Embed Size (px)
Citation preview

ww.sciencedirect.com
i n d i a n h e a r t j o u rn a l 6 5 ( 2 0 1 3 ) 3 1 5e3 1 8
Available online at w
journal homepage: www.elsevier .com/locate/ ih j
Case Report
Double jeopardy
Damien Cullington a,*, Natalie Dunford b, Stephen Beer b, Neil Hobson a,Sudipta Chattopadhyay b, Joseph John b
aCastle Hill Hospital, Castle Road, Cottingham, Kingston-Upon-Hull HU16 5JQ, UKb Scunthorpe General Hospital, UK
a r t i c l e i n f o
Article history:
Received 27 July 2012
Accepted 3 April 2013
Available online 19 April 2013
Keywords:
Methadone
Long QT
Torsades
Temporary Pacing
* Corresponding author. Tel.: þ44 (0) 1482 62E-mail address: damiencullington@hotm
0019-4832/$ e see front matter Copyright ªhttp://dx.doi.org/10.1016/j.ihj.2013.04.016
a b s t r a c t
Torsades de pointes (“twisting of points”) (TdP) is a broad complex tachyarrhythmia which
was first described in 1966 by Francois Dessertenne and usually results from prolongation
of the QT interval.1 A wide variety of drugs have been shown to prolong the QT interval in
susceptible individuals.2 We present the case of a former intravenous heroin user pre-
senting with several episodes of TdP which were caused by QT prolongation due to
methadone treatment and exacerbated by hepatitis B/C infection. Despite aggressive
medical treatment and withdrawal of methadone, he had recurrent episodes of TdP which
required continuous temporary cardiac pacing for six days. He was found to have moderate
LV dysfunction on his echocardiogram and unobstructed coronary arteries on coronary
angiography. He underwent implantation of a defibrillator due to concerns about further
episodes of ventricular arrhythmias which could recur even in the absence of further
methadone use.
Copyright ª 2013, Cardiological Society of India. All rights reserved.
1. Introduction 2. Case presentation
Prolongation of the QT interval is a known side effect of
methadone therapy. Patients with a history of hepatitis,
however, who are prescribed methadone may be at greater
risk of hazardous QT interval prolongation compared to pa-
tients with no prior history of liver disease. Patients intending
to start a methadone programme should have an ECG recor-
ded before starting methadone, after 30 days of therapy and
after a change in dosage. ECGs should then be performed on
an annual basis. The acute management of TdP will vary from
one institution to another but when transvenous pacing is not
available, a variety of therapeutic measures can usually sta-
bilize a patient.
4 073; fax: þ44 (0) 1482 62ail.com (D. Cullington).2013, Cardiological Societ
A 43-year-old man presented to his general practitioner (GP)
with a history of several “panic attacks” and paroxysms of
dyspnea occurring over the previous 24 h.While attending the
GP surgery he was syncopal in the waiting room and required
a short period of cardiopulmonary resuscitation. He had no
preceding chest pain, dyspnea or palpitations. On arrival to
the emergency department, a further episode of syncope
occurred and the cardiac monitor recorded a broad complex
tachyarrhythmia. To restore hemodynamic stability, electrical
cardioversion was required (Fig. 1).
Our patient had no previous history of cardiovascular
problems. He was a former intravenous heroin user, hepatitis
B and C positive and enrolled in a drug treatment program. He
4 071.
y of India. All rights reserved.
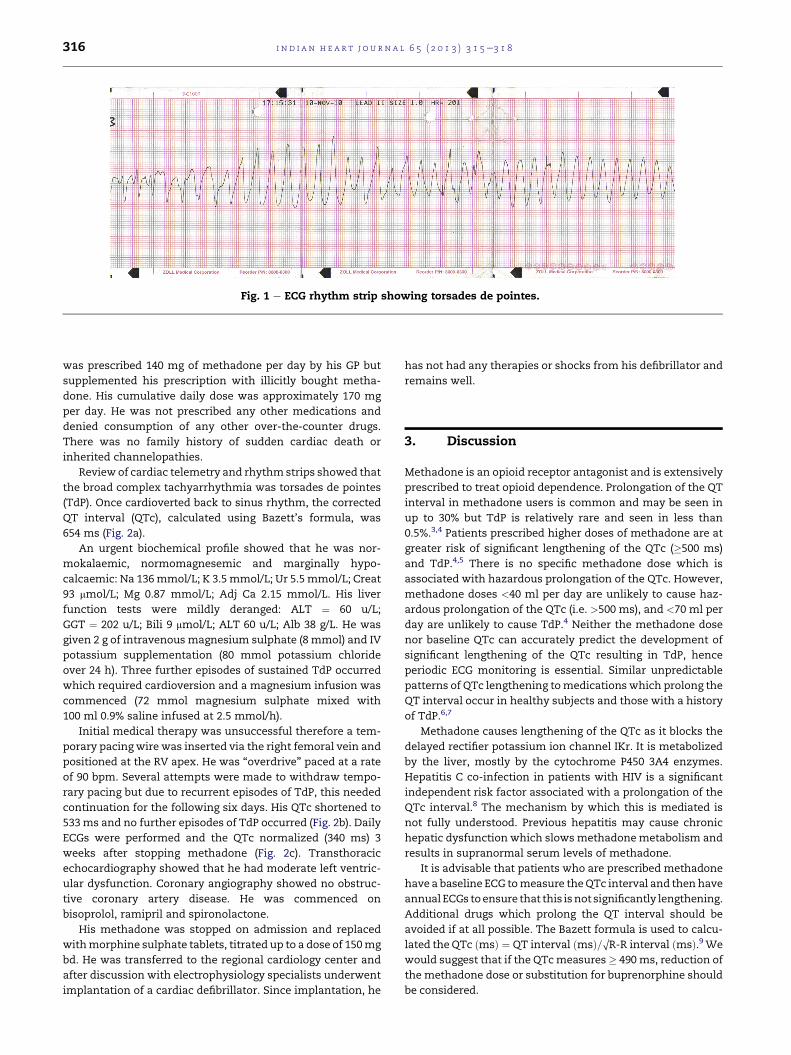
Fig. 1 e ECG rhythm strip showing torsades de pointes.
i n d i a n h e a r t j o u r n a l 6 5 ( 2 0 1 3 ) 3 1 5e3 1 8316
was prescribed 140 mg of methadone per day by his GP but
supplemented his prescription with illicitly bought metha-
done. His cumulative daily dose was approximately 170 mg
per day. He was not prescribed any other medications and
denied consumption of any other over-the-counter drugs.
There was no family history of sudden cardiac death or
inherited channelopathies.
Review of cardiac telemetry and rhythm strips showed that
the broad complex tachyarrhythmia was torsades de pointes
(TdP). Once cardioverted back to sinus rhythm, the corrected
QT interval (QTc), calculated using Bazett’s formula, was
654 ms (Fig. 2a).
An urgent biochemical profile showed that he was nor-
mokalaemic, normomagnesemic and marginally hypo-
calcaemic: Na 136mmol/L; K 3.5mmol/L; Ur 5.5 mmol/L; Creat
93 mmol/L; Mg 0.87 mmol/L; Adj Ca 2.15 mmol/L. His liver
function tests were mildly deranged: ALT ¼ 60 u/L;
GGT ¼ 202 u/L; Bili 9 mmol/L; ALT 60 u/L; Alb 38 g/L. He was
given 2 g of intravenous magnesium sulphate (8 mmol) and IV
potassium supplementation (80 mmol potassium chloride
over 24 h). Three further episodes of sustained TdP occurred
which required cardioversion and a magnesium infusion was
commenced (72 mmol magnesium sulphate mixed with
100 ml 0.9% saline infused at 2.5 mmol/h).
Initial medical therapy was unsuccessful therefore a tem-
porary pacing wire was inserted via the right femoral vein and
positioned at the RV apex. He was “overdrive” paced at a rate
of 90 bpm. Several attempts were made to withdraw tempo-
rary pacing but due to recurrent episodes of TdP, this needed
continuation for the following six days. His QTc shortened to
533ms and no further episodes of TdP occurred (Fig. 2b). Daily
ECGs were performed and the QTc normalized (340 ms) 3
weeks after stopping methadone (Fig. 2c). Transthoracic
echocardiography showed that he had moderate left ventric-
ular dysfunction. Coronary angiography showed no obstruc-
tive coronary artery disease. He was commenced on
bisoprolol, ramipril and spironolactone.
His methadone was stopped on admission and replaced
withmorphine sulphate tablets, titrated up to a dose of 150mg
bd. He was transferred to the regional cardiology center and
after discussion with electrophysiology specialists underwent
implantation of a cardiac defibrillator. Since implantation, he
has not had any therapies or shocks from his defibrillator and
remains well.
3. Discussion
Methadone is an opioid receptor antagonist and is extensively
prescribed to treat opioid dependence. Prolongation of the QT
interval in methadone users is common and may be seen in
up to 30% but TdP is relatively rare and seen in less than
0.5%.3,4 Patients prescribed higher doses of methadone are at
greater risk of significant lengthening of the QTc (�500 ms)
and TdP.4,5 There is no specific methadone dose which is
associated with hazardous prolongation of the QTc. However,
methadone doses <40 ml per day are unlikely to cause haz-
ardous prolongation of the QTc (i.e. >500 ms), and <70 ml per
day are unlikely to cause TdP.4 Neither the methadone dose
nor baseline QTc can accurately predict the development of
significant lengthening of the QTc resulting in TdP, hence
periodic ECG monitoring is essential. Similar unpredictable
patterns of QTc lengthening tomedicationswhich prolong the
QT interval occur in healthy subjects and those with a history
of TdP.6,7
Methadone causes lengthening of the QTc as it blocks the
delayed rectifier potassium ion channel IKr. It is metabolized
by the liver, mostly by the cytochrome P450 3A4 enzymes.
Hepatitis C co-infection in patients with HIV is a significant
independent risk factor associated with a prolongation of the
QTc interval.8 The mechanism by which this is mediated is
not fully understood. Previous hepatitis may cause chronic
hepatic dysfunction which slowsmethadonemetabolism and
results in supranormal serum levels of methadone.
It is advisable that patients who are prescribed methadone
have a baseline ECG tomeasure theQTc interval and then have
annual ECGs toensure that this isnot significantly lengthening.
Additional drugs which prolong the QT interval should be
avoided if at all possible. The Bazett formula is used to calcu-
lated theQTc ðmsÞ ¼ QT interval ðmsÞ=OR-R interval ðmsÞ.9We
would suggest that if the QTcmeasures � 490 ms, reduction of
the methadone dose or substitution for buprenorphine should
be considered.
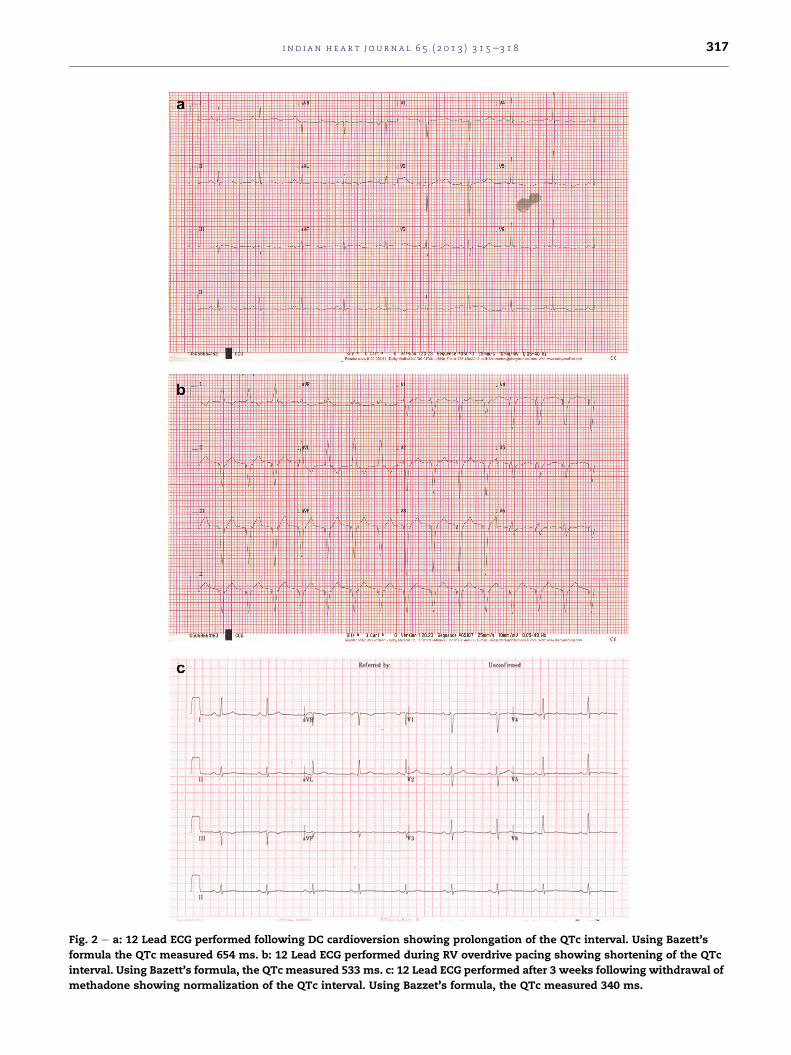
Fig. 2 e a: 12 Lead ECG performed following DC cardioversion showing prolongation of the QTc interval. Using Bazett’s
formula the QTc measured 654 ms. b: 12 Lead ECG performed during RV overdrive pacing showing shortening of the QTc
interval. Using Bazett’s formula, the QTc measured 533 ms. c: 12 Lead ECG performed after 3 weeks following withdrawal of
methadone showing normalization of the QTc interval. Using Bazzet’s formula, the QTc measured 340 ms.
i n d i a n h e a r t j o u rn a l 6 5 ( 2 0 1 3 ) 3 1 5e3 1 8 317

i n d i a n h e a r t j o u r n a l 6 5 ( 2 0 1 3 ) 3 1 5e3 1 8318
The key aspects of clinical management to treat TdP are i)
correct electrolyte disturbances (Kþ, Mg2þ, Ca2þ); ii) cease any
medications which prolong the QTc; iii) administer 2 g IV
magnesium over 1e2 min, repeated if necessary after
5e15min iv) increase the heart rate to reciprocally shorten the
QTc.10 Patients with episodes of TdP, which recur despite
intravenous magnesium sulphate and during correction of
electrolytes, should ideally be transvenously paced at rates
�90 per minute.11,12 Although amiodarone commonly in-
creases the QTc interval, it is safe and rarely causes TdP when
used chronically.13 However, in the acutemanagement of TdP,
amiodarone should be avoided since it may be pro-
arrhythmic. Intravenous isoprenaline or atropine infusions
can increase heart rate and shorten the QTc and repeated
administration of IV magnesium boluses or a magnesium
infusion (3e20 mg/min) can successfully treat TdP but these
measures should be used viewed as bridging measures until
temporary pacing is organized.11,14
Up to 20%of subjectswith drug inducedTdPmayhave forme
fruste varieties of the LQTS which may be ‘unmasked’ by QT
prolonging drugs or electrolyte disturbances.15 Genetic testing
for longQTsyndromemutationsmaybe considered for the index
case and recording a 12 lead ECG is recommended for first-
degree relatives.16 It is possible that our patient had exces-
sively high serum levels ofmethadone due to impaired hepatic
metabolism, changing the predicted pharmacokinetic profile,
but we were unable to confirm this. Although the pharmaco-
logical trigger for QT prolongation was stopped on admission,
our patient underwent elective implantation of a defibrillator.
In some patients who have experienced drug induced TdP, the
recurrence risk of TdP may remain elevated despite cessation
of offending medications.17 Patients with an opiate addiction
are at high risk of recidivism, and for some patients with
intractable methadone dependence, implantation of a defi-
brillator may be necessary as a precautionary measure.18
4. Learning points
1. The normal QTc interval in men <430 ms and in women
<450 ms. A baseline ECG should be performed before pre-
scription of methadone, annually thereafter and if the dose
is uptitrated >100 mg/day.
2. Risk of QT prolongation is increased for females, electrolyte
disturbance (hypokalemia, hypomagnesemia, hypocalce-
mia), CYP3A4 inhibiting drugs, hepatic dysfunction,
concomitant prescription of QT prolonging drugs, left
ventricular dysfunction and high doses of methadone.
3. Consensus guidelines have suggested that if the QTc in-
creases between 450 and 500 ms, discussion of pros and
cons of continued methadone treatment, avoidance of QTc
prolongingmedications andmore frequent ECGmonitoring
should occur. If the QTc increases above 500 ms, with-
drawal of other exacerbating drugs/electrolyte disturbance,
reducing the methadone dose or substitution with an
alternative is advisory.19
4. Initial medical management of TdP includes IVmagnesium
and correction of electrolytes. Early institution of overdrive
pacing is an effective remedy for drug induced TdP in cases
which are refractory to medical therapy. Where temporary
pacing is not immediately available, isoprenaline or atro-
pine can be used as bridging therapy.
5. An excellent reference regarding what drugs prolong the
QT interval can be found at www.qtdrugs.org.
Conflicts of interest
All authors have none to declare.
r e f e r e n c e s
1. Dessertenne F. La tachycardie ventriculaire a deux foyersopposes variables. Arch Mal Coeur Vaiss. 1966;59:263e272.
2. Roden DM. Drug-induced prolongation of the QT interval. NEngl J Med. 2004;350:1013e1022.
3. Sticherling C, Schaer BA, Ammann P, et al. Methadone-induced torsade de pointes tachycardias. Swiss Med Weekly.2005;135:282e285.
4. Ehret GB, Voide C, Gex-Fabry M, et al. Drug-induced long QTsyndrome in injection drug users receiving methadone. ArchIntern Med. 2006;166:1280e1287.
5. Priori SG, Schwartz PJ, Napolitano C, et al. Risk stratificationin the long-QT syndrome. N Engl J Med. 2003;348:1866e1874.
6. Kannankeril PJ, Norris KJ, Carter S, Roden DM. Factorsaffecting the degree of QT prolongation with drug challengein a large cohort of normal volunteers. Heart Rhythm.2011;8:1530e1534.
7. Kaab S, Hinterseer M, Nabauer M, et al. Sotalol testingunmasks altered repolarisation in patients with suspectedacquired long-QT syndrome e a case-control pilot study usingIV sotalol. Eur Heart J. 2003;24:649e657.
8. Nordin C, Kohli A, Beca S, et al. Importance of hepatitis Ccoinfection in the development of QT prolongation inHIV-infected patients. J Electrocardiol. 2006;39:199e205.
9. Bazett HC. An analysis of the time-relations ofelectrocardiograms. Heart. 1920;7:353e370.
10. Gowda RM, Khan IA, Wilbur SL, et al. Torsade de pointes: theclinical considerations. Int J Cardiol. 2004;96:1e6.
11. Tzivoni D, Banai S, Schuger C, et al. Treatment of torsade depointes withmagnesium sulphate. Circulation. 1988;77:392e397.
12. DiSegni E, Klein HO, David D. Overdrive pacing in quinidinesyncope and other long QT-interval syndromes. Arch InternMed. 1980;140:1036e1140.
13. Mattioni TA, Zheutin TA, Sarmiento JJ, et al. Amiodarone inpatients with previous drug-mediated torsade de pointes. AnnInter Med. 1989;111:574e580.
14. Khan IA, Gowda RM. Novel therapeutics for treatment of long-QT syndrome and torsade de pointes. Int J Cardiol. 2004;95:1e6.
15. Lehtonen A, Fodstad H, Laitinen-Forsblom P, et al. Furtherevidence of inherited long QT syndrome gene mutations inantiarrhythmic drug-associated torsades de pointes. HeartRhythm. 2007;4:603e607.
16. HRS/EHRA Expert Consensus Statement on the state ofGenetic testing for the channelopathies andCardiomyopathies. Heart Rhythm. 2011;8:1308e1339.
17. Monnig G, Kobe J, Loher A, et al. Role of implantablecardioverter defibrillator therapy in patients with acquiredlong QT syndrome: a long-term follow-up. Europace.2012;14:396e401.
18. Patel AM, Singh JP, Ruskin JN. Role of implantablecardioverter-defibrillators in patients with methadone-induced long QT syndrome. Am J Cardiol. 2008;101:209e211.
19. Krantz MJ, Martin J, Stimmel B, et al. QTc interval screening inmethadone treatment. Ann Inter Med. 2009;150:387e395.