Embed Size (px)
Citation preview

Dr. Anurag Mehta
Director Lab services
RGCI & RC

Carl Sternberg
Dorothy Reed
Sir Samuel Wilks
Thomas HodgkinCD15

Long history > 150 years
Enigmas
EBV
Origin of RS cell
Mélange of
Antigens
Milieu
Clustering
&
familial
Overlapping
features with
Several Lymphoma
types
Despite long history and not being infrequent
Difficult D/D

References: 1. American Cancer Society. Cancer Facts & Figures 2013. Atlanta, GA: American Cancer Society; 2013. 2. Types of non-Hodgkin lymphoma.
American Cancer Society Web site. http://www.cancer.org/cancer/non-hodgkinlymphoma/detailedguide/non-hodgkin-lymphoma-types-of-non-hodgkin-lymphoma.
Updated November 14, 2013. Accessed December 19, 2013. 3. Küppers R. Nat Rev Cancer. 2009;9(1):15-27. 4. International T-Cell Lymphoma Project.
J Clin Oncol. 2008;26(25):4124-4130. 5. Swerdlow SH et al, eds. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 4th ed.
Lyon, France: IARC; 2008. Note: B-cell and T-cell sub-classifications are illustrated on slides 10 and 11, respectively.
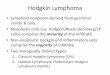
Nodular lymphocyte-
predominant
Hodgkin lymphoma (NLPHL)
(5%)
Non-Hodgkin
lymphoma (NHL)
Hodgkin
lymphoma (HL)
Classical Hodgkin
lymphoma (cHL)
(95%)
Lymphoma

1. The Hodgkin lymphoma is separated into
2 types for several reasons.
2. One amongst them is the morphology of
neoplastic cells
• RS cells, Hodgkin Cells & variant
→ cHL
• LP Cells → NLPHL
3. Immunophenotypic attributes
4. And now also on the basis of cell
of origin

The classical Hodgkin Lymphoma is further
divided into subtypes on the basis of
1. Quantity of RS cells
2. Host response: Nature of the inflammatory
components
3. Fibrosis
• Banded fibrosis
• Birefringent, fibrillar
• Non-birefringent, amorphous

Hodgkin Lymphoma: Classifications
WHO 2008
Nodular lymphocyte predominant HL
Classical HL
1. Nodular sclerosis
2. Mixed cellularity
3. Lymphocyte depleted
4. Lymphocyte-rich
Although classification is mainly
based on histopathology, recent
studies have demonstrated that
these disease entities are
biologically different, with different
genomic alterations, gene-
expression patterns, cytokine
milieu and clinical behavior.
1. Devilard E, Bertucci F, Trempat P, et.al. Gene expression profiling defines molecular subtypes
of classical Hodgkin’s disease. Oncogene 2002, 21:3095-3102.
2. Levy A, Armon Y, Gopas J, Ariad S, et.al. : Is classical Hodgkin’s disease indeed a single entity?
Leuk Lymphoma 2002, 43:1813-1818.

LP CELL
What is the cell of origin of RS Cells & LP cell?
Difficult to identify till recently
• Neoplastic population is sparse
• Strange phenotypes
Rescued from apoptosis
and transforming events

Granzyme B /perforin
CD30
Extensive
reprogramming. USP
loss of the B cell
identity, so that these
“failed” B cells escape
the apoptosis
LMP1

How is a GCB cell with crippling mutation rescued/ why doesn’t it die
an apoptotic death?
1.LMP1 mimics an active CD40 receptor, a central costimulatory molecule for B cells
2.LMP2a carries a cytoplasmic motif that resembles the signaling module of the BCR

LP Cells
1. Express B-lymphocyte markers, including GCB Ag like BCL-6 and
activation-induced cytidine deaminase.
2. LP cells grow in a follicular pattern in assn. with FDCs & THFC
3. LP cells express functional BCR
4. A gene expression study of isolated LP cells indicate that these cells
resemble an intermediate developmental stage between germinal
centre and memory B cells.
Marafioti, T. et al. Origin of nodular lymphocyte-predominant Hodgkin's disease from a clonal
expansion of highly mutated germinal-center B cells. N. Engl. J. Med. 337, 453- 458 (1997).
Brune, V. et al. Origin and pathogenesis of nodular lymphocyte-predominant Hodgkin
lymphoma as revealed by global gene expression analysis. J. Exp. Med. 205, 2251- 2268
(2008).

RS and Hodgkin cells of cHL
1. B-cells of the germinal center origin with crippling mutations –
somehow rescued – loses several B cell phenotypes including
immunoglobulin receptors
2. Create a unique histology by to and fro exchange of cytokine-ligand
interactions
3. 40% of cases associated with EBV in Western countries; higher in
developing countries ~ 60%
Marafioti T, et al. Hodgkin and Reed-Sternberg cells represent an expansion of a single
clone originating from a germinal center B-cell with functional immunoglobulin gene
rearrangements but defective immunoglobulin Transcription. Blood. 2000;95(4):1443–
1450.

Familial Predisposition
1. Genetic predisposition observed in 1% of Hodgkin lymphoma.
2. 3- to 7-fold increased risk of developing the disease in siblings.
3. KLHDC8B loss of function mutations / SNP with reduced function
4. germline frame shift mutation of the NPAT gene was found in a
family with four members affected by NLPHL
5. Suspected germline alterations responsible for familial HL are
PVT1, REL, GATA3
and a germline variation leading to the deletion of serine 724 was found in several cases
suggesting an elevated risk for the disease (odds ratio = 4.11; P = .018). NPAT is thus far
the first gene implicated in nodular lymphocyte predominant Hodgkin lymphoma
predisposition.
Saarinen S1, Aavikko M et.al., Exome sequencing reveals germline NPAT mutation as
a candidate risk factor for Hodgkin lymphoma. Blood. 2011 Jul 21;118(3):493-8. doi:
10.1182/blood-2011-03-341560. Epub 2011 May 11.

Proc Natl Acad Sci U. S A. 2009 Sep 1; 106(35): 14920–14925.
Published online 2009 Aug 12.
Genetics
Mutations in a gene encoding a midbody kelch protein in familial and sporadic
classical Hodgkin lymphoma lead to binucleated cells
Stephen J. Salipante,a Matthew E. Mealiffe,b,1 Jeremy Wechsler,c
ABSTRACT
Classical Hodgkin lymphoma (cHL) is a malignancy of B-cell origin in which the neoplastic cells, known as
“Reed-Sternberg” (RS) cells, are characteristically binucleated. Here we describe a family where
multiple individuals developing cHL have inherited a reciprocal translocation between
chromosomes 2 and 3. The translocation disrupts KLHDC8B, an uncharacterized gene from a
region (3p21.31) previously implicated in lymphoma and related malignancies, resulting in its loss of
expression. We tested KLHDC8B as a candidate gene for cHL and found that a 5′-UTR polymorphism
responsible for decreasing its translational expression is associated with cHL in probands from other
families with cHL and segregates with disease in those pedigrees. In one of three informative sporadic
cases of cHL, we detected loss of heterozygosity (LOH) for KLHDC8B in RS cells, but not reactive T
lymphocytes, purified from a malignant lymph node.

HL: Definition
Characterized by presence of a tiny population of
neoplastic cells in a defined milieu
1.The Neoplastic cell- RS cell, Hodgkins cell,
variants and LP cells
2.The Milieu


Mature & small lymphocytes
Can have abundance of Histiocytes

Occasionally paucicellular for
lymphocytes
Some plasma cells??

Eosinophils
Delicate fibrosis between cells

The concept of context/ milieu is actually fluid. Not
something carved in stone. Most of the
lymphocytes are mature (95%). Exceptions occur.
Reactive and atypical lymphocytes sometimes make
up the milieu
Sohani AR, Jaffe ES, Harris NL et.al
Nodular lymphocyte-predominant Hodgkin
lymphoma with atypical T cells: a morphologic
variant mimicking peripheral T-cell lymphom
Am J Surg Pathol. 2011 Nov;35(11):1666-78.
10.1097/PAS.0b013e31822832de.

TypeLympho
cyte
Histio
cyteEo
Plasma
cell
Banded
collagen
Fibrous
tissueRS cell
NLPHL 5+ + to 3+ 0 0 0 0LP cells
±
LRCHL 4+ + to 3+ 0 to + 0 to + 0 0 +
NS + to 4+ + to 2+ + + + to 4+ + +, +++
MC 2+ to 3+ + to 3+ 2+ + 0 2+ 2+ to 3+
LD 0 to + 0 to + + to 2+ + 0 + to 4+ 2+ to 5+
Cellular Composition & types of HL

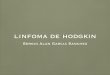
Nodular Lymphocyte Predominant Hodgkin Lymphoma (NLPHL)
1. 5-6% 0f all HL
2. Nodules of B cells + Spheroidal collection of FDCs + LP cells in center
3. Evolve from a nodular → nodular and diffuse→ diffuse.
4. All ages, including children. 4th decade
5. M:F = 2.5:1
6. Mostly Stage I
7. Cervical, axillary, inguinal Lymph nodes most often involved.
8. Rare involvement of mediastinum. Extranodal disease in NLPHL is
rarely observed, with the exception of splenic involvement, which can
be seen in 10%–15% of cases. Liver involvement occurs in 10% of
patients, and bone marrow or lung infiltration is found in 5%.
9. 10-15% in higher stages

Nodules in
NLPHL
Sclerosis can occur in older
nodes

NLPHL

Plasma cells in
NLPHL
Rosettes around the L P
cells

CD20 nodules
CD20 nodulesCD20 nodules &
LP Cells
LCA

CD20
CD20
PAX5
PAX5

CD3
CD57
CD4
CD57

EMA

CD23

BOB-1
CD30 expression
in NLPHL
OCT2

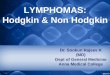
Nodular Lymphocyte Predominance Hodgkin Lymphoma:
Immunophenotype of LP/L&H Cells
1. CD45 + (95%)
2. CD30 - (10% weak +)
3. CD15 - (10% +)
4. CD20, PAX-5 + (95%)
5. Bcl-6, bcl-2 + (95%)
6. EMA +/- (70%)
7. CD3, CD43, CD10 - (0%)
8. Consistent lack of EBV markers
9. CD4 and CD57 co expressing T cells ring around the LP cells