Embed Size (px)
Citation preview

PII S0360-3016(01)01663-7
BIOLOGY CONTRIBUTION
DOSIMETRIC COMPARISON OF RADIONUCLIDES FOR THERAPY OFSOMATOSTATIN RECEPTOR–EXPRESSING TUMORS
PETER BERNHARDT, PH.D.,* SVEN ANDERS BENJEGÅRD, M.SC.,* LARS KOLBY, M.D., PH.D.,†
VIKTOR JOHANSON, M.D., PH.D.,‡ OLA NILSSON, M.D., PH.D.,† HÅKAN AHLMAN, M.D., PH.D.,‡ AND
EVA FORSSELL-ARONSSON, PH.D.*
Departments of *Radiation Physics,†Surgery, and‡Pathology, Lundberg Laboratory for Cancer Research, Sahlgrenska UniversityHospital, University of Go¨teborg, Go¨teborg, Sweden
Purpose: Therapy of tumors expressing somatostatin receptors,sstr, has recently been clinically tested usingsomatostatin analogues labeled with111In and 90Y. Several other radionuclides, i.e.,131I, 161Tb, 64Cu, 188Re,177Lu, and 67Ga, have also been proposed for this type of therapy. The aim of this work was to investigate theusefulness of the above-mentioned radionuclides bound to somatostatin analogues for tumor therapy.Methods: Biokinetic data of 111In-labeled octreotide in mice and man were used, primarily from our studies butsometimes from the literature. Dosimetric calculations were performed with the assumption that biokinetics weresimilar for all radionuclides bound to somatostatin analogues. The cumulated tumor:normal-tissue activityconcentration, TNC, was calculated for the various physical half-lives of the radionuclides. Using mathematicalmodels, the tumor:normal-tissue mean absorbed dose rate ratio, TN D˙ , and tumor:normal-tissue mean absorbeddose ratio, TND, were calculated for various tumor sizes in mice and humans.Results: TNC of radionuclide-labeled octreotide increased with physical half-life for most organs, both in miceand in humans. TN D showed that radionuclides emitting electrons with too high energy are not suitable fortherapy of small tumors. Furthermore, radionuclides with a higher frequency of photon emissions relative toelectron emissions will yield lower TN Dand are thus less suitable for therapy than radionuclides with a lowerfrequency of photon emissions. The TND was highest for161Tb in both mice and humans.Conclusions: The results demonstrate that long-lived radionuclides, which emit electrons with rather low energyand which have low frequency of photon emissions, should be the preferred therapy for disseminated smallsstr-expressing tumors. © 2001 Elsevier Science Inc.
Dosimetry, Therapy, Somatostatin analogues, Neuroendocrine tumors, Radionuclides.
INTRODUCTION
Neuroendocrine tumors frequently overexpress somatosta-tin receptors (sstr). Somatostatin analogues, e.g. octreotide,lanreotide, and Woc3a, have been labeled with the follow-ing radionuclides:131I (1), 111In (2), 90Y (3), 161Tb (4),64Cu(5), 188Re (6), and67Ga (7). After i.v. injection of theseradiolabeled somatostatin analogues in animals or humans,high activity concentrations insstr-expressing tumor tissuecompared to normal tissue were found, suggesting a poten-tial therapeutic role of these radiopharmaceuticals.
Initially 123I-Tyr3-octreotide was used to visualize endo-crine pancreatic tumors by single photon emission com-puted tomography (SPECT) (8). The results indicated apotential use of131I-labeled octreotide for systemic radia-tion therapy ofsstr-expressing tumors (9, 10). Today,111In-DTPA-D-Phe1-octreotide has become the dominant radio-labeled somatostatin analogue for visualization ofsstr-
expressing tumors (e.g. 11). The high111In activityconcentration in such tumors after i.v. injection of111In-DTPA-D-Phe1-octreotide has led to attempts with systemicradiotherapy using this compound (2, 11–13).
Several other radionuclides bound to somatostatin analogueshave been tried for therapy ofsstr-expressing tumors. Studiesin vitro and in rats have shown that161Tb-DTPA-D-Phe1-octreotide is a promising radiopharmaceutical both for intra-operative scintillation detection and radiation therapy (4). Re-cent animal studies using90Y-DOTA-octreotide have showncomplete regression of rat pancreatic tumors (14). Also, inclinical trials 90Y-DOTA-octreotide or90Y-DOTA-lanreotidereduced the growth rate of tumors and caused tumor regressionin individual cases (15, 16). Theb-emitter 131I has recentlybeen bound to the somatostatin analogue Woc-3a and admin-istered i.v. in therapeutic amounts (59 GBq) to a patient (1).Using intratumoral injection of the radiolabeled somatostatin
Reprint requests to: Peter Bernhardt, Department of RadiationPhysics, Go¨teborg University, Sahlgrenska University Hospital,S-413 45 Go¨teborg, Sweden. Tel:146-31-3421916; Fax:146-31-822493; E-mail: [email protected]
This work was supported by grants from the Swedish Cancer
Society (2998, 3427) and the Swedish Medical Research Council(5220, 6534).
Received Nov 6, 2000, and in revised form May 8, 2001.Accepted for publication May 10, 2001.
Int. J. Radiation Oncology Biol. Phys., Vol. 51, No. 2, pp. 514–524, 2001Copyright © 2001 Elsevier Science Inc.Printed in the USA. All rights reserved
0360-3016/01/$–see front matter
514

analogue188Re-RC-160, Zamoraet al.(6) obtained therapeuticeffects onsstr-expressing tumors in nude mice. High uptake of64Cu-TETA-Y3-TATE in sstr-expressing tumor tissue wasrecently shownin vitro and in vivo (5). Furthermore, biodis-tribution studies in rats have demonstrated high uptake of67Ga-DFO-octreotide insstr-expressing tissues (7), and177Luhas also been suggested as a suitable radionuclide for this typeof therapy (17). One of the limiting factors in radionuclidetherapy is the absorbed dose to normal tissues. The radionu-clides mentioned above emit either electrons or positrons to-gether with photons. The electrons and positrons will deposittheir energy locally (within a few nm to mm from the site ofdecay). On the other hand, the photons will contribute to thewhole-body irradiation, which should be kept low in radiationtherapy.
Most of the biokinetic data on radiolabeled somatostatinanalogues in man have been collected up to 72 h afterinjection (18–20). To predict the therapeutic efficacy ofmore long-lived radionuclides, long-term biokinetics areneeded. We have therefore followed the biokinetics up to 22days both for tumor and normal tissues in a patient withmetastatic midgut carcinoid, diagnosed and treated with111In-DTPA-D-Phe1-octreotide (11, 21). We have also stud-ied the biokinetics of111In-DTPA-D-Phe1-octreotide 0.5 hto 14 days after injection into mice bearing a GOT1 tumorxenograft derived from this patient (22, 23).
The aim of this study was to compare the dosimetry of theproposed radionuclides bound to somatostatin analogues forradiotherapeutic purposes. Human biokinetic data of111In-labeled octreotide from our own patients and the literature(cf. 18–21, 24) were used, together with long-term bioki-netics of111In-DTPA-D-Phe1-octreotide in GOT1-bearing nudemice (23).
METHODS AND MATERIALS
Computer simulationsFrom the biokinetic data, the tumor:normal-tissue activity
concentration ratio, TNC, was obtained as
TNC5CT~t!
CN~t!
for various normal tissues, whereCT(t) and CN(t) are thedecay-corrected activity concentrations (% of administeredactivity per gram [%IA/g]) in the tumor,T, and normal,N,tissue, respectively, at time post administration. The cumu-lated tumor:normal-tissue activity concentration ratio,TNC,
was calculated for different radionuclides in Eq. 1:
TNC5
ECT~t! z e2ltdt
ECN~5! z e2ltdt
5CT
CN
(1)
wherel is the physical decay constant for the radionuclidestudied.
The tumor:normal-tissue mean absorbed dose rate ratio,TN D, was estimated both for mouse and man. The bodywas simulated by an ellipsoid representing normal tissue.Tumors were modeled as spheres and randomly distributedthroughout the ellipsoid. The distribution of radionuclidesin the spheres and in the ellipsoid was assumed to beuniform. The mean absorbed dose rate to the normal tissue,DN(t), for uniformly distributed activity in the ellipsoid wasas follows (Eq. 2):
DN~t! 5 CN~t!~Oi
Ee,ine,ifN,e,i 1 Oi
Ep,inp,ifN,p,i!
1 CT~t!mT
mNO
iEp,inp,i~fN,p,i 2 fT,p,i! (2)
whereEe,i andEp,i are the energies of the emitted electrons andphotons, respectively, per transitioni, ne,i and np,i are thenumbers of emitted electrons and photons, respectively, pertransition,fN,e,i andfN,p,i are the mean absorbed electron andphoton energy fractions, respectively, per transition,mN andmT are the mass of the normal and tumor tissue, respectively,andfT,p,i is the mean absorbed photon energy fraction in thetumor. In general, the deposition of the electron energy wasassumed to take place at the decay site; i.e., the fraction of theelectron energy absorbed in the normal tissue,fN,e,i, was 1.The mean absorbed fraction in the normal tissue from electronsoriginating from the tumor was neglected.
The mean absorbed dose rate to the tumor,DT(t), is then(Eq. 3):
DT~t! 5 @CT~t! 2 CN~t!#~Oi
Ee,ine,ifT,e,i 1 Oi
Ep,inp,ifT,p,i!
1 CN~t!~Oi
Ee,ine,i 1 Oi
Ep,inp,ifN,p,i! (3)
wherefT,e,i isthe mean absorbed electron energy fraction inthe tumor. For tumors#1 g, the absorbed fraction in thetumor from photons in the tumor was neglected.
The tumor:normal-tissue mean absorbed dose rate ratio,TN D, is as follows in Eq. 4:
TND 5
~TNC2 1!~Oi
Ee,ine,ifT,e,i 1 Oi
Ep,inp,ifT,p,i ! 1 Oi
Ee,ine,i 1 Oi
Ep,inp,ifN,p,i
Oi
Ee,ine,i 1 Oi
Ep,inp,ifN,p,i 1 TNCmT
mNO
iEp,inp,i~fN,p,i 2 fT,p,i!
(4)
515Radionuclides for tumor therapy● P. BERNHARDT et al.

Fig
.1.
The
calc
ulat
edcu
mul
ated
tum
or:n
orm
al-t
issu
eac
tivity
conc
entr
atio
nra
tio,T
NC
˜ ,vs
.the
phys
ical
half-
life
ofth
era
dion
uclid
efo
rth
efo
llow
ing:
(a–
c)i.v
.-in
ject
ed111 In
-DT
PA
-D-P
he1-
octr
eotid
ein
nude
mic
ebe
arin
gG
OT
1tu
mor
(23)
and
(d)
i.v.-
inje
cted
111 In
[DO
TA
,Tyr
3]o
ctre
otid
ein
patie
nts
with
neur
oend
ocrin
etu
mor
s(1
9).T
heha
lf-liv
esof
the
stud
ied
radi
onuc
lides
are
indi
cate
d.

The tumor:normal-tissue mean absorbed dose ratio, TND,was calculated for the whole body (Eq. 5):
Equation 5 is then valid for a homogeneous radionuclidedistribution in the whole body.
We calculated the TND for an organ, assuming that thephotons irradiating the organ and tumor originate from ahomogeneous radionuclide distribution in the whole body(Cw[t]), instead of a single tissue. TNDorganis asfollows (Eq. 6):
The mean absorbed photon and electron energy fractionsThe mean absorbed photon energy fractions,fN,p,i, for
a 70-kg (human) or 30-g (mouse) ellipsoid, with principalaxes forming the ratio 1:1.8:9.27, were taken from MIRDpamphlet No. 3 (25) and No. 8 (26), respectively. Thedecay properties of the radionuclides were taken from theWorld Wide Web table of radioactive isotopes (27). Themean absorbed electron energy fraction totumors,fT,e,i,
Table 1.Some physical properties of radionuclides proposed for therapy using radiolabeled somatostatin analogues
Radionuclide Half-life Decay mode Electron energy (keV) Abundance (%) p/e
64Cu 12.7 h b, EC, b1 190 37 1.5278 18
67Ga 3.26 days EC 0–1 169 4.57–10 61.3
84–92 3190Y 2.67 days b 935 100 1.8 1026
111In 2.83 days EC 0–4 293 1119–22 16
145–167 10219–242 6
131I 8.04 days b 191 89 246–97 14
250–360 2161Tb 6.91 days b 1.5–8.0 254 0.18
17–26 5140–49 54135 23154 67180 10
177Lu 6.7 days b 47–48 17 0.24102–113 18
149 79188Re 17 h b 728 25 0.07
795 72
p/e 5 photon: electron energy ratio.
TNDwhole bod y5
~TNC2 1!~Oi
Ee,ine,ifT,e,i 1 Oi
Ep,inp,ifT,p,i! 1 Oi
Ee,ine,i 1 Oi
Ep,inp,ifN,p,i
Oi
Ee,ine,i 1 Oi
Ep,inp,ifN,p,i 1 TNCmT
mNO
iEp,inp,i~fN,p,i 2 fT,p,i!
(5)
TNDorgan 5
~CT 2 CN!~Oi
Ee,ine,ifT,e,i 1 Oi
Ep,inp,ifT,e, j 1 Oi
Ep,inp,ifT,p,i! 1 CNOi
Ee, jne, j 1 CWOi
Ep,inp,ifN,p,i
CNOi
Ee,ine,i 1 CWOi
Ep,inp,ifN,p,i 1 CT
mT
mNO
iEp,inp,i~fN,p,i 2 fT,p,i!
(6)
517Radionuclides for tumor therapy● P. BERNHARDT et al.
518

was calculated using the method of Howellet al. (28),which uses the experimental determined energy rangerelationship by Cole (29). The calculation of the meanabsorbed fraction by the tumor,fT,e,i, was carried out fordifferent tumor sizes and electron energies. The tumorsizes ranged from one single cell with a mass of 1 ng (Rc
5 6.2 mm) to a tumor of 1 kg (Rc 5 6.2 cm). Allcalculations were made with a program written in IDL(Research Systems Inc., USA) and were carried out on aMacintosh Quadra 950 computer.
Biokinetic data of 111In-DTPA-D-Phe1-octreotide innude mice, transplanted with a well-differentiated carci-noid, GOT1 (cf. 22), were used in the calculation of TNC˜
and TND for the mouse (23). The111In activity concen-tration in various tissues (tumor, blood, thigh muscle,adrenals, omental fat, heart, small intestine, kidneys,liver, lungs, salivary glands, spleen, pancreas, and wholebody) was obtained at 0.5 h to 14 days after i.v. injectionof the radiopharmaceutical. For each tissue, bi- or three-exponential time activity curves,C(t), were fitted to the111In activity concentration for each tissue, corrected forphysical decay.
To estimate TNC˜ in man, the mean biokinetic data of111In-DOTA-D-Tyr3-octreotide from 18 patients were used(19). For each tissue, bi-exponential time activity curves,C(t), were fitted.
The TNDwhole bodywas calculated for both man and mice.For man, the mean whole-body activity concentration from13 patients injected with111In-DTPA-D-Phe1-octreotide(18) was used, together with biokinetic data on the tumortissue from the patient with midgut carcinoid tumor fromwhich the GOT1 cell line was derived (21).
The TNDbone marrowin man and mice was calculatedwith the assumption that the activity concentration inbone marrow was similar to that in blood. The bloodactivity concentrations from Krenninget al. (24) wereused for man. The small dimensions of the bone cavitiesin mice mean that only a small energy fraction of high-energy electrons will be absorbed in the red marrow.Therefore, for bone marrow in mice, we have also usedthe absorbed fractions 10% and 46% for the electronsfrom 90Y and 131I, respectively (30).
TND and TN D were calculated for the radionuclides131I, 111In, 90Y, 161Tb, 177Lu, 64Cu, 188Re, and67Ga. Thephysical properties of the radionuclides used in the calcu-lations are listed in Table 1.
RESULTS
TNC was calculated based on the biokinetics of111In-DTPA-D-Phe1-octreotide in nude mice carrying the humancarcinoid tumor GOT1 (Fig. 1a–c). TNC˜ increased withincreasing physical half-life of the radionuclide. Similarresults were obtained from the published human data on111In-DOTA-D-Phe1-octreotide (Fig. 1a–c) (cf. 19).
The relation between TN D˙whole body, TNDwhole body, and
tumor size are given in Fig. 2 for the radionuclides studied.TN Dwhole body is rather low for radionuclides emitting ahigh fraction of energy as photons, e.g. for111In and67Ga.The high-energy electron emitters90Y and 188Re give highTN Dwhole body for tumors larger than 1 g. However, forsmaller tumors TN D˙ whole bodyis reduced because of the lowabsorbed energy fractions.
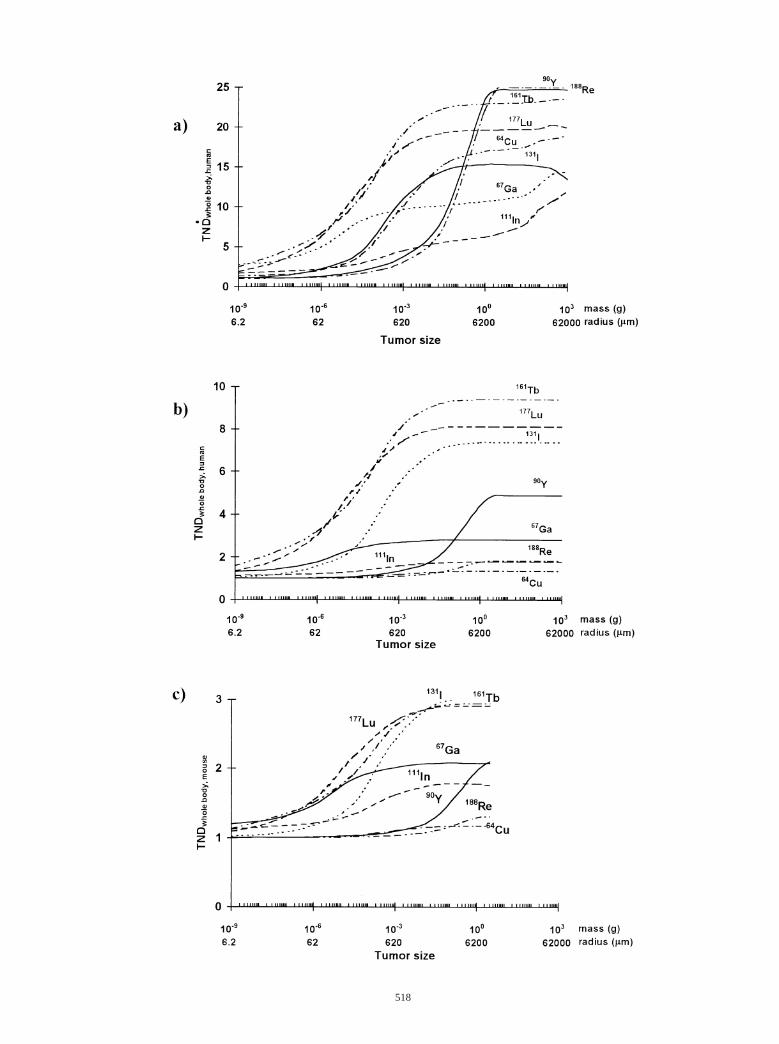
TNDwhole body was calculated for mice and man. Thelong-lived radionuclides161Tb and131I gave relatively highTNDwhole body, whereas the short-lived64Cu and188Re gavelow TNDwhole body. Both for man and mouse, TNDwhole body
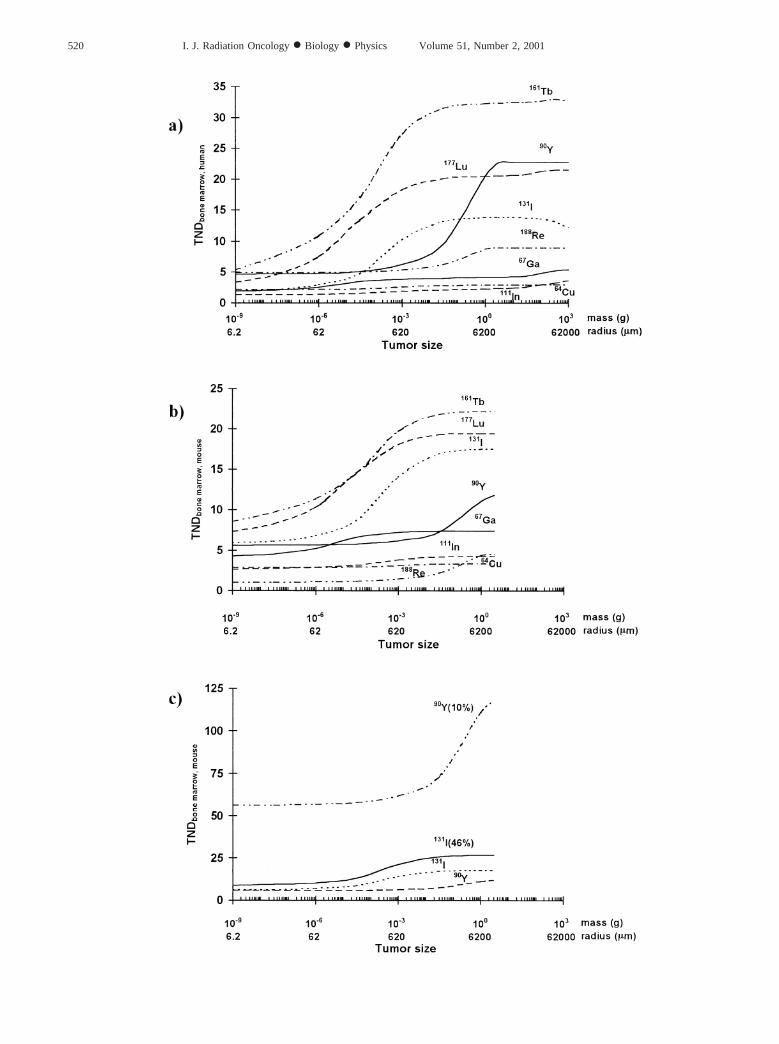
was lower for radionuclides emitting a high abundance ofphotons and higher for pure electron emitters. Figure 3shows the TNDbone marrowfor mice and man. In Fig. 3c isshown the calculation of TNDbone marrowin mice, given theassumption that only a fraction of emitted electrons will beabsorbed in bone marrow. TNDbone marrowfor 90Y and 131Iare increased if the fractions of electrons absorbed by thebone marrow are decreased.
DISCUSSION
For successful therapy with radiopharmaceuticals, theabsorbed dose in the tumor must be higher than in thenormal tissue. The tumor:normal-tissue activity concen-tration ratio, TNC, varies with time because of differentpharmacokinetics in the tissues and physical decay of theradionuclide. This is taken into account in the cumulatedtumor:normal-tissue activity concentration ratio, TNC˜ .TNC can accordingly be used to predict the therapeuticpotential of a radiopharmaceutical, if the radiation isassumed to be absorbed at the site of decay. Quite oftenthe radionuclides emit not only particles but also photons,which are not locally absorbed. The absorbed fraction ofthe emitted electrons depends on the electron energy andsize of the target. The tumor:normal-tissue absorbed doserate ratio, TN D, takes into account the electron energy,the abundance of emitted photons, and the tumor size.The tumor:normal-tissue absorbed dose ratio, TND, takes
Fig. 2. (a) Thetumor:normal-tissue mean absorbed dose rate ratio for the whole body, TN D˙wholebody, vs. tumor mass for various
radionuclides in the simulated human model. The TNC is set to 25. (b) The tumor:whole-body mean absorbed dose ratio,TNDwhole body, vs. tumor mass for various radionuclides in a simulated human model. The biokinetic data for tumor are fromAnderssonet al. (21) and for whole body are from Forssell-Aronssonet al. (18) for all studied radionuclides. (c) The tumor:whole-body mean absorbed dose ratio, TNDwhole body, vs. tumor mass for various radionuclides in a simulated mouse model. The biokineticdata for tumor are from Bernhardtet al. (23) for all studied radionuclides.
519Radionuclides for tumor therapy● P. BERNHARDT et al.
520 I. J. Radiation Oncology● Biology ● Physics Volume 51, Number 2, 2001

into account furthermore the pharmacokinetics and phys-ical half-life of the radionuclide. It is important to com-pare TND values when radionuclides suitable for therapyare to be chosen. However, the radiosensitivity and anydose rate effects are not included in the present models.
To analyze the physical properties of radionuclides fortherapy ofsstr-expressing tumors, the observed long-termbiodistribution of 111In-DTPA-D-Phe1-octreotide in thetransplantable well-differentiated human carcinoid tumorGOT1 in nude mice was used (23). There are several humanpharmacokinetic studies of111In-DTPA-D-Phe1-octreotide,but to our knowledge only one includes biokinetics fortumor tissue (cf. 21). We also used data observed for111In-DOTA-Tyr3-octreotide (19) and111In-DTPA-Phe1-octreotide in man (18).
TNC increased immediately after the injection of111In-DTPA-D-Phe1-octreotide for all studied organs inthe GOT1-bearing nude mice and remained elevated dur-ing the time of study (0.5 h to 14 days), except in thespleen, liver, and muscle, where TNC was maximal at 3to 7 days after injection (23). A similar pattern was seenfor TNC of the original GOT1 tumor in the patient (21).This increase in TNC with time indicates a favorabletherapeutic situation for long-lived radionuclides. To il-lustrate these conditions, TNC˜ vs. physical half-life wascalculated (Fig. 1). It was then assumed that the activityconcentration in the tumor was not affected by therapeu-tic effects during the course of the study. This seems tobe a reasonable assumption, because release of radioac-tivity during tumor regression may relate to a similardecrease in tumor mass. The present results clearly showthat it is favorable not to use radionuclides with shorterhalf-lives, because this will result in lower TNC˜ values(Fig. 1). With long-lived 161Tb and 131I, 2 to 4 timeshigher TNCvalues were obtained compared to the moreshort-lived64Cu and188Re. High TNCwas also seen for111In-DOTA-Tyr3-octreotide in man (Fig. 1d) (19). How-ever, in the latter study, the biodistribution was onlyfollowed for 48 h, a fact that limits its predictive valuefor a long-lived radionuclide.
The absorbed dose in a tumor depends on the radiationrange and the tumor size. Electrons and positrons haveranges from tenths of nm to several mm, depending ontheir energy. For uniform activity distribution in larger
tumors (.1 g), almost all energy of the emitted electronswill be deposited in the target. However, for small tumors(,1 g) a small energy fraction from the emitted electronsand positrons will be deposited within the tumor. Bycalculating the TND rate, i.e., having TNC fixed, it ispossible to compare the influence of photon abundanceand electron energy for the different radionuclides (Fig.2a). 90Y and 188Re emit electrons with high energy,which gives high TN D˙ for tumor masses larger than 1 gand will rapidly decrease with decreasing tumor mass.Radionuclides emitting lower electron energies are thusmore suitable for therapy of small tumors. Most radio-nuclides suggested forsstr-based radiotherapy also emitphotons to varying degrees. The photons will deposittheir energy in a nonlocalized way and will thus givereduced TN D˙ values. The low electron energy emitters111In and 67Ga also emit numerous photons, as reflectedby their low TN D levels.
The biokinetics of radiolabeled octreotide was consid-ered in the mathematical TND model. The short-livedradionuclides had markedly lower TND compared withthe long-lived radionuclides (Fig. 2b and 2c). The TND-
whole bodywas lower in mice than in man, which is partlyexplained by the high activity concentration in the kid-neys of mice (more than half of the activity content).Even if our results demonstrate that long-lived radionu-clides are preferred for therapy ofsstr-positive tumors, itis known that somatostatin analogues will have differentbiodistributions and affinities with different chelates andradionuclides (31). There might also be an interpatientvariability of the biokinetics that has to be studied fur-ther. Therefore, the benefit of using long-lived radionu-clides has to be further investigated by comparative stud-ies of different radiolabeled analogues. Furthermore, theuse of radionuclides that are too long lived will givelow-dose rates that might reduce the biologic efficiency(32).
TNDbone marrowwas calculated with the assumption thatthe activity concentration in bone marrow was similar tothat in blood. To our knowledge, no detailed study on thepharmacokinetics in bone marrow have been performed forradiolabeled somatostatin analogues. We have measured the111In activity concentration in human bone marrow in threesurgical samples from patients injected with111In-DTPA-
Fig. 3. (a) Thetumor:bone-marrow mean absorbed dose ratio, TNDbone marrow, human, vs. tumor mass for various radionuclides in asimulated human model. The biokinetic data for tumor are from Anderssonet al. (21), for whole body are from Forssell-Aronssonet al. (18), and for blood are from Krenninget al. (24) for all studied radionuclides. (b) The tumor:bone-marrow mean absorbed doseratio, TNDbone marrow, mouse, vs. tumor mass for various radionuclides in a simulated mouse model. The biokinetic data for tumor arefrom Bernhardtet al. (23) for all studied radionuclides. (c) The tumor:bone-marrow mean absorbed dose ratio, TNDbone marrow, mouse,vs. tumor mass for various radionuclides in a simulated mouse model. The biokinetic data for the tumor are from Bernhardtet al. (23)for the studied90Y and131I. The emitted electrons in bone marrow are assumed to be totally absorbed90Y and131I, or only a fractionof the emitted electron energies were assumed to be absorbed. For90Y, this fraction was 10% (90Y[10%]), and for131I this fractionwas 46% (131I[46%]) according to Muthuswamyet al. (30). In all figures, the bone marrow activity concentration was assumed tobe the same as in the blood.
521Radionuclides for tumor therapy● P. BERNHARDT et al.

D-Phe1-octreotide and obtained bone marrow:blood ratiosof 1.6–2.7 (33). Therefore, our TNDbone marrowvalues mightbe somewhat overestimated for111In. TNDbone marrowmustalso be investigated for each radionuclide and labelingmethod. Given our assumption about similar pharmacoki-netics, it was shown that the radionuclides emitting a highabundance of photons gave lower TNDbone marrowin thehuman model than in the mouse model because of a higherabsorbed fraction of photons in the normal tissue. Further-more, TNDbone marrowwas higher for pure electron emittersin man than in mice because of higher TNC (Fig. 3a and3b). However, the emitted high-energy electrons will not betotally absorbed into the small red bone cavities in mice, incontrast to the bone cavities of man. In mice, Muthuswamyet al.(30) have calculated that the mean absorbed fraction ofthe emitted electrons in bone marrow from90Y and131I was10% and 46%, respectively. This fact will increase thecalculated TNDbone marrowconsiderably, especially for high-energy electron emitters such as90Y (Fig. 3c). Therefore,the bone marrow in mice will probably not be such a criticalorgan for high-energy electron emitters, whereas in man it is(15).
The results indicate that radionuclides for therapy ofsmall disseminated tumors should emit few photons, havea rather long half-life (T1/2 . 2 days), and emit moderateelectron energy. Of the radionuclides proposed forsstr-based radiotherapy, it seems that111In and67Ga emit toomany photons to be optimal. However, both these radio-nuclides emit Auger electrons, which may enhance theradiobiologic effect if the radionuclides are depositedclose to the nucleus of tumor cells (cf. 34). In our studyon tumor cell cultures incubated with111In-DTPA-D-Phe1-octreotide and studied by electron microscopic au-toradiography,111In was mainly located in the cytoplasmand also, to some extent, in the nucleus (35). If Augerelectrons are to be of therapeutic use, an Auger electronemitter with low amounts of photons and rather lowenergies of the conversion electrons would be preferred(23). The very high TNC values obtained in patients withadvanced neuroendocrine tumors may explain the posi-tive effects (reduced hormonal symptoms and stabiliza-tion of tumor growth) observed after111In-DTPA-D-Phe1-octreotide therapies (2, 11–13). No complete tumorremission has been reported in man. The toxicity relatedto treatment included various grades of anemia and my-elosuppression. The toxicity on red blood marrow cellsmight be reduced by using radionuclides emitting lowabundance of photons.
The positron emitter64Cu will give relatively low TNDvalues because of its short half-life. Studies on64Cu, boundto the somatostatin analogues TETA-OC and TETA-Y3-TATE, have been done (5). If64Cu-TETA-Y3-TATE wereused for therapy, it would be limited by low TNC valuesimmediately after injection. Another short-lived radionu-clide proposed for radionuclide therapy is188Re. Intratu-
moral injection of188Re-RC-160 into xenografted humanprostate tumors (6) obtained demonstrable therapeutic re-sponses. For systemic therapy, the short half-life will, how-ever, limit the possibility of reaching high TND values.Furthermore, it will be difficult to treat small, disseminatedtumors with this agent, because of the high energy of itselectrons.
Use of90Y-DOTA-D-Phe1-[Tyr3]-octreotide (14) achievedcomplete remission of transplants of the rat pancreatic tumorCA 20948 in rats, without side effects. Also in clinical trials,marked regression of neuroendocrine tumors have been ob-served (15). Side effects, i.e., renal toxicity, anemia, andthrombocytopenia, were observed. Therapy ofsstr-expressingtumors by high-energy electron emitters bound to somatostatinanalogues such as90Y-DOTA-D-Phe1-[Tyr3]-octreotide mustbe further studied. It will, however, be difficult to treat small,disseminated tumors with this agent because of the high energyof its electrons.
The b-emitter 131I has recently been bound to thesomatostatin analogue Woc-3a and administered i.v. intherapeutic amounts (59 GBq) to a patient (1). The ther-apeutic amount administered was based on pharmacoki-netics obtained from diagnostic scintigraphy (59 MBq131I-Woc-3a up to 48 h p.i.). However, the activity stayedlonger in the body than the authors had calculated, andthe patient died from a myocardial infarction 5 days afteradministration of the radiopharmaceutical. Biopsy dem-onstrated coagulation necrosis of both brain and lungtumors. No evidence of radiation damage to the normaltissues could be confirmed. Further trials with131I-Woc3ahave been stopped.
De Jonget al. (4) performed distribution studies in ratsafter administration of161Tb-DTPA-D-Phe1-octreotide withpromising results, but no further studies have since beenpublished with this radionuclide. Very recently, markedtumor reduction has been obtained in animal studies with[177Lu-DOTA, Tyr3]octreotate (36). In our calculations,161Tb and177Lu showed the highest TND values. Therefore,we propose that these radionuclides should be further in-vestigated for therapy using radiolabeled somatostatin ana-logues in the future.
The human carcinoid tumor GOT1 xenografted to nudemice is a novel model for the study of radionuclide therapyof sstr-positive tumors. Comparison of TNC˜ and TND val-ues from our animal and human studies revealed similarresults, indicating that the optimal radionuclides shouldemit few photons and have relatively long half-lives. It wasalso evident that radionuclides emitting high-energy elec-trons were not suitable for treatment of small tumors, be-cause of the low absorbed energy fraction in small tumors.However, the differences between mice and humans inregard to TND values of kidneys and bone marrow must beconsidered when planning and evaluating radionuclide ther-apy studies in mice.
522 I. J. Radiation Oncology● Biology ● Physics Volume 51, Number 2, 2001

REFERENCES
1. Espenan GD, Nelson JA, Fisher DR,et al. Experience withhigh dose radiopeptide therapy: The health physics perspec-tive. Health Phys1999;76(3):225–235.
2. Krenning EP, Bakker WH, Kooij PPM,et al. Radiotherapywith a radiolabeled somatostatin analogue [111In-DTPA-Phe1] octreotide. In: Wiedenmann B, Kvols LK, Arnold R,Rieken EO, editors. Molecular and cell biological aspectsof gastroenteropancreatic neuroendocrine tumor disease.Ann N Y Acad Sci1994;733:496 –506.
3. Otte A, Jermann E, Behe M,et al. DOTATOC: A powerfulnew tool for receptor-mediated radionuclide therapy.EurJ Nucl Med1997;24:792–795.
4. de Jong M, Breeman WAP, Bernad BF,et al. Evaluation invitro and in rats of Tb-DTPA-octreotide, a somatostatinanalogue with potential for intraoperative scanning andradiotherapy.Eur J Nucl Med1995;22:608 – 616.
5. Lewis JS, Srinivasa A, Schmidt MA, Anderson CJ. In vitroand in vivo evaluation of Cu-TETA-Tyr-Octreotate. A newsomatostatin analogue with improved target tissue uptake.Nucl Med Biol1999;26:267–273.
6. Zamora PO, Gulhke S, Bender H,et al. Experimentalradiotherapy of receptor-positive human prostate adenocar-cinoma with Re-RC-160, a directly-radiolabeled somatosta-tin analogue.Int J Cancer1996;65:214 –220.
7. LaznıckovaA, Laznıcek M, Tretjnar F, Ma¨cke HR. Studiesin rats on octreotide labelled with Ga-67 –a potential ra-diopharmaceutical for the treatment of receptor-positivetumors (IAEA-SR-209/20). In: International Seminar onTherapeutic Applications of Radiopharmaceuticals. Pro-ceedings of a symposium (Hyderbad, 1999). InternationalAtomic Energy Comission, Vienna, 1999.
8. Lamberts S, Bakker W, Reubi J-C,et al. Somatostatinimaging in the localization of endocrine tumours.N EnglJ Med 1990;323:1246 –1253.
9. Breeman WAP, Hofland LJ, Bakker WH,et al. Radioiodi-nated somatostatin analogue RC-160: Preparation, biolog-ical activity, in vivo application in rats and comparisonwith 123I-Tyr3-octreotide.Eur J Nucl Med1993;20:1089 –1094.
10. Buxton-Thomas M, Ramage JK, Williams R. Comparisonof indium-111-labelled octreotide and I-123-metaiodo-benzylguanidine imaging in patient with secondary carci-noid tumours of the liver.Eur J Nucl Med1994;21(Suppl):200.
11. Fjalling M, Andersson P, Forssell-Aronsson E,et al. Sys-temic radionuclide therapy using Indium-111-DTPA-D-Phe1-octreotide in midgut carcinoid syndrome.J Nucl Med1996;37(9):1519 –1521.
12. McCarthy KE, Woltering EA, Espenan GD, Cronin M,Maloney TJ, Anthony LB. In situ radiotherapy with In-pentetreotide: Initial observations and future directions.Cancer J Sci Am1998;4:94 –102.
13. Krenning EP, de Jong M, Kooij PP,et al. Radiolabelledsomatostatin analogue(s) for peptide receptor scintigraphyand radionuclide therapy.Ann Oncol 1999;10(Suppl. 2):S23–29.
14. Stoltz B, Weckbecker G, Smith-Jones PM, Albert R, RaulfF, Bruns C. The somatostatin-targeted radiotherapeutic[90Y-DOTA-D-Phe1, Tyr3]octreotide (Y-SMT 487) eradi-cates experimental rat pancreatic CA 20948 tumours.EurJ Nucl Med1998;25:668 – 674.
15. Otte A, Hermann R, Heppeler A,et al. Yttrium-DOTA-TOC: First clinical results.Eur J Nucl Med1999;26:1439 –1447.
16. Leimer M, Kurtaran A, Smith-Jones P,et al. Response totreatment with Yttrium 90-DOTA-Lanreotide of a patient
with metastatic gastrinoma.J Nucl Med 1998;39:2090 –2094.
17. Wiseman GA, Kvols LK. Therapy of neuroendocrine tu-mors with radiolabeled MIBG and somatostatin analogues.Semin Nucl Med1995;25(3):272–278.
18. Forssell-Aronsson E, Lanhede B, Fja¨lling M, et al. Phar-macokinetics and dosimetry of111In-DTPA-D-Phe1-oct-reotide in patients with neuroendocrine tumors. In SixthInternational Radiopharmaceutical Dosimetry Symposium,Proceedings of a Conference held at Gatlinburg, Tennessee,May 7–10, 1996 (Edited by A Schlafke-Stelson and EEWatson).1999.
19. Cremonesi M, Ferrari M, Zoboli S,et al. Biokinetics anddosimetry in patients administrated with111In-DOTA-Tyr3-octreotide: Implication for internal radiotherapy with90Y-DOTATOC. Eur J Nucl Med1999;26:877– 886.
20. Virgolini I, Szilvasi I, Kurtaran A, et al. Indium-111-DOTA-Lanreotide: Biodistribution, Safety and radiationabsorbed dose in tumor patients.J Nucl Med 1998;39:1928 –1936.
21. Andersson P, Forssell-Aronsson E, Gre´tarsdottir J, et al.Biokinetics and dosimetry after repeated injections of111In-DTPA-D-Phe1-octreotide. In: Schlafke-Stelson A,Watson, EE, editors. Proceedings of the Sixth InternationalRadiopharmaceutical Dosimetry Symposium. Gatlinburg,TN: May 7–10, 1996 . 1999.
22. Kolby L, Ahlman H, Wangberg B,et al. A transplantedhuman midgut carcinoid as a model for somatostatin recep-tor- and amine transporter mediated radionuclide uptake.Submitted.
23. Bernhardt P, Ko¨ lby L, Johansson V,et al. Biokinetics ofIn-DTPA-D-Phe-octreotide in nude mice transplanted witha human carcinoid tumor. Submitted.
24. Krenning EP, Bakker WH, Kooij PPM,et al. Somatostatinreceptor scintigraphy with Indium-111-DTPA-D-Phe-1-oc-treotide in man: Metabolism, dosimetry and comparisonwith iodine-123-Tyr-3-octreotide.J Nucl Med 1992;33:652– 658.
25. Brownell GL, Ellett WH, Reddy AR. Absorbed fractionsfor photon dosimetry. MIRD pamphlet No. 3.J Nucl Med1968;1(Suppl. 1):27–39.
26. Ellett WH, Humes RM. Absorbed fractions for small vol-umes containing photon-emitting radioactivity. MIRDPamphlet No.8.J Nucl Med1971;12(Suppl. 5):25–32.
27. Chu SYF, Ekstro¨m LP, Firestone RB. The Lund/LBNLNuclear Data Search: version 2.0, February 1999. http://nucleardata.nuclear.lu.se/nucleardata/toi/index.asp
28. Howell RW, Rao DV, Haydock C. Dosimetry techniquesfor therapeutic applications of incorporated radionuclides.In The joint symposium on dosimetry of administered ra-dionuclides, Proceedings held at Washington D.C, Septem-ber 1989:215–256.
29. Cole A. Absorption of 20 eV to 50000 eV electron beamsin air and plastic.Radiat Res1969;38:7–33.
30. Muthuswamy MS, Roberson PL, Buchsbaum DJ. A mousebone marrow dosimetry model.J Nucl Med1998;39:1243–1247.
31. Reubi JC, Scha¨r J-C, Waser B,et al. Affinity profilesfor human somatostatin receptor subtypes SST1-SST5of somatostatin radiotracers selected for scintigraphicand radiotherapeutic use.Eur J Nucl Med200;27:273–282.
32. O’Donoghue JA, Bardies M, Wheldon TE. Relationshipsbetween tumor size and curability for uniformly targetedtherapy with beta-emitting radionuclides.J Nucl Med1995;36:1902–1909.
33. Forssell-Aronsson E, Fja¨lling M, Nilsson O, Tisell LE,
523Radionuclides for tumor therapy● P. BERNHARDT et al.

Wangberg B, Ahlman H.111In activity concentration inhuman tissue samples after i.v. injection of111In-DTPA-Phe1-octreotide.J Nucl Med1995;36:7–12.
34. Sastry KS. Biological effects of the Auger emitter iodine-125: A review. Report No. 1 of AAPM Nuclear MedicineTask Group No. 6.Med Phys1992;19(6):1361–1370.
35. Andersson P, Forssell-Aronsson E, Johanson V,et al. In-
ternalization of 111In into human neuroendocrine tumorcells after incubation with111In-DTPA-D-Phe1-octreotide.J Nucl Med1996;37:2002–2006.
36. de Jong M, Breeman WAP, Bernad BF,et al.[DOTA,Tyr3]octreotate, labeled with177Lu, is most prom-ising for radionuclide therapy of somatostatin receptor-positive tumours.Nucl Med Commun2000;21(6):569.
524 I. J. Radiation Oncology● Biology ● Physics Volume 51, Number 2, 2001