Embed Size (px)
Citation preview

Dr. M G MurphyClinical Director NWIS
Caldicott Guardian for Wales General practitioner
[email protected] @martinmurphy001
Blog sowhatfollows.wordpress.com
Transforming Care in WalesOpportunities
RSA

Structured data •Demographic•Pathology•Radiology •Medication•IHR
WCP – CORE
Unstructured data•WCRS•Shared care record
GP System GP System
CommunityMental health
Social caresystem
CommunityMental health
Social caresystem
Innovation SpaceWork flowPathways
ExistingHospital Existing
Hospital
Etc.
WCCG
WORKING INSIDEOUR WELSH PSBASECURENETWORK
IDENTIFING STAFFUNIQUELY
WITH NADEX
CONTROLACCESS TO WHO SEES WHAT
PROACTIVELY AUDIT EVERY
ACCESS TO EVERY RECORD
MHOLMHOL

Structured data •Demographic•Pathology•Radiology •Medication•IHR
CORE RECORD
Patients Documents•WCRS•Shared care record
GP System GP System
CommunityMental health
Social caresystem
CommunityMental health
Social caresystem
Innovation SpaceWork flowPathways
ExistingHospital Existing
Hospital Etc.
WCCG
WORKING INSIDEOUR WELSH PSBASECURENETWORK
IDENTIFING STAFFUNIQUELY
WITH NADEX
CONTROLACCESS TO WHO SEES WHAT
PROACTIVELY AUDIT EVERY
ACCESS TO EVERY RECORD
MHOLMHOL
National Diabeticsystem
National Diabeticsystem
National Ophthalmology
system
National Ophthalmology
system

Current position• Modern SOA Architecture • Private PSBA, data centers, Active Directory• Core services provided provided slowly rolling
out • Created room for innovation – to use Best of
Breed apps
All our activity is internally focused – obsessed with communicating with each other

So What ? sowhatfollows.wordpress.com

ZZZZZZZZZZ….ZZZZZZZZZZ….


A short history of the NHS
• 1947 – but the care process is 150 years old• The consultation – based on face to face contact• The patient travels to see the doctor / service• Institutional and building focus to provision• System was designed for episodic & infectious
problems • Separate health, social and mental health
services

But We are facing a perfect storm •Declining resources •Aging population with increasing care needs – social, mental , physical •Hospital emergency care has clogged up already with the frail elderly •Great difficulty in caring for people in their own home as numbers and frailty increases•People die in the wrong place – in hospital


NHSDirectWebSite
NHSDW239k
Paid calls
Mental health services
Police
Ambulance325k calls
500k journeys
Outpatients
Community pharmacy70% population use in a year
GP OOH
497k
Social worker
District nurse midwife14% pop. see DN per year
Admissions 343k
A & E714k
(4% FU rate)
DentistDentist
3.2M Welsh Citizens800kLTC
GP Practices5.5M contact s
unscheduled (16M total)
84% surgery10% phone
4% visits
15M new illness episodes(family, friends, voluntary help web etc)
70% population70% populationsee a dentist see a dentist In a year In a year
10m
641k
403k
273k
- 99
9
338k
338k
427
227k189kk
3k
3k
20k
55% journeysstarted in eachcategory are stopped
10k
20k (3k)
24k
78k (1k )
17k
31k
143k
2k
38k
32k
53k9k
6k
1k Died
343k
48k
66k
10k
126k
10k
18k emergency transfer
392
Nursing Home 19k
12k
7k
7k p
ath
1
11
15+ 15
7+
7+
498
Number of call centres , telephones calls

Transition in care services 20th Centaury Care •Medical Hospital disease model
•Episodic reactive (fail and fix)
•Goal is Prevention of death
•All Care is provided by the state
21st Century care •Holistic Community health and social care model •Long term management ( predict and prevent)
•Goal is maximize quality of life & Good death
•Coproduction self care

Individual at home or usual
place of residence
Individual at home or usual
place of residence
24 hour care usually in hospital
24 hour care usually in hospital
Telephone advice or telephone
consultation
Telephone advice or telephone
consultation
Travel – 99.8% they citizen travel to the
services
Travel – 99.8% they citizen travel to the
services
Face to face consultation
with professional
Face to face consultation
with professional
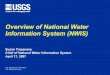
The Visual Care Cycle The basic risk management process in all care services
If the individual or family feel they cannot manage the problem themselves and feel at risk they ring for help
If the professional feels they cannot manage the risk without seeing the individual they arrange a face to face assessment
If after assessment the professional feels that there is residual risk and they cannot safely be returned home they arrange that the person stays in contact with the service 24 hours a day
When the service believes the risk has diminished to an acceptable level the individual return home or to their usual place of residence Individual continues
to self care
Indi
vidu
al co
ntinu
es to
self
care
©MGMurphy

Dealing with risk • Uncertainty = anxiety = risk = cost • Its about human contact – not being alone • We deal with risk – by keeping a closer eye on the patient
i.e. by staying in contact – This is true during a single episode – But it is also true over your lifetime and the reason that 70% of
the cost of care is incurred during the last year of life – morbidity compression
– At the present time the lack of alternatives means we admit put people in hospital beds
Opportunity to use technology to stay in touch – in terms of distance and time

The Great Firewall of Wales (PSBA)
Public servicesNHS,LASocial careMental health
The PublicThe CitizenThe carerThe third sector

Can put the citizen at the Center in our networked world Paradigm shift - we use the technology they have to communicate
Third sectorThird sector Health Health
Citizen Citizen
Mental health Mental health
Social care
Social care
CarerCarer
• One global network, global services – no outside, no inside
• Mobile Always on – anytime, any place, anywhere
• Each of the 15 links can carry voice, video & data
• The security of each link can change depending on type of communication and citizens requirement for confidentiality

Health servicesHealth services Social care Social care Voluntary services
Voluntary services
MHOL•Book appointments•Order prescriptions•Message GP•Access to my GP record
MHOL•Book appointments•Order prescriptions•Message GP•Access to my GP record
Access Knowledge
Internet – Ap CymruAccredited sites •Conditions•Treatments•Performance•Directories
My global communicationsUsed for Tele Health •Video , telephone•Email, Text, IM, HTTPS •Secure social networks•Instant messaging •Communications HUB•Tele devices
Undertake Tasks
GP system GP system
Health vault ( Own store)My copies of •Care plans •Contact details carers•Tests •Schedule •Self monitoring etc
Health vault ( Own store)My copies of •Care plans •Contact details carers•Tests •Schedule •Self monitoring etc
Apps to help me manage my health and social problems
Self monitoringPoint of care
Use my record
Monitor myself

What do we need ?
1. Enable patients to use the technology they have to communicate with the service
2. Enable staff to use the technology the patient has to communicate with patients and with each other
But there is a problem with current way our Networks, PSBA, security & Data centers are configured that will get in the way of delivering this change.

4 Strategic implications for Wales
1. Separate the care record services from the communications services – they require different approaches to privacy, confidentiality & security
2. Shrink the great firewall back to securing the care record data - the way other information services are delivered
3. Provision of the record data over secured link to mobile devices any where – including hospitals, estate & most importantly all homes in Wales
4. Shift the whole of human communications onto global cloud services available to the citizens

Opportunities ?1. Open Wi-Fi – in public estate and homes2. Simple reliable cloud VC – internet TVs etc. 3. Mobile working – seamless use of the above 4. Transformation of care – unscheduled care– Long term – Long term condition management
Its the right time finally for this revolution because we now have a network that reaches into people homes & the technology has moved beyond public services ability to manage it.


Wakey Wakey ...Wakey Wakey ...

Home
“PhoneFirst”
For help
Transport
Assess FaceTo
Face
24 hourCare
Individual unwell
Individual unwell
FamilyfriendsFamilyfriends
Voluntary sector
Voluntary sector
Web Directory
Web Directory
individual Stable at
home
individual Stable at
home
111 call handler 111 call handler
999 call handler 999 call handler
Clinical assessment Mental health assessment
Social care assessment
Clinical assessment Mental health assessment
Social care assessment
Ambu
lanc
e
Ambu
lanc
e
Clin
ic O
P ap
poin
tmen
t Cl
inic
OP
appo
intm
ent
OO
H v
isit
OO
H v
isit
OO
H
appo
intm
ent
OO
H
appo
intm
ent
GP
surg
ery
GP
surg
ery
A&E
A&E
Com
mun
ity
Phar
mac
yCo
mm
unity
Ph
arm
acy
Soci
al W
orke
rSo
cial
Wor
ker
Spec
ialis
t ad
vice
e.g
. D
iabe
tic n
urse
Spec
ialis
t ad
vice
e.g
. D
iabe
tic n
urse
Signpost
Signpost
Hospital Inpatient Hospital Inpatient
24/7 homeCare package
24/7 homeCare package
NursingResidential
NursingResidential
With access to the IHR, Core H & SC recordsCare plan (ELP)& Specialist advice for staff on MH, palliative care Acute physicians e
Mon
itorin
g at
hom
e
Residual
Risk
Residual
Risk
Physical & virtualCall center
With call location& demographic linkage
DN
/CPN
DN
/CPN
USC episode
Phone(SKYPE)
Hot transfer Hot transfe
r
Advice & information
Advice & information
Opt
omat
rist
Opt
omat
rist
Priv
ate
sect
orPr
ivat
e se
ctor
EmergencyRespiteSafe haven
Rapid responseHome care Hospital at home
Hol
istic
ass
essm
ent