Embed Size (px)
Citation preview

1
ISS
UE
27
. 202
0
ISSUE 27 . Winter 2020ISSUE 27 . Winter 2020
Down Syndrome and Congenital Heart DefectsTop Medical Professionals Weigh In
Down Syndrome and Pediatric PodiatryA Professional Mom Shares Her Insights
Exploring Different DisabilitiesRubinstein-Taybi Syndrome

WH
Y H
ASC
CENT
ER?
1. Simple signup process for families, staff and brokers
2. Hands-on experienced FI Coordinators to provide assistance from your first call
3. Work with our agency brokers or a broker of your choice.
4. Control your Com Hab, Respite and SEMP staff’s salary’s and hours
5. Electronic timesheets and invoice processing
6. Reimbursements to families and vendors average less than a month
7. Access to community classes, memberships, transportation, housing, family reimbursed respite and more
HASC Center is dedicated to provide people with intellectual disabilities the necessary empowerment tools to live as independently as possible. With our 40+ years of experience in enhancing lives, we are uniquely suited to matching both children and adults with special needs, with services to help them thrive. Our person-centered approach is legendary.
At HASC Center, we offer our expertise for all phases of Self-Directed planning. As a Fiscal Intermediary provider, we will help you manage the financial ins and outs of your plan. Our highly advanced computerized services offers easy and technologically advanced assistance in maintaining budgets.
Self-Directed/Fiscal Intermediary Service
HASC Center is now accepting new Self-Direction/FI cases in all 5 boroughs, Nassau/Suffolk Counties
For the Greatness Within
Ready to start planning your Self-Directed life? Reach out to us today!
718.434.8217 | [email protected] | 1221 East 14th St. Brooklyn, NY 11230

Individualized and Group Programmatic Focus On:• Continuing year round academic and personal growth, in enriching daily special education classes under the leadership of professional teachers.
• Availability of Physical, Occupational and Speech therapies.
• Reinforcement of Davening, Brachos, Bentching and performance of Mitzvos.
• Enhancement of each camper’s independence and strengthening of their social development.
• A broad spectrum of outdoor activities, adaptive physical education and daily swimming sessions.
• Outstanding nutritionally sound meals with the capacity to address a full spectrum of special diets.
• Reliable and safe transportation is provided for day campers.
Program is geared for campers who are eligible to receive OPWDD Respite funding.
Camp HASC’sChavivim Program
For young children with special needs, age 9 and below.
To learn more, or to apply,email: [email protected]: (718) 686-2607
Space is extremely limited!
Chavivim is Tons of Fun!
Sleepover and Day Camper options available.
Your child is part of the overall Camp HASC magic which includes themed special events, famous concerts, performances and recreation productions.


Everyone'sFAVORITE
Every child’s dreama party with Klein’s ice cream!

Open Forum8 Editor’s Message
12 Mailbag
Did You Know
14 An Important Pediatric Podiatry Issue
FeaturesTHEME: DS AND CHD
18 Prenatal Diagnosis and Management of CHD in Down Syndrome
24 Early Childhood; Down Syndrome and CHD
30 Down Syndrome and Pulmonary Hypertension
32 Cardiac Care of the Adult with DS
40 Preparation is Key
42 On the Double
50 Butterflies
52 The Bond That Ties…
54 Chapter 21
56 We Cannot Let Them Suffer Alone
58 Can I Have A Cookie?
60 My Precious Child
61 Why I Love My Nurses
62 In Memory Of Shloimy Schlesinger
36 Yiddishe Nachas
78 Up Syndrome
ExploringDisabilities/ conditions
67 About Rubinstein-Taybi Syndrome
68 Living With Rubinstein-Taybi Syndrome
Sibs' Niche' /Teen Scene72 What She Taught Me
74 Special In Every Way
75 Who I Am
76 Hold On To Them!
77 What Is Closest To My HeartCO
NT
EN
TS
Please Mail All Correspondence To:Down Syndrome Amongst Us32 Rutledge StreetBrooklyn, NY 11249Email: [email protected]
To purchase back issues of DSAU, kindly email: [email protected] contact the editor for permission to reprint anything in this issue.
Can be purchased individually for $5.00
Design: [email protected]
Down Syndrome Amongst
Us
6IS
SU
E 2
7 . 2
020

The premier Yeshiva within a Yeshiva for boys withDown Syndrome & other disabilities located in Torah Vodaath
425 East 9th Street, Brooklyn, NY 11218718-693-9032 | [email protected]
A full Limudei Kodesh curriculum
Comprehensive general studies
Vocational training program
Speech, OT, PT
State-of-the-art computer center
Warm, caring environment
Licensed Rebbeim/Teachers
Emphasis on social skills & life skills
Day hab program
A full Limudei Kodesh curriculum
Comprehensive general studies
Vocational training program

OP
EN
FO
RU
MEditor’s Message:
If you have been reading Down Syndrome Amongst Us for a while, you probably know that I enjoy “myth-busting”, i.e. shattering false beliefs that have been long held.
My oldest daughter teaches a lovely honor student who has a three year old brother with Down syndrome, also named Moishey. One morning last week I received a text from her student’s mother. The mother wrote: ‘I just returned from the PTA meeting where I met your daughter for the first time. It seems that both our Moishey’s did not affect their siblings adversely.’
So much for “damaged siblings” caused by the child with Down syndrome.
At a recent Shabbos aufruf at our shul, the bride’s father traveled from a distant community to join the festivities. We asked him why his 7-year-old-son, who has Down syndrome, was not present. He replied that the kallah protested, “It’s my last Shabbos at home and you want to take him away??”
So little brother stayed home where his sister enjoyed last licks with him.
When our son recently married his delightful young bride, the old shidduch myth was busted too. Siblings of individuals with Down syndrome can certainly marry wonderful spouses from wonderful families.
Years ago, I received and published a letter to the editor that spewed ignorance and bias toward individuals with Down syndrome. The writer claimed that these kids are like robots, with no emotions.
During our erev Shabbos phone call on the last Friday of camp, this past summer, I asked Moishey whether he was excited to come home. He replied that he was. I asked him, “Are you laughing or crying about it?” He said, “Neither”. I prodded on, “What then, Moishey?” and he said, “I am emotional about it.”
Recently, on the first anniversary of the Pittsburg Synagogue attacks, which Moishey had read about in the newspapers, he asked to dedicate one song of the Friday night zemiros to the Pittsburg victims, and he actually broke down and sobbed as he sang.
Let us bury myths that foster fear and confusion, and face the reality that brings clarity and joy.
Just a mere 3-4 months ago we observed a season of introspection and teshuva. We were inundated with articles and speeches about accepting blame and refraining from attributing faults to others.
Different folks have different locations where they repent – some in synagogues, others in open fields, cemeteries, etc.
Moishey repents in the shower.
That is where he self-talks and self-lectures and offers important insights
8IS
SU
E 2
7 . 2
020

OP
EN
FO
RU
M
that we can all learn from, like the golden nugget that blasted past the locked bathroom door: “You’re gonna learn to grow up and take your punishment like a man, if you know what’s good for you.”
Definitely a sobering lesson from a young man with a disability.
I am aware that the readers of Down Syndrome Amongst Us have come to enjoy my fiction stories based on reality. In this edition of DSAU, I will present one non-fiction story here and it will be a based on facts.
At a chuppah my husband and I attended, we stood on the two sides of the aisle, each of us with quite a different view. I observed young children, whose parents were present among the guests, jumping on and off the platform where the chuppah was occurring, running in front of the photographers’ lenses, tripping the tripod and equipment and raising a ruckus. There wasn’t a parent in sight to discipline any of the kids whose behavior was so appalling.
I had a fleeting thought: “If these kids had Down syndrome, everybody would have decried their inappropriate behavior and would have pointed fingers at how untrained they are. Everyone would have proclaimed that they should not be brought to simchos and not even kept at home.” Just a fleeting thought…
On the men’s side of the aisle, my husband was being verbally pummeled by the grandfather of a young child with Down syndrome and secondary disabilities. He was extremely upset at us for making it our mission to convince parents to keep their children with Trisomy 21 home. His grandchild is “difficult, wild and unruly” and his children don’t want to hear of giving the child up.
We met after the chuppah and discussed what we each had experienced. It was an eye opener on so many levels. First, grandparents are key players in their children’s lives, and if they offer advice that is detrimental to their relationship with their children and grandchildren, they are causing lifelong damage. Yes, it is painful for parents to watch their children struggle, but by lending support they are defusing an already challenging situation.
Distinguished faculty • License-eligible • BCBA + LBA approved • Selected classes available onlineFor info and to apply visit shs.touro.edu/aba | Use code CBAWAIVER to waive application fee
in Applied Behavior Analysis on Touro’s Manhattan campus.
9
ISS
UE
27
. 202
0

OP
EN
FO
RU
M In addition, there are children who don’t have Down syndrome and are
untrained and unruly, as witnessed during the chuppah. Why take advantage of children with special needs and dump negative stereotypes upon them, when in all reality their typical counterparts are guilty of the same or worse behaviors? Let us spare these children and place the blame where it belongs; if children are not raised properly with derech eretz and social etiquette, they will grow like wild weeds, whether or not they have Down syndrome.
My husband is in touch with a young avreich in Israel who has partnered with another parent of a child with Down syndrome, in a mission to educate Rabbonim and Admorim about the ins and outs of Down syndrome. Of the 60 chashuva spiritual leaders they visited, 58 immediately agreed with these 2 fathers that a child’s best place is home; the remaining two were convinced after having an eye-opening discussion with them. One chashuva Rebbe exclaimed to them, “I wish you would have come a week ago; my advice to a new set of parents would have been very different.”
While my husband and I embarked upon the same project locally several years ago, our wings were clipped very early on in our venture. These 2 brave fathers have now given flight to this cause and have given us courage to renew our efforts here in the USA.
An interesting statistic that was proven by these 2 yungeleit is, that if families get proper guidance after their child with Down syndrome is born, not even one family ever regretted taking their child home with them. That says something about proper education and guidance…in every aspect of life.
At a visit to the cemetery prior to our son’s wedding, to invite our deceased parents z’l to the Simcha, I came to a sad and painful realization that echoes the sentiments of Down syndrome stigma years ago.
As I walked toward the section where young children were buried r’l, I noticed that the tombstones that were very aged were also very small, with very little information on them. They did not even feature the child’s family name. It was as though it was shameful to have died as a child. The more recent gravestones were larger, more prominent and were engraved with the child’s full name, family name, name of parents, etc. When realization dawned, it tore at my heart; years ago, it was a shame to lose a child r’l, so even the stone was shrouded in secret. Nowadays, when a child is r’l niftar, parents understand that it is not something to be ashamed of and they bury their children with the proper kavod.
How unnerving to realize the similarities between that horrific challenge and Down syndrome years ago and now.
How wonderful to see that people’s outlook can change for the better.
Best wishes for a toasty winter. See you on July 1st ’20 iy’Hashem!
Sarah [email protected]
10IS
SU
E 2
7 . 2
020

OP
EN
FO
RU
MReachingHigher
HCSNY.ORG
718.854.2747777777777777777777777777777111111111111111111111118888888888888888888888888888..........888888888888888888888888885555555555555555555555555544444444444444444444444444.............222222222222222222222222227777777777777777777777774444444444444444444444447777777777777777777777
HCSNY.ORG
Reaching Higher
HCSNY.ORG | 718.854.2747
• RESIDENTIAL PROGRAMS
• COMMUNITY HABILITATION
• FAMILY SUPPORT SERVICES
• EMPLOYMENT SERVICES
• ASSISTIVE TECHNOLOGY
• BEHAVIOR MANAGEMENT
• RENT ASSISTANCE
• DAY HABILITATION
• CAMP RESPITE
• SELF DIRECTION
• RESPITE
• AND MORE
pivotgroup.nyc

OP
EN
FO
RU
M
Mailbag
Dear Sarah:
Guess what?! I got my copy of DSAU #26! To paraphrase Dovid, “sof, sof”!
What a beautiful magazine. I love the cover!
How many hours does Moishey pose for G&B? Dovid would love such a “job” - he’s great at acting.
I very much liked the story you wrote “Of Mind Games.” Well written and so true. Honestly, the lesson learned can be translated to almost anything in life. Do we know what is best for us? Sometimes, accepting a “hardship” instead of trying to “fix Hashem’s world” is the best thing. Only after we messed up do we see how much good we could have had.
Dovid “paskened” that he is allowed to listen to music during the three weeks because he needs to practice his dance steps for our upcoming wedding!!!
Hatzlacha with your chasunah prep!
SGYerushalayim
Dear Sarah:
This is in response to your request in the recent issue of DSAU to hear from families with over-30-year-old children who have Down syndrome, regarding mainstreaming.
Our daughter, Devorah, who has Down syndrome, is 34 years old and is doing
very well, even out in public where she commutes on the subway by herself and holds several jobs. I have been in touch with you and DSAU over the years about her progress. She was always in a class with other high-functioning special needs children who were called educable at that time. I feel that was far better for her than a mainstreamed class (especially after about age 3) where she would have been very overwhelmed and would also have had more trouble making friends.
Devorah has always had a tremendous amount of pride in her accomplishments and a high sense of self-esteem. She may have not had such pride if she was always trying to keep up with the typical children and constantly saw the difference in their abilities. She made progress throughout the years but at her own pace.
Devorah remembers her schools fondly and even keeps in touch with some of her teachers.
B’Ahava,Andrea D. Lieberman
North Bellmore, New York
Dear Editor:
When I was in tenth grade, I had to give an informative speech on any topic, as an English assignment. Since I had a brother with Down syndrome, I chose to speak about that. I have to admit, I took my whole speech directly from “Down Syndrome Amongst Us”. I think it may
12IS
SU
E 2
7 . 2
020

OP
EN
FO
RU
M
have been in the first issue. My teacher loved it! (Maybe because she has a son with Down syndrome.)
Thank you so much!Have a great day!
M.P.
Dear Sarah,
Thank you so much for your amazing and informative magazine. Each issue is filled with such a great balance of chizuk, guidance, humor and realistic fiction. Our family really appreciates all of it. May you be gebentscht.
I am specifically writing this letter in regard to your story “Of Mind Games and Arm Twists”. Boy! are you right. This story is the story of many unfortunate families.
Close to four years ago a friend and I both gave birth to babies with Down syndrome. My family has B’H been loving every minute with our dear darling. She has brought tons of light, nachas and joy into our lives. We wouldn’t trade her for ANYTHING in the world.
At the same time, my friend, who like Bashy in the story, was emotionally prepared and ready to take on the challenge with joy and love, was convinced, wheedled and FORCED to send away her dear baby. She has never truly recovered. She seems to put one foot in front of the other. She tries to get on with life and to be there for her other children. But, the light in her eyes is gone. Her simchas hachayim has unfortunately been extinguished.
Please continue to spread the information that children with Down syndrome may come with challenges, but the nachas more than makes up for it many many times over, and the hole in a heart from losing a live child r’l is not repairable.
May Hashem grant you true siyata dishmaya to continue to be a source of inspiration to the many Yiddishe families
dealing with challenges with devotion and love.
Sincerley,C.S. - Yerushalayim
Dear Editor:
I live in a different country than you do. For the purpose of protecting the privacy of the protagonist in this letter, I will be somewhat vague.
Approximately four years ago I got a call about a family I know that was blessed with a baby born with Down syndrome. The mother adamantly refused to take the baby home and left her at the hospital. A Jewish foster home was found. Luckily. For Pesach of that year, the family was traveling to New York and I worked hard to establish an appointment with this family and a prominent NY advocate for children with Down syndrome. Even after their meet, this mother was still not convinced. Her husband and children were begging to bring the baby home; they were constantly visiting the foster family and even giving the baby baths there.
I, myself a parent of a darling with Down syndrome, was reading one of your magazines and came across an article that was very similar to what this family was experiencing. I texted her, asking whether she was ready to read the article. She replied that she was and that her sister was coming to my neighborhood the following day and would pick up the magazine.
That Friday night, husband and wife sat on the couch and read this article. They made their decision.
This adorable four-year-old little girl is with her family ever since. The father always says that the article in Down Syndrome Amongst Us is what brought his child back home to her biological family!
R.S.Europe
13
ISS
UE
27
. 202
0

DID
YO
U K
NO
W?
An Important Pediatric Podiatry Issue
The foot of a child with Down syndrome is unique and
special, and therefore, cannot be ignored. It is one of the most important parts of the body. While this may be true of any person, it is especially significant in a child with Down syndrome.
Podiatrists take care of painful conditions in children such as ingrown toenails and warts, but pediatric Podiatrists are also intricately involved in the preventative care of children with Down syndrome. Our goal is to prevent damage to the joints of the foot, ankle, knee and hip. Damage to these areas can occur if left without proper support.
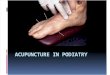
It is important to understand how the foot normally functions in order to understand how the foot of a child with Down syndrome is different. A normal foot functions between pronation (flattening of the arch), and supination (raising the arch) during gait. When the foot is supinated, it is rigid and stiff,
as when the heel first hits the ground and when the foot is about to toe-off and propel the body forward. When the foot pronates, it becomes flexible and moldable to adapt to the variable ground surface. Problems arise
when the foot either pronates or supinates at times during stance and the gait cycle, when it should not.
Most persons with Down syndrome, (specifically 88% of the population) experience very loose joints and are very flexible and therefore non-supportive. These conditions are called ligamentous laxity and hypermobility, which contribute to excessive pronation. That, along with the low muscle tone, is the precise cause of the majority of issues in the Down syndrome foot. When more complex medical issues take precedent, feet are neglected, although they must also be addressed.
The most obvious foot issue occurs when the pronation/flattening does not resolve
Arianna Sabghir, DPM
Down Syndrome Amongst
Us
Down Syndrome Amongst
Us
Note how the lines straighten out when the feet are properly supported in
the right orthotic.
14IS
SU
E 2
7 . 2
020

DID
YO
U K
NO
W?
on its own unlike other young children. If left unsupported, the foot will go on to cause irreversible destruction to the entire lower extremity. As this occurs, the ability to maintain core strength, coordination and overall strength is compromised. Ultimately, this means while your child is working so hard to master goals in Physical Therapy, their own feet are working against them. The child with Down syndrome cannot keep up with peers if they lack the necessary tools to do so—tools they can be given!
Orthotics play a life-long role in the Down syndrome foot. The orthotic will improve coordination, balance, pain, posture, strength and result in more stable and functional walking. Most children with Down syndrome can use an orthotic that fits and is hidden inside the shoe itself. Some feet require the additional support of an SMO (Supramalleolar Orthotic), a brace that extends just above the ankle joint, or AFO (Ankle Foot Orthotic) brace which extends up the back of the leg. It is important that the foot is not over-braced so joints are not restricted.
Physical therapy should be started early for children with Down syndrome and continue well into adulthood to continue building proper muscle memory and strength.
When a child with Down syndrome sees a Podiatrist, it should be someone comfortable treating children, and experienced with treating one with special needs. As a mother of a child with Down syndrome, and a doctor of podiatric medicine, I know how challenging that can be! The child with Down syndrome should have the feet, knees, hips evaluated, especially as they walk.
Most children born with Down syndrome have a characteristic space between the first and second toes—the sandal gap. This makes the forefoot wider than a typical foot. A foot with significantly loose and hypermobile joints and ligaments and a space between the toes, presents with a very wide foot. This is one of the factors making shoe-fitting a challenge.
The Down syndrome foot not only has a very wide forefoot, but it also has a very narrow heel.
Important shoe features include a supportive sole that is not too flexible (a shoe
should only bend at the toes), have a removable lining, and lace-up. A wide or extra-wide is crucial to avoid blistering and irritation on the foot. Many shoes that fit these criteria, are New Balance, Falcotto and Naturino, Billy, and Stride-Rite (to name a few).
At the end of the day, it is important that Podiatry is among your child’s regular specialists, in addition to the Cardiologist, ENT, Dentist, Gastroenterologist, and Oncologist. The foot has the potential to “silently” cause life-altering damage.
We all want our children with Down syndrome to reach their maximum potential, so don’t forget about one of the most important parts of them!
Arianna Sabghir, DPM is a Podiatrist who specializes in pediatric podiatry and biomechanics. She has her own private practice on the Upper West Side in Manhattan. She is also a Clinical Director for the Special Olympics. Dr. Sabghir is a mom to a precious 4-year-old boy with Down syndrome.
15
ISS
UE
27
. 202
0

DID
YO
U K
NO
W?

DID
YO
U K
NO
W?
Walk-Ins Welcome!
1312 38th Street | 718.686.76001278 60th Street | EzraMedical.org
EzraMedicalCenter
TAKE CHARGE OF YOUR HEALTH AT EZRA.Ezra Medical offers comprehensive medical
care services, from primary care to physical
therapy, and everything in between. If you’ve
got lots on your wellbeing task list, take care
of it all at Ezra.

FE
AT
UR
ES
/ TH
EM
E
Prenatal Diagnosis and Management of Congenital
Heart Disease (CHD) in Down Syndrome
What is Down syndrome?Down syndrome is a genetic disorder
which affects the 21st chromosome (out of the 23 pairs present in every cell). It is caused when abnormal cell division results in an extra full or partial copy of chromosome 21; hence it is also called Trisomy 21. This extra genetic material causes the birth defects, learning challenges and physical features of Down syndrome. It was first described by John Langdon Down, a British physician, in 1866 but the genetic abnormality was only confirmed in 1959. Of note, Dr. Down’s grandson was born with Down syndrome.
What causes Down syndrome?There are 3 different causes
The most common cause is Trisomy 21 (tri
meaning three) where there are three copies of the 21st chromosome instead of two. This is the cause in 95% of all cases.
Rarely (in ~4% cases), either a full or partial copy of chromosome 21 attaches to another chromosome. This is called translocation and this is the only form of Down syndrome that may be inherited.
Very rarely (in 1-2% cases), a child may have some normal cells (with 2 copies of chromosome 21) and some abnormal cells (with 3 copies of chromosome 21). This is called mosaicism and in this condition, there may be fewer symptoms of Down syndrome since some of the cells are normal.
Is it inherited?In the majority of cases (95%), it is not
inherited. However, in roughly 4% of cases
Prema Ramaswamy, MDDirector, Pediatric Cardiology
Maimonides Children’s Hospital
Down Syndrome Amongst
Us
18IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
/ TH
EM
E
there may be a risk of inheriting it either from the father or the mother due to the presence of a genetic translocation in either of them – a condition where part of chromosome 21 has been transferred to another chromosome. A genetic evaluation can confirm its presence.
How often does it occur?Each year, in the US, about 6,000 babies
are born with Down syndrome, which is about 1 in every 700 babies born.
Which women are considered at high risk for having a baby with Down syndrome?
Women who are above the age of 35 years, women whose babies have an abnormal ultrasound test and women who have had a previous baby or a close family member with Down syndrome.
Are most children with Down syndrome born to women above 35 years of age?
Actually, most children with Down syndrome are born to women under the age of 35 years since many more babies are born to younger women.
Why are women above 35 years at higher risk of having a baby with Down syndrome?
As the natural aging of a woman’s eggs results in more chromosomal abnormalities, the average 40-year-old woman will have as many as 60% of chromosomally abnormal eggs.
Are women who have had a previous baby with Down syndrome at higher risk of having another baby with Down syndrome?
Yes. This is related to the advancing age of the mother. In addition, if there is a translocation, that may increase the chances of recurrence.
Can Down syndrome be diagnosed
before birth?Yes. Generally, there are two types of
tests you can have when you are pregnant- screening and diagnostic. A screening test is suggestive and tells you what your chances are of the baby having a chromosomal condition. The diagnostic test is confirmatory and can tell for sure.
What are the screening tests?These are blood tests performed on the
mother and are of two main types. The first (also called the triple test or quad screening) measures the proteins in the serum. This is usually combined with measuring the amount of fluid at the back of the baby’s neck (also called nuchal translucency) and is performed between 11 and 14 weeks. The other test (also called cell free or cfDNA) measures small fragments of fetal genetic material. This test can be done after 10 weeks of pregnancy and is considered to be very accurate in diagnosing Down syndrome.
What are the diagnostic tests?There are two. An amniocentesis (or
amnio for short) is a procedure where a needle is inserted into the uterus to remove some of the fluid surrounding the baby to study the baby’s skin cell DNA. This is usually performed between 15 - 18 weeks. The second is called CVS (chorionic villus sampling) and is performed between the 10th and 13th weeks. There is a very small risk of miscarriage with these tests (usually quoted as 0.1-0.3%)
Are babies with Down syndrome at risk of CHD?
Yes. Almost half of all babies with Down syndrome have congenital heart disease.
Can heart disease in Down syndrome be diagnosed before birth?
Yes. This is done by a fetal echocardiogram. This is a sonogram of the heart but different from the one performed by your obstetrician. It is very detailed in its scope and looks at the fetal heart and the arteries and veins
19
ISS
UE
27
. 202
0

FE
AT
UR
ES
/ TH
EM
Ethat enter it in multiple views. It can tell the position, size, structure, function and rhythm of the unborn baby’s heart.
Is a fetal echo the same as an ultrasound that my obstetrician performs and if not, who performs it?
A fetal echo is not the same as a sonogram performed by an obstetrician. It is a higher quality test that is capable of picking up more of the baby’s heart structure. It is usually performed by pediatric cardiologists as well as some perinatologists.
How long does it take to perform a fetal echo?
It can take from 45 minutes to 120 minutes depending on the fetal position and complexity of the heart disease.
How accurate is a fetal echo and what are the limitations of a fetal echo?
Fetal echocardiography is highly accurate in determining the structure of the heart itself. However, there are a few abnormalities that could be missed, even by a detailed fetal echocardiogram, such as small holes in the heart or mild abnormalities in the veins and the great artery that arise from it.
When is the ideal time for performing a fetal echo?
It is typically done in the second trimester between 18 to 24 weeks.
Are there any side effects to a fetal echo?
There are no side effects from a fetal echo since it uses sound waves similar to those used in sonograms. It does not use radiation as is used in X- rays. So, this is a test that could be repeated multiple times, if needed.
Why is it important to diagnose congenital heart disease (CHD) prenatally?
It is important so that doctors can get ready for problems that may occur during pregnancy or during delivery. In some cases, early delivery may be scheduled; in others, a caesarian section may be planned if the baby needs a procedure immediately after birth. If the baby has problems with either too fast or too slow heart rates, then medicines can be given to treat that. Also importantly, it gives parents time to educate themselves about the heart condition and the treatment or surgeries that may be required after birth.
What are the most common CHD seen in Down syndrome?
The most common CHD noted in Down syndrome are AV canal defect (also called atrioventricular septal defect - AVSD) and ventricular septal defects (VSD). AVSDs account for 1/3 of all heart disease in Down
syndrome. In an AVSD, the valves in between the upper and lower chambers of the heart do not develop normally and, in addition, there may be holes in the wall between the upper and lower chambers of the heart. A VSD is a hole in the wall between the two lower pumping chambers of the heart. The other defects
that are common are an atrial septal defect (ASD - a hole in the wall between the upper chambers of the heart) and a patent ductus arteriosus (PDA - an artery that connects the two large arteries arising from the heart. This is present in all fetuses and typically closes within 2 weeks after birth).
Is there a CHD which may suggest the possibility of Down syndrome in a fetus?
Occasionally, a diagnosis of Down syndrome is made after the discovery of an AVSD on a fetal echo since this condition is
“Is there a CHD which may suggest
the possibility of Down syndrome
in a fetus?”
20IS
SU
E 2
7 . 2
020

FE
AT
UR
ES

FE
AT
UR
ES
/ TH
EM
Ecommonly associated with Down syndrome. Interestingly, patients with Down syndrome tend to have a “complete” form of AV canal defect with a large VSD component, whereas babies with an AV canal but no Down syndrome tend to have more partial AV canal and more abnormalities of the left side of the heart.
If my baby has a CHD, what does that mean for the pregnancy and delivery?
That depends on what CHD the baby has. In the most commonly seen abnormalities such as AVSD, VSD and an atrial septal defect, there is usually no effect on pregnancy nor mode and timing of delivery. However, it is standard to evaluate the baby and perform a pediatric echocardiogram soon after birth to confirm or rule out any abnormality. If the baby indeed, has a significant narrowing, then an intravenous medication may be required to open up the artery connecting the two large arteries exiting the heart (the PDA) and these babies will need surgery soon after.
Are there any interventions that can be made in utero?
For the most commonly noted CHD in Down syndrome, no intervention is required in utero. However, rhythm problems (such as with a very fast heart rate) may be treated by giving the mother medications.
Does CHD in Down syndrome always need surgery?
No. A complete AVSD almost always needs surgery and this is typically done between 3-6 months of age. A large VSD also needs surgery by 3-6 months. However, with
an ASD or a VSD where the lung pressures are normal, surgery may be delayed for a few years if the defect is moderate in size or not needed at all, if small.
What results can we expect with surgery?
In the current era, babies with Down syndrome have a similar survival to that seen in babies without Down syndrome for the most common heart defect surgeries. They may however, have a longer stay in the hospital. This may either be secondary to feeding issues in younger babies as well as post-operative infections and lung issues.
Can I continue to see my obstetrician and deliver my baby locally?
Yes, in the vast majority of cases. Most of the common heart defects in Down syndrome do not require surgery at birth and are best addressed in the first few months of life (and in some cases even later).
Can I have a vaginal delivery?
Yes, in most of the cases.
Should my baby have a postnatal echo even if I had a normal fetal echo?
Yes. Since the incidence of heart disease is very high (~50%) in Down syndrome, all babies with this condition should have an echocardiogram at birth (or definitely within 6 weeks) - even if they have had a normal fetal echocardiogram. This is since the fetal echo may miss some abnormalities of the pulmonary veins and the aorta. Moreover, there are some conditions (such as a PDA) which are normal in pregnancy and can only be diagnosed as abnormal if they have not closed after birth.
In the current era, babies with Down syndrome have a similar survival to that seen in
babies without Down syndrome for the most common heart defect surgeries.
22IS
SU
E 2
7 . 2
020

FE
AT
UR
ES

FE
AT
UR
ES
/ TH
EM
E
How common is congenital heart disease in children with Down syndrome?
About 0.7% of infants are born with some form of congenital heart disease, ranging from minor defects to complex, life-threatening cardiac malformations. This prevalence is increased to about 40-60% in infants born with Down syndrome.
Why is congenital heart disease so common in children with Down syndrome?
There is a clear genetic basis to heart disease seen in children with Down syndrome. While not all genetic mechanisms have been completely identified, a variety of potential genes have been found to be associated with associated cardiac (and non-cardiac) problems.
How is congenital heart disease usually
diagnosed?Echocardiography, which is an ultrasound
of the heart, is used to delineate the structure and function of the heart. It is the ideal imaging modality to identify cardiac defects.
Are there other (cardiac) test that may be needed in children with Down syndrome who have congenital heart disease?
All patients will usually have a standard 12-lead electrocardiogram. On occasions, a cardiac CT or MRI scan may be needed. Very rarely, a diagnostic heart catheterization procedure has to be performed.
When is the diagnosis of congenital heart disease usually made?
If the diagnosis of Down syndrome was made during pregnancy, then usually a
Early Childhood: Down Syndrome and Congenital
Heart DefectsRalf J. Holzer, MD MSc FACC FSCAI
David Wallace – Starr FoundationProfessor of Pediatric Cardiology
Chief, Division of Pediatric CardiologyWeill Cornell Medicine
Director, Pediatric Cardiac CatheterizationNewYork-Presbyterian Komansky Children’s Hospital
Down Syndrome Amongst
Us
24IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
/ TH
EM
E
fetal heart scan (echocardiography) is being performed, which is able to identify the vast majority of the more significant cardiac abnormalities. However, even a specialized fetal scan may not be able to detect all forms of congenital heart disease, in particular smaller septal defects (ASD, VSD) or abnormalities of the aortic arch (e.g. coarctation). As such, a postnatal scan is usually recommended, in particular if someone identifies a heart murmur, or any abnormalities on EKG, or abnormalities of blood pressure and/or oxygen content after birth. If the diagnosis of Down syndrome is made after birth, then every child will require a cardiac echocardiography to rule out any cardiac defect.
What are the most common heart defects in Children born with Down syndrome?• Atrioventricular Septal Defect (AVSD):
~25-30% of CHD in Children with Down syndrome
• Ventricular Septal Defect (VSD): ~20-25% of CHD in Children with Down syndrome
• Atrial Septal Defect (ASD): ~20% of CHD in Children with Down syndrome
• Tetralogy of Fallot (TOF): ~4-5% of CHD in Children with Down syndrome
• Persistent Ductus Arteriosus (PDA): ~15% of CHD in Children with Down syndrome
• Other Congenital Heart Disease (including complex CHD): ~5-10% of CHD in Children with Down syndrome
If a heart defect is identified, does my child require any treatment?
This depends on the type of heart defect (more details below) and its size. As a general rule, about 50% of children with Down syndrome who were born with a congenital heart defect require heart surgery early in life. Some defects can be just watched and monitored with regular follow-up visits in clinic, while other defects can get smaller with time, or may even correct themselves completely. The latter applies to small ASDs, small VSDs (in particular those surrounded by thick muscle), as well as PDAs. However, certain forms of congenital heart disease,
such as an atrioventricular septal defect or Tetralogy of Fallot, do not have any propensity to correct themselves completely.
My child requires heart surgery: is the outcome any worse in patients with Down syndrome?
Studies have looked at important outcome parameters after heart surgery in children with Down syndrome. With current management, there is no significant difference in terms of survival after open heart surgery, and there is no difference in the frequency of tracheostomy (a special form of airway management). There is however a difference in the length of hospital stay with patients with Down syndrome staying longer in hospital. This is mainly due to the time it takes to start feeding, and some children with Down syndrome may require a temporary gastrostomy/feeding tube after surgery.
My child requires open heart surgery: how long can I expect to stay in hospital?
A lot depends how early surgery needs to be performed and what type of underlying heart defect is present. If a child with Down syndrome requires surgery in the neonatal period, then the length of stay may be as much as 3 weeks, often related to feeding problems after surgery and the need for the infant to “learn” how to feed. Later during infancy, recovery may be quicker, and the time to discharge in some infants with VSDs where the child was feeding well before the procedure could be as little as 4-5 days from the time of surgery.
Can you tell me more about the most common cardiac defects associated with Down syndrome?
Atrioventricular Septal Defect (AVSD)Definition: This is a malformation of the
central portion of the heart, where there is one instead of two separate AV valves, and defects of the atrial and/or ventricular septum above and below the AV valves.
25
ISS
UE
27
. 202
0

FE
AT
UR
ES
/ TH
EM
ESymptoms: Symptoms depend on the size
of the holes and the functioning of the AV valves (such as presence of leakiness). Some patients with Down syndrome may not have any symptoms, while in others symptoms are present early and worst around 4-6 weeks of age. Symptoms are non-specific and can also occur with other unrelated medical problems, but in general include heavy and fast breathing, breathlessness and tiring with feeds, sweating with feeds, and poor weight gain (failure to thrive). The lack of or improvement of symptoms does not always mean that defects are getting smaller, and in fact can sometimes be a warning sign with the need to perform surgery earlier.
Management: Surgery is required in the vast majority of patients. Large defects are usually corrected between 3-6 months of age, while smaller ones occasionally are deferred until 4-5 years of age. Some patients may require diuretics (water medicine) and other medication until the time of surgery.
Surgical mortality: The surgical mortality is about 1-2%
Long-term outcome: The long-term outcome is generally good. While surgery can improve valve function, it does not make the valves normal. Some patients have leakiness or narrowing of the AV valves even after surgery, and very few may require further valve surgery or even valve replacement in the future.
Ventricular Septal Defect (VSD)Definition: This is a defect of the wall
between the two pumping chambers. Some defects are surrounded by muscle (muscular VSDs), while others are located closer to the aortic valve within the membranous portion of the ventricular septum (peri-membranous VSDs).
Symptoms: Symptoms depend on the size of the defect. Similar to AVSDs, some patients with Down syndrome may not have any symptoms, while in others symptoms are present early and worst around 4-6 weeks of age. Symptoms are non-specific and can also occur with other unrelated medical problems, but in general include heavy and
fast breathing, breathlessness and tiring with feeds, sweating with feeds, and poor weight gain (failure to thrive). As mentioned for AVSDs, the lack of or improvement of symptoms does not always mean that defects are getting smaller, and in fact can be a warning sign to perform surgery earlier.
Management: Management options depend on the size of the defect. Large (non-restrictive) defects need to be closed surgically within the first 3-6 months of life. If the defect is small enough to protect pulmonary artery pressures (pressures in the lungs), then surgery can often be deferred and patients can initially be managed medically. Some defects, in particular smaller muscular VSDs, can close completely over time, while others can become so small, that no medical or surgical therapy may be needed. Similar to AVSDs, some patients may require diuretics and other medication until the time of surgery.
Surgical mortality: The surgical mortality is about 0.6%
Long-term outcome: The long-term outcome is excellent. Patients who had successful closure of their defects, may not require any cardiac procedure for the rest of their lives. Patients with small (residual) defects should be followed loosely once a year, in particular if the defect is closely related to the aortic valve. Very rarely, a small defect may over time make the aortic valve leaky, in which case such a defect would then need to be closed surgically.
Tetralogy of Fallot (TOF)Definition: This is a combination of a
ventricular septal defect (defect between the two pumping chambers), the aorta being pushed anterior (to the front) and thereby being located right on top of the VSD (overriding the VSD). This then creates a narrowing of the blood flow to the lungs either at the valve, or more commonly below the valve, combined with thickening of the right heart muscle that tries to overcome the narrowing towards the lungs.
Symptoms: Symptoms depend on the degree of narrowing towards the artery going to the lungs. In severe forms, patients are very blue as there is not enough blood
26IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
Contact Us 212-746-3561 Our Locations Upper East Side: 525 East 68th Street Lower Manhattan: 156 William Street
Compassionate, cutting-edge pediatric and fetal cardiology care for you and your family.
The Pediatric Cardiology Service at Weill Cornell Medicine has expertise in a wide range of cardiac conditions including:
Congenital heart disease Heart murmur Arrhythmias Chest pain Palpitations Cardiomyopathy Kawasaki disease Marfan syndrome Syncope (fainting) Fetal heart care (pre-natal/post-natal) Holter and event recording Transition to adult care Care for adult patients whose heart disease is congenital or acquired Other complex and common cardiology conditions
Affiliated with NewYork-Presbyterian, New York City’s #1 ranked children’s hospital in U.S. News & World Report
weillcornell.org/services/pediatric-cardiology
reaching the lungs to carry the oxygen needed in the body. This can present as sudden “blue spells” where the lips and tongue/face of the child become very dusky (which is an emergency and requires to see a doctor immediately). At the other end of the spectrum, if the narrowing to the lungs is extremely mild, then symptoms may resemble those of an isolated ventricular septal defect.
Management: Surgery is required in all of these patients. In the absence of “blue spells”, surgery is usually performed between 3-9 months of age, and involves the closure of the VSD, as well as enlargement of the pathway to the lungs using a patch. If blue spells are present early in life, the child may need an additional form of blood supply to the lungs, which can be delivered through a shunt (a connection created surgically between a systemic artery and a vessel to the lung, usually using a small Gore Tex tube). Some patients may undergo heart catheterization under X-ray guidance and have either a stent placed towards the lungs, or through a small persistent arterial duct (if still present). If patients are “blue” early after birth, they may be started on a special medication (called prostaglandin) directly after delivery to allow extra blood flow going to the lungs via an arterial duct, until a more permanent source can be created through either surgery or cardiac catheterization. Patients who underwent a shunt procedure, usually undergo full surgical correction closer to the end of the first year of life.
Surgical mortality: The surgical mortality of the “full” correction is about 1-2%
Long-term outcome: The long-term outcome is good. However, it is important to emphasize that “full surgical correction” does not mean that the heart is now normal. Patients will always need follow up and usually require additional surgical and/or transcatheter procedures later in life. The need for additional procedures is due to often residual or recurrent narrowing of the blood vessels going to the lungs, as well as the need for a competent pulmonary valve later in life (which in many patients can be implanted using a transcatheter approach, thereby avoiding open heart surgery).
Atrial Septal Defect (ASD)Definition: This is a defect of the wall between the two
collecting chambers.
Symptoms: Most patients do not have any symptoms the first 1-2 decades of life. However, changes within the heart such as right heart dilation are present much earlier, and are the reason to proceed with transcatheter or surgical closure. A few patients with Down syndrome may have non-specific symptoms that are difficult to attribute to other causes, which may or may not disappear after closure of the defect.

FE
AT
UR
ES
Management: These defects will require closure, usually performed sometime between 1-5 years of age. 90% of defects can be closed using a minimally invasive heart catheterization procedure (suture-less, just through a small puncture in the groin), where patients have no scars and are discharged the day after the procedure. 10% of patient will require open heart surgery.
Surgical/Cath mortality: The surgical mortality is about 0.29%. Mortality associated with a minimally invasive transcatheter approach is less than 0.1%.
Long-term outcome: The long-term outcome is excellent for both, surgery and heart catheterization, and patients are expected to live a completely normal life (in relation to the heart).
Persistent Ductus Arteriosus (PDA)Definition: A PDA is present in all babies
in the womb to allow blood to bypass the lungs. It usually closes after birth. When it does not close, then it is called a persistent ductus arteriosus.
Symptoms: Most patients do not have any symptoms whatsoever. Very few infants can present with symptoms that resemble those of a VSD, such as heavy and fast breathing, breathlessness and tiring with feeds, sweating with feeds, and poor weight gain (failure to thrive).
Management: As many PDA close spontaneously, most patients are observed conservatively for the first year of life, unless symptoms require to have the PDA closed earlier. If a PDA has not closed by 1 year of age, it is unlikely to close on its own, and then usually the duct can be closed using a minimally invasive cardiac catheterization procedure.
Cath mortality: The mortality associated with a minimally invasive transcatheter approach is less than 0.1%.
Long-term outcome: The long-term outcome is excellent and patients are usually discharged from follow up one year after the transcatheter procedure.
ACCESS HOTLINE
1-800-603-OHEL LIVE HELP ONLINE
www.ohelfamily.org CONFIDENTIAL RESPONSE
When an individual with developmental disabilities enters the world of OHEL Bais Ezra,
their lives change forever. Every day.Foundation for Independent Living • 24/7 Housing & Supported Apartment Program • Day Habilitation • Vocational Training & Employment
Community Services • Respite Programs: In-home, End of Summer, Shabbatons • Support Groups • Sibshops • Community Habilitation • Family Support Services
NEW First-of-Kind Program Autism Awake: Recreational over-night program that provides additional respite for families.
28IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
TikvahPesachC L I N I C A L , R ES I D E N T I A L & S U P P O RT S E RV I C ES
� � � � � � � T H E D O O R O F H O P E������� ������� ������������������ �������������� ������������� ���������������� ������������������� .

FE
AT
UR
ES
/ TH
EM
E
Down Syndrome and Pulmonary Hypertension
“My baby has already been seen by her cardiologist, so why
are we seeing another cardiologist?” This is a very common question I am asked, when I consult on a child with Down syndrome and pulmonary hypertension. Most infants with Down syndrome (DS) in the current era have been diagnosed prenatally and families do know what to expect with regards to congenital heart disease, hypothyroidism, gut abnormalities etc. But pulmonary hypertension is something that really cannot be predicted with prenatal echocardiography or ultrasound scans or by any other form of routine testing.
What is pulmonary hypertension? Simply speaking, it means high blood pressures in the pulmonary arteries. When we speak of high blood pressures in an adult, we are referring to pressures in the aorta and its branches, something we can measure using a BP cuff
around the arm or leg. But pulmonary hypertension (PH) refers to high pressures in the pulmonary arteries which take blood from the right ventricle to the lungs. The only way to suspect PH is by doing an echocardiogram where the cardiologist gets indirect evidence of increased pressures in the right side of the heart and pulmonary arteries. PH can be confirmed by cardiac catheterization where the pressures are directly measured in the “Cath lab” and the child is usually under anesthesia for the procedure.
There are multiple reasons why children with Down syndrome develop PH. Firstly, they may have persistent PH of the newborn. All babies are born with high pressures in the right side of the heart. But in most babies, this comes down rapidly to normal levels (of 20% of the left sided pressures) in a few days to a few weeks. If the normal decrease in right sided pressures does not happen (due
Usha S. Krishnan, MD, DM, FAHAProfessor, Pediatrics (Cardiology) at CUMC
Associate Director, Pulmonary Hypertension Center
Columbia University Irving Medical Center
New York, NY 10032
Tel: (212)3054436 Fax: (212)3421443
Down Syndrome Amongst
Us
30IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
to various newborn causes including DS), we call this condition as persistent PH of the newborn or PPHN. Often this may just represent a delay in the normal process and the baby recovers after initial intensive care and doesn’t need long-term PH medications. In some infants, the pressures do not come down and they may need specific testing and directed therapies for their PH.
Nearly half of all infants with DS have heart defects, commonly, patent ductus arteriosus, ventricular septal defect or atrioventricular septal defects. Babies with large PDA or VSD with DS can develop PH early because of large shunts and may need earlier surgery than non-DS infants. Atrioventricular septal defects are caused by failure of complete formation of the walls between the two sides of the heart and separation into right and left atrioventricular valves. The baby often develops symptoms very early and may need a lot of help with feeding, breathing and growth. They usually need surgery in the first 2-6 months of life. These infants develop PH because of excessive blood flow to the lungs from the shunts within the heart. After surgery, they may have residual defects and the pulmonary hypertension may persist. When an infant has congenital heart disease involving elevated pressures in the left side of the heart they can develop PH because of backpressure into the pulmonary capillaries within the lungs. At baseline or after surgery, if there is significant mitral valve regurgitation (leaking) or valve narrowing, or if there is narrowing of the pulmonary veins coming to the left atrium, there is back pressure into the lungs, causing PH. These children may need reoperation to fix the mitral valve or pulmonary veins as the case may be.
Even without congenital heart disease, babies with DS can have PH. They are often born with immature lungs, lungs which have not developed normally (hypoplastic lungs or simplified alveoli), or lungs with subpleural cysts in them. Because of abnormal lungs, they are prone to infections leading to further lung damage, leading to inflammation and secondary PH. Infants with DS may have bronchomalacia, where the larger airways may collapse (because they are softer), and
this can lead to collapse of the lungs beyond, leading to inflammation and PH. Older children with DS often develop enlarged tonsils and adenoids or their large tongue may obstruct the airways during sleep and they can develop obstructive sleep apnea, which results in PH. These children may need their tonsils and adenoids removed and older patients may need CPAP to keep their airways open and prevent obstructive sleep apnea.
Infants and children with DS often also have gastroesophageal reflux (GER), which causes stomach acid/ and foods to come up the food-pipe, and sometimes enter the airways. This leads to aspiration pneumonias and lung infections and damage with associated PH.
So, in answer to the question, why are you seeing my child, I do give a detailed explanation to my families, and also evaluate for these issues which may impact the care of a child with DS and PH.
WWW.YIDDISHPLAYS.COM
5
SPECIAL ENTERTAINMENTFOR SPECIAL CHILDREN
31
ISS
UE
27
. 202
0

FE
AT
UR
ES
/ TH
EM
E
Cardiac Care of the Adult with Down Syndrome
Congenital Heart Defects in Down Syndrome
About 50% of babies born with Down syndrome will have some form of a congenital heart defect. Congenital heart defects result from disruption of the normal development of the heart chambers, valves and/or arteries in the first three months of pregnancy. These defects are diagnosed by performing a heart ultrasound (echocardiogram) during pregnancy or shortly after birth. Babies with significant heart defects often develop clinical signs and symptoms including a heart murmur, low oxygen level (cyanosis), fast breathing, or difficulty feeding and growing. The majority of babies with Down syndrome will need to have one or more surgical or catheterization interventions early in life to counteract the effects of the congenital heart defect and allow the child to grow and develop. Over the past 20 years the results of surgery and catheter-based interventions for congenital heart defects have improved dramatically, to the point where the vast majority of patients are
now expected to survive to adulthood. As a result of these remarkable improvements, the cardiac care of adults with Down syndrome and congenital heart disease plays an important role in allowing Down syndrome patients to maintain a good quality of life as they age.
Late Effects of Congenital Heart Defects
Interventions to treat congenital heart defects are performed with the goal of normalizing blood flow through the heart and improving heart function. The interventions performed are tailored to the specific type of congenital heart defect present. In broad strokes, interventions to correct congenital heart defects include establishing normal connections by closing or opening holes between heart chambers, redirecting blood to and from major arteries and repairing or replacing narrowed or leaking valves. In some cases, bioprosthetic or artificial materials are used to achieve these goals. While interventions for congenital heart defects
Daphne T. Hsu, MDProfessor of Pediatrics, Albert Einstein College of Medicine
Director, Montefiore Adult Congenital Heart Disease ProgramChief of Pediatric Cardiology and Co-Director of the Pediatric Heart Center,
Children’s Hospital at Montefiore
Down Syndrome Amongst
Us
32IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
/ TH
EM
E
result in remarkable clinical improvements, patients with repaired congenital heart defects can develop symptoms from cardiac issues as they age. Thus, all patients with congenital heart disease, particularly those with Down syndrome, require regular heart monitoring throughout their life.
Cardiac Issues in Adult Patients with Congenital Heart Disease
The cardiac issues that arise in adults with congenital heart disease fall into four main categories:
1. Residual congenital heart lesions: leaking valves, narrow arteries, residual holes in the heart, or undersized heart structures because of growth failure
2. Heart dysfunction: impaired pumping or filling of the heart
3. Arrhythmias: tachyarrhythmias (too fast) and bradyarrhythmias (too slow)
4. Adult-onset heart disease: hypertension, stroke, coronary artery disease
If one or more of these issues arise, they can lead to symptoms of heart failure such as fatigue, exercise intolerance, trouble breathing, edema, poor weight gain, dizziness or fainting.
CoMorbidities in Adult Patients with Congenital Heart Disease
Patients with congenital heart defects can have abnormalities of organ function that may exacerbate cardiac issues. In patients with Down syndrome, obstructive sleep apnea is common and can contribute to heart failure by causing high pressures in the lungs and worsens symptoms of fatigue and exercise intolerance. Scoliosis is common in patients with congenital heart disease and can impair lung function and negatively affect exercise tolerance. Lung function can also be impaired due to restrictive lung disease following a sternotomy or thoracotomy. Neurologic issues such as a stroke or transient ischemic attack can occur in patients who have a residual hole in the heart because the hole allows a clot to travel from the right to the left side of the heart and then to the brain. Kidney function may be impaired in the patient who has undergone
open heart surgery or has heart failure and can worsen water retention. Liver disease such has hepatic cirrhosis or hepatocellular carcinoma has recently been recognized as an important noncardiac complication of elevated right heart filling pressures. Obesity, type 2 diabetes, polycystic ovary disease can accelerate the development of adult-onset cardiac diseases.
Monitoring of the Adult Patient with Congenital Heart Disease- Who, What, Where and When?
Who: As an increasing number of patients with congenital heart defects survive into adulthood, the need for subspecialists with expertise in the issues facing the adult with congenital heart disease has grown. Recently, fellowship training programs for adult or pediatric cardiologists who have an interest in adult congenital heart disease have been established with a focus on improving the long-term outcomes of congenital heart disease by establishing methods to best evaluate and treat affected patients. Subspecialty board certification in adult congenital heart disease is now offered by the American Board of Internal Medicine to those who have completed a fellowship. Currently, the number of cardiologists who have completed fellowship training programs is small and unable to meet the growing needs of adult congenital heart disease patients. Luckily, a cadre of adult and pediatric cardiologists who have longstanding clinical expertise in the care of congenital heart disease patients is also available to provide care to this population.
What: Monitoring of the patient with adult congenital heart disease includes:
1. Detailed history and physical examination
2. Noninvasive imaging (echocardiography, cardiac MRI, cardiac CT) to assess the function of the heart and the presence and severity of residual lesions
3. Arrhythmia evaluation with an electrocardiogram, 24 - 48 hour Holter monitoring and longer term rhythm monitoring
4. Exercise stress testing 5. Invasive testing such as cardiac
33
ISS
UE
27
. 202
0

FE
AT
UR
ES
/ TH
EM
Ecatheterization, electrophysiology testing. Decisions regarding the frequency and modes of testing that should be performed is dependent on the type of congenital heart disease, the presence of risk factors, and the severity of the clinical signs and symptoms. If a surgical or catherization-based intervention is being considered, more extensive testing including cardiac catheterization and/or electrophysiology testing is often performed.
Where: Adult patients with congenital heart disease and in particular those who have undergone surgical or catheter-based intervention often receive their care at centers that offer these interventions. The Adult Congenital Heart Disease Association maintains a database of adult congenital heart disease programs and the services offered at the programs (https://www.achaheart.org/your-heart/clinic-directory/). If a patient is geographically remote from an adult congenital heart disease program, patients may benefit from a “spoke and wheel” arrangement where the routine cardiac surveillance (clinical history, echocardiogram, electrocardiogram, rhythm monitoring, exercise stress testing) is provided by a local cardiologist with close review and collaboration with subspecialists in advanced imaging, cardiac catheterization, arrhythmia treatment, congenital heart disease surgery and heart failure at a comprehensive adult congenital heart disease program.
When: The American Heart Association and American College of Cardiology recently published the 2018 Guideline for the Management of Adults with Congenital Heart Disease (Journal of the American College of Cardiology VOL. 73, NO. 12, 2019). This extensive document outlines the rationale and general principles for the overall evaluation and management of patients with congenital heart defects and makes specific recommendations for timing and testing for each congenital heart defect. This guideline serves as an excellent roadmap for care for the adult congenital heart disease patient, however specific plans should be modified and tailored to individual patient’s needs and situation.
Treatment of Adult Patients with Congenital Heart Disease
The goals of treatment for cardiac issues in adult patients with congenital heart disease fall into several categories.
1. Symptom relief: Symptoms of heart failure can develop in adults with congenital heart disease and are most commonly the result of fluid retention or inadequate delivery of oxygen to the tissues. Fluid retention can be managed with the use of a diuretic to increase urine output. In patients with fatigue and an inadequate cardiac output initial treatment involves intravenous medications to acutely improve heart function, followed by neurohormonal blockade if the underlying issue is cardiac muscle damage. Surgical or catheter-based intervention is indicated if the underlying issue is a residual congenital heart defect.
2. Arrhythmia management: Patients with tachyarrhythmias can develop heart failure or syncope and are treated initially with antiarrhythmic medications chosen, based on the type of arrhythmia present. Catheter ablation, if successful, can offer a more definitive therapy for arrhythmia control. An anti-tachycardia pacemaker or implantable cardiac defibrillator (ICD) are also effective interventions to manage significant atrial or ventricular tachyarrhythmias. Patients with bradycardia can present with heart failure because the heart rate cannot keep up with demand. Pacemaker placement to increase the heart rate is often the treatment of choice.
3. Correction of residual defects: Surgical or catheter-based intervention for residual lesions are performed to relieve symptoms or may be performed in the asymptomatic patient to prevent a progressive decline in heart function. Decisions regarding invasive intervention requires the clinician and patient to critically evaluate the goals of treatment and carefully weigh the risks and benefits of the potential intervention against conservative management.
4. Management of end-stage heart failure: Adult patients with congenital heart disease can develop primary heart muscle dysfunction that is not caused by a residual heart lesion. If unresponsive to medical therapy, patients can be considered for a mechanical heart (ventricular assist device) or
34IS
SU
E 2
7 . 2
020

FE
AT
UR
ESAdvances in the diagnosis and treatment of congenital heart disease have resulted in
over 1.5 million patients surviving into adulthood in the US. These patients deserve specialized care
that can be provided in an Adult Congenital Heart Disease program. Daphne T. Hsu, MD, Director of the
Montefiore Adult Congenital Heart Disease (MAtCH) Program leads one of only two such programs in New York
State. The program’s highly-trained experts in pediatric cardiology and Adult Congenital Heart Disease (ACHD)
understand the intricacies of congenital heart disease and provide comprehensive medical, interventional and
surgical treatment for children, adolescents and adults. The Montefiore-Einstein commitment to providing this type
of cutting-edge care is helping to change the face of cardiovascular medicine and the futures of millions.
To learn more about MAtCH, visit www.cham.org/ACHD
or call Montefiore’s Adult Congenital Heart Disease Program at 718-920-5882.
Children’s Hospital at Montefiore is
consistently ranked nationally by U.S. News & World Report in areas including Cancer,
Gastroenterology and Gastrointestinal Surgery,
Neonatology, Nephrology, Neurology and
Neurosurgery, Orthopedics and Urology.
A BRIGHTER OUTLOOK FOR THOSE WITH CONGENITAL HEART DISEASE

YID
DIS
HE
NA
CH
AS
36IS
SU
E 2
7 . 2
020

YID
DIS
HE
NA
CH
AS
37
ISS
UE
27
. 202
0

FE
AT
UR
ES
/ TH
EM
Eheart transplant procedure.
5. Prevention or treatment of adult onset cardiovascular disease: As patients with congenital heart disease age, they are not immune to the development of adult-onset cardiovascular disease. Literature has suggested that Down syndrome patients may be less predisposed to the development of coronary artery disease. Nonetheless, interventions that can reduce obesity, manage hypertension and avoid type 2 diabetes should be implemented.
6. Pregnancy: Pregnancy results in a significant increase in circulating blood volume in order for the maternal circulation to support the fetus. At the time of delivery there are also significant changes in blood pressure and volume that occur. In patients with certain types of congenital heart defects, an increased volume load and pressure load can lead to the development of heart failure and/or arrhythmias. Pre-conception counseling is essential to decide if the initiation of medical, surgical or catheter-based interventions prior to pregnancy are indicated. During pregnancy, the management of the pregnant patient with congenital heart disease should be multidisciplinary with participation from obstetrics, nursing, cardiology, anesthesia, and neonatology.
7. Pulmonary hypertension: Although decreasing in frequency, pulmonary hypertension remains an important cause of morbidity and mortality in the adult congenital heart disease patient. Management strategies include removing the stimulus to pulmonary hypertension, treatment with pulmonary vasodilators, and in rare cases heart-lung transplantation. Patients with pulmonary hypertension should have careful management at adult congenital heart disease specialty centers.
Special Treatment Considerations for the Adult with Congenital Heart Disease
1. Exercise: Patients with significant residual lesions, heart failure or pulmonary hypertension do require exercise restrictions. For the majority of patients with mild or repaired congenial heart defects, exercise
restrictions are rare in patients and recreational sports are encouraged because of the benefits of decreasing risk factors for adult-onset cardiovascular disease. Patients with Down syndrome who do not have pulmonary hypertension should be encouraged to exercise regularly.
2. Endocarditis prophylaxis: The recommendations for the use of antibiotics for endocarditis prophylaxis were revised in 2007. The use of antibiotic prophylaxis was limited to select groups of patients at high risk for infective endocarditis. These groups included patients who have prosthetic valves or prosthetic material used in a valve repair, patients who have had endocarditis in the past, patients who have low oxygen saturation, patients who have undergone placement of patch material in the heart within six months and patients who have undergone a heart transplant and have a valve abnormality.
3. Dental Care: Regular dental cleaning is recommended for all patients with particular attention to those patients in the groups at high risk for infective endocarditis listed in the previous section.
4. Diet: No particular dietary restrictions are recommended for patients with congenital heart disease. A heart-healthy diet that maintains an ideal body weight and prevents type 2 diabetes and hyperlipidemia is recommended. Patients who are taking warfarin should follow a diet that limits or standardizes intake of Vitamin K rich foods.
Cardiac Care of the Adult with Down Syndrome: Summary
The success of cardiac surgery and catheter-based interventions in the management of the Down syndrome patients with congenital heart defects has resulted in a remarkable increase in the number of Down syndrome patients who are living well into their adult years. Regular follow-up care by a specialist in adult congenital heart disease should be life-long. Routine surveillance for the presence of heart failure or arrhythmia has the potential to identify issues before they become clinically important. Treatment decisions should be made based on a careful assessment of the potential risk and benefits of all the potential options.
38IS
SU
E 2
7 . 2
020

FE
AT
UR
ES

FE
AT
UR
ES
/ TH
EM
E
Preparation is KeyRuchie Szlafrok - Orlansky, LCSW
Having your child undergo medical
testing, invasive procedures, surgery, or other medical interventions can be a very frightening experience for a parent. Even as an adult, these events can induce fear and anxiety; even more so for a child and especially for a child with a disability. Children with Down syndrome often have other medical conditions that require medical attention at various points in their lives.
Preparing your child properly for what they may experience is a key factor to avoiding a traumatic response as a result of medical intervention. Here are some to tips to help you prepare your child for their medical appointment.
1. Hospital/Office Tour A preliminary tour of the hospital or office can be helpful to acclimate your child to unfamiliar surroundings. Many hospitals
and medical offices allow this - you just need to ask in advance. The calmer and more prepared your child is, the easier it will be for the physician to treat your child. Having your child see the facility, meet the staff, and get familiar with the environment takes away some of the anxiety that your child may experience that day. This is most
helpful for children with Down syndrome as they often have difficulty processing change and adjusting to new things. This takes away a lot of the guess work for them and can help them know what to expect.
2. Social Stories This is
a safe and developmentally appropriate way for adults to give over information to children. You can do this yourself, or ask your child’s teacher or therapist to help you do it. Depending on the medical intervention your child will experience, include age appropriate depictions of the
Down Syndrome Amongst
Us
“Preparing your child properly for what
they may experience is key factor to
avoiding a traumatic response as a
result of medical intervention.”
40IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
procedure and facility, and pictures of your child in the story. Page by page, include scenes starting from the night before the intervention, all the way through the end of it. Step by step, depict what your child will see and experience. Review this book with your child a number of times and ask your child to summarize it for you to ensure they understand. Reward your child for his/her efforts. If you are short on time, you can find a number of children’s books at the library that address this topic as well.
3. Regulation Techniques Your child may get overwhelmed at points throughout the medical experience. It is important that your child know how to self-sooth or regulate themselves with your help. For example, teach your child a breathing technique. Smell the flower (Inhale) and blow out the candle (Exhale). This is a good tool to have in your back pocket so that if you see your child is getting nervous, you can focus on his/her breathing to help them relax. Many children with Down syndrome have difficulty with emotional regulation, so practicing this in advance can really help your child in the moment.
4. Preferred Objects If your child has a teddy bear, blanket or squish toy that they prefer to have with them, bring it along! This feeling of security and familiarity can help your child stay grounded and calm in an otherwise chaotic and confusing time.
5. Something New The medical world can be a scary and unfamiliar place for a child. Buy a new game or toy to keep your child occupied and distracted while they are in the waiting room or once they are recovering. The newness can be something that your child is excited about, and rewarding them for being brave and trying their hardest is something they may respond well to.
Ruchie Szlafrok-Orlansky, LCSW has over 15 years of experience working with children with disabilities. She works in private practice in Brooklyn and Monsey. For additional support, feel free to contact Ruchie at [email protected].
Minimum Patchke.Minimum Patchke.Maximum Crunch.Maximum Crunch.

FE
AT
UR
ES
/ TH
EM
E
On The Double…Hendy Rosner
Tell us about your double surprise birth…
On Erev Sukkos, September 22, 2010, 5 minutes before the zman of Yom Tov, after a very challenging, high-risk pregnancy, which was threatened numerous times, our twin boys were born prematurely at 34 weeks. Right after they were born, the NICU team showed the babies to me and I was able to see them briefly before they were whisked away. Weighing approximately 3 pounds each, they were crying and seemed to be doing well. Nothing appeared to be suspicious…yet.
While I was in recovery, my husband went up to the NICU to see the babies. He was met with the concerned faces of doctors and nurses, while one of the twins was being examined with a Doppler for cardiac issues. After questioning, my husband was told that Twin A had a lesion in his heart and therefore they were examining Twin B as well. In addition, they seemed to be having characteristics of a syndrome.
There wouldn’t be a definite answer until further testing was done.
I was still in recovery. My husband’s facial expression upon his return to my bedside told me that something was very wrong.
It was after a long, tiring day; I was very weak and still being monitored closely. I was trying to process it all: how could it be that both might be having a syndrome and had the heart lesion? I had millions of unanswered questions… (at that point I was
not yet aware that they are identical twins) Meanwhile, I was reacting physically as well, with sky-rocketing blood pressure and heart palpitations with shivers. Since I was still in recovery, I was rushed for an EKG to make sure nothing else was happening.
The hospital staff was very nice and considerate about our situation and offered us a private room so that my husband could stay there with me all the time. The following morning, Sukkos day, my family and friends walked across the Williamsburg Bridge and came to visit me to the Manhattan hospital
Down Syndrome Amongst
Us
42IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
where I gave birth, but I refused to go see the babies with them. I was afraid of what the twins looked like. I envisioned them being attached to invasive medical apparatus and it frightened me.
When the babies were 2 days old, the doctors told us that their characteristics pointed to Down syndrome. A call on Hoshana Raba confirmed it. Both twins were indeed born with Down syndrome.
In addition to Down syndrome, what other challenges did your babies face?
They were medically frail, both born with congenital heart defects.
Describe each one’s congenital medical defects.
They both had an AV canal, a common heart defect in the Down syndrome population, which eventually needed surgical intervention to be corrected. Twin B had a slightly larger lesion than Twin A. We were told that typically this condition gets repaired at approximately 6 – 9 months of age, in order for the babies to first become bigger and stronger. This enables the surgery to be more successful and for the patient to have an easier recovery. (I was told at that point, that their heart is the size of a walnut, which makes it very complicated and risky to be worked on.) The cardiologist mentioned that right now my babies were very stable and doing well medically. When they were approximately 2 weeks old he even said, “Let alone their syndrome, I can’t believe how well they’re doing for 34 weekers.”
The twins came home when they were 4 weeks old. I had to visit the cardiologist every month until the team would decide when surgery could be considered. In the interim, my babies were doing very well. They gained weight nicely and were able to have their brissim at 6 weeks of age. The babies were named Yossi and Levi. Considering how well they were doing, I couldn’t believe that I had two cardiac babies home.
Take us down memory lane to the early stages of Yossi’s life.
Yossi was the first one to come home at 3 ½ weeks of age, weighing barely 4 pounds. Because he was doing so well otherwise, I was given the option to
Minimum Patchke.Minimum Patchke.Maximum Presentation.Maximum Presentation.

FE
AT
UR
ES
/ TH
EM
Etake him home. I was advised that I have to make sure he gets 35 ccs of formula at every feeding – it was not optional; it was a MUST. That was very challenging in the beginning because he sucked very slowly and kept on falling asleep. However, his cardiac condition didn’t play a major role at this point yet.
Now, take us down memory lane to the early stages of Levi’s life.
The same applied to Levi. He came home from the hospital a couple of days later than Yossi; his feedings were also slow and challenging, but the monthly visits to the cardiologist yielded positive results, with the babies gaining weight nicely.
On Motzei Shabbos January 1st, I suspected that Levi was breathing faster than normal, but doubted my self-assessment. By Wednesday, I put one baby next to the other one to compare their breathing. My doubts were confirmed. I became very nervous and called the cardiologist immediately. He told me to come see him the following morning. Since it was already 3 weeks past our previous appointment he asked that I bring Yossi along as well. With the help of my mother, we got to the doctor’s office Thursday afternoon. We were assigned to different examining rooms with each baby, where an echocardiogram was performed. The doctor then told us that Yossi’s echo looked fine, however, Levi developed a condition called pulmonary hypertension. This is a very devastating, rare condition where the pressure in the lungs is very high, therefore, the heart can not pump the blood as fast as it comes in. This results in a higher heart rate which causes the baby to breathe very fast. The doctor seemed very concerned.
In retrospect, I realize how naive I was and how serious Levi’s condition was. I can also say, since this a quite rare condition, regular cardiologists don’t have much experience in this field and we were therefore not under the proper care at the time.
As the weekend was progressing, Levi’s condition became obviously worse. He was
breathing faster by the hour. By Sunday morning, his breathing was so rapid that he was not able to drink his bottle. It was impossible for him to breathe and suck. Although I was told to come in Sunday night to get him prepped for his scheduled Monday morning catheterization, I realized we wouldn’t be able to wait. We arrived to the hospital Sunday afternoon and Levi was immediately put on oxygen and had a blood transfusion. I still didn’t realize how serious his condition was.
Thus began a dramatic journey that lasted a number of years, with Levi’s life hanging on a hair, with situations of touch ‘n go becoming the abnormal norm in our lives, of code blues, of droves of doctors performing CPR, of intubations and extubations and of our own hearts fluttering in fear.
Levi had three open-heart surgeries in a time span of 3 months, each one being 4 – 5 weeks apart. His first surgery was performed on Wednesday, February 2, 2011 to close up his AV canal. When the doctor came out of surgery, he reported that Levi’s mitral valve was very distorted. He had seen something like this before perhaps only once in all his doctoring years. Thank G-d he was able to repair it successfully and was hopeful. However, since Levi was in heart failure and very sick when he went into surgery, we were told that he had only a 70% chance of survival and would most likely have to come down from surgery on an ECMO machine. Boruch Hashem, he was able to come out of surgery ‘only’ on a ventilator, but the doctors were not able to close his chest because his heart was too big. This resulted in keeping him on paralytics until closure could be considered. It was also a grotesque and pathetic sight to behold. It took until the following Monday for closure of Levi’s chest to occur.
While all of this was occurring, the doctors suggested that because the babies are identical twins, there was a valid concern that we could have a ‘copy paste’ situation with Yossi. It was something we all wanted to avoid. So, on Friday morning, two days after surgery, while Levi was still so critical,
44IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
The Pixie Perfect Snack.
Only 14g sugar
No artificial color & flavor
Strawberry& Vanilla
Economical & Nutritious

FE
AT
UR
ES
/ TH
EM
EYossi came in for an evaluation to determine when surgery can be considered for him. After the appointment, my brother met us at the hospital, took Yossi home with him for Shabbos, while we stayed with Levi in the hospital.
After examining Yossi, his doctors advised that his heart be repaired asap so as not to take the same path as his twin brother. Yossi was scheduled for surgery for Monday, February 14th. In the ICU this was groundbreaking; they never had two brothers in the same unit simultaneously. Initially, for convenience sake, the twins were going to be placed next door to each other. Upon reflection, the medical staff changed their minds; the risk of mixing up babies and medications was too great. The babies were placed on opposite sides of the length of the hallway and there were color posters on each baby’s room reading, “I Am Yossi” and “I Am Levi”.
Yossi was extubated 3 hours after surgery, while Levi continued to struggle on the ventilator. The comparison hit me in the face: Levi was a very, very sick baby. Yossi returned home two and a half weeks after surgery. Levi was extubated and re-intubated in the interim. On March 8, he was finally extubated, but his breathing was very labored due to an obstructed aorta, which can happen in 5% of cases post-surgery, due to a very enlarged heart, which resulted from pulmonary hypertension. When things finally fell into place, scar tissue situated into the aorta; this literally obstructed blood flow to Levi’s body. Doctors were hoping that with support they’d be able to hold off from additional surgery so that Levi can grow bigger and stronger; he was all of 8 pounds at that point. The hope was short-lived and
Levi was scheduled for an emergency surgery, which took place on Friday, February 11th at 1 pm, to remove the scar tissue. The surgical team wanted to tighten Levi’s mitral valve as well, because they realized it was very leaky since its repair. The surgery was expected to last a minimum of 6 hours, which would take us into Shabbos. The zman was very early and we had no connection or support from anybody while this was occurring.
Levi responded immediately to the surgery and was actually doing better than ever before. His doctors were extremely pleased. They told us Levi would most likely be extubated the
following day, putting our hopes up high…but not for long… Within a few hours Levi developed fluid in his lungs, delaying
extubation. From then, things never became better – only worse. As the days progressed, Levi’s valve became more and more leaky, to the point where it almost wasn’t working. The nature of the distorted valve made it very complicated to be fixed. The medical team had tried their hardest and didn’t believe they would ever get to this impasse. Levi’s pulmonary hypertension acted up like crazy in addition to his mitral valve crisis. His prognosis at that point seemed very bleak. It was then that I begged Hashem to please do what’s good for my child. I couldn’t see Levi suffer any longer.
After intense testing and agonizing contemplation, with no options left, the doctors decided to replace Levi’s mitral valve. This procedure is very seldom done in kids so
46IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
/ TH
EM
E
young and of such low body weight (still only 8 lbs.) There were dual reasons for hesitation: putting a child on lifelong blood thinner is a struggle and this would now become the protocol for Levi, and when a valve is replaced in a child this young, it needs to be changed more often until the patient reaches adulthood.
Levi’s third open-heart surgery to replace his mitral valve was scheduled for Wednesday, March 13, four days before Pesach. After having been critically ill for so long, Levi was finally getting better, albeit very slowly. The situation seemed to be headed in the right direction with nurses commenting on Levi’s being more alert and not so irritable like he had been. Because Levi was doing better it was decided that I would stay with him for second days Pesach and my husband would stay at his parents with our children.
As I was packing my bags to settle in to the hospital for Yom tov, I checked with the nurse via telephone how Levi was doing. The situation wasn’t good. Once I arrived there, several ‘smaller’ issues had been resolved, like his clogged central line which had been delivering his medications and obviously couldn’t do its job when clogged. Later in the afternoon when Levi woke up, he was not doing well. The numbers on the ventilator had dropped and his oxygen level was not stable. As it was being monitored closely I suddenly noticed that Levi’s right foot was totally discolored. The nurse became extremely concerned, explaining that this was a sign of failed blood circulation to his right foot and she ran to call the doctor. Levi was heading towards sepsis; even though he was being treated with various anti-biotics, he was fighting a staphepi infection. The doctor was positive
that because the bacteria was identified, he would target it with different medications. However, as the night progressed, Levi’s condition deteriorated. Upon continued intense examination, it was determined that Levi also had a clot in his mitral valve. The situation was dire indeed. I was asked to leave the room and wait in the lounge. From my vantage point I was able to see white coats running in and out of the room. A very passionate floor doctor came to talk to me, offering to call my husband to come support me. Halachically, I wasn’t sure whether that was permissible. I dejectedly walked to the Bikur Cholim room, hoping to meet somebody who could advise me. There I met one religious Jewish man. I told him my baby was very sick and I was there myself, asking whether I was allowed to call my husband. He didn’t think so because my baby was under doctor’s care and it wasn’t pikuach nefesh. So, I went back up to the ward. In the interim, the doctors had reached the surgeon who told them that taking Levi in for another surgery was not an option; he would not survive. He suggested something totally experimental, something that was never tried on such a young baby – giving Levi TPA, a clot buster. TPA is usually reserved
for stroke patients, to resolve their clots immediately so no further damage would result. The risks of hemorrhaging from all major organs is always very high. Being that Levi was post-surgery and he still had central lines open, the risk was even higher. I gave my
consent because there was no other option and I figured I had nothing to lose. Then the cardiologist who was on call that weekend called me into a private room and said, “Mrs. Rosner, your baby is dying. I don’t think he
47
ISS
UE
27
. 202
0

FE
AT
UR
ES
/ TH
EM
Ewill make it through the rest of the day, not even the next few hours. Whoever from the family wants to be here…now is the time to come.” Teary-eyed and in a state of panic, I raced back to the Bikur Cholim room where I met the same gentleman I had seen earlier. I started screaming hysterically, “My baby is dying! What do I do? Should I still not call my husband?” He looked at me and advised that I may. I asked what I should do or recite at the baby’s bedside. He answered, “Say Shema Yisroel!” I so desperately needed someone to lean onto for emotional support, but surprisingly he didn’t offer to come join me in prayer. Only later did he apologize to my husband that he couldn’t come to the dying baby because he is a Kohein.
At this point I accepted the doctor’s offer to call my husband and after several tries at my in-laws’ home, my 15-year-old son picked up and he was told the baby is dying. He ran to shul to call my husband, who in turn, called a car service and came right to the hospital. In the interim I was sitting in the lobby sobbing. Levi’s room was besieged with medical personnel while all the other personnel from the floor, as well as social workers, tried talking to me. I didn’t remove my eyes from the entrance to Levi’s room. At one point I saw them taking in a CPR board, so I was sure they were giving it one more chance. At some point my husband arrived and the doctors apologetically told him that they’re trying their best. My husband ran to a corner to finish his prayers, not knowing what was coming. At around 2 pm doctors told us that Levi’s abdomen looked very distended and they were afraid he was hemorrhaging internally. They were going to do a scan to verify. At 4:30 they came to tell us that he was
not hemorrhaging, but because his kidneys and liver shut down he had no way to get rid of his body fluids, hence the distended abdomen. At 6 pm an echo was done to see whether the TPA was doing its job. The good news was that the clot did become smaller and there was more blood flow to Levi’s heart. At 10 pm, when we were finally allowed into Levi’s room, I was shocked to see a saturation level of 100%! I questioned one of the nurses how this was possible and she said, “Mom, we’re worlds away from where we were this morning.” I then questioned how they were able to maintain and bring up his oxygen levels when the ventilator was no longer able to do its job on Levi hours ago. She
told me something astounding: “Two nurses were manually bagging him for 8 hours, taking turns!”. I couldn’t believe it; the depth of their caring and belief that he could pull through were remarkable. Levi was still extremely ill, with only a 50% chance to make it. I
hadn’t seen him since morning and when I did go into his room, he was unrecognizable. His body was more wiring than baby and wider than longer (reminding me of Humpty Dumpty).
On Tuesday, Achron Shel Pesach, Levi was taken off paralytics and finally opened his eyes. He had completed the TPA stint, which cannot be administered for longer than 48 hours. He was so weak that he couldn’t even lift up his hand. But from then, there was slow but steady progress. By the following Monday, after being on a ventilator for four months, Levi was finally extubated. Thus, started a long road to recovery, with lots of ups and downs, the painful weaning of Levi off narcotics and getting him to breathe on his own. On June 3rd, after being in the
48IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
/ TH
EM
E
pediatric intensive care unit for 143 days, Levi was finally taken down to the main floor. In mid-July he was transferred to Children’s Specialized Rehab facilities. On August 15th, seven months from his initial hospitalization, Levi finally came home and reunited with the family. He was eleven months old, weighed a ‘whopping’ ten pounds, was on a 24-hour tube-fed drip and on eleven doses of medication daily.
Is there a great gap between Yossi and Levi developmentally?
Yes; quite significant
Why so?Because of Levi’s rocky road medically,
he was B’H saved but unfortunately came out of it damaged. Since he was ventilated for 4 months, his left vocal cord is paralyzed, leaving him with a hoarse and quiet voice, making it hard to be noticed and heard when among people.
In addition, as indicated above, there was no perfusion to his right foot at one point. This damaged his growth plates, causing a limb length discrepancy. According to doctors, his foot will only grow 30%. This condition already required 2 reconstructive knee surgeries. Limb lengthening is considered in the near future.
Levi’s general state of being is physically disabled (non-ambulatory) and verbally
affected. However, his cognitive function was B’H not affected. He learns and understands and can express his needs. He is very alert and smart and understands everything that goes on around him.
At which point did life finally settle down, or has it?
At about 2 years of age, when Levi was finally medically much more stable, life took on a new norm. B’H we are a busy, happy family with the twins keeping us entertained all the time.
Give us a brief current update on the twins
Yossi and Levi are best twin brothers, truly caring about each other. It’s funny to see how they can carry on a conversation and nobody can understand what they’re discussing, but they totally understand each other. It always amazes me to see how passionate Yossi is towards Levi. He lives and breathes Levi. The first thing he asks when coming home is, “Where is Levi?”. He will always schlep or carry Levi to places. If Levi is not okay or cries, Yossi gets teary-eyed as well.
The boys attend 2 different school programs. Because Levi is non-ambulatory, he was not able to go to Yossi’s school. This is quite challenging because I am dealing with two different school administrations. Thankfully, Levi is doing much better physically than when he was initially placed and we hope that eventually they can both attend the same educational program.
Can you share some final thoughts?At some point during our ordeal we were
told that the statistics of this happening, identical twins with Down syndrome, is one in a million. My husband and I look at our boys and then our eyes fall on Levi as we quietly whisper – ‘our son who died three times, yet is still alive’.
I sometimes wonder whether Hashem paired them up so that Yossi can always be there for Levi…a true Master Plan!
49
ISS
UE
27
. 202
0

FE
AT
UR
ES
ButterfliesShaindy Ziegler
SometimesYou form your fists
Into a heartCatch a butterflyPulsing within
Tender silkinessOf fragile wings
Beat inside your palmPotential, hopeVitality of life
Whispering on your skin
You smile, gently cajoling herThroughout her wobbly
Failed attemptsYour passion inspires
Hidden colorsYour love unfurls tentative wings
Suddenly you sense a bursting strengthOf graceful power
Twirling, dancing in achievement
Those breathless moments A magical display of possibility
Joy as vibrant as the flittering sensationYou draw it close to your chest
Heartbeat and butterflies fluttering in sync
Then it’s timeTo let go
Swallowing, blinkingYour heart returns to handsA trail of colors and blood
ReleasedAlong with a gust of emotions
You lean back, squintingChin pointing heavenwardThe spring breeze cooling
Your clammy fistsYou observe wistfullyProudly, longinglyAs the butterflyYour butterfly
Explores its independence amongThe sunshine dust and floral fragrances
Wings glinting in euphoria
Then you stare atYour empty palmsFlutters tingling
Colors echoing in the hollowness
AndYou form your fists into
A heartRaise it to the sun’s glowGold flooding the void
PerhapsYou’ll catch
Another butterfly.
Down Syndrome Amongst
Us
This poem was inspired while parting with my special needs students, evoking bittersweet emotions; just about when the progress finally started to show, summer arrived and it was time to let go.
50IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
At Hamaspik Theragen we are dedicated to providing individualized care to all
members of the I/DD community. Our care leads to real life advances for OPWDD
eligible individuals, from those who just graduated to experienced seniors.
It’s Therapy Centered Around You.
Introducing...
HamaspikTheragen
Physical TherapyOccupational TherapySpeech TherapySocial Work & Counseling
Providing clinical services
For the OPWDD population
Call Us 845.655.0600
HamaspikTheragen.orgPsychiatry ServicesPsychological EvalsNutrition Services
Brooklyn: 293 Division AvenueMonsey: 58 Route 59Monroe: 1 Hamaspik Way

FE
AT
UR
ES
The Bond That Ties…Sarah Sander
Dearest Morah –
Moishey is reporting almost on a daily basis that he is not behaving in school, and the various punishments that he is receiving.
Is this true, or is he just playing around with our blood pressure?
Gut Shabbos,Sarah Sander
Moishey was very “testy” yesterday; he took full advantage of having 2 substitute paras.
School Notice: May Schedule:Wednesday, May 24 – Staff Development
Day – No SchoolMonday, May 29 – Memorial Day – No
SchoolClerical Half Days: Tuesday, June 4 and
Thursday, June 13Dear Parents: The Chancellor has
designated the above-mentioned days as clerical half days. Please note the following: Pupils will be dismissed promptly at 11:30
Please Note: June 6 is Brooklyn Day; school will be closed.
Dear Morahs:
The principal told me that Moishey might be filmed today for some kind of internet program.
Please make sure that his grooming is impeccable: tucked in shirt, clean face, payos dampened and brushed straight down, glasses clean and worn over combed payos, yarmulke placed properly on head. Thanks so much. By having Moishey look his best, we will end up inspiring many people who have ignorant misconceptions about the DS population.
Thanks again –Sarah Sander
My Personal School Diary’
I had a surprise Mazel Tov that just happened and nobody in yeshiva didn’t hear
Down Syndrome Amongst
Us
School Home Moishey Himself
52IS
SU
E 2
7 . 2
020
Excerpts From Moishey’s Communication and Homework Notebooks Of His School Days

FE
AT
UR
ES
this big news and here is what is happening - my brother Shiya just started to have braces on his teeth and I am the Baal Hasimcha because of my brother.
Dear Morahs amush:
How true ‘Der Eibishter Shlugt nisht Mit Tzvei Shtekens’. Just this morning I was going to award Moishey with a ‘Monster of the Day’ certificate, so obnoxious was his behavior. How wonderful it was B’H when he arrived home from school with his ‘Student of the Month’ award. My heart swelled with pride. I guess we all deserve a Mazel Tov for making it possible.
Thanks for the uplift.
Gut Shabbos.Sarah Sander
Moishey’s Homework Sheet for Parshas Bo: Most of the Questions Have Been Skipped in Order to Get to the Prize at the End -
Teacher’s Responses are in parentheses:
1. What did Pharoh say to the Yidden? (work hard)
2. Pharoh took a cup of water. He started to drink and…(icchh! It was blood)
3. Moshe said… “If you don’t let them go, (frogs will jump on you”)
4. What did the Yidden carry? (matzos)
– Moishey’s initial response: roller skates
Dearest Morah R shetichya:
Thanks for a wonderful PTA meeting. My husband and I went out for dinner afterward, and even though I was starved I was hardly able to eat anything. I immediately became very full. I concluded that I must have been ‘plotzing’ with nachas B’H.
Thank you for being the source of Moishey’s progress B’H.
Sarah Sander
Dearest Morah R –
My husband has reached a grand conclusion: no more PTA meetings! If Moishey turns into a horror after glowing reports, then forget it. And if the reports are anything less than glowing, then who wants to hear?
How’s that?Sarah Sander
Teacher’s Response:
Fine with me.
Perhaps we should write a goal on Moishey’s IEP – ‘will tolerate praise without letting it get to his head.’
53
ISS
UE
27
. 202
0

FE
AT
UR
ES
Chapter 21Rana Reisman
THEY say it’s all about perspective.One door closes and another one opens.Chapters do as well, as they flow easily
from one to another.So here we are at Chapter 21.The transition from school to day hab.Why don’t I believe that?I’m trying to understand my feelings.What am I feeling?Angst?Uncertainty ?Stagnation ?Frustration?I’m having a difficult time having my son
Yehuda transition from his school years to day hab.
What’s the road ahead?Is this his future?
My son Yehudah is happily in day hab.He joins his friends and is busy with his
daily routine.He labels, sorts, packs his way through his
day.He truly seems to enjoy his work.He seems fulfilled.He seems to have transitioned smoothly
from his school days.But…
Gone are the therapies.Gone are the teachers.Gone are the little yellow school buses.Gone are the IEP meetings.Gone are the PTA meetings.Gone are the yearly goals.Gone Gone Gone...Is it all over?I spent Yehuda’s entire life pushing him to
achieve his goals, be it academic or personal.Has it come to a complete Stop??What’s next for him?
Who will encourage him to speak clearly?Who will work with him to write neater?Who will push him to increase his reading
comprehension?Who will push him to be more precise
with his addition?I guess the DOE has determined that age
21 is a fair cut off point to determine a child’s educational goals accomplished.
So what’s next?A person doesn’t simply fall off the planet
at 21…He needs to learn more skills:Job skillsInterpersonal communicationTravel training
Down Syndrome Amongst
Us
54IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
Ride the busesUse a metro cardBecome more independent by:Doing laundryPreparing mealsShopping for groceriesMaking personal decisionsMove out into a group home
Who will teach him these crucial skills?Who?
While I truly appreciate his day hab experience, and I see how happy and satisfied he is, I wonder what more he can accomplish.
He’s “working” .He’s learning in the morning and working
in the afternoon.He’s a “learner-earner” type of boy.
Is it possible to push these young people with disabilities to do more?
But then I wonder, given their cognitive delays coupled with their quirky behaviors, if working in a more mainstream environment is really feasible.
It’s a difficult balance between exposing him to the demands of the outside ‘real world’ and being nestled in the safety and security of his sheltered environment.
He needs both.The balance is tricky.
So, I need to adjust my expectations.Yehudah isn’t me .I’m a person who likes to accomplish.Yehuda is limited .And yet has so much potential.It’s sometimes frustrating to see where his
limitations lie.Maybe I’m guilty of transferring my own
unmet goals onto him?Maybe I’m transferring my personal
frustration with my untapped potential .
I sense his feelings of accomplishment doing the “jobs” he is given.
He’s happy. Go figure.I know many “typical people” who are
miserable, receiving little satisfaction from their jobs.
I see how comfortable and happy he is spending time with his peers, gaining a sense of satisfaction from his work.
Maybe he doesn’t need to run the rat race we are all accustomed to running.
Maybe he doesn’t need to accomplish more.
Maybe just “being”... is his goal, his journey.
Maybe just being satisfied with what he has going is enough for him.
Maybe.Maybe not.But I’m not satisfied.This cannot be the plateau.He needs to reach higherHe needs to be challenged further.His journey can’t be over.He needs to learn moreHe needs to accomplish moreHe needs to become more independent.
There is no simple and neat ending to this essay, as I don’t know what’s ahead.
Maybe I need to adjust MY expectations of where he is headed and what more he can accomplish.
Maybe, sadly, not much more.Maybe time has run its course and time
for improvement is up.MAYBE HIS PRESENT IS HIS FUTURE.Perhaps this stage is the end of the line.Maybe this is his plateau.I simply don’t know.And that uncertainty bothers me deeply.My job as his mother is far from over.I still have many goals for him to
accomplish.There is so much more I need him to be.But simultaneously, I take such pleasure
in his company, and truly enjoy him.But I do know one thing…And that is my complete and fully
encompassing love I have for him.And that will always be there, at any age.Because no one ages out of love .
55
ISS
UE
27
. 202
0

FE
AT
UR
ES
“We Cannot Let Them Suffer Alone”
Press Release by Office of Senator Simcha Felder
A longtime advocate for children with special needs, Senator Simcha
Felder, joined by a group of special needs children, families and educators converged at City Hall on November 12th and together delivered a strong and unified message: Mr. Mayor, keep your promise to thousands of special needs children and their families.
The group demanded that Mayor de Blasio finally force the Department of Education (DOE) into federal compliance with the Individuals with Disabilities Education Act (IDEA) and end the era of neglect and hardship suffered at the hands of DOE.
Standing outside together on the first frigid day of the year the Senator’s remarks warmed hearts and inspired cheers. “We are here for the kids and the parents. For the kids who are once again being neglected by the city, and for the parents who year after year suffer pain, humiliation and economic hardship from an abusive system.”
“There is no magic cure known to man for permanent conditions like Down syndrome and autism, so why are these parents under constant stress to meet numerous deadlines and submit mounds of documentation year after year to secure necessary services? It’s
unconscionable. Mr. Mayor, these children are just like all other children; they deserve the best education possible and they deserve your attention.”
“But, you have been negligent in your care for this vulnerable population. Repeated, well-documented efforts in the form of meetings, letters and phone calls to your office have all been ignored. For years,
parents of children with special needs have had to wait for the City to settle legitimate claims for tuition reimbursement. Left with no other choice, we have come here to stand at your doorstep, because we cannot let them suffer alone.”
“In 2014 you held a press conference where you said every child in this City
Down Syndrome Amongst
Us
56IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
deserves a quality education. ‘Today, we are turning the page, making changes that will ease the burden on these parents. We are cutting red tape, speeding up the process and reaching outcomes that do right by families.’ Those are your words. That was your promise in 2014. It is now 2019 and things haven’t changed.”
“Let me be perfectly clear, we are not asking for any favors. The City is lawfully obligated, under federal law (IDEA) to provide appropriate education and services in a timely manner. The deadlines are clear - at most it should take two months to resolve disputes and begin making reimbursements,
not two years! Unfortunately, that is now common.”
“The law has been ignored, the deadlines ignored, the bills ignored. NYC DOE is not in compliance with the law. New Yorkers are required to abide by the law. Compliance is not an option, it’s the law - and New York City is not above the law.”
“Please, Mayor de Blasio, keep your promise to these kids and their families. They’ve suffered long enough.”
Watch the video on Senator Felder’s website: https://www.nysenate.gov/senators/simcha-felder
"Disability is a matter of perception. If you can do just one thing well,
you’re needed by someone."
on
57
ISS
UE
27
. 202
0

FE
AT
UR
ES
Can I Have a Cookie?S.G. Rosenhan
“Mommy, cook-kie?”His limited
speech is endearing. This “cookie” is a new word. He pronounces it as if two words, but he definitely knows its meaning.
“No, we don’t have cookies for now.”“Mommy, cook-kie?”“Cookies are not for now.”“Mommy, want cook-kie!”It’s a legal holiday and he is home from
school. I am diapering the baby. She is trying to reach for the wipes, as I clean her. She twists her body as she pulls. I need to concentrate to avoid dirtying myself.
“No cookies now.”“Want.”“Come,” I hold out my one free hand.
The other is holding the now-clean baby. “Let’s go make lunch,” I say in an attempt to distract and get past this.
I am followed to the kitchen only to hear again “Mommy, cook-kie?”
His eyes beseech and I am tempted to give in to him. “No cookies now, we are making lunch.”
He eyes the potatoes, chicken and spices
on the counter. “No cook-kie?”Shake of the head; “no cookies”.
A half-hour of blissful quiet passes as I put together food for the family. He busies himself with clicks. The baby is in the swing.
“Mommy, cook-kie?”He is six years old. He is sitting on
the floor in front of a pile of clicks, his hands working determinedly, though unsuccessfully, to connect them. He is not even looking at me. When did he outgrow his short-term memory?
“Cookies are not for now.”“Like cook-kies.”
We distract by putting up another load of laundry…
“Look, your shirt is going into the washing machine.”
“Now, cook-kie?”“No.”“Want, cook-kie.”“See, now we are putting in the socks.”“Cook-kie.”
Down Syndrome Amongst
Us
58IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
As I clean out the boys’ room…“See, we found your lost shoe! Isn’t that
exciting?”“Now, cook-kie?”
As I organize and fold the stray blankets in the linen closet…
“Mommy, cook-kie, want.”
As I wipe down the kitchen table…“Mommy, see, cook-kie! Want cook-kie”
And waiting for the older ones to come home. “Mommy, cook-kie?”
He still has not given up. “No cookies before lunch.”
The kitchen table is cluttered with plates at various stages of lunch. Chicken bones lie randomly, uneaten peas roll about and mounds of overflowed ketchup decorate the tablecloth. A spilled cup of juice adds some color. He sits at his seat among the others picking at his food. “Mommy, want cook-kie?”
“But, you are in the middle of eating lunch.”
With a shake of the head “No `tato, want cook-kie.”
“Finish your lunch. It’s also yummy.”
I am sitting at the table. A 2nd grade math workbook is open on my left side with an 8-year-old writing in the answers. At my right is an English textbook open to a story being read by another daughter.
“Mommy, 16 divided by 4 is 4?”“Mommy, what does conquer mean?”“Mommy, cook-kie?”I turn around. He is right behind me,
trying his luck again.He’s cute. I smile at him “I am helping
with homework. No cookies now.”
He was all ready for bed, bathed in pajamas and cuddled on the couch treasuring the few minutes left until he would have to go in.
“Mommy, cook-kie?”Did he really think, after all this time?“You know what?” He looked up with wide, hopeful eyes.“You were such a good boy the whole
day. You cleaned up the clicks, let Mommy take care of the baby, got all ready for bed so quickly. You can have a cookie.”
The smile on his face was worth that cookie. With a jump, he ran ahead of me to the cabinet and watched, open eyed, with such anticipation as I took one cookie out of the package. His chubby hand reached out with the expectation of its treat. Cookie in hand, he settled on the couch to indulge its pleasure. He separated the sandwich and first licked out the sugary cream. Then with delicate bites finished off the cookies savoring each bit. I watched him in amazement as he ate.
When he was done, he came over to me and said with a smile as wide as a bridge “Thank you, Mommy. Like cook-kie,” then he planted a sticky kiss on my cheek.
Wow. He must have asked me over
100 times in one day. Despite all the negative responses, he kept requesting. No, persevering. Determined, he kept at his goal. ONE cookie.
I learned quite a few important lessons from him that day:
I, and I alone, was the key to that coveted cookie. He knew that the other children did not have the “rights” to give him the cookie. It was only me and so he went directly to me each time. ‘Tov lachsos ba’Shem miv’toach ba’adam.’
He never lost track of his goal. Despite all the distractions, even though he had an enjoyable day, he never forgot. His request was always on his mind. ‘L’olam lo ashkach pikudecha ki vam chisani.’
59
ISS
UE
27
. 202
0

FE
AT
UR
ES
His sweet persistence was cute. It impressed me and endeared me to him enough to grant his request. ‘Yismach lev mivakshei Hashem.’
Don’t hesitate to continue requesting. Ask and ask again. ‘Kavei el Hashem, chazak v’ametz leibecha, v’kavei el Hashem.’ Patient persistence will get you there.
And lastly, not to be forgotten, ‘Mizmor l’sodah … bo’uh lifanav birnana.’
As I gave him a kiss in bed and tucked
his blanket under him, he smiled warmly with half-closed eyes as he wistfully asked “’morrow, more cook-kie?”
My Precious CHILDSora Gitty Spitzer
Catch him being good. A child seeks attention and will even seek negative attention rather than no attention at all. Look for every opportunity to give your child positive attention (praise him when he’s playing quietly etc.) so that he will not need to look for negative attention.
Hear your child. Whenever possible, if your child wants to tell you something, try to stop what you’re doing, make eye contact and show that you are fully with him.
I love you, unconditionally. Tell your child often that you love him. NEVER CONNECT YOUR LOVE TO ANY ACTION PERFORMED BY HIM. Your CHILD MUST BE CONFIDENT THAT you love him ONLY for who he is, because he is your beloved child.
Label the action – not the child. If your child was generous, tell him he did a kind deed by sharing with his sibling. If he grabbed his friend’s snack, tell him he did a mean thing. Never say good boy or naughty girl. A child’s essence is good, always. In addition, if you call him good boy today and bad boy tomorrow you COULD CONFUSE HIM – what am I - good or bad?.
Descriptive praise. Give details when praising the child – you painted with such pretty colours and within the line (if you make a general statement like ‘you’re such an artist!’ it is likely that your child will not believe you). You brushed your sister’s hair so neatly and used such a pretty bobble! Your child will believe you and know that your praise is genuine.
CC
HH
II
LL
DD
60IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
Why I Love My NursesAnonymous for Obvious Reasons
They make my house smelldon’t bother to ring the bellthe job they do, nah, not at all swell really don’t know how to do anything wellOn stupidities they dwellat the other kids they yelland in an emergency just turn to jellin an idiotic spell
They, don’t respect our privacyignore the no-perfume policywalk into the bedroom- causing me major anxietywhat is wrong with this society
Oh,If only...they would bother to really suctionnot be busy all day eating ham and lokshen (pasta)and just listen to mommy’s instructionnot to cause medical destructionand quit already with all their ruction
If only...the agency would stop sending creeps who on the job sleepand ignore all the beepswhen the equipment peepspoor baby, not heeding her silent cries and bleeps
If only...after using the bathroom they would the seat wipeand not leave colors of all stripesand be on the phone with Facebook, Youtube & Candy Crush swipeI wouldn’t have all day about what to gripebecause then about what would be the hype?
I would just accept the nisayon b’ahavastop with all this ga’avaand spewing of lavabecause normal nurses I can handle but these, don’t even hold a candleit’s mamash a scandal
So mommy should go to nursing schoolinstead of wasting my days sitting nearby on a stoolwatching these nurses of ‘jewel’ (think of cruel)who all day just fooland don’t listen to the rule(s)now, that would be really cool
With a nursing degree as a powerful toolEveryone will droolAs NURSE MOMMY RULES!
Down Syndrome Amongst
Us
61
ISS
UE
27
. 202
0

FE
AT
UR
ES
IN MEMORY OF MY UNCLE
Shloimy Schlesingerשלמה מאיר בן נפתלי צבי
May 24, 1960 – October 20, 2019In Tribute to My Incredible Grandparents, להבחל“ח Naftuli and Tzirel Schlesinger
By: Miriam (Schlesinger) DembitzerEdited by: Chaya Rifky Schlesinger
This is an article that I began to write mentally countless
times over the years. I can’t believe that it is on the night of my dear Uncle Shloimy’s shloishim that I actually sit down to begin writing.
I have read many articles from the perspective of parents and siblings of special needs children. I don’t recall having read an article written from the perspective of a niece, someone who experienced the effects of growing up with a special needs family member - a generation later. It is difficult to find the words to adequately express the impact Shloimy had on my life - because it was tremendous. From affecting our overall family culture, to the many family functions that revolved around him, to my career choice as a special educator, to the stories and lines we continuously repeat.
My father’s brother, Shloimy Schlesinger, had Down syndrome. He was born in an era (1960) when it was rare to keep such a child home. The Schlesinger family is an extremely loving, tight-knit clan that is always there for
each other, no matter the occasion. I wonder how much of this family culture came about as a result of growing up with a special needs sibling.
My grandparents, Tzirel and Naftuli Schlesinger, married in 1958. My grandmother’s twin sister, Leah, had married a few weeks earlier. The sisters both had their first babies in 1959. My grandmother had a boy and Leah a girl. Leah’s daughter, Esty, was born with Down syndrome, something none of them had previously heard of. They had no idea what it was or how it would affect their lives. Since they lived in close proximity to each other, they spent a lot time raising their children together.
A year later, in 1960, they both gave birth to their second babies. This time my grandmother gave birth to Shloimy, a special neshama, who also had Down syndrome. My grandparents entered, what was for them, uncharted territory. They did not have information about what to expect and how to deal with his differences. Additionally, they (and their siblings) became the talk of
Down Syndrome Amongst
Us
62IS
SU
E 2
7 . 2
020

FE
AT
UR
ES
the town, with people debating whether or not they were doing the right thing. They demonstrated what love and acceptance is. Shloimy was raised as an integral part of the family.
My grandmother invested a lot of effort into raising Shloimy, without the guidance of special educators and therapists. She taught him to the best of her abilities and was very protective over him. My grandmother would downplay my uncle’s milestones so as not to hurt her sister and make it obvious that Esty was behind.
My grandparents had eight children, close in age to each other. Shloimy’s siblings recall how difficult the early years were. They were labeled “The Mongolian Family,” and some assumed all the children were crazy. The siblings reminisce about not having friends because of their strange brother. They often didn’t get invited to events because people didn’t want Shloimy there. Despite all that, the siblings were fiercely protective of Shloimy.
When Shloimy was of age to attend school, he attended the same cheder as his brothers due to the lack of options. (HASC was founded in 1963 and didn’t yet have the capabilities to cater to Shloimy’s needs.) He remained in the same class for a few successive years, at some point being classmates with 3 of his younger brothers. The roles reversed, with Shloimy’s younger brothers often acting as their older brother’s protector. My grandfather would pay the rebbe in cheder a monthly stipend to keep him in the classroom. Years later, my grandfather was horrified to discover that despite taking his money, the rebbe would lock Shloimy in the cellar daily shortly after his arrival.
As a young child, Shloimy was very wild. He used to run around, jump on beds and couches; bang on things, and be hard to reason with. It became obvious that the cheder was not the right setting for him and he was eventually switched to HASC at the age of ten. Shloimy was finally in a setting that catered to his needs, which transformed him and the entire family. He became a happy, well-behaved, calm person. He loved going to school every day, coming home and
sharing the details of his day. He picked up on so many new skills!
During shiva for Shloimy, Shmuel Kahan, the current director of HASC and the son of the founders of HASC - Rabbi Max and Blanche Kahan, came to be menachem avul. He reminded my grandfather that once, in the early days of HASC, his father desperately needed money and sent him to my grandfather to fundraise. My grandfather gave him a check for $17,000, which was a lot of money in those days. My grandfather recognized the importance of having a special school that catered to special children, and he did everything he could to help HASC develop.
By the time the two youngest siblings were growing up, Shloimy was a completely different child than the one the older siblings had known in the early days. He had a great sense of humor and laughed a lot. He was fun, warm, gentle and entertaining to be around. He was very predictable and disciplined. They often had friends over, who thought he was the cutest guy. A lot of fun family functions revolved around Shloimy, such as the HASC Chanukah parties, the HASC concert and visiting day in Camp HASC.
Shloimy would sit in the same seat playing Hi-Q for hours straight. He loved listening to the radio, keeping up with the news. He had a special love for the Yankees and listened to all the games. When they won it was a big celebration and when they lost it was also ok because they just came second. Shloimy was a hard-core conservative Republican. When elections came around, he always made sure in advance that there would be someone available to take him to vote.
63
ISS
UE
27
. 202
0

FE
AT
UR
ES
Shloimy had such a feeling for anything to do with Yiddishkeit. He insisted on saying a p’shetel for his bar mitzvah. Shloimy loved going to shul and kept up with the davening. Despite not being able to read, he was always on the correct page in the siddur. He would remind everyone to say Hallel and Yaleh Veyovo, when applicable. He really connected with gelilah and my grandfather would buy it for him yearly. He would also ensure that Shloimy got it every week in Camp HASC during his summer stays there. Later, the siblings would also make sure to buy gelilah when he came to visit.
Shloimy loved Shabbos! It was the highlight of his week. He always made Kiddush and when he went to camp he took along a special little becher and small grape juice bottles. He loved music and singing zmiros. After all the standard zmiros were sung, he would continue singing more. He counted down to all the Yomim Tovim (and of course the HASC concert). He would fast every fast and could not be tricked into breaking it early if he wasn’t feeling well.
Shloimy was so well trained by his parents. He made his bed perfectly every morning. He always packed away after himself, and others as well, never complaining. He had his erev Shabbos chores that he performed religiously. He repeatedly thanked everyone for everything they did for him and was quick to apologize. He was extremely respectful and treated his parents with utmost reverence.
He had a huge heart. He picked up on other people’s challenges and would try to help to the best of his capabilities.
Shloimy loved his siblings and rejoiced in their milestones. He celebrated being reunited with them after any separation. As his siblings got married and new members joined the family, he became more excited
with each additional sibling-in-law. He was never resentful about being skipped. He was the family human countdown clock and informed everyone how many days left to simchas. He knew everyone’s birthdays and anniversaries and would call a day in advance. He also knew everyone’s phone numbers and could not resist calling a relative every time he had access to a phone.
Camp HASC was a really big deal in our family. Shloimy spoke about it all year long. He couldn’t wait to go. His amazing counselors kept up with him year-round. The entire family would come on visiting day; it was the highlight of everyone’s summer. All the grandchildren were picked up from their camps to attend. He knew exactly who was
there and who wasn’t. My grandparents would show up with food, nosh and prizes. We looked forward to the canteen and the entertainment. It was a special annual family event. Shloimy loved receiving dollars for the soda machine. My grandparents would invite any of Shloimy’s friends who didn’t have visitors to join us and give them care packages. Shloimy would give us a tour of the camp and introduce us to the staff members. He was so proud of his
family. As one of the oldest campers, he was a fixture in camp. They called him Zaidy.
We grandchildren knew him as a gentle person who was fun to be around. We loved him and we knew he loved us. He gave the best hugs. He snuggled with the babies and caressed their heads gently. He taught us all so much. His excitement for all things Yiddishkeit inspired us. His highlights became everyone else’s highlights. He infused so much joy into all of our lives. You couldn’t be in a bad mood around him.
Growing up with him, made us all more sensitive and caring people. There wasn’t really a time when it was spelled out to us
“He was the family human
countdown clock and informed everyone how many
days left to simchas.”
64IS
SU
E 2
7 . 2
020

FE
AT
UR
ES

FE
AT
UR
ES
that he was different and must be treated so. As we grew up, and slowly realized that he was different, we were so proud of him, and especially of our family. We understood that being chosen to be his family made our family special.
As the grandchildren grew up, the roles would also reverse. When he came to our
parents’ homes for Shabbos or Yom Tov we would also contribute to his care.
As my grandparents aged, Shloimy needed an alternative place to live. Interestingly enough, he chose his new living arrangements by himself! He was out for
pizza with my aunt Ruchy, when he simply stated “I want to go to your house.” He did, and ended up staying for about 5 years. They really enveloped him into their family and all the children were involved in his care. My uncle, Yossi, was especially devoted to his medical needs. During those years, whenever my aunt needed a break or had guest, Shloimy would go to one of his other siblings for Shabbos. Unfortunately, my aunt’s family experienced a major trauma when their son, Chesky, was hit by a car. Shloimy was distraught by the car accident. Chesky had been especially close to Shloimy and had really helped out with all aspects of his care. With life changed for Ruchy, Shloimy went to live with my parents, Yocheved and Eli for two years.
During the years that he lived with my parents, most of the physical aspects of his care was provided by my mother, his sister-in-law, with love and devotion. At that point he was already forgetful and starting to decline so he needed more help. Because he already
forgot so many of the little things that made him unique, it was even clearer to see the things that were most important to him, like Shabbos (he wanted to wear a white shirt every day) and davening (he asked what time davening was all day and had pressure to go to shul on time). His face still lit up at the sight of any of his siblings.
Right before my sister got married, Shloimy deteriorated to the point where my mother and his aids could no longer manage his care. The siblings arranged for him to go to a rehab facility. It was an extremely painful, but necessary move. My single siblings who were used to living with him were devastated. Throughout the two years that Shloimy was in the rehab my aunt Hindy arranged for a constant family presence at his side and feedings for each meal. For a large percent of that time, Hindy went to feed him breakfast every morning.
This Sukkos was an exciting time for our family, because my grandfather was going to Israel for the first time in eighteen years, along with one of his sons and family. The first night of Yom Tov Shloimy was taken into the hospital. His siblings rotated being with him throughout the first days. Not wanting to disrupt his trip, the siblings tried to keep the information from my grandfather, but he overheard. My grandfather figured out how serious the situation was when he realized that all the siblings that were in town were in the hospital at the same time. He made the decision to fly back Motzei Shabbos. When he landed at 4 a.m. on Hoshana Rabba, he was told to come straight to the hospital. The siblings waited with bated breath, praying that Shloimy would spend his final moments with his father at his side, like they both deserved. Shloimy indeed waited for his father, the man who had raised him with love and devotion for close to 60 years, and they got to spend a full hour together before he returned his special neshama to his Maker.
Shloimy had a happy, quality life. Having him in our family made each one of us more caring people and pushed us to be better versions of ourselves. We are grateful to have had the zechus of being chosen to be his family.
66IS
SU
E 2
7 . 2
020

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
s
Rubinstein-Taybi Syndrome
About
DESCRIPTIONRubinstein-Taybi syndrome is a
condition characterized by short stature, moderate to severe intellectual disability, distinctive facial features, and broad thumbs and first toes. Additional features of the disorder can include eye abnormalities, heart and kidney defects, dental problems, and obesity. These signs and symptoms vary among affected individuals. People with this condition have an increased risk of developing noncancerous and cancerous tumors, including certain kinds of brain tumors. Cancer of blood-forming tissue (leukemia) also occurs more frequently in people with Rubinstein-Taybi syndrome.
Rarely, Rubinstein-Taybi syndrome can involve serious complications such as a failure to gain weight and grow at the expected rate (failure to thrive) and life-threatening infections. Infants born with this severe form of the disorder usually survive only into early childhood.
FREQUENCY
This condition is uncommon; it occurs in an estimated 1 in 100,000 to 125,000 newborns.
CAUSES
Mutations in the CREBBP gene are responsible for some cases of Rubinstein-Taybi syndrome. The CREBBP gene provides instructions for making a protein that helps control the activity of many other genes. This protein, called CREB binding protein, plays an important role in regulating cell growth and division and is essential for normal fetal development. If one copy of the
CREBBP gene is deleted or mutated, cells make only half of the normal amount of CREB binding protein. Although a reduction in the amount of this protein disrupts normal development before and after birth, researchers have not determined how it leads to the specific signs and symptoms of Rubinstein-Taybi syndrome.
Mutations in the EP300 gene cause a small percentage of cases of Rubinstein-Taybi syndrome. Like the CREBBP gene, this gene provides instructions for making a protein that helps control the activity of other genes. It also appears to be important for development before and after birth. EP300 mutations inactivate one copy of the gene in each cell, which interferes with normal development and causes the typical features of Rubinstein-Taybi syndrome. The signs and symptoms of this disorder in people with EP300 mutations are similar to those with mutations in the CREBBP gene; however, studies suggest that EP300mutations may be associated with milder skeletal changes in the hands and feet.
Some cases of severe Rubinstein-Taybi syndrome have resulted from a deletion of genetic material from the short (p) arm of chromosome 16. Several genes, including the CREBBP gene, are missing as a result of this deletion. Researchers believe that the loss of multiple genes in this region probably accounts for the serious complications associated with severe Rubinstein-Taybi syndrome.
About half of people with Rubinstein-Taybi syndrome do not have an identified
continued on page 69
67
ISS
UE
27
. 202
0

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
sDown
Syndrome Amongst
Us
LIVING WITHRubinstein-Taybi Syndrome
R.V.
As the flames of the tall bonfires died down and the melodies of
the lively tunes faded into the atmosphere, the day marking the passing of the holy Taaneh R’ Shimon Bar Yachai, came to a halt. And with that ending, came a new beginning, the birth of our little tzaddik, Shimon.
As I held and cuddled my gorgeous newborn, I considered myself the luckiest mother alive. Shimon was born after two girls so this was a real excitement. I had always dreamed of having a son and now he was here!
No one could prepare me for what was about to change my life. The baby’s numbers and scores were fluctuating wildly. A pediatrician was consulted to check the baby before moving me from the labour ward to the post-natal ward where I was supposed to spend the rest of my stay. As she checked him, she shook her head. My son’s heart rate was measuring 245 beats per minute, which was a whopping number. A normal healthy heart rate measures between 120 to 180 beats. Anything over 200 indicates tachycardia. Furthermore, she informed me of some other issues which needed checking and monitoring, and he would have to undergo observation
in the neo-natal unit. I accompanied my 3-hour-old son to the specialised unit which would become his home for the next 10 days. After his admission to the high-dependency unit, a kind consultant came to talk to us. She inquired if anyone in our family has a heart condition, to which we both replied in the negative. She then went on to explain that our son has a cardiac condition called SVT, which stands for Super Ventricular Tachycardia. Loosely translated it meant that the actual organ, the heart, was functioning; however, the surrounding areas were malfunctioning. He would have to be prescribed beta blocker medication which he would have to take daily several times to prevent another episode from occurring, plus have several check-ups with a cardiologist to monitor his condition. Naturally, we grew very concerned and wondered how such a thing could go unnoticed during 9 months of pregnancy. We had loads of questions and were filled with anxiety. But instead of gaining clarity in our increasing concern, we were piled on with new complications. They also suspected sepsis, which had to be treated with anti-biotics intravenously.
Every day of his stay in the hospital brought on another speculation; every
68IS
SU
E 2
7 . 2
020

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
s
meeting with the doctor brought additional concerns. Taking our baby home for Shabbos seemed impossible; they had to prolong his stay due to further monitoring and blood work.
With each visit to the neo-natal unit I grew closer to my little boy and bonded by gripping onto his clutch through the holes in the glass incubator. Since he was tube fed, I only had the privilege of nursing him when he was moved at a week old to the lower dependency unit known as the special care baby unit. He was no longer in an incubator but was hooked to the monitor. I remember attempting to nurse him and noticed he was almost choking on his feed. This happened several times during feeding. In retrospect, I am still amazed that the doctors and nurses failed to notice another significant problem which took 6 torturous months to diagnose.
After 10 long days and several vital tests later, my baby was safe to be discharged. Along with his cardiac medication, we finally strapped him into his car seat and bound for home.
We made his bris a few days later and he recovered well. After that we were thrown into a whirlwind of appointments, and
hospital outpatient visits. I became very familiar with medical jargon, as I tried to adjust to it all.
My life became hectic. Trying to juggle a household with a new born is no easy feat in any situation. Especially, when challenges arise such as feeding difficulties. My baby would splutter and choke during almost every feed. When he eventually did
finish his feed, it was after a big battle and was almost time for his next portion. I was feeding my baby most of the day with hardly any let up. Never feeling that he was fully satisfied, and because his feeds took so long, I found it difficult leaving him with a babysitter. I had to give up on attending simchos or nights out.
At about 4 weeks of age, my baby started to projectile vomit some feeds. I dismissed my concerns, blaming it on colic or reflux. At 2 months of age, I noticed my baby wasn’t lifting his head up at all or attempting to roll over. With his feedings having become increasingly difficult, I gave up nursing. I then decided to visit a pediatrician in one of London’s private hospitals known as The Wellington. I put every bit of hope into this doctor’s visit wishing that he would finally give me some answers. After a full check-up and a
mutation in the CREBBP or EP300 gene or a deletion in chromosome 16. The cause of the condition is unknown in these cases. Researchers predict that mutations in other genes are also responsible for the disorder.
INHERITANCE PATTERN
This condition is considered to have an autosomal dominant pattern of inheritance, which means one copy of the altered gene in each cell is sufficient
to cause the disorder. Most cases result from new mutations in the gene and occur in people with no history of the disorder in their family. Inasmuch as Down syndrome is a genetic disorder but is not inherited, so too, Rubinstein-Taybi syndrome is not hereditary.
OTHER NAMES FOR THIS CONDITION
• Broad Thumb-Hallux Syndrome• RSTS• RTS
continued from page 67 69
ISS
UE
27
. 202
0

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
swhopping doctor’s bill, I was advised to change Shimon’s formula to whey powder instead of cow’s milk. I blindly followed this advice and got this special formula prescribed. I did not notice any changes. I tried switching bottles but to no avail. Something was off, and I couldn’t put my finger on it.
At the age of 4 and a half months, in defeat of trying to bottle feed him, I attempted giving Shimon solids.
Yom Kippur and Succos were spent in Israel, where I went from specialist to specialist, hoping to find some miracle cure for our son’s mysterious problems. We were referred from pediatrician to neurologist to ophthalmologist. Except for footing the hefty medical bills, we still had no clarity as to what could be causing my son failure to thrive. Because he was also gaining weight steadily, he was never classified as a high priority. I credit my persistence in feeding him and getting enough nutrition into him. I was so busy sitting and feeding him for such a large portion of the day that I suffered terrible lower back pains from sitting so long in an uncomfortable position. At one point I concluded that perhaps I was just an over reactive parent.
We traveled back home, and once again my son caught a bad cold which lead to fever which lead to a battle of getting fluids into him since his nose was badly blocked. After a weekend of administering Nurofen to bring his fever down, and with a syringe trying to get fluids into him we took him into the local hospital’s emergency room.
Our salvation came to us in the form of a doctor who remembered our Shimon from when he was staying in the neo-natal unit. While we waited for results, and had suction and saline inhaler administered, she remarked that she happened to look
at his medical records and took note of all his problems. She mentioned that she might have a lead with regards to his diagnosis. Looking at all his problems, plus his thumbs, which were unnaturally broad and long, she determined that Shimmy
had a very rare genetic disorder called Rubinstein Taybi Syndrome. However, he would need a visit to a geneticist and undergo genetic screening to confirm and to learn how to proceed. The atmosphere in the room was a combination of shock and fear on my husband’s part and my own bittersweet joy at finally welcoming a sensible diagnosis.
Thus, began a flurry of appointments to a host of specialists and therapists. My son needed an MRI on his brain because his head appeared small, needed top-notch ophthalmological care because he had a lazy eye known as Duane syndrome, and he was being seen in the departments of cardiology and urology. Shimon’s facial
structure was somewhat disconcerting so I visited a cranio-facial specialist at the other end of London, but after several treatments there was no change and I stopped those appointments.
At about 6 months of age, I was sent to see a Speech and Language therapist with regards to his feeding. She concluded that Shimon has trouble swallowing and this is what is causing the choking, as well as the unexplained forceful vomiting. She prescribed a thickening agent called Carobel, thus enabling him to establish a safe method of swallowing without causing fluid to leak into his lungs. I later learned that this condition is called dysphagia. I was also scheduled a video-fluoroscopy, which is an x-ray of the throat, also known as a swallow study to determine how bad the dysphagia was. The final conclusion
70IS
SU
E 2
7 . 2
020

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
s
was that he was only permitted custard-thickness consistency in replacement of regular fluids.
At around the same time the video-fluoroscopy was scheduled, an appointment with a geneticist was also arranged. Shimon was 10 months old at the time. I remember being called into the office where they delivered the verdict. Shimon was officially diagnosed with Rubinstein-Taybi Syndrome, also known as Broad Thumb Syndrome, a very rare, non-inherited condition. In basic terms, he was created with the deletion of a gene which was caused by his own genetic mutation. He was also diagnosed with global developmental delay, which played a big role in his condition.
Once we received his diagnosis, we were able to access therapies and treatment plans more easily and frequently.
At 2 years of age, after having several semi-yearly 24-hour heart monitors and a dozen ECG’s and echocardiograms, the cardiologist was pleased to discharge Shimon from her clinic. He had also stopped taking the daily beta blockers at the age of 1 and a half. Concluding that the only single episode of SVT he had as a new-born baby, which never occurred again, he must have outgrown the problem.
After 2 minor surgeries that passed uneventfully, he was also discharged from urology.
Bechasdei Hashem, after a follow up video-fluoroscopy at the age of 2, Shimmy has outgrown his dysphagia and drinks normal liquids just like any other child can.
Shimmy’s story doesn’t end here. He has had to endure and is still undergoing a lot of intense physiotherapy, speech and language therapy, occupational therapy, play therapy, as well as reflexology and massage and cranial to control his balance and strengthen his muscles.
He still doesn’t walk or talk but and has limited communication skills. However, I, as his parent, notice the little changes for the better. At his own pace he is developing and thriving.
He is now in nursery and is adored by all members of the staff. Shimon is a happy-natured, smiley and healthy child. He is our ray of sunshine.
I am most privileged to be his mother and I do not stop thanking Hashem for sending me a beautiful gift of life, a beating heart inside a gorgeous sunny personality.
O V E R 2 0 Y E A R S E X P E R I E N C E !BOARD CERTIFIED BY THE AMERICAN BOARD OF PEDIATRIC DENTISTRY
2525 Nostrand Ave. Suite 1C Brooklyn, NY 11210T 718.339.3435 · F 718.339.3751
WE WELCOME CHILDREN WITH special needsANESTHESIA OPTIONS DETAILed
TO CUSTOMIZE INDIVIDUAL DENTAL NEEDS

Sib
s' N
ich
e'/
Tee
n S
ce
ne
What She Taught Me
Faigy Furst - Age 17 Down Syndrome Amongst
Us
I couldn’t possibly visualize how the people residing in Eretz Yisroel
officially use the Egged buses as their means of transportation. There I was, squished on the bus for barely fifteen minutes and I couldn’t imagine myself surviving if I didn’t get off that second! Had I known that we still had a half hour to go I would have most likely disembarked right then and there. But I didn’t know, so I stood there, literally gasping for breath until the doors finally burst open and released all of the choking occupants.
It was Mincha time when I finally made my way toward the Kosel. I squirmed my way through the masses of people and cut through security…and then I was there! All the pictures, information, visualization and imagination came crashing down upon me as I suddenly faced the Western Wall for my very first time. The tears sprang forth as if on their own and I did not suppress them. I felt like I was floating above.
Slowly, reluctantly, I inched my way closer to the Wall, and then I was standing right there. I reached for the cool beige stones and an electrical feeling raced through my body; ‘I am here, HERE! I am standing at the place where my forefathers all stood! I am touching the stones that are saturated with tears and prayer!’ Suddenly, all my tefillos, concerns, names and prayers seemed irrelevant as I slowly rested my head on the shiny stones. It
felt like a touch of Heaven, a feeling of total tranquility. It was just me and Hashem; no one else existed. I felt like staying there forever.
I started reciting chapters of Tehillim, totally at peace. I felt like I had everything, need nothing, except Moshiach.
And then I was interrupted by a gentle tap on my shoulder. “Slicha,” a young woman with a Sephardi accent and colorful kerchief on her head interjected, “atu yechol le, ani rotzeh le…” Noticing the look of confusion on my face, the young lady clarified in a broken English, “You mind moving over a bit? We’re trying to make room for a wheelchair.” I stepped to the side, all the while still immersed in my Tehillim, when I suddenly felt something hard bump into my side. I turned slowly and then I saw ‘her’.
She looked like she was about fifteen years old and by her movements it was quite obvious that she had Cerebral Palsy. But it was her Yiddishe chein that captured my heart; it was her sparkling eyes, it was the way her dark wavy hair fell over her shoulders, it was the way she looked at the stones, the way she touched them.
Two young ladies slowly helped her get out of her wheelchair and she rested her crippled body heavily against the wall for support. And then she buried her face between the cracks of the stones and wept. They were sobs I never heard before, wails coming straight from a
72IS
SU
E 2
7 . 2
020

Sib
s' N
ich
e'/
Tee
n S
ce
ne
brave Jewish soul who had a tortured body. There was not a dry eye in the vicinity.
Finally, I closed my Tehillim and slowly turned to leave, but not before hearing her repeat her few slurred words again and again, “Toda Abba, Toda Abba (thank you, Father, thank you, Father).” And then I left the Kosel Plaza.
Oftentimes, like when I brush my hair or walk to school, I cannot help but wonder about something that really amuses me. I’ve seen so many places, met so many people. Why then, when I think about my visit to Eretz Yisroel, is this the image I think about first? One day it hit me; it was not about what the girl looked like, or how she appeared. It was about the words she said, standing next to the Kosel Wall. She could have chosen to ask anything of Hashem! She could have begged Him to relieve her of her pain and discomfort. Yet, all she said was, “Toda Abba”.
Now, how thankful do I have to be?
Note about the author: Faigy is the proud sibling of a sister with special needs. Faigy says: ‘Since Malky joined my life I’ve grown so much! I learned to be patient and caring. I learned to smile and love. Yes, Malky is truly a gift from Hashem!’
73
ISS
UE
27
. 202
0

Sib
s' N
ich
e'/
Tee
n S
ce
ne
Special in Every Way
By Goldie Steinberg - Age 11
Would you ever want to live by a different family
and be disowned by your own family? No! The thought of it is just awful! Well neither do children with special needs. Children with special needs are not meant to be given away.
One reason why children with special needs should be kept at home is if you don’t give away normal children, you don’t give away special children. No one ever asked Hashem why He gave them a nice house, a lot of money, or a beautiful healthy child. Every person has a special neshama, but these kids have it special in a different way. They are definitely no less than your house and money which you hold onto tightly.
Secondly, before every child is born Hashem lets him choose the family he wants to be born into, a family who will love him and help him grow. The same is true with a special needs child. He chose you as his mother, and you want to give him away? How could you? He trusted that you will love him and give him more care and attention than any other woman in the world! How can you ever think of giving him away?!
When the doctors told Mrs. S. that her
son has Down syndrome she cried. But they were not tears of pain or sorrow. They were tears of love and acceptance. Mrs. S. didn’t even dream for one second of giving away her son. She gave birth to him. She can’t just wave her hand good bye to her own flesh and blood. A mother should care enough about her children’s feelings. She would never want her mother to give HER away. You have to care for special children’s feelings more than anybody else (even if you think they are beyond feeling).
Lastly, it was proven that the best people to raise a child are its own parents. The love from a different parent does not compare to the love of a true parent. When Chaim’s mother gave birth to him, she made the decision that due to him having Down syndrome and other family circumstances, the right thing to do would be to give him away. Mrs. S. who has already been mentioned before, welcomed Chaim warmly into her home. She already had her own special child and knew the ins and outs of raising children like him. The S. family relates “We love having a brother with Down syndrome. It reminds us how thankful we have to be and to love other
Down Syndrome Amongst
Us
74IS
SU
E 2
7 . 2
020

Sib
s' N
ich
e'/
Tee
n S
ce
ne
You look at meAnd you see A flat noseand slanty eyes
You look at meAnd you don’t seeHappy eyesand a smiling face
You seeSmall handsand short feet
You don’t seeFar-reaching handsand hardworking feet
You seeA disability and limited strength
You don’t seePast my disabilityand toward my successes
You seeMeThrough your eyes
You don’t seeMeFor who I am
another human being just because he is Hashem’s creation. My mother cares for Chaim like her own son, but it doesn’t compare to the love his real mother could show him.” Only a mother can understand that.
Some people might argue and say that having a child with special needs is way too hard. They are right! But the schar (heavenly reward) for doing it despite the difficulties is immeasurable, the feeling indescribable and there are some rewarding moments too. Many children with special needs are very expressive and loving. Also, some financial help is provided by the government.
In conclusion, it is beautiful to keep your child with special needs home because you do that with your other children, and he is yours just the same. Also, he chose your family to be born into, and it’s only right for you to respect his choice. Lastly, our children will be most loved and cared for by their own parents. May all you readers never have to be faced with this difficult decision. But if Hashem selects you as most fit for the challenge, I am sure you will not think of giving your child away.
Who I AmBy F.W. – Age 16
75
ISS
UE
27
. 202
0

Sib
s' N
ich
e'/
Tee
n S
ce
ne
Hold On To Them!
Gitty Hollender8th Grade
There are many types of people in this world.
Some people say that Down syndrome is a disease, while others say that it is a disability. Parents who are gifted with a baby that has Down syndrome can sometimes feel that their world stopped. They want to give their child away to another family. Parents should not do that.
Schooling, entertainment and recreational programs are much more established for children with disabilities. These programs are there for these kids on days when their schools are closed, for example legal holidays, and also at the end of the school day, when there is still a long afternoon.
Kids with Down syndrome are very pleasing, warm-hearted, cute and smart. They will never harm anyone else. If they see someone crying or sad they will give that person a kiss and stay next to them until they are smiling again. When they are around it’s never boring. With their bright
smiles they can light up dark rooms and sad hearts.
Children with Down syndrome are very smart. If you teach them something they will remember it for a long time. My brother remembers the way to our house via many different routes. He also recognizes his friend’s house after being there only once, to visit when his friend was sick. He and his friends are the sweetest kids in the world.
Parents who want to give away their child with Down syndrome sometimes say that the child will not be well taken care of at home. Children with Down syndrome need no extra care more than healthy children do, and most of them are overall healthy, with only minor limitations due to their syndrome.
Parents should think twice before giving away their children with Down syndrome, because it doesn’t pay to do so.
It’s just like having an expensive diamond and giving it away.
Down Syndrome Amongst
Us
76IS
SU
E 2
7 . 2
020

Sib
s' N
ich
e'/
Tee
n S
ce
ne
I have a brother with Down syndrome. He is the closest thing to my heart.
He is so cute, loving, and sweet. I feel Hashem gave our family a special gift.
He cares for everyone. If someone cries or is sad he comes over, gives him a kiss and says ‘I'm sorry’.
He is so cute - one time (when he was still little and not talking much) he wanted ices and I told him ‘Mommy said no’; he answered me, ‘Mommy says yu’. We went back and forth until he ran crying to my mother, ‘Rifky chepa’ (fight); it was too cute, so of course he got his ices.
What Is Closest to My Heart
Rifky Hollender – Age 11
Down Syndrome Amongst
Us
77
ISS
UE
27
. 202
0

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
sU
P S
YN
DR
OM
E
Grounds for Divorce – Dovid’s
VersionMy newly married daughter and son-in-
law were at our home. My son-in-law had to leave and my daughter stayed. Dovid asked her where her husband went. She said that he left. Dovid shook his head and said that he’ll find her a new husband. My daughter asked why and he told her that a husband that leaves his wife is not a good husband; he’ll get her a new one!
Senior Citizens:
My husband visited Yeshiva Bonim Lamokom where Baruch excitedly told him that he turned 33 the day before. My husband wished him ‘Happy Birthday’ and then back-slapped him and jokingly told Baruch that he’s an old guy. From across the room a smart-aleck friend called out, “Yeh, where’s your cane and wheelchair, Baruch?”
Family DynamicsEleven-year-old Miri came home from
school on Monday of Parshas Toldos and I browsed through her sedra book with her. When she spoke about the ‘bechor’ I wasn’t sure if she understood what it meant, so I explained it to her and asked who the bechor is in our family (Avi), the bechor in Avi’s family, the bechor in my brother-in-law’s family and so on, just
giving examples of the meaning of the word.
A day later Miri asked me, “Mummy, will you please make lentil soup? I want to buy the bechora off Avi so that I can be the oldest in our family!”
Ahhh…The Sweet Smell Of -!
My teenaged Baruch learnt all about personal hygiene at Yeshiva Bonim Lamokom and came home with his personal kit of supplies.
Several days later I walked in on him in the bathroom spraying Febreeze room deodorizer under his arm.
It’s All About…Food!
Motzei Rosh Hashana Dovid insisted on having a seudah.
I explained to him that there is no Melave Malka on Motzei Yom Tov.
He shook his head and said “seudas hamafsekas - tomorrow is a fast!”
Up Syndromecontinued from back page
78IS
SU
E 2
7 . 2
020

EX
PL
OR
ING
DIS
AB
ILIT
IES
/cond
ition
s
Pesach in July12-year-old Burech’s mother was
cleaning his nose with a saline wash. As the salty water dripped down the back of his throat Burech announced, ‘This is karpas’.
The Midas TouchWe were at the hospital for a follow-up
checkup on Dovid’s heart. The technician taking the echo turned the screen so Dovid could see. She pointed to the screen and showed him that this was his heart. He shook his head and said, “That cannot be my heart. My heart is gold and that one is black and white.”!
US Currency OnlyIt was middle night of Rosh Hashono
and I collapsed onto our sofa and dozed off. I was in twi-light zone when the men walked in from shul and I heard my husband say to Moishey, ‘What do you say to Mommy?’ seeing me sprawled on the couch in a slumber. Moishey said, ‘The Mama is vert cash (the mother is worth cash)!’
Radiant!Moishey’s dorm counselor became
engaged. When I asked Moishey whether the new chussen is happy, Moishey replied, ‘Yes! I can see it on his forehead!”
79
ISS
UE
27
. 202
0

Up Syndrome
continued on page 78
Master Mechanech:
Moishey received an ugly text from a friend of his. Following, is Moishey’s text response to the friend, editted for brevity: (Moishey repeats words unnecessarily in writing, so I removed those; however, the message is intact) ‘Okay, so let me tell you Shmiely (name changed to protect privacy), you know that I still love you with all my hearts, but on one condition. In order for me to love you again in the future iy’H you cannot say NO ‘nivel peh’ right in front of me. Because a person who is a Yid should only use words from the Heiliga Torah Hakdosha and not the words from the ‘nivel peh’diga’ words only a goy could say. But when a person looks like a Yid, a Yid should never and ever use such words; it’s the words that a goy uses. So my ‘tyera’ Shmiely, I still love you and I still like you so dearly but on one condition - in my name and in Hakodosh Baruch Hu’s name we are asking you so nicely and so pleasant-fully to please STOP SAYING SUCH CRAZY WORDS, THE WORDS WHICH HAVE TO DO WITH NIVEL PEH, BECAUSE I DO NOT LIKE IT, OKAY my sweety, Mr. Shmiely.