Embed Size (px)
Citation preview

8/18/2015
1
Charlie Colquitt,BS,PharmD,CPhAssociate Professor of Pharmacy Practice
Florida A & M University, Tampa Bay CenterClinical Pharmacist
Community Health Centers of Pinellas, Inc.August 22nd, 2015
I, do not have a vested interest in or affiliation with any corporate organization offering financial support or grant money for this continuing education program, or any affiliation with an organization whose philosophy could potentially bias my presentation.
At the end of this presentation, the participants should be able to:◦ Describe the process of hemostasis and thrombosis◦ Discuss the pathogenosis of deep vein thrombosis
(DVT) and pulmonary embolism (PE)◦ Recognize the risks, signs and symptoms of DVT and
PE◦ Describe the novel anticoagulant options indicated for
VTE◦ Discuss the management of bleeding◦ Discuss options for use in the underserved population
At the end of this presentation pharmacy technicians should be able to:◦ Define DVT and PE◦ Identify the novel anticoagulant options◦ Recognize options for use in the underserved
population

8/18/2015
2
Diagnosed VTE at 2 to 3 per 1000 Incidence increases with age Estimated incidence of 8 per 1000 in those
over 80 years Rates are slightly higher in men than woman 2/3 of VTE are DVT and 1/3 PE DVT-associated massive PE causes as many
as 300,000 deaths annually in the US.
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
Platelet Plug Formation◦ On vascular injury, platelets adhere to the site of
injury. Platelet adhesion results in subsequent activation and aggregation. During platelet aggregation, additional platelets are recruited from the circulation to the site of vascular injury, leading to the formation of an occlusive platelet thrombus.◦ The platelet plug is anchored and stabilized by the
developing fibrin mesh.
Yusen R, Eby C, Gage B. Disorders of hemostasis and thrombosis. In:Foster C, Mistry N, PeddiP. The Washington Manual of Medical Therapeutics. 33rd ed. Philadelphia, Pa: 2010.
Clotting factors normally circulate inactive. Two pathways of blood coagulation: extrinsic
and intrinsic. Coagulation is initiated by tissue factor (TF)
exposure. TF with FVIIa, activates FIX and FX. FIXa binds to FVIII activating FX to form FXa. FXa binds FV which converts prothrombin to thrombin. Thrombin activates FXIII that cross-links fibrin to form a stabilized clot.
Yusen R, Eby C, Gage B. Disorders of hemostasis and thrombosis. In:Foster C, Mistry N, PeddiP. The Washington Manual of Medical Therapeutics. 33rd ed. Philadelphia, Pa: 2010.

8/18/2015
3
The intact endothelium adjacent to the damaged tissue actively secretes several antithrombotic substances.
Thrombomodulin causes protein C to convert to its active form activated protein C (aPC). When joined with its cofactor protein S, aPCinactivates FVa and FVIIIa regulating coagulating complexes.
Antithrombin (or antithrombin III) neutralizes thrombin
Tissue factor pathway inhibitor (TFPI)
Yusen R, Eby C, Gage B. Disorders of hemostasis and thrombosis. In:Foster C, Mistry N, PeddiP. The Washington Manual of Medical Therapeutics. 33rd ed. Philadelphia, Pa: 2010.
Platelet and Fibrin aggregation video Fibrin Formation Animation
Emboli - detached, traveling intravascular mass at a site distant from its point of origin.
Thrombi – intravascular mass which is fastened at the point of origin.
Proximal DVT - DVT that occurs in the veins of the thigh (femoral vein, deep femoral vein, common femoral vein, iliac veins, popliteal vein)
Distal DVT - DVT that occurs in the veins of the calf (anterior tibial vein, posterior tibialvein, peroneal vein)

8/18/2015
4
Age History of VTE Major General Surgery Major Orthopedic Surgery Spinal Cord Injury Multiple Trauma Malignancy MI Immobility Oral Contraceptives & Hormone Replacement Antiphospholid Antibody Syndrome
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
Antithrombin Deficiency – pts are at the great risk for VTE than those with protein C and S deficiency.◦ In a study up to 85% of pts with AT deficiency
experienced a thromboembolic event by age 50. Protein C and S deficiencies APC Resistance – Factor V Leiden Factor II – high in whites of European descent. Coagulation Factors VIII, IX and XI have been
linked with increased thrombotic risk.
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
Symptoms◦ Leg swelling◦ Pain◦ Warmth
Signs◦ Superficial veins may be dilated◦ Palpable cord◦ Pain in back of knee
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
8/18/2015
5
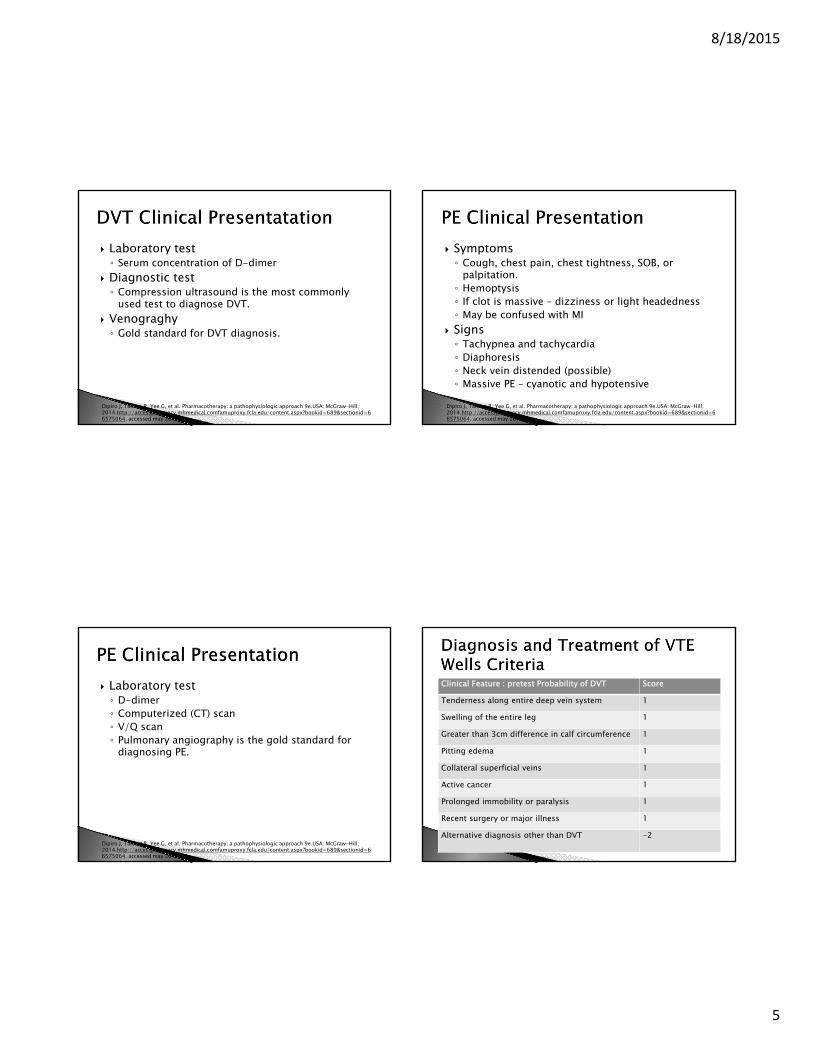
Laboratory test◦ Serum concentration of D-dimer
Diagnostic test◦ Compression ultrasound is the most commonly
used test to diagnose DVT. Venograghy◦ Gold standard for DVT diagnosis.
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
Symptoms◦ Cough, chest pain, chest tightness, SOB, or
palpitation.◦ Hemoptysis◦ If clot is massive – dizziness or light headedness◦ May be confused with MI
Signs◦ Tachypnea and tachycardia◦ Diaphoresis◦ Neck vein distended (possible)◦ Massive PE – cyanotic and hypotensive
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
Laboratory test◦ D-dimer◦ Computerized (CT) scan◦ V/Q scan◦ Pulmonary angiography is the gold standard for
diagnosing PE.
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
Clinical Feature : pretest Probability of DVT Score
Tenderness along entire deep vein system 1
Swelling of the entire leg 1
Greater than 3cm difference in calf circumference 1
Pitting edema 1
Collateral superficial veins 1
Active cancer 1
Prolonged immobility or paralysis 1
Recent surgery or major illness 1
Alternative diagnosis other than DVT -2

8/18/2015
6
High—3 or greater (75% risk of DVT)
Moderate—1 or 2 (20% risk of DVT)
Low—0 (3% risk of DVT)
Clinical Feature: Pretest Probability of PE score
Clinical evidence of DVT 3
Other Dx less likely than PE 3
Heart rate > 100 1.5
Immobility > 3 day or major surgery within 4 weeks 1.5
Previous DVT/PE 1.5
Hemoptysis 1
Malignancy 1
Dipiro J, Talbert R, Yee G, et al. Pharmacotherapy: a pathophysiologic approach 9e.USA: McGraw-Hill; 2014.http://accesspharmacy.mhmedical.comfamuproxy.fcla.edu/content.aspx?bookid=689§ionid=66575064. accessed may 2015
High—6 or greater (>70% risk of PE)
Moderate—2–6 (20–30% risk of PE)
Low—less than 2 (2–3% risk of PE)
Compression stockings Intermittent pneumatic compression (IPC) IVC filters ambulation

8/18/2015
7
The acute phase of VTE (7 days) requires rapid anticoagulation to prevent thrombus extension and embolization.
Early maintenance phase (7days to 3 months) is aimed to reduce the risk of long-term sequalae
Holbrook A, Schulman S, Witt D, et al. Evidence based management of anticoagulant therapy: antithrombictherapy and prevention of thrombosis . Chest 2012; 141 (2 supp): e184s. Accessed may 2015
FDA Approvals
Dabigatran Rivaroxaban Apixaban Edoxaban
VTE prophylaxis
No Yes Yes No
VTE treatment
Yes Yes Yes Yes
trials

8/18/2015
8
PharmacokineticsDabigatran Rivaroxaban Epixaban Edoxaban
Target Thrombin FXa FXa FXa
Peak effect (h)
2-3 3-4 3-4 1-2
Half-life (h) 12-17 5-13 8-15 10-14
Dosing Bid Qd Bid Qd
Clearance 80% renal20% biliary
66% renal33% biliary
25% renal75% biliary
50% renal50% bile/ intestinal
Dabigatran◦ Treatment: 150mg po bid after 5-10 days of
parental anticoagulation. CrCl > 30ml/min◦ Reduction of risk of recurrence: 150mg po bid after
previous treatment. CrCl > 30ml/min.◦ CrCl <30ml/min or on dialysis dosing
recommendations cannot be provided.◦ CrCl <50ml/min with concomitant us of P-gp
inhibitors. Avoid concomitant use.
Pradaxa [package insert].Ridgefield,CT: Boehringer, Ingelheim Pharmaceutical Inc; 2015
Dabigatran Swallow capsule whole and take with full
glass of water. If dose is not taken on time, take as soon as
possible on same day or skip dose if it cannot be taken at least 6hrs before the next dose.
DO NOT DOUBLE UP
Pradaxa [package insert].Ridgefield,CT: Boehringer, Ingelheim Pharmaceutical Inc; 2015
Dabigatran Converting from warfarin◦ d/c warfarin and start Pradaxa when INR <2
Converting to warfarin◦ CrCl > 50, start warfarin 3 days before d/c dabigatran◦ CrCl 30-50, start warfarin 2 days before d/c
dabigatran◦ CrCl 15-30, start warfarin 1 day before d/c
dabigatran◦ CrCl < 15 no recommendation can be made.
Pradaxa [package insert].Ridgefield,CT: Boehringer, Ingelheim Pharmaceutical Inc; 2015

8/18/2015
9
Dabigatran Converting from parentals◦ Start dabigatran 0-2 hrs before the time that the
next parental drug was to have been administered or at the time parental is d/c
Converting to parentals◦ Wait 12 hrs (CrCl >30) or 24hrs (CrCl <30) after the
last dose of dabigatran before initiating parental anticoagulant.
Pradaxa [package insert].Ridgefield,CT: Boehringer, Ingelheim Pharmaceutical Inc; 2015
Dabigatran Discontinuation for surgery◦ d/c dabigatran 1-2 days (CrCl >50) or 3-5 days
(CrCl <50) before surgery. ◦ Consider longer times for pt undergoing major
surgery, spinal puncture, epidural catheter, or port
Pradaxa [package insert].Ridgefield,CT: Boehringer, Ingelheim Pharmaceutical Inc; 2015
Rivaxoban◦ Treatment DVT/PE and reduction in recurrence:
15mg po bid with food for the first 21 days, then 20mg po qd with food for the remaining.◦ Prophylaxis of DVT following Hip or Knee surgery:
10mg po qd with or without food ◦ CrCl < 15 avoid use ◦ Hepatic impairment (Child-Pugh B and C) avoid use◦ Avoid concomitant use with P-gp and strong
CYP3A4 inhibitors
Xarelto [package Insert]. Titusville, NJ: Jannsen Pharmaceuticals;2011
Rivoraxaban◦ Food considerations – 15mg and 20mg tablets
should be taken with food while the 10mg can be take with or without food.◦ Tablets may be crushed and mixed applesauce
immediately prior to use. Stable is water or applesauce for up to 4 hrs◦ Tablets can be given via NG tube or gastric feeding
tube
Xarelto [package Insert]. Titusville, NJ: Jannsen Pharmaceuticals;2011

8/18/2015
10
Rivaroxaban Converting from warfarin◦ d/c warfarin and start rivaroxaban when INR<3
Converting to warfarin◦ No clinical trial data available. Recommended to d/c
rivaroxaban and begin both a parental and warfarin at the time the next dose is do.
Xarelto [package Insert]. Titusville, NJ: Jannsen Pharmaceuticals;2011
Rivaroxaban Converting to other anticoagulants◦ d/c rivaroxaban and give 1st dose of other drug at
time of next dose of rivaroxaban would have been taken.
Converting from other anticoagulant ◦ Start 0-2 hrs prior to next scheduled evening
administration of the drug and d/c the administration of the other anticoagulant.
Xarelto [package Insert]. Titusville, NJ: Jannsen Pharmaceuticals;2011
Rivaroxaban Discontinuation for Surgery◦ Stop 24hrs before procedure to reduce the risk of
bleeding. Restart after surgery as soon as hemostasis has been established.
Xarelto [package Insert]. Titusville, NJ: Jannsen Pharmaceuticals;2011
Apibaxan Treatment of DVT/PE: 10mg bid for 7 days
followed by 5mg bid. Reduction in the risk of recurrent DVT and PE:
2.5mg po bid Prophylaxis of DVT after hip/knee
replacement: 2.5mg bid Hepatic: no dose adjustments Renal: adjustment are not required for this
indications
Eliquis [package Insert]. Princeton, New Jersey: Bristol-Myers Squibb; 2014

8/18/2015
11
Apixaban Administration considerations◦ 5mg and 2.5mg may be crushed and suspended in
60ml D5W and immediately given through NG tube
Eliquis [package Insert]. Princeton, New Jersey: Bristol-Myers Squibb; 2014
Apixaban Converting from warfarin◦ d/c warfarin and start apixaban when INR<2
Converting to warfarin◦ d/c apixaban and start warfarin and parental
anticoagulant at the same time the next dose of apixaban would have been taken. d/c parental when INR > 2
Converting between apixaban and other anticoagulants.◦ d/c one and begin taking at time of next scheduled.
Apixaban Surgery considerations◦ Apixaban should be d/c at least 48 hrs prior to
surgery with a moderate or high risk of unacceptable bleeding.◦ Apixaban can be d/c at least 24hrs prior to low risk
surgery.◦ Bridging coagulation between during the 24-48hrs
after stopping is not required.◦ Restart after surgery.
Eliquis [package Insert]. Princeton, New Jersey: Bristol-Myers Squibb; 2014
Edoxaban Treatment of DVT/PE: 60mg qd Not indicated for prophylaxis CrCl 15-50ml/min or body weight less than
or equal 60kg or who use certain P-gp, recommended dose is 30mg qd
Renal: not recommended in CrCl <15 Hepatic: not recommened in moderate to
severe impairment (Child-Pugh B and C). No dose reduction needed in mild (A).
Sayvasa [package Insert]. Tokyo, Japan: Daiichi Sankyo Company: 2015

8/18/2015
12
Edoxaban Administration Considerations Take without regard to food If dose is missed take as soon as possible on
the same day. Dosing should resume as normal the next day.
Do not double up.
Sayvasa [package Insert]. Tokyo, Japan: Daiichi Sankyo Company: 2015
Edoxaban Converting to Edoxaban
From Recommendation
warfarin d/c warfarin and start edoxaban when INR<2.5
Other anticoagulants d/c current anticoagulant and start edoxabanat the next scheduled dose of other
LMWH d/c LMWH and start Edoxaban at the time of next scheduled administration of LMWH
UFH d/c the infusion and start edoxaban 4 hours later
Sayvasa [package Insert]. Tokyo, Japan: Daiichi Sankyo Company: 2015
Edoxaban Converting from Edoxaban
From Recommendation
edoxaban If taking 60mg reduce to 30mg and begin warfarin. If taking 30mg reduce to 15mg and begin warfarin. d/c edoxaban once INR > 2
edoxaban Parenteral option: d/c edoxaban and administer a parental anticoagulant and warfarin at the time of the next scheduled dose. Once INR > 2 d/c parental anticoagulant and continue warfarin
edoxaban D/c edoxaban and start the anticoagulant at the time of the next dose of edoxaban
edoxaban d/c edoxaban and start the parental anticoagulant at the time of the next dose of edoxaban
Surgery◦ Discontinue edoxaban at least 24 hours before
invasive or surgical procedure. ◦ Restart after the surgery as soon as adequate
hemostasis has been established◦ Pharmcodynamic effect time of onset is 1-2 hours. ◦ Administer a parental anticoagulant and then switch
to edoxaban.
Sayvasa [package Insert]. Tokyo, Japan: Daiichi Sankyo Company: 2015

8/18/2015
13
Risk Factors for Major Bleeding While Taking Anticoagulation Therapy◦ Anticoagulation intensity◦ Initiation of therapy (1st few days and weeks)◦ Unstable anticoagulation response◦ Age >65◦ Concurrent antiplatelet therapy◦ Concurrent NSAIDs use◦ history of GI Bleeding
Risk Factors for Major Bleeding While Taking Anticoagulation Therapy◦ Recent surgery or trauma◦ High risk for fall/trauma◦ Heavy alcohol use◦ Renal failure◦ Cerebrovascular disease◦ Malignancy
Fresh Frozen Plasma (FFP) Obtained from human blood and contains all
the clotting factors found in plasma Dosing is based on pt weight. Each unit of
FFP contains 200-250mls
Clotting Factor Concentrates Contain one or more clotting factors Four major types of products◦ rFVIIa◦ Three factor PCC which contains II,IX,X (inactivated)◦ Four factor PCC which contains II,IX,X and VII
(inactivated)◦ Activated PCC contains VII (activated) and II,IX and X
(inactivated) There is no specific reversal for NOACs

8/18/2015
14
Antidote neutralizing agents◦ Aripazine Synthetic small molecule with broad activity against
heparin, LMWH, and NOACs◦ Andexanet Modified FXa direct reversal agent used against the
FXA inhibitor medications◦ Idarucizumab◦ Humanized antibody fragment directed against
dabigatran
FL Medicaid FL medicaid drug formulary (April 20th 2015) http://www.fdhc.state.fl.us/medicaid/Prescri
bed_Drug/pharm_thera/pdf/PDL_2015-04-24.pdf
Pradaxa 75mg and 150mg Eliquis 2.5mg and 5mg Xarelto 10mg,15mg and 20mg
Medicare population http://www.q1medicare.com/PartD-2015-
SearchPDPMedicareDrugFinder.php

8/18/2015
15
Affordable Healthcare Act
The online marketplace will help low and middle-income Floridians qualify for ACA tax credits that will ensure that good coverage is also affordable coverage.
Exemptions to ACA
Unaffordable coverage options Low Income / no filing requirement
(automatic) Hardship exemption
Volunteers in Medicine◦ Provides primary care, preventive health education,
laboratory studies and most medications at no cost to Jacksonville uninsured patients.◦ Patients are without private or government funded
medical insurance.◦ Eligibility Annual income between $13,000-29,425 with
additional $4160 allowed for each household dependant.
One or more family members must be gainfully employed at least 20hr/wk and live or work in Duval County
Volunteers in medicine website◦ http://vim-jax.org/patients/

8/18/2015
16
GoodRx website◦ Collect and compare Prices◦ Find free coupons◦ Shows the lowest price at each pharmacy near you
www.goodrx.com
Manufacturer coupon◦ https://www.pradaxa.com/savings
Manufacturer assistance program◦ http://us.boehringer-
ingelheim.com/our_responsibility/patients-families.html
Manufacturer Coupon◦ http://www.xareltocarepath.com/reducing-stroke-
risk/xarelto-savings-programs
Manufacturer Patient Assistance◦ http://www.jjpaf.org/index.html
Manufacturer Coupon◦ https://www.eliquis.com/eliquis/eliquis-360
Manufacturer Patient Assistance◦ http://www.bmspaf.org/Pages/Home.aspx

8/18/2015
17
1. What is the brand of Edoxaban? Savaysa2.Which NOAC is not a FXa inhibitor?
Dabigatran3. Which NOAC (s) can not be used
prophylactically for VTE? Dabigatran and Edoxaban
4. Which NOAC is 25% renally cleared and doesn’t require adjustment? Eliquis
5. Do to product breakdown from moisture and loss of potency, the FDA has issued a safety announcement for this medication to be dispensed and stored in the original bottle? Pradaxa
6. According to the guidelines name the 4 non pharmacological treatments for DVT/PE?
Compression stocking, IPC, IVC filters, ambulation
7. Upon vascular injury, these are the first to be activated and respond to the area of need?
Platelets
8. Which factor(s) is part of the extrinsic pathway and thus use (PT) for measurement?
Factor VII

8/18/2015
18
9. What is the name of FIIa and is considered a significant part of the cascade because of its feedback mechanism? Thrombin
10.Your have 5 secs to name all the components of Virchow’s Triad?Stasis vessel, wall injury, hypercoagulability
11. In the clotting cascade, where does the extrinsic and intrinsic meet? FX
12. Which factors make up the common pathway? FX,FV,FII and FI
13. How should Pradaxa be given? Swallow whole and take with a full glass of water
14. Is Edoxaban taken with food?It is taken without regard to food
15. Xeralto can be given via NG tube or gastric feeding tube. Name the two things it can be crushed and mixed in? also how long is it stable for once mixed?
Water and applesauce for up to 4 hrs
16. Rivaroxaban come in 10mg, 15mg and 20mg tabs. Are they taken with or without food?
10mg is with or without15mg and 20mg should be taken with food
17. If a patient misses their morning dose of Dabigatran at 8AM ? Can they take that missed dose at 11am and continue with their evening scheduled dose at 8PM?
Yes. A pt can take as soon as possible on same day or skip dose if it can not be taken at least
6hrs before next dose. Do not double up

8/18/2015
19
Eliquis 2.5mg and 5mg maybe crushed and suspended in how mls of (x) and given per NG tube? 60mls of D5W
Any Questions?





























