Embed Size (px)
Citation preview
ulster.ac.uk
Living and coping with head and
neck cancer – implications for
practice
Dr Cherith SempleReader in Clinical Cancer Nursing
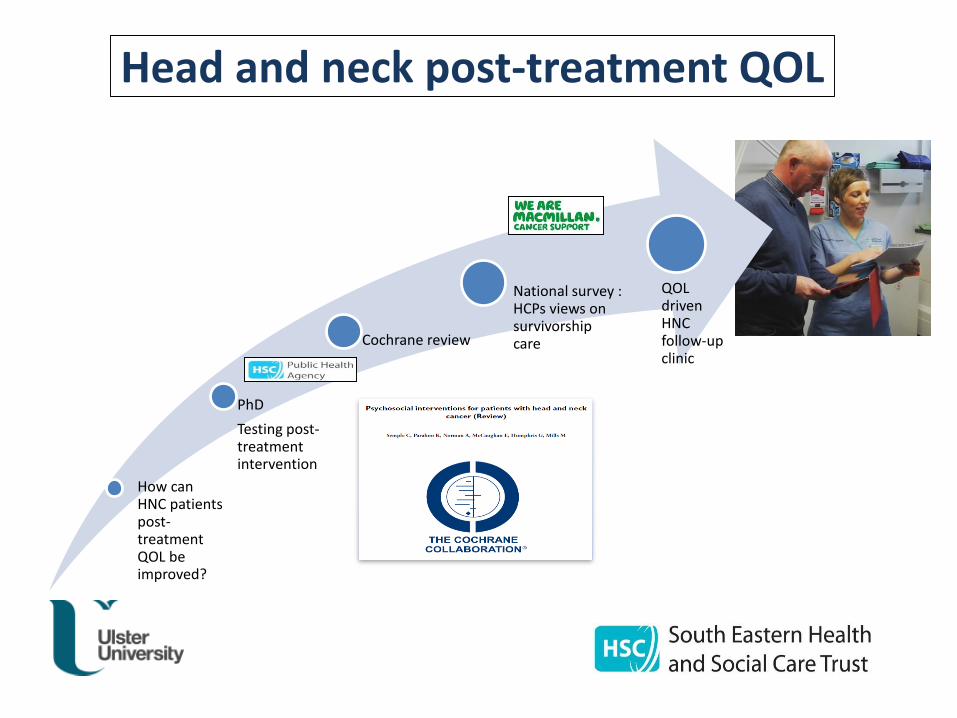
Partnership postCurrent programmes of work
Clinical questions
Robustresearch
Impact on CARE
delivery
Show me the evidence
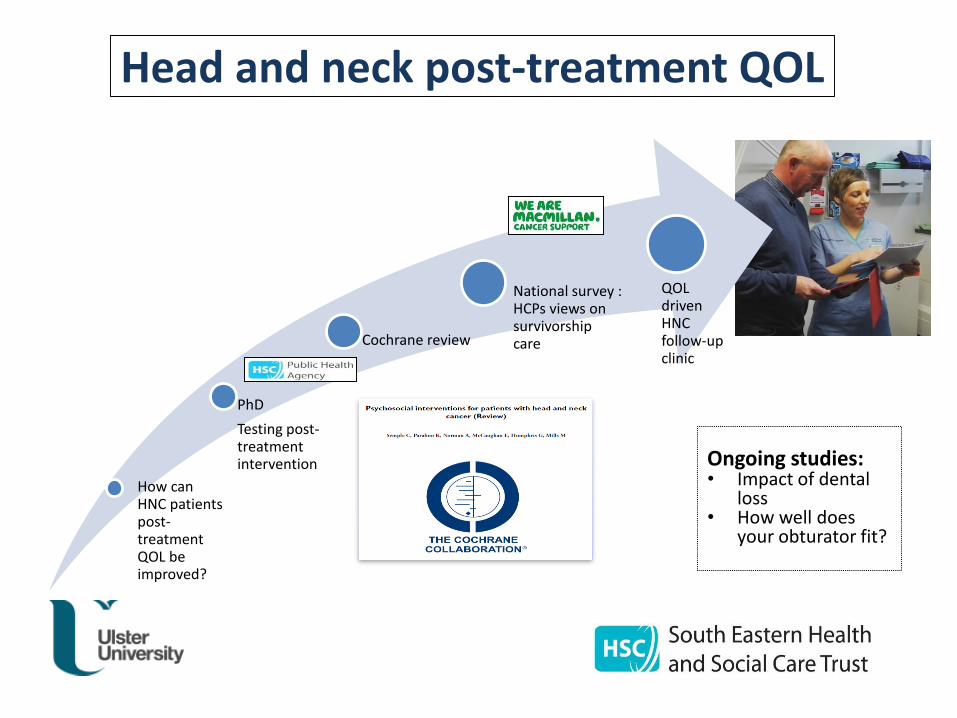
How can HNC patients post-treatment QOL be improved?
PhD
Testing post-treatment intervention
Cochrane review
National survey : HCPs views on survivorship care
QOL driven HNC follow-up clinic
Head and neck post-treatment QOL
Ongoing studies:• Impact of dental
loss• How well does
your obturator fit?
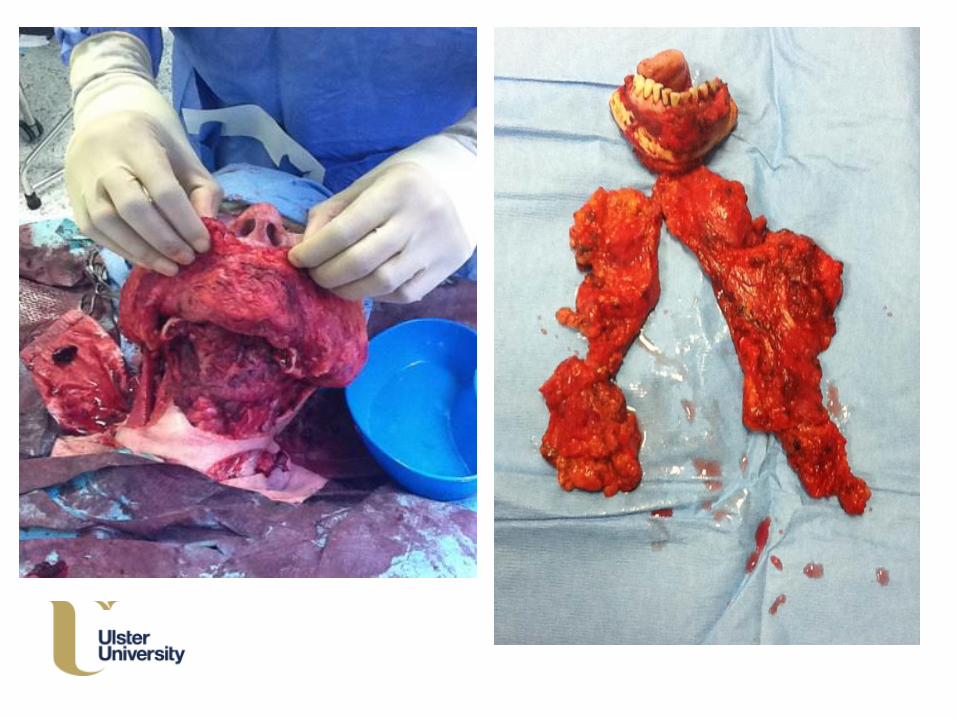
BACKGROUND: Patient’s journey

Primary unique
challenges of
H&NC
Location –
‘it’s in your face’
Function –
‘it affects what I eat
and how I speak’
Despite an impressive list of advancements in
medicine we cannot forget the other important
needs of patients, in particular emotional well-
being (Fallowfield, 1990)
Must consider quality of
life as well as quantity of life
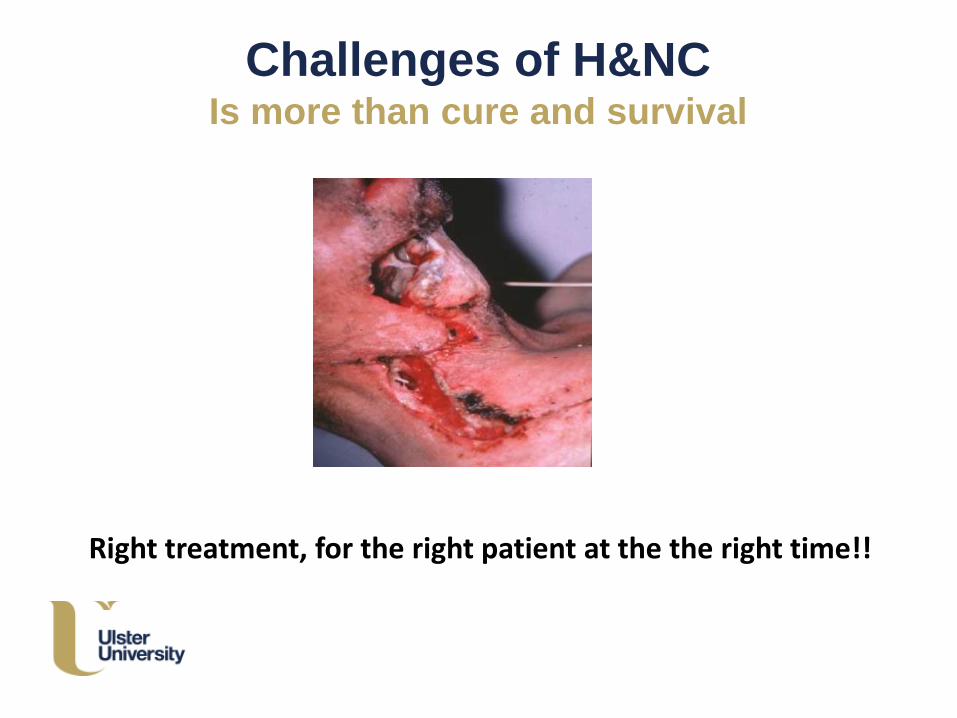
Challenges of H&NCIs more than cure and survival
Right treatment, for the right patient at the the right time!!
World Health Organisation
Definition of QOL
‘individuals perception of their position
in life in the context of culture and
value systems in which they live
and in relation to their goals,
expectations, standards and concerns’
KEY: Get to know your patient

Patient journey
J Ad Nursing ORIGINAL RESEARCH
Changes and challenges to patients’ lifestyle patterns following
treatment for head and neck cancerCherith Jane Semple, Lynn Dunwoody, William George Kernohan, Eilis McCaughan & Kate Sullivan
Factors affecting QOL for patients with HNC
• Disfigurement
• Dysfunction of daily activities, e.g.
eating and drinking – PEG tubes
speech
• Pain
• Shoulder dysfunction
• Occupation
• Sexuality
• Depression and anxiety
• Fatigue
• Employment
Disfigurement
Enormous importance placed
on the head and neck area
People with facial
disfigurement feel
stigmatised in society
Disfigurement and adjustment –
caused by surgery or radiotherapy
• Most influential factor is not degree of disfigurement
BUT
Importance and meaning attributed to appearance
• Personality – optimism
• Cognitive processes – fear of being negatively viewed by others
• Preoperative expectations - regret
• Psychological – distress, depression, anxiety
• Social support
• Age
Implications for practiceWhile in hospital
• View the face and neck (to include oral cavity)
- begins the process of understanding how appearance has changed
- charting progress
- integrating this change into their internalised body image
• Encourage and facilitate self-care routines – shaving, brushing hair etc.
• Social interaction
Post-operatively
• Information and support
• Normalise – not to keep life on hold
• Social skills training
• Assess level of distress – may require input from psychological services
(CBT)
• Surgical interventions
Eating and swallowing difficulties
Causes:
• Mucosal and soft tissue loss / damage
– Fibrosis
– Lymphoedema
• Trismus
• Dentition
• Mucositis
• Xerostomia
Eating & swallowing
Many patients with intraoral reconstruction require a modified diet
– - 72% of patients with cancer to their oropharynx required a modified diet
Inhibits normal socialisation – social embarrassment- 67% feelings of shame while eating- 25% would not eat out following treatment
Correlation between eating and QOL
– Trial and error– Person-centred approach – dietetic input
Long-term feeding tube – very poor predictor of QOL
Xerostomia: Physiological Impact
❖Impaired lubrication of oral tissues
❖Impaired food bolus preparation
▪Buffering capacity compromised increased risk of
dental caries
▪Oral flora become more pathogenic candidacies
▪Demineralization of teeth and tooth decay
▪Periodontal disease can accelerate
▪Poor quality of sleep
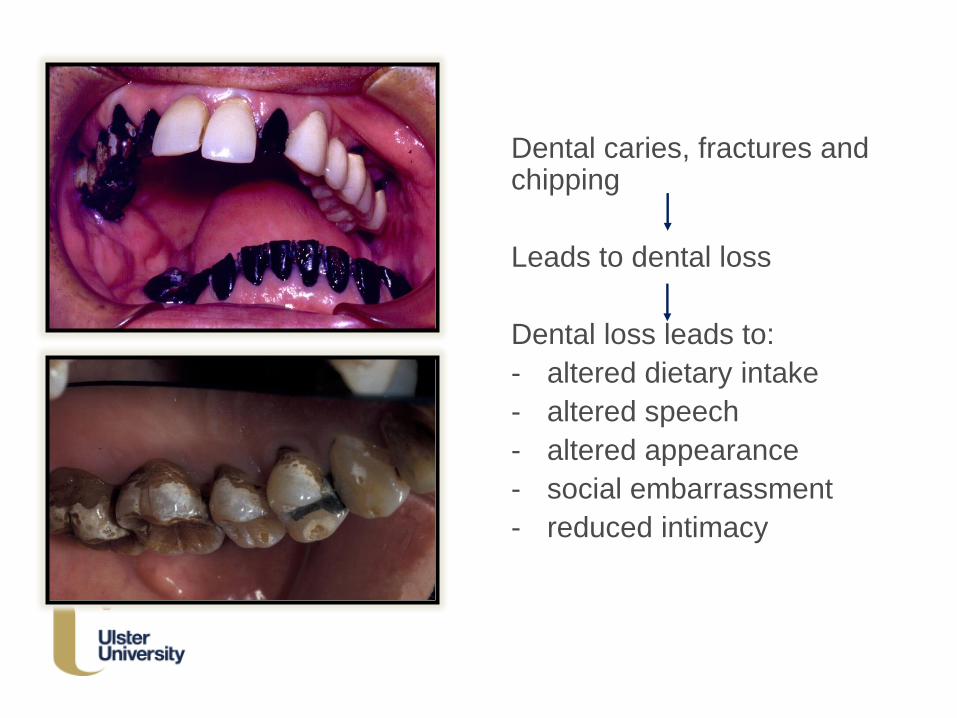
Dental caries, fractures and chipping
Leads to dental loss
Dental loss leads to:
- altered dietary intake
- altered speech
- altered appearance
- social embarrassment
- reduced intimacy
Management may include:
• More frequent visits to the dentist
• Treatment of secondary infection
• Smoking cessation advice
• Adequate hydration/lubricants
• Products with fluoride
• Stimulants: chewing gum/sugar free sweets
• Humidification during sleep
Sexual functioning
Sexual dysfunction is common in patients with head and neck cancer – prevalence 33 - 50%
Due to
- altered appearance
- dry mouth (xerostomia)- coughing and mucus - fear of failure- unwilling partner - fatigue- pain
- HPV
LIMITED evidence:– some pointing to psycho-educational interventions targeting patients along with their partners - element of sexual counselling or therapy
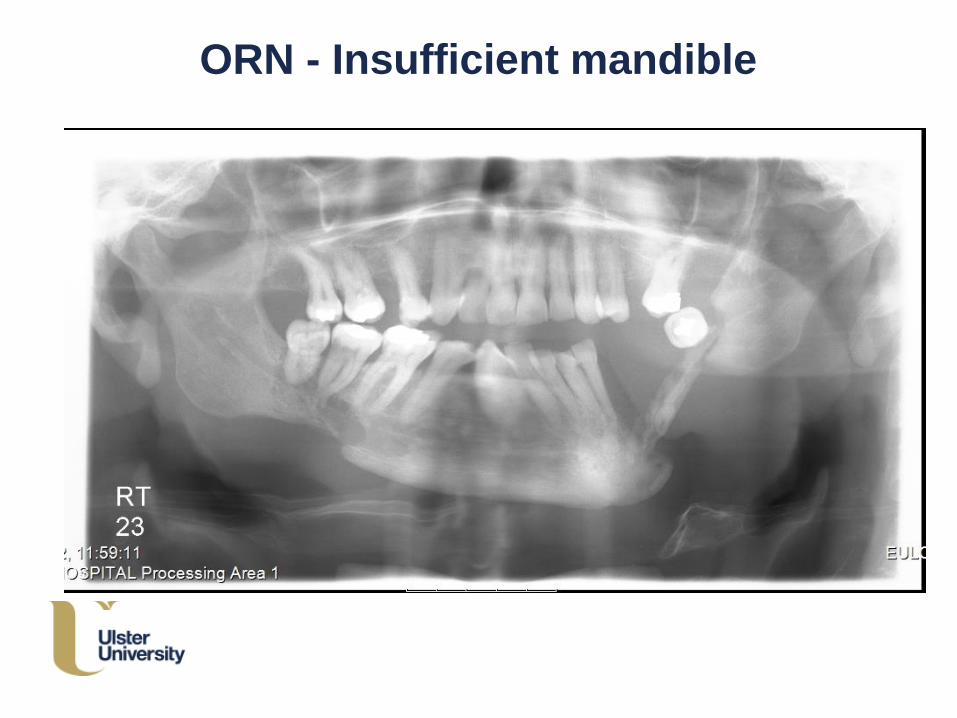
ORN - Insufficient mandible
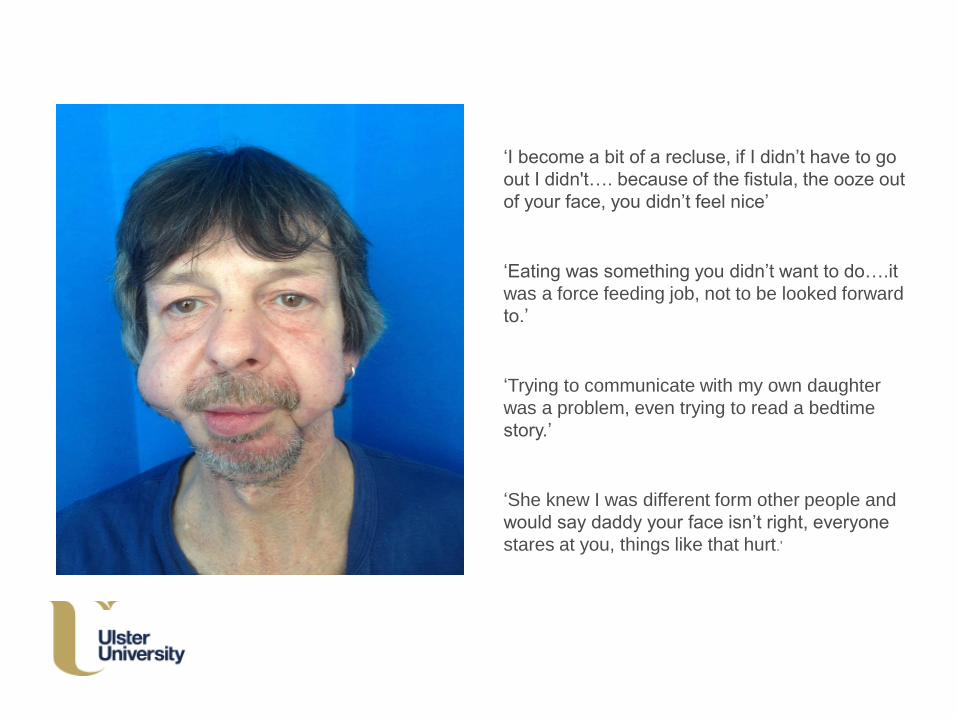
‘I become a bit of a recluse, if I didn’t have to go
out I didn't…. because of the fistula, the ooze out
of your face, you didn’t feel nice’
‘Eating was something you didn’t want to do….it
was a force feeding job, not to be looked forward
to.’
‘Trying to communicate with my own daughter
was a problem, even trying to read a bedtime
story.’
‘She knew I was different form other people and
would say daddy your face isn’t right, everyone
stares at you, things like that hurt.’
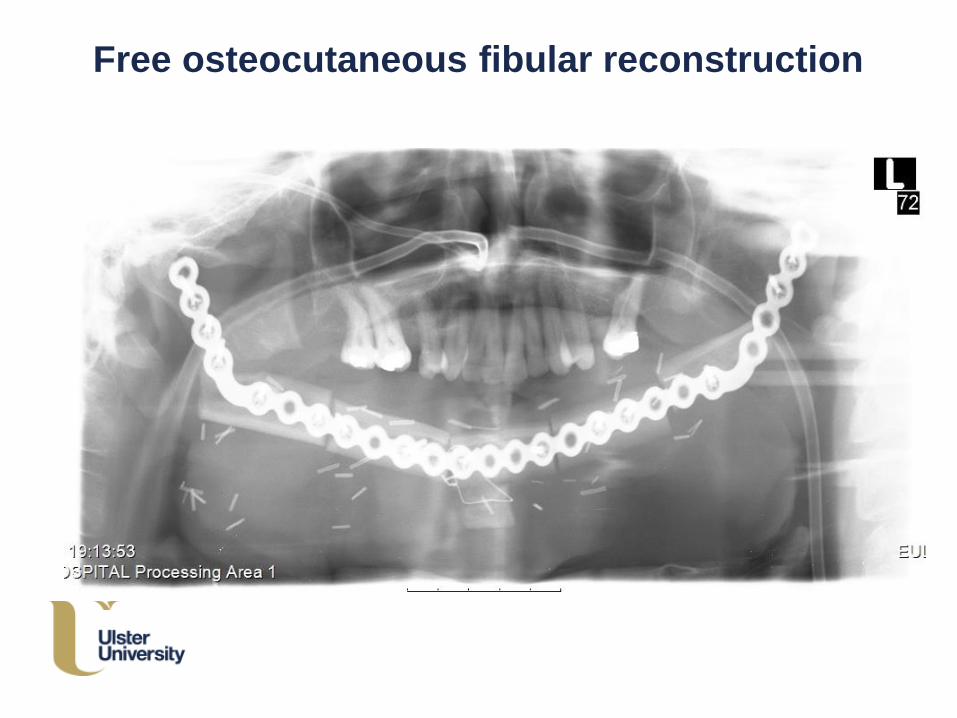
Free osteocutaneous fibular reconstruction
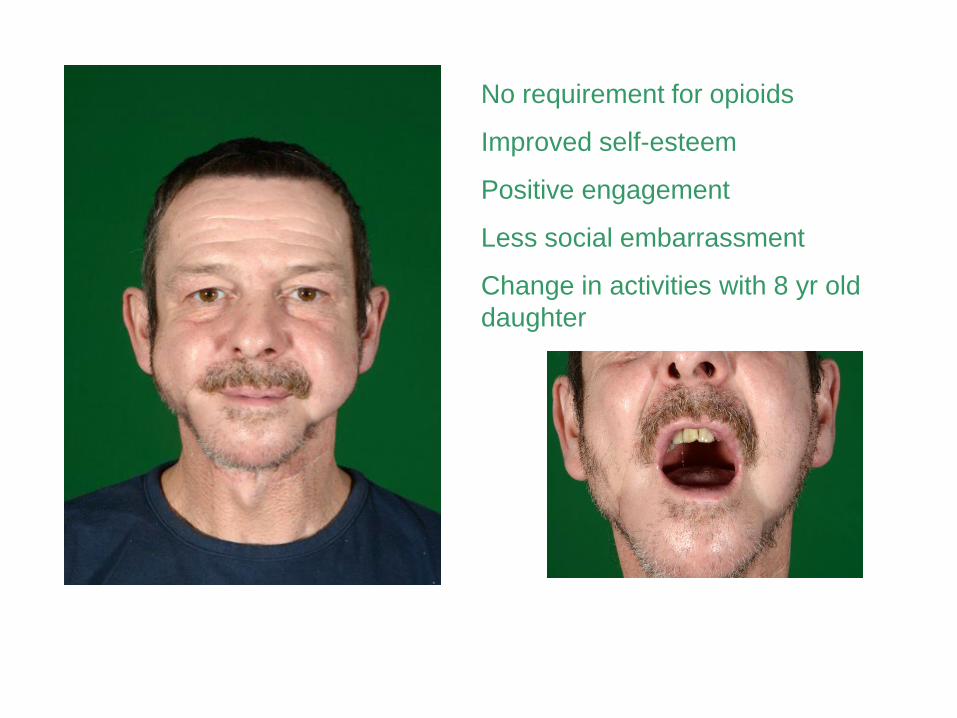
No requirement for opioids
Improved self-esteem
Positive engagement
Less social embarrassment
Change in activities with 8 yr old
daughter
‘It has changed my
life 100%, it has made a fantastic difference, the biggest thing is no pain, eating has become a pleasure instead of a miserable experience and I’m more confident socially.’
Pain
❖ Can occur as a consequence of the disease or from the treatment
❖ Often associated with recurrence
❖ Augmented because of the vital functions within the head and neck area
❖ 48% of patients had pain at diagnosis, 25% and 26% at 6 and 12 months
❖ Higher levels of pain - associated with depression and poorer QOL
Employment issues
Returning to the usual place of work can pose some
difficulty
70% of laryngectomies were employed at time of diagnosis
compared to 34% afterwards
Other studies demonstrated that patients may need to find
alternative employment, reduce working hours
Simply doing the same will not deliver the improvements that our cancer survivors expect NOR will be affordable for the NHS
Research – routine review clinic
How can HNC patients post-treatment QOL be improved?
PhD
Testing post-treatment intervention
Cochrane review
National survey : HCPs views on survivorship care
QOL driven HNC follow-up clinic
Head and neck post-treatment QOL
During HNC follow-up care
• 74% patients had at least one unmet need (Wells et
al 2015)
• 68% unmet post-treatment needs – many
psychological in nature (Henry et al 2014)
• Range of variables that can impact an individual’s
situation
AIM
Develop a holistic surgical head and neck cancer follow-up clinic, through personalisedidentification and prioritisation of post-treatment concerns and issues, on a touchscreen computer, to promote patient empowerment and enablement
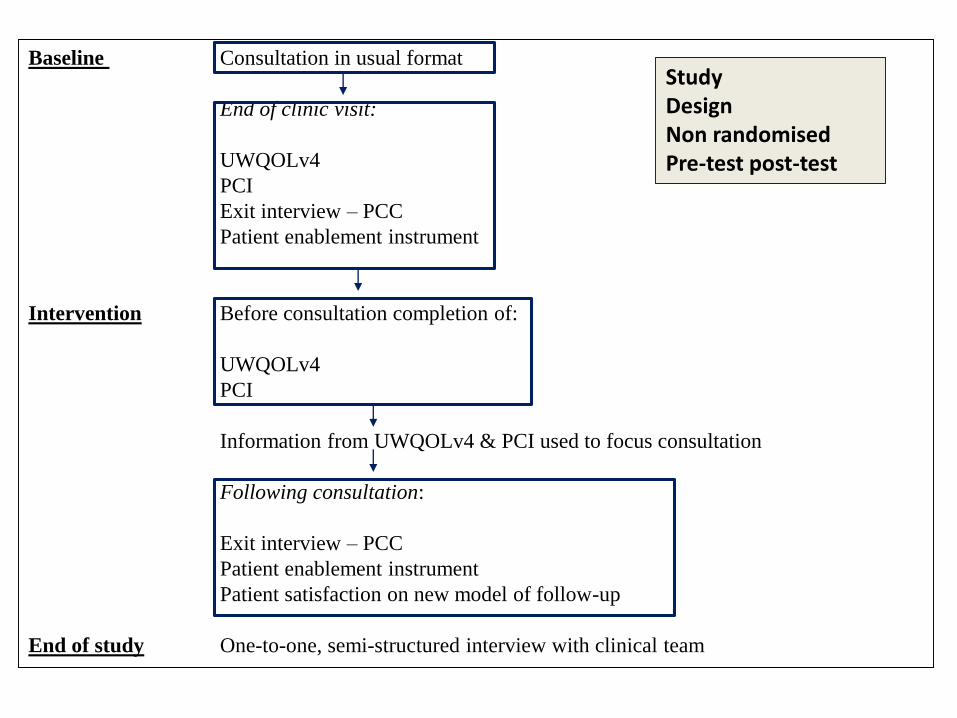
Baseline Consultation in usual format
End of clinic visit:
UWQOLv4
PCI
Exit interview – PCC
Patient enablement instrument
Intervention Before consultation completion of:
UWQOLv4
PCI
Information from UWQOLv4 & PCI used to focus consultation
Following consultation:
Exit interview – PCC
Patient enablement instrument
Patient satisfaction on new model of follow-up
End of study One-to-one, semi-structured interview with clinical team
StudyDesignNon randomisedPre-test post-test
Patient confirmation
Raymond’s storyhttps://www.youtube.com/watch?v=WotHwFWLmmA
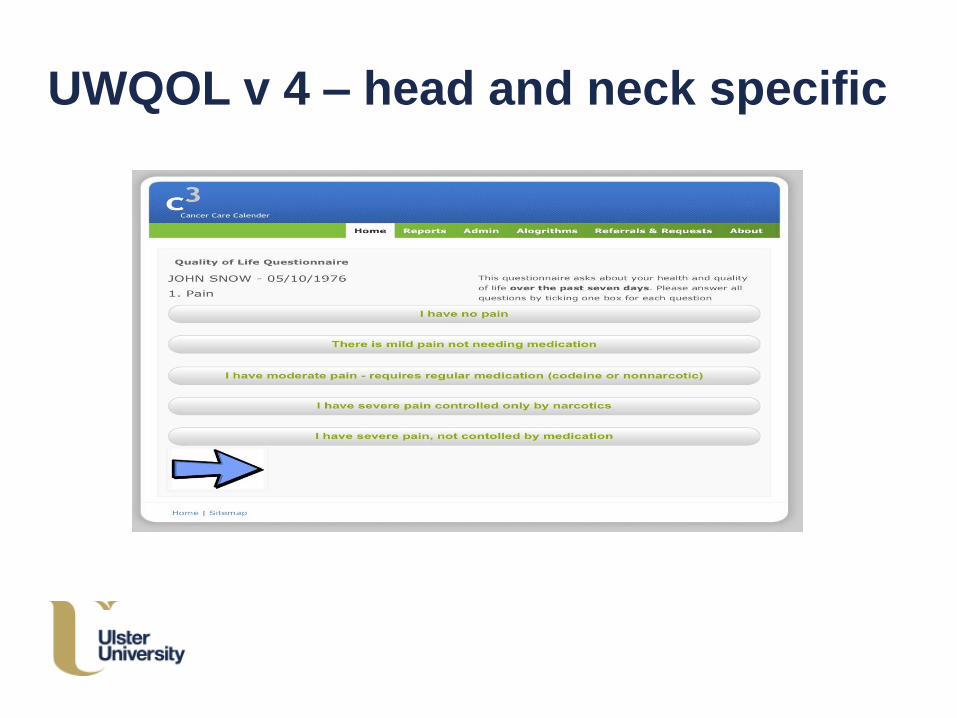
UWQOL v 4 – head and neck specific
Patient Concerns Checklist
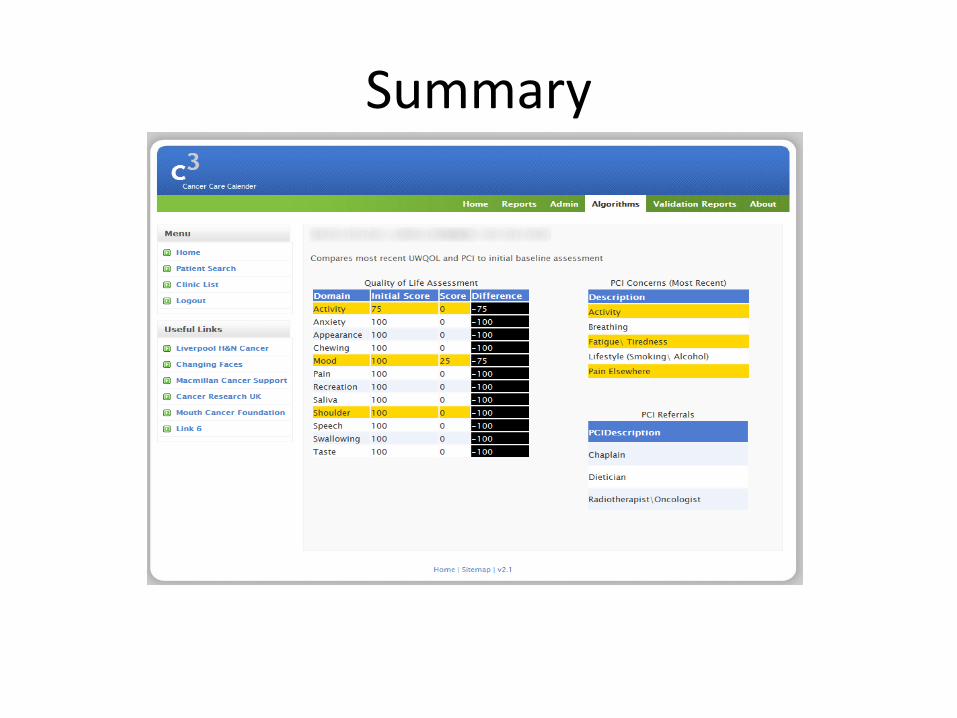
Summary
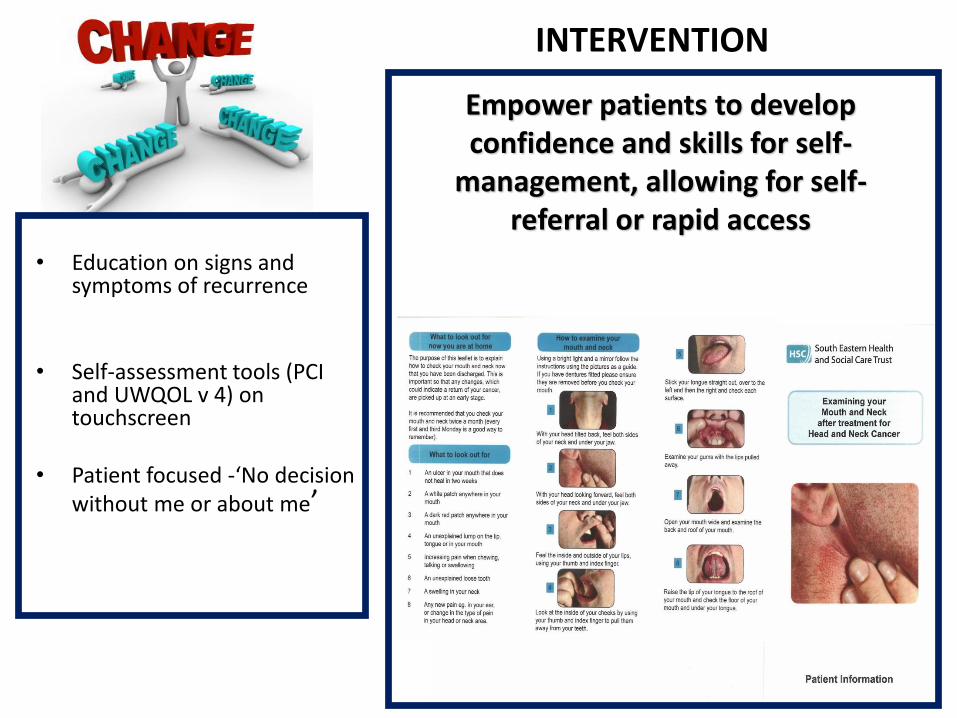
• Education on signs and symptoms of recurrence
• Self-assessment tools (PCI and UWQOL v 4) on touchscreen
• Patient focused -‘No decision without me or about me’
Empower patients to develop confidence and skills for self-
management, allowing for self-referral or rapid access
INTERVENTION
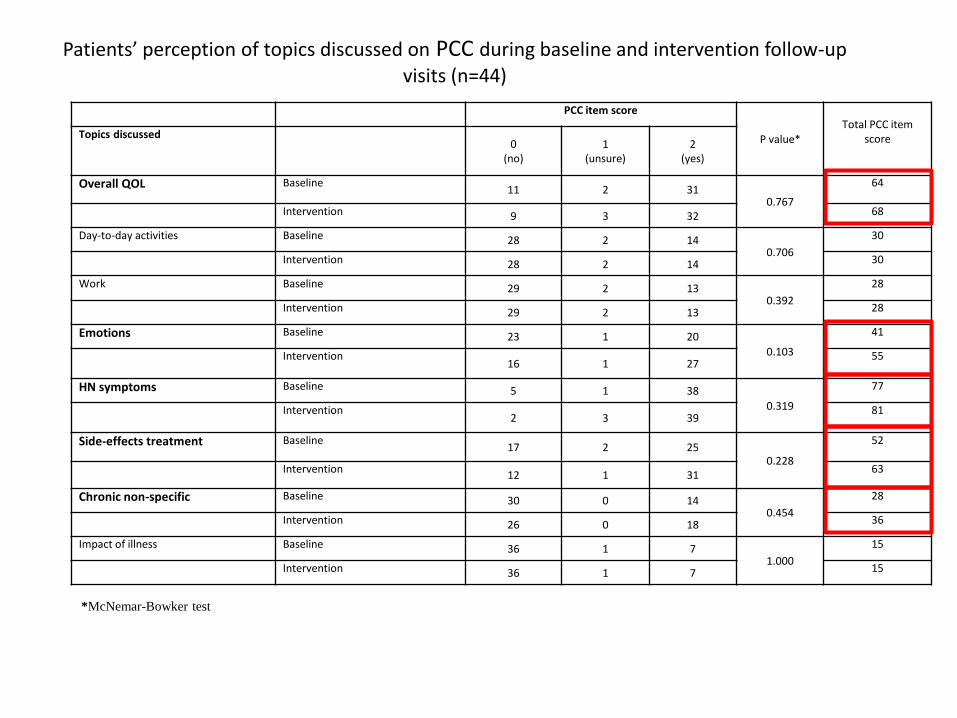
Patients’ perception of topics discussed on PCC during baseline and intervention follow-up visits (n=44)
PCC item score
P value*Total PCC item
scoreTopics discussed0
(no)1
(unsure)2
(yes)
Overall QOL Baseline11 2 31
0.767
64
Intervention 9 3 32 68
Day-to-day activities Baseline 28 2 140.706
30
Intervention 28 2 14 30
Work Baseline 29 2 130.392
28
Intervention 29 2 13 28
Emotions Baseline 23 1 20
0.103
41
Intervention16 1 27
55
HN symptoms Baseline 5 1 38
0.319
77
Intervention2 3 39
81
Side-effects treatment Baseline17 2 25
0.228
52
Intervention12 1 31
63
Chronic non-specific Baseline 30 0 140.454
28
Intervention 26 0 18 36
Impact of illness Baseline 36 1 71.000
15
Intervention 36 1 7 15
*McNemar-Bowker test
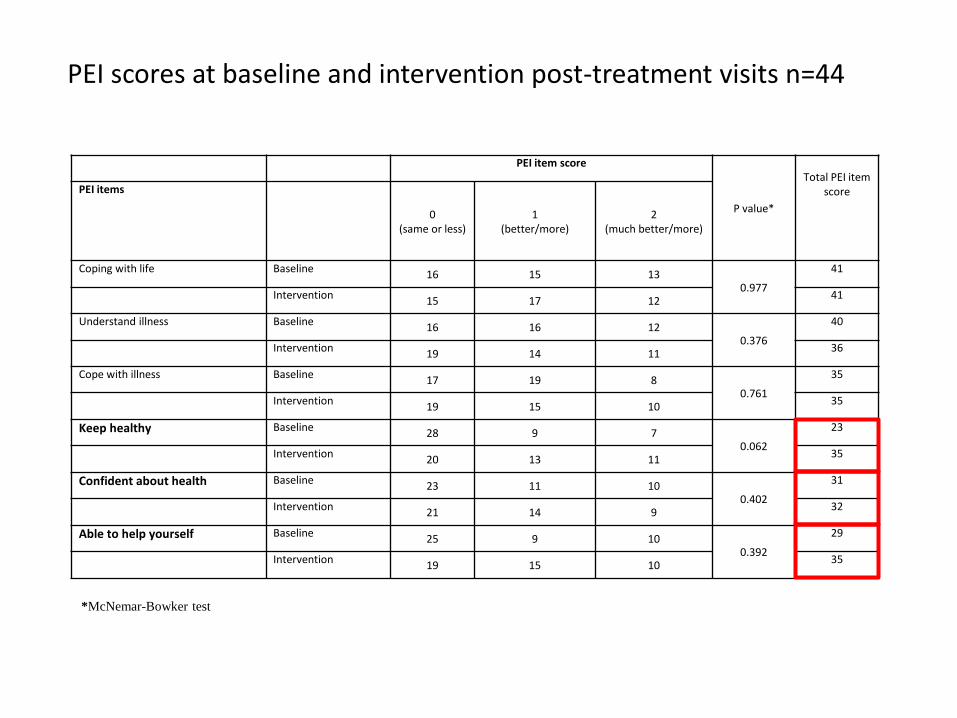
PEI scores at baseline and intervention post-treatment visits n=44
*McNemar-Bowker test
PEI item score
P value*
Total PEI item scorePEI items
0(same or less)
1(better/more)
2(much better/more)
Coping with life Baseline16 15 13
0.977
41
Intervention15 17 12
41
Understand illness Baseline16 16 12
0.376
40
Intervention19 14 11
36
Cope with illness Baseline17 19 8
0.761
35
Intervention19 15 10
35
Keep healthy Baseline28 9 7
0.062
23
Intervention20 13 11
35
Confident about health Baseline23 11 10
0.402
31
Intervention21 14 9
32
Able to help yourself Baseline25 9 10
0.392
29
Intervention19 15 10
35
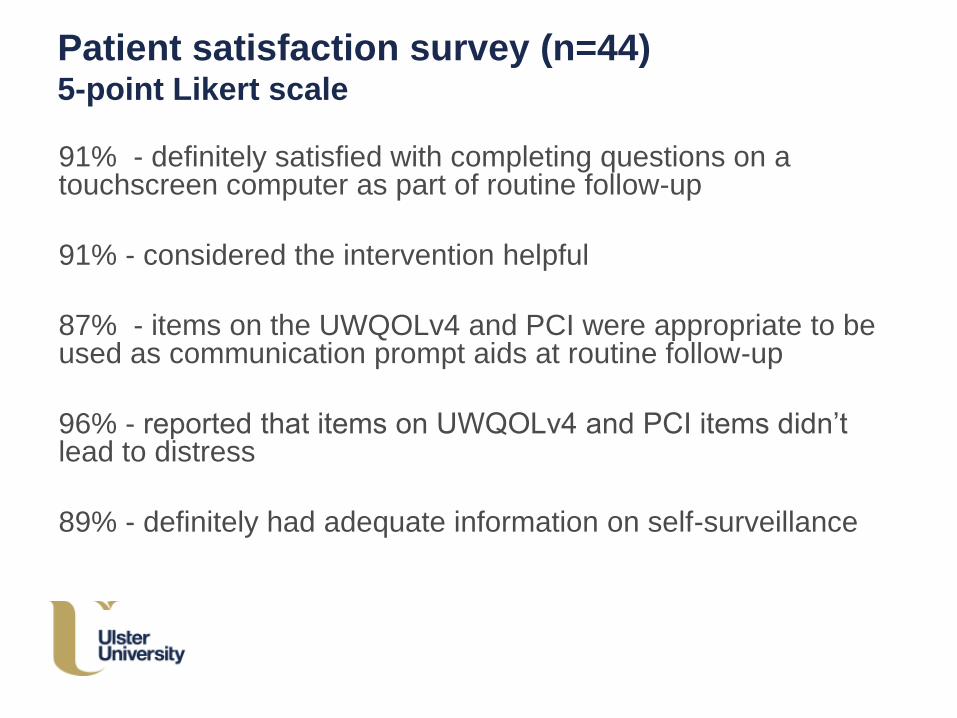
Patient satisfaction survey (n=44)5-point Likert scale
91% - definitely satisfied with completing questions on a touchscreen computer as part of routine follow-up
91% - considered the intervention helpful
87% - items on the UWQOLv4 and PCI were appropriate to be used as communication prompt aids at routine follow-up
96% - reported that items on UWQOLv4 and PCI items didn’t lead to distress
89% - definitely had adequate information on self-surveillance
Clinicians - ‘provided greater ownership and
control to patients’
• New information acquired despite the clinical team knowing the patients well
• Broader range of topics discussed during consultation
• Initiated onward referrals to members of MDT
• Accurate and consistent with the clinical assessment
• Identified patient priorities & concerns surrounding ‘what matters to them’
• Holistic approach to post-treatment management
• Promotion of self-management
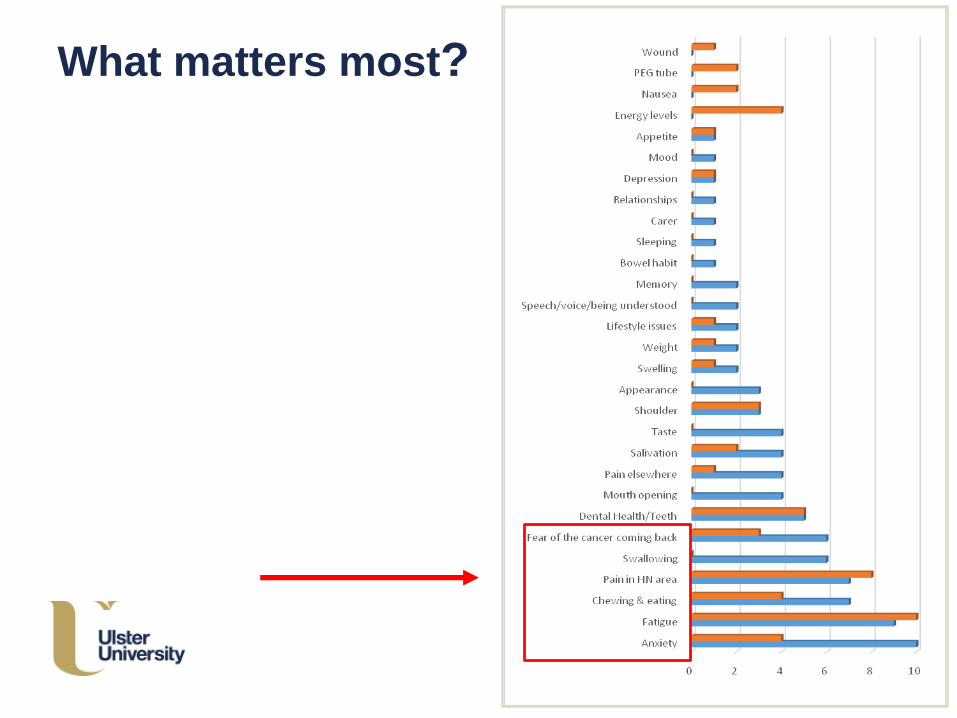
What matters most?
Key findings
QOL questionnaire and question prompt list facilitate the
identification of unmet needs
Permit timely and appropriate intervention being initiated
Feasible to use in routine clinical practice
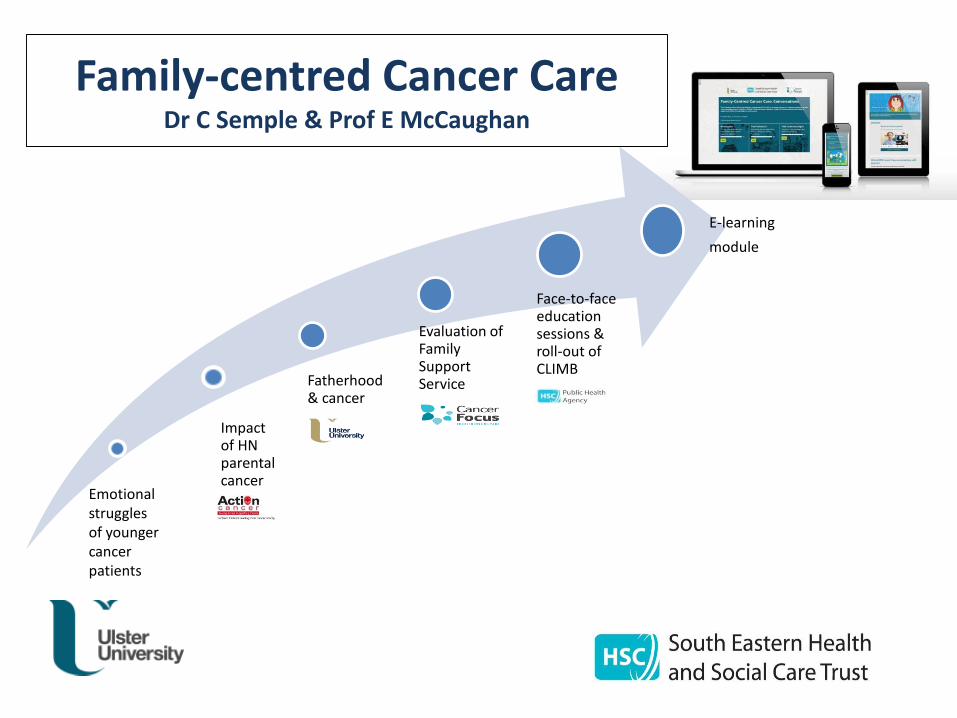
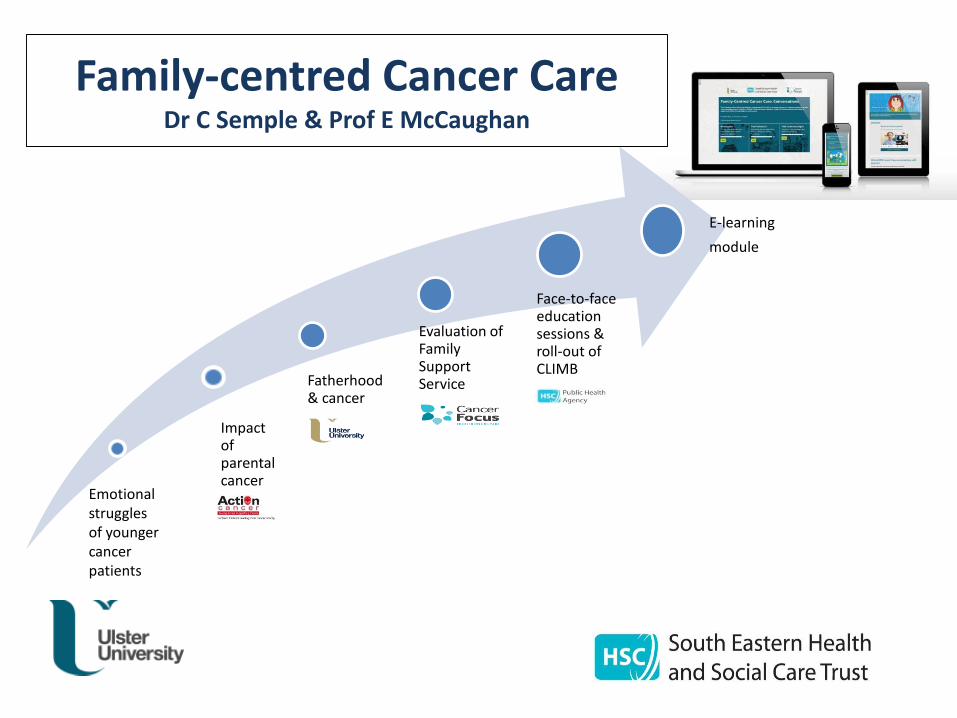
Impact of HN parental cancer
Fatherhood & cancer
Evaluation of Family Support Service
Face-to-faceeducation sessions & roll-out of CLIMB
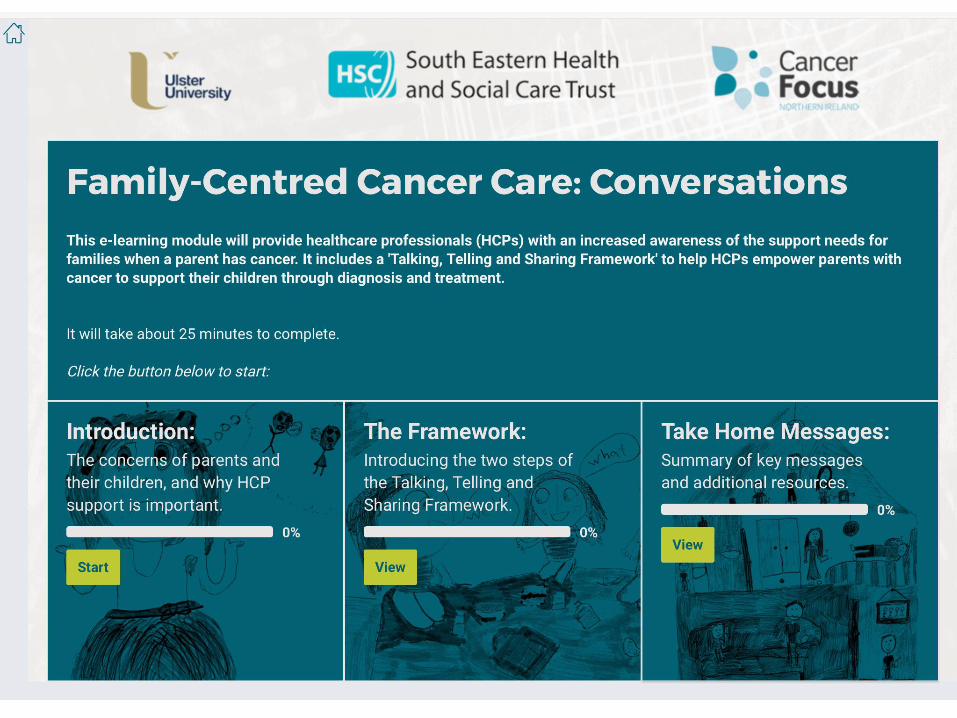
E-learning
module
Family-centred Cancer CareDr C Semple & Prof E McCaughan
Emotional struggles of younger cancer patients
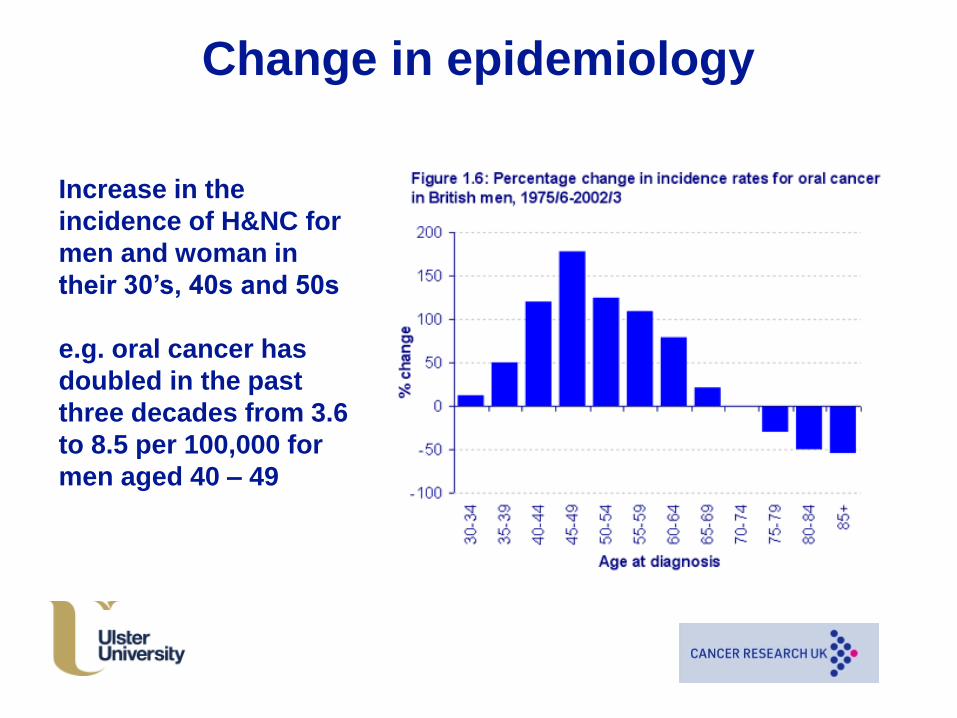
Change in epidemiology
Increase in the
incidence of H&NC for
men and woman in
their 30’s, 40s and 50s
e.g. oral cancer has
doubled in the past
three decades from 3.6
to 8.5 per 100,000 for
men aged 40 – 49
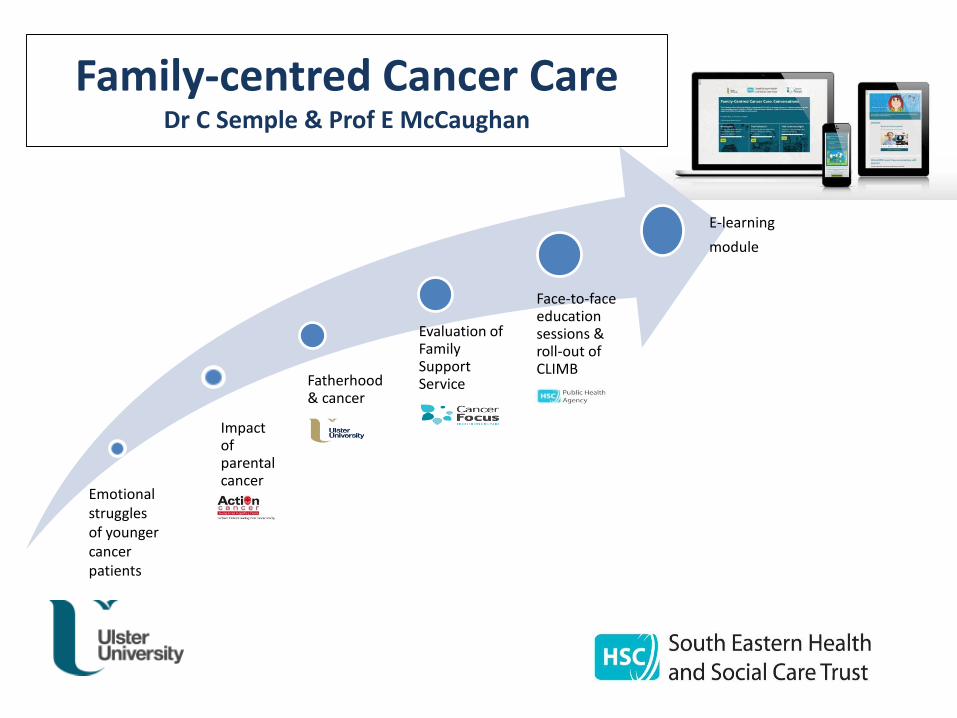
Impact of parental cancer
Fatherhood & cancer
Evaluation of Family Support Service
Face-to-faceeducation sessions & roll-out of CLIMB
E-learning
module
Family-centred Cancer CareDr C Semple & Prof E McCaughan
Emotional struggles of younger cancer patients
Experience of parents diagnosed with HNC
who are caring for young children
Dr Cherith Semple & Prof Tanya McCance
Literature review:
Keywords: ‘parent, cancer, communication, parenting’
• 13 studies focused on parents experience of cancer who have young
children
3 predominant themes
o being a good parent
o maintaining routine at home
o telling the children
• Notable gaps in the literature: studies – mainly focused on woman
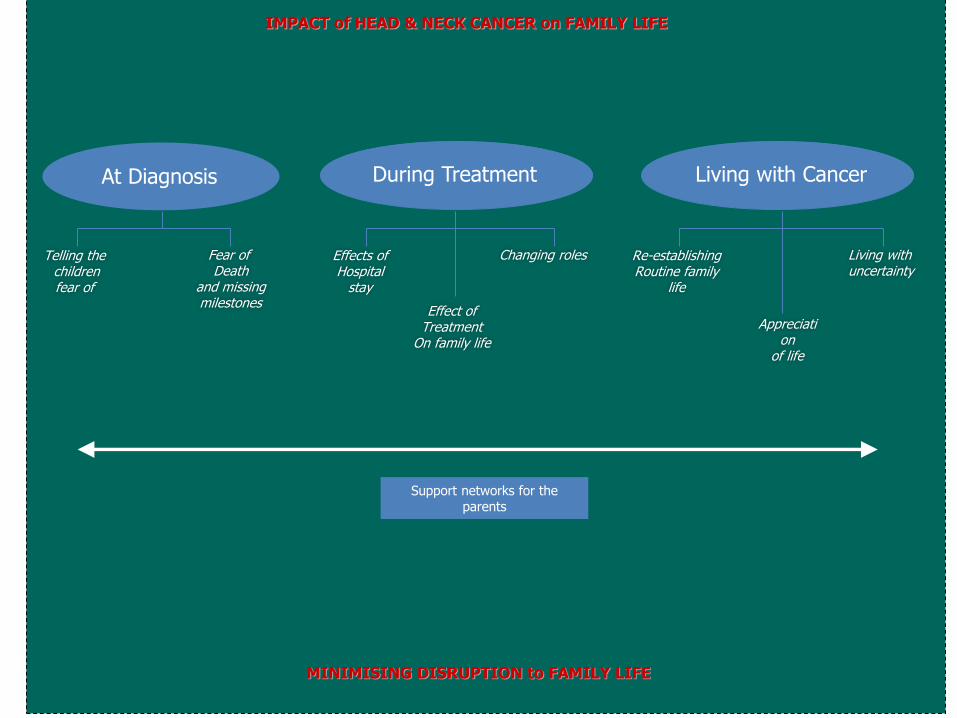
IMPACT of HEAD & NECK CANCER on FAMILY LIFE
MINIMISING DISRUPTION to FAMILY LIFE
Support networks for the parents
At Diagnosis
Telling the childrenfear of
Fear of Death
and missingmilestones
During Treatment
Effects ofHospital
stay
Effect ofTreatment
On family life
Changing roles
Living with Cancer
Re-establishingRoutine family
life
Appreciation
of life
Living withuncertainty
At diagnosis
Fear of death &
missing
milestones
‘I didn’t know what
to do, all I could
think of was death.
.. I just though my
children;
I’m never going to
see them grow up’
Fear of telling the
children
‘Well the initial feeling was
total shock, this isn’t
happening to me. Yes, yea
em it wasn’t till I was half
way through the journey
home that I was thinking
well how am I going to tell
the children’. (P1)
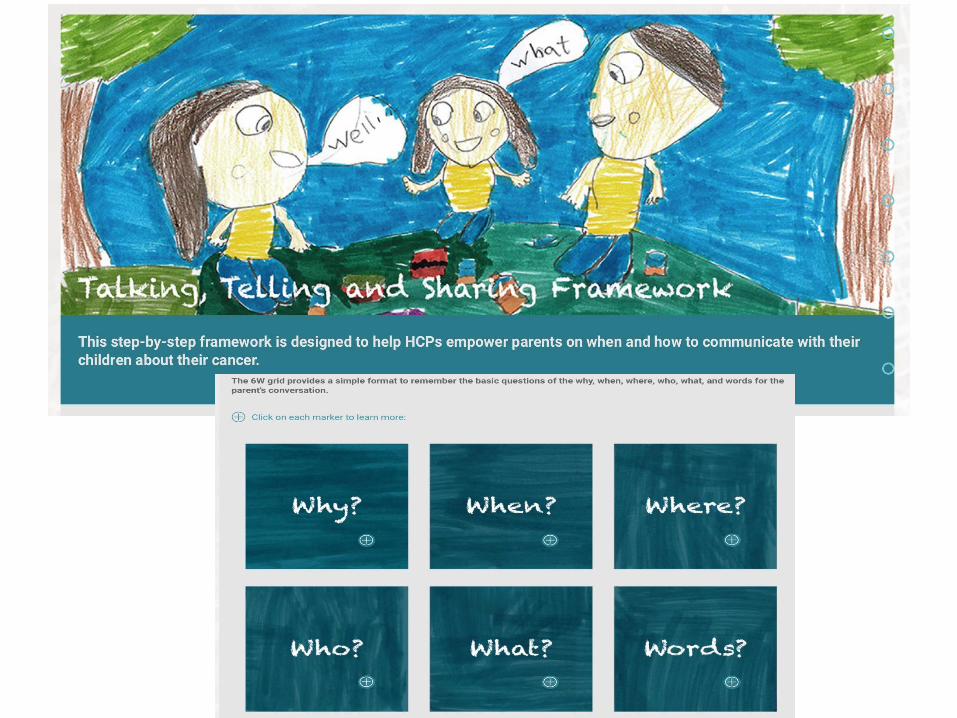
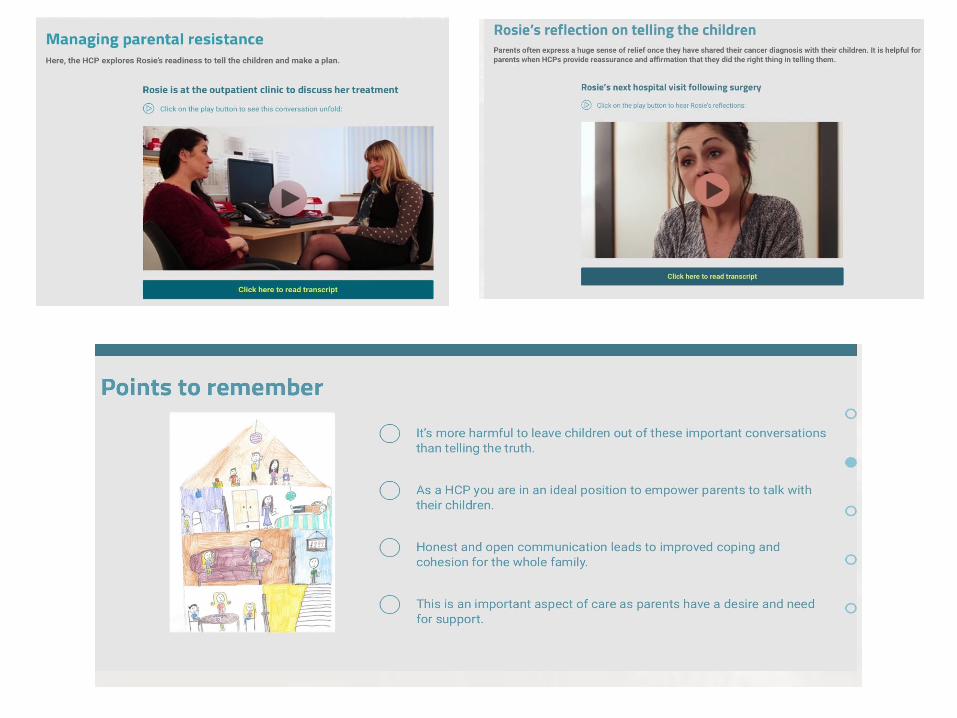
Telling the children about their HNC
CHALLENGING
Dealing with their own emotions
Guilt and concern - how their diagnosis would impact the children
Wanted to protect the children acutely aware that their children were perceptive of changes at home
hospital visitschange of emotionsvisible nature of the cancer
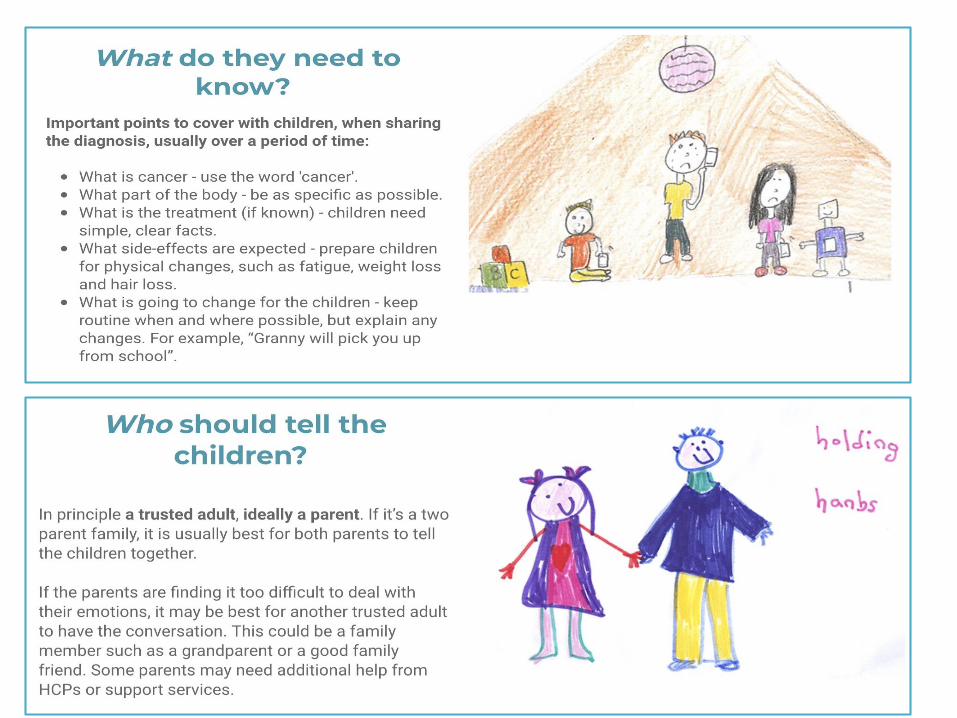
❖Numerous decision – when, how much information
Lack of instructive support from professionals
Challenges confronting families
Communicating with the children about cancer - children's perspective
Data collection: semi-structured interviews and drawings
Key findings:
▪Sensed something was wrong at home
▪Desire for information, include ongoing updates
▪Viewed cancer as a serious condition
Effects of cancer treatment - children's reflections
Sick in bed Need for medicine
Misconceptions
Contagious
‘It’s a bit stupid but I used to think that you could catch
cancer
Blamed themselves
‘I thought it was my fault..by being annoying sometimes’
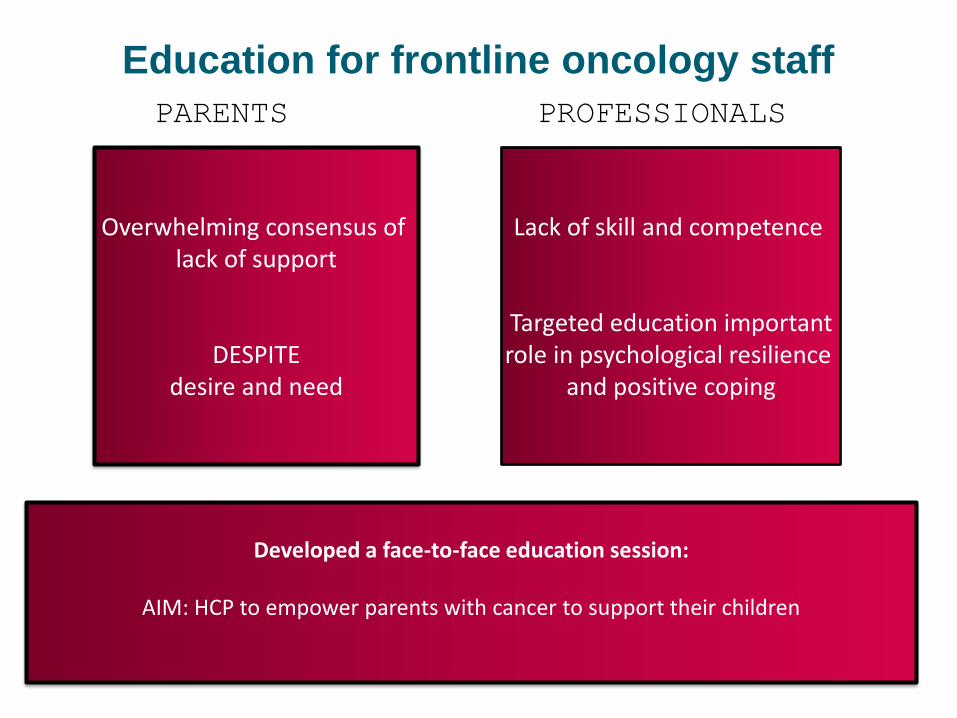
Education for frontline oncology staff
PARENTS PROFESSIONALS
Overwhelming consensus of lack of support
DESPITEdesire and need
Lack of skill and competence
Targeted education importantrole in psychological resilience
and positive coping
Developed a face-to-face education session:
AIM: HCP to empower parents with cancer to support their children
Impact of parental cancer
Fatherhood & cancer
Evaluation of Family Support Service
Face-to-faceeducation sessions & roll-out of CLIMB
E-learning
module
Family-centred Cancer CareDr C Semple & Prof E McCaughan
Emotional struggles of younger cancer patients

In conclusion
Remember ‘we treat people, not a
collection of parts’





























