Embed Size (px)
Citation preview

Douglas Dieterich,1 Vicente Soriano,2 Mark Nelson,3 Jürgen Kurt Rockstroh,4 Keikawus Arastéh,5 Sanjay Bhagani,6 Andrew Talal,7 Cristina Tural,8 Richard Vinisko,9 and Jens Kort 9
STARTVerso 4: High rates of early virologic response in HCV genotype 1/HIV-co-infected patients treated
with faldaprevir plus pegIFN and RBV
1Mount Sinai School of Medicine, New York, NY, USA; 2Hospital Carlos III, Madrid, Spain; 3Chelsea and Westminster Hospital, London, UK; 4University of Bonn, Bonn, Germany; 5EPIMED, Vivantes Auguste-Viktoria Hospital, Berlin,
Germany; 6Royal Free Hospital, London, UK; 7State University of New York, Buffalo, NY, USA; 8Hospital Universitari Germans Trias i Pujol, Barcelona, Spain; 9Boehringer Ingelheim Pharmaceuticals Inc., Ridgefield, CT, USA
20th Conference on Retroviruses and Opportunistic Infections, March 3–6, 2013

Presenter disclosure
I have had financial relationships within the last 12 months relevant to my presentation with:
Boehringer Ingelheim Pharmaceuticals AND
My presentation includes information on faldaprevir, which is an investigational
compound and is not yet approved
Douglas Dieterich, MDMount Sinai School of Medicine,
New York, USA

Introduction to faldaprevir
• Faldaprevir is a potent and selective
inhibitor of the HCV NS3/A4 protease
‒ The pharmacokinetics of FDV allow
oral once daily administration
• Phase IIb data demonstrated potent
antiviral activity against HCV GT-1 for:
‒ Faldaprevir combined with pegIFN/RBV
‒ An IFN-free combination of faldaprevir
with BI 207127 and RBV
• Phase III trials are ongoing for the
iFree and iBased faldaprevir clinical
development programsLlinàs-Brunet M, et al. J Med Chem 2010;53:6466–6476;
Lemke CT, et al. J Biol Chem 2011;286:11434–11443;Sulkowski MS, et al. Hepatology 2013 Jan 28 [Epub ahead of print];
Zeuzem S, et al. AASLD Congress November 9–13, 2012 [Abstract No. 232].
GT, genotype; HCV, hepatitis C virus;IFN, interferon alpha; RBV, ribavirin;BI 207127, a non-nucleoside inhibitor of HCV RNA polymerase
Faldaprevir: Interaction with NS3/4A protease
Green = hydrophobic Blue = mildly polarPurple = H bonding

Phase III open-label, sponsor-blinded study in treatment-naïve and relapser patients with chronic HCV GT-1 and HIV infection
LLoQ, lower limit of quantification <25 IU/mL HCV RNA; pegIFN: pegylated interferon alfa-2a 180 µg once weekly; QD, once daily; SVR, sustained virologic response at 12 weeks after end of treatment.; ETS, early treatment successRBV: ribavirin 1000 or 1200 mg daily dose for body weight <75 kg or ≥75 kg, respectively
Patients with HCV RNA below LLoQ, at Week 4, and HCV RNA below LLoQ target not detected at Week 8 (=ETS) will be re-randomized 1:1 at week 24 to stop treatment or continue pegIFN/RBV through week 48Patients who did not achieve ETS will continue pegIFN/RBV through week 48
STARTVerso 4: Study design (1)
Faldaprevir 120 mg QD + pegIFN/RBV
Day 1 Week 12 Week 24 Week 48
pegIFN/RBV
pegIFN/RBV
Faldaprevir 240 mg QD + pegIFN/RBVFaldaprevir 240 mg QD
+ pegIFN/RBV
pegIFN/RBV
Randomization 1:1
Primary endpoint: SVR12Interim data

STARTVerso 4: Study design (2)
No ART
Raltegravir ormaraviroc
based
120 or 240 mg QD
Efavirenzbased
Darunavir/ritonavir oratazanavir/ritonavir
basedART
regimen
Faldaprevir dosage
RANDOMIZED
120 mg QD240 mg QD
ART, antiretroviral therapy; QD, once daily
ALLOCATED
• HCV GT-1 infection, including compensated cirrhosis
‒ HCV treatment-naive or relapsers

STARTVerso 4: Patient disposition(Week 12 interim data)
Allocated/Randomized(N=153/N=157)
Screen failure(N=143)
aIncludes: viral rebound ≥1 log10 HCV RNA from previous undetected level; lack of HCV RNA reduction from baseline by ≥ 2 log10 at Week 12; lack of viral response at Week 24. bIncludes: protocol violation, withdrawal by subject, or other reasonsAE, adverse event; ATZ, atazanavir; DRV, darunavir; EFV, efavirenz; r, ritonavir
Completed 12 weeks of treatment(N=176)
Faldaprevir (120 or 240 mg QD) + pegIFN/RBV
(N=308)
Screened(N=453)
Not treated(N=2)
HCV treatment-naïve(N=239)
Relapser(N=69)
Not available (N=18)Discontinued (N=45)
15 Due to AE
12 Lack of efficacya
18 Other reasonb
Not available (N=4)Discontinued (N=7)
3 Due to AE
1 Lack of efficacya
3 Other reasonb
Completed 12 weeks of treatment(N=58)

STARTVerso 4: Baseline characteristics
Treatment-naïve(N=239)
Relapser(N=69)
Total(N=308)
Age, years (mean) 47 47 47
Male, n (%) 184 (77) 64 (93) 80
Race, n (%) WhiteBlack or
African AmericanOthera
179 (75)39 (16)21 (9)
63 (91)2 (3)4 (6)
7913 8
ART, n (%) EFV-basedATZ/r- or
DRV/r-basedRal-
based and otherb
No ART (ARV-naïve), n (%)
67 (28)60 (25)
105 (44) 7 (3)
17 (25)7 (10)
41 (59)4 (6)
84 (27)67 (22)
146 (47)11 (4)
Mean baseline CD4+ T cell count, cells/µL 544 549 545
Baseline HCV RNA ≥800 000 IU/mL, n (%) 197 (82) 49 (71) 246 (80)
HCV Genotype-1a, n (%) 184 (77) 55 (80) 239 (78)
Cirrhosis F4 or FibroScan >13 kPa, n (%) 40 (17) 11 (16) 51 (17)aIncludes Asian, Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, and missing data.bIncludes 1 patient taking maraviroc plus emtricitabine/tenofovir disoproxil fumarate, 1 patient taking emtricitabine/tenofovir disoproxil fumarate only. Ral, raltegravir

STARTVerso 4: Interim safety and tolerability
Most frequent AEs in >20% of patients No. of patients (%)
NauseaFatigueDiarrheaHeadacheAsthenia
113 (37)102 (33)83 (27)71 (23)68 (22)
Other AEs of interest No. of patients (%)
Anemia Neutropenia Rash Loss of HIV suppressiona
55 (18)49 (16)55 (18)
0
Most frequent serious AEs (>1 patient) No. of patients (%)
PyrexiaAbdominal painDiarrheaGastroenteritisVomitingAnemiaRashDehydration
4 (1)3 (<1)3 (<1)2 (<1)2 (<1)2 (<1)2 (<1)2 (<1)
aIncrease of HIV plasma RNA >200 copies/mL on two consecutive measurements from prior <40 copies/mLThree deaths: dyspnea; hemorrhage, cerebrovascular accident; Drug reaction with eosinophilia and systemic symptoms

Series10
20
40
60
80
100
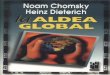
8086
60
82
Pro
port
ion
of p
atie
nts
(%)
191/239
143/239
Week 4 Week 12
206/239
195/239
Early virologic response in HIV/HCV co-infected patients: HCV treatment-naïve
Treatment-naïve <LLoQ Treatment-naïve <LLoQ TND
TND target not detected

Series10
20
40
60
80
100
8086
60
82
91 93
74
91
Pro
port
ion
of p
atie
nts
(%)
191/239
143/239
Week 4 Week 12
206/239
195/239
Early virologic response in HIV/HCV co-infected patients: HCV treatment-naïve and relapsers
64/69
63/69
63/69
51/69
Treatment-naïve <LLoQ Treatment-naïve <LLoQ TND
Relapser <LLoQ Relapser <LLoQ TND

Series10
20
40
60
80
100
8086
60
82
91 93
74
91
76
93
Pro
port
ion
of p
atie
nts
(%)
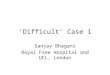
aSILEN-C1 study arm of 240mg QD FDV plus pegIFN/RBV in HCV GT1 treatment-naïve monoinfected patients without cirrhosis; data on file
191/239
143/239
Week 4 Week 12
206/239
195/239
Early virologic response in HIV/HCV co-infected patients: comparison with HCV mono-infected patients
64/69
63/69
63/69
51/69
Treatment-naïve <LLoQ TND
Treatment-naïve <LLoQ Treatment-naïve <LLoQ TND
Relapser <LLoQ Relapser <LLoQ TND
a
a
108/142
132/142
Mono-infected patients, SILEN-C1 study:

Series10
20
40
60
80
100
77
88P
ropo
rtio
n of
pat
ient
s (%
)
184/239
61/69
Response guided therapy criteria (ETS) in STARTVerso 4
Treatment-naïve Relapser
ETS criteria: Wk 4 HCV RNA <LLoQ, + Wk 8 <LLOQ, TND
aData missing for 4 patients.ETS, early treatment success
a
YES
50% Stop treatment at week 24 50% continue with pegIFN/RBV through week 48

Summary and conclusions
• AEs were comparable to those with faldaprevir and pegIFN/RBV in HCV mono-infected patients
• ETS was observed in 80% of patients‒ Half of these patients will stop treatment at Week 24
• 12-week data show high rates of early virologic response to faldaprevir + pegIFN/RBV
• Interim data compare well with early response rates in mono-infected patients
• Sustained virologic response data will be used to determine the feasibility of response-guided therapy with faldaprevir
Overall reductions in HCV RNA Treatment-naïve Relapsers
Week 4 <LLoQ :Week 12 <LLoQ TND:
80%82%
91%91%

• Patients, and study investigators and site staff at 67 study centers:
• Boehringer Ingelheim for sponsoring the study and the Boehringer Ingelheim 1220.19 team
• The external Data Monitoring Committee
Acknowledgments
Brazil Hans Jäger Josep Mallolas Chloe Orkin Marina Nunez
Carlos Eduardo Brandão Mello Arastéh Keikawus Juan Antonio Pineda Alison Uriel Gerald Pierone
Raymundo Ferreira Filho Hartwig Klinker Daniel Podzamczer United States Michael Saag
Paulo Ferreira Jürgen Kurt Rockstroh Cristina Tural John Baxter Michael Somero
Juvencio Furtado Italy Jorge Vergas Maurizio Bonacini Richard Sterling
Beatriz Grinsztejn Giacchino Angarano, Switzerland Cynthia Brinson Mark Sulkowski
Jose Madruga Andrea Antinori Manuel Battegay Douglas Dieterich Andrew Talal
France Giovanni Di Perri Enos Bernasconi Richard Elion Kristen Marks
Marc Bourliere Gaetano Filice Jan Fehr Jerome Ernst
Laurent Cotte Francesco Mazzotta Andri Rauch Douglas G. Fish
Pierre-Marie Girard Paola Nasta United Kingdom Federico Hinestrosa
Caroline Lascoux-Combe Massimo Puoti Kosh Agarwal Mamta Jain
Marc-Antoine Valantin Spain Sanjay Bhagani Anthony LaMarca
Germany Francisco Blanco Martin Fisher Eric Lawitz
Johannes Bogner Manuel Crespo, Ranjababu Kulasegaram Cheryl McDonald
Christian Hoffmann Josep Guardiola Clifford Leen Karam Mounzer
Patrick Ingiliz Juan Carlos Lopez Mark Nelson Ronald Nahass