-
Dosimetric comparison of brachyterapy
techniques for APBI
Tibor MajorNational Institute of Oncology, BudapestNational
Institute of Oncology, Budapest
Euro-Asian Breast Brachytherapy School, October 9-10. 2014,
Erlangen
-
Outline
• classification of BT irradiation techniques for APBI
• dosimetry and optimization in multicatheter interstitial
BT
• single lumen balloon and multilumen applicators
• intraoperative electronic brachytherapy with X-ray
• beyond the TG-43 brachytherapy dose calculation formalism
-
APBI
brachytherapy
endocavitary
interstitial electronic
endocavitary
MammoSite Contura SAVI ClearPath
HDR seedIntrabeam Axxent
-
• classification of BT irradiation techniques for APBI
• dosimetry and optimization in multicatheter interstitial
BT
• single lumen balloon and multilumen applicators
• intraoperative electronic brachytherapy with X-ray
• beyond the TG-43 brachytherapy dose calculation formalism
-
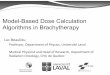
Dose dependence on distance in brachytherapy
0,8
1
1,2
1,4
Rel
ativ
e do
se
Ir-192
Ra-226
Correction for absorption and scattering in water
2x1
D ≈
0
0,2
0,4
0,6
0 1 2 3 4 5 6 7 8 9 10 11
Rel
ativ
e do
se
Distance (cm)
I-125Pd-103
inverse square law inhomogeneous dose distribution
-
Dose homogeneity in brachytherapy
Dose non-uniformity ratio (DNR)
Dose homogeneity index (DHI) for implant
100
150
VV
DNR =
DNRV
VVDHI
100
150100 −=−= 1
Dose homogeneity index (DHI) for target
V100V150V100
DHI−=
V100 = volume receiving equal to or greater than the prescribed
dose
V150 = volume receiving equal to or greater than 1.5 x the
prescribed dose
V100 = percentage volume of the target receiving equal to or
greater than the prescribed dose
V150 = percentage volume of the target receiving equal to or
greater than 1.5 x prescribed dose
For homogeneous dose distribution the DNR is low and DHI is
high
-
Definition of dose non-uniformity ratio (DNR)
Vref V1.5xref
V1.5xrefDNR =
Vref
DNR is specific to the implant geometry and prescription
isodose
The dose distribution is optimal when the DNR is minimal
Vref = volume receiving equal to orgreater than the reference
dose
V1.5xref = volume receiving equal to or greaterthan 1.5 x the
reference dose
-
PTV
ref
VPTV
CI =
Definition of coverage index (CI) and conformal index (COIN)
ref
ref
PTV
ref
VPTV
VPTV
COIN ⋅=
Both indices (CI, COIN) have to be maximized during opti
mization
-
1. No optimization (Paris Dosimetry System)• uniform dwell
times
2. Forward optimization• manual optimization (editing dwell
times/weights)• geometrical optimization (on distance and volume)•
polynomial optimization on
Optimization methods in HDR BT
• polynomial optimization on- distance dose points (dwell time
gradient restrictions)- volume dose points (SSDS – extension of
PDS)- dose points on the target surface (conformal)
• graphical optimization (only for local adjusments)
3. Inverse optimization (IPSA)• anatomy based with surface and
volume dose objectives
-
Manual optimization
changing dwell times individually
-
Geometrical optimization
- no dose points are needed (only for normalization) - the dwell
time at a dwell position is inversely proportional to the
dosedelivered by other dwell positions
- the dose at the dwell position given by another dwell position
isinversely proportional to the square of its distance to that
dwell position
-
Graphical optimization
-
Distance dose points50 %
100 %150 %
Paris50 %
100 %150 %
Dose distributions at different optimizations for radiogra
phy-based implants
GO50 %
100 %150 %
Conformal50 %
100 %150 %
-
CI DNR COIN
Distance dose points 0.70 0.35 0.40
Paris system 0.61 0.25 0.34
Average values of volumetric indices for 17 patients
GO 0.66 0.25 0.50
Conformal 0.92 0.55 0.74
Since no optimization method can compensate for the inadeq uate
implant
geometry, preimplant 3D anatomical information is requ ired for
planning the
catheter positions in order to obtain optimal dose distribu
tion.
Major et al. Strahlenther Onkol 181:89-96. 2005
-
Preimplant CT for defining the catheter positions
-
3D anatomical and catheter reconstruction
-
Conformal dose distribution after geometrical and graphi cal
optimization
-
GO vs. GO + GRO(25 patients)
GO GO + GRO p
CI 0.87 0.91 0.0003
DNR 0.30 0.33 0.0098DNR 0.30 0.33 0.0098
COIN 0.64 0.67 < 0.0001
GO: geometrical optimizationGRO: graphical optimization
The graphical optimization improved the quality of dose
distributions
-
GO + GRO
Conformal
GO + GRO vs. CONF
Conformal
-
GO + GRO vs. CONF(28 patients)
GO + GRO CONF p
CI 0.91 0.88 0.0013
DNR 0.33 0.54 < 0.0001
COIN 0.68 0.77 < 0.0001COIN 0.68 0.77 < 0.0001
Vref (ccm) 75.3 64.3 < 0.0001
GO: geometrical optimizationGRO: graphical optimizationCONF:
conformal (dose point optimization)
Major et al. Radiother Oncol 90:48-55. 2009
The conformal dose point optimization provided highly conformal
plans,but at the cost of unacceptable high dose inhomogeneity
-
Interstitial breast brachytherapy study
Interstitial brachytherapy alone vs. external beam radia tion
therapy after breastconserving surgery for low risk invasive
carcinoma and low risk duct carcinomain-situ (DCIS) of the female
breast
Phase III Multicenter Trial - European Brachytherapy Breast
Cancer GEC-ESTRO Working Group
DVH analysis for plan evaluation
Conventional planning
• Vref, V1.5xref, V1.5xMCD• DNR ( 0.90)• DHI• COIN
-
Average plan parameters for 49 patients(GEC-ESTRO Phase III.
trial)
Major et al. Brachytherapy 10:421-426. 2011
-
Author n V90 V100 D90 DHI
Fluoroscopy guided + postimplant CT Vicini (1999)Kestin
(2000)Cuttino (2005)Weed (2005)Major* (2005)
811151017
NRNR
89%68%76%
68%68%
96% †
58%70%
69%NRNRNR
72%
0.890.830.77NR0.65
Clinical studies reporting dose-volume parametersof
high-dose-rate interstitial breast brachytherapy
CT image-guided (pre-, postimplant CT)Kolotas (1999)Das
(2004)Cuttino (2005)Aristei (2007)Major** (2011)
4250144649
NRNR
95%NR
96%
90%95%
98% †
NR92%
NRNRNR
96%102%
NR0.730.820.760.65
*Major et al.: Strahlenther Onkol 181:89-96. 2005**Major et al.
Brachytherapy 10:421-426. 2011
n = number of patients, NR = not reported, * for PTV 2 cm, † for
PTV 1 cm, ‡ dose homogeneity index for the implant
-
Permanent breast seed implant technique
Dpresc = 90 GyMean no. of. Pd-103 seeds: 75Mean no. of needles:
17Mean total activity: 181.8 UPreimplant V100 = 97%Postimplant V100
= 88%
Pignol et al. IJROBP 64:176-81.2006Keller et al. IJROBP
83:84-92.2012
-
0,6
0,8
1,0
1,2
1,4
Re
alt
ive
do
se
Radial dose funtions for different isotopes
Ir-192
0,0
0,2
0,4
0,6
0 1 2 3 4 5 6 7 8 9 10
Re
alt
ive
do
se
Distance (cm)
I-125Pd-103
-
Permanent breast seed implant with Pd-103 or I-125 ?
Emean= 21 keVT1/2= 17 days
Emean= 27.4 keVT1/2= 59 days
The 1% isodose line is just below the skin for the Pd-103,
whereas the 5% isodose line is about at the same position for the
I-125 case. The Pd-103 implant is associated with a rapid dose fa
ll-off.
Less than 5 mSv dose to the patient’s partner with Pd-103
seeds
Keller et al. IJROBP 62:358-365. 2005
-
• classification of BT irradiation techniques for APBI
• dosimetry and optimization in multicatheter interstitial
BT
• single lumen balloon and multilumen applicators
• intraoperative electronic brachytherapy with X-ray•
intraoperative electronic brachytherapy with X-ray
• beyond the TG-43 brachytherapy dose calculation formalism
-
Intracavitary BT applicators
MammoSite balloon catheter
- single and multilumen (central + 3 lumens)
Contura Multiple Lumen Balloon Catheter
- central + 4 lumens
ClearPath Brachytherapy System
- 6 tubes
SAVI (Strut-Adjusted Volume Implant)
- 6-10 struts
-
MammoSite breast balloon applicator
single lumen for the Ir-192source
-
PTV generation with volume expansion
PTV csak emlıszövetet tartalmazPTV includes breast tissue
only
-
Dose distribution around MammoSite applicator
ref. point
Dose prescription point is at 1cm from balloon surface
point source linear source
compensation for the anisotropy of the Ir-192 source
-
Dose homogeneity vs. balloon diameter
Dmax at the balloon surface is in the range of 175 – 250% of the
prescribed dose
-
Volume parameters for interstitial and MammoSite BT
IBCONV - conventional interstitial brachytherapyIBCONF -
conformal interstitial brachytherapyMSB - MammoSite
brachytherapy
Major et al. Radiother Oncol 79:321-28. 2006
-
Quality indices for interstitial and MammoSite BT
IBCONV - conventional interstitial brachytherapyIBCONF -
conformal interstitial brachytherapyMSB - MammoSite
brachytherapy
Major et al. Radiother Oncol 79:321-28. 2006
-
Dose parameters for interstitial and MammoSite BT
IBCONV - conventional interstitial brachytherapyIBCONF -
conformal interstitial brachytherapyMSB - MammoSite
brachytherapy
Major et al. Radiother Oncol 79:321-28. 2006
-
Skin and chest wall dose with multi-catheter (MC) a nd
MammoSite(MS) breast brachytherapy: Implications for late toxi
city
The dosimetric data for 43 patients treated with the MC
technique and 83 patients treated with the MS at Virginia
Commonwealth University were reviewed.
Cuttino et al. Brachytherapy 8:223-226. 2009
The MC technique results in more conformal dose delivery, with
significantly lower mean skin and chest wall doses.
-
Single and multiple dwell position methods in MammoSite
single dwell position multiple dwell positions
Kim et al. JACMP 11:54-63. 2010data from plans of 19
patients
-
Drawbacks of MammoSite applicator
- circular dose distribution in perpendicular plane to balloon
axis
- balloon asymmetry leads to asymmetric PTV coverage
- the dose to OARs is determined by their position relative to
the applicator
- the only option to reduce dose to the organs at risk (OARs) is
by reducing
the prescription dose and hence the target dose
multilumen applicator
-
Optimization and comparison of balloon-based partia l breast
brachytherapyusing a single source, a standard plan line source,
and both forward and
inverse planned multilumen (ML) techniques(12 patients, virtual
ML plans)
single source line source
forward ML inverse ML
- multiple sources in a single catheter improve coverage at
catheter ends, whereas ML can further improve coverage and reduce
dose to organs at risk.
- patients previously ineligible for treatment with a single
catheter may be treated using ML applicator.
Eyre et al. Brachytherapy 12:107-113. 2013
-
Other multilumen breast applicators
Contura multi-lumen balloon (MLB) ClearPath applicator SAVI
applicator
-
- avoidance of high dose in the skin - reduction of the size of
an air/fluid pocket in the planning target volume through the use
of vacuum ports
Advantages of Contura multilumen balloon catheter over
MammoSite
Contura multi-lumen balloon (MLB) applicator
5 mm
Central lumen + four catheters
-
Contura catheter has a sixth lumen (vacuum ports)through which
air/fluid can be removed
before suctioning air after suctioning air7.7 % of PTVEVAL 0.4 %
of PTVEVAL
Suctioning air/fluid improves tissue-balloon conformance,
thereby allowing a higherdose of radiation to be delivered to the
breast tissue at greatest risk of tumor cells.
-
Contura vs. MammoSite catheter regarding the applicabil ity for
APBI
Two treatment planning goals:- maximum skin dose
-
Dosimetrical comparison between multilumen MammoSiteand Contura
Multilumen Balloon applicators
(median values in % of prescribed dose)
V95 V150 V200 Skinmax Ribmax
ML MammoSite (8 pts.) 98.0 31.6 7.4 92.5 92.7
Contura (12 pts.) 97.6 28.2 7.5 98.2 104.0Contura (12 pts.) 97.6
28.2 7.5 98.2 104.0
Both applicators have shown the ability of dose shaping for
providing
sufficient target coverage while concurrently limiting dose to
skin and rib
Fu et al. University of Pittsburgh Cancer Institute, Pittsburgh,
PA
-
Improvements of dose distributions with inverse planning
(IPSA)
- 4 treatment plans for 24 patients- 2 optimization methods
(IPSA, dose points)- 2 types of applicators (Contura multilumen,
simulated single lumen)
Skowronek et al. J Contemp Brachytherapy 5:134-38. 2013
- dose distribution obtained using multi-lumen IPSA optimized
application was characterized with the highest target coverage
while preserving acceptable doses to organs at risk
- optimization method was proven to be more important than the
number of catheters in the applicator, however, overall outcome of
multi-lumen application gives more possibilities of dose
distribution adjustment
-
ClearPath breast applicator
6 catheters
-
Multicatheter hybrid breast brachytherapy: A potenti al
alternative for patients with inadequate skin distance
- 11 patients not treated with MammoSite due to inadequate skin
distance- simulated plans with ClearPath catheter
Beriwal et al. Brachytherapy 7:301-304. 2008
The hybrid CP catheter reduced the skin dose significantly
without compromising the planning target volume coverage, DHI, or
dose to other critical organs.
-
MammoSite ClearPath p
PTV coverage
V90% 99.6 99.7 ns.
V100% 96.5 96.5 ns.
High dose region
V150% 42.1 42.9 ns.
V200% 11.4 15.2 < 0.05
A dosimetric comparison of MammoSite and ClearPath bra
chytherapy devices(mean values for 15 patients)
V200% 11.4 15.2 < 0.05
OAR
Ipsilateral breast (V50%) 19.8 18.0 < 0.05
Ipsilateral lung (V30%) 3.7 2.8 < 0.05
Heart (V5%) 57.0 54.3 < 0.05
Maximal skin dose (%) 92 80 < 0.05
Dickler et al. Brachytherapy 8:14-18. 2009
The MammoSite and ClearPath methods of PBI offer comp arable
target volume coverage,
however the ClearPath device achieves increased OAR sparing.
-
Strut-Adjusted Volume Implant (SAVI) applicator(central + 6-8-10
peripheral struts)
-
Clinical implementation of SAVI
- the dose distribution can conform to the modified PT V
(PTVEVAL)- less skin dose- patients not eligible for MammoSite can
be treated with SA VI
Scanderberg et al. Radiother Oncol 90:36-42. 2009
-
Clinical experience with the SAVI brachytherapy appli cator
SAVI applicator with very close skin margin skin dose is kept
low
Yashar et al. Brachytherapy 8:367-372. 2009
Almost half of evaluated patients were not candidates for other
single-entry
brachytherapy devices because of skin spacing or brea st size,
demonstrating an
expansion of candidates for single-entry partial br east
brachytherapy
-
- 9 patients treated with SAVI- plans for MammoSite and
3D-CRT
Evaluation of three APBI techniques under NSABP B-3 9
guidelines
preimplant 3D-CRTSAVI
Scanderberg et al. J Appl Clin Med Phys 11:274-280. 2010
The maximum rib, lung and skin doses were lowest for the
SAVI
-
Nonivasive image-guided breast brachytherapy (AccuBoost
system)
Hepel et al. Brachytherapy 2014
- the breast is positioned between the compression plates and
immobilized with gentle compression- a kV image is obtained where
the tumor bed is identified- appropriately sized and shaped
applicators are selected to target, the position is determined by
the localization grid- the applicators are attached to an Ir-192
HDR afterloader for treatment delivery- the process is then
repeated in an orthogonal axis.
Composite dosimetry using a fixed model
-
Dosimetric characterization of AccuBoost system
applicators
Geometry for MC calculations
Experimental setup for measurements
30 mm depth 0 mm depthClinical application
Rivard et al. Med Phys 36:5027-32. 2009
Geometry for MC calculations 30 mm depth 0 mm depth
Isodose distribution for parallel-opposed„beams” using two
applicators with Θ6 cm
Dose profiles on film and with MC Dose distributionson
radiochromic film
Clinical application
-
• classification of BT irradiation techniques for APBI
• dosimetry of and optimization in multicatheter interstitial
BT
• single lumen balloon and multilumen applicators
• intraoperative electronic brachytherapy with X-ray
• beyond the TG-43 brachytherapy dose calculation formalism
-
Intrabeam X-ray (Carl Zeiss Meditec AG)(max. 50 kV)
X-ray source
Floor stand Spherical aplicatorswith diameters of
1.5 – 5.0 cm
spherical dosedistribution
TARGIT-A study (TARGeted Intraoperative radioTherapy) 5-year
results in Lancet 2013
-
Intrabeam clinical application – single treatment for appr ox.
30 minutes
20 Gy at the surface5-7 Gy at 1 cm depth
high hose gradient
large dose inhomogeneity
-
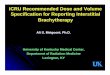
Radial dose functions for isotopes and photon energies use d in
BT
Rivard et al. Med Phys 33:4020-32, 2006
-
Axxent TM eBx system (Xoft Inc., CA, USA)(40 – 50 kV X-ray)
- similar dose distribution to LDR I-125- similar dose rate to
HDR Ir-192 (0.6 Gy/min)- can be switched off
radiation source in a balloon applicator
-
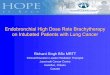
Contura multilumen balloon BT vs. 50 kV X-ray IORT
- 14 patients treated with Contura- replanning for 50 kV X-ray
system with TG-43 data for Xoft system
50 kV X-ray Contura20 Gy15 Gy10 Gy
20 Gy15 Gy10 Gy
Jones et al. Brachytherapy
http://dx.doi.org/10.1016/j.brachy.2014.04.005
A representative comparison of dose distributions
-
The HDR brachytherapy plans were superior to 50 kV superficial
photon plans forIORT in all dosimetric parameters except for the
heart and rib dosimetric parameters
Jones et al. Brachytherapy
http://dx.doi.org/10.1016/j.brachy.2014.04.005
-
• classification of BT irradiation techniques for APBI
• dosimetry of and optimization in multicatheter interstitial
BT
• single lumen balloon and multilumen applicators
• intraoperative electronic brachytherapy with X-ray•
intraoperative electronic brachytherapy with X-ray
• beyond the TG-43 brachytherapy dose calculation formalism
-
),()(),(
),(),( Θ⋅⋅
ΘΘ⋅Λ⋅=Θ
•rFrg
rG
rGSrD k
00
Med. Phys. 22:209-234. 1995.
Sk = air-kerma strengthΛ = dose rate constantG(r,Θ) =
geometrical functiong(r) = radial dose functionF(r,Θ) = anizotropy
function
-
- no inhomogeneity correction (CT/MRI/UH only in the backg round
for
catheter/applicator reconstruction)
- assumption of full scattering condition (infinite mediu m)
- no correction for source movement of HDR source (only dwe ll
times)
- no correction for applicator/catheter absorption
- no correction for seed absorption
Limitations of TG-43 formalism
Model-based dose calculation algorithms (MBDCAs) either
explicitly simulate thetransport of radiation in the actual media
or employ multiple dimensional scatter integration techniques to
account for the dependence of scatter dose on the 3D geometry.
Beaulieu et al. Med Phys 39.6208-36. 2012
-
Dosimetrical comparison between TG43 and MBDCA for APBI
patients
Differences between dose calulations using TG-43 and TG-186
formalisms
Preliminary results based on 38 APBI patients data
On average, percentage differences between MBDCA and TG43-based
dosimetric indices are:- < 1% for the PTV and 1-1.5% for dose
homogeneity and conformity indices- 6% for skin (D0.1cc) -10% for
the lung (V10Gy) - with a strong correlation of the observed
differences to the target location
Bilateral research cooperation between Medical Physics
Laboratory, Medical School, University of Athensand National
Institute of Oncology, Radiotherapy Department, Budapest