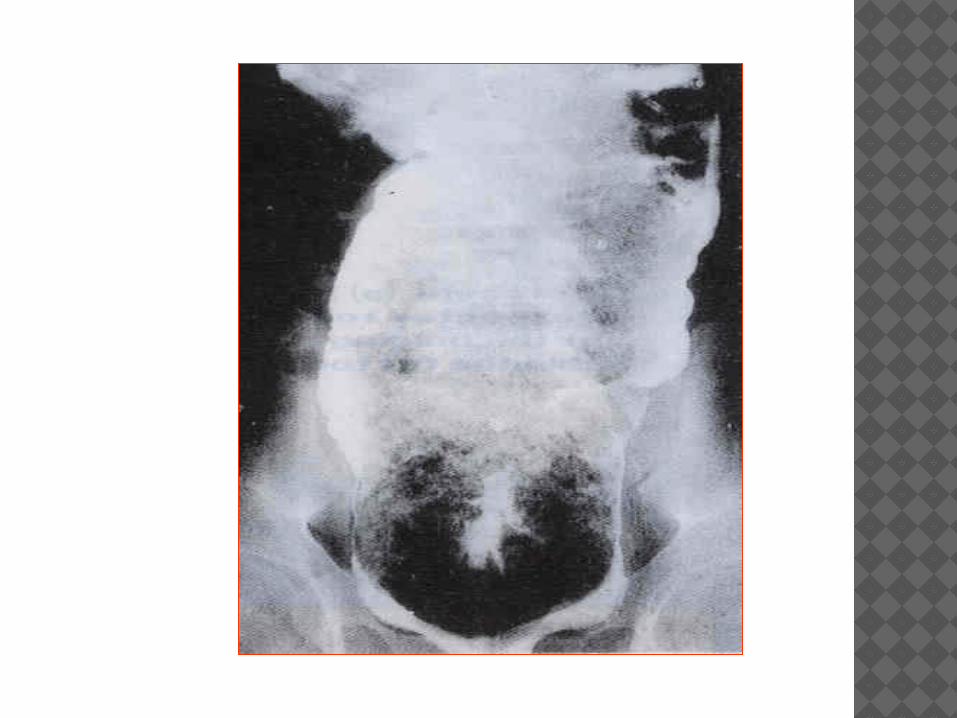
sufficient to document fecal retention • A negative rectal examination in the
presence of encopresis requires plain abdominal roentgenograms.
• The presence of fecal retention is evidence of chronic constipation
CLINICAL MANIFESTATIONSMany children with encopresis present
with abnormal anal sphincter physiology as documented either by electromyography or difficulty in defecating a rectal balloon.
The inability to defecate a balloon at presentation is associated with poorer response to treatment
CLINICAL MANIFESTATIONSAbnormal anal sphincter function is a
marker for chronic constipation; children with this pathology do not appear to have a higher incidence of behavioral or psychiatric disorders than those without.

CLINICAL MANIFESTATIONS
Associated behavioral or psychiatric problems obviously may complicate the treatment of encopresis,especially when parents respond to soiling with retaliatory, punitive measures and children become angry, ashamed, and resistant to intervention.
School performance and attendance may be secondarily affected as the child becomes the target of scorn and derision from schoolmates because of the offensive odor
LABORATORY INVESTIGATIONS
Thyroid functions Serum calcium, electrolyte levels,
magnesium and urea nitrogen. Urinalysis and urine culture The plain abdominal radiograph may be
of value in the child in whom an abdominal examination is difficult or to monitor compliance.
Lumbosacral spine radiographs or magnetic resonance imaging if indicated.
LABORATORY INVESTIGATIONS
Unprepared barium enema for the transition zone or strictures from necrotizing enterocolitis.
The contrast enema defecogram has a definite role in assessing pelvic muscle function following surgery or in the context of central nervous system disease.
Anorectal manometry is available to evaluate internal anal sphincter relaxation and determine the level of pressure awareness in older children.
It also will identify the 25% of chronically constipated children who exhibit a paradoxic increase in external anal sphincter pressure.
LABORATORY INVESTIGATIONS
A few centers now offer total colonic motility, a valuable tool in the evaluation of neuropathic or muscular dysmotility in chronic intestinal pseudo-obstruction.
The value of the suction rectal biopsy has increased with the ability to stain the tissue for both ganglion cells and acetylcholinesterase.
The rectal biopsy also can be of diagnostic value in the child who has amyloidosis, graft versus host disease, lipid storage disease, or Crohn disease.

EVALUATIONHistory Delayed passage of
meconium Preceding acute diarrheal
illness Painful defecation Blood on stool Problems with toilet
training Dietary issues Family history
Laboratory (not necessary in all cases)
Complete blood count Thyroid tests (only in unclear cases) Test for celiac disease Barium enema Anorectal manometry Rectal biopsy - suction or surgical
full-thickness Motility studies
Physical examination • Mass in suprapubic area • Abdominal distention • Anal fissure • Soiled underwear • Anal sphincter tone • Size of rectal vault • Impacted stool (hard or
soft) • Lower back skin defects
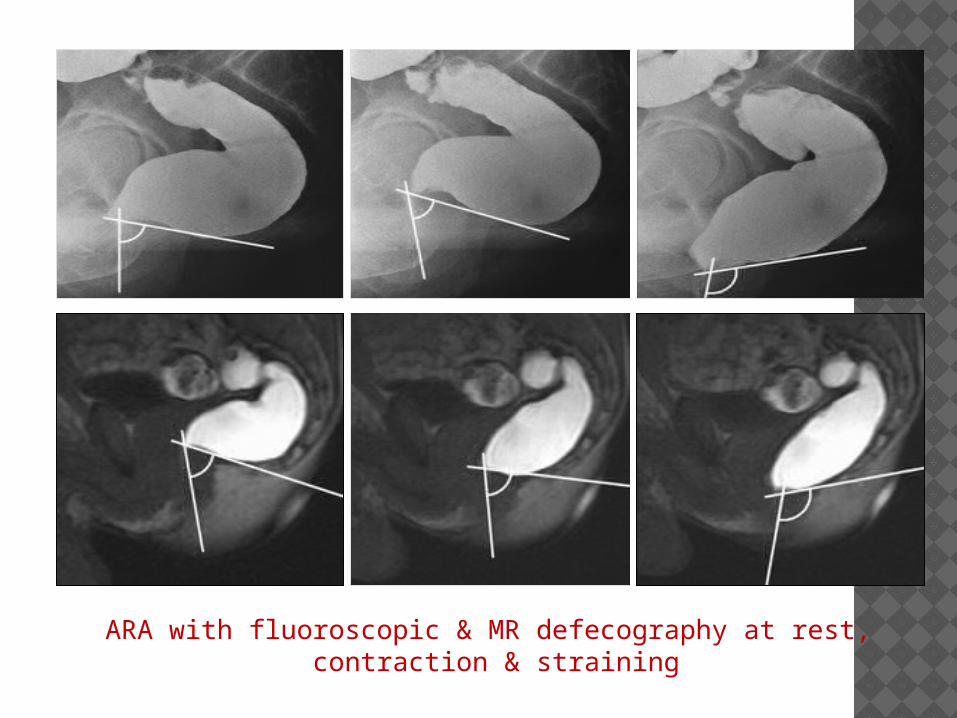
ARA with fluoroscopic & MR defecography at rest, contraction & straining
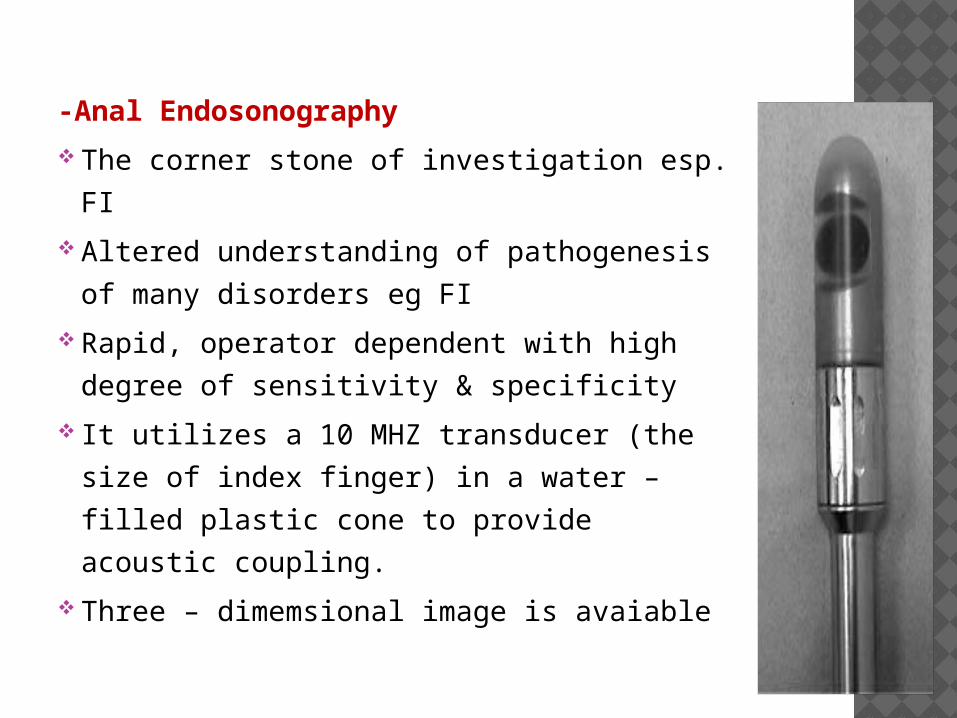
-Anal Endosonography
The corner stone of investigation esp. FI
Altered understanding of pathogenesis
of many disorders eg FI
Rapid, operator dependent with high
degree of sensitivity & specificity
It utilizes a 10 MHZ transducer (the size
of index finger) in a water – filled plastic
cone to provide acoustic coupling.
Three – dimemsional image is avaiable
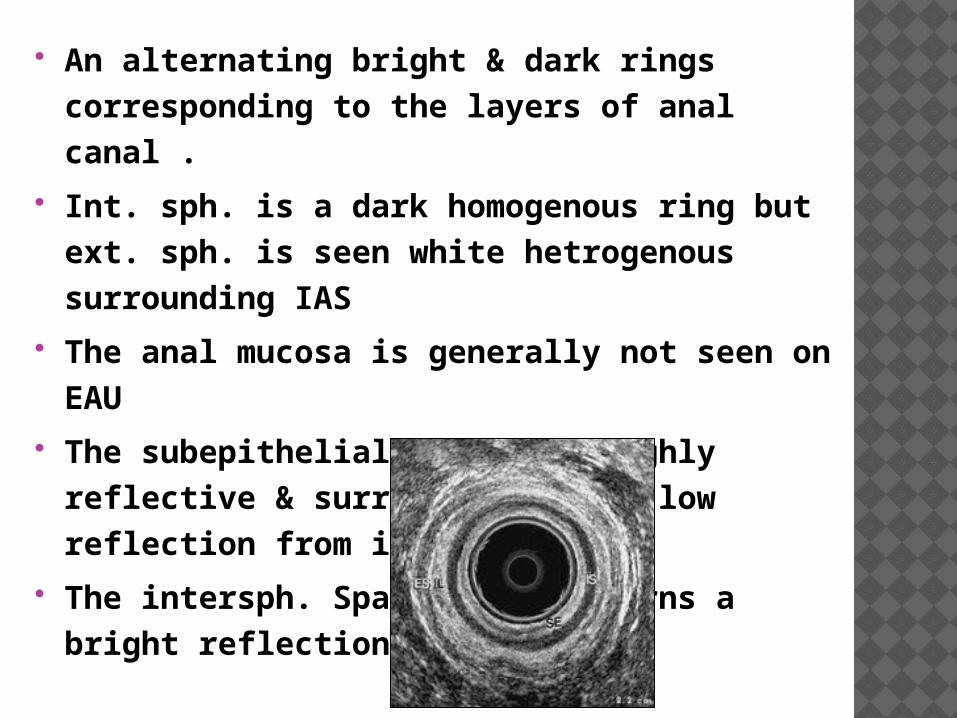
An alternating bright & dark rings corresponding to the layers of anal canal .
Int. sph. is a dark homogenous ring but ext. sph. is seen white hetrogenous surrounding IAS
The anal mucosa is generally not seen on EAU
The subepithelial tissue is highly reflective & surrounded by the low reflection from int. sph.
The intersph. Space often returns a bright reflection.


TREATMENTOn some occasions, manual disimpaction
is required before the treatment can begin; rarely megacolon is observed and referral to a gastroenterologist is required.
Once impacted stool is removed, the combination of constipation management and simple behavior therapy is successful in the majority of cases, though it is often a period of months before soiling stops completely
TREATMENTParents should be actively encouraged to
issue rewards for compliance to the child from the outset of treatment and to avoid power struggles with the child.
Keeping records of the child's progress is necessary Long-term laxative use is contraindicated.
TREATMENTImprovement in some children on tricyclic
antidepressants Tricyclic antidepressants often cause or
exacerbate constipation and should be avoided in children with retentive encopresis Encopresis eventually resolves in most children, regardless of treatment approach.
SUMMARYEncopresis refers to the passage of feces
into inappropriate places after a chronologic age of 4 yr
Subtypes include: Retentive encopresis and Nonretentive encopresis Encopresis may be: Primary or Secondary The first consideration in managing
encopresis is assessment of fecal retention.

SUMMARYPrimary encopresis in boys is associated
with global developmental delays and enuresis,
Secondary encopresis is associated with high levels of psychosocial stressors and conduct disorder
the combination of constipation management and simple behavior therapy is successful in the majority of cases
TREATMENTThe standard treatment approach to
encopresis begins with 1. Clearance of impacted fecal material 2. Short-term use of mineral oil or laxatives to
prevent further constipation. Concomitant behavioral management is also
indicated. The focus of behavioral treatment should be
on compliance with: 1. Regular postprandial toilet sitting and 2. adoption of a high-fiber diet.

Elimination disorders occur in children who have problems going to the bathroom—both defecating and urinating. Although it is not uncommon for young children to have occasional "accidents," there may be a problem if this behavior occurs repeatedly for longer than 3 months, particularly in children older than 5 years.
There are two types of elimination disorders, encopresis and enuresis.
Encopresis is the repeated passing of feces into places other than the toilet, such as in underwear or on the floor. This behavior may or may not be done on purpose.
Enuresis is the repeated passing of urine in places other than the toilet. Enuresis that occurs at night, or bed-wetting, is the most common type of elimination disorder. As with encopresis, this behavior may or may not be done on purpose.

What Is the Outlook for Children with Encopresis?
Encopresis tends to get better as the child gets older, although the problem can come and go for years. The best results occur when all educational, behavioral and emotional issues are addressed. A child may still have an occasional accident until he or she regains muscle tone and control over his or her bowel movements.
There may be an imbalance in neuromuscular control of defecation in constipated patients with encopresis that results in incontinence as a consequence of the increased time to recovery and duration of relaxation of the internal anal sphincter.

WHAT IS NORMAL ? The frequency of stools in most children
decreases from a mean of four per day in the first week of life to 1.7 per day by the age of 2 years.
Over this interval, stool volume increases more than tenfold while maintaining a consistent water content of approximately 75%.
Intestinal transit time from mouth to rectum increases from 8 hours in the first month of life to 16 hours by 2 years of age to 26 hours by the age 10.
HOW DOES IT WORKS Normal continence is maintained by the resting
tonicity of the internal anal sphincter It can be enhanced by contraction of the puborectalis
muscle, which creates a 90-degree angle of rectum to the anal canal.
When more than 15 cc of stool enters the normal rectum, stretch receptors and nerves in the intramural plexus are activated.
Inhibitory interneurons decrease the resting tone in the involuntary smooth muscle of the internal anal sphincter.
HOW DOES IT WORKS (CONT.)
Relaxation of the sphincter allows the stool to reach the external anal sphincter and the urge to defecate is signaled.
If the child relaxes the external anal sphincter, squats to straighten the anorectal canal, and increases intra-abdominal pressure the rectum is evacuated of stool.

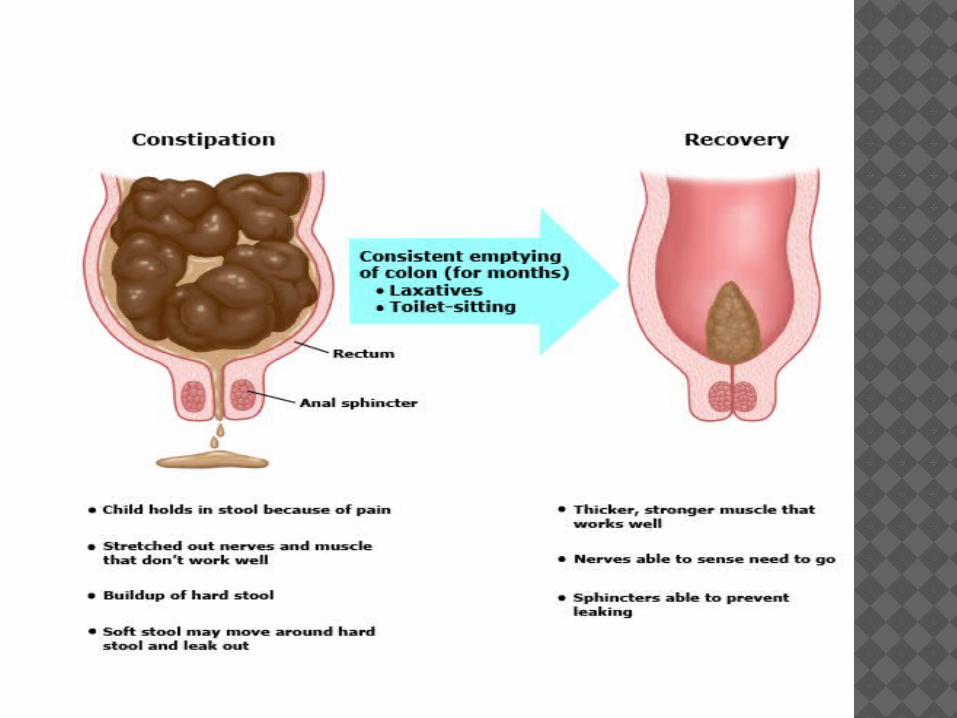
WHY IT MAY NOT WORK If, however, the child tightens the external anal
sphincter and the gluteal muscles, the fecal mass is pushed back into the rectal vault and the urge to defecate subsides.
Repetitive denial of evacuation leads to stretching of the rectum and eventually of the lower colon, producing a reduction in muscle tone and retention of stool.
The longer the stool remains in the rectum, the more water is removed, and the harder the stool becomes to the point of impaction.
Unprepared barium enema for the transition zone or strictures from necrotizing enterocolitis.
The contrast enema defecogram has a definite role in assessing pelvic muscle function following surgery or in the context of central nervous system disease.
Anorectal manometry is available to evaluate internal anal sphincter relaxation and determine the level of pressure awareness in older children.
It also will identify the 25% of chronically constipated children who exhibit a paradoxic increase in external anal sphincter pressure.

DEFINITIONS: (ROME III) FUNCTIONAL DISORDERS OF DEFECATION CATEGORIES
• Functional constipation:
1. - In infants and preschool children2. - In children 4 to 18 years old3. - Infant dyschezia4. - Nonretentive fecal incontinence
ROME III CRITERIA FOR THE DIAGNOSIS OF FUNCTIONAL CONSTIPATION IN CHILDREN
Infants and toddlers :At least two of the following present for at least one month: Two or fewer defecations per week At least one episode of incontinence after the acquisition of toileting
skills History of excessive stool retention History of painful or hard bowel movements Presence of a large fecal mass in the rectum History of large-diameter stools that may obstruct the toilet
Children with developmental age 4 to 18 years :At least two of the following present for at least two months: Two or fewer defecations per week At least one episode of fecal incontinence per week History of retentive posturing or excessive volitional stool retention History of painful or hard bowel movements Presence of a large fecal mass in the rectum History of large-diameter stools that may obstruct the toilet
ROME III CRITERIA FOR THE DIAGNOSIS OF FUNCTIONAL CONSTIPATION IN CHILDREN infant dyschezia : at least 10 minutes of straining and crying before
successful passage of soft stool in an otherwise healthy infant younger than 6 months of age .The symptom is caused by failure to relax the pelvic floor during the defecation effort, and generally resolves
spontaneously.
fecal incontinence : functional constipation ("retentive incontinence" 80
percent) without constipation ("nonretentive incontinence",
20 percent)
RED FLAG SIGNS: Delayed passage of meconeum Abdominal distension, biliousvomiting, ileus , Sign of spinal cord lesion Presence of pilonidal dimple/hair tuft Inactive, bradycardia, poor growth Abnormal anus opening Scyballa mass in abd with empty rectum• Infrequent small or ribbon stools• Constant leaking especially if linked with urinary leaking too