Embed Size (px)
Citation preview

Double-Duty Actions to Combat the Double/Triple Burden of Malnutrition
Linda S. Adair, PhD
Professor
Department of Nutrition
Gillings School of Global Public Health
University of North Carolina at Chapel Hill
Chapel Hill, NC USA
UN Decade of Action on Malnutrition and the SDGs: End all forms of malnutrition

Outline
• What is the dual/triple burden of nutrition?
• Levels: Individual, household, community, region/country
• Epidemiology
• Shared drivers of undernutrition and overweight/obesity
• Dual duty solutions

The dual/double burden of malnutrition:
• Co-occurrence of overweight and/or obesity, with undernutrition manifested as stunting, wasting, or underweight
• Concept has been expanded to the Triple Burden of Malnutrition, to include micronutrient deficiencies
Undernutrition Indicators based on WHO growth standard median
Child:Stunting: length or height for age Z-score <-2 Wasting: weight-for-length or height <-2 Underweight: weight Z-score <-2 medianAdult:Thinness: BMI < 18.5 kg/m2
Overweight Child < 5 years old: weight-for-length or height Z-score >2Child 5-18 years: BMI Z-score >1Adult: BMI> 25 kg/m2
Obesity: Child: BMI Z-score >1Adult: BMI>30 kg/m2
Definitions

Epidemiology of the triple burden in Low- and Middle-Income countries (LMIC)
• Despite declines in many countries, child stunting and underweight remain significant public health problems
• Multiple micronutrient deficiencies in children and women during the reproductive years persist and are rising in some settings.
• Iron deficiency is the most prevalent of micronutrient deficiencies among children and women of childbearing age, especially during pregnancy
• Overweight and obesity are increasing among all age groups, with the most rapid increases among lower income groups

Global trends in child (under 5 years) stunting
Vaivada T, Akseer N, Akseer S, Somaskandan A, Stefopulos M, Bhutta ZA. Stunting in childhood: an overview of global burden, trends, determinants, and drivers of decline. Am J Clin Nutr. 2020;112(Supplement_2):777S-791S.


Population weighted average prevalence of underweight, overweight, and obesity for women aged 20–49 years, UN regions and globallyRobert E Black , et al. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 2013; 382(9890): 427 – 451.

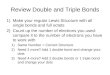
Estimates of the proportion of obese children and adolescents aged 5–19 years, by region, published by the Non-Communicable Diseases Risk Factor Collaboration
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
Female Male Female Male Female Male Female Male Female Male Female Male Female Male Female Male Female Male
Sub-SaharanAfrica
South Asia East andSoutheast Asia
High-incomeAsia-Pacific
Latin Americaand the
Caribbean
North Africa,the Middle
East andCentral Asia
High-incomeWesterncountries
Central andEastern Europe
Oceania
Pro
po
rtio
n1975 2016
Di Cesare et al. “The epidemiological burden of obesity in childhood: a worldwide epidemic requiring urgent action.” BMC medicine vol. 17,1 212. 25 2019

Studies from Indonesia:Nutritional Capacity Assessment in Indonesia: UNICEF, Indonesia Family Life Survey, Millennium Challenge Study
• Low birth weight: 10.2%
• Anemia • Children<5 years 36.8%
• Childbearing age women 22.7%
• Pregnant women 37.1%
2014-15 Survey in South Sumatra, Central Kalimantan,
and West Kalimantan. Children aged 0-35 months in 190
keca-matan (subdistricts) N= 2,469

Trends in Stunting, underweight, and risk of overweight in Indonesian Children IFLS 1993-2007
0
10
20
30
40
50
60
Stunted Underweight BMI Z>1
Pre
vale
nce
(%
)
Wave 1 (1993) Wave 2 (1997) Wave 3 (2000) Wave 4 (2007)
Stunting and underweight relate to:• Lower birth weight• Breastfed for >6 months• Parental undernutrition• Lack of maternal formal education
Overweight and obesity relate to:• Younger child age• Being male• Parental overnutrition• High paternal formal education
Rachmi, CN et al (2016). Stunting, Underweight and Overweight in Children Aged 2.0-4.9 Years in Indonesia: Prevalence Trends and Associated Risk Factors. PloS one, 11(5), e0154756.

Stunting, wasting and overweight trends in Indonesian children (UNICEF)• In 2018, nearly 3 in 10 children under 5 years of age were stunted while 1
in 10 were wasted. A fifth of primary school-aged children are overweight or obese.


The triple burden occurs at multiple levels
• Individual
• Household
• Community
• Country/population

• Overweight/obesity and undernutrition in the same person• Concurrent:
• Stunting with overweight or obesity in children and adolescents
• Short stature and central adiposity in adults
• Overweight/obesity with micronutrient deficiencies (e.g. iron deficiency anemia) in children and adults
• Over the life course in individuals: • Prenatal undernutrition→ low birth weight → higher adiposity later in life
• Stunting and/or wasting in childhood followed by increased adiposity in adulthood
The triple burden in individuals

White Caucasian, 3500 g Indian, 2700 g
Offspring of malnourished Indian mothers have deficits in lean body mass but a higher percentage of body fat: the “thin fat” phenotype
Yajnik CS Proc Nutr Soc 2004; 63:387-96

The triple burden: Individuals over the life course
• Developmental Origins of Adult Health and Disease (DOHaD) research links undernutrition in utero or infancy with increased risk of obesity in later life
• Nutrient-sparing/energy saving adaptations that enhance survival in nutrient-restricted prenatal environments may increase risk of obesity and related cardiometabolic diseases when the postnatal environment provides plentiful calories
• Excess weight gain following prior undernutrition may be unhealthy if it is comprised of mostly adipose tissue rather than lean mass

Sequential stunting and obesity
• Some evidence that stunted children develop physiologic mechanisms to poor nutrition to favor energy conservation and storage of fat. This can be detrimental when consuming energy dense diets.
• Fat deposition may be disproportionately central/abdominal.
• BUT… our COHORTS study in 5 LMICs and other studies show NO increased risk of obesity in adults who were stunted in the first 2 years of life.
• Risk may depend on how much environmental conditions change and on diet and activity patterns
0.0%
2.0%
4.0%
6.0%
8.0%
10.0%
12.0%
14.0%
16.0%
Mal
es
Fem
ales
Mal
es
Fem
ales
Mal
es
Fem
ales
Mal
es
Fem
ales
Mal
es
Fem
ales
Pelotas Guatemala New Delhi Cebu Soweto
Not Stunted Stunted

Obesity and anemia
Obesity (especially central adiposity)
Inflammation Elevated hepcidin & other inflammatory biomarkers
Decreased serum iron
Decreased iron absorption
Iron Deficiency Anemia
Limited exercise capacity
Inactivity
Fatigue
Other factors:Higher iron needs?Diet high in energy, low in bioavailable iron

Evidence for the obesity-iron deficiency link
• Meta-analysis of 26 studies involving 40,000 participants:• Persons with overweight or obesity had 31% higher odds of developing Iron
Deficiency Anemia (IDA) [Zhao et al 2015]
• Bangladeshi Women of reproductive age: • Overweight and obesity are highly prevalent among women with IDA (43% vs
to 34% at comparable age in other studies) [Binte Ali et al. 2020 MCN]
• Mexican Women: • At similar iron intake levels, individuals with overweight/obesity have lower
serum iron and iron binding capacity [Cepada-Lopez et al. 2011]

The Triple Burden within Households
• Individuals with overweight or obesity and undernourished individuals living in the same household
• Different generations• Overweight/obese mother, underweight, stunted, or micronutrient deficient child
• Poor quality diets and high rates of infections cause poor growth (stunting) and micronutrient deficiencies in children, who have high micronutrient, protein and energy needs
• Adults with high energy density diets and low physical activity gain weight despite poor diet quality
• Overweight/obese mother who has difficulty breastfeeding
• Overweight child, underweight mother or grandmother• Preferential allocation of food to the child (China 4:2:1 Grandparent:parent:child ratio)
• Same generation• Sibling differences, reflecting age differences or gender norms resulting in inequitable
intrahousehold food distribution or gendered behaviors

The Triple Burden: Community and country level
• Most commonly reported, based on separate survey statistics for each outcome
• Overweight/obesity and undernutrition in different segments of the population
• Regional: different areas with different resources• By SES within countries or communities• Urban-rural differences

Estimates of country-level dual burden prevalence are based on overall prevalence of stunting and overweight/obesity
Increasing dual burden prevalence largely reflects increases in overweight and obesity

Populations: Studies
beginning 20 years ago:
Wasting and Overweight
and in Preschool
Children
de Onis M, Blössner M. Prevalence and trends of overweight among preschool children in developing countries. Am J Clin Nutr 2000;72:1032–39.

Wojcicki BMC Public Health 2014 14:1124 doi:10.1186/1471-2458-14-1124

Individual data from the same surveys
Low Income countries:• 2.3% of all children were
stunted and overweight• 5.7% of stunted children were
overweight
In middle income countries:• 2.9% were stunted and
overweight• 9.9% of stunted children were
overweight
Country Level data (DHS surveys through 2012) on Stunting and Overweight in children < 5 years

Estimates of the prevalence of the dual burden of stunting and overweight/obesity in Indonesia
• 11% Rural Indonesia 2000-2003 (Indonesia Nutrition Surveillance System)
• 16% IFLS
• 19% 12,048 households IFLS 2007
• 30.6% Rural West Java (using BMI<23.5 kg/m2).
• 24.7% Urban Surabaya (36.4% child stunting, 70.2% maternal overweight/obesity)
Mahmudiono, T.; Segalita, C.; Rosenkranz, R.R. Socio-Ecological Model of Correlates of Double Burden of Malnutrition in Developing Countries: A Narrative Review. Int. J. Environ. Res. Public Health 2019, 16, 3730.

Causes
SES disparities are strongly related to stunting, overweight and obesity, and micronutrient deficiencies

.
SES disparities in Prevalence of stunting (HAZ <–2 )
and overweight (BMI Z >2 ) among children <5 in
highest and lowest wealth quintiles in selected countries
Red circles = lowest wealth quintileBlue circles = highest wealth quintile
Black RE, et al. Maternal and child undernutritionand overweight in low-income and middle-income countries. Lancet. 2013 Aug 3;382(9890):427-51
Stunting
Overweight

Dual Burden within Households: 1990s data from Brazil, China, Indonesia, the Kyrgyz Republic, Russia, Vietnam and the US
• 22–66% of households with an underweight person also had an overweight person.
• Highest prevalence of dual burden was in countries in the middle range of gross national product (GNP).
• Compared to underweight only households, dual burden households were more likely to be urban and have higher income.
• Compared to overweight only households, in Brazil and Russia, dual burden households were more likely to be urban and lower income, but in China, Indonesia, the Kyrgyz Republic, US Vietnam they were similar.
Percentage of households with an overweight and an underweight person, ordered by GNP. Shaded bars are estimates adjusted for household size.
Doak CM, Adair LS, Bentley M, Monteiro C, Popkin BM. The dual burden household and the nutrition transition paradox. Int J Obes (Lond). 2005 Jan;29(1):129-36.

• Changes in nutritional status that accompany economic growth, globalization, technological change
• Changes largely reflect
• DIET
• PHYSICAL ACTIVITY
• CONSEQUENCE = increased overweight/obesity and a transition from infectious to chronic disease
The Triple Burden is a consequence of the Nutrition Transition

Major Global Dietary Shifts
• Increased intake of:• Caloric sweeteners• Oil in most LMIC• Animal source foods• Processed and ultra-processed foods, refined carbohydrates
• Reduced intake of:• Fruits and vegetables and legumes
• Reduced food preparation time, increased intake of pre-cooked, “fast” and processed foods
• More snacking, away-from-home eating

From Traditional to Modern, Processed Foods

Young Indonesian children frequently consume commercially produced snack foods
• Household spending on beverage and packaged foods across all income levels: expenditures on packaged foods 18-32% of monthly HH expenditure (Deloitte 2015)
• Widespread consumption of snack foods: 54% of 6-24 month oldchildren in East Java ate commercial biscuits, fried snacks, cakes or sweets in past 24 hours
Matern Child Nutr. 2019 Jun; 15(Suppl 4): e12764. Published online 2019 Jun 21. doi: 10.1111/mcn.12764

High intake of sugary snack foods among Indonesian childrenPercentage of Bandung City 0-3 year old children who consumed commercial snack foods or sugar-sweetened beverages in the past week
0
10
20
30
40
50
60
70
80
90
100
Commercial Snack Food Commercial SSB
6 to 12 12 t0 18 18 to 24 24 to 30 30 to 36
What are they consuming?
0 20 40 60 80 100
Sweet biscuits
Savory snacks
Candy
Cakes
Ice cream
Instant noodles
Sweetened milks
Sweetened teas
Packaged juices
Soda
Green et al. Matern Child Nutr. 2019 Jun; 15(Suppl 4): e12764

Changing patterns of sedentary and moderate to vigorous physical activity
• Less • Physically demanding occupations
• Physically demanding household chores
• Transportation-related activity (less walking, more driving)
• More• Screen time (TV, other electronic media)
• Sedentary leisure activities

From Traditional to Modern Market Work

From Traditional to Modern Leisure

Ng S.W. & Popkin B.M. Obesity Reviews (2012). “Modernization , Time Use and Physical Activity: A shift away from movement across the globe“
0
5
10
15
20
25
30
35
100
150
200
250
2002 2006 2010 2014 2018 2022 2026 2030
Ave
rage
ho
urs
per
wee
k b
ein
g Se
den
tary
Ave
rage
MET
-ho
urs
per
wee
k
Year
Active leisure
Travel
Domestic
Occupational
Sedentary time
by 2030: 151 MET-hr/week
2008: 214 MET-hr/week
by 2020: 180 MET-hr/week
Brazilian Adults Met-hours per Week Of Physical Activity & Hours/Week Of Time In Sedentary Behavior:
Measured For 2002-2008 And Forecasted For 2009-2030

Double Duty Actions
A term coined in the 2015 Global Nutrition Report
Interventions, programs, and policies that simultaneously prevent or reduce the risk of nutritional deficiencies leading to underweight, wasting, stunting and micronutrient deficiencies, and to obesity related non-communicable diseases.
Actions aim to maximize benefits of addressing one form of nutrition to benefit another
SDGs stress addressing malnutrition IN ALL OF ITS FORMS

Double Duty Actions
• Historically, the focus of national nutrition programs and donor efforts have been on undernutrition
• Overweight, obesity, and associated non-communicable diseases (NCDs) are rising rapidly in LMICs
• Mechanisms to address these 2 conditions have been separate, BUT…
• There is an urgent need to address these problems SIMULTANEOUSLY, and use the same platforms for both (Hawkes et al, Lancet Series)

Guiding Principles for Actions
• Focus on shared drivers of under and excess nutrition
• Address needs at all stages of the life course because effects are synergistic or cumulative
• Recommendations need to be multisectoral and coordinated

Understanding shared drivers of stunting, micronutrient deficiencies and obesity can inform prevention strategies
• UNICEF Conceptual Model adapted for stunting based on 2020 review
• Adaptable to address overweight and obesity

Child StuntingChild CharacteristicsLBW, IUGR, multiple birth
Child sex
Maternal CharacteristicsAge, adolescent pregnancy, maternal
anemia, malaria,Maternal BMI, height, parity, pregnancy
interval
DiseaseInfections, ARI, vitamin/mineral deficiencies
Inadequate dietary intakeDiet diversity, micronutrients, breastfeeding
Unhealthy household environment
Urbanization, water and sanitation, crowding
Inadequate care and health services
Vaccination, skilled birth attendance, antenatal care, access
to health facilities, preventive health care, nutrition supplements
Inadequate feeding practices and food insecurity
Breastfeeding, complementary feeding
Nutrition Sensitive and Specific ProgramsCash transfer, national nutrition policies, MCH health programs
Basic Causes(Distal)
Socioeconomic FactorsWealth, education, occupation
Macrolevel social, economic, political and environmental context and factors
Basic Causes(Intermediate I)
Underlying Causes(Intermediate II)
Immediate Causes(Proximal)
Vaivada T, et al Stunting in childhood: an overview of global burden, trends, determinants, and drivers of decline. Am J Clin Nutr. 2020;112(Supplement_2):777S-791S.

Overweight & ObesityChild CharacteristicsLBW, IUGR, multiple birth
Child sex
Maternal CharacteristicsAge, nutritional history, parity
Inadequate Physical ActivitySedentary jobs, screen time, lack of leisure time exercise
Inappropriate dietary intakeHigh energy, low micronutrients
Unhealthy household environment
Urbanization, water and sanitation, crowding, safety,
chemical exposures
Inadequate care and health services
MCH services (prevention of LBW, IUGR, growth faltering)
Adolescent health services, OW/OB screening
Inadequate feeding practices and food insecurity
Breastfeeding, complementary feeding, high energy density foods, SSBs
Nutrition Sensitive and Specific ProgramsCash transfer, national nutrition policies, MCH health programs
Basic Causes(Distal)
Socioeconomic FactorsWealth, education, occupation
Macrolevel social, economic, political and environmental context and factors
Basic Causes(Intermediate I)
Underlying Causes(Intermediate II)
Immediate Causes(Proximal)

All stages of the life course
• PrenataI: Optimize fetal growth, physiology and body composition• Prevent LBW (IUGR and preterm birth)
• Optimize infant and young child nutrition and health• Promote and support breastfeeding• Emphasize the linear growth and appropriate weight• Promote appropriate complementary foods and supplements (when needed) • Promote healthy environments (WASH, toxic exposures)
• SchooI-age children: balance promotion of healthy diets and physical activity.
• Focus on adolescent diet and health to with added benefit of addressing prepregnacy health and nutritional status
At all stages, combine management of concurrent under and over nutrition.

Multisectoral
• Health services to optimize maternal health, birth outcomes, and early child growth and development
• Social safety nets
• Educational settings: school environments and programs
• Agriculture, food systems and food environments • Address multiple aspects of the food environment
• Establish food policies that promote healthy diets

Recommended Actions: Hawkes et al. Lancet 2020
Health services
1. Scale up new WHO antenatal care recommendations to promote
optimal maternal health and weight gain
2. Scale up programs to protect, promote, and support breastfeeding
3. Redesign guidance for complementary feeding practices and related
indicators: avoid feeding high energy, sugar, salt products, include
obesity prevention guidance
4. Redesign existing growth monitoring (GMP) programs
5. Prevent undue harm from energy-dense and micronutrient-fortified
foods and ready to use supplements

Recommended Actions: Hawkes et al Lancet 2020
Social Safety Nets6. Redesign cash and food transfers, subsidies, and vouchers:
Educational Settings7. Redesign school feeding programs and devise new nutritional guidelines for food in and around educational institutions
Agricultural, food systems, food environments
8. Scale up nutrition-sensitive agriculture programs9. Design new agricultural and food system policies to support healthy diets10. Implement policies to improve food environments from the perspective of malnutrition in all its forms

The Lancet 2020 395142-155DOI: (10.1016/S0140-6736(19)32506-1)
Double Duty Actions

Roles and Responsibilities of stakeholder groups: Hawkes et al. Lancet 2020

Summary and conclusions:UNICEF focus on Southeast Asia and the Pacific Triple Trouble: Research and Analysis on the Multiple Burdens of Malnutrition in Southeast Asia and the Pacific Region
“Over the last 20 years, the East Asia and the Pacific Region has made dramatic progress in child nutrition, with a 55 per
cent reduction in the number of stunted children (38 million to 17 million). However, the region is facing a stagnation in
reducing undernutrition, while witnessing one of the world’s fastest growing rates of childhood obesity. With our analysis
indicating that malnutrition is driven by poor maternal nutrition, low quality diets, inequity and poverty, we call for five
concerted actions:
1. Addressing all forms of malnutrition across the life cycle
2. Improving women's nutrition
3. Supporting an integrated multisectoral approach
4. Expanding nutrition‐sensitive social protection programmes
5. And strengthening data collection, analysis and use.”

Lancet Series on the Dual Burden 2019-20
A future direction for tackling malnutrition: Vol. 395, No. 10217Dynamics of the double burden of malnutrition and the changing nutrition realityBarry M Popkin, Camila Corvalan, Laurence M Grummer-StrawnVol. 395, No. 10217The double burden of malnutrition: aetiological pathways and consequences for healthJonathan C Wells, Ana Lydia Sawaya, Rasmus Wibaek, Martha Mwangome, Marios S Poullas, Chittaranjan S Yajnik, Alessandro DemaioVol. 395, No. 10217Double-duty actions: seizing programme and policy opportunities to address malnutrition in all its formsCorinna Hawkes, Marie T Ruel, Leah Salm, Bryony Sinclair, Francesco BrancaVol. 395, No. 10218Economic effects of the double burden of malnutritionRachel Nugent, Carol Levin, Jessica Hale, Brian HutchinsonVol. 395, No. 10218