Embed Size (px)
Citation preview

AMERICAN ACADEMY OF PEDIATRICSCommittee on Genetics
Health Supervision for Children With Down Syndrome
ABSTRACT. These guidelines are designed to assistthe pediatrician in caring for the child in whom thediagnosis of Down syndrome has been confirmed bykaryotype. Although the pediatrician’s initial contactwith the child is usually during infancy, occasionally thepregnant woman who has been given the prenatal diag-nosis of Down syndrome will be referred for counseling.Therefore, these guidelines offer advice for this situationas well.
Children with Down syndrome have multiplemalformations and mental impairment be-cause of the presence of extra genetic material
from chromosome 21. Although the phenotype isvariable, usually there is enough consistency to en-able the experienced clinician to suspect the diagno-sis. Among the more common physical features arehypotonia, small brachycephalic head, epicanthicfolds, flat nasal bridge, upward slanting palpebralfissures, Brushfield spots, small mouth, small ears,excessive skin at the nape of the neck, single trans-verse palmar crease, and short fifth finger with cli-nodactyly. A wide space, often with a deep fissurebetween the first and second toes, is also common.The degree of mental impairment is variable, rangingfrom mild (IQ: 50–70) to moderate (IQ: 35–50), andonly occasionally to severe (IQ: 20–35). There is anincreased risk of congenital heart defects (50%); leu-kemia (,1%); hearing loss (75%); otitis media (50%–70%); Hirschsprung disease (,1%); gastrointestinalatresias (12%); eye disease (60%), including cataracts(15%) and severe refractive errors (50%); acquiredhip dislocation (6%); obstructive sleep apnea (50%–75%); and thyroid disease (15%). The social quotientmay be improved with early intervention techniques,although the level of function is exceedingly vari-able. Children with Down syndrome often functionbetter in social situations than might be expectedfrom their IQ.
In approximately 95% of children with Down syn-drome, the condition is because of nonfamilial tri-somy 21. In approximately 3% to 4% of persons withthe Down syndrome phenotype, the extra chromo-
somal material is the result of an unbalanced trans-location between chromosome 21 and another acro-centric chromosome, usually chromosome 14.Approximately three fourths of these unbalancedtranslocations are de novo, and approximately onefourth are the result of familial translocations. If thechild has a translocation, a balanced translocationmust be excluded in the parents. If there is a trans-location in either parent, additional familial studiesand counseling should be instituted. In the remain-ing 1% to 2% of persons with the Down syndromephenotype, 2 cell lines are present: 1 normal and 1trisomy 21. This condition is called mosaicism. Thesepersons, on average, may be phenotypically less se-verely affected than persons with trisomy 21 ortranslocated chromosome 21, but their conditions aregenerally indistinguishable in all other aspects.
Medical management, home environment, educa-tion, and vocational training can significantly affectthe level of functioning of children and adolescentswith Down syndrome and facilitate their transitionto adulthood. The following outline is designed tohelp the pediatrician to care for children with Downsyndrome and their families.1–4 It is organized by theissues that need to be addressed in the various agegroups (see Table 1).
Several areas require ongoing assessment through-out childhood and should be reviewed periodicallyat developmentally appropriate ages. These includethe following:
• Personal support available to family.• All other financial and medical support programs
for which the child and family may be eligible.• Supplemental Security Income benefits.• Injury and abuse prevention with special consid-
eration of developmental skills.• Diet and exercise to maintain appropriate weight.
THE PRENATAL VISITPediatricians may be asked to counsel a family in
which a fetus has a genetic disorder. In some set-tings, the pediatrician may be the primary resourcefor counseling. At other times, counseling may havebeen provided for the family by a clinical geneticist,obstetrician, or developmental pediatrician. In addi-tion, parents may have received information from aDown syndrome program, a national Down syn-drome organization, or an Internet site. Because of aprevious relationship with the family, the pediatri-cian may be asked to review this information andassist in the decision-making process. As appropri-ate, the pediatrician should discuss the followingtopics with the family:
The recommendations in this policy statement do not indicate an exclusivecourse of treatment for children with genetic disorders, but are meant tosupplement anticipatory guidelines available for treating the healthy childprovided in the AAP publication, “Guidelines for Health Supervision.”They are intended to assist the pediatrician in helping children with geneticconditions to participate fully in life. Diagnosis and treatment of geneticdisorders are changing rapidly. Therefore, pediatricians are encouraged toview these guidelines in the light of evolving scientific information. Clinicalgeneticists may be a valuable resource for the pediatrician seeking addi-tional information or consultation.PEDIATRICS (ISSN 0031 4005). Copyright © 2001 by the American Acad-emy of Pediatrics.
442 PEDIATRICS Vol. 107 No. 2 February 2001

TA
BL
E1.
Hea
lth
Supe
rvis
ion
for
Chi
ldre
nW
ith
Dow
nSy
ndro
me—
Com
mit
tee
onG
enet
ics*
Pren
atal
Infa
ncy,
1M
onth
to1
Yea
rE
arly
Chi
ldho
od,1
to5
Yea
rsL
ate
Chi
ldho
od,
5to
13Y
ears
,A
nnua
l
Ad
oles
cenc
e,13
to21
Yea
rs,
Ann
ual
Neo
nata
l2
Mon
ths
4M
onth
s6
Mon
ths
9M
onth
s12
Mon
ths
15M
onth
s18
Mon
ths
24M
onth
s3
Yea
rs4
Yea
rs
Dia
gnos
isK
aryo
type
revi
ew†
••
Phen
otyp
ere
view
••
Rec
urre
nce
risk
s•
•A
ntic
ipat
ory
guid
ance
Ear
lyin
terv
enti
onse
rvic
es•
••
••
••
••
••
Rep
rod
ucti
veop
tion
s•
‡•
‡•
‡•
•Fa
mily
supp
ort
••
••
••
••
••
••
••
Supp
ort
grou
ps•
••
•L
ong-
term
plan
ning
••
•§
•§
Sexu
alit
y•
•M
edic
alev
alua
tion
Gro
wth
oo
oo
oo
oo
oo
oo
oT
hyro
idsc
reen
ing
o¶o
oo
oo
oo
Hea
ring
scre
enin
go
S/o
S/o
S/o
S/o
S/o‡
S/o‡
S/o
S/o
S/o§
S/o
‡‡
Vis
ion
scre
enin
gS/
oS/
o‡S/
oS/
oS/
o‡S/
oS/
o‡S/
oS/
oS/
o\S/
oC
ervi
cal
spin
ero
entg
enog
ram
o**
Ech
ocar
dio
gram
•o
CB
Co
oPs
ycho
soci
alD
evel
opm
ent
and
beha
vior
alS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oS/
oSc
hool
perf
orm
ance
oo
oo
oSo
cial
izat
ion
SS
S
*A
ssur
eco
mpl
ianc
ew
ith
the
Am
eric
anA
cad
emy
ofPe
dia
tric
s“R
ecom
men
dat
ions
for
Prev
enti
vePe
dia
tric
Hea
lth
Car
e.”
•5
tobe
perf
orm
ed;S
5su
bjec
tive
,by
hist
ory;
and
o5
obje
ctiv
e,by
ast
and
ard
test
ing
met
hod
.†
Or
atti
me
ofd
iagn
osis
.‡
Dis
cuss
refe
rral
tosp
ecia
list.
§G
ive
once
inth
isag
egr
oup.
¶A
ccor
din
gto
stat
ela
w.
\A
sne
eded
.**
See
dis
cuss
ion.
AMERICAN ACADEMY OF PEDIATRICS 443

1. The prenatal laboratory or fetal imaging studiesleading to the diagnosis.
2. The mechanism for occurrence of the disorder inthe fetus and the potential recurrence rate for thefamily.
3. The prognosis and manifestations, including thewide range of variability seen in infants and chil-dren with Down syndrome.
4. When applicable, additional studies that may re-fine the estimation of the prognosis (eg, fetal echo-cardiogram, ultrasound examination for gastroin-testinal malformations).
5. Currently available treatments and interventions.This discussion needs to include the efficacy, po-tential complications and adverse effects, costs,and other burdens associated with these treat-ments. Discuss early intervention resources, par-ent support programs, and any plausible futuretreatments.
6. The options available to the family for manage-ment and rearing of the child using a nondirectiveapproach. In cases of early prenatal diagnosis, thismay include discussion of pregnancy continua-tion or termination, rearing the child at home,foster care placement, and adoption.
If the pregnancy is continued, a plan for deliveryand neonatal care must be developed with the obste-trician and the family. Offer parent-to-parent con-tact. As the pregnancy progresses, additional studiesmay be valuable for modifying this managementplan (eg, detection of a complex heart defect byechocardiography). When appropriate, referral to aclinical geneticist should be considered for a moreextended discussion of clinical outcomes and vari-ability, recurrence rates, future reproductive op-tions, and evaluation of the risks for other familymembers.
HEALTH SUPERVISION FROM BIRTH TO 1MONTH: NEWBORNS
ExaminationConfirm the diagnosis of Down syndrome and
review the karyotype with the parents. Review thephenotype. Discuss the specific findings with bothparents whenever possible, and talk about the fol-lowing potential clinical manifestations associatedwith the syndrome. These may have to be reviewedagain at a subsequent meeting.
Discuss and Review• Hypotonia• Facial appearance
Evaluate for• Feeding problems• Strabismus, cataracts, and nystagmus at birth or
by 6 months• Congenital hearing loss with objective testing,
such as brainstem auditory evoked response orotoacoustic emission at birth or by 3 months5
• Heart defects (approximately 50% risk). Performcardiac evaluation (consultation by a cardiologist
with expertise and experience in pediatric patientsand echocardiogram recommended).
• Duodenal atresia• Constipation with increased risk of Hirschsprung
disease• Leukemia—more common in children with Down
syndrome than in the general population, but stillrare (,1%); leukemoid reactions, on the otherhand, are relatively common as is polycythemia(18%). Obtain complete blood count.
• Congenital hypothyroidism (1% risk)• Respiratory tract infections
Anticipatory Guidance• Discuss increased susceptibility to respiratory
tract infection• Discuss the availability and efficacy of early inter-
vention.• Discuss the early intervention services in the com-
munity.• Inform the family of the availability of support
and advice from the parents of other children withDown syndrome.
• Supply names of Down syndrome support groupsand current books and pamphlets (see “Bibliogra-phy and Resources for New Parents”).
• Discuss the strengths of the child and positivefamily experiences.
• Check on individual resources for support, such asfamily, clergy, and friends.
• Talk about how and what to tell other familymembers and friends. Review methods of copingwith long-term disabilities.
• Review the recurrence risk in subsequent preg-nancies and the availability of prenatal diagnosis.
• Discuss unproven therapies.6–12
HEALTH SUPERVISION FROM 1 MONTH TO1 YEAR: INFANCY
Examination
Physical Examination and Laboratory Studies• Review the risk of serous otitis media (50%–70%).
If the tympanic membranes cannot be visualized,or if the parents express any concern about theirchild’s hearing, refer the infant to an otolaryngol-ogist. Review the prior hearing evaluation (brain-stem auditory evoked response and otoacousticemission and refer back to the otolaryngologistand audiologist if the initial evaluation was abnor-mal for follow up examination and testing. A be-havioral audiogram should be obtained at 1 yearin all children examined.
• Check for strabismus, cataracts, and nystagmus by6 months, if not done at birth. Check the infant’svision at each visit, using developmentally appro-priate subjective and objective criteria. By 6months, refer the infant to a pediatric ophthalmol-ogist or an ophthalmologist with special expertiseand experience with infants with disabilities.
• Verify results of newborn thyroid function screen.Because of increased risk of acquired thyroid dis-ease, repeat at 6 and 12 months and then annual-ly.13,14
444 HEALTH SUPERVISION FOR CHILDREN WITH DOWN SYNDROME

• Administer pneumococcal vaccine, as well asother vaccines recommended for all children un-less there are specific contraindications.
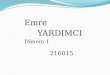
Anticipatory Guidance• Review the infant’s growth and development rel-
ative to other children with Down syndrome (Figs1–4).15
• Review availability of Down syndrome supportgroups (see “Bibliography and Resources for NewParents”).
• Assess the emotional status of parents and in-trafamily relationships. Educate and support sib-lings and discuss sibling adjustments. At 6 to 12months, review the psychological support and in-trafamily relationships, including long-term plan-ning, financial planning, and guardianship.
• Review the early intervention services relative tothe strengths and needs of the infant and family
(see “Bibliography and Resources for New Par-ents”).
• Review the family’s understanding of the risk ofrecurrence of Down syndrome and the availabilityof prenatal diagnosis.
HEALTH SUPERVISION FROM 1 TO 5 YEARS:EARLY CHILDHOOD
• Obtain a history and perform a physical examina-tion with attention to growth and developmentalstatus.
• Review the risk of serous otitis media with hearingloss. If the tympanic membranes cannot be com-pletely visualized (because of the frequent prob-lem of stenotic ear canals), check the child’s audio-gram every 6 months up to 3 years or up to whena pure tone audiogram is obtained. Refer the childto an otolaryngologist or audiologist if necessary
Fig 1. Percentiles for height and weight offemales with Down syndrome, 1 to 36months of age. From Cronk C, Crocker AC,Pueschel SM, et al. Growth charts for chil-dren with Down syndrome: 1 month to 18years of age. Pediatrics. 1988;81:102–110.
AMERICAN ACADEMY OF PEDIATRICS 445

(approximately 50%–70% risk of serous otitis me-dia between 3 and 5 years).
• Check the child’s vision annually, using develop-mentally appropriate subjective and objective cri-teria. Refer the child to a pediatric ophthalmolo-gist or ophthalmologist with special expertise andexperience with children with disabilities every 2years (approximately 50% risk of refractive errorsbetween 3 and 5 years).
• At 3 to 5 years, obtain radiographs for evidence ofatlantoaxial instability or subluxation. These maybe obtained once during the preschool years. Theneed for these studies has been questioned, butthey may be required for participation in the SpecialOlympics. These studies are more important for chil-dren who may participate in contact sports and areindicated in those who are symptomatic.16–19
• Perform thyroid screening tests annually.• Discuss symptoms related to obstructive sleep ap-
nea, including snoring, restless sleep, and sleepposition. Refer to a specialist as indicated.20
Anticipatory Guidance• Review early intervention, including physical
therapy, occupational therapy, and speech, in thepreschool program and discuss future schoolplacement and performance.
• Discuss future pregnancy planning, risk of recur-rence of Down syndrome, and prenatal diagnosis.
• Assess the child’s behavior, and talk about behav-ioral management, sibling adjustments, socializa-tion, and recreational skills.
• Encourage families to establish optimal dietaryand physical exercise patterns that will preventobesity.
HEALTH SUPERVISION FROM 5 TO 13 YEARS:LATE CHILDHOOD
• Obtain a history and perform a physical examina-tion with attention to growth and developmentalstatus.
• Obtain audiologic evaluation annually.• Obtain ophthalmologic evaluation annually.
Fig 2. Percentiles for height and weight offemales with Down syndrome, 2 to 18 yearsof age. From Cronk C, Crocker AC, PueschelSM, et al. Growth charts for children withDown syndrome: 1 month to 18 years of age.Pediatrics. 1988;81:102–110.
446 HEALTH SUPERVISION FOR CHILDREN WITH DOWN SYNDROME

• Perform thyroid screening tests annually (3%–5%risk of hypothyroidism).
• If appropriate, discuss skin problems: very dryskin and other skin problems are particularly com-mon in patients with Down syndrome.
• Discuss symptoms related to obstructive sleepapnea, including snoring, restless sleep, andsleep position. Refer to a specialist as indi-cated.20
Anticipatory Guidance• Review the child’s development and appropriate-
ness of school placement and developmental in-tervention.
• Discuss socialization, family status, and relation-ships, including financial arrangements andguardianship.
• Discuss the development of age-appropriate socialskills, self-help skills, and the development of asense of responsibility.
• Discuss psychosexual development, physical andsexual development, menstrual hygiene and man-agement, fertility, and contraception.21
• Discuss the need for gynecologic care in the pu-bescent female. Talk about the recurrence risk ofDown syndrome with the patient and her family ifshe were to become pregnant.22 Review the factthat although there have been 2 case reports in
Fig 3. Percentiles for height and weightof males with Down syndrome, 1 to 36months of age. From Cronk C, CrockerAC, Pueschel SM, et al. Growth chartsfor children with Down syndrome: 1month to 18 years of age. Pediatrics.1988;81:102–110.
AMERICAN ACADEMY OF PEDIATRICS 447

which a male has reproduced, males with Downsyndrome are usually infertile.22
HEALTH SUPERVISION FROM 13 TO 21 YEARS OROLDER: ADOLESCENCE TO EARLY ADULTHOOD
Examination• Perform physical examination including CBC and
thyroid function tests.• Obtain annual audiologic evaluation.• Obtain annual ophthalmologic evaluation.• Discuss skin care.
Anticipatory Guidance• Discuss issues related to transition into adulthood.• Discuss appropriateness of school placement with
emphasis on adequate vocational training withinthe school curriculum.20,23
• Talk about the recurrence risk of Down syndromewith the patient and her family if she were tobecome pregnant.22
• Discuss sexuality and socialization. Discuss theneed for and degree of supervision and/or theneed for contraception. Make recommendationsfor routine gynecologic care.
• Discuss group homes and independent living op-portunities, workshop settings, and other commu-nity-supported employment.
• Discuss intrafamily relationships, financial plan-ning, and guardianship.
• Facilitate transfer to adult medical care.
Committee on Genetics, 2000–2001Christopher Cunniff, MD, ChairpersonJaime L. Frias, MDCelia Kaye, MD, PhDJohn B. Moeschler, MDSusan R. Panny, MDTracy L. Trotter, MD
LiaisonsFelix de la Cruz, MD, MPH
National Institutes of Health
Fig 4. Percentiles for height and weight ofmales with Down syndrome, 2 to 18 years ofage. From Cronk C, Crocker AC, Pueschel SM, etal. Growth charts for children with Down syn-drome: 1 month to 18 years of age. Pediatrics.1988;81:102–110.
448 HEALTH SUPERVISION FOR CHILDREN WITH DOWN SYNDROME

James W. Hanson, MDAmerican College of MedicalGenetics
Michele Lloyd-Puryear, MD, PhDHealth Resources and ServicesAdministration
Cynthia A. Moore, MD, PhDCenters for Disease Control andPrevention
John Williams III, MDAmerican College of Obstetriciansand Gynecologists
Section LiaisonH. Eugene Hoyme, MD
Section on Genetics
ConsultantsMarilyn J. Bull, MDWilliam I. Cohen, MDFranklin Desposito, MDBeth A. Pletcher, MDNancy Roizen, MDRebecca Wappner, MD
StaffLauri A. Hall
REFERENCES1. American Academy of Pediatrics Committee on Genetics. Health su-
pervision for children with Down syndrome. Pediatrics. 1994;93:855–8592. Cohen WI. Health care guidelines for individuals with Down syndrome
(Down syndrome preventive medical checklist). Down Syndrome Q.1996;1:1–10
3. Cooley WC, Graham JM Jr. Down syndrome: an update and review forthe primary pediatrician. Clin Pediatr (Phila). 1991;30:233–253
4. de la Cruz F. Medical management of mongolism or Down syndrome.In: Mittler P, de Jong JM, eds. Biomedical Aspects. Research to Practice inMental Retardation: Fourth Congress of the International Association for theScientific Study of Mental Deficiency. Vol 3. Baltimore, MD: UniversityPark Press; 1977;221–228
5. Dahle AJ, McCollister FP. Hearing and otologic disorders in childrenwith Down syndrome. Am J Ment Defic. 1986;90:636–642
6. National Down Syndrome Congress. Position Statement on Sicca CellTherapy. Atlanta, GA: National Down Syndrome Congress; 1989
7. Nickel RE. Controversial therapies for young children with develop-mental disabilities. Infants Young Child. 1996;8:29–40
8. National Down Syndrome Society. Position Statement on Vitamin RelatedTherapies. New York, NY: National Down Syndrome Society; 1997.Available at: http://www.ndss.org. Accessed June 1998
9. National Down Syndrome Society. Position Statement on Use of Piracetam.New York, NY: National Down Syndrome Society; 1996. Available at:http://www.ndss.org. Accessed June 1998
10. National Down Syndrome Congress. National intervention in childrenwith Down syndrome. Atlanta, GA: National Down Syndrome Congress;1999. Available at: http://www.ndsccenter.org. Accessed November1999
11.
11. Spigelblatt L, Laine-Ammara G, Pless IB, Guyver A. The use of alter-native medicine by children. Pediatrics. 1994;94(6 pt 1):811–814
12. American College of Medical Genetics. Statement on Nutritional Supple-ments and Piracetam for Children With Down Syndrome. Bethesda, MD:American College of Medical Genetics; 1996
13. Cutler AT, Benezra-Obeiter R, Brink SJ. Thyroid function in youngchildren with Down syndrome. Am J Dis Child. 1986;140:479–483
14. Karlsson G, Gustafsson J, Hedov G, Ivarsson SA, Anneren G. Thyroiddysfunction in Down’s syndrome: relation to age and thyroid autoim-munity. Arch Dis Child. 1998;79:242–245
15. Cronk C, Crocker AC, Pueschel SM, et al. Growth charts for childrenwith Down syndrome: 1 month to 18 years of age. Pediatrics. 1988;81:102–110
16. Davidson RG. Atlantoaxial instability in individuals with Downsyndrome: a fresh look at the evidence. Pediatrics. 1988;81:857–865
17. Msall ME, Reese ME, DiGaudio K, Griswold K, Granger CV, Cooke RE.Symptomatic atlantoaxial instability associated with medical and reha-bilitative procedures in children with Down syndrome. Pediatrics. 1990;85(3 pt 2):447–449
18. Pueschel SM, Findley TW, Furia J, Gallagher PL, Scola FH, Pezzullo JC.Atlantoaxial instability in Down syndrome: roentgenographic, neuro-logic, and somatosensory evoked potential studies. J Pediatr. 1987;110:515–521
19. Pueschel SM, Scola FH. Atlantoaxial instability in individuals withDown syndrome: epidemiologic, radiographic, and clinical studies. Pe-diatrics. 1987;80:555–560
20. Pueschel SM, Pueschel JK, eds. Biomedical Concerns in Persons With DownSyndrome. Baltimore, MD: Brookes Publishing; 1992
21. de la Cruz FF, LaVeck GD, eds. Human Sexuality and the MentallyRetarded. New York, NY: Brunner/Mazel; 1973
22. Jagiello G. Reproduction in Down syndrome. In: de la Cruz FF, GeraldPS, eds. Trisomy 21 (Down Syndrome): Research Perspectives. Baltimore,MD: University Park Press; 1981;151–162
23. Fenner ME, Hewitt KE, Torpy DM. Down’s syndrome: intellectualbehavioural functioning during adulthood. J Ment Defic Res. 1987;31(pt3):241–249
BIBLIOGRAPHY AND RESOURCES FOR NEWPARENTS
BibliographyCairo S, Cairo J, Cairo T. Our Brother Has Down’s Syndrome: An Introduction
for Children. Toronto, Ontario: Annick Press Ltd; 1985Hanson MJ. Teaching the Infant With Down Syndrome: A Guide for Parents and
Professionals. 2nd ed. Austin, TX: Pro-Ed; 1987Pueschel SM. A parent’s guide to Down syndrome. Baltimore, MD: Brookes
Publishing; 1990Stray-Gunderson K. Babies With Down Syndrome: A New Parents Guide.
Kensington, MD: Woodbine House; 1986 (English and Spanish editions)
ResourcesMarch of Dimes, Birth Defects Foundation, 1275 Mamaroneck Ave, White
Plains, NY 10605; Telephone: 914/428–7100National Down Syndrome Congress, 1605 Chantilly Dr, Suite 250, Atlanta,
GA 30324; Telephone: 404/633–1555 or 800/232–6372National Down Syndrome Society, 666 Broadway, New York, NY 10012;
Telephone: 212/460–9330 or 800/221–4602
AMERICAN ACADEMY OF PEDIATRICS 449