Embed Size (px)
Citation preview

7/5/2017
1
dsaw.org
Down’s Syndrome: an OverviewDr. Amanda Votruba, M.D. FAAP
Dr. Amanda Votruba, M.D. FAAP
• Pediatrician with Methodist Physicians Clinic
• Board Certified in Pediatrics
• No disclosures
Objectives
• Goal: More clear understanding of the problems associated with Down’s Syndrome and the special management they require.
-History and Incidence
-Characteristic physical features and their implications
-Problems associated with Down’s syndrome and the management
-Routine screening tests
-Specific management issues in the newborn period and throughout their life time
Down Syndrome
• First recognized in 1866 by John Langdon Down
• During this time period there were many theories of causality
• First reference to Down’s Syndrome was 10 years later.
• 1959 described as chromosomal condition
• It took until 1965 for it to be the accepted term.

7/5/2017
2
John Langdon DownWhat is Down Syndrome?
Typically, people are born with 46 chromosomes
Down syndrome is a condition in which a person has an extra set of chromosomes
Etiology
• Most are a full trisomy- nondisjunction, most common form (95%)
• Mosaics- are rare, mixture of two types of cells. Some are the usual 46, and some 47. (1%)
• Translocation- Total number of chromosomes is 46 but a full or partial copy of chromosome 21 attaches to another chromosome (4%)
Etiology
• Translocation is inheritable
• 1/3 of the cases a parent is a carrier
• Genetic counseling is recommended
• Most frequent is Robertsonian translocation

7/5/2017
3
Incidence by Age Group Diagnosis
• In Utero
• Physical characteristics
• Chromosomal analysis- necessary for confirmation FISH/karyotype
s3.amazonaws.com
Down syndrome features
• General: Hypotonia
• CNS: Mental deficiency
• Craniofacial: Brachycephaly, upslanting palpebralfissures, hypoplasia of frontal sinuses, small nose and epicanthal folds
• Eyes: Brushfield spots, myopia, cataracts
• Ears: small, hearing loss
• Dentition: hypoplasia and abnormal placement
• Neck: Appears short

7/5/2017
4
Down’s Syndrome Features
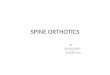
• Hands: Short metacarpals and phalanges, fifth finger hypoplasia, Simian crease,
• Feet: Wide gap between toes
• Pelvis: abnormal iliac crest
• Cardiac: Endocardial cushion defect
• Skin: Loose posterior neck, dry skinSmith’s Recognizable Patterns of Human Malformations
Physical characteristics of Down syndrome
Up slanted palpebral Fissures
-The outer corner of the eye will be turned up rather than down.
Upslanted Palpebral fissures Other Eye Findings:Brushfield spots-white flecks that can be seen close to the periphery of the iris.
-Sometimes described as stars

7/5/2017
5
Epicanthal Folds Optho management
• Their eyes should be tested at birth and again at 1 year or sooner if concerns exist.
• By adulthood, 15% have cataracts
• Myopia is common
Hearing
• Children with DS are at increased risk for hearing loss. Up to 80%
• Hearing should be tested at birth and again every 6 months in early childhood until normal hearing can be documented in both ears. Then, may go to yearly testing.
• Increased risk due to recurrent middle ear fluid and infections. (conductive loss)
• Treatment may be tubes
Myringotomy tubes

7/5/2017
6
Dentition
• Hypoplasia and irregular placement
• Delayed eruption
• Management –early involvement of pediatric dentist. Good dental hygiene.
Geneticdisorders.ifo
Neurologic
• Hypotonia
• Gait disturbance
• Intellectual deficiency
• Developmental delay
• Seizures
• Psychiatric issues
• Cervical cord compression
• Dementia
Hypotonia
• Leads to tendency to keep mouth open and protrude tongue
• May lead to feeding issues in newborn

7/5/2017
7
Hypotonia
• Strength normalizes as children age.
Intellectual delay
• Level of impairment varies.
• Linguistic abilities affected disproportionately to overall cognitive abilities
(Sivaswamy, L. 2013)
• Delayed spoken language
• Delayed potty training-most by 5 years
Developmental Delay
• Treatment: early specific therapies. Examples: physical therapy, occupational therapy, Early Intervention
• Parents should have high expectations of their children
Seizures
• Epilepsy occurs in 1-13%
(Sivaswamy, L. 2013)
• Infantile Spasms may occur in first year of life
• Treatment: Recognition
Same as in the general population

7/5/2017
8
www.choc.org
Psychiatric Issues
• 18-38%
• Depression, ADHD, Oppositional Defiant Disorder, impulsive and disruptive behaviors
• Autism- occurs in 18%
Cervical Cord Compression
• Children with DS have a 1-2 % risk of atlantoaxial instability
• Average age is 10.5 years
• Previous guidelines recommended cervical spine radiographs between 3-5 yo, the 2011 guidelines do not. Careful surveillance instead
• The special Olympics may still require them. Sports putting them at risk: soccer, football , and gymnastics
Runragnar.com

7/5/2017
9
Neurologic
• A neurologic exam should be performed yearly to evaluate for changes in tone
• Physical exam changes: brisk DTRs, up-going plantar response
• Parents should notify their physician of any changes in gait, arm or hand function, bowel or bladder control
Dementia
• Early Alzheimer’s- by age 40 almost all individuals have significant plaques and tangles
• More than 75% older than 65 years have Alzheimer’s. 6 times that without.
Symboluk.co.uk
Endocrine
• Thyroid level is tested at birth in the Nebraska Newborn screen. It should be repeated at 6 months and 1 year
• Yearly after
• 50-60% develop hypothyroidism by adulthood

7/5/2017
10
Cardiac Concerns
• 40-50% of children with DS may have a cardiac anomaly. Therefore, all infants with DS should have a screening echocardiogram
• Most common is an AV canal, second is isolated VSD and the Tetralogy of Fallot
• Major cause of early mortality
• Treatment: Diagnosis specific surgery. 10-15% are severe requiring surgery in the first months of life
Endocardial cushion defect
Heart defect
• Physical exam finding may not be obvious in first days of life. Heart murmur is most typical finding or irregular or fast breathing.
• Untreated may result in feeding problems, cyanosis, increased chest infections
Respiratory System
• Most common cause of hospitalization
• Increased lung infections
• Infections are more severe
• Craniofacial features add to issues. Narrowed nasopharynx, flattened midface, macroglossia, and airway size
• Airway abnormalities

7/5/2017
11
Obstructive Sleep Apnea
• Obstructive Sleep Apnea- every child with Down syndrome should have a sleep study by the age of 4.
• Sleep apnea may lead to behavioral problems
• Increased strain on the heart over time
Asthma
• Studies have been equivocal if there is an increased risk of asthma in DS
GI Concerns
• Second most common condition. 10% of children will have an abnormality
• Newborn issues: Duodenal atresia, tracheo-esophageal fistula, Hirschsprung disease and imperforate anus
• Continued issues: Celiac, GERD, constipation
Duodenal Atresia
• If severe, may be diagnosed on prenatal ultrasound
• May present if first hours of life with emesis, possibly bilious, or failure to stool
• The diagnosis can be made with plain films with the presence of the “double bubble sign”
• Treatment- Decompression with NG or OG tube. Ultimately, is a surgical cure
• Without surgery may not survive

7/5/2017
12
Double Bubble sign Imperforate Anus
• Frequently associated with Down syndrome.
• Completely blind rectum and usually 2 cm above perineal skin
• When properly operated on, good prognosis for bowel function
• Anal stenosis- less severe but may result in constipation. Treatment may be dilation but often requires surgery as well
Imperforate anus Hirschsprung Disease
• Rare -2%
• An abnormality of the large bowel where nerve cells are missing
• Symptoms:
In newborn-failure to pass stool
Long term- chronic constipation, poor weight gain, and vomiting
• Diagnosis- exam, xray, biopsy
• Treatment-surgical

7/5/2017
13
Celiac disease
• 5% will develop
• Celiac disease can present in many ways: diarrhea, constipation, poor weight gain, weight loss, behavior changes and abdominal pain
• Diagnosis-blood test then biopsy
• Treatment- removal of gluten
• Management- testing if symptoms present
Musculoskeletal
• Hypoplasia of 5th digit
• Simian Crease
• Ligamentous laxity
• Abnormal pelvis with shallow hip joint and flared iliac wings
• Short neck with loose folds.
• Lower bone density found in adults
Simian Crease Simian Crease/ Sandal Foot Deformity

7/5/2017
14
Hip Problems
• 5-8% of joint instability due to hypotonia and ligamentous laxity
• Can result in subluxation of hip. Peak age 3-13 Symptoms: painful limp
Diagnosis: xray
Treatment: Immobilization and surgery
• Legg-Calve Perthes- loss of blood supply and the bone becomes weak and misshapen
Symptoms: painless limpAmerican Academy of Orthopaedic sugeons, AAOS.org
Hip instability
Knee/Feet problems
• 20% of knee instability resulting in dislocation
• Braces for conservative management
• Surgery
• Often flat footed- orthotics may be helpful American Academy of Orthopaedic sugeons, AAOS.org
Hematologic Issues:
• People with Down syndrome have a high risk of developing leukemia. Possibly as high as 20-30 times the general population. (1%)
• Neonates and infants can have transient myeloproliferative syndrome. Exam findings include: hepatosplenomegaly, anemia, and thrombocytopenia. (occurs in 10%)

7/5/2017
15
Management of Hematologic issues
• A CBC should be completed at birth. If normal no further work up.
• If a child ever has weight loss, pallor, fevers, or petechiae a CBC should be performed.
• Yearly CBCs
General management
• Previous growth curves were made in 1988
• In 2011, it was recommended to stop using the specialized growth curve and use the standard curve
• Currently, work is being done to establish a BMI chart
General Management
• Aap.org has specific guidelines for each age group
Wisdom from a pediatrician mom of Aaron-5 year old with Down Syndrome
• “This is not a bad diagnosis! It comes with it’s own set of worries but it also brings unbelievable joy, love, and faith!”

7/5/2017
16
References
• Nelson’s Textbook of Pediatrics, Copyright 2000• Recognizable Patterns of Human Malformation, Smith’s 1997• “Down Syndrome,” Pediatrics in Review, December 2013, Vol 34/
Issue 12 • Gastrointestinal Issues in Children with Down Syndrome, Marder, Liz• Alz.org “Down syndrome and Alzheimer’s disease” 2015• Musculoskeletal Disorders In Down Syndrome, Leshin, L, 2013• American Academy of Orthopaedic sugeons, AAOS.org• Down-syndrome.org• Dseinternational.org• Healthychildren.org• Ndss.org
Photo references
www.featureshoot.com
http://www.earcentergreensboro.com/
Ndss.org- Page 8
Noahsdad.com-page 5
Theblessingofverity.com-page 13