Embed Size (px)
Citation preview
1
Dorset HealthCare University NHS Foundation Trust
Part 1 Board Meeting
A meeting of the Board will be held on 30 September 2015 at Sentinel House, 4-6
Nuffield Road, Poole, Dorset, BH17 0RB commencing at 1:00pm
If you are unable to attend please notify Keith Eales on 01202 277008.
Yours Sincerely,
Ann Abraham
Chair
Initials Paper Time 1. Welcome, Apologies and Previous
Meetings 1:00
1.1 Apologies AA 1.2 Patient Story - Hidden Talents Film FH Film
1.3 Quorum
To confirm that the meeting is quorate.
AA
Verbal
1.4 Declarations of interests in relation to
agenda items AA Verbal
1.5 Minutes
To approve the Minutes of the meeting held on 29 July 2015
AA App A 1:15
1.6 Matters Arising
To consider progress.
AA App B
1.7
Chair’s Report To receive the update of the Chair
AA
App C
1:20

2
2. Strategy Implementation: Current Affairs and Operational Performance
2.1 Acting Chief Executive’s Report
To consider a report from the Acting Chief Executive
FH App D 1:35
2.2
Integrated Corporate Dashboard for August 2015 To consider the monthly dashboard
NK App E
1:45
2.3 Finance Report
To consider the report for August
JC App F 2:00
2.4 People Management
To consider the monthly update
CLH App G 2:20
2.5 Minutes of the Audit Committee 20th May
2015 To consider the minutes of the meeting
JMcB App H 2:30
3. Strategy Development:
Policy Formulation and Decision Making
3.1 Stages of Excellence
To approve a framework for assessing the achievement of the strategic goals set out in the Trust strategy 2015 to 2020
SH App I 2:35
4. Regulatory and Compliance Matters
4.1 Six Monthly Review of Inpatient Nurse
Staffing Establishment: Ensuring Safe Staffing To consider the findings of the six month review
FH App J
2:55
4.2 Occupational Health, Safety and Wellbeing
Annual Report 2014/15 To consider the Annual Report
CLH
App K 3:10

3
4.3 Trust Meeting Calendar 2016 To approve the meeting programme for 2016
KE App L 3:20
4.4 Reappointment of Mental Health Act Panel
Members To reappoint Panel members
SM App M 3:25
4.5
Board Annual Cycle of Business To agree the annual cycle of business
KE App N 3:30
5. Other Matters
5.1 Any Other Business AA Verbal 3:35
5.2 Questions from Governors AA Verbal 3:45 6. Date and Time of Next Meeting
The next Meeting will be held on Wednesday 28 October 2015 at Sentinel House (Training Rooms 1&2) 4-6 Nuffield Road, Poole, Dorset, BH17 0RB commencing at 1:00pm
7. Exclusion of the Public
To resolve that representatives of the Press and other members of the public, be excluded from the remainder of this meeting having regard to the confidential nature of the business to be transacted, publicity of which would be prejudicial to the public interest.

1
Part 1 Matters Arising
Board Meeting 30 September 2015
Matters Arising from Trust Board Meeting 29 July 2015
Minute Topic Action Lead Deadline Response
390/15 Finance Report-areas for investment
It was agreed that
Further information on the areas of investment in 2015/16 would be submitted to the next meeting
Future reports would separate medical and nursing agency expenditure.
JC Sept 2015
Completed
398/15 Board Assurance Framework
The Chair of the Audit Committee, Director of Finance and Trust Secretary would liaise to recommend updated risk descriptions and control measures in respect of the financial challenge strategic risk.
KE October 2015
The BAF risk is under review by the Executive Performance and Corporate Risk Group. The meeting agreed at the last Board will be held prior to the revised BAF being submitted to the October Audit Committee and Board.
399/15 Standing Financial Instructions
It was agreed that SFI’s would be submitted to the next meeting of the Audit Committee and then to the Board for approval.
JC October 2015
Report scheduled for the Audit Committee on 20 October
Keith Eales, September 2015

Chair’s Report
Part 1 Board Meeting 30 September 2015
Author Ann Abraham, Chair
Sponsoring Board Member
Ann Abraham, Chair
Purpose of Report To report on discussions at the recent meeting of the Council of Governors.
Recommendation The Board is asked to note the report
Engagement and Involvement
-
Previous Board/Committee Dates
Council of Governors September 2015
Monitoring and Assurance Summary
This report links to the Strategic Goals
To provide high quality care; first time, every time; To be a valued partner and expert in partnership working
with Patients, Communities and organisations; To be a learning organisation, maximising our partnership
with Bournemouth University and promoting innovation, research and evidence based practice;
To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare;
To be a national leader in the delivery of integrated care; To ensure that all of the Trust’s resources are used in an
efficient and sustainable way; To raise awareness within the Trust and externally of the
impact that our work has on people and our environment, and take steps to reduce any negative effects.
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability
Information Management &Technology
Equality Impact Assessment
Freedom of Information
2
1. Introduction 1.1 The Council of Governors held a relatively short meeting prior to the AMM on 16
September. However, there were two important matters discussed which are relevant to the work of the Board. This note provides a short briefing on these two matters, as part of my overall Chair’s Report for the month.
2. Membership of the Council 2.1 The outcome of a review of the Partner and Local Government Governor positions has
been approved the Council. 2.2 Whilst there have been two Local Government Governors on the Council since 2014, it has
been the perception for some time that individual representation for Bournemouth and Poole Councils is appropriate.
2.3 The current composition of the Council allows an additional Local Government Governor
position to be created without requiring an increase in the number of Public Governors.
2.4 In addition, discussions have been held with the Chair of Dorset CCG about its Governor position. The Chair of the CCG agreed that, given the potential conflict of interests and the time demands on their representatives, the CCG was willing to give up its Partner Governor position.
2.5 The Council has agreed to increase by one the number of Governors and also to the
reallocation of a Partner Governor position from the CCG. These changes allow individual Governor positions to be allocated to Bournemouth and Poole Borough Councils.
2.6 On this basis, the composition of the Council is now
14 Public Governors
Five Staff Governors
Four Local Government Governors, representing Bournemouth Borough Council; Poole Borough Council; Dorset County Council; the remaining Dorset District Councils
Four Partnership Governors, representing Bournemouth University; Dorset Police, Probation and Prison Services; Service User Group Representative; Third Sector Organisations
2.7 The Council has agreed the necessary changes required to the Constitution.
3. Annual Self-Assessment of the Council
3.1 Governors have considered a report on the outcome of the annual self-assessment of the
Council.
3.2 The self-assessment, which was facilitated by The Folio Partnership, was undertaken over the summer of 2015.
3.3 The key conclusions from the self-assessment were that
3
Considerable progress had been made in establishing clarity in respect of the role of the Council, mechanisms for fulfilling that role and positive and productive relationships with the Board
There was considered to be considerable scope to strengthen the link between Governors and the membership
An early priority should be to recruit Governors to the vacant positions on the Council
Mechanisms for holding Non-Executive Directors to account for the performance of the Board should be strengthened
3.4 An initial action plan has been agreed. This will be developed into an overall action plan, for
review at the November awayday of the Council, drawing on the self-assessment report, the external governance review and the CQC inspection report.
3.5 The Council emphasised the importance of seeking the views of the Board on the report and the relationship with the Council. It is suggested that the October Council meeting provides an opportunity for dialogue between the Board and Council
4. Recommendation 4.1 The Board is asked to
(a) note the report
(b) endorse the revised allocation of Governor positions and the changes required to the
Constitution
(c) note the outcome of the self-assessment of the Council and the proposal for further discussion between Governors and Board Directors at the October Council meeting.
Ann Abraham Chair September 2015

Acting Chief Executive’s Report
Part 1 Board Meeting 30 September 2015
Author Eugine Yafele/Fiona Haughey
Sponsoring Board Member
Eugine Yafele/Fiona Haughey
Purpose of Report To give an overview of the current priorities and key work areas of the Chief Executive and other significant issues in the Trust.
Recommendation The Board is asked to note the report
Engagement and Involvement
-
Previous Board/Committee Dates
-
Monitoring and Assurance Summary
This report links to the Strategic Goals
To provide high quality care; first time, every time; To be a valued partner and expert in partnership working
with Patients, Communities and organisations; To be a learning organisation, maximising our partnership
with Bournemouth University and promoting innovation, research and evidence based practice;
To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare;
To be a national leader in the delivery of integrated care; To ensure that all of the Trust’s resources are used in an
efficient and sustainable way; To raise awareness within the Trust and externally of the
impact that our work has on people and our environment, and take steps to reduce any negative effects.
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability
Information Management &Technology
Equality Impact Assessment
Freedom of Information

2
1. Introduction 1.1 My monthly report to the Board highlights
Significant priorities or other matters that the Board should be aware of which are not covered elsewhere on the agenda
External developments to bring to the attention of the Board
Consultations or other documents that will form future reports to the Board.
2. Current Priorities 2.1 There are a number of matters that I would like to update the Board on this month:-
Care Quality Commission (CQC) Inspection Reports
2.2 The draft CQC inspection reports were received on 16 September. These remain
confidential until published by the CQC after the Quality Summit.
2.3 The Trust has 10 days to respond to any factual inaccuracies in the report. At the time of writing, the review process is underway. Further details will be provided in the confidential part of the meeting.
2.4 The Quality Summit, which will be chaired by Monitor, will take place on 9 October. A
number of Board Directors will be at the meeting. Further details about the arrangements for the Summit are awaited. There will be an opportunity for a more detailed briefing on the arrangements at the Board Workshop on 7 October.
External Governance Review
2.5 The draft report, following the review by PM Governance, was received on 17 September.
2.6 The report is currently being reviewed by the Chair and Trust Secretary to identify areas
requiring clarification.
2.7 PM Governance will attend the Board Workshop on 7 October to present the report. The report and action plan will be submitted to the Board meeting in October, following which Monitor will be notified of the key recommendations and action proposed.
Clinical Leadership in the Trust 2.8 Over recent months the Chief Executive, in conjunction with the Executive and clinicians,
has been developing a clinical leadership model for the Trust.
2.9 Following extensive consultation and discussion a proposal has been developed and is currently being reviewed by the Executive and clinical leaders prior to implementation. The proposal, once agreed, will be distributed to Board members.
Weymouth and Portland Community Urgent Care Centre
2.10 Dorset Clinical Commissioning Group (CCG) issued a tender on 4 September 2015 for the provision of a 7-day, 08:00-23:00 minor injuries and ailments service based at Weymouth Community Hospital.

3
2.11 The service replaces a Minor Injuries Service provided by the Trust and a Walk-In Centre for minor ailments provided by The Practice.
2.12 The Trust is responding to the tender as lead provider, working with the local GP
Federation, Two Harbours Healthcare, and Dorset County Hospital NHS Foundation Trust as partners and subcontractors. The Southwest Ambulance Service NHS Foundation Trust has also been closely involved in ensuring appropriate interface/integration with its services.
2.13 The deadline for the return of the tender bid is 16 October 2015. 3. Recommendation 3.1 The Board is asked to note the report.
Eugine Yafele/Fiona Haughey Acting Chief Executive September 2015
Trust Board Integrated Corporate Dashboard August 2015
Part 1 Board Meeting 30th September 2015
Author Fiona Haughey, Director of Nursing and Quality; Jackie Chai, Director of Finance; and Colin Hague, Director of Human Resources
Sponsoring Board Member
Dr Nick Kosky, Medical Director / Fiona Haughey, Director of Nursing and Quality
Purpose of Report To provide the Board with insight and foresight of Trust performance and support effective decision making, highlighting areas of exception and good practice. The Trust performance reported here is underpinned by ward/team level information and aims to provide Board line of sight to performance within wards and teams. This integrated corporate report brings together the Trust’s performance on quality, workforce and finance against the Trust’s plans and targets.
Recommendation The Board is asked to note the report and actions planned.
Engagement and Involvement
All directors, localities – performance business partners, finance, human resources and quality teams. There has been wide-scale engagement with the new quality metrics with clinical staff from across the organisation.
Previous Board/Committee Dates Executive Performance and Corporate Risk Group
Monitoring and Assurance Summary
This report links to the Strategic Goals
To provide high quality care; first time, every time; To be a valued partner and expert in partnership working with
Patients, Communities and organisations; To be a learning organisation, maximising our partnership with
Bournemouth University and promoting innovation, research and evidence based practice;
To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare;
To be a national leader in the delivery of integrated care; To ensure that all of the Trust’s resources are used in an efficient and
sustainable way; To raise awareness within the Trust and externally of the impact that
our work has on people and our environment, and take steps to reduce any negative effects.
Board of Directors September 2015
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated: Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality Board Assurance Framework Risk Register Legal / Regulatory People / Staff Financial / Value for Money / Sustainability Information Management & Technology Equality Impact Assessment Freedom of Information

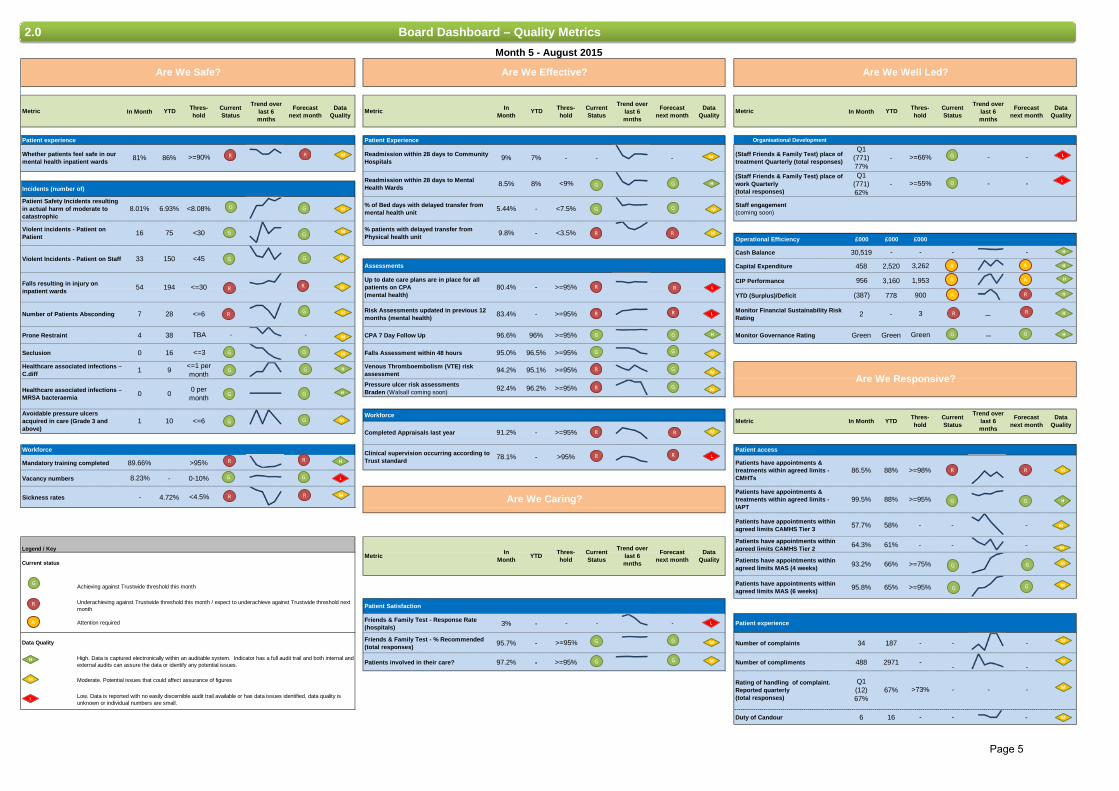
Trust Board Integrated Corporate Dashboard
Month 5 – August 2015
Contents1.0 Executive Summary & Performance Synopsis Pages 2-4
7.0 Indicator Overviews
2.0 Board Dashboard – Quality Metrics
2.1 Exception Reports - Are we Safe?
2.2 Exception Reports - Are we Effective?
2.4 Exception Reports - Are we Well Led?
2.5 Exception Reports - Are we Responsive?
4.0 Areas of good practice
3.0 Areas of concern or risk
Page 5
Pages 6-10
Pages 11-17
Page 18
Page 19
5.0 National Reporting Frameworks
5.1 Board Dashboard – Monitor Indicators
7.1 Indicator Overview – Quality Metrics
5.2 CQUINS (Quarterly)
5.3 External Benchmarking (as appropriate)
5.4 Nationally reportable concerns (CQC)
Pages 26-27
Pages 21-25
Pages 28-29
N/A
N/A
N/A
7.2 Indicator Overview – Monitor RAF
Pages 33-34
Page 35
2.3 Exception Reports - Are we Caring? N/A
5.5 Research and Development Metrics (Quarterly) N/A
5.6 Mental Health Act Metrics (Quarterly) N/A
6.0 Quality Priorities Page 31-32
5.7 Inpatient Nursing Staffing Page 30
2.6 Additional Report Page 20
Page 2

Are we Safe?
• The percentage of mental health inpatients stating they felt safe has fallen, althoughthe number of surveys completed has risen
• Falls continue to show an upward trend. The Trust’s falls lead is working with wardsto minimise the number of falls
• Absconding numbers for August have risen to above the threshold• Mandatory training has plateaued below the threshold• Sickness rates are still below the threshold
• The Trust continues to shows improvement around patients restraint and seclusion
• The Director of Human Resources has agreed the target for vacancy rates which isincluded for the first time this month and performance is in the green threshold
Are we Effective?
• Delayed transfers of care for physical health units have risen compared to lastmonth
• We continue to fall below the performance threshold for patients with up to date careplans
• Risk assessment data has remained almost static compared to the last two monthsand remains below the performance threshold
• Two clinical risk assessments (venous thromboembolism (VTE) and Braden riskassessments for pressure ulcers) fell below performance this month
• Workforce effectiveness thresholds for completed appraisals and clinical supervisionare still not being achieved
• A good practice example of Tarrant Ward’s accreditation for end of life care isincluded in the report
Are we Caring?
• Year to date, the percentage of patients who would recommend us to their friendsand family has been good
• The number of respondents is far lower than we would wish
• A good practice example of the work engaging with staff in mental health inpatientareas to increase the uptake of surveys and learning from patient experience isincluded in the report
Are we Well Led?
• The capital expenditure is behind the expected spend forecast for the end of August• The financial performance, including CIP, is still showing as a concern, although in
month there was a surplus against the budget• The main areas showing adverse performance are against recruitment, agency
spend, sickness and out of area placements• There is a concern about medical staffing pay budget overspend• The above issues have impacted negatively on the new Monitor rating for Financial
Sustainability, which has replaced the previous Continuity of Services rating. Furtherdetail is available in the separate Finance Report
1.0 Executive Exception Summary
Page 3
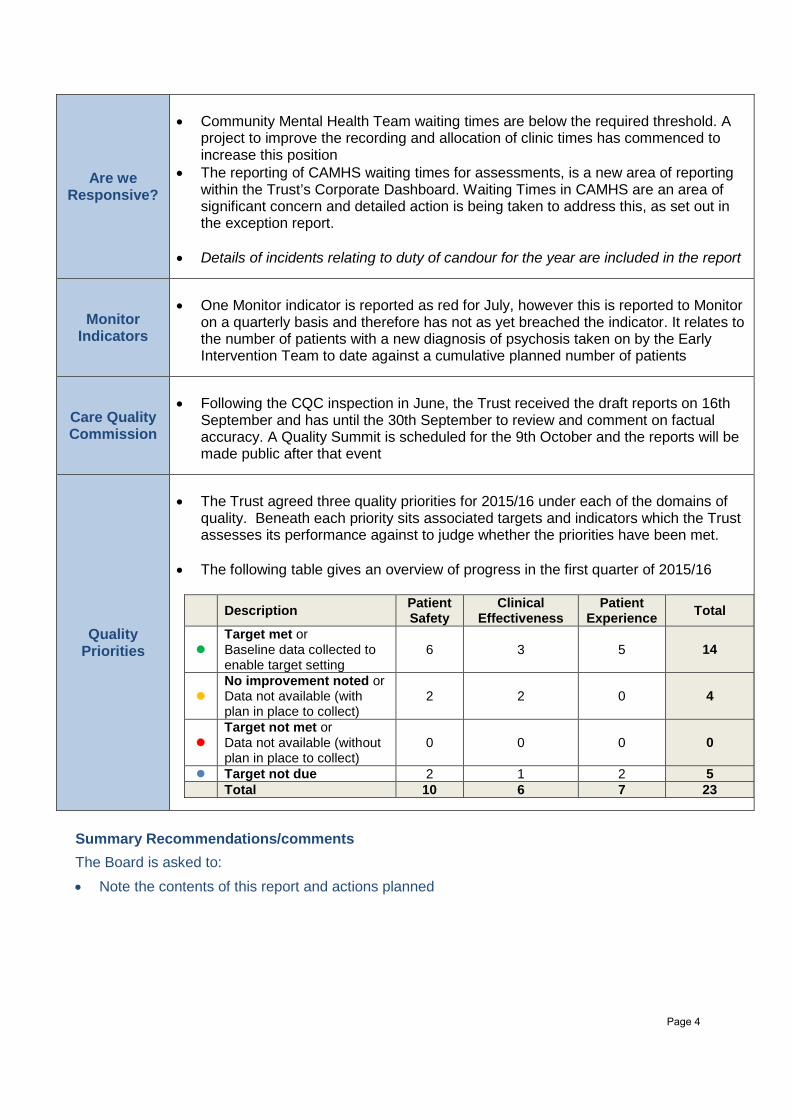
Are we Responsive?
• Community Mental Health Team waiting times are below the required threshold. Aproject to improve the recording and allocation of clinic times has commenced toincrease this position
• The reporting of CAMHS waiting times for assessments, is a new area of reportingwithin the Trust’s Corporate Dashboard. Waiting Times in CAMHS are an area ofsignificant concern and detailed action is being taken to address this, as set out inthe exception report.
• Details of incidents relating to duty of candour for the year are included in the report
Monitor Indicators
• One Monitor indicator is reported as red for July, however this is reported to Monitoron a quarterly basis and therefore has not as yet breached the indicator. It relates tothe number of patients with a new diagnosis of psychosis taken on by the EarlyIntervention Team to date against a cumulative planned number of patients
Care Quality Commission
• Following the CQC inspection in June, the Trust received the draft reports on 16thSeptember and has until the 30th September to review and comment on factualaccuracy. A Quality Summit is scheduled for the 9th October and the reports will bemade public after that event
Quality Priorities
• The Trust agreed three quality priorities for 2015/16 under each of the domains ofquality. Beneath each priority sits associated targets and indicators which the Trustassesses its performance against to judge whether the priorities have been met.
• The following table gives an overview of progress in the first quarter of 2015/16
Description Patient Safety
Clinical Effectiveness
Patient Experience Total
Target met or Baseline data collected to enable target setting
6 3 5 14
No improvement noted or Data not available (with plan in place to collect)
2 2 0 4
Target not met or Data not available (without plan in place to collect)
0 0 0 0
Target not due 2 1 2 5 Total 10 6 7 23
Summary Recommendations/comments The Board is asked to: • Note the contents of this report and actions planned
Page 4
Metric In Month YTD Thres-hold
Current Status
Trend over last 6 mnths
Forecast next month
Data Quality
Metric In Month
YTD Thres-hold
Current Status
Trend over last 6 mnths
Forecast next month
Data Quality
Metric In Month YTD Thres-hold
Current Status
Trend over last 6 mnths
Forecast next month
Data Quality
Patient experience Patient Experience Organisational Development
Incidents (number of)
Operational Efficiency £000 £000 £000
Cash Balance 30,519 - - - -
Assessments Capital Expenditure 458 2,520 3,262
CIP Performance 956 3,160 1,953
YTD (Surplus)/Deficit (387) 778 900
Prone Restraint 4 38 TBA - - CPA 7 Day Follow Up 96.6% 96% >=95% Monitor Governance Rating Green Green Green −
Seclusion 0 16 <=3 Falls Assessment within 48 hours 95.0% 96.5% >=95%
Pressure ulcer risk assessmentsBraden (Walsall coming soon) 92.4% 96.2% >=95%
Workforce
Workforce Patient access
Mandatory training completed 89.66% >95%
Vacancy numbers 8.23% - 0-10%
Sickness rates - 4.72% <4.5%
Patients have appointments within agreed limits CAMHS Tier 3 57.7% 58% - - -
Legend / KeyPatients have appointments within agreed limits CAMHS Tier 2 64.3% 61% - - -
Patients have appointments within agreed limits MAS (4 weeks) 93.2% 66% >=75%
Patients have appointments within agreed limits MAS (6 weeks) 95.8% 65% >=95%
Patient Satisfaction
Friends & Family Test - Response Rate (hospitals) 3% - - - - Patient experience
Data Quality Friends & Family Test - % Recommended (total responses) 95.7% - >=95% Number of complaints 34 187 - - -
Patients involved in their care? 97.2% - >=95% Number of compliments 488 2971 -- -
Duty of Candour 6 16 - - -
Q1 (771)77%
Monitor Financial Sustainability Risk Rating -2
Staff engagement(coming soon)
(Staff Friends & Family Test) place of work Quarterly(total responses)
-
(Staff Friends & Family Test) place of treatment Quarterly (total responses)--
Rating of handling of complaint. Reported quarterly (total responses)
Q1(12)67%
67%
86.5% 88%
>95%-
->73%
Are We Caring?
Patients have appointments & treatments within agreed limits - CMHTs
Patients have appointments & treatments within agreed limits - IAPT
Clinical supervision occurring according to Trust standard
In Month YTD Thres-
holdCurrent Status
-
Forecast next month
Data QualityMetric
78.1%
Trend over last 6 mnths
Month 5 - August 2015
<=30
Are We Safe?
>=66%
Are We Well Led?Are We Effective?
Readmission within 28 days to Mental Health Wards
-
Healthcare associated infections – C.diff
Readmission within 28 days to Community Hospitals
% of Bed days with delayed transfer from mental health unit
% patients with delayed transfer from Physical health unit
>=95%
-
Up to date care plans are in place for all patients on CPA (mental health)
8% <9%
9%
8.5%
5.44%
7%
9.8% - <3.5%
80.4% -
- <7.5%
>=90%
Falls resulting in injury on inpatient wards
Number of Patients Absconding
8.01% 6.93%
16 75
54
33 150
Whether patients feel safe in our mental health inpatient wards
Violent Incidents - Patient on Staff
81% 86%
Violent incidents - Patient on Patient
Patient Safety Incidents resulting in actual harm of moderate to catastrophic
-
-
-
->=55%
3
Thres-hold
-
>=98%
Are We Responsive?
YTD
Q1(771)62%
In Month Data Quality
194
1 9
7 28
0 0
−
<=1 per month
Venous Thromboembolism (VTE) risk assessment 94.2% 95.1% >=95%
Risk Assessments updated in previous 12 months (mental health) >=95%83.4% -
<8.08%
<45
<30
<=6
0 per month
Low. Data is reported with no easily discernible audit trail available or has data issues identified, data quality is unknown or individual numbers are small.
Moderate. Potential issues that could affect assurance of figures
Achieving against Trustwide threshold this month
Current status
Underachieving against Trustwide threshold this month / expect to underachieve against Trustwide threshold next month
Attention required
High. Data is captured electronically within an auditable system. Indicator has a full audit trail and both internal and external audits can assure the data or identify any potential issues.
Healthcare associated infections – MRSA bacteraemia
Avoidable pressure ulcers acquired in care (Grade 3 and above)
<=61 1091.2%Completed Appraisals last year -
>=95%
>=95%Metric
88%99.5%
Forecast next month
Trend over last 6 mnths
Current Status
2.0 Board Dashboard – Quality Metrics
G
R
H
M
L
A
H
H
H
H
H
H
H
H
H
H
H
H
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
M
L
L
L
L
L
M
L
R
G
G
G
R
G
G
R
R
R
G
G
G
G
G
G
G
R
R
R
A
G
R
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
G
A
R
R
G G
G
G
A A
R
G
R
G
G
M
M
G
G
A R
G
R
R
R
R
R
R
R
M
M
R
R
R
G G
R
Page 5
In month YTD Trend Data
Quality
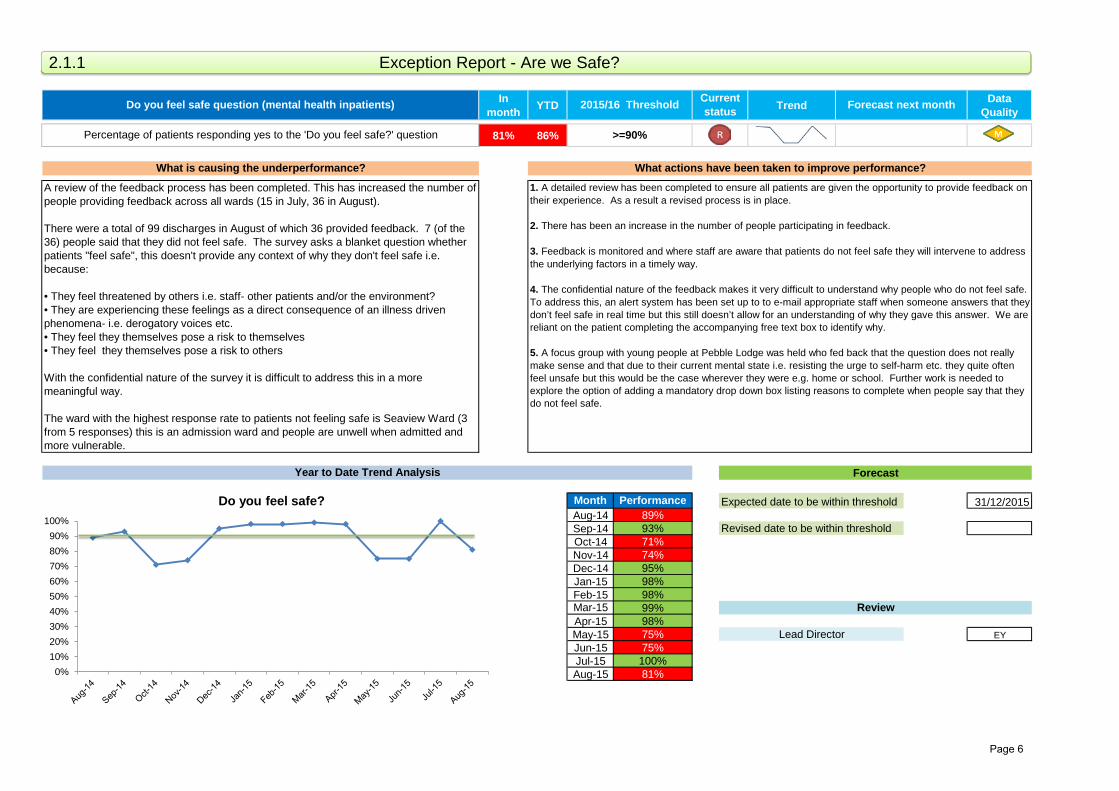
81% 86%
Month Performance 31/12/2015Aug-14 89%Sep-14 93%Oct-14 71%Nov-14 74%Dec-14 95%Jan-15 98%Feb-15 98%Mar-15 99%Apr-15 98%May-15 75% EYJun-15 75%Jul-15 100%Aug-15 81%
Forecast next month
>=90%
What is causing the underperformance? What actions have been taken to improve performance?
Do you feel safe question (mental health inpatients) 2015/16 Threshold Current status
Lead Director
Percentage of patients responding yes to the 'Do you feel safe?' question
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
A review of the feedback process has been completed. This has increased the number of people providing feedback across all wards (15 in July, 36 in August).
There were a total of 99 discharges in August of which 36 provided feedback. 7 (of the 36) people said that they did not feel safe. The survey asks a blanket question whetherpatients "feel safe", this doesn't provide any context of why they don't feel safe i.e.because:
• They feel threatened by others i.e. staff- other patients and/or the environment?• They are experiencing these feelings as a direct consequence of an illness drivenphenomena- i.e. derogatory voices etc.• They feel they themselves pose a risk to themselves• They feel they themselves pose a risk to others
With the confidential nature of the survey it is difficult to address this in a more meaningful way.
The ward with the highest response rate to patients not feeling safe is Seaview Ward (3 from 5 responses) this is an admission ward and people are unwell when admitted and more vulnerable.
1. A detailed review has been completed to ensure all patients are given the opportunity to provide feedback ontheir experience. As a result a revised process is in place.
2. There has been an increase in the number of people participating in feedback.
3. Feedback is monitored and where staff are aware that patients do not feel safe they will intervene to addressthe underlying factors in a timely way.
4. The confidential nature of the feedback makes it very difficult to understand why people who do not feel safe.To address this, an alert system has been set up to to e-mail appropriate staff when someone answers that they don’t feel safe in real time but this still doesn’t allow for an understanding of why they gave this answer. We arereliant on the patient completing the accompanying free text box to identify why.
5. A focus group with young people at Pebble Lodge was held who fed back that the question does not reallymake sense and that due to their current mental state i.e. resisting the urge to self-harm etc. they quite oftenfeel unsafe but this would be the case wherever they were e.g. home or school. Further work is needed toexplore the option of adding a mandatory drop down box listing reasons to complete when people say that theydo not feel safe.
2.1.1 Exception Report - Are we Safe?
0%10%20%30%40%50%60%70%80%90%
100%
Do you feel safe?
Page 6

In month YTD Trend Data
Quality
54 194
Month Performance 31/03/2016Aug-14 52Sep-14 30Oct-14 54Nov-14 24Dec-14 34Jan-15 50Feb-15 52Mar-15 35Apr-15 32May-15 33 FHJun-15 39Jul-15 36Aug-15 54 Data from 2014 used to set threshold, therefore not RAG rated.
Forecast next month
<=30
What is causing the underperformance? What actions have been taken to improve performance?
Falls resulting in injury on inpatient wards 2015/16 Threshold Current status
Lead Director
Number of falls resulting in injury on inpatient wards
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
The total number of inpatient falls in August was 118 with 54 (46%) falls resulting in injury. The following graph shows the harm from the fall.
Two patients sustained a fracture to an upper limb as a result of their falls (Linden Unit and Alumhurst Ward).
The falls with injury occurred across 20 wards. The wards with the highest number of falls resulting in injury were:- St Brelades Ward - 10 falls resulted in injury from 21 reported patient falls- Jersey Ward - 6 falls resulted in injury from 10 reported patient falls- Castletown Ward - 4 falls resulted in injury from 6 reported patient falls
Chalbury Ward had the second highest number of falls (14), three of these falls resulting in patient injury. Two patients on this ward each fell on four occasions in the month.
1. The risk register entries for falls have been reviewed and amalgamated into one overarching risk:There is a risk that patients may fall whilst under the care of DHC due to their individual medicalcondition, environmental factors, poor compliance with preventive measures, advice and recommendations, cognitive impairment, failure of staff to follow clinical guidelines and/or local policy in the management and prevention of falls.
2. A roadshow has been held at Westminster Memorial Hospital in Shaftesbury and falls awarenesstraining given.
3. The falls champions met in August and discussed falls prevention awareness and champions were given a poster to help continue to raise awareness with their colleagues.
4. The falls lead had a discussion with one of the patients on Jersey Ward, who had fallen, to understand the patient's perspective of the fall. There was some learning regarding listening to and acting on patients' concerns, particularly with regard to the type of equipment given. This has been shared with the ward and locality manager and discussed at the Safe Care Steering Group Meeting. The falls lead plans on collecting more patient stories going forward where possible.
5. An internal audit of the Trust's management of falls commenced in August. This is still ongoing.
2.1.2 Exception Report - Are we Safe?
M
0
10
20
30
40
50
60
70
Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug
Falls Resulting in Injury on Inpatient Wards
Aug-14 to Aug-15
Aug-13 to Aug-14
Page 7
8 | Page
In month YTD Trend Data
Quality
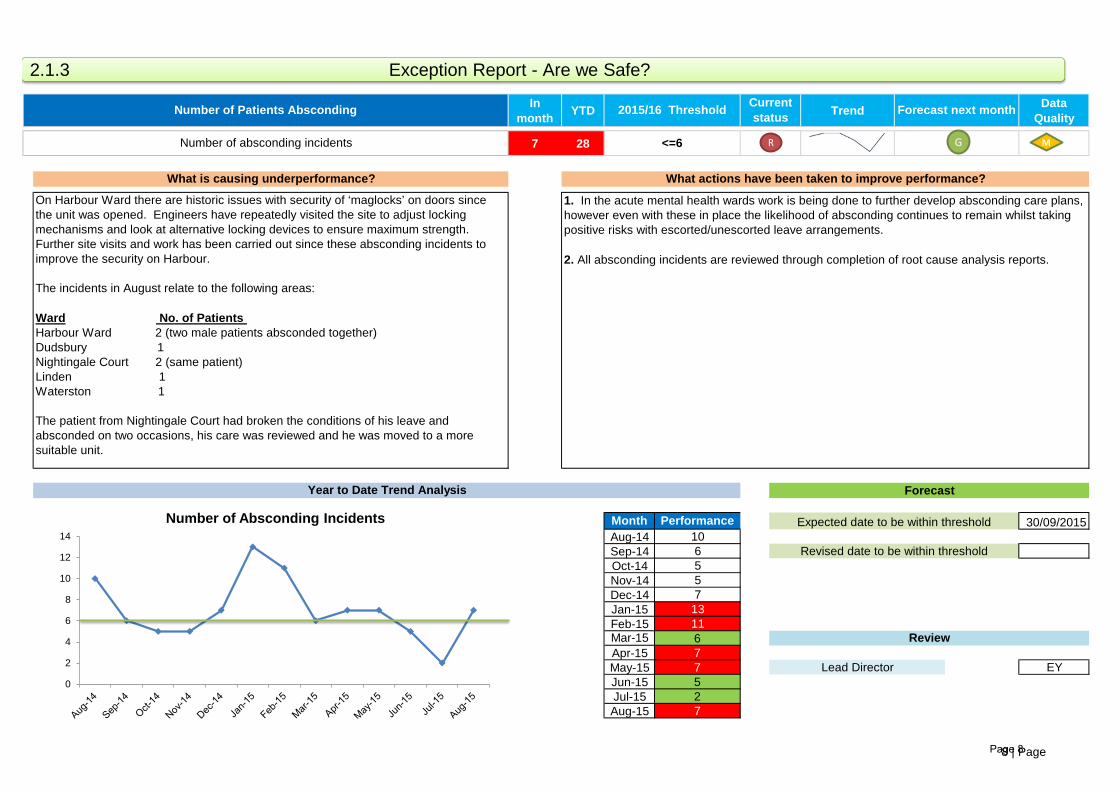
7 28
Month Performance 30/09/2015Aug-14 10Sep-14 6Oct-14 5Nov-14 5Dec-14 7Jan-15 13Feb-15 11Mar-15 6Apr-15 7May-15 7 EYJun-15 5Jul-15 2Aug-15 7
Lead Director
On Harbour Ward there are historic issues with security of ‘maglocks’ on doors since the unit was opened. Engineers have repeatedly visited the site to adjust locking mechanisms and look at alternative locking devices to ensure maximum strength. Further site visits and work has been carried out since these absconding incidents to improve the security on Harbour.
The incidents in August relate to the following areas:
Ward No. of Patients Harbour Ward 2 (two male patients absconded together)Dudsbury 1Nightingale Court 2 (same patient) Linden 1Waterston 1
The patient from Nightingale Court had broken the conditions of his leave and absconded on two occasions, his care was reviewed and he was moved to a more suitable unit.
1. In the acute mental health wards work is being done to further develop absconding care plans, however even with these in place the likelihood of absconding continues to remain whilst taking positive risks with escorted/unescorted leave arrangements.
2. All absconding incidents are reviewed through completion of root cause analysis reports.
Number of absconding incidents
Year to Date Trend Analysis Forecast
Review
Expected date to be within threshold
Revised date to be within threshold
Number of Patients Absconding 2015/16 Threshold Current status Forecast next month
<=6
What is causing underperformance? What actions have been taken to improve performance?
M R
2.1.3 Exception Report - Are we Safe?
0
2
4
6
8
10
12
14
Number of Absconding Incidents
G
Page 8
In month YTD Trend Data
Quality
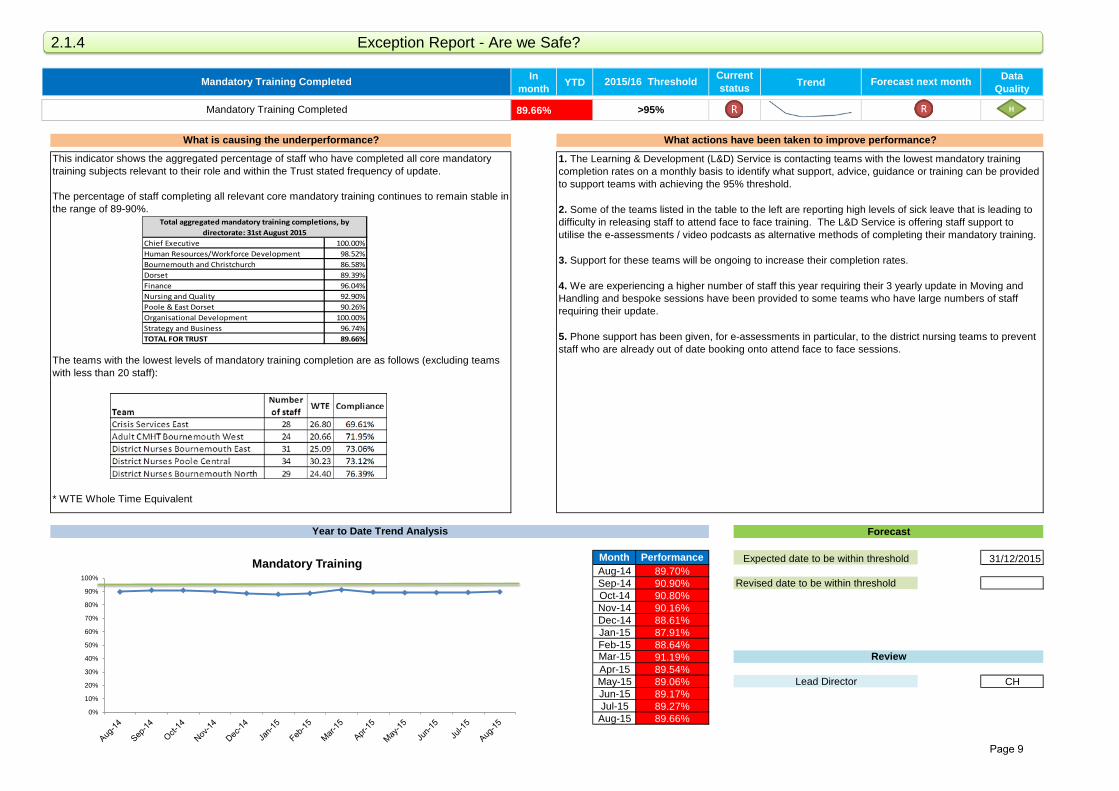
89.66%
Month Performance 31/12/2015Aug-14 89.70%Sep-14 90.90%Oct-14 90.80%Nov-14 90.16%Dec-14 88.61%Jan-15 87.91%Feb-15 88.64%Mar-15 91.19%Apr-15 89.54%May-15 89.06% CHJun-15 89.17%Jul-15 89.27%Aug-15 89.66%
Lead Director
This indicator shows the aggregated percentage of staff who have completed all core mandatory training subjects relevant to their role and within the Trust stated frequency of update.
The percentage of staff completing all relevant core mandatory training continues to remain stable in the range of 89-90%.
The teams with the lowest levels of mandatory training completion are as follows (excluding teams with less than 20 staff):
* WTE Whole Time Equivalent
1. The Learning & Development (L&D) Service is contacting teams with the lowest mandatory training completion rates on a monthly basis to identify what support, advice, guidance or training can be provided to support teams with achieving the 95% threshold.
2. Some of the teams listed in the table to the left are reporting high levels of sick leave that is leading to difficulty in releasing staff to attend face to face training. The L&D Service is offering staff support to utilise the e-assessments / video podcasts as alternative methods of completing their mandatory training.
3. Support for these teams will be ongoing to increase their completion rates.
4. We are experiencing a higher number of staff this year requiring their 3 yearly update in Moving and Handling and bespoke sessions have been provided to some teams who have large numbers of staff requiring their update.
5. Phone support has been given, for e-assessments in particular, to the district nursing teams to prevent staff who are already out of date booking onto attend face to face sessions.
Mandatory Training Completed
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
Mandatory Training Completed 2015/16 Threshold Current status Forecast next month
>95%
What is causing the underperformance? What actions have been taken to improve performance?
2.1.4 Exception Report - Are we Safe?
H
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Mandatory Training
Chief Executive 100.00%Human Resources/Workforce Development 98.52%Bournemouth and Christchurch 86.58%Dorset 89.39%Finance 96.04%Nursing and Quality 92.90%Poole & East Dorset 90.26%Organisational Development 100.00%Strategy and Business 96.74%TOTAL FOR TRUST 89.66%
Total aggregated mandatory training completions, by directorate: 31st August 2015
Page 9

In month
Rolling 12
monthTrend Data
Quality
- 4.72%
Month Rolling 12 months
Aug-14 4.76% 30/06/2016Sep-14 4.78%Oct-14 4.78% 31/01/2016Nov-14 4.79%Dec-14 4.77%Jan-15 4.77%Feb-15 4.76%Mar-15 4.75%Apr-15 4.73%May-15 4.72%Jun-15 4.64% CHJul-15 4.66%Aug-15 4.72%
Lead Director
1. Human Resources Coordinators support line managers aligned with the localities. The coordinators work very closely with first line managers and locality managers to offer guidance and advice in all aspects of attendance.
2. The coordinators also deliver quarterly Absence Management training, the most recent held 16th September 2015 with 16 delegates in attendance.
3. Support for managers is delivered in one to one face to face meetings / coaching, training sessions and attendance at head of department and locality meetings. There are good relationships between managers and the Human Resource Coordinators.
4. Work is ongoing supporting areas of the organisation with high absence rates. In respect of the service areas highlighted, each of these areas specifically have some significant long term sickness concerns. Work is ongoing with line managers to support successful returns to work, adjustments, medical redeployments or progressing to capability hearings (ill health).
5. Line managers are encouraged to take responsibility for commencing the absence management process for short term sickness upon staff reaching the trigger points set down by the Trust.
Sickness rates
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
The Trust rolling 12 month position is 4.72% for August 2015 against a threshold of <4.5%.
Excluding teams with less than 20 staff, the highest sickness absence levels are shown below:
* WTE Whole Time Equivalent
Sickness rates 2015/16 ThresholdRolling 12 months
Current status Forecast next month
<4.5%
What is causing the underperformance? What actions have been taken to improve performance?
2.1.5 Exception Report - Are we Safe?
M
3.0%
3.5%
4.0%
4.5%
5.0%Sickness Rate
Page 10
In month YTD Trend Data
Quality
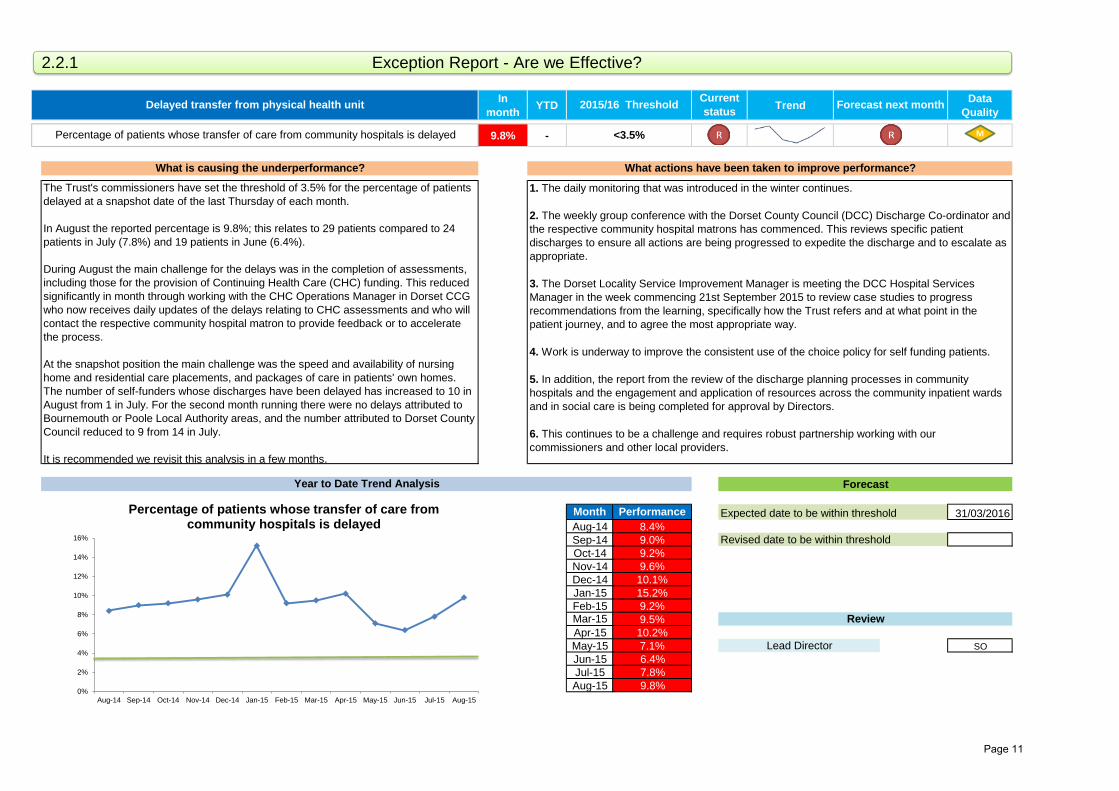
9.8% -
Month Performance 31/03/2016Aug-14 8.4%Sep-14 9.0%Oct-14 9.2%Nov-14 9.6%Dec-14 10.1%Jan-15 15.2%Feb-15 9.2%Mar-15 9.5%Apr-15 10.2%May-15 7.1% SOJun-15 6.4%Jul-15 7.8%Aug-15 9.8%
Forecast next month
<3.5%
What is causing the underperformance? What actions have been taken to improve performance?
Delayed transfer from physical health unit 2015/16 Threshold Current status
Lead Director
The Trust's commissioners have set the threshold of 3.5% for the percentage of patients delayed at a snapshot date of the last Thursday of each month.
In August the reported percentage is 9.8%; this relates to 29 patients compared to 24 patients in July (7.8%) and 19 patients in June (6.4%).
During August the main challenge for the delays was in the completion of assessments, including those for the provision of Continuing Health Care (CHC) funding. This reduced significantly in month through working with the CHC Operations Manager in Dorset CCG who now receives daily updates of the delays relating to CHC assessments and who will contact the respective community hospital matron to provide feedback or to accelerate the process.
At the snapshot position the main challenge was the speed and availability of nursing home and residential care placements, and packages of care in patients' own homes. The number of self-funders whose discharges have been delayed has increased to 10 in August from 1 in July. For the second month running there were no delays attributed to Bournemouth or Poole Local Authority areas, and the number attributed to Dorset County Council reduced to 9 from 14 in July. It is recommended we revisit this analysis in a few months.
1. The daily monitoring that was introduced in the winter continues.
2. The weekly group conference with the Dorset County Council (DCC) Discharge Co-ordinator and the respective community hospital matrons has commenced. This reviews specific patient discharges to ensure all actions are being progressed to expedite the discharge and to escalate as appropriate.
3. The Dorset Locality Service Improvement Manager is meeting the DCC Hospital Services Manager in the week commencing 21st September 2015 to review case studies to progress recommendations from the learning, specifically how the Trust refers and at what point in the patient journey, and to agree the most appropriate way.
4. Work is underway to improve the consistent use of the choice policy for self funding patients.
5. In addition, the report from the review of the discharge planning processes in community hospitals and the engagement and application of resources across the community inpatient wards and in social care is being completed for approval by Directors.
6. This continues to be a challenge and requires robust partnership working with our commissioners and other local providers.
Percentage of patients whose transfer of care from community hospitals is delayed
Year to Date Trend Analysis Forecast
Review
Expected date to be within threshold
Revised date to be within threshold
2.2.1 Exception Report - Are we Effective?
M
0%
2%
4%
6%
8%
10%
12%
14%
16%
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Percentage of patients whose transfer of care from community hospitals is delayed
Page 11

In month YTD Trend Data
Quality
80.4% -
Month Performance 31/03/2016Aug-14Sep-14Oct-14Nov-14Dec-14Jan-15Feb-15 83.3%Mar-15 82.4%Apr-15 81.4%May-15 77.5% EY/LB/SOJun-15 81.3%Jul-15 80.6%Aug-15 80.4%
Forecast next month
>=95%
What is causing the underperformance? What actions have been taken to improve performance?
Up to date care plans are in place for all patients on CPA 2015/16 Threshold Current status
Lead Director
Percentage of patients on CPA with up to date care plans (mental health)
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
This relates to 547 individual patients where a specific problem or issue hasn’t been updated within the care plan on the electronic clinical record. Care plans can consist of several parts with interventions in place for each.
Some basic analysis has been undertaken on the exceptions and this indicates that some care plans are not being closed on discharge from inpatient services or from transfer/movement between teams. This means the person responsible for updating and/or closing down the care plan may no longer be involved within the persons care following the transition.
Clinical teams need to ensure they are updating and/or closing individual problems as soon as they are no longer relevant.
The Trust is compliant with completing formal reviews of patients on CPA within 12 months (August 95.5%), this process should include the review of all care plans. Reports from the clinical system show that the written care plans are not being updated at the same rate showing a lower performance for this metric.
1. A data quality review of reporting has been undertaken to ensure the reports are pulling the correct data.
2. Exceptions are sent to all teams to address.
3. Reports have been updated to include the person who wrote the care plan problem as well as the person's care-coordinator who is responsible for their ongoing care.
4. Care Plan training forms part of the Mental Health Foundation Pathway which is mandatory training for mental health staff.
5. Work to agree the consistency of care plans and documentation has been undertaken (such as the Care Plan Tool Box) and has been implemented to assist the care planning process.
2.2.2 Exception Report - Are we Effective?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Up to Date Care Plans in Place for all Patients on CPA
Page 12
In month YTD Trend Data
Quality
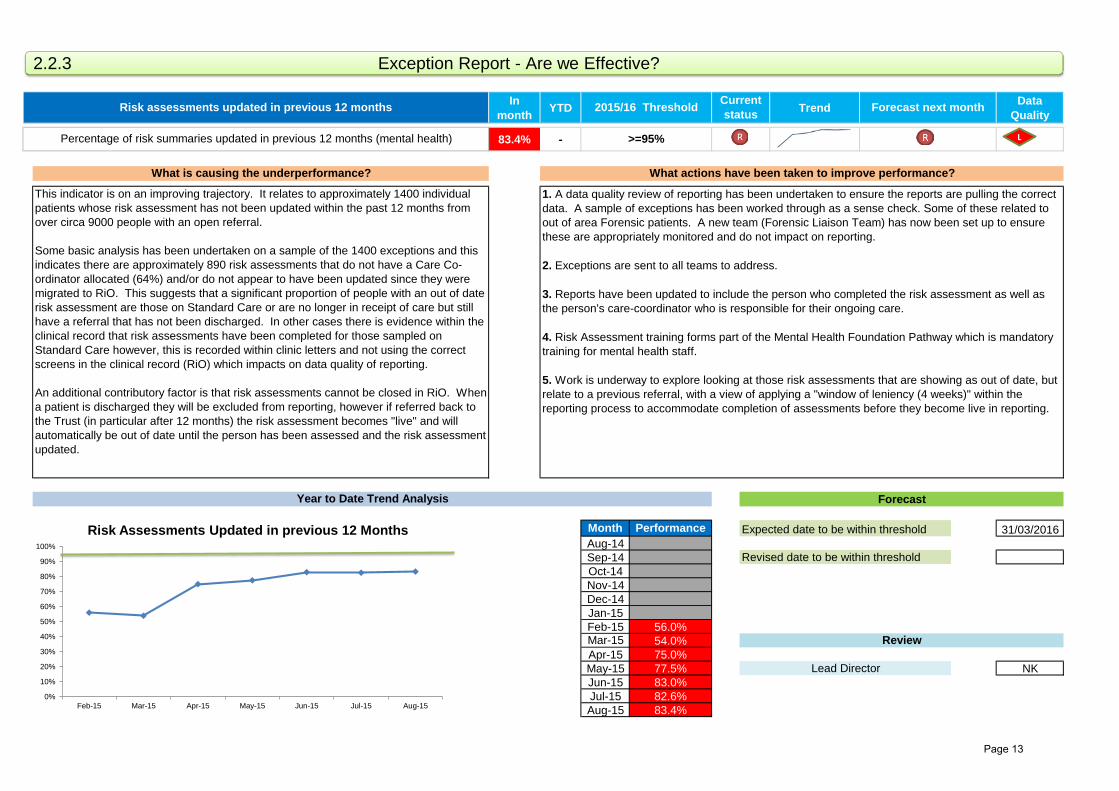
83.4% -
Month Performance 31/03/2016Aug-14Sep-14Oct-14Nov-14Dec-14Jan-15Feb-15 56.0%Mar-15 54.0%Apr-15 75.0%May-15 77.5% NKJun-15 83.0%Jul-15 82.6%Aug-15 83.4%
Lead Director
Percentage of risk summaries updated in previous 12 months (mental health)
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
This indicator is on an improving trajectory. It relates to approximately 1400 individual patients whose risk assessment has not been updated within the past 12 months from over circa 9000 people with an open referral.
Some basic analysis has been undertaken on a sample of the 1400 exceptions and this indicates there are approximately 890 risk assessments that do not have a Care Co-ordinator allocated (64%) and/or do not appear to have been updated since they were migrated to RiO. This suggests that a significant proportion of people with an out of date risk assessment are those on Standard Care or are no longer in receipt of care but still have a referral that has not been discharged. In other cases there is evidence within the clinical record that risk assessments have been completed for those sampled on Standard Care however, this is recorded within clinic letters and not using the correct screens in the clinical record (RiO) which impacts on data quality of reporting.
An additional contributory factor is that risk assessments cannot be closed in RiO. When a patient is discharged they will be excluded from reporting, however if referred back to the Trust (in particular after 12 months) the risk assessment becomes "live" and will automatically be out of date until the person has been assessed and the risk assessment updated.
1. A data quality review of reporting has been undertaken to ensure the reports are pulling the correct data. A sample of exceptions has been worked through as a sense check. Some of these related to out of area Forensic patients. A new team (Forensic Liaison Team) has now been set up to ensure these are appropriately monitored and do not impact on reporting.
2. Exceptions are sent to all teams to address.
3. Reports have been updated to include the person who completed the risk assessment as well as the person's care-coordinator who is responsible for their ongoing care.
4. Risk Assessment training forms part of the Mental Health Foundation Pathway which is mandatory training for mental health staff.
5. Work is underway to explore looking at those risk assessments that are showing as out of date, but relate to a previous referral, with a view of applying a "window of leniency (4 weeks)" within the reporting process to accommodate completion of assessments before they become live in reporting.
Risk assessments updated in previous 12 months 2015/16 Threshold Current status Forecast next month
>=95%
What is causing the underperformance? What actions have been taken to improve performance?
2.2.3 Exception Report - Are we Effective?
L
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Risk Assessments Updated in previous 12 Months
Page 13
16 | Page
In month YTD Trend Data
Quality
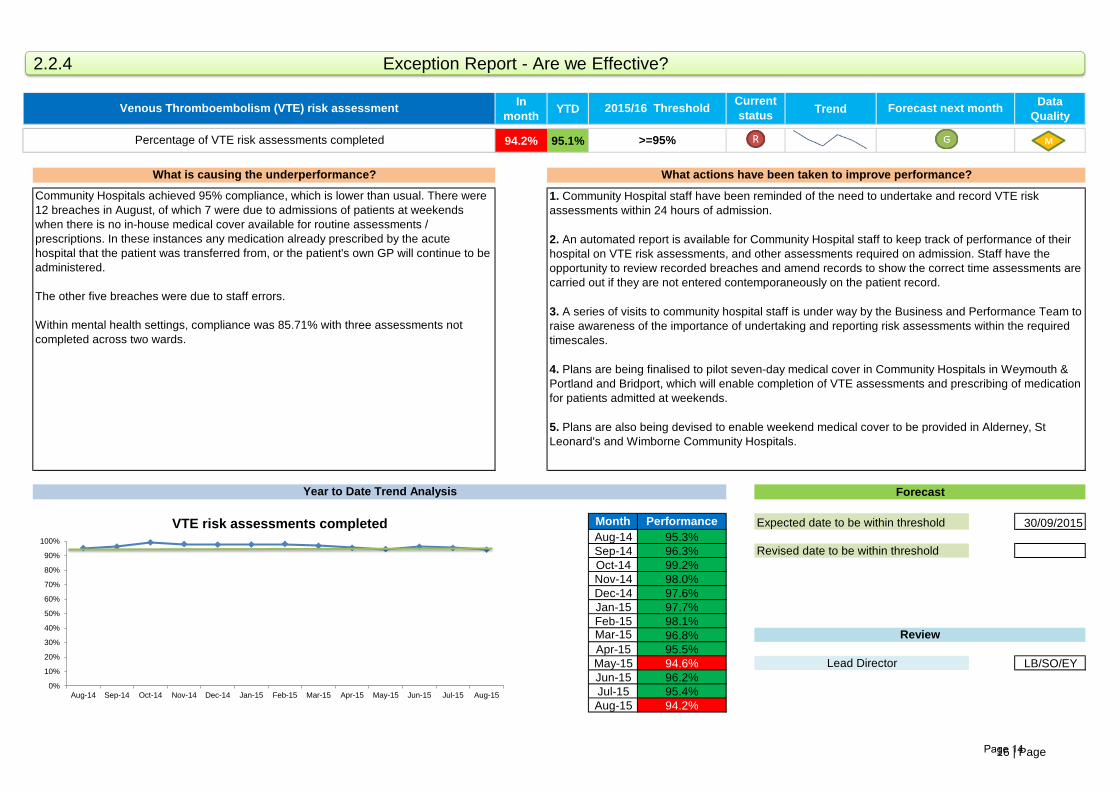
94.2% 95.1%
Month Performance 30/09/2015Aug-14 95.3%Sep-14 96.3%Oct-14 99.2%Nov-14 98.0%Dec-14 97.6%Jan-15 97.7%Feb-15 98.1%Mar-15 96.8%Apr-15 95.5%May-15 94.6% LB/SO/EYJun-15 96.2%Jul-15 95.4%Aug-15 94.2%
Forecast next month
>=95%
What is causing the underperformance? What actions have been taken to improve performance?
Venous Thromboembolism (VTE) risk assessment 2015/16 Threshold Current status
Lead Director
Percentage of VTE risk assessments completed
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
Community Hospitals achieved 95% compliance, which is lower than usual. There were 12 breaches in August, of which 7 were due to admissions of patients at weekends when there is no in-house medical cover available for routine assessments / prescriptions. In these instances any medication already prescribed by the acute hospital that the patient was transferred from, or the patient's own GP will continue to be administered.
The other five breaches were due to staff errors.
Within mental health settings, compliance was 85.71% with three assessments not completed across two wards.
1. Community Hospital staff have been reminded of the need to undertake and record VTE risk assessments within 24 hours of admission.
2. An automated report is available for Community Hospital staff to keep track of performance of their hospital on VTE risk assessments, and other assessments required on admission. Staff have the opportunity to review recorded breaches and amend records to show the correct time assessments are carried out if they are not entered contemporaneously on the patient record.
3. A series of visits to community hospital staff is under way by the Business and Performance Team to raise awareness of the importance of undertaking and reporting risk assessments within the required timescales.
4. Plans are being finalised to pilot seven-day medical cover in Community Hospitals in Weymouth & Portland and Bridport, which will enable completion of VTE assessments and prescribing of medication for patients admitted at weekends.
5. Plans are also being devised to enable weekend medical cover to be provided in Alderney, St Leonard's and Wimborne Community Hospitals.
2.2.4 Exception Report - Are we Effective?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
VTE risk assessments completed
M
Page 14
16 | Page
In month YTD Trend Data
Quality
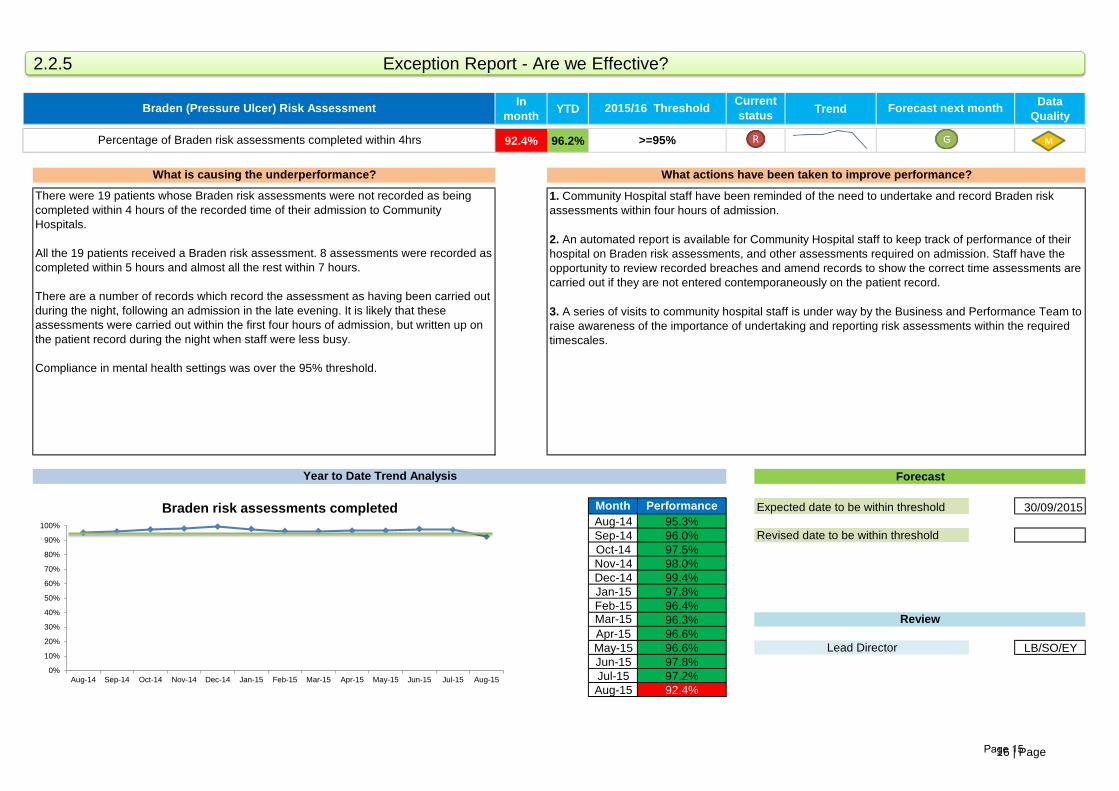
92.4% 96.2%
Month Performance 30/09/2015Aug-14 95.3%Sep-14 96.0%Oct-14 97.5%Nov-14 98.0%Dec-14 99.4%Jan-15 97.8%Feb-15 96.4%Mar-15 96.3%Apr-15 96.6%May-15 96.6% LB/SO/EYJun-15 97.8%Jul-15 97.2%Aug-15 92.4%
Lead Director
Percentage of Braden risk assessments completed within 4hrs
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
There were 19 patients whose Braden risk assessments were not recorded as being completed within 4 hours of the recorded time of their admission to Community Hospitals.
All the 19 patients received a Braden risk assessment. 8 assessments were recorded as completed within 5 hours and almost all the rest within 7 hours.
There are a number of records which record the assessment as having been carried out during the night, following an admission in the late evening. It is likely that these assessments were carried out within the first four hours of admission, but written up on the patient record during the night when staff were less busy.
Compliance in mental health settings was over the 95% threshold.
1. Community Hospital staff have been reminded of the need to undertake and record Braden risk assessments within four hours of admission.
2. An automated report is available for Community Hospital staff to keep track of performance of their hospital on Braden risk assessments, and other assessments required on admission. Staff have the opportunity to review recorded breaches and amend records to show the correct time assessments are carried out if they are not entered contemporaneously on the patient record.
3. A series of visits to community hospital staff is under way by the Business and Performance Team to raise awareness of the importance of undertaking and reporting risk assessments within the required timescales.
Braden (Pressure Ulcer) Risk Assessment 2015/16 Threshold Current status Forecast next month
>=95%
What is causing the underperformance? What actions have been taken to improve performance?
2.2.5 Exception Report - Are we Effective?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Braden risk assessments completed
M
Page 15
In month YTD Trend Data
Quality
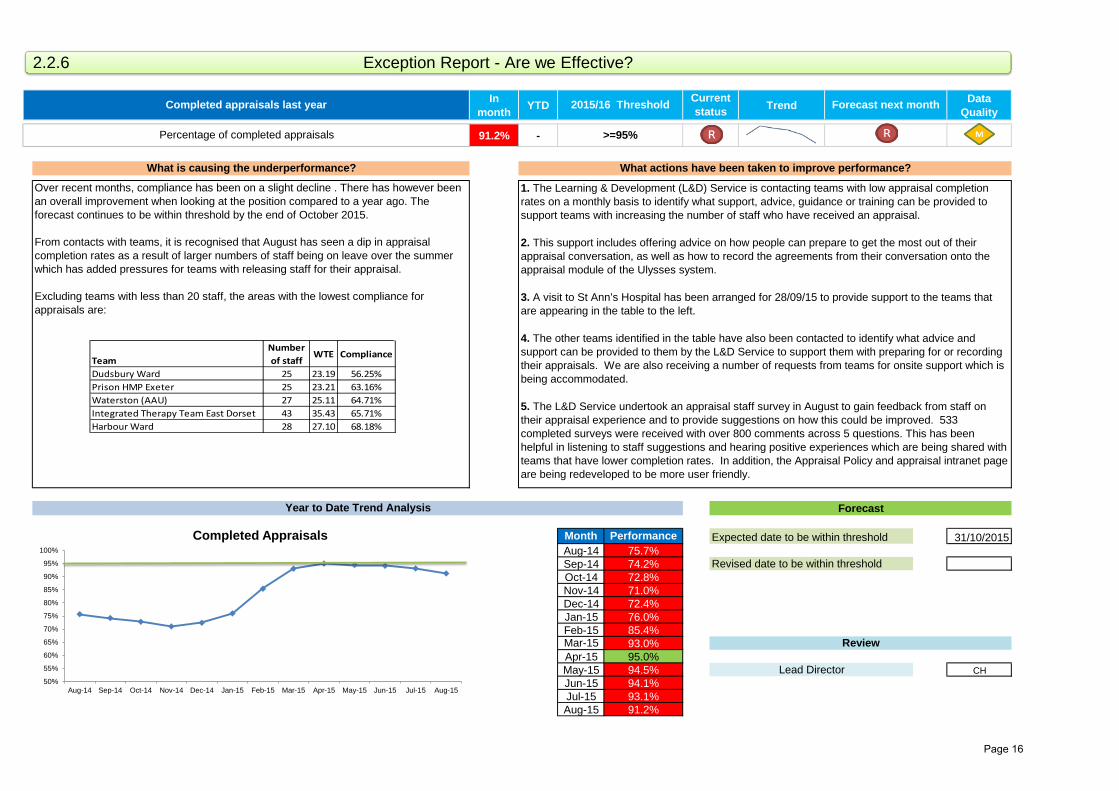
91.2% -
Month Performance 31/10/2015Aug-14 75.7%Sep-14 74.2%Oct-14 72.8%Nov-14 71.0%Dec-14 72.4%Jan-15 76.0%Feb-15 85.4%Mar-15 93.0%Apr-15 95.0%May-15 94.5% CHJun-15 94.1%Jul-15 93.1%Aug-15 91.2%
Lead Director
Percentage of completed appraisals
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
Over recent months, compliance has been on a slight decline . There has however been an overall improvement when looking at the position compared to a year ago. The forecast continues to be within threshold by the end of October 2015.
From contacts with teams, it is recognised that August has seen a dip in appraisal completion rates as a result of larger numbers of staff being on leave over the summer which has added pressures for teams with releasing staff for their appraisal.
Excluding teams with less than 20 staff, the areas with the lowest compliance for appraisals are:
1. The Learning & Development (L&D) Service is contacting teams with low appraisal completion rates on a monthly basis to identify what support, advice, guidance or training can be provided to support teams with increasing the number of staff who have received an appraisal.
2. This support includes offering advice on how people can prepare to get the most out of their appraisal conversation, as well as how to record the agreements from their conversation onto the appraisal module of the Ulysses system.
3. A visit to St Ann’s Hospital has been arranged for 28/09/15 to provide support to the teams that are appearing in the table to the left.
4. The other teams identified in the table have also been contacted to identify what advice and support can be provided to them by the L&D Service to support them with preparing for or recording their appraisals. We are also receiving a number of requests from teams for onsite support which is being accommodated.
5. The L&D Service undertook an appraisal staff survey in August to gain feedback from staff on their appraisal experience and to provide suggestions on how this could be improved. 533 completed surveys were received with over 800 comments across 5 questions. This has been helpful in listening to staff suggestions and hearing positive experiences which are being shared with teams that have lower completion rates. In addition, the Appraisal Policy and appraisal intranet page are being redeveloped to be more user friendly.
Completed appraisals last year 2015/16 Threshold Current status Forecast next month
>=95%
What is causing the underperformance? What actions have been taken to improve performance?
2.2.6 Exception Report - Are we Effective?
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Completed Appraisals
TeamNumber of staff
WTE Compliance
Dudsbury Ward 25 23.19 56.25%Prison HMP Exeter 25 23.21 63.16%Waterston (AAU) 27 25.11 64.71%Integrated Therapy Team East Dorset 43 35.43 65.71%Harbour Ward 28 27.10 68.18%
Page 16
In month YTD Trend Data
Quality
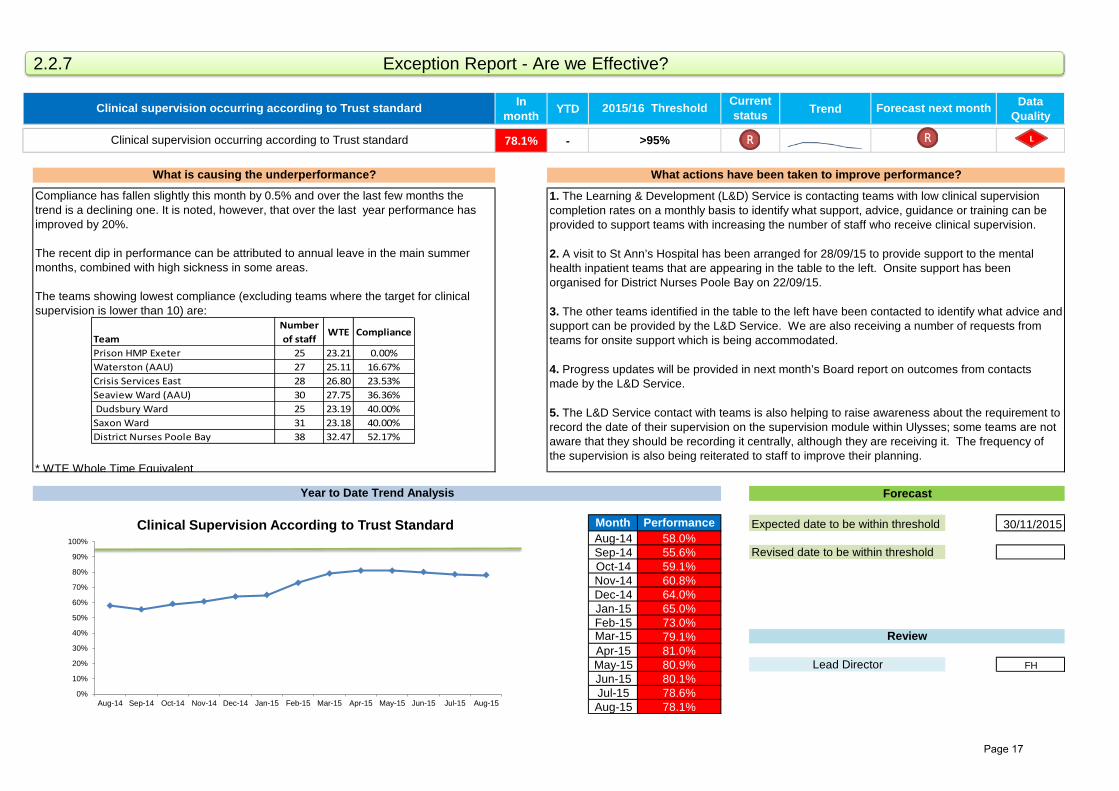
78.1% -
Month Performance 30/11/2015Aug-14 58.0%Sep-14 55.6%Oct-14 59.1%Nov-14 60.8%Dec-14 64.0%Jan-15 65.0%Feb-15 73.0%Mar-15 79.1%Apr-15 81.0%May-15 80.9% FHJun-15 80.1%Jul-15 78.6%Aug-15 78.1%
Lead Director
Compliance has fallen slightly this month by 0.5% and over the last few months the trend is a declining one. It is noted, however, that over the last year performance has improved by 20%.
The recent dip in performance can be attributed to annual leave in the main summer months, combined with high sickness in some areas.
The teams showing lowest compliance (excluding teams where the target for clinical supervision is lower than 10) are:
* WTE Whole Time Equivalent
1. The Learning & Development (L&D) Service is contacting teams with low clinical supervision completion rates on a monthly basis to identify what support, advice, guidance or training can be provided to support teams with increasing the number of staff who receive clinical supervision.
2. A visit to St Ann’s Hospital has been arranged for 28/09/15 to provide support to the mental health inpatient teams that are appearing in the table to the left. Onsite support has been organised for District Nurses Poole Bay on 22/09/15.
3. The other teams identified in the table to the left have been contacted to identify what advice and support can be provided by the L&D Service. We are also receiving a number of requests from teams for onsite support which is being accommodated.
4. Progress updates will be provided in next month’s Board report on outcomes from contacts made by the L&D Service.
5. The L&D Service contact with teams is also helping to raise awareness about the requirement to record the date of their supervision on the supervision module within Ulysses; some teams are not aware that they should be recording it centrally, although they are receiving it. The frequency of the supervision is also being reiterated to staff to improve their planning.
Clinical supervision occurring according to Trust standard
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
Clinical supervision occurring according to Trust standard 2015/16 Threshold Current status Forecast next month
>95%
What is causing the underperformance? What actions have been taken to improve performance?
2.2.7 Exception Report - Are we Effective?
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Clinical Supervision According to Trust Standard
TeamNumber of staff
WTE Compliance
Prison HMP Exeter 25 23.21 0.00%Waterston (AAU) 27 25.11 16.67%Crisis Services East 28 26.80 23.53%Seaview Ward (AAU) 30 27.75 36.36% Dudsbury Ward 25 23.19 40.00%Saxon Ward 31 23.18 40.00%District Nurses Poole Bay 38 32.47 52.17%
Page 17
In month YTD Trend Data
Quality
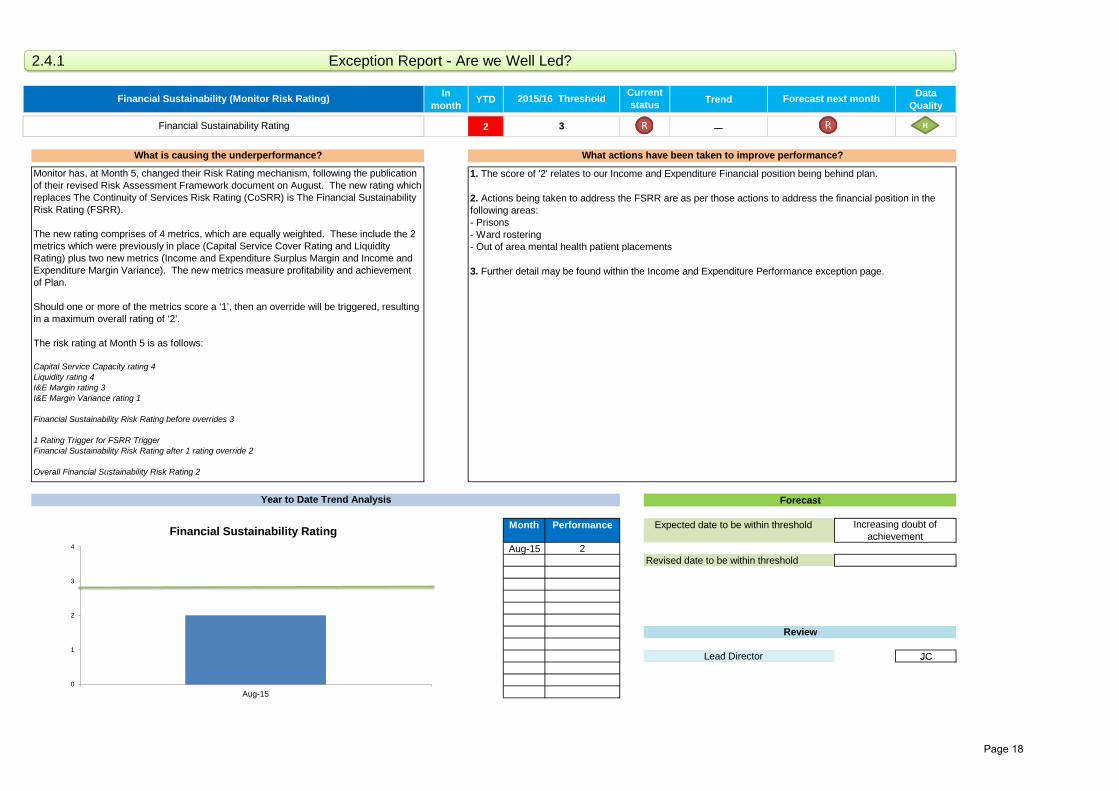
2 −
Month Performance
Aug-15 2
JCLead Director
Monitor has, at Month 5, changed their Risk Rating mechanism, following the publication of their revised Risk Assessment Framework document on August. The new rating which replaces The Continuity of Services Risk Rating (CoSRR) is The Financial Sustainability Risk Rating (FSRR).
The new rating comprises of 4 metrics, which are equally weighted. These include the 2 metrics which were previously in place (Capital Service Cover Rating and Liquidity Rating) plus two new metrics (Income and Expenditure Surplus Margin and Income and Expenditure Margin Variance). The new metrics measure profitability and achievement of Plan.
Should one or more of the metrics score a ‘1’, then an override will be triggered, resulting in a maximum overall rating of ‘2’.
The risk rating at Month 5 is as follows:
Capital Service Capacity rating 4Liquidity rating 4I&E Margin rating 3I&E Margin Variance rating 1 Financial Sustainability Risk Rating before overrides 3 1 Rating Trigger for FSRR TriggerFinancial Sustainability Risk Rating after 1 rating override 2 Overall Financial Sustainability Risk Rating 2
1. The score of '2' relates to our Income and Expenditure Financial position being behind plan.
2. Actions being taken to address the FSRR are as per those actions to address the financial position in the following areas:- Prisons- Ward rostering- Out of area mental health patient placements
3. Further detail may be found within the Income and Expenditure Performance exception page.
Financial Sustainability Rating
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
Increasing doubt of achievement
Financial Sustainability (Monitor Risk Rating) 2015/16 Threshold Current status Forecast next month
3
What is causing the underperformance? What actions have been taken to improve performance?
2.4.1 Exception Report - Are we Well Led?
H
0
1
2
3
4
Aug-15
Financial Sustainability Rating
Page 18
In month YTD Trend Data
Quality
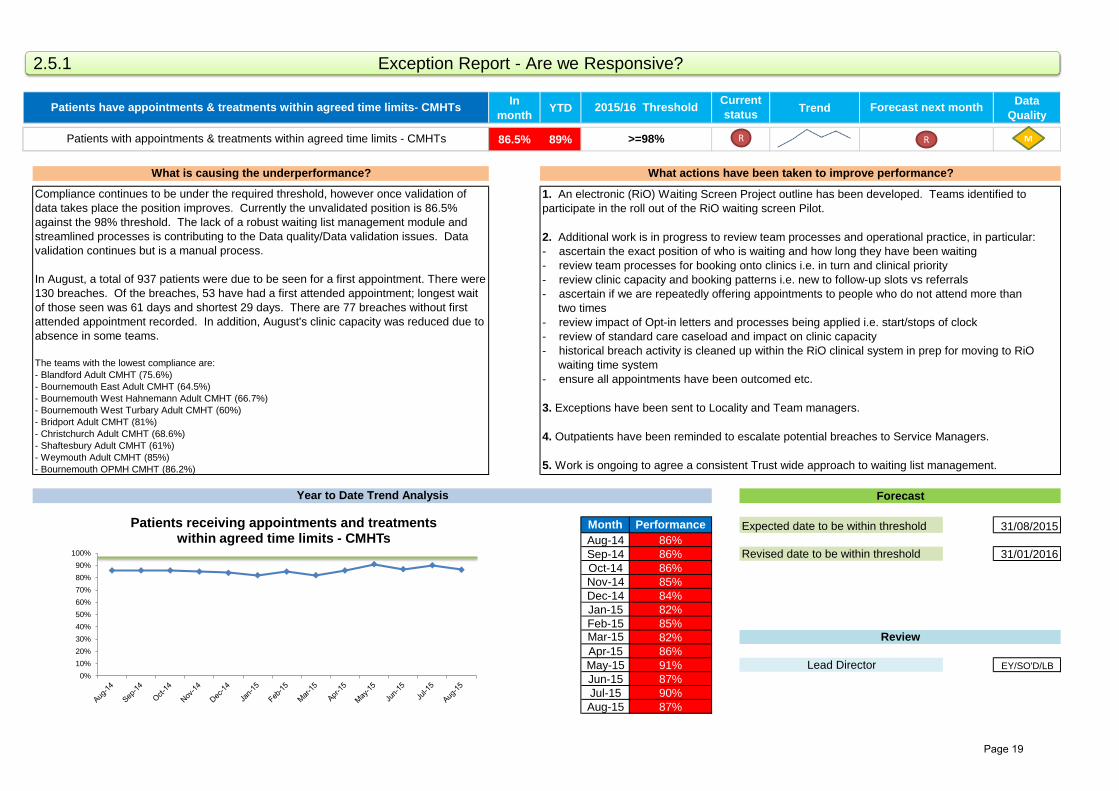
86.5% 89%
Month Performance 31/08/2015Aug-14 86%Sep-14 86% 31/01/2016Oct-14 86%Nov-14 85%Dec-14 84%Jan-15 82%Feb-15 85%Mar-15 82%Apr-15 86%May-15 91% EY/SO'D/LBJun-15 87%Jul-15 90%Aug-15 87%
Lead Director
Patients with appointments & treatments within agreed time limits - CMHTs
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
Compliance continues to be under the required threshold, however once validation of data takes place the position improves. Currently the unvalidated position is 86.5% against the 98% threshold. The lack of a robust waiting list management module and streamlined processes is contributing to the Data quality/Data validation issues. Data validation continues but is a manual process.
In August, a total of 937 patients were due to be seen for a first appointment. There were 130 breaches. Of the breaches, 53 have had a first attended appointment; longest wait of those seen was 61 days and shortest 29 days. There are 77 breaches without first attended appointment recorded. In addition, August's clinic capacity was reduced due to absence in some teams.
The teams with the lowest compliance are: - Blandford Adult CMHT (75.6%)- Bournemouth East Adult CMHT (64.5%)- Bournemouth West Hahnemann Adult CMHT (66.7%)- Bournemouth West Turbary Adult CMHT (60%) - Bridport Adult CMHT (81%)- Christchurch Adult CMHT (68.6%)- Shaftesbury Adult CMHT (61%)- Weymouth Adult CMHT (85%)- Bournemouth OPMH CMHT (86.2%)
1. An electronic (RiO) Waiting Screen Project outline has been developed. Teams identified to participate in the roll out of the RiO waiting screen Pilot.
2. Additional work is in progress to review team processes and operational practice, in particular: - ascertain the exact position of who is waiting and how long they have been waiting - review team processes for booking onto clinics i.e. in turn and clinical priority - review clinic capacity and booking patterns i.e. new to follow-up slots vs referrals- ascertain if we are repeatedly offering appointments to people who do not attend more than two times- review impact of Opt-in letters and processes being applied i.e. start/stops of clock - review of standard care caseload and impact on clinic capacity - historical breach activity is cleaned up within the RiO clinical system in prep for moving to RiO waiting time system- ensure all appointments have been outcomed etc.
3. Exceptions have been sent to Locality and Team managers. 4. Outpatients have been reminded to escalate potential breaches to Service Managers.
5. Work is ongoing to agree a consistent Trust wide approach to waiting list management.
Patients have appointments & treatments within agreed time limits- CMHTs 2015/16 Threshold Current status Forecast next month
>=98%
What is causing the underperformance? What actions have been taken to improve performance?
2.5.1 Exception Report - Are we Responsive?
R
0%10%20%30%40%50%60%70%80%90%
100%
Patients receiving appointments and treatments within agreed time limits - CMHTs
R
Page 19

In month£000
YTD£000 Trend Data
Quality
6
Month Number N/A
Apr-15 3May-15 3Jun-15 2Jul-15 2Aug-15 6Sep-15Oct-15Nov-15Dec-15 FHJan-16Feb-16Mar-16
Forecast next month
- - -
How many have been reported? What actions have been taken?
Duty of Candour - number of cases identified
Duty of Candour 2015/16 Threshold£000
Current status
16
Expected date to be within threshold
Revised date to meet target
Review
Lead Director
Year to Date Trend Analysis Forecast
Duty of candour is about openness and transparency and providing information, support and an apology when things go wrong with a person's care or treatment.
The Trust has identified 16 incidents relevant for duty of candour since April 2015. In August there were six.
Details of the types of incidents are given below:
The teams where duty of candour incidents have been identified are:
1. A three week deadline has been agreed for reviewing pressure ulcers to ensure that learning happens in a timely fashion and enables patients to get the results of any investigation quicker.
2. There is a process in place to monitor that an apology has been given in line with duty of candour. To enhance this process, the Trust is introducing the utilisation of the electronic adverse incident database to automate the process of requesting and processing root cause analysis reviews and recording details of duty of candour.
0
1
2
3
4
5
6
7
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
Number of Duty of Candour cases
2.6 Additional Report - Are we Responsive?
Page 20
In month YTD Trend Data
Quality
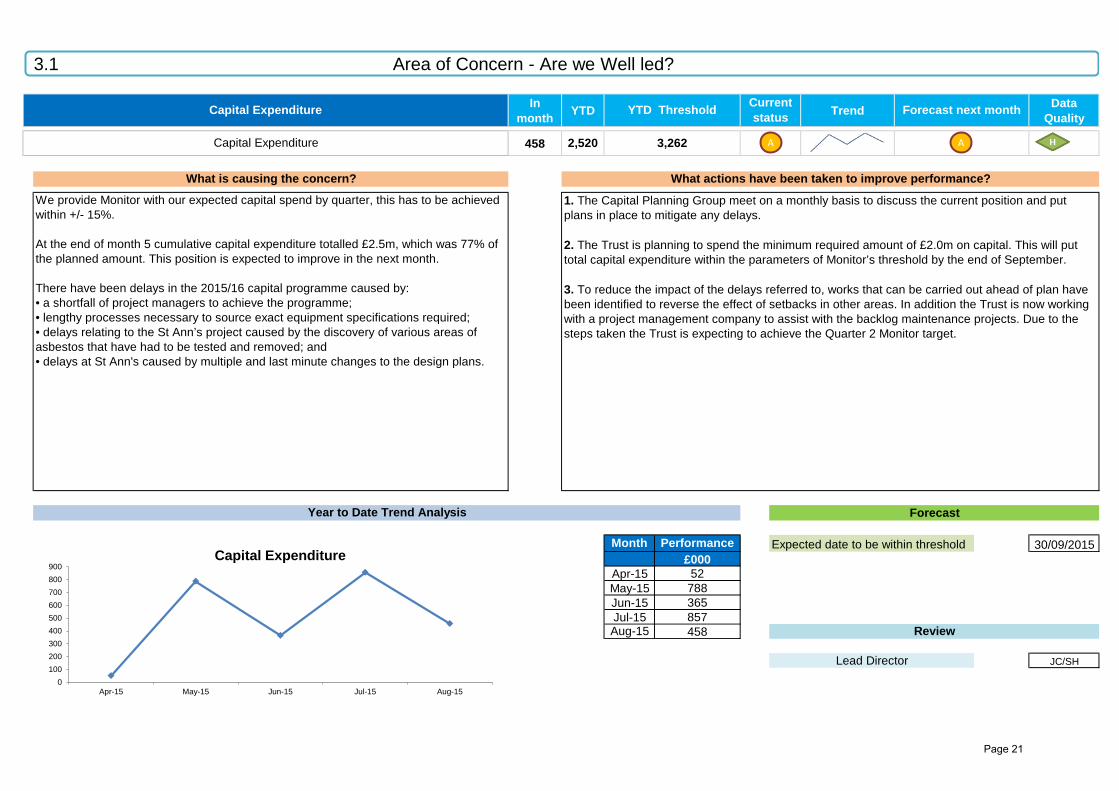
458
Month Performance 30/09/2015£000
Apr-15 52May-15 788Jun-15 365Jul-15 857Aug-15 458
JC/SHLead Director
Capital Expenditure
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Review
We provide Monitor with our expected capital spend by quarter, this has to be achieved within +/- 15%.
At the end of month 5 cumulative capital expenditure totalled £2.5m, which was 77% of the planned amount. This position is expected to improve in the next month.
There have been delays in the 2015/16 capital programme caused by: • a shortfall of project managers to achieve the programme; • lengthy processes necessary to source exact equipment specifications required; • delays relating to the St Ann’s project caused by the discovery of various areas of asbestos that have had to be tested and removed; and• delays at St Ann's caused by multiple and last minute changes to the design plans.
1. The Capital Planning Group meet on a monthly basis to discuss the current position and put plans in place to mitigate any delays.
2. The Trust is planning to spend the minimum required amount of £2.0m on capital. This will put total capital expenditure within the parameters of Monitor’s threshold by the end of September.
3. To reduce the impact of the delays referred to, works that can be carried out ahead of plan have been identified to reverse the effect of setbacks in other areas. In addition the Trust is now working with a project management company to assist with the backlog maintenance projects. Due to the steps taken the Trust is expecting to achieve the Quarter 2 Monitor target.
2,520
Capital Expenditure YTD Threshold Current status Forecast next month
3,262
What is causing the concern? What actions have been taken to improve performance?
3.1 Area of Concern - Are we Well led?
A
0100200300400500600700800900
Apr-15 May-15 Jun-15 Jul-15 Aug-15
Capital Expenditure
A
Page 21
In month YTD Trend Data
Quality
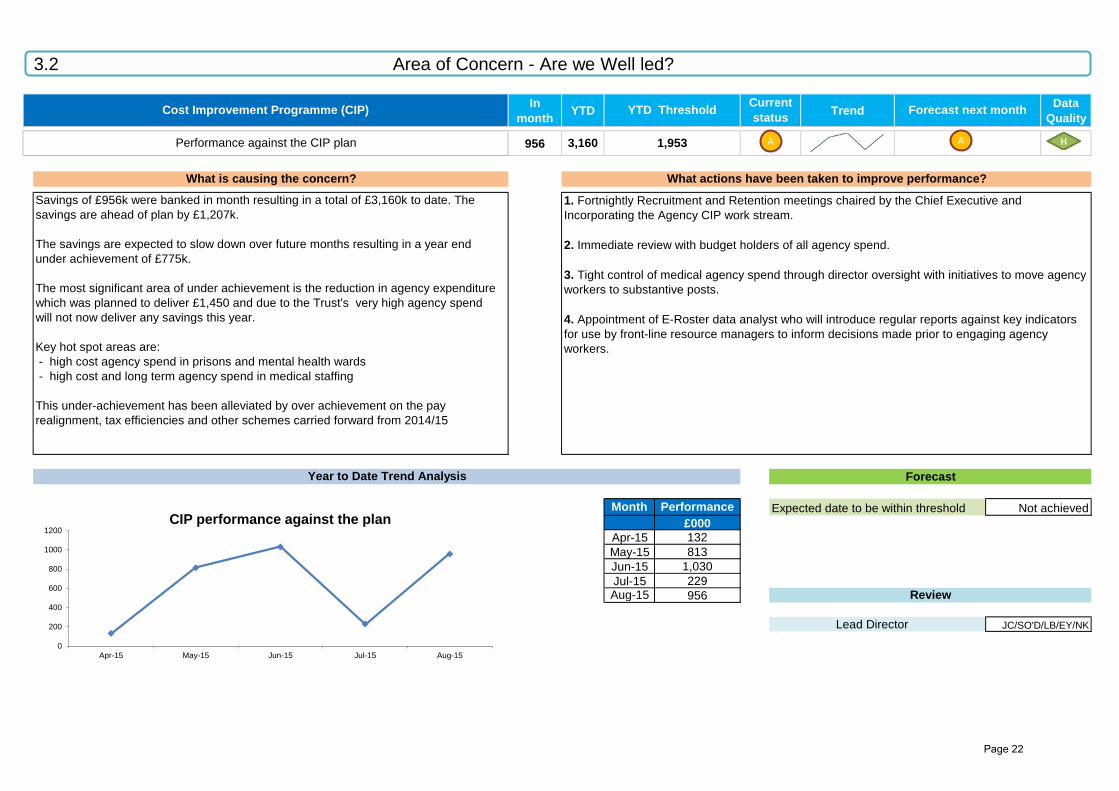
956
Month Performance£000
Apr-15 132May-15 813Jun-15 1,030Jul-15 229Aug-15 956
Lead Director
Performance against the CIP plan
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Review
1. Fortnightly Recruitment and Retention meetings chaired by the Chief Executive and Incorporating the Agency CIP work stream.
2. Immediate review with budget holders of all agency spend.
3. Tight control of medical agency spend through director oversight with initiatives to move agency workers to substantive posts.
4. Appointment of E-Roster data analyst who will introduce regular reports against key indicators for use by front-line resource managers to inform decisions made prior to engaging agency workers.
3,160
JC/SO'D/LB/EY/NK
Not achieved
Savings of £956k were banked in month resulting in a total of £3,160k to date. The savings are ahead of plan by £1,207k. The savings are expected to slow down over future months resulting in a year end under achievement of £775k. The most significant area of under achievement is the reduction in agency expenditure which was planned to deliver £1,450 and due to the Trust's very high agency spendwill not now deliver any savings this year.
Key hot spot areas are: - high cost agency spend in prisons and mental health wards - high cost and long term agency spend in medical staffing This under-achievement has been alleviated by over achievement on the pay realignment, tax efficiencies and other schemes carried forward from 2014/15
Cost Improvement Programme (CIP) YTD Threshold Current status Forecast next month
1,953
What is causing the concern? What actions have been taken to improve performance?
3.2 Area of Concern - Are we Well led?
A
0
200
400
600
800
1000
1200
Apr-15 May-15 Jun-15 Jul-15 Aug-15
CIP performance against the plan
A
Page 22

In month£000
YTD£000 Trend Data
Quality
(387)
Month Performance
£000Apr-15 357May-15 172Jun-15 469Jul-15 166Aug-15 (387)Sep-15Oct-15Nov-15Dec-15 JC/EY/SOJan-16Feb-16Mar-16
778
Expected date to be within threshold
Revised date to meet target
Review
Lead Director
Year to Date Trend Analysis Forecast
There has been an in month surplus against Trust's financial budget in August of £207k, reducing the YTD deficit to £1,678k. However, £900k of this relates to the planned deficit YTD. The key unplanned operational adverse variances within the remaining £778k are listed below. These are offset by underspends elsewhere, mainly within other pay areas:
1. Prison Services Pay - £917kThere is an ongoing issue within Offender Health Services due to long term sickness and recruitment and retention problems, resulting in high agency usage. There are currently 25 nursing vacancies in both Dorset and Devon. Additionally, we are short 2 whole time equivalent (WTE) doctors in Dorset and 1 WTE in Devon.
2. Mental Health Inpatient Wards Pay - £533kThere has been high bank and agency usage on mental health wards. There has been above average sickness in some areas and extra shifts rostered for high patient acuity. The recent pay budget realignment, adjusting ward cover levels to a standard 23% across the Trust has also uncovered higher levels of staff expenditure than expected, which is being investigated.
3. Out of Area Placements - £472kAcute Mental Health Inpatient Services have seen a high number of patients being admitted under sections of the MHA, breaching the Trust's available bed capacity, resulting in out of area placements.
The graph below reflects the unplanned adverse variance position, net of the planned deficit.
1. Prison healthcare has an extensive workforce development strategy which has been supported with project management resource to tackle the recruitment and retention issues. Task and Finish groups are in place in Dorset and Devon to focus on recruiting and retaining staff. This covers both medical and nursing staff. Actions include: Guys Marsh replacing GP initially by 1 day in October and if successful by 2 days with a nurse prescriber; Band 5 staff vacancies converted in Guys Marsh and Portland to Band 4s who have almost completed additional skills training; Band 4 programme being rolled out to the Verne. Further discussions taking place with a GP in North Dorset who has expressed interest in a post. Devon prison new rosters successfully implemented in Dartmoor and Channings Wood, projecting to bring monthly spend back into budget in October.
2. An additional control of a second approval function has been set for all ward rosters to ensure a consistent and effective approach to manage the inpatient staff resource. Ward managers will still be able to make necessary staffing changes to respond to short term sickness absence. Also, an e-roster workshop was held for all acute inpatient and rehabilitation staff on 18/08/15 to share information and build confidence and skill on the e-roster system. Any additional staffing requirements must have reasons clearly identified and the approval of the service manager.
3. Previously reported cost mitigation actions remain in place to reduce Out of Area mental health admissions. These are now starting to have a positive impact, with the current month number of patient placements remaining steady at 7.
Increasing doubt of achievement
Income and Expenditure Performance 2015/16 Threshold£000
Current status Forecast next month
900
What is causing the underperformance? What actions have been taken to improve performance?
Overspend against budget (EXCLUDING PLANNED DEFICIT)
3.3 Area of Concern - Are we Well Led?
H
-400
-300
-200
-100
0
100
200
300
400
500
600
Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Jan-16 Feb-16 Mar-16
£ 00
0s
Adve
rse/
(Fav
oura
ble)
Overspend against budget (excluding planned deficit)
Page 23

In month YTD£000 £000
14-40.686
During the month, the medical staffing pay budget is over spent by £14k, which has resulted in a year to date over spend of £69k. There is a substantial worsening of the position to arrive at a year end over spend of £981k. This is mainly due to the agency budget of £612k having run out this month. Please note that the above figures only relate to the centralised mental health medical staffing budgets. Many of the issues affecting mental health, however, also apply to other medical staffing budgets. The issues are as follows: Lack of a formal budget structureThe budgets were split and devolved to individual services so there was no central oversight of the whole medical staffing budgetary performance. Consultant over establishmentThere has been a historical failure to match recruitment with budget. High locum spendWhilst locums have been necessary to cover sickness, the majority are used to cover the significant number of vacancies at consultant and trainee level. These vacancies have arisen for a number of reasons:
- there is a national shortage of psychiatric trainees- our banding supplement paid to trainees for the rota intensity is low at 20%; pay is important to trainees rather than the number of hours they work- our geography makes recruitment difficult.
1. The Medical Director now has budgetary responsibility for the mental health budgets and meets with Human Resources and Finance to discuss the financial position as well as all medical vacancies, recruitment and locums across the Trust. 2. Whilst this is not an ideal situation, these posts are key to service delivery and in future no recruitment will take place without finance approval. 3. Every locum has, and is being, reviewed to see if locum cover is necessary; if the post can be covered at a different grade or by a non medic; and, if the locum can be split across two posts. 4. The banding supplement is being reviewed with the possibility of paying a higher rate but for increased hours. 5. The intention is to fill some vacancies with nurse practitioners or GP sessions which are less expensive options. 6. Recruitment of trainees from abroad is being explored and initial steps to progress this are underway.
7. The consultant recruitment process has been streamlined so that no Royal College approval is required before the post goes to the interview panel. 8. Salaries are being offered higher up the scale to secure appointments. 9. Job descriptions have been improved so they are accurate and the recruitment process has been made more user friendly. 10. A culture is being developed so that all medical staff are aware of the financial position. 11. The aforementioned run parallel with the nursing staff developments. 12. All local trainees are being contacted and offered a meeting with our Medical Director to discuss their career opportunities. Our high quality locums are being offered the chance to apply for substantive posts.
Medical Staffing Pay Expenditure
What is causing the underperformance? What actions have been taken to improve performance?
Overspend against budget 69
3.4 Area of Concern - Are we Well Led?
Page 24
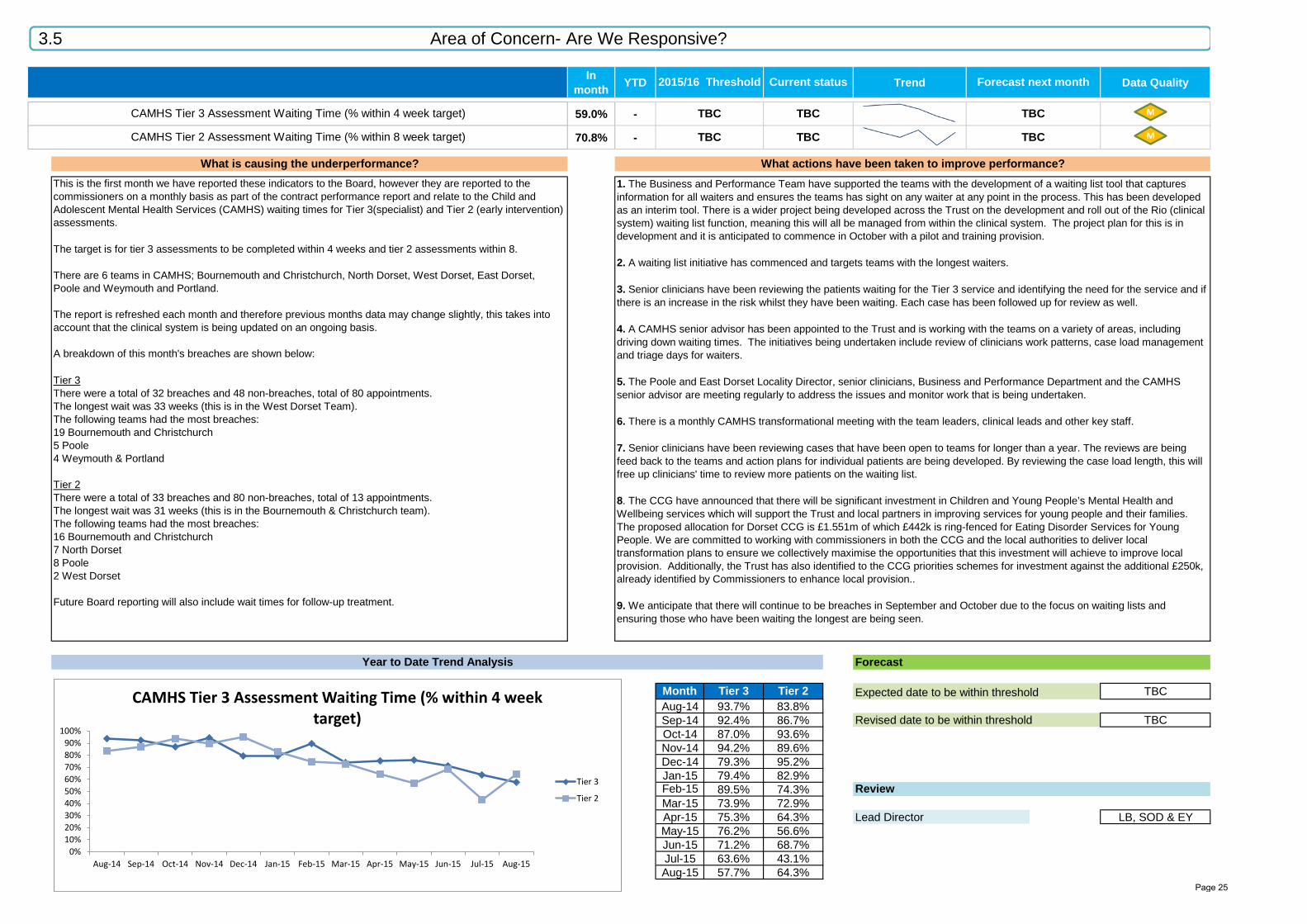
In month YTD Trend Data Quality
59.0% -
70.8% -
Forecast
Month Tier 3 Tier 2 TBCAug-14 93.7% 83.8%Sep-14 92.4% 86.7% TBCOct-14 87.0% 93.6%Nov-14 94.2% 89.6%Dec-14 79.3% 95.2%Jan-15 79.4% 82.9%Feb-15 89.5% 74.3% ReviewMar-15 73.9% 72.9%Apr-15 75.3% 64.3% Lead Director LB, SOD & EYMay-15 76.2% 56.6%Jun-15 71.2% 68.7%Jul-15 63.6% 43.1%Aug-15 57.7% 64.3%
Forecast next month
TBC TBC TBC
2015/16 Threshold Current status
Revised date to be within threshold
What actions have been taken to improve performance?
Expected date to be within threshold
TBC
Year to Date Trend Analysis
This is the first month we have reported these indicators to the Board, however they are reported to the commissioners on a monthly basis as part of the contract performance report and relate to the Child and Adolescent Mental Health Services (CAMHS) waiting times for Tier 3(specialist) and Tier 2 (early intervention) assessments. The target is for tier 3 assessments to be completed within 4 weeks and tier 2 assessments within 8.
There are 6 teams in CAMHS; Bournemouth and Christchurch, North Dorset, West Dorset, East Dorset, Poole and Weymouth and Portland.
The report is refreshed each month and therefore previous months data may change slightly, this takes into account that the clinical system is being updated on an ongoing basis.
A breakdown of this month's breaches are shown below:
Tier 3There were a total of 32 breaches and 48 non-breaches, total of 80 appointments. The longest wait was 33 weeks (this is in the West Dorset Team).The following teams had the most breaches:19 Bournemouth and Christchurch5 Poole4 Weymouth & Portland
Tier 2There were a total of 33 breaches and 80 non-breaches, total of 13 appointments. The longest wait was 31 weeks (this is in the Bournemouth & Christchurch team).The following teams had the most breaches:16 Bournemouth and Christchurch7 North Dorset 8 Poole2 West Dorset
Future Board reporting will also include wait times for follow-up treatment.
1. The Business and Performance Team have supported the teams with the development of a waiting list tool that captures information for all waiters and ensures the teams has sight on any waiter at any point in the process. This has been developed as an interim tool. There is a wider project being developed across the Trust on the development and roll out of the Rio (clinical system) waiting list function, meaning this will all be managed from within the clinical system. The project plan for this is in development and it is anticipated to commence in October with a pilot and training provision.
2. A waiting list initiative has commenced and targets teams with the longest waiters.
3. Senior clinicians have been reviewing the patients waiting for the Tier 3 service and identifying the need for the service and if there is an increase in the risk whilst they have been waiting. Each case has been followed up for review as well.
4. A CAMHS senior advisor has been appointed to the Trust and is working with the teams on a variety of areas, including driving down waiting times. The initiatives being undertaken include review of clinicians work patterns, case load management and triage days for waiters.
5. The Poole and East Dorset Locality Director, senior clinicians, Business and Performance Department and the CAMHS senior advisor are meeting regularly to address the issues and monitor work that is being undertaken.
6. There is a monthly CAMHS transformational meeting with the team leaders, clinical leads and other key staff.
7. Senior clinicians have been reviewing cases that have been open to teams for longer than a year. The reviews are being feed back to the teams and action plans for individual patients are being developed. By reviewing the case load length, this will free up clinicians' time to review more patients on the waiting list.
8. The CCG have announced that there will be significant investment in Children and Young People’s Mental Health and Wellbeing services which will support the Trust and local partners in improving services for young people and their families. The proposed allocation for Dorset CCG is £1.551m of which £442k is ring-fenced for Eating Disorder Services for Young People. We are committed to working with commissioners in both the CCG and the local authorities to deliver local transformation plans to ensure we collectively maximise the opportunities that this investment will achieve to improve local provision. Additionally, the Trust has also identified to the CCG priorities schemes for investment against the additional £250k, already identified by Commissioners to enhance local provision..
9. We anticipate that there will continue to be breaches in September and October due to the focus on waiting lists and ensuring those who have been waiting the longest are being seen.
CAMHS Tier 3 Assessment Waiting Time (% within 4 week target)
What is causing the underperformance?
TBCCAMHS Tier 2 Assessment Waiting Time (% within 8 week target) TBC
0%10%20%30%40%50%60%70%80%90%
100%
Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
CAMHS Tier 3 Assessment Waiting Time (% within 4 week target)
Tier 3
Tier 2
3.5 Area of Concern- Are We Responsive?
M
M
Page 25

Tarrant Ward at Blandford Community Hospital has passed the Gold Standards Framework (GSF) Community Hospitals Accreditation. This means the ward will be awarded the GSF Quality Hallmark Award in End of Life Care. The staff involved will be presented with the award at a celebratory conference on Friday 25th September 2015 in London.
Fewer than 20 community hospitals have been accredited to date and Blandford Community Hospital is the first in Dorset to be accredited. The report states:
you are trailblazers in this area and we at the GSF Centre are really delighted and proud of your achievements.
The GSF is a Quality Improvement Programme involving training, evaluation and quality assessment. The GSF Accreditation process involves cumulative ratings against a number of key areas.
Accreditations are independently validated and the findings are presented to an independent panel that includes representation from the Community Hospital Association and Age UK Experts by Experience.
The GSF Centre keeps a record of accredited community hospitals on their database accessible to NHS Choices and the public, and also informs the Care Quality Commission.
The GSF Community Hospital Quality Hallmark Award lasts for the next 3 years, with annual appraisals and re-accreditation in 2018.
1. The framework aims to put patients at the heart of their care, enabling people to be proactive in planning their own care and sharing their wishes with people caring for them.
2. Good care planning can help to reduce unnecessary and unwanted hospital admissions and enable people to die with dignity in the place of their choice, such as their own home, or the Community Hospital.
3. The programme has helped staff to be more confident in assisting patients who are reaching the end of their life, and provide high quality care and treatment that meets the wishes of their patient.
4. More hospitals in the Trust are undertaking the programme and staff from Blandford Community Hospital will be on hand to share their experience and best practice with colleagues.
5. As more Community Hospitals become accredited the Trust will improve its ability to provide high quality end of life care to patients across the county, enhancing our reputation to become better every day.
What is driving the success? What are the contributory factors? What lessons can be shared and how is this planned?
Does people's care, treatment and support achieve good outcomes, promote a good quality of life and is based on the best available evidence?Tarrant Ward, Blandford Community Hospital - National Gold Standards Framework in End of Life Care
4.2 Areas of Good Practice: Are we Effective?
Page 26
Patient Feedback is essential to drive improvements to services. It enables the teams to see where their patients feel they did well, and focus on areas where they could develop their skills. Through Trust reporting, it has been identified that the number of responses to patient surveys has been very low, particularly within inpatient mental health services.
A project was undertaken to understand the issues relating to gathering feedback. Information was collated from ward staff to produce an action plan to increase uptake of the surveys. Staff reported a number of factors affecting the surveys, including:- staff thought that the survey results were not used after submission, or reported on- staff often struggled with the collection of feedback during the discharge procedure- technical issues with the electronic devices/uncertainty in how to upload surveys- problems with the alternative paper survey - use of different, non-standard surveys.
After gathering this information from the wards, the team worked with the Patient Experience Team at Sentinel House to look at the procedure for gathering patient feedback, and created a flowchart which shows the feedback process, including what happens to feedback after submission.
This confirmed that both electronic or paper copies of the feedback surveys are acceptable ensuring that the majority of patients are able to complete their feedback.
Questions relating to the electronic devices were addressed with the manufacturer, Elephant, who provided feedback and support to staff and new revised paper surveys were provided by the Patient Experience Team.
It is anticipated that this will result in an increase in the number of surveys completed, which will be demonstrated in future months reporting.
Dissemination of informationAn article has been written for the Trust's internal newsletter Quality Matters outlining the project, findings, action taken to promote the gathering of patient feedback. This includes a flowchart.
Simplifying processesBy carrying out this review of the patient feedback process, it is hoped that it will make collecting patient feedback much easier and straightforward for the wards.
Promote participationThe project has raised awareness of the importance of feedback, and hopefully changed the view that it is not seen or discussed by senior managers. Ward and team managers should begin to recognise feedback as a crucial part of service improvement, and encourage their teams to treat it as a priority.
Ongoing monitoringThe project team will continue to review the number of surveys received to monitor success of the project and dissemination of information.
What is driving the success? What are the contributory factors? What lessons can be shared and how is this planned?
Are services organised so that they meet people's needs?Project to highlight the importance of patient feedback to staff within mental health services
4.2 Areas of Good Practice: Are we Responsive?
Page 27

26 | Page
Current reporting month
Latest Quarter
Indicator No. Indicator Name
Weighting Target Aug-14 Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 April - June 2015
1 Clostridium Difficile - meeting the Clostridium Difficile objective 1.0 0 (above contract) 1 0 0 0 0 1 0 0 1 1 3 3 1 5
2 MRSA - meeting the MRSA objective 1.0 0 (above contract) 0 0 0 0 0 0 0 0 0 0 0 0 0 0
3 Referral to treatment waiting times within 18 weeks - admitted 1.0 > 90% 99.12% 98.02% 96.32% 93.91% 96.23% 98.47% 92.39% 91.89% 90.91% 93.10% 99.11% 90.15% 90.32% 94.77%
4 Referral to treatment waiting times within 18 weeks - non admitted 1.0 > 95% 100.00% 99.13% 98.02% 99.17% 98.92% 98.22% 98.98% 99.47% 98.79% 99.38% 100.00% 98.60% 99.39% 99.63%
5 Referral to treatment waiting times within 18 weeks - Incomplete Pathway 1.0 > 92% 98.72% 98.73% 98.68% 99.22% 98.86% 98.14% 98.12% 98.03% 98.13% 99.63% 97.59% 97.66% 97.61% 98.45%
6 A&E - % of patients waiting less than 4 hours 1.0 > 95% 99.95% 99.85% 99.94% 99.93% 99.93% 99.94% 100.00% 100.00% 100.00% 99.92% 99.98% 98.98% 99.95% 99.97%
7 Individuals on enhanced CPA receiving follow up within 7 days > 95% 96.36% 95.87% 98.25% 96.70% 98.95% 95.65% 98.06% 97.25% 95.58% 96.23% 95.82% 96.76% 96.60% 95.82%
8 Individuals on enhanced CPA having formal review within 12 months > 95% 95.6% 96.4% 96.0% 96.0% 95.9% 95.7% 97.3% 97.3% 97.9% 95.2% 95.7% 95.1% 95.5% 95.7%
9 Delayed discharges per annum 1.0 < 7.5% 14.0% 12.18% 13.80% 13.03% 9.22% 9.26% 8.86% 8.17% 5.01% 5.55% 5.23% 5.24% 5.44% 5.27%
10 Inpatient access to crisis resolution home treatment services 1.0 > 95% 98.86% 97.85% 100.00% 100.00% 96.39% 98.67% 98.73% 100.00% 96.15% 97.26% 97.18% 97.37% 98.75% 96.85%
11 New psychosis cases seen (taken on) by early intervention teams 1.0 > 95% 87.5% 95.7% 100.0% 94.2% 102.63% 105.00% 96.77% 103.00% 275.00% 136.36% 100.00% 81.8% 85.0% 100.0%
12 Data completeness: identifiers 1.0 > 97% 99.6% 99.6% 99.6% 99.6% 99.6% 99.6% 99.6% 99.7% 99.7% 99.7% 99.7% 99.7% 99.6% 99.7%
13 Access to healthcare for people with a learning disability 1.0 Compliance against 6 criteria 6 6 6 6 6 6 6 6 6 6 6 6 6 6
14 Data completeness: outcomes 1.0 > 50% 64.7% 51.1% 51.0% 51.2% 52.3% 54.3% 53.9% 54.8% 54.0% 54.1% 54.8% 54.3% 55.3% 54.3%
Data completeness: Community Services - RTT Information 92% 93% 92.87% 91.89% 91.80% 91.58% 92.10% 92.19% 92.78% 92.31% 92.04% 90.92% 92.60% 92.04%
Data completeness: Community Services - Referral Information 98% 95% 95.05% 91.45% 92.03% 95.89% 94.38% 93.97% 94.69% 96.06% 94.56% 97.28% 98.05% 94.56%
Data completeness: Community Services - Treatment Activity Information 91% 89% 87.91% 85.01% 85.63% 89.10% 86.05% 86.35% 85.47% 89.85% 87.29% 91.58% 91.93% 87.29%
16 Early intervention in Psychosis - care package within two weeks of referral 1.0 > 50% 88.88% 86.67% 83.47%
IAPT - common mental health problems treated within 6 weeks of referral 1.0 >75% 93.3% 92.9% 91.9% 92.5% 89..9%
IAPT - common mental health problems treated within 18 weeks of referral 1.0 >95% 99.9% 100% 99.9% 100.0% 99.9%
* Please note that the data reflects reports provided by our Patient Management System supplier (Mayden) based on guidance from HSCIC. Mayden are testing replica reports from HSCIC to allow up to date reporting to be completed by the service
17*
15 1.0 > 50%
Jun-15
TRUST POSITION
1.0
Month 5 - August 2015
5.1 Board Dashboard Monitor Indicators
Page 28
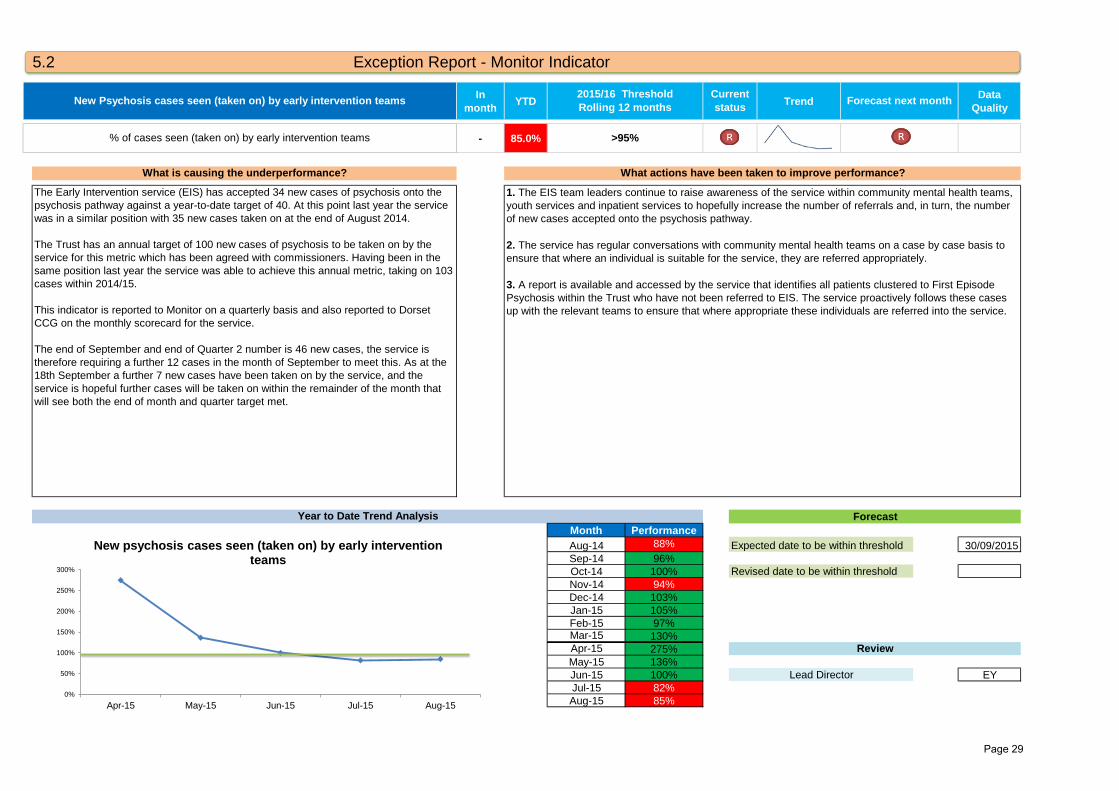
In month YTD Trend Data
Quality
- 85.0%
Month PerformanceAug-14 88% 30/09/2015Sep-14 96%Oct-14 100%Nov-14 94%Dec-14 103%Jan-15 105%Feb-15 97%Mar-15 130%Apr-15 275%May-15 136%Jun-15 100% EYJul-15 82%Aug-15 85%
Lead Director
1. The EIS team leaders continue to raise awareness of the service within community mental health teams, youth services and inpatient services to hopefully increase the number of referrals and, in turn, the number of new cases accepted onto the psychosis pathway.
2. The service has regular conversations with community mental health teams on a case by case basis to ensure that where an individual is suitable for the service, they are referred appropriately.
3. A report is available and accessed by the service that identifies all patients clustered to First Episode Psychosis within the Trust who have not been referred to EIS. The service proactively follows these cases up with the relevant teams to ensure that where appropriate these individuals are referred into the service.
Year to Date Trend Analysis Forecast
Expected date to be within threshold
Revised date to be within threshold
Review
The Early Intervention service (EIS) has accepted 34 new cases of psychosis onto the psychosis pathway against a year-to-date target of 40. At this point last year the service was in a similar position with 35 new cases taken on at the end of August 2014.
The Trust has an annual target of 100 new cases of psychosis to be taken on by the service for this metric which has been agreed with commissioners. Having been in the same position last year the service was able to achieve this annual metric, taking on 103 cases within 2014/15.
This indicator is reported to Monitor on a quarterly basis and also reported to Dorset CCG on the monthly scorecard for the service.
The end of September and end of Quarter 2 number is 46 new cases, the service is therefore requiring a further 12 cases in the month of September to meet this. As at the 18th September a further 7 new cases have been taken on by the service, and the service is hopeful further cases will be taken on within the remainder of the month that will see both the end of month and quarter target met.
New Psychosis cases seen (taken on) by early intervention teams 2015/16 ThresholdRolling 12 months
Current status Forecast next month
>95%
What is causing the underperformance? What actions have been taken to improve performance?
% of cases seen (taken on) by early intervention teams
5.2 Exception Report - Monitor Indicator
0%
50%
100%
150%
200%
250%
300%
Apr-15 May-15 Jun-15 Jul-15 Aug-15
New psychosis cases seen (taken on) by early intervention teams
Page 29
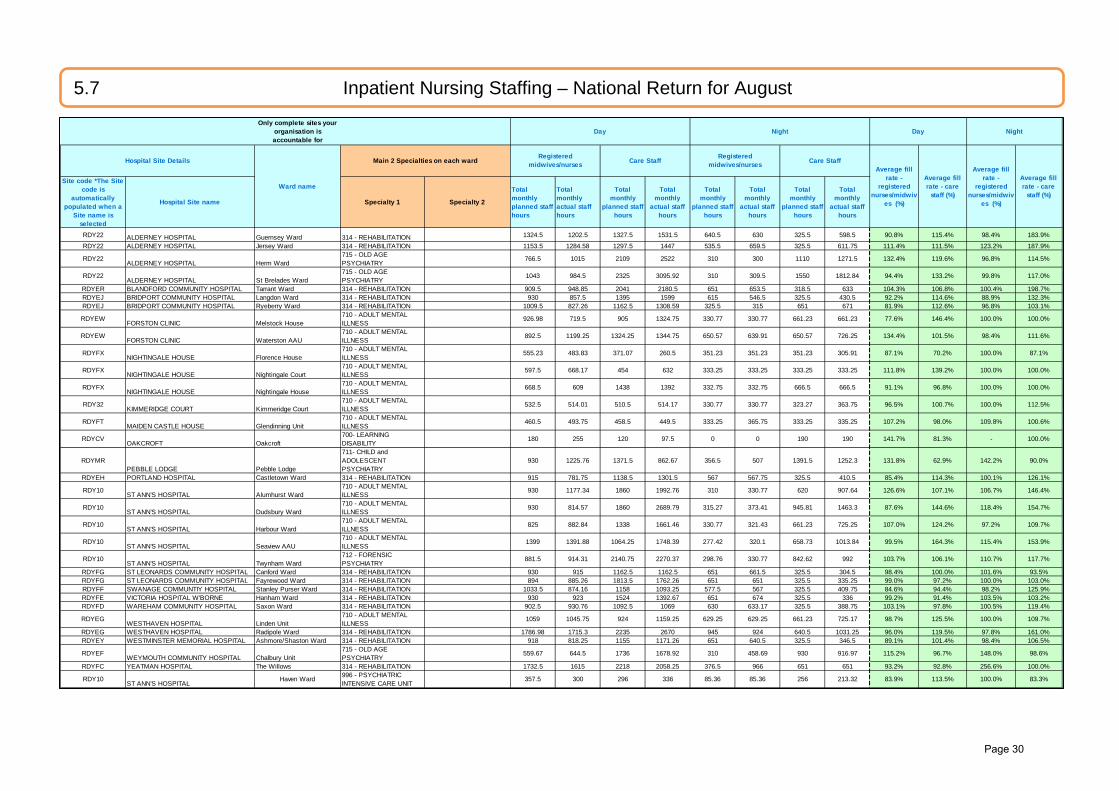
Only complete sites your organisation is accountable for
Site code *The Site code is
automatically populated when a
Site name is selected
Hospital Site name Specialty 1 Specialty 2
Total monthly planned staff hours
Total monthly actual staff hours
Total monthly
planned staff hours
Total monthly
actual staff hours
Total monthly
planned staff hours
Total monthly
actual staff hours
Total monthly
planned staff hours
Total monthly
actual staff hours
RDY22 ALDERNEY HOSPITAL Guernsey Ward 314 - REHABILITATION 1324.5 1202.5 1327.5 1531.5 640.5 630 325.5 598.5 90.8% 115.4% 98.4% 183.9%
RDY22 ALDERNEY HOSPITAL Jersey Ward 314 - REHABILITATION 1153.5 1284.58 1297.5 1447 535.5 659.5 325.5 611.75 111.4% 111.5% 123.2% 187.9%
RDY22ALDERNEY HOSPITAL Herm Ward
715 - OLD AGE PSYCHIATRY
766.5 1015 2109 2522 310 300 1110 1271.5 132.4% 119.6% 96.8% 114.5%
RDY22ALDERNEY HOSPITAL St Brelades Ward
715 - OLD AGE PSYCHIATRY
1043 984.5 2325 3095.92 310 309.5 1550 1812.84 94.4% 133.2% 99.8% 117.0%
RDYER BLANDFORD COMMUNITY HOSPITAL Tarrant Ward 314 - REHABILITATION 909.5 948.85 2041 2180.5 651 653.5 318.5 633 104.3% 106.8% 100.4% 198.7%RDYEJ BRIDPORT COMMUNITY HOSPITAL Langdon Ward 314 - REHABILITATION 930 857.5 1395 1599 615 546.5 325.5 430.5 92.2% 114.6% 88.9% 132.3%RDYEJ BRIDPORT COMMUNITY HOSPITAL Ryeberry Ward 314 - REHABILITATION 1009.5 827.26 1162.5 1308.59 325.5 315 651 671 81.9% 112.6% 96.8% 103.1%
RDYEWFORSTON CLINIC Melstock House
710 - ADULT MENTAL ILLNESS
926.98 719.5 905 1324.75 330.77 330.77 661.23 661.23 77.6% 146.4% 100.0% 100.0%
RDYEWFORSTON CLINIC Waterston AAU
710 - ADULT MENTAL ILLNESS
892.5 1199.25 1324.25 1344.75 650.57 639.91 650.57 726.25 134.4% 101.5% 98.4% 111.6%
RDYFXNIGHTINGALE HOUSE Florence House
710 - ADULT MENTAL ILLNESS
555.23 483.83 371.07 260.5 351.23 351.23 351.23 305.91 87.1% 70.2% 100.0% 87.1%
RDYFXNIGHTINGALE HOUSE Nightingale Court
710 - ADULT MENTAL ILLNESS
597.5 668.17 454 632 333.25 333.25 333.25 333.25 111.8% 139.2% 100.0% 100.0%
RDYFXNIGHTINGALE HOUSE Nightingale House
710 - ADULT MENTAL ILLNESS
668.5 609 1438 1392 332.75 332.75 666.5 666.5 91.1% 96.8% 100.0% 100.0%
RDY32KIMMERIDGE COURT Kimmeridge Court
710 - ADULT MENTAL ILLNESS
532.5 514.01 510.5 514.17 330.77 330.77 323.27 363.75 96.5% 100.7% 100.0% 112.5%
RDYFTMAIDEN CASTLE HOUSE Glendinning Unit
710 - ADULT MENTAL ILLNESS
460.5 493.75 458.5 449.5 333.25 365.75 333.25 335.25 107.2% 98.0% 109.8% 100.6%
RDYCVOAKCROFT Oakcroft
700- LEARNING DISABILITY
180 255 120 97.5 0 0 190 190 141.7% 81.3% - 100.0%
RDYMRPEBBLE LODGE Pebble Lodge
711- CHILD and ADOLESCENT PSYCHIATRY
930 1225.76 1371.5 862.67 356.5 507 1391.5 1252.3 131.8% 62.9% 142.2% 90.0%
RDYEH PORTLAND HOSPITAL Castletown Ward 314 - REHABILITATION 915 781.75 1138.5 1301.5 567 567.75 325.5 410.5 85.4% 114.3% 100.1% 126.1%
RDY10ST ANN'S HOSPITAL Alumhurst Ward
710 - ADULT MENTAL ILLNESS
930 1177.34 1860 1992.76 310 330.77 620 907.64 126.6% 107.1% 106.7% 146.4%
RDY10ST ANN'S HOSPITAL Dudsbury Ward
710 - ADULT MENTAL ILLNESS
930 814.57 1860 2689.79 315.27 373.41 945.81 1463.3 87.6% 144.6% 118.4% 154.7%
RDY10ST ANN'S HOSPITAL Harbour Ward
710 - ADULT MENTAL ILLNESS
825 882.84 1338 1661.46 330.77 321.43 661.23 725.25 107.0% 124.2% 97.2% 109.7%
RDY10ST ANN'S HOSPITAL Seaview AAU
710 - ADULT MENTAL ILLNESS
1399 1391.88 1064.25 1748.39 277.42 320.1 658.73 1013.84 99.5% 164.3% 115.4% 153.9%
RDY10ST ANN'S HOSPITAL Twynham Ward
712 - FORENSIC PSYCHIATRY
881.5 914.31 2140.75 2270.37 298.76 330.77 842.62 992 103.7% 106.1% 110.7% 117.7%
RDYFG ST LEONARDS COMMUNITY HOSPITAL Canford Ward 314 - REHABILITATION 930 915 1162.5 1162.5 651 661.5 325.5 304.5 98.4% 100.0% 101.6% 93.5%RDYFG ST LEONARDS COMMUNITY HOSPITAL Fayrewood Ward 314 - REHABILITATION 894 885.26 1813.5 1762.26 651 651 325.5 335.25 99.0% 97.2% 100.0% 103.0%RDYFF SWANAGE COMMUNTIY HOSPITAL Stanley Purser Ward 314 - REHABILITATION 1033.5 874.16 1158 1093.25 577.5 567 325.5 409.75 84.6% 94.4% 98.2% 125.9%RDYFE VICTORIA HOSPITAL W'BORNE Hanham Ward 314 - REHABILITATION 930 923 1524 1392.67 651 674 325.5 336 99.2% 91.4% 103.5% 103.2%RDYFD WAREHAM COMMUNITY HOSPITAL Saxon Ward 314 - REHABILITATION 902.5 930.76 1092.5 1069 630 633.17 325.5 388.75 103.1% 97.8% 100.5% 119.4%
RDYEGWESTHAVEN HOSPITAL Linden Unit
710 - ADULT MENTAL ILLNESS
1059 1045.75 924 1159.25 629.25 629.25 661.23 725.17 98.7% 125.5% 100.0% 109.7%
RDYEG WESTHAVEN HOSPITAL Radipole Ward 314 - REHABILITATION 1786.98 1715.3 2235 2670 945 924 640.5 1031.25 96.0% 119.5% 97.8% 161.0%RDYEY WESTMINSTER MEMORIAL HOSPITAL Ashmore/Shaston Ward 314 - REHABILITATION 918 818.25 1155 1171.26 651 640.5 325.5 346.5 89.1% 101.4% 98.4% 106.5%
RDYEFWEYMOUTH COMMUNITY HOSPITAL Chalbury Unit
715 - OLD AGE PSYCHIATRY
559.67 644.5 1736 1678.92 310 458.69 930 916.97 115.2% 96.7% 148.0% 98.6%
RDYFC YEATMAN HOSPITAL The Willows 314 - REHABILITATION 1732.5 1615 2218 2058.25 376.5 966 651 651 93.2% 92.8% 256.6% 100.0%
RDY10ST ANN'S HOSPITAL
Haven Ward 996 - PSYCHIATRIC INTENSIVE CARE UNIT
357.5 300 296 336 85.36 85.36 256 213.32 83.9% 113.5% 100.0% 83.3%
Day Night
Average fill rate - care
staff (%)
Average fill rate -
registered nurses/midwiv
es (%)
Average fill rate - care
staff (%)
Average fill rate -
registered nurses/midwiv
es (%)
Day
Care StaffMain 2 Specialties on each ward
Night
Hospital Site Details
Ward name
Registered midwives/nurses
Registered midwives/nursesCare Staff
5.7 Inpatient Nursing Staffing – National Return for August
Page 30
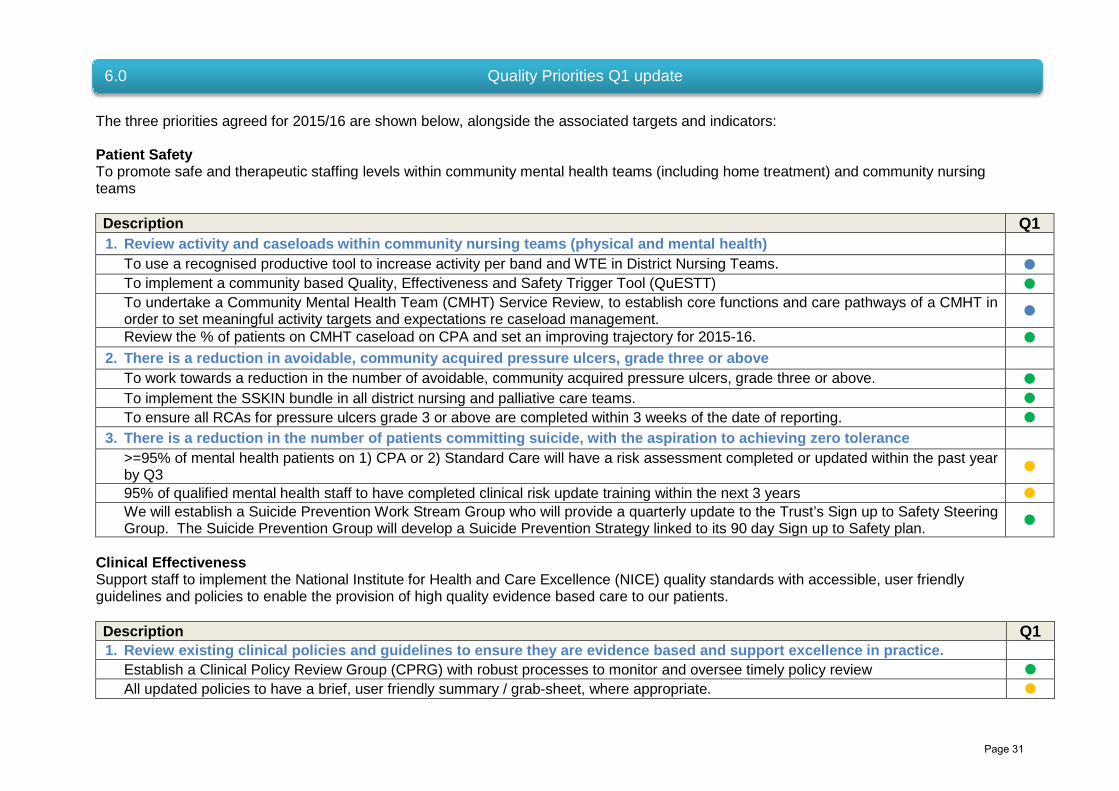
The three priorities agreed for 2015/16 are shown below, alongside the associated targets and indicators: Patient Safety To promote safe and therapeutic staffing levels within community mental health teams (including home treatment) and community nursing teams Description Q1 1. Review activity and caseloads within community nursing teams (physical and mental health)
To use a recognised productive tool to increase activity per band and WTE in District Nursing Teams. To implement a community based Quality, Effectiveness and Safety Trigger Tool (QuESTT) To undertake a Community Mental Health Team (CMHT) Service Review, to establish core functions and care pathways of a CMHT in order to set meaningful activity targets and expectations re caseload management. Review the % of patients on CMHT caseload on CPA and set an improving trajectory for 2015-16.
2. There is a reduction in avoidable, community acquired pressure ulcers, grade three or above To work towards a reduction in the number of avoidable, community acquired pressure ulcers, grade three or above. To implement the SSKIN bundle in all district nursing and palliative care teams. To ensure all RCAs for pressure ulcers grade 3 or above are completed within 3 weeks of the date of reporting.
3. There is a reduction in the number of patients committing suicide, with the aspiration to achieving zero tolerance >=95% of mental health patients on 1) CPA or 2) Standard Care will have a risk assessment completed or updated within the past year by Q3 95% of qualified mental health staff to have completed clinical risk update training within the next 3 years We will establish a Suicide Prevention Work Stream Group who will provide a quarterly update to the Trust’s Sign up to Safety Steering Group. The Suicide Prevention Group will develop a Suicide Prevention Strategy linked to its 90 day Sign up to Safety plan.
Clinical Effectiveness Support staff to implement the National Institute for Health and Care Excellence (NICE) quality standards with accessible, user friendly guidelines and policies to enable the provision of high quality evidence based care to our patients. Description Q1 1. Review existing clinical policies and guidelines to ensure they are evidence based and support excellence in practice.
Establish a Clinical Policy Review Group (CPRG) with robust processes to monitor and oversee timely policy review All updated policies to have a brief, user friendly summary / grab-sheet, where appropriate.
6.0 Quality Priorities Q1 update
Page 31

Description Q1 The Trust’s NICE assurance group will ensure all new NICE guidance and Quality Standards are aligned to relevant clinical guidance / policy.
2. Local clinical audits will be aligned to NICE guidance. All local audit notification forms to be screened to ensure aligned to NICE guidelines, where appropriate. Implement Ulysses database for recording of local clinical audits with ability to link audit standards to NICE guidelines.
3. All actions arising from NICE guidance and quality standard baseline assessments will be implemented within the agreed timescales. NICE group to assure robust action plans to achieve compliance which will help support staff to implement guidance in clinical practice and improve patient care.
Patient Experience Lessons learned from the findings from local investigations and reviews will be shared beyond the team involved to improve the experience of our patients Description Q1 1. Introduction of innovative methods and new ways of sharing learning
Introduce a new programme of learning events in which learning from serious incidents will be shared. Introduce a suite of videos to enable front line staff to share learning from incidents occurring within their service across the Trust.
2. All teams across the organisation will be aware of and learn from lessons that have arisen outside of their own service Lessons learned and common trends arising from complaints will be shared with team managers and staff by the Patient Experience and Customer Services team. Staff attending learning events will benefit from learning lessons that have occurred outside of their own service and understand how this learning can be applied to their own role. To develop the Trust Complaints Review Group; an open forum which considers complaints, reviews learning and shares this across the Trust.
3. Evidence of changes in practice as a result of lessons learned Evidence of service improvements as a direct outcome of learning from complaints. Evidence of service improvements as a direct outcome of learning from the Friends and Family Test (FFT).
The Trust has made good progress against the quality priorities selected for 2015/16, however, it is evident that there ongoing work required to achieve a successful outcome against these challenging quality priorities and associated indicators.
Page 32
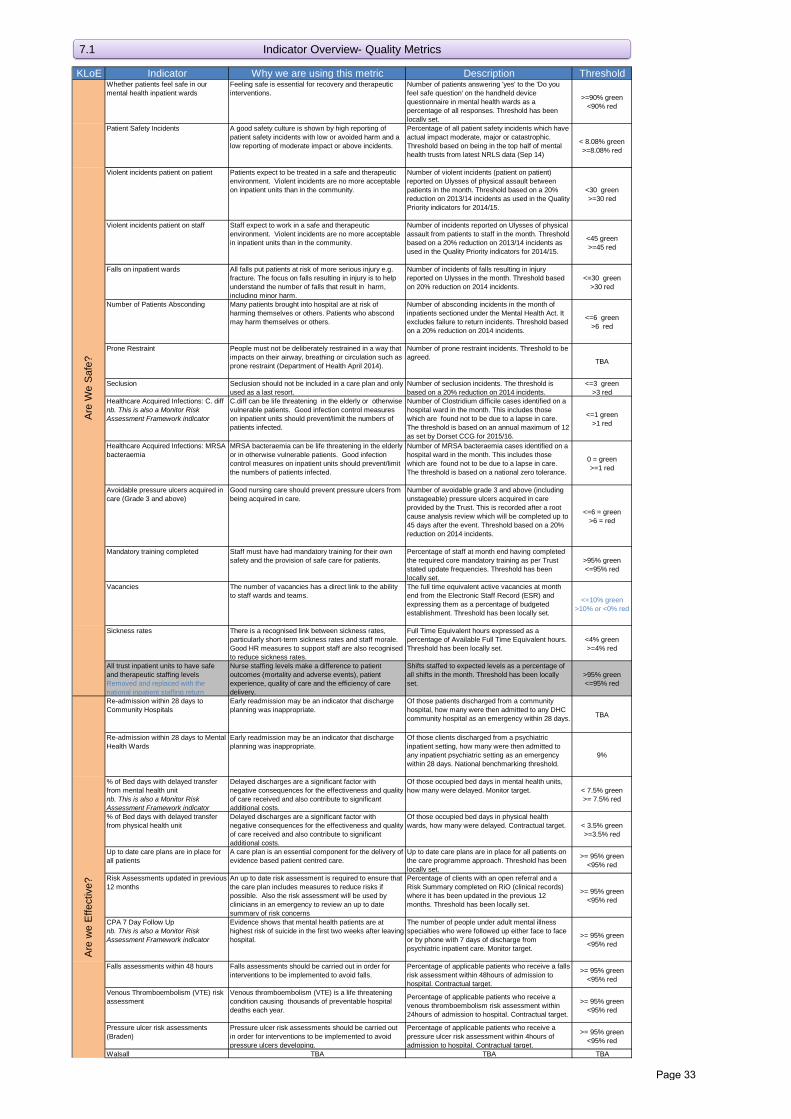
KLoE Indicator Why we are using this metric Description ThresholdWhether patients feel safe in our mental health inpatient wards
Feeling safe is essential for recovery and therapeutic interventions.
Number of patients answering 'yes' to the 'Do you feel safe question' on the handheld device questionnaire in mental health wards as a percentage of all responses. Threshold has been locally set.
>=90% green<90% red
Patient Safety Incidents A good safety culture is shown by high reporting of patient safety incidents with low or avoided harm and a low reporting of moderate impact or above incidents.
Percentage of all patient safety incidents which have actual impact moderate, major or catastrophic. Threshold based on being in the top half of mental health trusts from latest NRLS data (Sep 14)
< 8.08% green>=8.08% red
Violent incidents patient on patient Patients expect to be treated in a safe and therapeutic environment. Violent incidents are no more acceptable on inpatient units than in the community.
Number of violent incidents (patient on patient) reported on Ulysses of physical assault between patients in the month. Threshold based on a 20% reduction on 2013/14 incidents as used in the Quality Priority indicators for 2014/15.
<30 green>=30 red
Violent incidents patient on staff Staff expect to work in a safe and therapeutic environment. Violent incidents are no more acceptable in inpatient units than in the community.
Number of incidents reported on Ulysses of physical assault from patients to staff in the month. Threshold based on a 20% reduction on 2013/14 incidents as used in the Quality Priority indicators for 2014/15.
<45 green>=45 red
Falls on inpatient wards All falls put patients at risk of more serious injury e.g. fracture. The focus on falls resulting in injury is to help understand the number of falls that result in harm, including minor harm.
Number of incidents of falls resulting in injury reported on Ulysses in the month. Threshold based on 20% reduction on 2014 incidents.
<=30 green>30 red
Number of Patients Absconding Many patients brought into hospital are at risk of harming themselves or others. Patients who abscond may harm themselves or others.
Number of absconding incidents in the month of inpatients sectioned under the Mental Health Act. It excludes failure to return incidents. Threshold based on a 20% reduction on 2014 incidents.
<=6 green>6 red
Prone Restraint People must not be deliberately restrained in a way that impacts on their airway, breathing or circulation such as prone restraint (Department of Health April 2014).
Number of prone restraint incidents. Threshold to be agreed. TBA
Seclusion Seclusion should not be included in a care plan and only used as a last resort.
Number of seclusion incidents. The threshold is based on a 20% reduction on 2014 incidents.
<=3 green>3 red
Healthcare Acquired Infections: C. diff nb. This is also a Monitor Risk Assessment Framework indicator
C.diff can be life threatening in the elderly or otherwise vulnerable patients. Good infection control measures on inpatient units should prevent/limit the numbers of patients infected.
Number of Clostridium difficile cases identified on a hospital ward in the month. This includes those which are found not to be due to a lapse in care. The threshold is based on an annual maximum of 12 as set by Dorset CCG for 2015/16.
<=1 green>1 red
Healthcare Acquired Infections: MRSA bacteraemia
MRSA bacteraemia can be life threatening in the elderly or in otherwise vulnerable patients. Good infection control measures on inpatient units should prevent/limit the numbers of patients infected.
Number of MRSA bacteraemia cases identified on a hospital ward in the month. This includes those which are found not to be due to a lapse in care. The threshold is based on a national zero tolerance.
0 = green>=1 red
Avoidable pressure ulcers acquired in care (Grade 3 and above)
Good nursing care should prevent pressure ulcers from being acquired in care.
Number of avoidable grade 3 and above (including unstageable) pressure ulcers acquired in care provided by the Trust. This is recorded after a root cause analysis review which will be completed up to 45 days after the event. Threshold based on a 20% reduction on 2014 incidents.
<=6 = green>6 = red
Mandatory training completed Staff must have had mandatory training for their own safety and the provision of safe care for patients.
Percentage of staff at month end having completed the required core mandatory training as per Trust stated update frequencies. Threshold has been locally set.
>95% green<=95% red
Vacancies The number of vacancies has a direct link to the ability to staff wards and teams.
The full time equivalent active vacancies at month end from the Electronic Staff Record (ESR) and expressing them as a percentage of budgeted establishment. Threshold has been locally set.
<=10% green>10% or <0% red
Sickness rates There is a recognised link between sickness rates, particularly short-term sickness rates and staff morale. Good HR measures to support staff are also recognised to reduce sickness rates.
Full Time Equivalent hours expressed as a percentage of Available Full Time Equivalent hours. Threshold has been locally set.
<4% green>=4% red
All trust inpatient units to have safe and therapeutic staffing levelsRemoved and replaced with the national inpatient staffing return
Nurse staffing levels make a difference to patient outcomes (mortality and adverse events), patient experience, quality of care and the efficiency of care delivery.
Shifts staffed to expected levels as a percentage of all shifts in the month. Threshold has been locally set.
>95% green<=95% red
Re-admission within 28 days to Community Hospitals
Early readmission may be an indicator that discharge planning was inappropriate.
Of those patients discharged from a community hospital, how many were then admitted to any DHC community hospital as an emergency within 28 days. TBA
Re-admission within 28 days to Mental Health Wards
Early readmission may be an indicator that discharge planning was inappropriate.
Of those clients discharged from a psychiatric inpatient setting, how many were then admitted to any inpatient psychiatric setting as an emergency within 28 days. National benchmarking threshold.
9%
% of Bed days with delayed transfer from mental health unitnb. This is also a Monitor Risk Assessment Framework indicator
Delayed discharges are a significant factor with negative consequences for the effectiveness and quality of care received and also contribute to significant additional costs.
Of those occupied bed days in mental health units, how many were delayed. Monitor target. < 7.5% green
>= 7.5% red
% of Bed days with delayed transfer from physical health unit
Delayed discharges are a significant factor with negative consequences for the effectiveness and quality of care received and also contribute to significant additional costs.
Of those occupied bed days in physical health wards, how many were delayed. Contractual target. < 3.5% green
>=3.5% red
Up to date care plans are in place for all patients
A care plan is an essential component for the delivery of evidence based patient centred care.
Up to date care plans are in place for all patients on the care programme approach. Threshold has been locally set.
>= 95% green <95% red
Risk Assessments updated in previous 12 months
An up to date risk assessment is required to ensure that the care plan includes measures to reduce risks if possible. Also the risk assessment will be used by clinicians in an emergency to review an up to date summary of risk concerns
Percentage of clients with an open referral and a Risk Summary completed on RiO (clinical records) where it has been updated in the previous 12 months. Threshold has been locally set.
>= 95% green <95% red
CPA 7 Day Follow Upnb. This is also a Monitor Risk Assessment Framework indicator
Evidence shows that mental health patients are at highest risk of suicide in the first two weeks after leaving hospital.
The number of people under adult mental illness specialties who were followed up either face to face or by phone with 7 days of discharge from psychiatric inpatient care. Monitor target.
>= 95% green <95% red
Falls assessments within 48 hours Falls assessments should be carried out in order for interventions to be implemented to avoid falls.
Percentage of applicable patients who receive a falls risk assessment within 48hours of admission to hospital. Contractual target.
>= 95% green <95% red
Venous Thromboembolism (VTE) risk assessment
Venous thromboembolism (VTE) is a life threatening condition causing thousands of preventable hospital deaths each year.
Percentage of applicable patients who receive a venous thromboembolism risk assessment within 24hours of admission to hospital. Contractual target.
>= 95% green <95% red
Pressure ulcer risk assessments (Braden)
Pressure ulcer risk assessments should be carried out in order for interventions to be implemented to avoid pressure ulcers developing.
Percentage of applicable patients who receive a pressure ulcer risk assessment within 4hours of admission to hospital. Contractual target.
>= 95% green <95% red
Walsall TBA TBA TBA
Are
We
Saf
e?A
re w
e E
ffect
ive?
7.1 Indicator Overview- Quality Metrics
Page 33
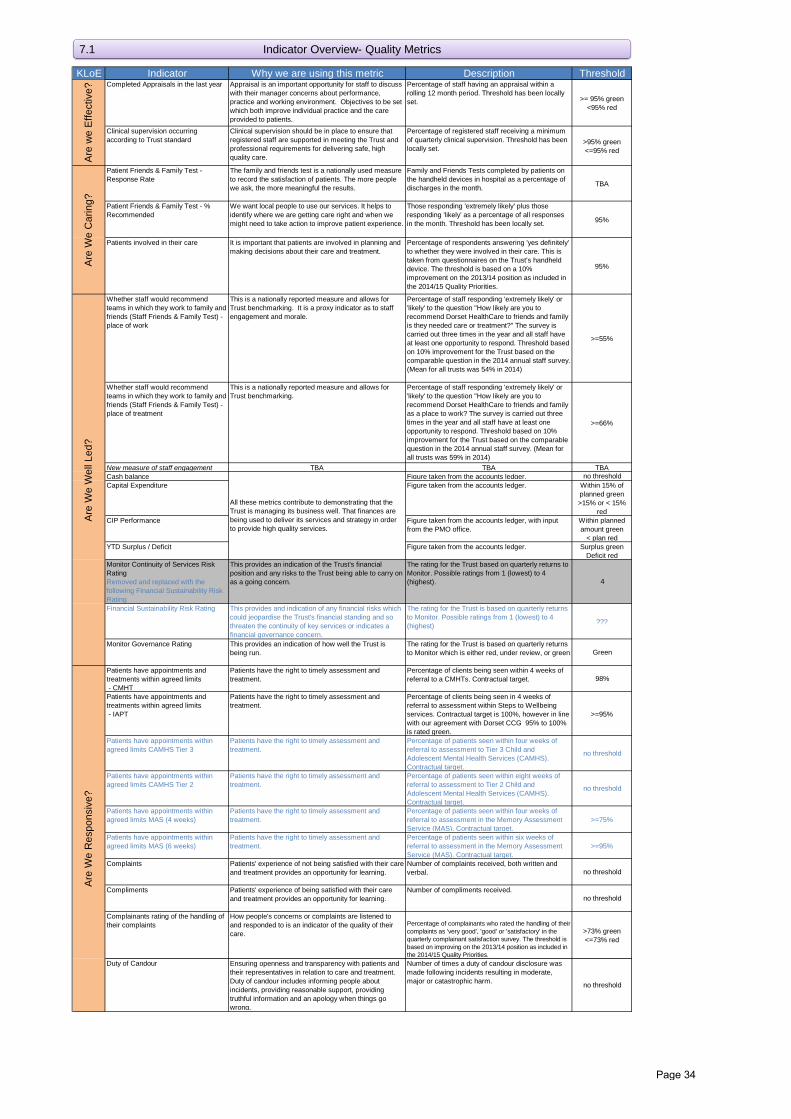
KLoE Indicator Why we are using this metric Description Threshold
7.1 Indicator Overview- Quality Metrics
Completed Appraisals in the last year Appraisal is an important opportunity for staff to discuss with their manager concerns about performance, practice and working environment. Objectives to be set which both improve individual practice and the care provided to patients.
Percentage of staff having an appraisal within a rolling 12 month period. Threshold has been locally set. >= 95% green
<95% red
Clinical supervision occurring according to Trust standard
Clinical supervision should be in place to ensure that registered staff are supported in meeting the Trust and professional requirements for delivering safe, high quality care.
Percentage of registered staff receiving a minimum of quarterly clinical supervision. Threshold has been locally set.
>95% green<=95% red
Patient Friends & Family Test - Response Rate
The family and friends test is a nationally used measure to record the satisfaction of patients. The more people we ask, the more meaningful the results.
Family and Friends Tests completed by patients on the handheld devices in hospital as a percentage of discharges in the month. TBA
Patient Friends & Family Test - % Recommended
We want local people to use our services. It helps to identify where we are getting care right and when we might need to take action to improve patient experience.
Those responding 'extremely likely' plus those responding 'likely' as a percentage of all responses in the month. Threshold has been locally set. 95%
Patients involved in their care It is important that patients are involved in planning and making decisions about their care and treatment.
Percentage of respondents answering 'yes definitely' to whether they were involved in their care. This is taken from questionnaires on the Trust’s handheld device. The threshold is based on a 10% improvement on the 2013/14 position as included in the 2014/15 Quality Priorities.
95%
Whether staff would recommend teams in which they work to family and friends (Staff Friends & Family Test) - place of work
This is a nationally reported measure and allows for Trust benchmarking. It is a proxy indicator as to staff engagement and morale.
Percentage of staff responding 'extremely likely' or 'likely' to the question "How likely are you to recommend Dorset HealthCare to friends and family is they needed care or treatment?" The survey is carried out three times in the year and all staff have at least one opportunity to respond. Threshold based on 10% improvement for the Trust based on the comparable question in the 2014 annual staff survey. (Mean for all trusts was 54% in 2014)
>=55%
Whether staff would recommend teams in which they work to family and friends (Staff Friends & Family Test) - place of treatment
This is a nationally reported measure and allows for Trust benchmarking.
Percentage of staff responding 'extremely likely' or 'likely' to the question "How likely are you to recommend Dorset HealthCare to friends and family as a place to work? The survey is carried out three times in the year and all staff have at least one opportunity to respond. Threshold based on 10% improvement for the Trust based on the comparable question in the 2014 annual staff survey. (Mean for all trusts was 59% in 2014)
>=66%
New measure of staff engagement TBA TBA TBACash balance Figure taken from the accounts ledger. no thresholdCapital Expenditure Figure taken from the accounts ledger. Within 15% of
planned green>15% or < 15%
redCIP Performance Figure taken from the accounts ledger, with input
from the PMO office.Within planned amount green
< plan redYTD Surplus / Deficit Figure taken from the accounts ledger. Surplus green
Deficit redMonitor Continuity of Services Risk RatingRemoved and replaced with the following Financial Sustainability Risk Rating
This provides an indication of the Trust's financial position and any risks to the Trust being able to carry on as a going concern.
The rating for the Trust based on quarterly returns to Monitor. Possible ratings from 1 (lowest) to 4 (highest). 4
Financial Sustainability Risk Rating This provides and indication of any financial risks which could jeopardise the Trust's financial standing and so threaten the continuity of key services or indicates a financial governance concern.
The rating for the Trust is based on quarterly returns to Monitor. Possible ratings from 1 (lowest) to 4 (highest) ???
Monitor Governance Rating This provides an indication of how well the Trust is being run.
The rating for the Trust is based on quarterly returns to Monitor which is either red, under review, or green Green
Patients have appointments and treatments within agreed limits - CMHT
Patients have the right to timely assessment and treatment.
Percentage of clients being seen within 4 weeks of referral to a CMHTs. Contractual target. 98%
Patients have appointments and treatments within agreed limits - IAPT
Patients have the right to timely assessment and treatment.
Percentage of clients being seen in 4 weeks of referral to assessment within Steps to Wellbeing services. Contractual target is 100%, however in line with our agreement with Dorset CCG 95% to 100% is rated green.
>=95%
Patients have appointments within agreed limits CAMHS Tier 3
Patients have the right to timely assessment and treatment.
Percentage of patients seen within four weeks of referral to assessment to Tier 3 Child and Adolescent Mental Health Services (CAMHS). Contractual target.
no threshold
Patients have appointments within agreed limits CAMHS Tier 2
Patients have the right to timely assessment and treatment.
Percentage of patients seen within eight weeks of referral to assessment to Tier 2 Child and Adolescent Mental Health Services (CAMHS). Contractual target.
no threshold
Patients have appointments within agreed limits MAS (4 weeks)
Patients have the right to timely assessment and treatment.
Percentage of patients seen within four weeks of referral to assessment in the Memory Assessment Service (MAS). Contractual target.
>=75%
Patients have appointments within agreed limits MAS (6 weeks)
Patients have the right to timely assessment and treatment.
Percentage of patients seen within six weeks of referral to assessment in the Memory Assessment Service (MAS). Contractual target.
>=95%
Complaints Patients' experience of not being satisfied with their care and treatment provides an opportunity for learning.
Number of complaints received, both written and verbal. no threshold
Compliments Patients' experience of being satisfied with their care and treatment provides an opportunity for learning.
Number of compliments received.no threshold
Complainants rating of the handling of their complaints
How people's concerns or complaints are listened to and responded to is an indicator of the quality of their care.
Percentage of complainants who rated the handling of their complaints as 'very good', 'good' or 'satisfactory' in the quarterly complainant satisfaction survey. The threshold is based on improving on the 2013/14 position as included in the 2014/15 Quality Priorities.
>73% green<=73% red
Duty of Candour Ensuring openness and transparency with patients and their representatives in relation to care and treatment. Duty of candour includes informing people about incidents, providing reasonable support, providing truthful information and an apology when things go wrong.
Number of times a duty of candour disclosure was made following incidents resulting in moderate, major or catastrophic harm. no threshold
Are
We
Res
pons
ive?
Are
We
Car
ing?
All these metrics contribute to demonstrating that the Trust is managing its business well. That finances are being used to deliver its services and strategy in order to provide high quality services.
Are
we
Effe
ctiv
e?A
re W
e W
ell L
ed?
Page 34
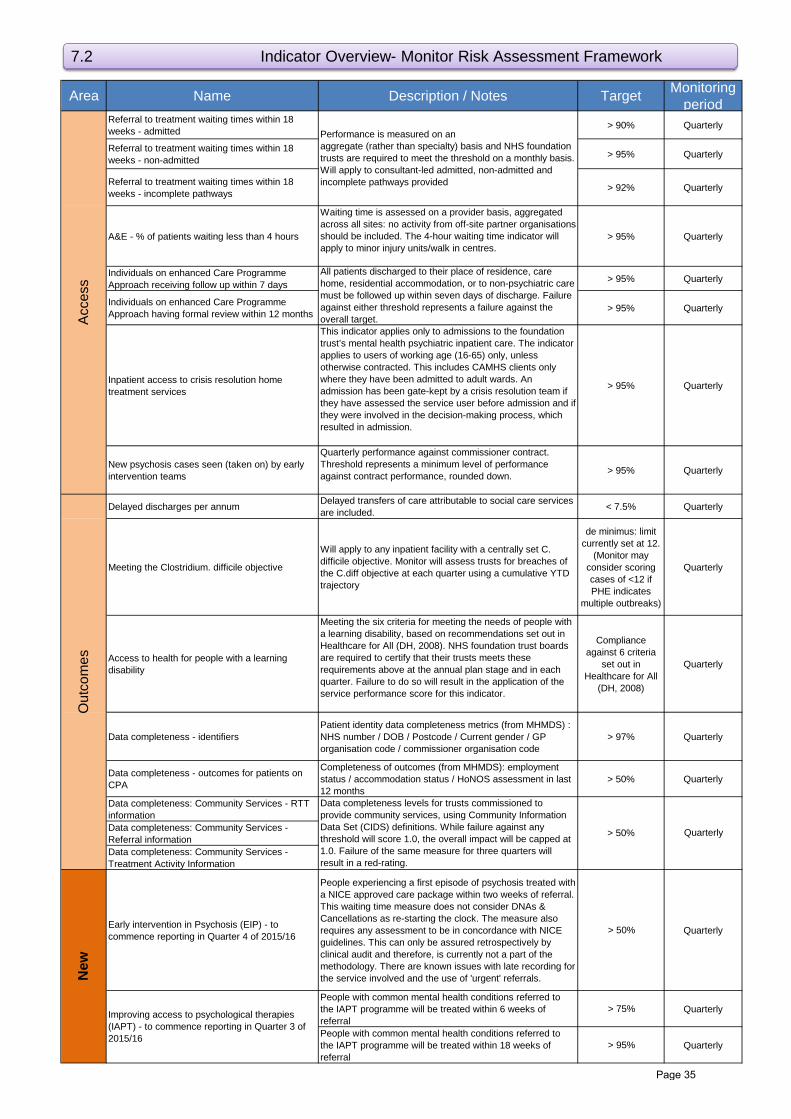
Area Name Description / Notes Target Monitoring period
Referral to treatment waiting times within 18 weeks - admitted > 90% Quarterly
Referral to treatment waiting times within 18 weeks - non-admitted > 95% Quarterly
Referral to treatment waiting times within 18 weeks - incomplete pathways > 92% Quarterly
A&E - % of patients waiting less than 4 hours
Waiting time is assessed on a provider basis, aggregated across all sites: no activity from off-site partner organisations should be included. The 4-hour waiting time indicator will apply to minor injury units/walk in centres.
> 95% Quarterly
Individuals on enhanced Care Programme Approach receiving follow up within 7 days > 95% Quarterly
Individuals on enhanced Care Programme Approach having formal review within 12 months > 95% Quarterly
Inpatient access to crisis resolution home treatment services
This indicator applies only to admissions to the foundation trust’s mental health psychiatric inpatient care. The indicator applies to users of working age (16-65) only, unless otherwise contracted. This includes CAMHS clients only where they have been admitted to adult wards. An admission has been gate-kept by a crisis resolution team if they have assessed the service user before admission and if they were involved in the decision-making process, which resulted in admission.
> 95% Quarterly
New psychosis cases seen (taken on) by early intervention teams
Quarterly performance against commissioner contract. Threshold represents a minimum level of performance against contract performance, rounded down. > 95% Quarterly
Delayed discharges per annum Delayed transfers of care attributable to social care services are included. < 7.5% Quarterly
Meeting the Clostridium. difficile objective
Will apply to any inpatient facility with a centrally set C. difficile objective. Monitor will assess trusts for breaches of the C.diff objective at each quarter using a cumulative YTD trajectory
de minimus: limit currently set at 12.
(Monitor may consider scoring cases of <12 if PHE indicates
multiple outbreaks)
Quarterly
Access to health for people with a learning disability
Meeting the six criteria for meeting the needs of people with a learning disability, based on recommendations set out in Healthcare for All (DH, 2008). NHS foundation trust boards are required to certify that their trusts meets these requirements above at the annual plan stage and in each quarter. Failure to do so will result in the application of the service performance score for this indicator.
Compliance against 6 criteria
set out in Healthcare for All
(DH, 2008)
Quarterly
Data completeness - identifiersPatient identity data completeness metrics (from MHMDS) : NHS number / DOB / Postcode / Current gender / GP organisation code / commissioner organisation code
> 97% Quarterly
Data completeness - outcomes for patients on CPA
Completeness of outcomes (from MHMDS): employment status / accommodation status / HoNOS assessment in last 12 months
> 50% Quarterly
Data completeness: Community Services - RTT informationData completeness: Community Services - Referral informationData completeness: Community Services - Treatment Activity Information
Early intervention in Psychosis (EIP) - to commence reporting in Quarter 4 of 2015/16
People experiencing a first episode of psychosis treated with a NICE approved care package within two weeks of referral. This waiting time measure does not consider DNAs & Cancellations as re-starting the clock. The measure also requires any assessment to be in concordance with NICE guidelines. This can only be assured retrospectively by clinical audit and therefore, is currently not a part of the methodology. There are known issues with late recording for the service involved and the use of 'urgent' referrals.
> 50% Quarterly
People with common mental health conditions referred to the IAPT programme will be treated within 6 weeks of referral
> 75% Quarterly
People with common mental health conditions referred to the IAPT programme will be treated within 18 weeks of referral
> 95% Quarterly
New
Improving access to psychological therapies (IAPT) - to commence reporting in Quarter 3 of 2015/16
> 50% Quarterly
Acc
ess
Out
com
es
Performance is measured on anaggregate (rather than specialty) basis and NHS foundation trusts are required to meet the threshold on a monthly basis. Will apply to consultant-led admitted, non-admitted and incomplete pathways provided
All patients discharged to their place of residence, care home, residential accommodation, or to non-psychiatric care must be followed up within seven days of discharge. Failure against either threshold represents a failure against the overall target.
Data completeness levels for trusts commissioned to provide community services, using Community Information Data Set (CIDS) definitions. While failure against any threshold will score 1.0, the overall impact will be capped at 1.0. Failure of the same measure for three quarters will result in a red-rating.
7.2 Indicator Overview- Monitor Risk Assessment Framework
Page 35
Trust Finance Report for Month 5, August 2015
Part 1 Board Meeting, 30 September 2015
Author Head of Management Accounts, Director of Finance
Sponsoring Board Member
Director of Finance
Purpose of Report To advise the Board of the financial position at Month 5, August 2015.
Recommendation The Board is asked to consider the report for August.
Engagement and Involvement
Directors and budget managers are involved in providing updates and information affecting the financial position.
Notable feedback and actions from Directorate teams with regard to their reported financial position are included within the report.
Previous Board/Committee Dates
Executive Performance and Corporate Risk Group
22 September 2015.
Monitoring and Assurance Summary
This report links to the Strategic Goals
To ensure that all of the Trust’s resources are used in an efficient and sustainable way;
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability
Information Management &Technology
Equality Impact Assessment
Freedom of Information

FINANCE REPORT FOR MONTH 5, AUGUST 2015
1. Executive Summary
1.1 The full year planned deficit is £2.2m, which reflects the importance the Trust places on investment in services. Financial performance at August was a cumulative deficit of £1.7m (1.6%), which is £0.8m (£1.2m at July) worse than plan to date.
1.2 The current year end projection is an adverse variance of £7.1m of which £2.2m is the planned deficit. This results in a forecast of £4.9m worse than plan. The financial deterioration projected is significantly due to pay and agency costs to provide services. Given the numerous actions taken and planned, there is potential to improve on this forecast but the impact of some actions are not yet clear and cannot yet be quantified.
1.3 This forecast position does not include £1.2m Contingency and £0.5m Severance
funding which is as yet unallocated. Given the scale of the deficit to resolve, the requirement to provide services safely, and high cost activity that is demand led, it is the Director of Finance’s view at this stage that the year end financial position is unlikely to be recovered without the use of the contingency and severance funding.
1.4 Whilst there is currently considerable focus on improving the forecast outturn, it is unlikely the actions planned or underway will significantly impact underlying performance for next month but it is expected that improvement will be seen from Month 7 onwards. There is concern that the Plan will not be achieved.
1.5 The key areas of the report are summarised as follows:
Metric YTD Position = Improved Performance
Summary
Budgetary Performance ↑
Summary position on budgetary performance: The key unplanned operational adverse variances driving performance at Month 5 are: 1. Prison Services Pay - £917k (£701k at July) Long term sickness and recruitment & retention problems, resulting in continued high agency usage. The workforce review for Devon has been completed, and is being implemented with a recruitment drive to match the new skill mix. Dorset’s workforce review is ongoing. The current forecast position assumes that Devon pay will return to budget during Q3 but that there will be a continuing overspend position for Dorset. Overspends incurred in advance of this point are not likely to be recovered. There are targeted actions to address agency expenditure across the Trust (see section 5.3). It is anticipated that this will reduce future pay costs but at present is not sufficiently evident to enable the financial impact to be quantified. The Dorset Locality, underspends within cost centres are being frozen and centralised to mitigate the overspend within Prisons. See also other mitigations below. 2. Out of Area Placements - £472k (£410k at July) The cost of MH Out of Area Placements remains high, though there has been no increase in patients for August. Previously reported actions continue to have a positive impact (see section 4). It is anticipated that these actions will continue to reduce future costs to the Trust but it is difficult to quantify the financial impact due
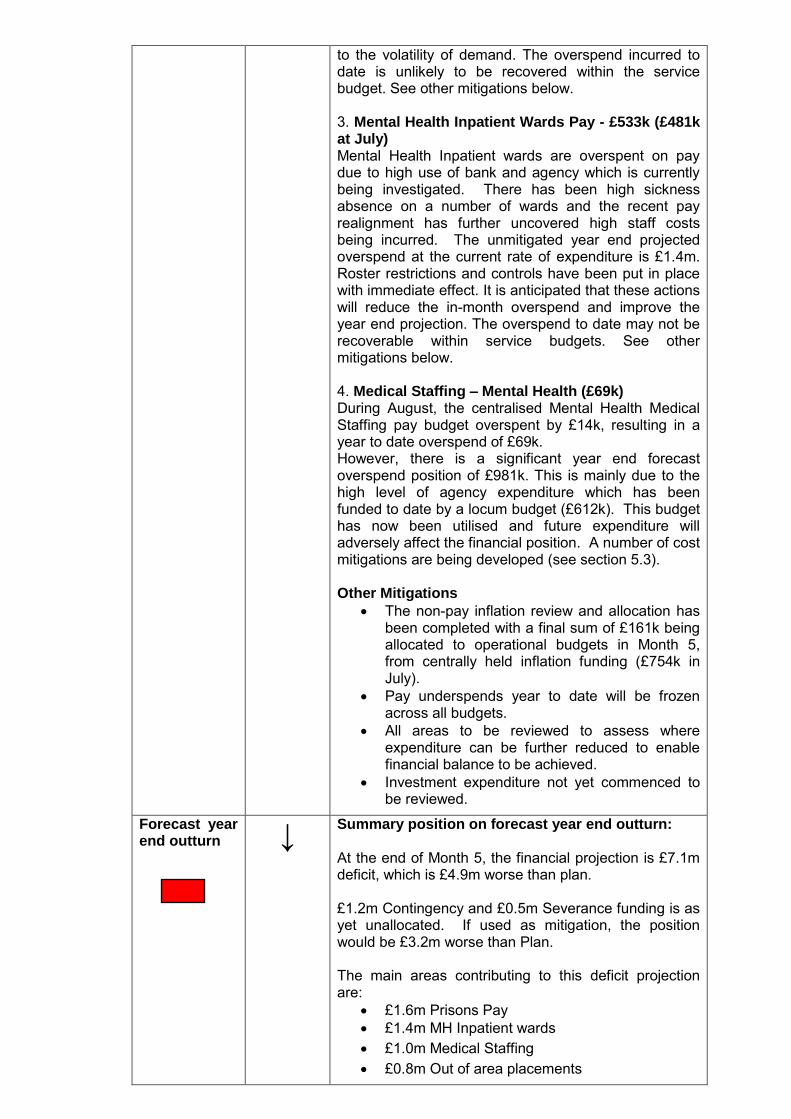
to the volatility of demand. The overspend incurred to date is unlikely to be recovered within the service budget. See other mitigations below. 3. Mental Health Inpatient Wards Pay - £533k (£481k at July) Mental Health Inpatient wards are overspent on pay due to high use of bank and agency which is currently being investigated. There has been high sickness absence on a number of wards and the recent pay realignment has further uncovered high staff costs being incurred. The unmitigated year end projected overspend at the current rate of expenditure is £1.4m. Roster restrictions and controls have been put in place with immediate effect. It is anticipated that these actions will reduce the in-month overspend and improve the year end projection. The overspend to date may not be recoverable within service budgets. See other mitigations below. 4. Medical Staffing – Mental Health (£69k) During August, the centralised Mental Health Medical Staffing pay budget overspent by £14k, resulting in a year to date overspend of £69k. However, there is a significant year end forecast overspend position of £981k. This is mainly due to the high level of agency expenditure which has been funded to date by a locum budget (£612k). This budget has now been utilised and future expenditure will adversely affect the financial position. A number of cost mitigations are being developed (see section 5.3). Other Mitigations
The non-pay inflation review and allocation has been completed with a final sum of £161k being allocated to operational budgets in Month 5, from centrally held inflation funding (£754k in July).
Pay underspends year to date will be frozen across all budgets.
All areas to be reviewed to assess where expenditure can be further reduced to enable financial balance to be achieved.
Investment expenditure not yet commenced to be reviewed.
Forecast year end outturn
↓ Summary position on forecast year end outturn: At the end of Month 5, the financial projection is £7.1m deficit, which is £4.9m worse than plan. £1.2m Contingency and £0.5m Severance funding is as yet unallocated. If used as mitigation, the position would be £3.2m worse than Plan. The main areas contributing to this deficit projection are:
£1.6m Prisons Pay
£1.4m MH Inpatient wards
£1.0m Medical Staffing
£0.8m Out of area placements
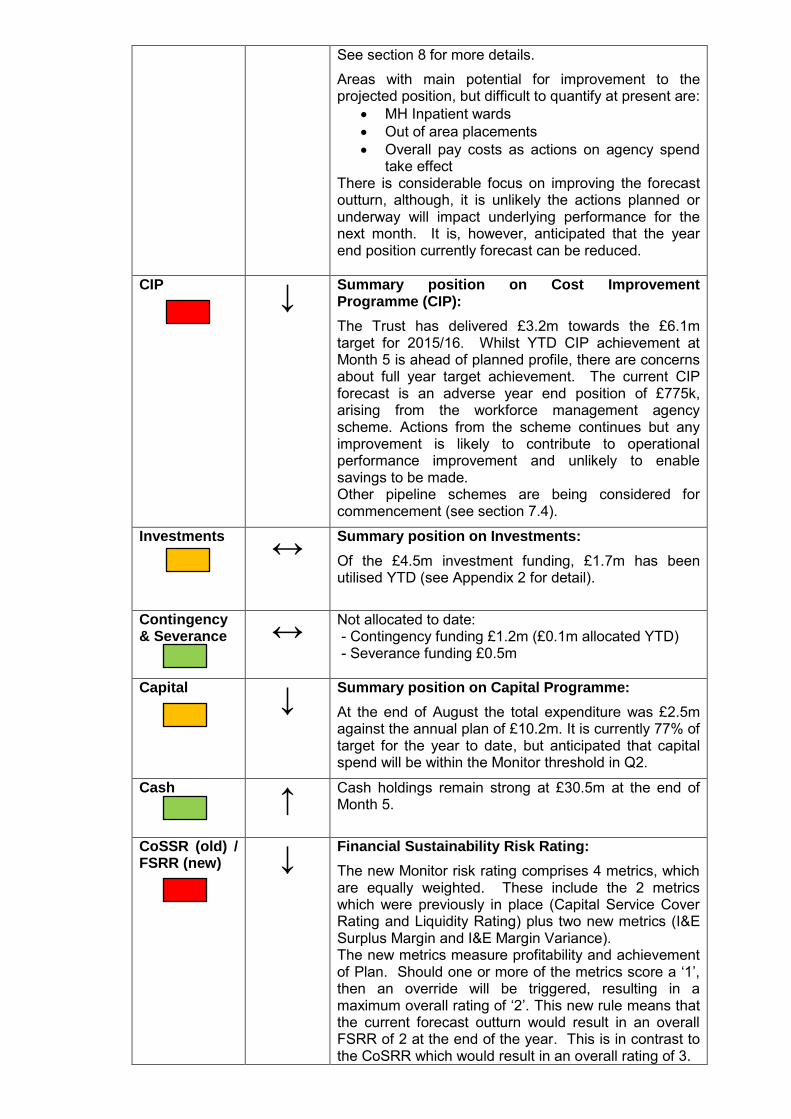
See section 8 for more details.
Areas with main potential for improvement to the projected position, but difficult to quantify at present are:
MH Inpatient wards
Out of area placements
Overall pay costs as actions on agency spend take effect
There is considerable focus on improving the forecast outturn, although, it is unlikely the actions planned or underway will impact underlying performance for the next month. It is, however, anticipated that the year end position currently forecast can be reduced.
CIP
↓
Summary position on Cost Improvement Programme (CIP):
The Trust has delivered £3.2m towards the £6.1m target for 2015/16. Whilst YTD CIP achievement at Month 5 is ahead of planned profile, there are concerns about full year target achievement. The current CIP forecast is an adverse year end position of £775k, arising from the workforce management agency scheme. Actions from the scheme continues but any improvement is likely to contribute to operational performance improvement and unlikely to enable savings to be made. Other pipeline schemes are being considered for commencement (see section 7.4).
Investments ↔
Summary position on Investments:
Of the £4.5m investment funding, £1.7m has been utilised YTD (see Appendix 2 for detail).
Contingency & Severance ↔
Not allocated to date: - Contingency funding £1.2m (£0.1m allocated YTD) - Severance funding £0.5m
Capital ↓
Summary position on Capital Programme:
At the end of August the total expenditure was £2.5m against the annual plan of £10.2m. It is currently 77% of target for the year to date, but anticipated that capital spend will be within the Monitor threshold in Q2.
Cash ↑
Cash holdings remain strong at £30.5m at the end of Month 5.
CoSSR (old) / FSRR (new)
↓ Financial Sustainability Risk Rating:
The new Monitor risk rating comprises 4 metrics, which are equally weighted. These include the 2 metrics which were previously in place (Capital Service Cover Rating and Liquidity Rating) plus two new metrics (I&E Surplus Margin and I&E Margin Variance). The new metrics measure profitability and achievement of Plan. Should one or more of the metrics score a ‘1’, then an override will be triggered, resulting in a maximum overall rating of ‘2’. This new rule means that the current forecast outturn would result in an overall FSRR of 2 at the end of the year. This is in contrast to the CoSRR which would result in an overall rating of 3.
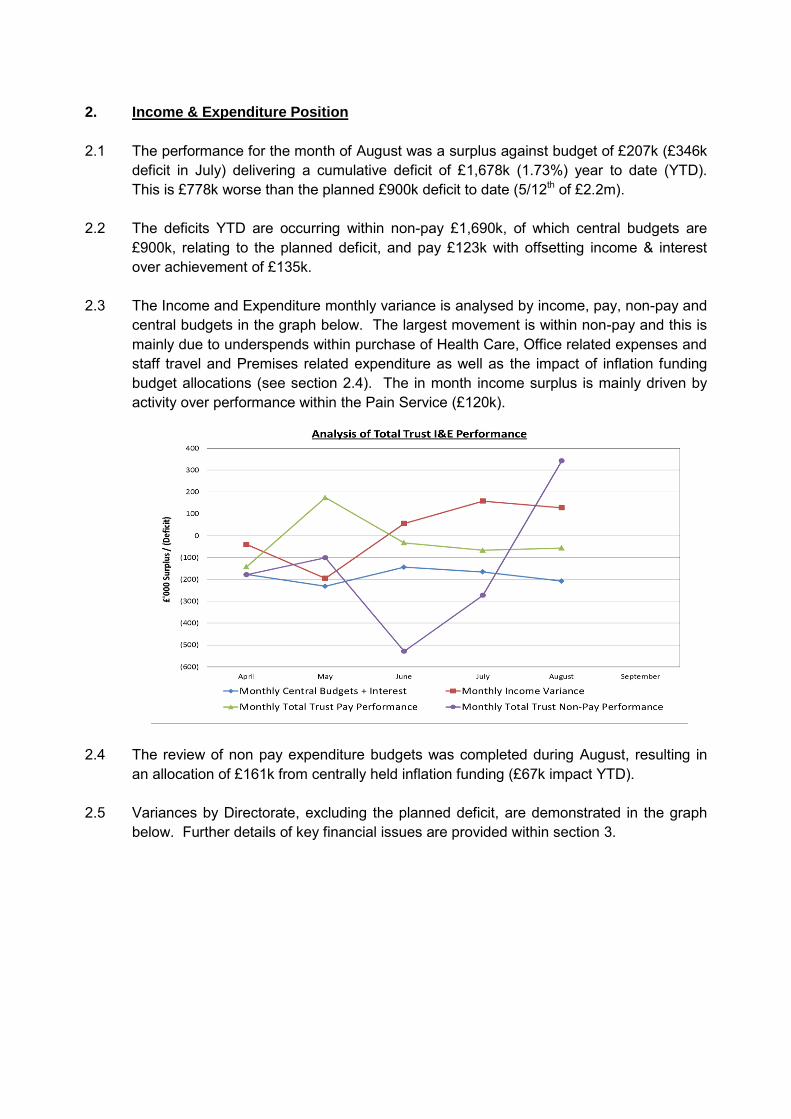
2. Income & Expenditure Position
2.1 The performance for the month of August was a surplus against budget of £207k (£346k
deficit in July) delivering a cumulative deficit of £1,678k (1.73%) year to date (YTD).
This is £778k worse than the planned £900k deficit to date (5/12th of £2.2m).
2.2 The deficits YTD are occurring within non-pay £1,690k, of which central budgets are
£900k, relating to the planned deficit, and pay £123k with offsetting income & interest
over achievement of £135k.
2.3 The Income and Expenditure monthly variance is analysed by income, pay, non-pay and
central budgets in the graph below. The largest movement is within non-pay and this is
mainly due to underspends within purchase of Health Care, Office related expenses and
staff travel and Premises related expenditure as well as the impact of inflation funding
budget allocations (see section 2.4). The in month income surplus is mainly driven by
activity over performance within the Pain Service (£120k).
2.4 The review of non pay expenditure budgets was completed during August, resulting in
an allocation of £161k from centrally held inflation funding (£67k impact YTD).
2.5 Variances by Directorate, excluding the planned deficit, are demonstrated in the graph
below. Further details of key financial issues are provided within section 3.
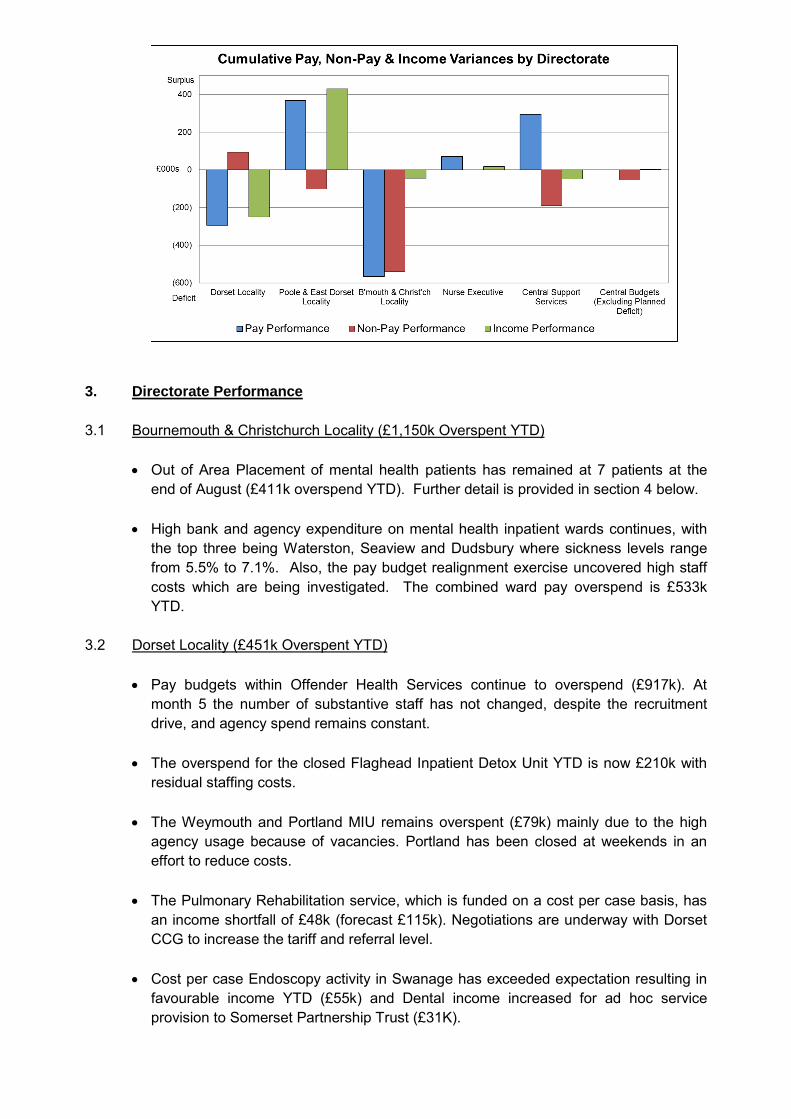
3. Directorate Performance
3.1 Bournemouth & Christchurch Locality (£1,150k Overspent YTD)
Out of Area Placement of mental health patients has remained at 7 patients at the
end of August (£411k overspend YTD). Further detail is provided in section 4 below.
High bank and agency expenditure on mental health inpatient wards continues, with
the top three being Waterston, Seaview and Dudsbury where sickness levels range
from 5.5% to 7.1%. Also, the pay budget realignment exercise uncovered high staff
costs which are being investigated. The combined ward pay overspend is £533k
YTD.
3.2 Dorset Locality (£451k Overspent YTD)
Pay budgets within Offender Health Services continue to overspend (£917k). At
month 5 the number of substantive staff has not changed, despite the recruitment
drive, and agency spend remains constant.
The overspend for the closed Flaghead Inpatient Detox Unit YTD is now £210k with
residual staffing costs.
The Weymouth and Portland MIU remains overspent (£79k) mainly due to the high
agency usage because of vacancies. Portland has been closed at weekends in an
effort to reduce costs.
The Pulmonary Rehabilitation service, which is funded on a cost per case basis, has
an income shortfall of £48k (forecast £115k). Negotiations are underway with Dorset
CCG to increase the tariff and referral level.
Cost per case Endoscopy activity in Swanage has exceeded expectation resulting in
favourable income YTD (£55k) and Dental income increased for ad hoc service
provision to Somerset Partnership Trust (£31K).

Other areas within the Locality continue to have high vacancy levels which are
contributing to a net remaining pay underspend of £671k YTD with the main element
being 2 vacant Medical posts (£104k).
3.3 Poole Locality (£700k Underspent YTD)
The Locality underspend has increased by £224k in August, mainly due to over
performance on cost per case Pain Service activity. The service undertook a data
cleansing review, which has contributed to the current month position, and the same
activity levels are not anticipated going forwards. The net service forecast is a £144k
surplus for the year.
There are still a number of vacancies driving the net YTD pay underspend (£370k).
However, the rate of underspend has dropped, as posts are being filled. The
vacancies within CAMHS medical staff continue to be covered by agency staff at an
average cost pressure of £33k per month (£163k YTD) which is anticipated to
continue until December 2015, after which time full establishment is expected to be
achieved.
The overspend on Orthotics has increased (£77k YTD) and is forecast to be £186k
overspent for the year. There is also an overspend within the Audiology service on
purchases of hearing aids (£69k YTD) with a reduced forecast position of £47k
overspent for the year.
3.4 Central Support Services (£149k Underspent YTD)
Vacancies within Estates (£223k), Finance and IM&T (£99k) and Nursing & Quality
(£72k) are the significant drivers of the favourable position. This is offset by
overspend on consultancy (£162k) (mainly driven by the Artelia strategy &
development outline business case work), and computer expenditure in IM&T (£80k
YTD, forecast £178k).
3.5 Centrally Held Funds & Interest (£926k Overspent YTD)
The adverse position within centrally held funds is being driven by 5/12th of the £2.2m
planned annual deficit (£900k).
4. Out of Area Placements
4.1 The number of patients has remained the same in August, with 6 new admissions and
discharges during the month, leaving 7 patients placed out of area at the end of the
month, of which 5 were female PICU.
4.2 Expenditure for the month is £222k (£1,271k YTD), causing an adverse variance of £62k
(£472k YTD). There was a £0.8m budget increase in 2015/16 giving a total annual
budget of £1.9m. As a comparison, expenditure in 2014/15 totalled £2.6m, generating an
overspend of £1.5m.
4.3 Patients that have been decanted from Haven Ward whilst the refurbishment works are
underway are excluded from the reported patient numbers and costs as they will be fully
funded from centrally held budget set aside during the annual planning process.

4.4 The various cost mitigations actions put in place, as previously reported, continue to
have a positive impact.
4.5 Activity is difficult to predict and subject to significant fluctuation making it very difficult to
forecast the expected cost accurately. The current forecast outturn expenditure is
£2,682k, which will result in an overspend of £765k. The inflow and outflow of patient
numbers over the past 12 months are demonstrated within the graph below.
5. Bank & Agency Expenditure
5.1 Agency expenditure in August is £1.2m (£5.9m YTD). Expenditure is £1.9m higher YTD
compared to the M5 position last year. Bank expenditure is £0.8m (£4.0m YTD) which
remains in line with expenditure to August 2014/15.
5.2 Within the YTD Agency expenditure, £3.0m relates to Nursing staff, £1.5m relates to
Medical staff and £1.4m has been spent on other staff groups.
5.3 The highest agency expenditure can be seen in:
£1,562k Offender Services – both nursing and medical staff
£1,054k Community Hospitals – nursing staff (including £277k for the
temporarily funded Canford Ward)
£1,038k Medical staff – locums
£661k IT & Information – mainly IT investment programme (£348k
budgeted) & other vacancies
£500k Mental Health Inpatient wards – nursing staff
5.4 Actions are being introduced to reduce the agency expenditure cost pressure:
A workforce development strategy has been implemented within Offender Health
Services, with Task & Finish groups in place to focus on recruitment and retention.
Responsibility for the Medical Staffing budget has transferred to the Medical Director
and various mitigation actions are being developed, such as:
- All locum cover is being scrutinised for necessity
- Employment terms and conditions are being reviewed
- The Medical recruitment process is being streamlined
- Alternative skill mix approaches are being considered
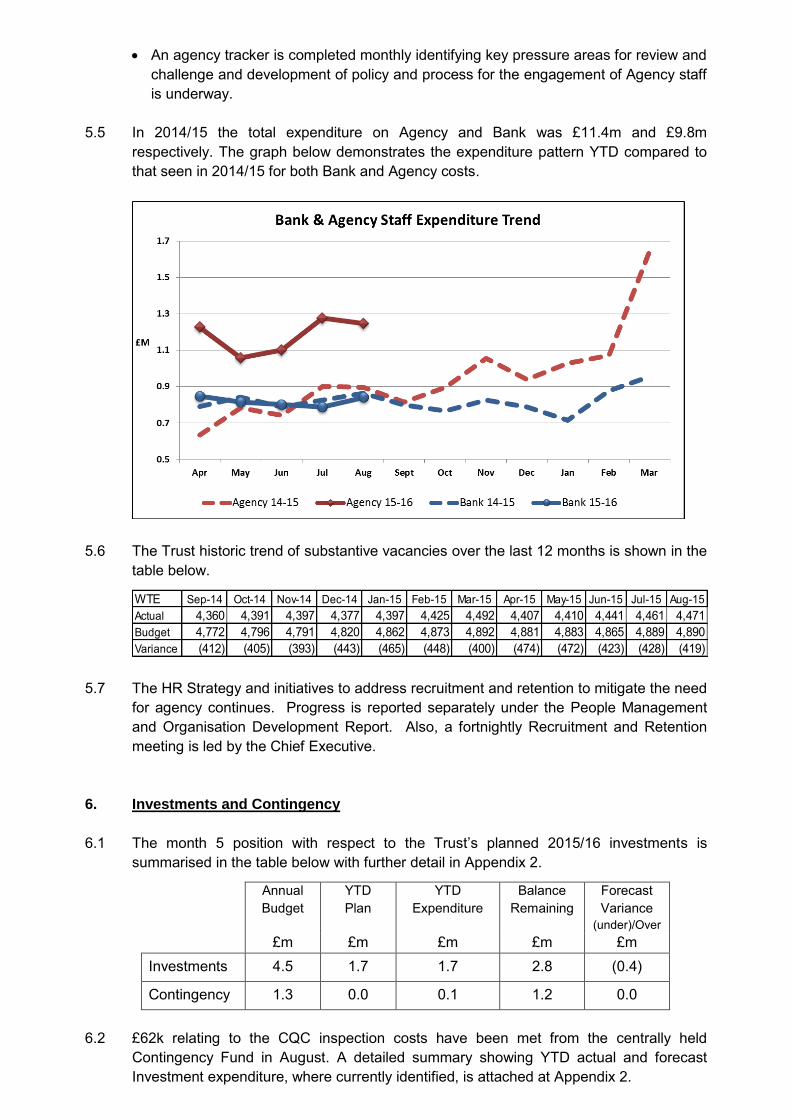
An agency tracker is completed monthly identifying key pressure areas for review and
challenge and development of policy and process for the engagement of Agency staff
is underway.
5.5 In 2014/15 the total expenditure on Agency and Bank was £11.4m and £9.8m
respectively. The graph below demonstrates the expenditure pattern YTD compared to
that seen in 2014/15 for both Bank and Agency costs.
5.6 The Trust historic trend of substantive vacancies over the last 12 months is shown in the
table below.
5.7 The HR Strategy and initiatives to address recruitment and retention to mitigate the need
for agency continues. Progress is reported separately under the People Management
and Organisation Development Report. Also, a fortnightly Recruitment and Retention
meeting is led by the Chief Executive.
6. Investments and Contingency
6.1 The month 5 position with respect to the Trust’s planned 2015/16 investments is
summarised in the table below with further detail in Appendix 2.
Annual
Budget
YTD
Plan
YTD
Expenditure
Balance
Remaining
Forecast
Variance
(under)/Over
£m £m £m £m £m
Investments 4.5 1.7 1.7 2.8 (0.4)
Contingency 1.3 0.0 0.1 1.2 0.0
6.2 £62k relating to the CQC inspection costs have been met from the centrally held
Contingency Fund in August. A detailed summary showing YTD actual and forecast
Investment expenditure, where currently identified, is attached at Appendix 2.
WTE Sep-14 Oct-14 Nov-14 Dec-14 Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15
Actual 4,360 4,391 4,397 4,377 4,397 4,425 4,492 4,407 4,410 4,441 4,461 4,471
Budget 4,772 4,796 4,791 4,820 4,862 4,873 4,892 4,881 4,883 4,865 4,889 4,890
Variance (412) (405) (393) (443) (465) (448) (400) (474) (472) (423) (428) (419)

6.3 The current forecast is an underspend of £408k mainly arising within IT investment
projects.
7. Cost Improvement Programme (CIP)
7.1 Savings totalling £956k was identified during Month 5 (£3,160k YTD). The annual target
is £6.1m. A summary of actual and forecast performance against CIP schemes in
2015/16 is set out at Appendix 3.
7.2 Pay budgets have now been realigned in line with the new budget policy. It is currently
estimated that a further £260k will be released as CIP. Non pay budgets have been
reviewed and inflation funding has been allocated from centrally held funds, with the
remaining balance of £427k being released as CIP.
7.3 Whilst YTD CIP achievement is ahead of the planned profile to Month 5, there are
concerns with regard to meeting the full year target of £6.1m. The current CIP forecast
is an adverse year end position of £775k (£281k at July), mainly due to anticipated non-
achievement of the Workforce Management Agency scheme (£1,450k). Whilst actions
relating to this scheme are vigorously pursued, it is anticipated that any improvement will
contribute to operational performance and unlikely to yield savings.
7.4 There are a number of pipeline schemes being developed, such as:
A skill mix review and realignment across various areas, such as a review of the
potential for introducing Nurse Consultants in place of doctors within Psychiatric Care.
Identify and withdraw from rented premises to reduce rental burdens.
Improved telecoms expense management.
8. Year End Projection
8.1 The year end projection at Month 5 is an adverse variance of £7,111k (£6,034k at Month
4), including the planned deficit of £2,160k. Key drivers are shown in the graph below.

8.2 The significant variances are listed below, most of which are detailed within other
sections of the report.
(Under)
Over
£000
Planned Outturn 2,160
Prisons Pay 1,555
MH Inpatient Wards Pay 1,352
Medical Staffing Pay 1,012
Other Pay net Vacancies (1,819)
IT Investment Slippage (408)
CIP Scheme Slippage 775
Out of Area Placements 765
NHS Property Transfer 346
Flaghead Unit Loss 273
NCA Income 162
Software, Licences & Maint 178
Orthotics Service 186
Estates contractors 140
Pulmonary Rehab Income 115
Other Misc 317
Month 5 Forecast Outturn 7,111
8.3 Items not specifically reported elsewhere are highlighted below:
Within Medical Staffing pay there is over establishment within the Consultant grade
and significant use of Agency to cover vacancies across all grades. The Trust holds
a budget for cover which is utilised as required and will be fully allocated during
Month 6, resulting in the forecast year end overspend position.
The NCA income shortfall (£162k) is due to reduced activity levels. This is a demand
led area and difficult to predict.
There is a forecast overspend for contractors within Estates which is driven by
substantive vacancies.
8.4 Within centrally held funding a favourable underspend of £0.5m is forecast against the
Pay Inflation reserve due to currently retained budget. Once the final outcome of the
recent pay budget realignment process is agreed by Directors, this budget will either be
moved to operational budget lines or offset against CIP. However, this will reallocate the
budget, not improve the Trust’s forecast outturn.
9. Risk
9.1 Within Offender Health Services there is a worsening Pay overspend of £917k as at
August. Whilst actions are being taken, the position is not likely to be back within budget
by year end. The risk is that permanent appointments are delayed and continued use of
agency is required. There remains the potential for significant cost pressure in this area.
9.2 Out of Area Placements relating to mental health patients has been an ongoing cost
pressure for the past two years. The overspend to Month 5, despite a significant budget
increase of £0.8m in 2015/16, is a cause for concern. Although costs are reducing as a

result of mitigating actions, this remains a significant financial risk to the Trust due to the
unpredictable and volatile nature of the service demand.
9.3 Although ahead of plan as at Month 5, the Cost Improvement Programme (CIP) target of
£6.1m for 2015/16 continues to be highlighted as a risk due to the size and number of
schemes and the current adverse CIP forecast of £775k. Progress is monitored via the
Project Management Office and a detailed monthly report is provided to Directors
separately.
9.4 The centralised Mental Health Medical Staffing pay budget is overspent by £69k YTD.
However, there is a significant year end forecast overspend position of £981k. This is
mainly due to the high level of agency expenditure which has been covered to date by a
locum budget (£612k). This budget has now been utilised and future spends will worsen
the financial position. A number of cost mitigations are being developed but this area
remains a risk to the Trust.
10. Capital
10.1 The St Ann’s facilities upgrade of Twynham, Dudsbury and Haven wards continues.
Haven ward was completed on 21st August in line with schedule, Dudsbury ward and lift
works are still in progress. The final area to start is the ECT, which is currently out to
tender. The final completion date is still planned as 18th December 2015, however the
project team continue to find further asbestos which is increasing the costs and causing
delays. The delays incurred are being made up elsewhere by the contractors.
Anticipated 2015/16 costs are now expected to exceed the £3m forecast by £500k. This
is due to the asbestos works, additional works above the original specification to ensure
patient safety including anti ligature fittings and lower VAT recovery than initially
anticipated. These are however, still subject to change. The capital programme has
been reviewed and it is anticipated that these costs can be managed and contained
within the overall capital budget of £10.2m.
10.2 Cumulative capital expenditure totalled £2.5m at the end of Month 5, which was 77% of
the target. This position is expected to improve in the next month.
10.3 The Trust is planning to spend the minimum required amount of £2.0m on capital. This
will put total capital expenditure within the parameters of Monitor’s threshold by the end
of September. There have been delays in the 2015/16 capital programme caused by:
a shortfall of project managers to achieve the programme.
Lengthy processes necessary to source exact equipment specifications required.
Delays mentioned above relating to the St Ann’s project.
10.4 To reduce the impact of these delays works that can be carried out ahead of plan have
been identified to reverse the effect of setbacks in other areas. In addition the Trust is
now working with a project management company to assist with the backlog
maintenance projects. Due to the steps taken the Trust is expecting to achieve the
Quarter 2 Monitor target.
10.5 A property transferred to the Trust by the demised PCT, Whitfield Rural Centre, is
required by Secretary of State to be transferred to NHS Property Services as the Trust is
no longer using the property for its services. The transfer will be for nil consideration.
There has been no further progress in agreement of transfer, however the Department of
Health have agreed that no further valuation is required by the Trust before transfer.

11. Balance Sheet
11.1 The Trust’s cash balance was £30.5m at the end of August. This is an increase of £3.1m from the end of July.
11.2 Sales ledger debt continues to be closely controlled with a decrease from £5.7m to
£2.4m in total. Overdue debt has increased slightly but the over 90 day debt has
reduced. Overall there was an increase of £13k of overdue debt. Since 31st August a
further £0.2m of the outstanding debt has been received.
11.3 There is still a large amount of NCA debt outstanding which continues to be rigorously
pursued and investigated. At 31st July there was £345k of over 90 day NCA debt, this
has reduced to £257k at the end of August. Monthly meetings are being held to monitor
this separately and to resolve outstanding issues.
11.4 A detailed statement of the Trust’s financial position at 31st August 2015 is attached at Appendix 4.
12. CoSRR
12.1 Monitor has, at Month 5, changed their Risk Rating mechanism, following the publication of their revised Risk Assessment Framework document in August. The new rating which replaces The Continuity of Services Risk Rating (CoSRR) is The Financial Sustainability Risk Rating (FSRR).
12.2 The new rating comprises 4 metrics, which are equally weighted. These include the 2 metrics which were previously in place (Capital Service Cover Rating and Liquidity Rating) plus two new metrics (I&E Surplus Margin and I&E Margin Variance). The new metrics measure profitability and achievement of Plan.
12.3 Should one or more of the metrics score a ‘1’, then an override will be triggered, resulting
in a maximum overall rating of ‘2’.
12.4 The risk rating at Month 5 is as follows:
Capital Service Capacity rating 4
Liquidity rating 4
I&E Margin rating 3
I&E Margin Variance rating 1
Financial Sustainability Risk Rating before overrides 3
1 Rating Trigger for FSRR Trigger
Financial Sustainability Risk Rating after 1 rating override
2
Overall Financial Sustainability Risk Rating 2
12.5 The current forecast outturn would result in an overall FSRR of 2 at the end of the year. This is in contrast to the CoSRR which would result in an overall rating of 3.
12.6 Based on the current expected annual revenue figure, the total year–end deficit would need to be reduced to below £3.0m i.e. less than £0.8m behind plan, to maintain our planned score of 3 under the new rating.

APPENDIX 1
INCOME & EXPENDITURE SUMMARY
Month 5 2015/16 (August)
CURRENT ANNUAL BUDGET YEAR TO DATE FORECAST @ M5
Total Budget Actual Variance Over/(Under)
Inc & Exp Pay Non-Pay Inc & Exp Pay Non-Pay Inc & Exp Pay Non-Pay Inc & Exp
£000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 % £000 £000 £000
INCOME
Baseline Income (227,469) (94,768) (94,768) (0) (0%) G 0
Dorset Locality (6,016) (2,785) (2,536) 250 9% R 708
Poole & East Dorset Locality (5,973) (3,256) (3,688) (432) (13%) G (304)
Bournemouth & Christchurch Locality (6,773) (2,927) (2,884) 44 1% R 116
Other Income (3,381) (1,445) (1,415) 30 2% R 45
Total Trust Income (249,612) (105,182) (105,290) (108) (0%) G 565
EXPENDITURE
Dorset Locality 51,479 18,475 69,954 21,502 7,695 29,197 21,796 7,603 29,398 294 (93) 201 1% R 654 29
Poole & East Dorset Locality 50,266 17,305 67,572 21,173 7,514 28,687 20,803 7,615 28,418 (370) 101 (269) (1%) G (228) 281
Bournemouth & Christchurch Locality 53,100 11,481 64,581 22,106 4,868 26,974 22,672 5,407 28,080 566 540 1,106 4% R 2,605 950
Nurse Executive & Quality 3,959 910 4,869 1,679 400 2,079 1,607 401 2,008 (72) 1 (71) (3%) G (108) 3
Finance, IT, Business Performance 9,354 5,078 14,432 3,559 2,547 6,105 3,460 2,682 6,141 (99) 135 36 1% R (477) 336
Human Resources 4,815 1,292 6,108 1,913 414 2,327 1,938 340 2,278 26 (75) (49) (2%) G 85 (65)
Strategy & Estates 6,509 6,851 13,360 2,700 2,813 5,513 2,446 2,911 5,357 (253) 97 (156) (3%) G (240) 152
Corporate Services 2,058 916 2,975 791 424 1,216 822 455 1,277 31 31 61 5% R 8 (78)
Central Budgets 0 1,168 1,168 0 (900) (900) 0 54 54 0 954 954 (106%) R (497) 3,162
Total Trust Expenditure 181,540 63,477 245,017 75,422 25,776 101,198 75,544 27,466 103,011 123 1,690 1,813 2% R 1,802 4,771
NET INCOME & EXPENDITURE (4,595) (3,984) (2,279) 123 1,690 1,705 1,802 4,771 565
Interest Received * (66) (27) (54) 0 0 (27) 99% G (27)
Public Dividend Capital Dividend 4,660 4,660 1,942 1,942 1,942 1,942 0 0 0 0% G
RETAINED (SURPLUS)/DEFICIT 0 (2,069) (392) 123 1,690 1,678 R 7,111
EBITDA 5.1% 2.3%
Memorandum Note Performance v Monitor Plan Segmental Performance
Annual Turnover (at Month End) Financed By; £000 Income versus Expenditure YTD Forecast
Annual YTD YTD £000 £000
Total Trust Income 249,612 Plan Plan Actual Bournemouth & Christ'ch Locality 1,396 5,426
Total Annual Turnover before Interest received 249,612 £000 £000 £000 Dorset Locality 721 2,057
Interest Received * 66 Poole & East Dorset Locality (440) (371)
Total Annual Turnover 249,678 Total 1,677 7,112
Pay Non-Pay Income
2,160 3,181 (392)
Pay Non-Pay
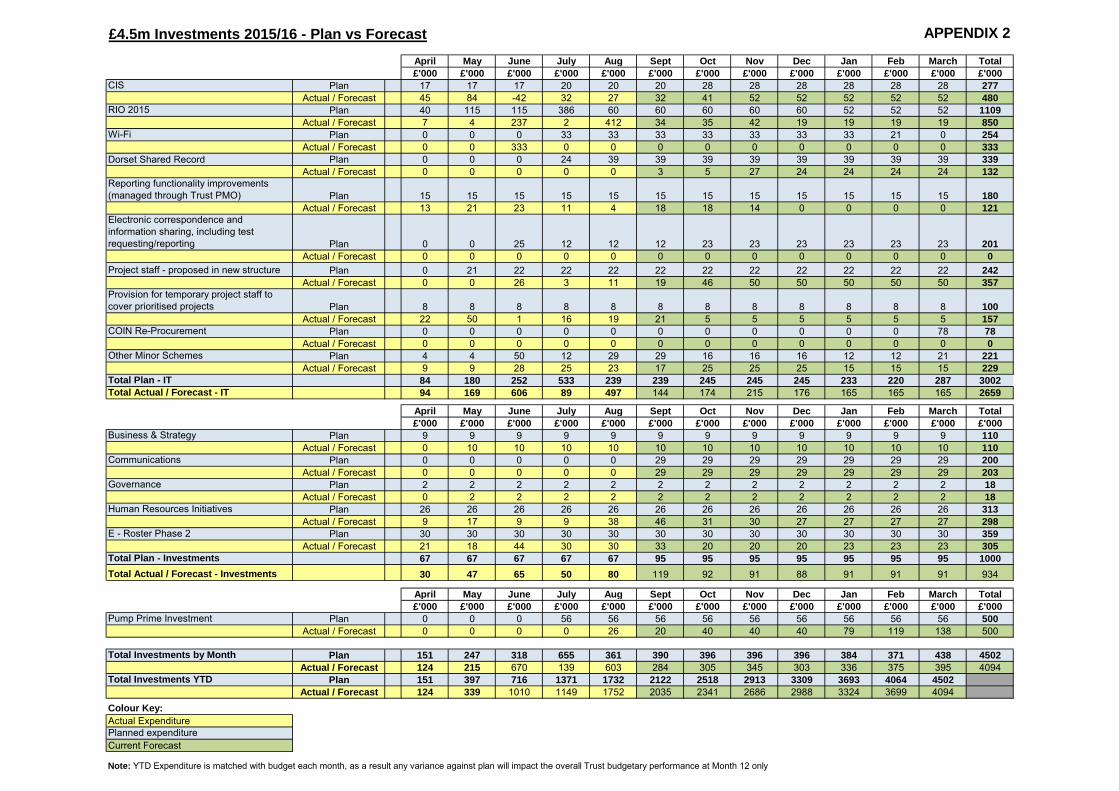
£4.5m Investments 2015/16 - Plan vs Forecast APPENDIX 2
April May June July Aug Sept Oct Nov Dec Jan Feb March Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
CIS Plan 17 17 17 20 20 20 28 28 28 28 28 28 277
Actual / Forecast 45 84 -42 32 27 32 41 52 52 52 52 52 480
RIO 2015 Plan 40 115 115 386 60 60 60 60 60 52 52 52 1109
Actual / Forecast 7 4 237 2 412 34 35 42 19 19 19 19 850
Wi-Fi Plan 0 0 0 33 33 33 33 33 33 33 21 0 254
Actual / Forecast 0 0 333 0 0 0 0 0 0 0 0 0 333
Dorset Shared Record Plan 0 0 0 24 39 39 39 39 39 39 39 39 339
Actual / Forecast 0 0 0 0 0 3 5 27 24 24 24 24 132
Reporting functionality improvements
(managed through Trust PMO) Plan 15 15 15 15 15 15 15 15 15 15 15 15 180
Actual / Forecast 13 21 23 11 4 18 18 14 0 0 0 0 121
Electronic correspondence and
information sharing, including test
requesting/reporting Plan 0 0 25 12 12 12 23 23 23 23 23 23 201
Actual / Forecast 0 0 0 0 0 0 0 0 0 0 0 0 0
Project staff - proposed in new structure Plan 0 21 22 22 22 22 22 22 22 22 22 22 242
Actual / Forecast 0 0 26 3 11 19 46 50 50 50 50 50 357
Provision for temporary project staff to
cover prioritised projects Plan 8 8 8 8 8 8 8 8 8 8 8 8 100
Actual / Forecast 22 50 1 16 19 21 5 5 5 5 5 5 157
COIN Re-Procurement Plan 0 0 0 0 0 0 0 0 0 0 0 78 78
Actual / Forecast 0 0 0 0 0 0 0 0 0 0 0 0 0
Other Minor Schemes Plan 4 4 50 12 29 29 16 16 16 12 12 21 221
Actual / Forecast 9 9 28 25 23 17 25 25 25 15 15 15 229
Total Plan - IT 84 180 252 533 239 239 245 245 245 233 220 287 3002
Total Actual / Forecast - IT 94 169 606 89 497 144 174 215 176 165 165 165 2659
April May June July Aug Sept Oct Nov Dec Jan Feb March Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Business & Strategy Plan 9 9 9 9 9 9 9 9 9 9 9 9 110
Actual / Forecast 0 10 10 10 10 10 10 10 10 10 10 10 110
Communications Plan 0 0 0 0 0 29 29 29 29 29 29 29 200
Actual / Forecast 0 0 0 0 0 29 29 29 29 29 29 29 203
Governance Plan 2 2 2 2 2 2 2 2 2 2 2 2 18
Actual / Forecast 0 2 2 2 2 2 2 2 2 2 2 2 18
Human Resources Initiatives Plan 26 26 26 26 26 26 26 26 26 26 26 26 313
Actual / Forecast 9 17 9 9 38 46 31 30 27 27 27 27 298
E - Roster Phase 2 Plan 30 30 30 30 30 30 30 30 30 30 30 30 359
Actual / Forecast 21 18 44 30 30 33 20 20 20 23 23 23 305
Total Plan - Investments 67 67 67 67 67 95 95 95 95 95 95 95 1000
Total Actual / Forecast - Investments 30 47 65 50 80 119 92 91 88 91 91 91 934
April May June July Aug Sept Oct Nov Dec Jan Feb March Total
£'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000 £'000
Pump Prime Investment Plan 0 0 0 56 56 56 56 56 56 56 56 56 500
Actual / Forecast 0 0 0 0 26 20 40 40 40 79 119 138 500
Total Investments by Month Plan 151 247 318 655 361 390 396 396 396 384 371 438 4502
Actual / Forecast 124 215 670 139 603 284 305 345 303 336 375 395 4094
Total Investments YTD Plan 151 397 716 1371 1732 2122 2518 2913 3309 3693 4064 4502
Actual / Forecast 124 339 1010 1149 1752 2035 2341 2686 2988 3324 3699 4094
Colour Key:
Actual Expenditure
Planned expenditure
Current Forecast
Note: YTD Expenditure is matched with budget each month, as a result any variance against plan will impact the overall Trust budgetary performance at Month 12 only
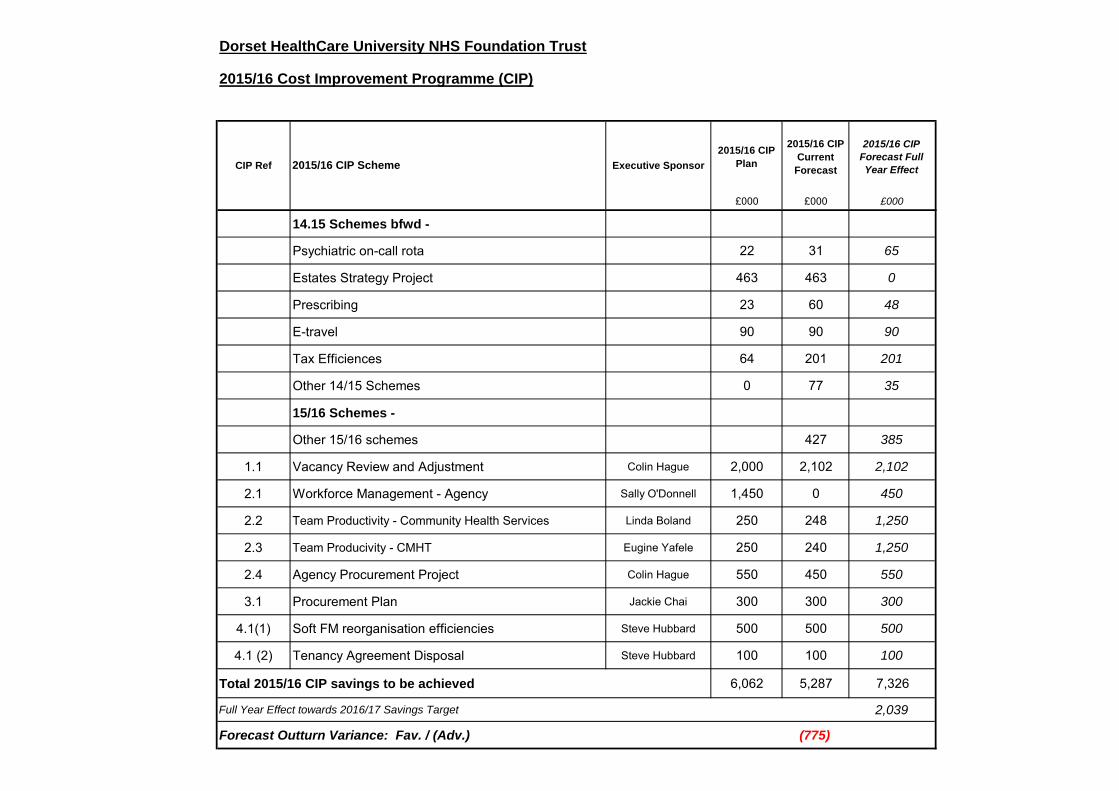
Dorset HealthCare University NHS Foundation Trust
2015/16 Cost Improvement Programme (CIP)
2015/16 CIP
Plan
2015/16 CIP
Current
Forecast
2015/16 CIP
Forecast Full
Year Effect
£000 £000 £000
14.15 Schemes bfwd -
Psychiatric on-call rota 22 31 65
Estates Strategy Project 463 463 0
Prescribing 23 60 48
E-travel 90 90 90
Tax Efficiences 64 201 201
Other 14/15 Schemes 0 77 35
15/16 Schemes -
Other 15/16 schemes 427 385
1.1 Vacancy Review and Adjustment Colin Hague 2,000 2,102 2,102
2.1 Workforce Management - Agency Sally O'Donnell 1,450 0 450
2.2 Team Productivity - Community Health Services Linda Boland 250 248 1,250
2.3 Team Producivity - CMHT Eugine Yafele 250 240 1,250
2.4 Agency Procurement Project Colin Hague 550 450 550
3.1 Procurement Plan Jackie Chai 300 300 300
4.1(1) Soft FM reorganisation efficiencies Steve Hubbard 500 500 500
4.1 (2) Tenancy Agreement Disposal Steve Hubbard 100 100 100
Total 2015/16 CIP savings to be achieved 6,062 5,287 7,326
Full Year Effect towards 2016/17 Savings Target 2,039
Forecast Outturn Variance: Fav. / (Adv.) (775)
CIP Ref 2015/16 CIP Scheme Executive Sponsor
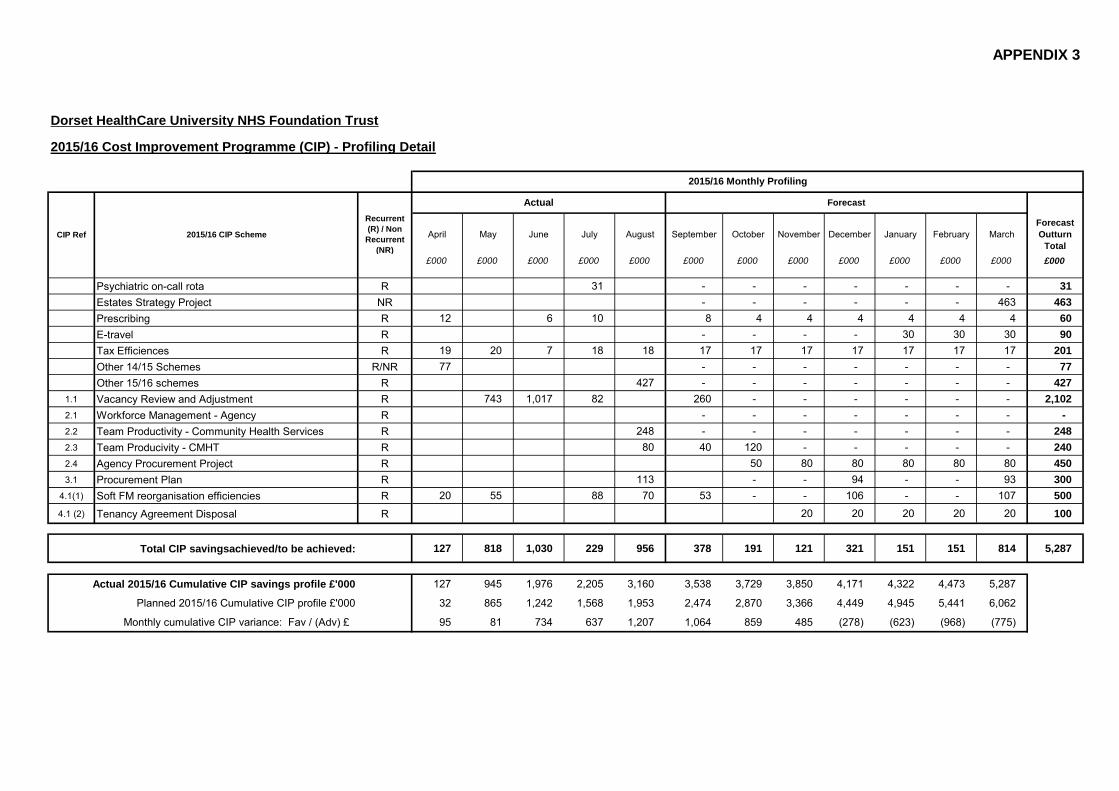
APPENDIX 3
Dorset HealthCare University NHS Foundation Trust
2015/16 Cost Improvement Programme (CIP) - Profiling Detail
Recurrent
(R) / Non
Recurrent
(NR)
April May June July August September October November December January February March
Forecast
Outturn
Total
£000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000 £000
Psychiatric on-call rota R 31 - - - - - - - 31
Estates Strategy Project NR - - - - - - 463 463
Prescribing R 12 6 10 8 4 4 4 4 4 4 60
E-travel R - - - - 30 30 30 90
Tax Efficiences R 19 20 7 18 18 17 17 17 17 17 17 17 201
Other 14/15 Schemes R/NR 77 - - - - - - - 77
Other 15/16 schemes R 427 - - - - - - - 427
1.1 Vacancy Review and Adjustment R 743 1,017 82 260 - - - - - - 2,102
2.1 Workforce Management - Agency R - - - - - - - -
2.2 Team Productivity - Community Health Services R 248 - - - - - - - 248
2.3 Team Producivity - CMHT R 80 40 120 - - - - - 240
2.4 Agency Procurement Project R 50 80 80 80 80 80 450
3.1 Procurement Plan R 113 - - 94 - - 93 300
4.1(1) Soft FM reorganisation efficiencies R 20 55 88 70 53 - - 106 - - 107 500
4.1 (2) Tenancy Agreement Disposal R 20 20 20 20 20 100
Total CIP savingsachieved/to be achieved: 127 818 1,030 229 956 378 191 121 321 151 151 814 5,287
Actual 2015/16 Cumulative CIP savings profile £'000 127 945 1,976 2,205 3,160 3,538 3,729 3,850 4,171 4,322 4,473 5,287
Planned 2015/16 Cumulative CIP profile £'000 32 865 1,242 1,568 1,953 2,474 2,870 3,366 4,449 4,945 5,441 6,062
Monthly cumulative CIP variance: Fav / (Adv) £ 95 81 734 637 1,207 1,064 859 485 (278) (623) (968) (775)
2015/16 Monthly Profiling
CIP Ref 2015/16 CIP Scheme
ForecastActual

APPENDIX 4
£000's £000's £000's £000's
NON-CURRENT ASSETS
31st March
2015
31st July
2015
31st
August
2015
Movement
(Month on
Month)
Intangible assets 107 94 90 (4)
Property, plant and equipment 151,933 151,289 151,247 (41)
TOTAL NON-CURRENT ASSETS 152,040 151,383 151,337 (45)
CURRENT ASSETS
Inventories 755 760 750 (10)
Non-current assets for sale 2,334 2,334 2,334 0
NHS receivables 2,783 3,145 1,375 (1,770)
Provision for impaired receivables (53) (46) (46) 0
Related Party receivable 0 0 0 0
Other receivables 1,508 3,541 1,626 (1,915)
NHS Accrued Income 1,299 6,064 7,794 1,730
Accrued Income 225 324 398 74
Prepayments 1,608 2,156 1,605 (551)
PDC dividend receivable 75 0 0 0
Cash and cash equivalents 30,115 27,434 30,519 3,085
TOTAL CURRENT ASSETS 40,649 45,712 46,355 643
CURRENT LIABILITIES
NHS payables (933) (1,998) (1,708) 290
Borrowings (8) (6) (5) 1
Other payables (9,830) (10,539) (10,578) (39)
PDC dividend payable 0 (1,478) (1,867) (389)
Trade payables - capital (672) (882) (547) 335
Related Party payable (12) (3) (2) 1
Accruals (6,967) (7,216) (8,468) (1,252)
Receipts in advance 0 0 0 0
Provisions (1,206) (1,053) (1,036) 17
TOTAL CURRENT LIABILITIES (19,627) (23,175) (24,211) (1,036)
TOTAL ASSETS LESS CURRENT LIABILITIES 173,062 173,920 173,481 (438)
NON-CURRENT LIABILITIES
Borrowings (1) (1) (1) 0
Provisions (2,494) (2,518) (2,521) (3)
TOTAL ASSETS EMPLOYED 170,567 171,401 170,959 (442)
FINANCED BY (TAXPAYERS' EQUITY)
Public Dividend Capital (31,080) (31,080) (31,080) 0
Income and expenditure reserve * (88,443) (89,277) (88,835) 442
Revaluation reserve (51,044) (51,044) (51,044) 0
TOTAL TAXPAYERS' EQUITY (170,567) (171,401) (170,959) 442
* This is the equivalent of Retained Earnings for a Limited Company. The working capital is: £22,144 k
DORSET HEALTHCARE UNIVERSITY NHS FOUNDATION TRUST
Statement of Financial Position
as at 31st August 2015

APPENDIX 4
000's 000's 000's 000's
31st March
2015
31st July
2015
31st
August
2015
Movement
(Month on
Month)
1. Sales Ledger Aged Debt Analysis Current - £2,338 £4,063 £690 (£3,373)
+30 days - £717 £688 £542 (£146)
+60 days - £173 £230 £428 £198
+90 days - £620 £764 £725 (£39)
Total Trade Debtors £3,849 £5,746 £2,385 (£3,361)
3. Not included in the above balance sheet, the Trust has the following amount in NHS bank accounts
in respect of patients' investments £32k.
NOTES
2. The interest rate as at 31st August 2015 for our Government Bankings Service Account and our
Lloyds TSB Account was 0.25%
People Management Part 1 Board Meeting 30 September 2015
Author Colin Hague
Sponsoring Board Member
Colin Hague, Director of HR
Purpose of Report To give an update on people management over the last two months.
Recommendations 1. The Board is asked to note the report
Engagement and Involvement
Appropriate Trade Union Partnership Forum, Doctors and Dentists Joint Negotiating Forum, Equality and Diversity Steering Group and Health and Safety Committee engagement and Executive Performance and Corporate Risk Group consideration has taken place on matters raised in this report.
Previous Board/Committee Dates
This follows a monthly Part 1 Board reporting on People Management and Organisation Development in July 2015.
Monitoring and Assurance Summary
This report links to the Strategic Goals
To provide high quality care; first time, every time; To be a valued partner and expert in partnership working
with Patients, Communities and organisations; To be a learning organisation, maximising our partnership
with Bournemouth University and promoting innovation, research and evidence based practice;
To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare;
To be a national leader in the delivery of integrated care; To ensure that all of the Trust’s resources are used in an
efficient and sustainable way; To raise awareness within the Trust and externally of the
impact that our work has on people and our environment, and take steps to reduce any negative effects.
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability
Information Management &Technology
Equality Impact Assessment
Freedom of Information

2
1. Summary
Positive steps have been taken to improve attraction which effects all 3 domains of quality including:
Coordinated recruitment and rolling advertisements
Promotion of external advertising including radio campaigns
Collaborative working with local Trusts
Recruitment open days in Community Hospitals Retentions action include:
In-depth analysis of leavers and exploration of reasons for leaving
Improving developments for Bands 1 through to 4
Active promotion of attraction, recruitment and retention work being undertaken In connection with recruitment:
Data confirms that more staff have been recruited and are in post involving an increase from 4338.85 fte at the end of August 2014 to 4470.95 at the end of August 2015.
The increased numbers of staff in post is supported by data extracted from the general ledger (reflecting the budgeted position) to indicate a reduction in vacancy levels from 8.62% in August 2014 to 8.23% in August 2015
Budgeted establishment has increased from 4769.99 in August 2014 to 4890.25 in August 2015, an overall increase of 120.26 fte where the Board has sought to increase establishments to support service improvement.
Vacant budgeted fte (without bank and agency cover) on the general ledger involved a decrease from 411.77 to 402.36 overall between August 2014 and August 2015.
There are more Nursing vacancies on the budgeted ledger increasing from 106 in August 2014 to 164 in August 2015 and likewise, the budgeted establishment for nurses has increased by 58 fte from 1595 to 1653.
Budgeted vacancies in other areas have decreased overall from 304 in August 2014 to 237 in August 2015.
Nursing vacancies still remain the most difficult staff group to recruit to with Older Persons Mental Health and Prison Healthcare services being the most difficult areas, with a vacancy factor of 11.49% and 29.41% respectively.
Most of the Community Hospitals have significant RGN vacancies at the moment; however the 13 job offers resulting from recruitment open days and overseas recruitment commenced employment in September 2015.
The report contains an update on national arrangements for mileage rates which affect the proposed harmonisation of local rates. Attention is being given to corporate actions to address agency expenditure for financial and workforce management reasons as well as from Secretary of State and Monitor expectations. NHS England are proposing to change Junior Doctors contracts. The Staff Survey for 2015 is about to commence. Flu programme plans and Learning and Development actions are set out in the report.
3
2. Organisational Change
The following Organisational Change programmes are in progress: On-call Consultation
IT: Consultation closed on 29 June 2015, the outcome of which was that there is a need to broaden the scope of the On-call pool of staff in order to address the issues that have been raised during consultation, such as the complexity of sites, required skills mix and need for a point of escalation. A new On-call scheme was developed and consultation commenced with a wider group of IT staff on 18th & 19th August. The new proposal is a three tier approach divided by roles and technical ability, to ensure the right skills are available to deliver the required On-call service. The Agenda for Change pay model will be aligned with the proposal for new scheme arrangements.
Estates: Consultation closed on 7 August 2015, the outcome of which is to implement streamlined On-call arrangements but maintain the current pay model as an interim measure. A review of the Estates (trades) roles will take place to consider all elements including On-call and Recruitment and Retention Premia, the roles will then be re-evaluated and once finalised the Agenda for Change On-call pay model will be implemented, subject to the provisions of the Pay Protection Policy.
Dorset Contraception and Sexual Health Services A formal Tender was submitted in early July and Dorset HealthCare were one of three shortlisted to interview. Interviews took place at the end of July and an outcome was anticipated towards the end of August. The Trust has now been advised that the Tender has been withdrawn and that Public Health are seeking guidance to enable them to extend existing contracts prior to a new Tendering process commencing. There are still a number of unanswered questions, particularly around the length of time existing contracts will be extended and associated budgets. It is hoped that the new Tender will include aspects of the previous one and therefore work completed can still be utilised. Flaghead Unit Formal consultation has ended and the majority of staff have already been successful in securing suitable alternative employment within the organisation. Two staff are now considered to be formally at risk and we are currently going through the process of seeking suitable alternative employment. Organisational Development, Participation and Communications Consultation The consultation has now been completed and one member of staff remains at risk of redundancy. Support continues to facilitate redeployment to a suitable alternative role. Secure – Counter Fraud, Security Management and Compliance Team The team of 3 people ceased to work following national changes to compliance. Two staff have been permanently redeployed and one member temporarily redeployed. NHS England has agreed a payment of over £40,000 to cover costs involved with this change. Consultation processes associated with the financial challenges Secure face are taking place. A full range of options are being explored individually including restructuring and secure transfer. Dorset Forensic Services Community Forensic caseload numbers have significantly increased over recent years due to an evolving service and increasing external demand. This has resulted in a need for increased capacity and intervention and there is now a requirement for strategic caseload management by the nursing team. In order to support the service going forward it is proposed to restructure the current nursing provision. Formal consultation commenced during the week of 7 September 2015.
4
Prison Dental Staff On 1 September 2015 a TUPE transfer into Dorset HealthCare took place for three dental staff previously employed by the Somerset Partnership NHS Trust, as a result of a decision to bring dental services for Dorset prisons in-house. Two of the staff will require a change of work base as they were previously located within a Somerset Partnership clinic and suitable alternative work bases are being identified.
3. Security Management Prosecutions
A Dorset HealthCare employee who works at Exeter Prison received threats from an inmate to kill them and their family. The case was reported to Police and the complainant was arrested/interviewed/charged and put before Exeter Crown Court on 3rd August 2015. He was convicted and received 4 years imprisonment. On 15th July 2015 a service user smashed his way into Hahnemann House and caused Criminal Damage. He threw a fire extinguisher through a window, poured water into the fire alarm system and forced his way through several access controlled doors. Staff needed to barricade themselves into offices. The individual responsible failed to appear at court at earlier hearings and a warrant was issued for his arrest. On 11th August 2015 the individual appeared before Bournemouth Magistrates Court where he pleaded guilty to criminal damage and was sentenced to 3 weeks imprisonment which was extended to 12 weeks with other offences taken into consideration.
4. Attraction Strategy
Consistent with the HR Strategy and Board Assurance Framework a range of activities continue to take place to support recruitment outcomes and recent/future activities include: Co-ordinated Recruiting and Rolling Adverts Community Nurse and Community Hospital Staff Nurse vacancies are being split into locality groups of adverts rather than one generic advert. It is anticipated that this will provide the localities with the opportunity to have more bespoke adverts and the ability to reach their target audience more directly. This approach is also being considered for Mental Health vacancies. NHS Jobs Attendance at the NHS Jobs User Group highlighted the following statistics on the use of NHS Jobs: - A new record of over 30,000 adverts were placed on NHS Jobs in July 2015 - 45,000 applications were made in July 2015 - Approximately 80,000 new job seekers register onto NHS Jobs each month As this demonstrates the volume of competitors as well as the high numbers of job seekers, a reminder has been put in HR Matters to encourage recruiting managers to make their adverts as attractive as possible to potential candidates, along with guidance. There is now less use of press adverts. In the last 12 months the HR Services Team have placed over 45 adverts in the following publications: the Blackmore Vale, Bournemouth Echo, Bridport News Series, Dorset Evening Echo, Salisbury Journal, Swanage and Wareham Advertiser and the Western Gazette The majority of adverts have been for Catering, Domestic, Nursing and Physiotherapy roles, with 80% having been appointed into so far.
5
A reminder was included in the September edition of HR Matters giving advice to managers on how to place an advert in a relevant external publication. Collaborative working with local Trusts A meeting was held on 1 September 2015, the key points of which are summarised below:
Both Poole and Royal Bournemouth Hospitals have offered a number of posts to nurses from the Philippines; however it now looks likely that they will not proceed due to Certificates of Sponsorship (COS) not being granted.
It was confirmed that Dorset HealthCare, Royal Bournemouth, Poole and Dorset County Hospital have responded to NHS Employers request for information to enable them to formally raise this issue and apply for nurses to be added to the Shortage Occupation List.
Royal Bournemouth Hospital are paying an additional allowance to staff working on older peoples wards. This appears to have limited impact on recruitment in view of the level of the payment.
Work is underway to agree a memorandum of understanding between Trusts on the supply of bank and agency staff, which will allow recruitment check information to be shared and thereby enable bank workers to join another Trust without having to go through the pre-employment checks again.
Recruitment for Bridport Community Hospital A recruitment open day was held on 11 September 2015, where a variety of roles were advertised and included:
RGN’s and HealthCare Assistants to work on the wards in the Hospital
RGN’s/District Nurses to work in community teams
RGN/RMN’s to work in Devon Prisons.
Bank Nurses
Domestic Staff to work in the Hospital Recruitment for Westhaven and Weymouth Community Hospitals A recruitment open day was held at Westhaven Hospital on 21 September 2015, supported by a radio advertising campaign to attract nurses, minor injuries practitioners, health visitors, physiotherapists and occupational therapists. Relocation Expenses The number of new starters that have claimed relocation expenses on difficult to recruit to positions to date is 23. This involves 2 year re-payment provisions. Refer a Friend Scheme The number of referral payments made to a member of existing staff when they have referred a friend is 2 so far. A number of other referrals have been made but not yet paid and the number is therefore expected to increase. Nurse Migration Requirements Representations have been made regarding requirements on migration that are affecting nurse recruitment in Dorset and Nationally. NHS Employers requested contributions to the review of the Tier 2 route affecting NHS Trusts so that a combined response could be submitted to Migration Advisory Committee (MAC) at the end of August. As part of the response from Dorset HealthCare we highlighted the challenges of restricting the Tier 2 route to only those on the shortage occupation list which currently does not include Nursing or Allied Health Professional roles. We are subsequently awaiting the outcome of a meeting with Head of Policy within the MAC secretariat to discuss the proposals in the Tier 2 review on 23 September 2015.
6
Risk Register The Risk Register position on Attraction and Retention is being updated.
5. Retention Strategy
A range of activities are taking place to support retention outcomes and recent activities have included: Leavers Leaver processes are being reviewed to support understanding of reasons for leaving and support for re-engagement and consideration on the professional register or remaining with the Trust on the Professional Nursing Support Team where appropriate. Improving development for Band’s 1-4 A drop in day was arranged for 18 September 2015 whereupon staff from Bournemouth University, Local Colleges and Trust Learning and Development were on hand to discuss the following:
Access Course, Apprenticeships, Mental Health Diploma.
Bridging programme.
Entry into: Adult, Child and Mental Health Nursing, Physiotherapy and Occupational Therapy professional programmes.
Salary Support Secondments to University.
Bands 1-4 Funding – Appraisals and the Learning Needs Analysis.
Shadowing opportunities, Leadership & Personal effectiveness.
Work Related Learning Salary Sacrifice Scheme. Nursing Strategy Launch Event The HR team attended the Nursing Strategy Launch Event on 10 September 2015 to promote some of the activity the team is currently engaged in to attract, recruit and retain staff, as well as to signpost current staff to some of the opportunities and benefits available. A challenge for the Board is how we can support nursing staff consistent with the Strategy.
6. Time to Hire
Average Time to Hire A further assessment on target setting for time to hire is taking place. A presentation took place on 28 August 2015 to look at an applicant tracking system called TRAC, which was attended by key stakeholders including the HR team, Learning and Development and Occupational Health, as well as a representative from Dorset County Hospital. The presentation demonstrated a system that could enable the recruitment process to work more efficiently, as well as providing more information and communication to recruiting managers and candidates themselves. Contact has also been made with other Trusts already using the system who have all reported the benefits of using the system and the difference it has made to speed up their recruitment timelines. Arrangements are therefore being explored for beginning the progress of implementing the new TRAC system in time for the end of 2015. This should support reducing further time to hire. Occupational Health and Job Matching Service Standards have been incorporated into the Work Plan to begin to monitor these as part of the time to hire information provided. These measures will be provided in the next People Management Board report.
7
Use of Skype for interviews The IT and HR Services Directorate are piloting the use of Skype for interviews. PC’s and laptops with Skype are available at Sentinel House, Forston Clinic and Alderney Hospital, Poole. One example of the use is that Skype interviews were undertaken at the beginning of September, which has supported a total of 10 overseas Band 5 Staff Nurses starting work at Alderney Hospital on 28 September 2015. Recruitment Feedback Three short surveys have been set up to gather feedback from candidates and managers on their experience of the recruitment process. The surveys are being promoted at three separate stages of recruitment:
When a candidate receives their conditional offer of employment
When a candidate receives their unconditional offer and contract of employment
When all pre-employment checks are completed and recruiting managers are asked to arrange a suitable start date
The surveys aim to gather feedback on the processes being followed and the length of time it has taken. Updates on the data gathered and impact on processes will be provided in future reports. NHS Jobs Feedback The Trust continues to score significantly above average in the feedback left by applicants on NHS Jobs after they have been through the application and shortlisting stages. An example of some of the comments received are as follows:
“Very disappointed when the job was pulled. However the way it was handled was excellent with personal contact made.”
“Very easy system to use to see available posts and submitting an application is also very user friendly. Confirmation email acknowledging that the application has been submitted and received is immediate which is a candidate’s main, initial concern”
“It was useful to be able to speak to a member of the recruitment staff from the unit prior to application. I was advised accordingly.”
“All information presented was to a high standard. I received a polite email informing me that I did not get an interview but I was reserve and this was sent in good time after the application date closed”
“I am waiting for my checks and references to go through and then hopefully I will be given a start date. So far the process has been very swift.”
“Fantastic communication from the prospective employer” Customer Service Feedback An example of some of the feedback received by HR Services from candidates that have been successful at interview is as follows:

8
The biggest reasons for new starters being attracted to join the Trust were for the role or the location, closely followed by opportunities for development and to make a difference to health care
82% of successful candidates rated the information they received from HR Services as either very good or excellent
82% of successful candidates rated the information they received from their new line manager as either very good or excellent
An example of some of the feedback received by HR Services from candidates going through recruitment checks is as follows:
An example of some of the feedback received by HR Services from recruiting managers is as follows:
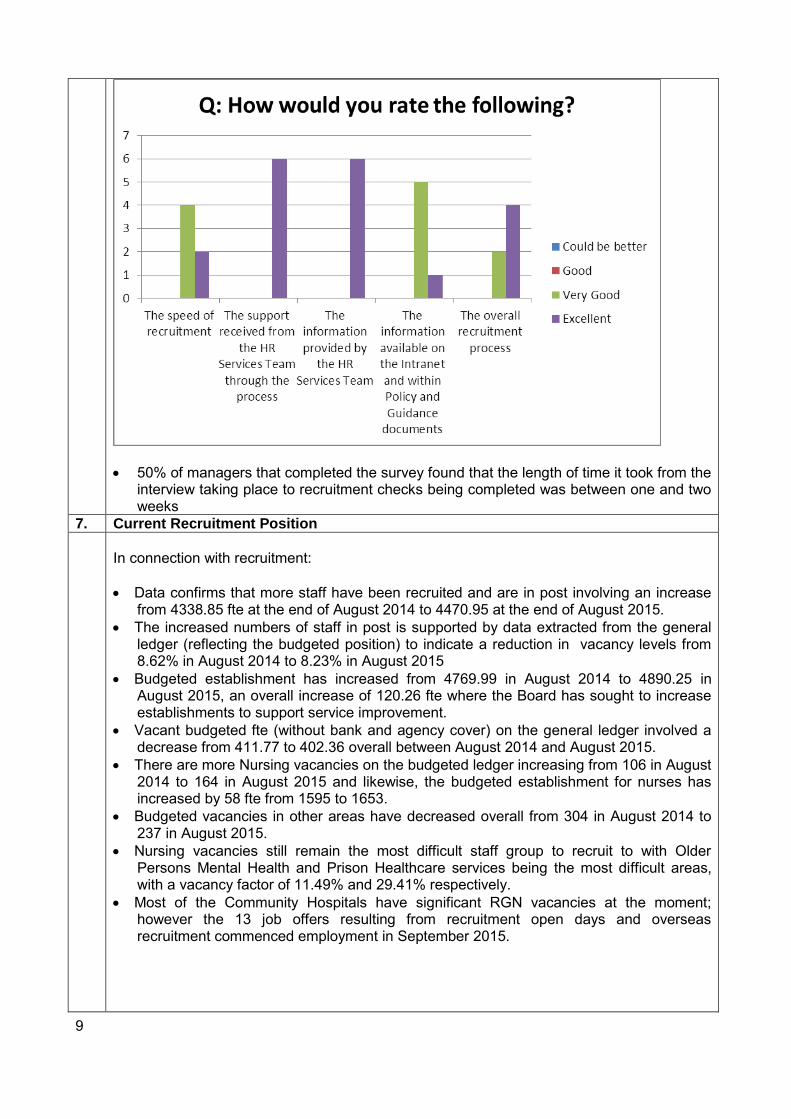
9
50% of managers that completed the survey found that the length of time it took from the interview taking place to recruitment checks being completed was between one and two weeks
7. Current Recruitment Position
In connection with recruitment:
Data confirms that more staff have been recruited and are in post involving an increase from 4338.85 fte at the end of August 2014 to 4470.95 at the end of August 2015.
The increased numbers of staff in post is supported by data extracted from the general ledger (reflecting the budgeted position) to indicate a reduction in vacancy levels from 8.62% in August 2014 to 8.23% in August 2015
Budgeted establishment has increased from 4769.99 in August 2014 to 4890.25 in August 2015, an overall increase of 120.26 fte where the Board has sought to increase establishments to support service improvement.
Vacant budgeted fte (without bank and agency cover) on the general ledger involved a decrease from 411.77 to 402.36 overall between August 2014 and August 2015.
There are more Nursing vacancies on the budgeted ledger increasing from 106 in August 2014 to 164 in August 2015 and likewise, the budgeted establishment for nurses has increased by 58 fte from 1595 to 1653.
Budgeted vacancies in other areas have decreased overall from 304 in August 2014 to 237 in August 2015.
Nursing vacancies still remain the most difficult staff group to recruit to with Older Persons Mental Health and Prison Healthcare services being the most difficult areas, with a vacancy factor of 11.49% and 29.41% respectively.
Most of the Community Hospitals have significant RGN vacancies at the moment; however the 13 job offers resulting from recruitment open days and overseas recruitment commenced employment in September 2015.
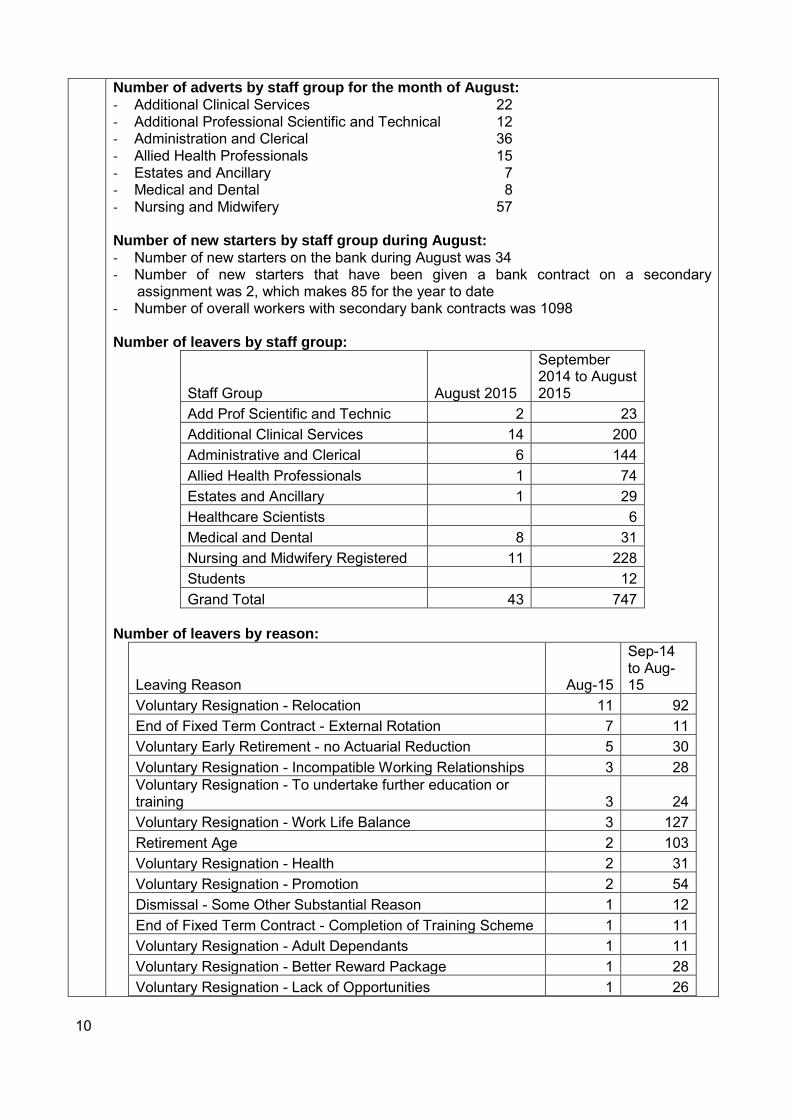
10
Number of adverts by staff group for the month of August:
- Additional Clinical Services 22 - Additional Professional Scientific and Technical 12 - Administration and Clerical 36 - Allied Health Professionals 15 - Estates and Ancillary 7 - Medical and Dental 8 - Nursing and Midwifery 57 Number of new starters by staff group during August:
- Number of new starters on the bank during August was 34 - Number of new starters that have been given a bank contract on a secondary
assignment was 2, which makes 85 for the year to date - Number of overall workers with secondary bank contracts was 1098 Number of leavers by staff group:
Staff Group August 2015
September 2014 to August 2015
Add Prof Scientific and Technic 2 23
Additional Clinical Services 14 200
Administrative and Clerical 6 144
Allied Health Professionals 1 74
Estates and Ancillary 1 29
Healthcare Scientists 6
Medical and Dental 8 31
Nursing and Midwifery Registered 11 228
Students 12
Grand Total 43 747
Number of leavers by reason:
Leaving Reason Aug-15
Sep-14 to Aug-15
Voluntary Resignation - Relocation 11 92
End of Fixed Term Contract - External Rotation 7 11
Voluntary Early Retirement - no Actuarial Reduction 5 30
Voluntary Resignation - Incompatible Working Relationships 3 28
Voluntary Resignation - To undertake further education or training 3 24
Voluntary Resignation - Work Life Balance 3 127
Retirement Age 2 103
Voluntary Resignation - Health 2 31
Voluntary Resignation - Promotion 2 54
Dismissal - Some Other Substantial Reason 1 12
End of Fixed Term Contract - Completion of Training Scheme 1 11
Voluntary Resignation - Adult Dependants 1 11
Voluntary Resignation - Better Reward Package 1 28
Voluntary Resignation - Lack of Opportunities 1 26

11
Death in Service 6
Dismissal - Capability 26
Dismissal - Conduct 6
Employee Transfer 34
End of Fixed Term Contract 19
End of Fixed Term Contract - End of Work Requirement 1
End of Fixed Term Contract - Other 2
Redundancy - Compulsory 17
Retirement - Ill Health 3
Voluntary Early Retirement - with Actuarial Reduction 1
Voluntary Resignation - Child Dependants 25
Voluntary Resignation - Other/Not Known 19
Grand Total 43 747
8. Agency Attention
Agency worker attention is taking place by the Executive Team as part of financial management and value for money. The Secretary of State and Monitor have set expectations and the framework in this area is changing. Approval will from 19th October 2015be expected by Monitor for engagement of any off framework agency staff. This will create challenges for Dorset Health Care and Trusts generally. These actions are likely to affect the Agency marketplace off Framework Agency engagement will need to be reviewed will approval considered which can affect cover. Taking account a current Agency expenditure these changes should be used to support reducing Agency costs. Monitor is also setting a target limit for agency staff, a different limit has been applied for. Actions being taken relating to this area include:
The Chief Executive is chairing a fortnightly Workforce Management, Recruitment &
Retention meeting with Director colleagues and other appropriate staff to ensure
progress against our action plan
There is a dedicated Operational Director taking oversight for the agency reduction
work.
The Medical Director is engaged in a plan to reduce medical agency expenditure
with actions planned to make skill mix changes to fill vacant junior doctor posts
Controls are being introduced to manage high cost agency spend (exceeding £50k)
the HR Director has been asked to take oversight of this work stream.
A Project lead is in place for the agency reduction CIP project.
A Project Management Office team is in place to monitor progress against this and
other CIP schemes.
We are strengthening the E-Roster team with a database administrator who will
provide improved management information to assist managers in controlling the use
of agency
A registered nurse to support recruitment, retention, training of bank staff, advice on
staff training and introduce the Professional Nursing Support Team.
The Prisons workforce development strategy is in place and being progressed at
pace with project management support
There will be fortnightly Directors meetings going forward to review progress and ensure pace of change.

12
It is anticipated that we will now see month on month reductions, as corrective action starts to take effect.
9. Junior Doctor and Consultant Contracts
The Junior Doctors’ Committee have decided not to re-enter negotiations regarding their contracts. NHS Employers will now consider the options available to progress work to implement a new Junior Doctors’ contract in August 2016 and say they are committed to engage with the Junior Doctors. A series of open meetings have been arranged. On the 11th September the consultants’ committee advised they would be re-entering negotiations and NHS Employers will work with them to progress the implementation for a new contract for implementation in April 2016. The Chief Executive of NHS Employers has written to the Trust regarding Junior Doctor contract reform. On 21 July the health secretary announced that he expected the British Medical Association (BMA) to make a decision on its willingness to work with the government to introduce modernised professional contracts. The Junior Doctors’ Committee have now reached the conclusion that re-entering negotiations is not a possibility for Junior Doctors’ contracts. NHS Employers say they are incredibly disappointed that the BMA continue to stand by their decision to walk away from the talks. The government’s implementation timetable is described as clear by NHS Employers involving:
early implementation of new terms for new consultants from April 2016 (moving existing consultants across by 2017)
The introduction of a new juniors’ contract from the August 2016 intake. Full details can be found in the government’s written ministerial statement: http://www.parliament.uk/business/publications/written-questions-answers-statements/written-statement/Lords/2015-07-16/HLWS128/ following the health secretary’s speech to the King’s Fund: www.nhsemployers.org/news/2015/07/ddrb-report-on-consultants-and-junior-doctors-contract-reform-published?utm_source=DRmail&utm_medium=Email&utm_term=150915&utm_campaign=para5 On Friday 11 September, the Consultants’ Committee advised that they would be re-entering into negotiations and NHS Employers will now work with them to progress the implementation of a new consultants’ contract for implementation in April 2016. NHS Employers will now consider the options available to progress work to implement a new Junior Doctors’ contract in August 2016. The NHS Employers Chief Executive states that he is clear that this implementation needs to be carried out in a manner which is thoughtful and fair, particularly given the highly unusual withdrawal of the JDC. NHS Employers say they are committed therefore to engage with the Junior Doctors and will write to them directly to seek their views on the contract reform. They will also invite them to attend a series of open meetings during October and early November to discuss this important issue with them directly.
13
These actions have led to recent reports in the national media reporting on Junior Doctor responses.
10. Mileage Allowance Review
The NHS Staff Council has agreed that there will be no recovery of overpayments or payment of arrears if mileage allowances change when the latest data on motoring costs is published. This arises from the changed rates being long overdue. In May each year the NHS Staff Council, using the latest information on motoring costs, reviews the rates of reimbursement given to employees who use their privately owned vehicles for NHS business. As National Employers are still waiting for the 2015/16 data to be published, the NHS Staff Council are unable to review these rates. As a result, they have agreed that if there is a change in rates following a review, a date for applying the new rates will be communicated to NHS organisations. They have also confirmed that employers would not be expected to recover overpayments, if rates go down, or calculate arrears, if rates go up. Further reviews scheduled for November 2015 and May 2016 will take place as normal. There would seem to be a likelihood that the National rates will go down. While we have noted this position and appreciate the reason of not retrospectively applying reductions, it is our belief that the May review should take place as soon as possible and not wait until November. We have therefore made contact with NHS Employers to express our concern in the light of pressures on budgets as reflected by the Secretary of State and Monitor communications, as it seems inappropriate to continue paying mileage rates above the costs actually involved with the mileage undertaken. The expected lower national rates may give an opportunity to harmonise the local Dorset HealthCare mileage rates for staff and complete the review of other mileage rates. With no current change in national rates a change in the local mileage rate harmonised up to the national rate would expect to involve an estimated cost of £87k. This would create an unfunded cost pressure if mileage rates are harmonised to the national rate without the scheduled review.
11. Equality, Diversity and Workforce
Equal Pay Audit The provisional results of an equal pay audit have been shared with the Equality and Diversity Steering Group, who arranged the attendance of the independent assessor during September 2015. A detailed action plan is being prepared for consideration by the Executive Team. Workplace Race Equality Standard (WRES) The WRES CCG Supplementary Technical Guidance was published on 20 July 2015 and sets out the framework within which CCG’s and Commissioning Support Unit’s should hold NHS Providers to account and have “due regard” themselves to the WRES. It complements the previous WRES Technical Guidance published in March 2015 (see below) which was primarily directed at NHS Providers. Also published on 20 July 2015 were the following:
WRES FAQs: aimed at addressing various questions raised at the WRES workshops undertaken between March and June 2015;
WRES good practice template: for all providers and CCGs to use as a means of sharing
14
any good practice that is being developed on any of the WRES metrics; and,
WRES Update for July, which captures updates on the development on the WRES programme.
Partnership Events (BiHR) The British Institute of Human Rights - Human Rights Tour 2015 will be coming to Dorset on Monday 5 October 2015. The event has been planned jointly by the Trust and West Dorset District Council and partners from the Dorset Forum for Equality and Diversity. More details about the event will be published in due course. World Mental Health Day 10 October 2015 The Trust has worked in partnership with Bournemouth University to develop a full programme of events in the build up to World Mental Health Day. Events will take place from 5 to 10 October 2015. Black History Month Events 2015 The Trust is supporting two major Black History Month events in Dorset:
10 October 2015 - South West Dorset Multicultural Network, Corn Exchange Dorchester; and,
15 October 2015 – Bournemouth University and Student Union.
A detailed programme confirming speakers and timings will be available soon. Recruitment of Community Development Worker A full time Community Development Worker has been appointed to the Access and Equalities Development Team and all employment checks have been completed. The new post holder has a confirmed started on 14 September 2015.
12. Tricuro
Three Dorset councils have joined forces to create a county-wide Local Authority Trading Company (LATC), the first of its kind in the UK, which will be a partner organisation but may also represent competition for some Trust services. Bournemouth Borough Council, Borough of Poole and Dorset County Council launched the company this summer. Named Tricuro, the company will combine some of the existing adult care services of all three councils, with a budget of over £38m and employing over 1,200 staff. Committed to service improvements and efficiencies in their respective authorities, in 2013, the three councils, along with health partners, formed the ‘Better Together’ partnership, designed to improve health and social care services for adults across Dorset. As well as extending the availability of residential care, home help and other services, the scheme will also generate extra income to reinvest into the company by designing and developing new services. However, unlike a private company, the three councils will hold 100 per cent of the shares in Tricuro and retain strategic control through an Executive Shareholder Group. This group is made up of ten elected members from across all three councils. An interim Chief Executive has been appointed and a Chair is being recruited.
15
Services provided by Tricuro include:
Residential services
Reablement services
Day services
Shared lives
Care catering services
Oh crumbs
Support time and recovery
Training projects
13. Health and Safety - Westminster Hospital, Shaftesbury
The Asbestos Lead has met with the independent expert who has now carried out personal air monitoring in areas which our trade staff will have entered over time. The activities carried out by the surveyors were deemed to simulate the worst case activity that our trade staff would have encountered whilst carrying out maintenance activities in the voids. None of the estimated exposures are likely to have exceeded the control limits averaged over a 4 hour period or the short term maximum exposure limit measured over a 10 minute period. Some exposure to asbestos may have occurred during work activities in one of the voids, but based on the results of personal air monitoring carried out in this area, any exposure would not have been considered to be gross exposure or in significant quantity to cause harm. Employees in question are being notified of this limited potential exposure and a note kept in their personnel records.
14. Staff Survey
Preparation is under way for this year’s staff survey.
The trust has again opted to survey all staff, with the exception of bank employees and those on long term sick leave.
This year we will be adopting a mixed mode approach. Staff with an active trust email address will be able to complete the survey online whilst those without an email address will receive a paper based survey as in previous years. This supports the Trust’s environmental objective.
The survey will commence during the last week of September and will last for 9 weeks. Initial analysis of the responses is expected early in the new year. There have been Governor and Trust Union representative meetings with the Chief Executive and other Directors following last year’s survey. Leadership development investment has increased and developed since the last survey. Air and Share meetings (originally called Listening Events) have been taking place involving the Chief Executive and Directors. There have been Chief Executive meetings with staff in different locations arising from the last Staff Survey. The Practice Development Team has been strengthened with Health Education England funding support. This helps support retention and nurse experience. Information on Learning and Development activities and developments are included in the section below.

16
Trade Union Partnership Forum, Doctors and Dentists Joint Negotiating Forum, Equality and Diversity Steering Group and Health & Safety Committee consideration of the staff survey have all taken place.
15. Learning and Development
Health Education Wessex SHINE awards Health Education Wessex has its annual SHINE awards ceremony in October 2015. The Shine Awards identify outstanding individuals and teams delivering high quality education and training in any healthcare or public health setting across Hampshire, Isle of Wight, Dorset and South Wiltshire. There are 6 categories plus a Chair award. We are delighted to advise that the Trust’s Learning and Development team is one of three finalists nominated for the following 3 awards:
Education and Training Innovation Champion of the Year – for the flexible range of learning offered to staff, with a particular emphasis on the proactive work the mandatory trainers and administrators do in targeting staff and supporting them with accessing a range of flexible options to support teams with completing their mandatory training.
High Performing Education and Training Team of the Year – for the Prevention and Management of Violence and Aggression training team and the excellent work they do on equipping staff with a range of engagement, communication and de-escalation skills and techniques to enable them to recognise and deal with potential aggressive and violent situations using the least restrictive interventions. The aim is to reduce the number of prone restraint interventions which has been achieved over the last year.
Hearing the Patient Voice in Education and Training 2015 – for the collaborative working between the Learning and Development Service and the Recovery Education Centre and local service user groups to embed the patient and carer voice in its education and training provision. Examples of this include:
A one hour patient and carer story on our Corporate Induction which all new starters receive prior to commencing in the workplace. We are also redesigning our Corporate Induction to enhance the co-delivery with patient and carers;
Co-designing and co-delivering a range of clinical, leadership and personal effectiveness programmes.
Enhancing the Quality of Appraisals The Learning and Development Service is working with staff to improve the appraisal process and help staff and appraisers to enhance the quality and experience of the appraisal conversation. An all user survey has been issued to gain feedback from staff on their appraisal experience, and to obtain their suggestions on how the whole experience can be improved. So far 533 completed surveys have been received from staff with over 800 comments on all questions. We are also correlating this with the learning from staff engagement events with the Chief Executive and Directors. From this information re-development of the appraisal intranet page, guidance and updating the Appraisal Policy is taking place. In addition, the appraiser and appraisee training will be tailored to include the suggestions.
17
One-to-one and/or team workplace support to staff on how to record their appraisal conversation is continuing, as well as targeting teams where appraisal completion rates are below the expected threshold to identify what support we can provide. Development Opportunities for Bands 1 – 4 The Learning and Development Service is hosting information and marketing event to showcase all of the learning, education and development opportunities that are on offer to staff across the Trust within Bands 1-4. This supports the Health Education England Widening Participation Agenda, the Talent for Care Partnership Pledge that the Trust has recently signed up to, and forms part of the Trust’s Attraction, Recruitment and Retention Plan. This drop in event will be held at Sentinel House on the 18th September from 11.30am. Reflecting our partnership working with education providers, Bournemouth University, Bournemouth & Poole College, Weymouth College, Kingston Maurward College and union learning reps will all be in attendance on the day, as well as Trust’s Learning & Development staff to discuss a range of topics with staff, including:
o Learning pathways that will provide staff with the academic entry requirements onto pre-registration programmes, including the Bridging programme and Access course
o Salary Support Secondments to University
o Apprenticeships
o Mental Health Diploma
o How the Trust funds Bands 1-4 development opportunities and its link to the Learning Needs Analysis.
o Shadowing opportunities within the Trust
o Leadership & personal effectiveness learning
o Work Related Learning Salary Sacrifice Scheme.
Enhancing Access for Staff into Pre-Registration Programmes From September 2015 the Learning and Development Service is piloting a new Bridging Programme with Bournemouth and Poole College to bridge the gap between National Vocational Qualification/ Qualifications and Credit Framework Level 3 training and pre-registration Nursing or Allied Health Professional training. There will be a screening and recruitment process internal to Dorset HealthCare led by the Learning and Development Service as numbers are limited. However, it is hoped that further cohorts will run in order to assist healthcare support workers move from level 3 training into university and study for degree level healthcare qualifications. This development for enhancing access for support workers has been achieved through collaborations with Health Education Wessex, Bournemouth University and Bournemouth and Poole College. Staff Survey Results - Role Specific Training for Administrative Staff In the 2014 Staff Survey, the feedback received from admin and clerical staff told us that the job relevant learning opportunities accessed by this staff group could be improved. In response to this, and in addition to the Bands 1 – 4 promotional event mentioned above, the Learning and Development Service is putting the spotlight on the wide range of job
18
relevant learning opportunities available to admin staff to support their continuous personal and professional development. These include:
an Administrative Development Programme designed to support staff to deliver a high quality administration service to the organisation;
personal effectiveness opportunities through e-Learning programmes from the South West Learning4Health platform
Line leader prospectus which comprises a range of learning modules which can be completed by admin team leaders and aspiring leaders.
Coaching to support individual development goals of admin staff
The Mental Health Learning Foundation Pathway which admin staff can access where relevant to gain further knowledge and understanding of mental health conditions appropriate to their role.
Nationally recognised Apprenticeships/Qualifications and Credit Framework Diplomas at Level 2 (GCSE equivalent), Level 3 (A level equivalent) or Level 5 (degree level equivalent) in Business Administration, Customer Services and Management.
We are also highlighting the importance of administration staff discussing and agreeing their development needs during their appraisal conversation and throughout the year. Increasing Practice Educator Capacity The Learning and Development Service is pleased to advise that it has recruited into two more of its practice educator roles. These roles have been hard to recruit to, due to the diverse nature of the roles and skill mix required. We now have two practice educators to work with mental health services and three for physical health services in the following areas: pre-registration student and mentor support, preceptorship support, bands 1 – 4 development pathways and to continue to enhance the design and delivery of a diverse range of role specific training for staff. Care Certificate Update As advised in the July Board report, the Care Certificate pilot commences across two sites in September 2015. The two pilot sites have a wide allocation of staff including healthcare support staff and allied health professions within both community health services and mental health. We are very pleased that within the pilot sites we have had volunteers from existing staff as well as for new starters. The pilots in September are providing an opportunity to trial a proposed 3 day induction that focuses on learning and practicing a number of skills in particular, for novice support workers, test out how the self-assessment documents can be used for new starters who already have qualifications or lots of experience in healthcare and evaluate the published workbooks from Health Education England and Skills for Health to benchmark competencies for new support workers. Work has been underway to find assessors in different areas of the Trust to support the pilot, with an introduction session having taken place early September for identified assessors. The pilots will hopefully provide the Trust with the opportunity to analyse the delivery of the Care Certificate before the full role out aimed for January 2016.

19
Creating a Positive Patient Experience As advised in the July Board report, in support of the Trust priorities, and in recognition that administrative staff who work in clinical teams have a powerful impact on the patient experience, we launched a new role specific development opportunity for clinical admin staff entitled: “Creating a Positive Patient Experience”. This has been positively received by staff with all five initial courses being fully booked by August. Additional sessions have been organised to meet the high demand on which staff are already booking. The course is co-designed and co-delivered with Jane Carey from the Recovery Education Centre. The Preceptorship Programme 2015/6 The revised multi-professional Preceptorship programme for 2015/6 is open for applications. The preceptorship describes the initial period of practice for newly registered health professionals. Every preceptee is allocated a mentor or preceptor in their place of work who offers pastoral support, practical guidance and relevant learning opportunities. The Trust supports the preceptorship process by providing six workshops over six months. In line with the Department of Health guidelines, these workshops are used to support the preceptee in their new professional capacity. The guidance also advocates that the preceptorship programme should involve practitioners from other specialisms. This model promotes mutual support and the appreciation of other professional roles which is essential in the provision of integrated services. The workshops include exploring value-based practice, reflective learning, leadership, professionalism and accountability, as well as providing peer and pastoral support. Additionally, there will be some scope to attend medication management, mental health awareness and other generic awareness training if required. There are three cohorts planned, commencing in October 2015, November 2015 and March 2016. Dementia Training The Learning and Development Service has commenced delivery in September 2015 of its new programme of Dementia training for staff working in frontline roles. There are three tiers of training which are designed to provide better care and outcomes for people with dementia through high quality education and training for health and care professionals. This is in line with the national Dementia Strategy. The Trust also has a Dementia CQUIN target for registered staff working in community hospitals and intermediate care services to provide a basic pre-assessment Memory Test to support appropriate referrals into Dementia Services. This Memory Test pre-assessment has been incorporated into the Tier 2 training. Procurement of an E-Learning Platform The Trust is losing access to its two main elearning platforms at the end of March 2016. These two platforms provide staff with access to mandatory training (national learning management system) and continuous professional development (Learning4Health). This provides the Trust with an opportunity to consolidate all its elearning provision and a new system is currently being procured and the selection process will include representatives from clinical services, learning and development, IT and procurement to ensure that a system is purchased that best meets our needs. The objectives for one, consolidated system, is to provide a user friendly experience and be easily accessible by staff, host all

20
elearning content (including e-assessments, videos and podcasts), be interactive and engaging, and record completions directly onto the Trust’s Learning Management System. Learning and Development Reports to Managers Following feedback sought from managers by the Learning and Development Service on its fortnightly suite of Learning and Development reports, it is recognised that the reports are appreciated and have helped people to ensure that staff complete and remain in date with core mandatory training, appraisals and clinical supervision. It is also recognised that people would appreciate the reports being updated more frequently. Listening to this feedback, and working with the Information Management and Technology team, we are pleased to advise that as from the middle of September 2015 we are providing managers with daily reports. This will allow them to receive more accurate and up to date information. The Learning and Development reports have also been updated to make them more user friendly and to include additional information, including staff who are due appraisals for the forthcoming year.
Health Education Wessex Salary Support Arrangements Health Education Wessex spends £8 million per year on salary support secondments. Dorset HealthCare has positively benefited from this funding over the past two years. In 2015/16 we received £472,553 for new salary support students which enabled us to support students commencing both pre-registration education programmes, e.g. adult nursing, mental health nursing, occupational therapy, as well as post-registration programmes, e.g. district nursing, school nursing, health visiting. However, the funding envelope from Health Education Wessex for Dorset HealthCare to support year one salary support secondments in 2016/17 is: £135,717. The impact of this reduction in funding for Dorset HealthCare is that we need to prioritise supporting post-registration salary support programme students in 2016/17, i.e. district nursing, school nursing and health visiting. Commissioning for these programmes is directly informed by Trusts through the salary support scoping exercise and not through the normal commissioning route, due to these staff already being employed by Trusts. Furthermore, the reduction has an impact on the Trust’s recruitment and retention plans for growing our own support workers. We are discussing with Health Education Wessex if there are any further opportunities to use other future funding streams to support growing our own staff through salary support type schemes. Further options will also be considered and discussed as part of the Recruitment and Retention Group. Health Education Wessex has explained that the main reason for the reduction in year one secondment funding for 2016/17 is due to the majority of the funding currently supporting year 2 and 3 students across the region. Another reason is due to the national Health Visiting (HV) funding ending as we are no longer growing the Health Visitor workforce. This funding, which previously inflated the overall salary support budget, has now returned to its usual level. However, we have reported to Health Education Wessex that in response to the national HV programme, we now have larger numbers of Health Visitors to retain due to service growth and members of the workforce retiring, going on maternity leave and returning part time, etc. Health Education Wessex is feeding this through to Health Education England. Furthermore, Health Education England nationally is reviewing arrangements across each of the 13 Local Education Training Boards with a view to harmonisation of salary support rates paid. Health Education England is at a very early stage of this work and the local Health
21
Education England South team will be engaged in national dialogue moving forward and will provide an update on this work and any implications for organisations within Health Education England South in due course. However, it is understood from Health Education Wessex that it is one of the more “generous” Local Education Training Boards for salary support. A suggested hypothesis is that the funding for salary support programmes from 2017/18 onwards could continue to be at a reduced level from what we have experienced over the past two years, to encourage Health Education Wessex to come in line with other Local Education Training Boards.
16. Occupational Health and Wellbeing
Occupational Health (OH) Staffing The OH Service has a nurse vacancy establishment of 3.2 wte, which is 33% of funded establishment. Only 0.8wte is being covered by temporary staff. There is a national shortage of qualified OH nurses and a new faculty of Occupational Health Nursing has been established to address the future training and education of occupational health nursing. Funding was secured through Local Education Training Boards (LETB) for this academic year to support a specialist training post in occupational health nursing. Unfortunately, two internal recruitment processes did not lead to filling the vacancy and it has now been filled via an external vacancy exercise. The successful candidate will complete a BSc (Hons) Specialist Community Public Health Nursing course over 2 years. Further funding is being sought from the LETB to support a post for the academic year 2016/2017. Work volume and staffing levels are having an impact on responses. There is also a 30% increase in new management referrals to Occupational Health in July compared with June. Attention is being given to non-attendance which reduced from 18.5% to 14.3% but there is a concern to reduce this further. Flu Programme The flu programme for staff is due to commence in early October. A flu survey was completed by over 700 staff and a number of key themes were identified which have helped to inform flu planning for this year. These were
17.5% of those vaccinated had the flu vaccine outside and 78% were immunised at GP surgery. Only 30% of those immunised elsewhere advised occupational health, the main reason for not notifying OH was a lack of knowledge that it was important to let OH know.
Two thirds of those completing the survey were immunised last year and 88% intend to be immunised this year.
33% of those who were unvaccinated had wanted the vaccine and the 2 main reasons for not having it were suitability of dates and times of clinics and difficulty getting to a drop in session close to their work location
For those who didn’t want to be vaccinated the main reasons given were not believing the vaccine to be very effective (32%), feeling that a previous vaccine had made them unwell (26%), and a worry about side effects (24%)
49% of staff have identified that having a peer vaccinator at work would make it easier to have the vaccine and 21% felt that having a voucher to allow vaccination at a pharmacy would help
Flu quiz - 55% of staff didn’t know that pregnant women could have the vaccine at any stage of pregnancy, 44% didn’t know that it can take up to 3 weeks post vaccination to develop antibodies, 41% didn’t know that patients with certain health conditions may not respond well to their own flu vaccine.
22
We have worked closely with the communications to develop bespoke branding and communications materials to support the campaign, including payslip leaflets, posters, pop up banners, and t-shirts for ‘The Flu Crew’ our team of vaccinators. A dedicated flu email address has been set up [email protected] to allow staff to contact the OH service during flu season. Additional peer vaccinators have been recruited this year from hospital and in patient units and a ‘roaming vaccinator’ approach will be taken to scheduled visits enabling staff to have the vaccine in their ward or clinical area by a visiting nurse. A number of roaming vaccinators have also been recruited to help support the OH nursing team. Sponsorship for a prize draw has been offered from Tusker one of our salary scheme partners and Unison will also be supporting the campaign this year. Details of the programme will be published on the intranet, internet and via regular and specific messages from communications. Health and Wellbeing The National Institute for Health and Care Excellence has recently published new guidance entitled Workplace Policy and Management Practices to Improve the Health and Wellbeing of Employees A task and finish group has been set up to benchmark the Trust against the recommendations in the guidance and an initial meeting has taken place and actions are being developed to meet any areas of non-compliance. Occupational Health and Organisational Development have agreed to work jointly to develop the employee health and wellbeing agenda, through a health and wellbeing manifesto, which reflects the Public Health Responsibility Deal Pledges, NICE guidance and Workplace Wellbeing Charter and summarises the key aims and objectives for the Trust in improving employee health and wellbeing. A part time employee has been deployed to Occupational Health to support promotion and development of Health at Work initiatives introduced consistent with the Public Health Responsibility Deal Pledges and the HR Strategy. A series of three health and wellbeing summits be organised in December. The aim of the summits will be to engage staff and to develop the employee wellbeing strategy and specific work streams to support the implementation of the strategy.
1
AUDIT COMMITTEE
Minutes of the Audit Committee Meeting
Wednesday 20th May 2015, 0930, Meeting Room 3, Sentinel House
Present: John McBride, Non-Executive Director (Chair)
Nick Yeo, Non-Executive Director
Lynne Hunt, Non-Executive Director
Peter Rawlinson, Non-Executive Director
In attendance: Jackie Chai, Director of Finance
Fiona Haughey, Director of Nursing & Quality
Keith Eales, Board Secretary
Sasha Lewis, Pricewaterhouse Coopers
Anna Blackman, Pricewaterhouse Coopers
Mark Stabb, Director of Audit TIAA
Kevin Goater, Interim Associate Director
Penny Headlam, Chief Financial Accountant
Roger Ringham, Security Management Services
Anna Webb, Governor (Observer)
Chris Balfe, Lead Governor (Observer)
Sandra North, (Minute Taker)
Action
1.
Apologies Karen Travers, Local Counter Fraud Specialist, Sarah Wright, Associate Director of Finance
2
2.1
Minutes of the Meeting held on 20th April 2014 It was agreed that the minutes of the previous meeting were an accurate and true reflection of the meeting subject to the following amendment: Page 6 point 18.1.3 refers “MS said if committee time allowed …” MS to be amended to “KE”
3
3.1
3.2
Matters Arising and Action Tracker Action tracker updated. Action tracker and forward plan to be updated to include actions from today’s meeting.
SN
4.
4.1
4.1.1
Year End Accounts and Reports A Finance
i. Review of final accounts 2014/15 (including summary of key points and movements)
PH presented report. The demise of the PCT led to a large asset transfer and increase in balance sheet last year.
2
4.1.2
4.1.3
4.2
4.2.1
4.2.2
4.2.3
4.2.4
4.2.5
4.2.6
4.2.7
4.2.8
4.3
Locality restructure is reflected in the segmental analysis. Cash has decreased contributed by the deficit position this year.
ii. PwC Report – Draft Report to those charged with governance (ISA260) SL presented the report. The accounts will be signed off next week on receipt of confirmation from Lloyds Bank. PwC have completed all their key audit work. Majority of work completed for the valuation of land and buildings without any issue. There is one query outstanding where there is a slight difference on some land areas compared to figures that have been used. If incorrect the maximum potential area is £693k understated which is not material and PwC would not suggest adjustment (page 10 refers). ACTION Finance to correct for 2015/16. Dilapidations provision of £1.6m at year end across 25 properties. PwC said this was not a material figure from their perspective but the Trust does have a liability here. SL highlighted this is an estimate. To ensure consistency going forward the Trust may want to review how this is being calculated. The Committee agreed it would want to look at this next year. ACTION Associate Director of Estates to arrange independent valuations. ACTION Item to be included on the forward plan for next year. CQUIN will realise full £4.4m and the Clinical Commissioning Group (CCG) have verbally agreed and the Trust has asked for confirmation from the CCG. PwC and the Committee agreed that charitable funds are not consolidated into the accounts. This is not material (£544k net assets and income for year of £300k). Discussion took place regarding related party transactions. PwC do not anticipate any issues that would need to be reported. Audit Committee to assure itself appropriate systems are in place. ACTION Related party transactions to be included on forward plan for later in the year. No significant issues with the Trust securing Economy, Efficiency and Effectiveness. PwC did not need to qualify the accounts this year as has been the case for the last 2 years. This was agreed by their independent board of partners. PR said it would be useful to attach the Going Concern paper which had previously gone to the Board. ACTION Going Concern paper to be provided to the Extraordinary Board by way of reminder. JM tested the points to be raised at Board as follows:
– The final outturn results as reported in the accounts show no significant differences to finance reports the Board has seen throughout the year.
– The financial cash position has reduced in line with expectations. – PWC are satisfied there are no material fraud cases the Committee need to
concern themselves with and a report on fraud is received at each committee meeting.
– The Committee is satisfied with the approach adopted by PwC and with their independence.
– Overseas visitors are not a material item for the Trust. – The Committee is satisfied that PwC have been provided with all relevant
information from the CQC and Monitor. – There are no other significant issues regarding provisions and accruals.
JC
IT SN
SN
JC
3
4.4
4.5
4.5.1
4.6
4.6.1
4.6.2
4.7
4.7.1
4.7.2
4.8
4.8.1
4.8.2
4.9
4.9.1
4.9.2
4.9.3
The Committee was happy to recommend the accounts to the Board subject to a Letter of Representation being provided to the Board by the Chief Executive (see point 4.6.1 below).
iii. Annual Internal Audit Report 2014/15 (includes Head of Internal Audit opinion)
MS presented the report. Overall opinion has moved from limited last year to reasonable assurance this year.
iv. Letter of Representation
AB said the purpose of the Letter of Representation signed by the Chief Executive (CEO) and Chair to PwC was to outline the Trusts responsibilities with respect to the accounts. It confirms the Trust takes responsibility for the preparation and content of the accounts and disclosures contained therein. PR said he was more used to a system whereby the CEO and team write a mirror Letter of Representation to the Board on the basis of which the Board then writes the Letter of Representation to the auditors. Discussion followed and JM will circulate a summarised list of all points discussed and expected to be raised at the Board meeting tomorrow. ACTION JM to prepare and circulate email to committee members. B Annual Report
i. Separate paper from KE summarising key points KE presented report. There is an outstanding matter regarding Code of Governance which the Trust Secretary will action. ACTION KE to complete required action. Board Assurance Framework (BAF) is now in place and the Committee will keep this under review.
C Quality
i. Separate paper from FH summarising key points FH presented report There are two mandated indicators and one selected locally by the Council of Governors. Some further work is required regarding the local indicator (dementia finding question) as staff have responded to the question differently leading to a variation in the outcome.
ii. PwC Report – Draft Long form report to the directors and governors on the Quality Report
PwC provided assurance there were no issues of consistency or content. For the compulsory performance indicator regarding treating patients within 18 weeks from referral, PwC could not form a conclusion. Data was not kept in a way which allowed PwC to check the data and AB outlined the reasons for this. AB said due to Monitor specific calculation directions on this indicator, the calculation cannot be done for any provider and is therefore not an auditable process at the moment. The Trust will not be out of line with other organisations For the third indicator selected locally, data and systems are not sufficiently robust at the moment for PWC to provide assurance on this indicator. This is not part of the audited Quality Report but will be reported to Monitor.
JM
KE

4
4.9.4
4.9.5
Discussion took place and the Quality Performance Group will need to consider what conclusion to draw from the patient perspective and a brief update to be provided to the Committee. ACTION Brief update on progress to be provided to the Committee. JM summarised there was a need for the Committee to review the adequacy of data quality generally. ACTION Item to be added to the forward plan.
FH
SN
5
5.1
5.2
Internal Audit Update inc: Reports & follow ups MS presented the report Focus has been mainly on the Monitor metrics and items reported to the Board. There is now a different approach following the work of the Business and Performance team and the new Data Quality Group which is recognising ownership at local level. This follows the three lines of defence model. For the management of complaints there are two areas of focus:
– Localities to better manage complaints with assistance from the complaints team at HQ
– Better engagement with the complainant throughout the process and the reports being shared across Directorates.
6.
6.1
6.2
6.3
6.4
6.5
6.6
6.7
6.8
6.9
Counter Fraud & Security – Security Management Services Report – IT assets RR presented the report Security Management Services (SMS) were commissioned to conduct an investigation into controls in place following the theft of laptops whilst the Trust was in the process of deploying SystmOne. There were two IT hubs working independently and in different ways and the report contains a number of suggestions for improved working arrangements. JM confirmed that all recommendations made have been agreed. Some recommendations are already implemented and the Trust had demonstrated a positive response to the incident. Discussion took place regarding the issue of data security and PR asked if the processes being proposed would provide assurance around data security. RR said the Trust had very robust policies in place regarding data protection. JC said in the case of the laptops no data had been compromised as they were new and unused. MS confirmed occasional testing of data protection procedures does take place and the report has been shared with the IT auditor. RR said this had been a unique situation. In future equipment which was not going to be used for quite some time would not be ordered and delivered so far in advance. MS will look at the procurement audit scheduled for quarter 3 to include checks on IT equipment ordering and delivery. The Committee commended RR for the quality and content of the SMS report. ACTION Item to be included on the forward plan for the Committee to look at it again before Christmas.
SN
7.
7.1
Governance & Disclosure Board Assurance Framework & Risk Register
5
7.1.1
7.1.2
7.1.3
7.1.4
7.2
7.2.1
7.2.2
7.3
7.3.1
7.3.2
KE presented the report Three risks were highlighted and these had been raised at the Executive Performance and Corporate Risk Group on the 19th May. Closure of Flaghead – this is reported as the highest risk for the Trust but recent Directors discussion has put actions in place to contain and mitigate risks. The risk is therefore not as high as reported. The wording requires refining to accurately reflect the risk. CIP target should be re-scored at amber. Staffing on Chalbury has been scored too high given the action that has been taken and will be rescored as amber. HMRC VAT Loss JC presented the report This has been reported to the March 2015 Board in Part 2. The paper concluded this was an unusual set of circumstances and the probability of a reoccurrence was quite low. The team have improved processes but it was difficult to know if any process would have detected the error. No further actions taken but there has been wider awareness that a set of circumstances can result in the perfect storm. CIP Process/Forward Plan 2016/17 JC presented the report The report was noted and in particular the earlier timetable for 2016/17 CIP planning. JM asked that a draft report be available before Christmas for the Non-Executive Directors. ACTION Action tracker to be updated.
SN
8.
8.1
Minutes of Quality Assurance Committee Meeting held on 20th April 2015 The committee noted the minutes.
9.
9.1
Points to Escalate to the Board JM to prepare the action points from today’s meeting regarding the yearend reports and circulate to the Board before tomorrow’s meeting (point 4.6.2 refers).
10.
10.1
Forward Plan To be updated with items raised today.
SN
11
11.1
Any Other Business None
12.
Date and Time of Meetings in 2015 Monday 20th July 0930–1200 Meeting Room 3, Sentinel Wednesday 21st October 0930–1200 Meeting Room 3, Sentinel
Stages of Excellence: how will we know if we have achieved our Strategic
Goals?
Part 1 Trust Board Meeting 30 September 2015
Author Director of Strategy and Business Development
Sponsoring Board Member Director of Strategy and Business Development
Purpose of Report To propose a framework for assessing achievement of the Strategic
Goals set out in the Trust Strategy 2015 to 2020
Recommendation/Action for Group
The Board is asked to approve the use of the Stages of Excellence Model as a means of recording progress in the delivery of the seven strategic goals.
Engagement and Involvement Consultation with Directors
Previous Board/Committee/s Dates
The assessment framework was discussed previously by the Board in February 2015.
Monitoring and Assurance Summary
This report links to the following Strategic Goals
To provide high quality care; first time, every time;
To be a valued partner and expert in partnership working with Patients, Communities and Organisations;
To be a learning organisation, maximising our partnership with Bournemouth University and promoting innovation, research and evidence based practice;
To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare;
To be a national leader in the delivery of integrated care;
To ensure that all of the Trust’s resources are used in an efficient and sustainable way;
To raise awareness within the Trust and externally of the impact that our work has on people and our environment, and take steps to reduce any negative effects.
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability
Information Management &Technology
Estates
Equality Impact Assessment
Freedom of Information

Page 1 of 3
Stages of Excellence
How will we know if we have achieved our strategic goals?
1. Introduction
1.1 At the January 2015 Board Meeting, the Board approved seven Strategic Goals for the
next five years. The Director of Strategy and Business Development was tasked with designing a means by which the Trust could annually assess progress in delivering these Strategic Goals.
1.2 At the February 2015 meeting a draft dashboard was presented which attempted to collect evidence from a number of different sources to demonstrate delivery of the Strategic Goals.
1.3 The Trust already collects a vast amount of information evidencing service delivery and quality, so where possible the draft measures described in this draft dashboard used information already available.
1.4 However, after discussion, the Board felt that this approach was not ambitious enough and did not capture the challenge the Trust had set itself in setting its strategic objectives. The Directorate was asked to radically rethink the approach.
1.5 This report proposes a different methodology using the Stages of Excellence model to assess strategic progress.
2. Stages of Excellence Model
2.1 In its simplest form, the Stages of Excellence model is a means by which organisations
make statements which describe what excellence would look like for each of their Strategic Goals. The organisation then scores itself out of five, determined over a given period of time, based on how well it has done in delivering against its excellence statements.
2.2 For example, for the Trust strategic goal: To provide high quality care; first time, every
time, excellence could be described in the following ways:
At level 5
All services are rated Outstanding by the CQC
A fully developed and embedded quality management culture to ensure quality is maintained and promoted at all levels in the Trust
Seamless and effective quality management systems are used across the Trust, to systematically identify and escalate operational and strategic risk
At level 3
There are services that are rated as Requiring Improvement by the CQC
There is a quality management culture, however it requires improvement
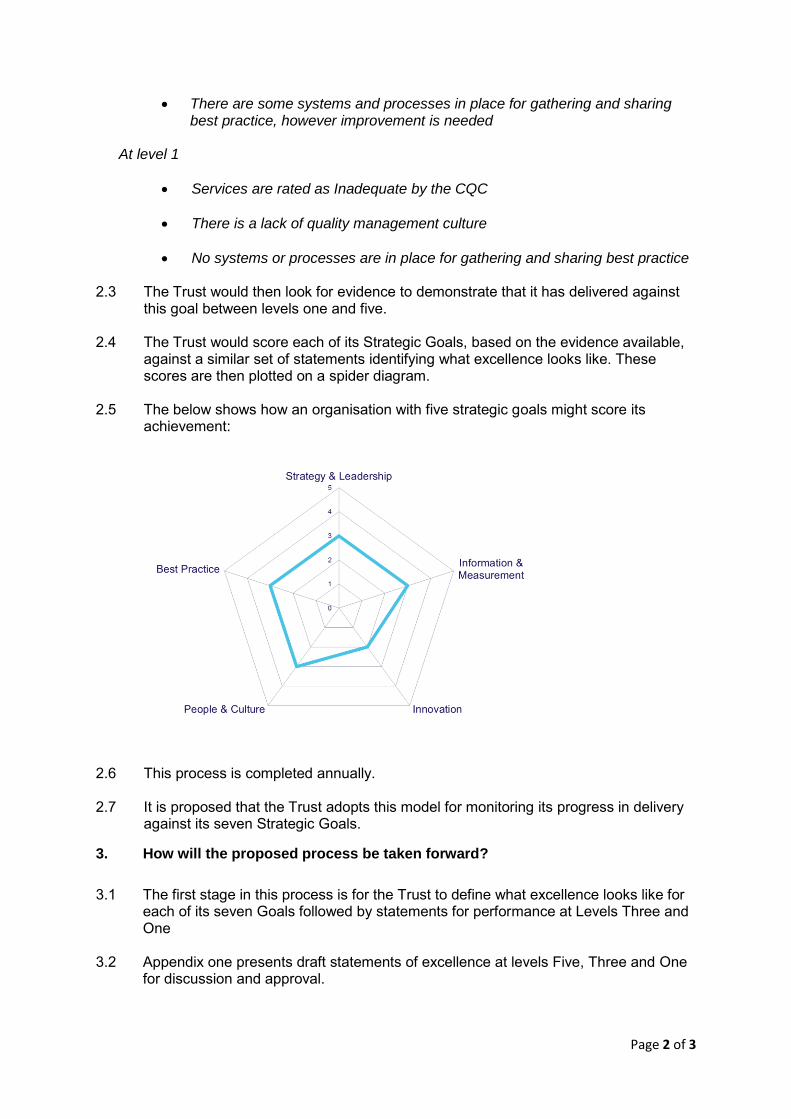
Page 2 of 3
There are some systems and processes in place for gathering and sharing best practice, however improvement is needed
At level 1
Services are rated as Inadequate by the CQC
There is a lack of quality management culture
No systems or processes are in place for gathering and sharing best practice
2.3 The Trust would then look for evidence to demonstrate that it has delivered against this goal between levels one and five.
2.4 The Trust would score each of its Strategic Goals, based on the evidence available,
against a similar set of statements identifying what excellence looks like. These scores are then plotted on a spider diagram.
2.5 The below shows how an organisation with five strategic goals might score its
achievement:
2.6 This process is completed annually. 2.7 It is proposed that the Trust adopts this model for monitoring its progress in delivery
against its seven Strategic Goals.
3. How will the proposed process be taken forward?
3.1 The first stage in this process is for the Trust to define what excellence looks like for
each of its seven Goals followed by statements for performance at Levels Three and One
3.2 Appendix one presents draft statements of excellence at levels Five, Three and One
for discussion and approval.
Page 3 of 3
3.3 Once approved it is proposed that consultation events are undertaken between October and December 2015 with the Governors, Staff, service users and other partners.
3.4 At these events stakeholders will be asked to use the stages of excellence model to
score and provide examples of how the Trust is progressing in delivering against its Seven Strategic Goals.
3.5 This information, along with evidence taken from the Trust`s delivery against key
performance indicators within the Trust’s integrated governance process, will be presented at the February Board for review and scoring of progress. This score will then be recorded on a spider diagram.
3.6 This proposed process will then be completed on an annual basis.
4. Recommendation
4.1 The Board is recommended to approve the use of the Stages of Excellence Model as
described, as a means of recording progress in delivery against the seven Strategic Goals.
Steve Hubbard Director of Strategy and Business Development September 2015
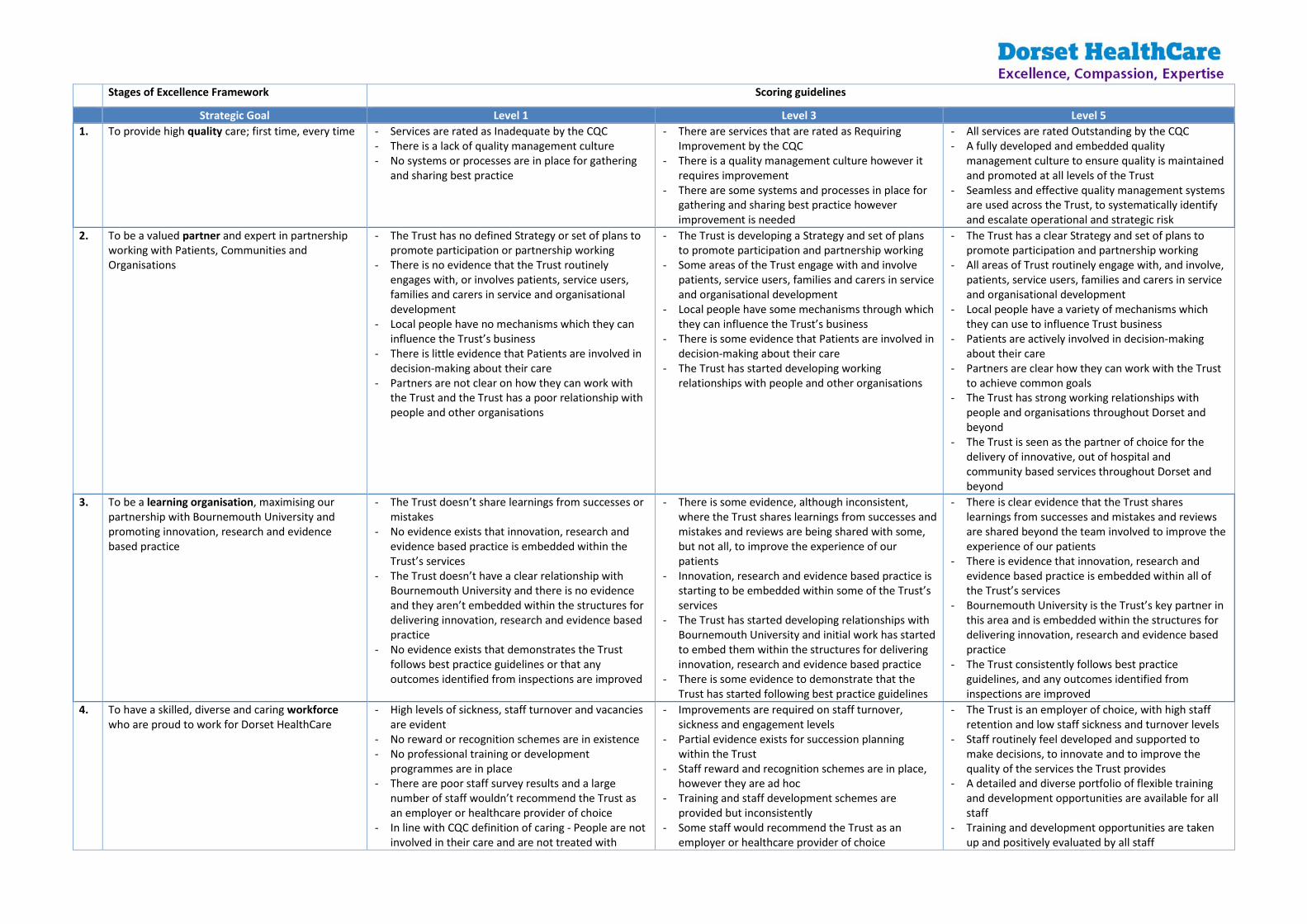
Stages of Excellence Framework Scoring guidelines
Strategic Goal Level 1 Level 3 Level 5
1. To provide high quality care; first time, every time - Services are rated as Inadequate by the CQC - There is a lack of quality management culture - No systems or processes are in place for gathering
and sharing best practice
- There are services that are rated as Requiring Improvement by the CQC
- There is a quality management culture however it requires improvement
- There are some systems and processes in place for gathering and sharing best practice however improvement is needed
- All services are rated Outstanding by the CQC - A fully developed and embedded quality
management culture to ensure quality is maintained and promoted at all levels of the Trust
- Seamless and effective quality management systems are used across the Trust, to systematically identify and escalate operational and strategic risk
2. To be a valued partner and expert in partnership working with Patients, Communities and Organisations
- The Trust has no defined Strategy or set of plans to promote participation or partnership working
- There is no evidence that the Trust routinely engages with, or involves patients, service users, families and carers in service and organisational development
- Local people have no mechanisms which they can influence the Trust’s business
- There is little evidence that Patients are involved in decision-making about their care
- Partners are not clear on how they can work with the Trust and the Trust has a poor relationship with people and other organisations
- The Trust is developing a Strategy and set of plans to promote participation and partnership working
- Some areas of the Trust engage with and involve patients, service users, families and carers in service and organisational development
- Local people have some mechanisms through which they can influence the Trust’s business
- There is some evidence that Patients are involved in decision-making about their care
- The Trust has started developing working relationships with people and other organisations
- The Trust has a clear Strategy and set of plans to promote participation and partnership working
- All areas of Trust routinely engage with, and involve, patients, service users, families and carers in service and organisational development
- Local people have a variety of mechanisms which they can use to influence Trust business
- Patients are actively involved in decision-making about their care
- Partners are clear how they can work with the Trust to achieve common goals
- The Trust has strong working relationships with people and organisations throughout Dorset and beyond
- The Trust is seen as the partner of choice for the delivery of innovative, out of hospital and community based services throughout Dorset and beyond
3. To be a learning organisation, maximising our partnership with Bournemouth University and promoting innovation, research and evidence based practice
- The Trust doesn’t share learnings from successes or mistakes
- No evidence exists that innovation, research and evidence based practice is embedded within the Trust’s services
- The Trust doesn’t have a clear relationship with Bournemouth University and there is no evidence and they aren’t embedded within the structures for delivering innovation, research and evidence based practice
- No evidence exists that demonstrates the Trust follows best practice guidelines or that any outcomes identified from inspections are improved
- There is some evidence, although inconsistent, where the Trust shares learnings from successes and mistakes and reviews are being shared with some, but not all, to improve the experience of our patients
- Innovation, research and evidence based practice is starting to be embedded within some of the Trust’s services
- The Trust has started developing relationships with Bournemouth University and initial work has started to embed them within the structures for delivering innovation, research and evidence based practice
- There is some evidence to demonstrate that the Trust has started following best practice guidelines
- There is clear evidence that the Trust shares learnings from successes and mistakes and reviews are shared beyond the team involved to improve the experience of our patients
- There is evidence that innovation, research and evidence based practice is embedded within all of the Trust’s services
- Bournemouth University is the Trust’s key partner in this area and is embedded within the structures for delivering innovation, research and evidence based practice
- The Trust consistently follows best practice guidelines, and any outcomes identified from inspections are improved
4. To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare
- High levels of sickness, staff turnover and vacancies are evident
- No reward or recognition schemes are in existence - No professional training or development
programmes are in place - There are poor staff survey results and a large
number of staff wouldn’t recommend the Trust as an employer or healthcare provider of choice
- In line with CQC definition of caring - People are not involved in their care and are not treated with
- Improvements are required on staff turnover, sickness and engagement levels
- Partial evidence exists for succession planning within the Trust
- Staff reward and recognition schemes are in place, however they are ad hoc
- Training and staff development schemes are provided but inconsistently
- Some staff would recommend the Trust as an employer or healthcare provider of choice
- The Trust is an employer of choice, with high staff retention and low staff sickness and turnover levels
- Staff routinely feel developed and supported to make decisions, to innovate and to improve the quality of the services the Trust provides
- A detailed and diverse portfolio of flexible training and development opportunities are available for all staff
- Training and development opportunities are taken up and positively evaluated by all staff

compassion. They feel vulnerable and isolated - In line with CQC definition of caring - There are
times when people do not feel well supported or cared for
- Staff would recommend the Trust as an employer or healthcare provider of choice
- Staff engagement and recognition programmes are in place and widely used by staff
- In line with CQC definition of caring - people are truly respected and valued as individuals and are empowered as partners in their care
5. To be a national leader in the delivery of integrated care
- None of the Trust’s services are seen as national exemplars for the delivery of high quality, integrated care
- The Trust isn’t seen as a leader in the provision of integrated care
- The Trust isn’t seen as a natural partner for integration
- The Trust hasn’t developed a track record in the development and delivery of integrated care
- A few of the Trust’s services are seen as national exemplars for the delivery of high quality, integrated care
- Some of the Trust’s services are seen as leaders in the provision of integrated care
- The Trust is starting to be seen at a national level as a leader in the development of integrated care
- The Trust is starting to be seen as a natural partner for integration although improvements are still needed
- The Trust is starting to develop a track record, at a national level, in the development and delivery of integrated care
- A large number of the Trust’s services will be seen as national exemplars for the delivery of high quality, integrated care
- The Trust will be seen as leaders in the provision of integrated care with its staff regularly asked to present on the national stage
- The Trust will increasingly be seen at a national level as a leader in the development of integrated care through the development of partnerships and be seen as a natural partner for integration
- The Trust has a comprehensive and proven track record, at a national level, in the development and delivery of integrated care
6. To ensure that all of the Trust’s resources are used in an efficient and sustainable way
- When benchmarked against other NHS organisations, the Trust is seen in the lower quartile for how it uses its resources in an efficient and sustainable way
- Information is not timely, robust or easily accessible to enable effective decision making to ensure transparency as to the quality of care
- There is no evidence of the Trust harnessing the power of technology to improve efficiencies and productivity in both clinical care and support function pathways
- There is no evidence that the Trust has developed new ways of effective working including appropriate skill mixing opportunities
- When benchmarked against other NHS organisations, the Trust is seen in the middle quartile for how it uses its resources in an efficient and sustainable way
- There is some evidence that information is timely, robust and easily accessible to enable effective decision making to ensure transparency as to the quality of care, but improvements could be made
- There is some evidence of the Trust harnessing the power of technology to improve efficiencies and productivity in both clinical care and support function pathways
- The Trust has started to develop new ways of effective working including skill mixing opportunities
- When benchmarked against other NHS organisations, the Trust is seen in the top of the upper quartile for how it uses its resources in an efficient and sustainable way
- There is excellent provision of timely, robust and easily accessible information to enable effective decision making to ensure transparency as to the quality of care
- The Trust effectively harnesses the power of technology to improve efficiencies and productivity in both clinical care and support function pathways, including improved and interoperable information flows easier and secure access to those that need it
- The Trust has developed new ways of effectively working including appropriate skill mixing opportunities
7. To raise awareness within the Trust and externally of the impact that our work has on people and our environment and take steps to reduce any negative effects
- None of the Trust’s services have an up-to-date impact assessment
- No areas of the business routinely maximise opportunities to utilise electronic workflow channels, available systems, paper reduction and workflow efficiencies
- There is no evidence of the Trust starting to improve the way it engages or involves patients and the public in the work of the Trust; from individual patient experience to collective involvement or by being held to account by those we serve
- There is no evidence to support that the Trust effectively uses its resources to ensure equity of provision across Dorset
- Some of the Trust’s services have an up-to-date impact assessment
- Some areas of the business routinely maximise opportunities to utilise electronic workflow channels, available systems, paper reduction and workflow efficiencies
- The Trust is starting to improve the way that it engages and involves patients and the public in the work of the Trust, from individual patient experience through to collective involvement and being held to account by those we serve
- There is some evidence to support that the Trust effectively uses its resources to ensure equity of provision across Dorset
- All of the Trust’s services have an up-to-date impact assessment with all negative effects of the Trust’s operations being actively managed
- The Trust routinely maximises opportunities to utilise electronic workflow channels, available systems, paper reduction and workflow efficiencies
- There is evidence of improving the way that the Trust engages and involves patients and the public in the work of the Trust, from individual patient experience through to collective involvement and being held to account by those we serve
- The Trust effectively uses its resources to ensure equity of provision across Dorset

1
SIX MONTHLY REVIEW OF INPATIENT NURSE STAFFING ESTABLISHMENT: ENSURING SAFE STAFFING
Part 1 Board Meeting 30 September 2015
Author Roy Plowman, Fiona Haughey, Matthew Chapman, Rachel Wilson, Michaelene Holder-March
Sponsoring Board Member
Fiona Haughey Director of Nursing and Quality
Purpose of Report This paper forms the six month review of nurse staffing in line with the commitment requested by the National Quality Board (2013). This paper focuses on the nursing reviews that have taken place in the last six months with reference to national changes and guidance from NICE, NHS England and Monitor (Foundation Trust Regulator). The paper includes the staffing data relevant for this reporting period. This is the fourth staffing report to the Board.
Recommendation The Board is asked to consider and note:
• The work undertaken to date and the ongoing work to further understand inpatient staffing levels and in community mental health and district nursing services.
• The acuity/dependency in the Community Hospital Inpatients and Older Peoples Mental Health Units from the application of the Safer Staffing Tool.
• The need to further consider and review the funded establishment of the OPMH organic wards.
• Compliance in meeting the national monthly submission of staffing data through the Unify2 system and posting this information on NHS Choices and on the Trust Internet.
• Monitoring of our planned and actual nurse staffing levels has been reported on a monthly basis to the Trust’s Executive Quality and Clinical Risk Group.
• The dependence on bank and agency staffing to meet our staffing shortfalls which poses an operational and financial challenge; however, it is being strategically supported and managed. It is envisaged that the introduction of e-rostering will strengthen and improve off duty planning; safer staffing levels and have a positive impact on variable pay expenditure.
Engagement and Involvement
Previous Committee/s Dates
February 2015 Board Meeting
Monitoring and Assurance Summary
This report links to the � We will deliver high quality, safe patient care
2
following Strategic Objective(s)
� We will support staff to innovate and improve care
� We will work with partners to deliver joined up care closer to home
� We will remain a high performing organisation
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated: Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality �
Board Assurance Framework � �
Risk Register � �
Legal / Regulatory � �
People / Staff � �
Financial / Value for Money / Sustainability � �
Information Management &Technology � �
Equality Impact Assessment � �
Freedom of Information � �

3
EXECUTIVE SUMMARY
The Trust is required to undertake a review of staffing establishments every six months. This is the fourth report to the Board following the initial paper in February 2014 recommending safe staffing levels of the inpatient units. It fulfils the expectation of the National Quality Board requirements for the Trust in relation to safe nurse staffing sections 1,5,6 and 7 (see Appendix1). During the year monthly staffing reports have continued to be presented to the Executive Quality and Risk Group and the Quality Governance Committee informing them of the Trust’s ongoing nursing staff situation. The paper highlights the work to date to review, monitor and agree safe staffing levels on our inpatient wards (mental health and community/intermediate care beds). The major focus of this report is the Community Hospital Wards as the Trust has now undertaken three rounds of the Safe Staffing Tool, including the Care Contact Time which has been used to inform the recommendations within this report. The Additional funding of £430,715 for Community Hospital inpatient wards Jersey, Guernsey wards (Alderney Hospital), Langdon and Ryeberry wards (Bridport Hospital) and Radipole ward (Westhaven Hospital) approved by the Board in February 2015 has now been used to increase the nursing establishment.
Key Points:
• The Trust has continuously worked to establish a position on safe staffing using
various methods to capture both numbers of patients per nurse, planned and actual staffing by registered and non-registered nurses on a daily basis and acuity/dependency levels. There are no nationally defined minimum safe staffing levels for community or intermediate care inpatient units. This is also the case for Mental Health services although NICE Guidance on safe staffing of mental health wards was expected in the autumn. Professional judgement alongside any recognised tools for acuity continue to be utilised.
• Since the report to the Board in February 2015 further work has been undertaken relating to staffing levels and acuity for all physical health wards and three older peoples organic mental health wards.
• The Community Hospital wards have established safe staffing levels partly through
using the Safer Nursing Care Tool and by professional judgement and consideration of the other skills available to the wards, e.g. Occupational Therapy and Physiotherapy. The fourth review took place from 13th July to 7th August 2015. The initial results show six wards where the nursing requirements exceed the funded establishment. Once all results are interpreted a separate paper will outline overall findings and be presented to a future Executive Risk and Clinical Quality Group meeting.
• Three organic Older People’s Mental Health wards (Chalbury, St Brelades and Herm) and the two functional Older People’s Mental Health wards Alumhurst and Melstock have been included in the Safer Staffing Tool exercise for the period mentioned above.
• During May and June 2015 two wards (Flaghead Unit, May 2015 and Haven Ward
June 2015) have been closed – one temporarily. The staff working on these wards
4
were redeployed thus assisting staffing levels on other wards. Haven reopened after a refurbishment in late August with the staff returning to this Unit.
• The additional 16 intermediate/rehabilitation care beds at St Leonard’s Community Hospital (Canford Ward) to support the winter pressures on the Acute Hospital Trusts has remained open to date. The ward is reporting planned and actual staff on a shift
by shift basis as with all the other wards.
• On 4th June 2015 the government suspended NICE (the National Institute for Health and Care Excellence) from producing further guidance on safe staffing levels in the NHS. Simon Stevens, Chief Executive NHS England has requested Jane Cummings, Chief Nurse NHS England, to incorporate nurse workforce planning into the 5 year forward plan initiatives.
• At the same time the NHS Mental Health Staffing Framework and the Acute Mental Health Multiplier tool were launched. The Framework focuses on mental health inpatient care, and was commissioned as part of the NHS England’s ‘Compassion in Practice programme’. The framework provides support in seeking organisational assurance and describes how to complete a workforce analysis. The mental health staffing framework is focused on:
o psychological rather than physical care o personal and user behavioural risks o giving less emphasis to environmental risks or infection control.
• A separate paper is being prepared outlining the impact of implementation of the framework within our mental health wards. This report will be presented to a future Board meeting.
• The Trust is compliant in meeting the national expectation of submitting staffing data through the Unify system and posting this information on NHS Choices. This is also posted on the Trust website. The latest data at the time of producing this report (July 2015) indicates where the average fill rate for registered nurses falls short of 100% there is an over establishment of non-registered nurses. The data also identifies where the fill rate is above 100%. This is due to patients requiring additional support and a higher ratio of nurses to support their needs. The Executive Dashboard at the end on this report shows a summary of the wards falling below thresholds between February and July 2015. See Appendix 3
• During the period covered by this report work is ongoing to progress the transition from using the local RAG Tool to full reliance on the E-rostering system to generate the monthly staffing report. The revised date for the monthly staffing report to be compiled using the e-rostering system is September 2015 (August data). The first staffing report using e-rostering data will presented to Executive Quality and Risk Group in October 2015.
• The Board is asked to consider this information and the work that is ongoing to further understand the staffing requirements of the wards using the evidence based tools, professional judgement and other data as it becomes available.
• A quality priority for 2015/16 is to understand the staffing requirements for our community services, specifically Community Mental Health Teams and District Nursing Team and this work is in progress. Additionally specific work has taken
5
place within the Health Visitor workforce to agree caseload sizes according to deprivation and geography. This being implemented in line with the health visitor call to action programme.
1. BACKGROUND
1.1 Following a number of high profile national reviews and reports it is clear that a key
determinant of high quality care is having the right staff with the right skills and competencies to meet patient needs. This paper outlines the ongoing work to ensure that the Trust is both aware of current staffing levels and has information to determine if these are the correct levels to deliver safe care.
1.2 This is the fourth report to Board. This report aims to update the Board on progress
made since the third report and to outline recommendations for the future. The Trust is required to undertake a review of staffing establishments every six months.
1.3 Since the first report to the Board in February 2014, an additional investment of just
under £1.2 million has been made to staffing across our inpatient wards. 1.4 The paper looks at all inpatient areas across the Trust and the focus for
recommendations is within the Community Hospitals and Older People’s Mental Health wards.
2. PREVIOUS REVIEWS
2.1 The Trust provides inpatient services for elderly care rehabilitation / medicine and
mental health patients across 32 wards with a capacity of up to 535 beds. See
Appendix 2.
2.2 Current ward staffing for all inpatient units is illustrated in Appendix 2.
2.3 The first two staffing reports highlighted a need for investment in staffing within our mental health inpatient wards. The last (third) report outlined the need to invest in the Trust’s physical health wards. On all previous occasions the Board agreed with the recommendations and the finances made available to recruit to the areas identified. To date the allocated funds have been used to increase staffing levels.
3. REVIEW OF THE RECOMMENDED STAFFING LEVELS
3.1 Recognising the significant challenge to retain staff and attract new staff to the Trust
has a strong focus on Human Resources workforce development, retention and recruitment. Different approaches have been taken including relocation expenses, attending job fairs, radio advertising and advertising in various publications. The Trust is also working alongside other local trusts to look at joint recruitment initiatives. The staffing challenge to the Trust is recognised as a risk and included in the Board Assurance Framework/Corporate Risk Register.
3.2 The National Institute for Health and Care Excellence (NICE) states that having more
than eight patients to one nurse on a ward in the day should act as a trigger for checking if care was being compromised. This guidance was issued in July 2014 and was targeted at adult inpatient wards in acute hospitals.
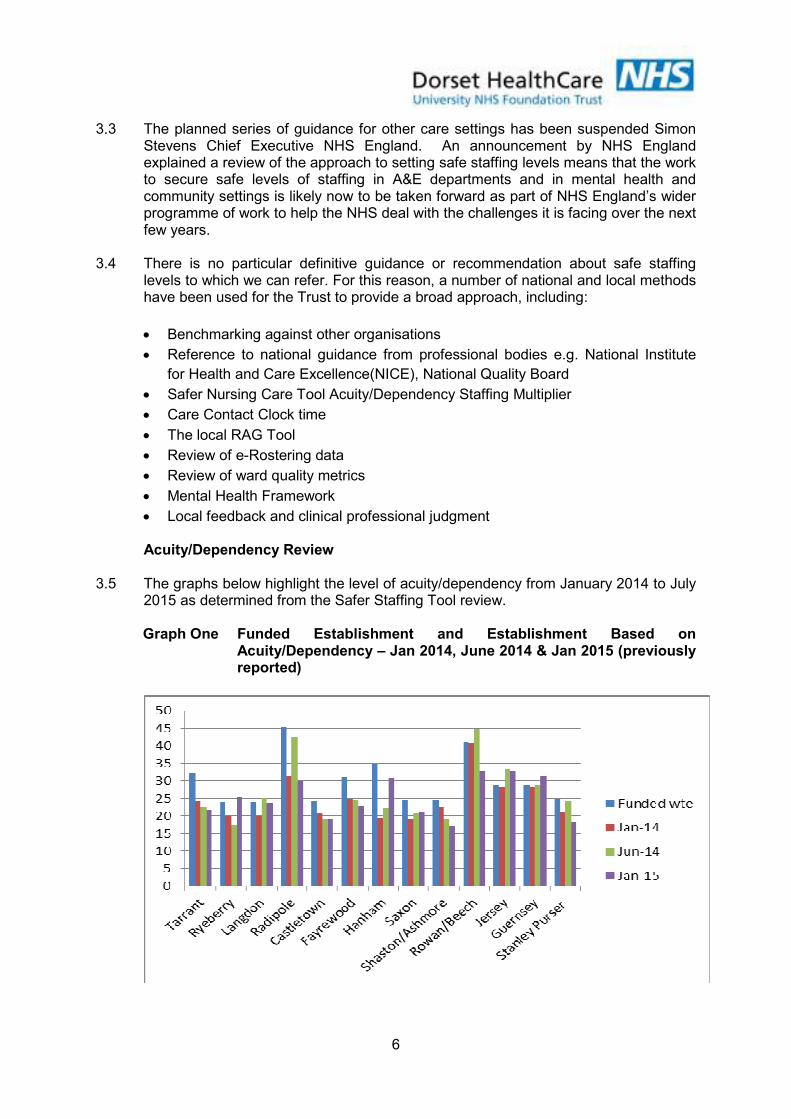
6
3.3 The planned series of guidance for other care settings has been suspended Simon Stevens Chief Executive NHS England. An announcement by NHS England explained a review of the approach to setting safe staffing levels means that the work to secure safe levels of staffing in A&E departments and in mental health and community settings is likely now to be taken forward as part of NHS England’s wider programme of work to help the NHS deal with the challenges it is facing over the next few years.
3.4 There is no particular definitive guidance or recommendation about safe staffing
levels to which we can refer. For this reason, a number of national and local methods have been used for the Trust to provide a broad approach, including:
• Benchmarking against other organisations
• Reference to national guidance from professional bodies e.g. National Institute
for Health and Care Excellence(NICE), National Quality Board
• Safer Nursing Care Tool Acuity/Dependency Staffing Multiplier
• Care Contact Clock time
• The local RAG Tool
• Review of e-Rostering data
• Review of ward quality metrics
• Mental Health Framework
• Local feedback and clinical professional judgment Acuity/Dependency Review 3.5 The graphs below highlight the level of acuity/dependency from January 2014 to July
2015 as determined from the Safer Staffing Tool review. Graph One Funded Establishment and Establishment Based on
Acuity/Dependency – Jan 2014, June 2014 & Jan 2015 (previously reported)
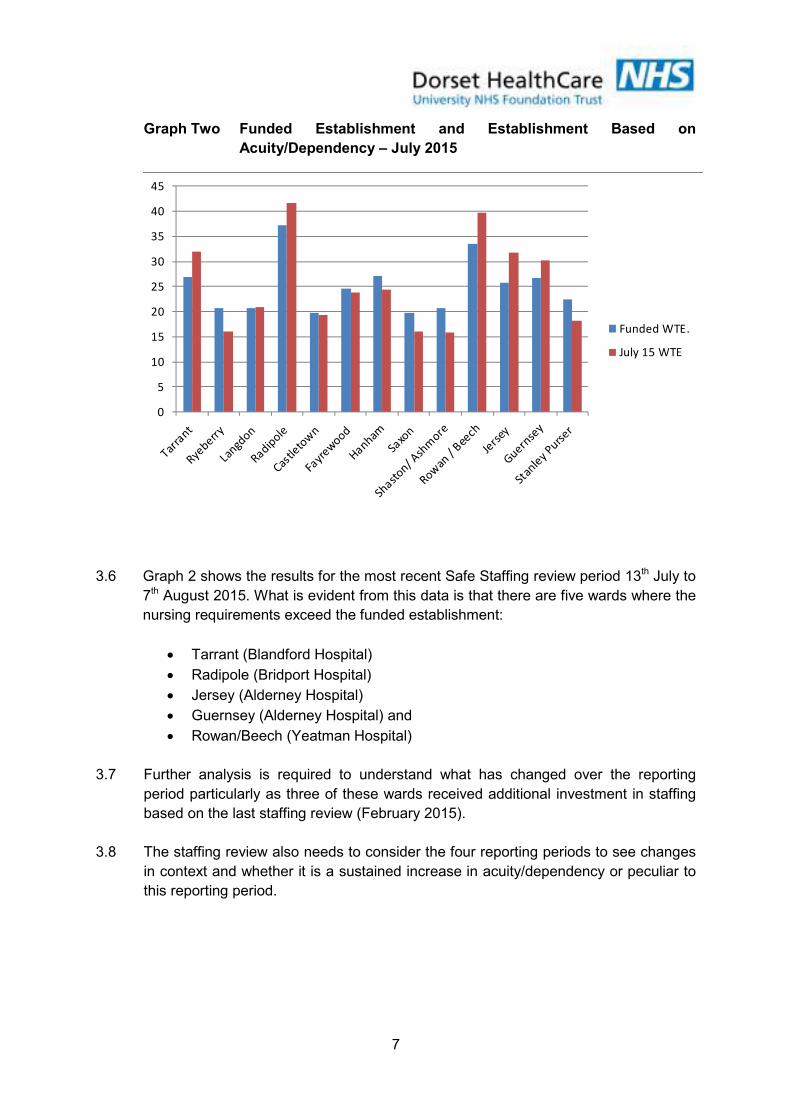
7
Graph Two Funded Establishment and Establishment Based on
Acuity/Dependency – July 2015
0
5
10
15
20
25
30
35
40
45
Funded WTE.
July 15 WTE
3.6 Graph 2 shows the results for the most recent Safe Staffing review period 13th July to
7th August 2015. What is evident from this data is that there are five wards where the
nursing requirements exceed the funded establishment:
• Tarrant (Blandford Hospital)
• Radipole (Bridport Hospital)
• Jersey (Alderney Hospital)
• Guernsey (Alderney Hospital) and
• Rowan/Beech (Yeatman Hospital)
3.7 Further analysis is required to understand what has changed over the reporting
period particularly as three of these wards received additional investment in staffing
based on the last staffing review (February 2015).
3.8 The staffing review also needs to consider the four reporting periods to see changes
in context and whether it is a sustained increase in acuity/dependency or peculiar to
this reporting period.

8
Graph Three Funded Establishment and Establishment Based on
Acuity/Dependency – OPMH organic wards Jan 2015
Graph Four Funded Establishment and Establishment Based on
Acuity/Dependency – OPMH organic wards July 2015
0
5
10
15
20
25
30
35
40
45
50
Herm Ward St Brelades Chalbury Ward
Funded WTE.
July 15 WTE
3.9 Graph one demonstrates that within the OPMH organic wards the funded
establishment exceeded the acuity/dependency requirement of the patients. This
was the first time this tool was used on these wards and it is recommended to use
the tool for at least three reporting cycles before any determinations can be reliably
made.
3.10 Graph 2 shows the results from the reporting period 13th July to 7th August 2015.
What is evident from this data is that there is one ward where the nursing
requirements exceed the funded establishment. (St Brelades). Herm and Chalbury
wards highlighted the funding establishment to be far in excess of the
acuity/dependence of the patients during the reporting period.
3.11 For the organic older people’s wards Chalbury and Herm, the same acuity scoring
was applied as for the community hospital inpatient wards. St Brelades Ward,
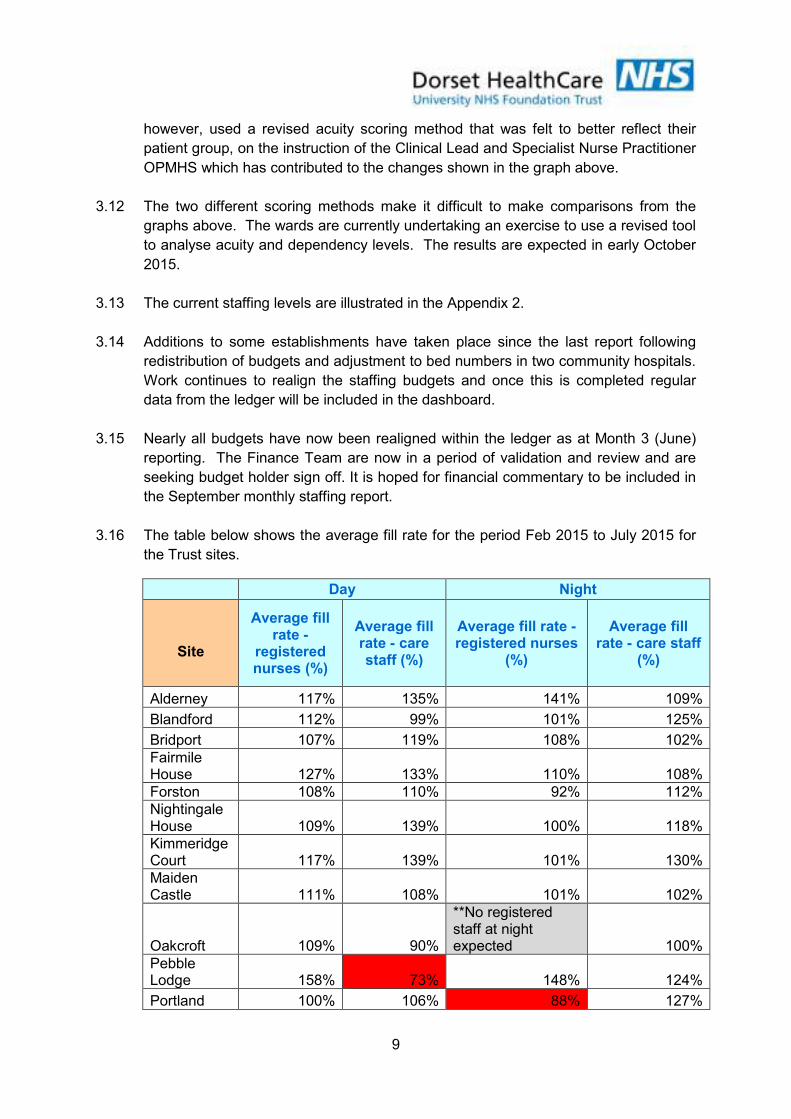
9
however, used a revised acuity scoring method that was felt to better reflect their
patient group, on the instruction of the Clinical Lead and Specialist Nurse Practitioner
OPMHS which has contributed to the changes shown in the graph above.
3.12 The two different scoring methods make it difficult to make comparisons from the
graphs above. The wards are currently undertaking an exercise to use a revised tool
to analyse acuity and dependency levels. The results are expected in early October
2015.
3.13 The current staffing levels are illustrated in the Appendix 2.
3.14 Additions to some establishments have taken place since the last report following
redistribution of budgets and adjustment to bed numbers in two community hospitals.
Work continues to realign the staffing budgets and once this is completed regular
data from the ledger will be included in the dashboard.
3.15 Nearly all budgets have now been realigned within the ledger as at Month 3 (June)
reporting. The Finance Team are now in a period of validation and review and are
seeking budget holder sign off. It is hoped for financial commentary to be included in
the September monthly staffing report.
3.16 The table below shows the average fill rate for the period Feb 2015 to July 2015 for
the Trust sites.
Day Night
Site
Average fill rate -
registered nurses (%)
Average fill rate - care staff (%)
Average fill rate - registered nurses
(%)
Average fill rate - care staff
(%)
Alderney 117% 135% 141% 109%
Blandford 112% 99% 101% 125%
Bridport 107% 119% 108% 102%
Fairmile House 127% 133% 110% 108%
Forston 108% 110% 92% 112%
Nightingale House 109% 139% 100% 118%
Kimmeridge Court 117% 139% 101% 130%
Maiden Castle 111% 108% 101% 102%
Oakcroft 109% 90%
**No registered staff at night expected 100%
Pebble Lodge 158% 73% 148% 124%
Portland 100% 106% 88% 127%

10
Day Night
Site
Average fill rate -
registered nurses (%)
Average fill rate - care staff (%)
Average fill rate - registered nurses
(%)
Average fill rate - care staff
(%)
St Anns 112% 113% 102% 115%
St Leonards 101% 100% 99% 98%
Swanage 107% 106% 181% 69%
Victoria Hospital 117% 118% 101% 142%
Wareham Hospital 104% 114% 109% 125%
Westhaven 112% 113% 80% 131%
Westminster 104% 103% 175% 63%
Weymouth Hospital 103% 98% 137% 83%
Yeatman Hospital 102% 122% 108% 99%
3.17 Wards generally meet the determined local staffing levels. However, where there are occasions when the number of registered nurses are lower than expected, the number of non-registered nurses are increased to compensate for this ensuring a safe staff environment exists for patient safety.
3.18 Investments in staffing in 2014/15 have also improved the planned staffing ratios at
night however there remains 2 sites, Portland and Westhaven where the percentage of registered nurses is below 90%. On both these sites the number of non-registered nurses was increased to compensate for this. There is ongoing recruitment of registered nurses in these areas and they are difficult areas to recruit to due to location / geography.
4. CARE CONTACT TIME
4.1 The “Safer Staffing: A Guide to Care Contact Time” was issued by the Chief Nursing Officer on the 26 November 2014. The guideline recognises that a range of elements make up the role of the nurse. All of these are important in ensuring that the patient
receives the best possible quality of care. NICE guidelines recommend monitoring and action to ensure patients are receiving ‘the nursing care and contact time they need’ with the emphasis on ‘safe patient care, not the number of available staff’. There has been much debate regarding the need to go beyond the numbers to determine ‘safe’ staffing levels.
4.2 It is noted that whilst a significant element of nursing staff time should be spent
providing direct care, such as patient hygiene, this needs to be balanced with indirect patient care (meeting family, carer’s, liaison meeting and record keeping).
4.3 The guide to Care Contact Time is endorsed by the National Quality Board (NQB).
The expectation is for commissioners and providers to optimise nursing, midwifery
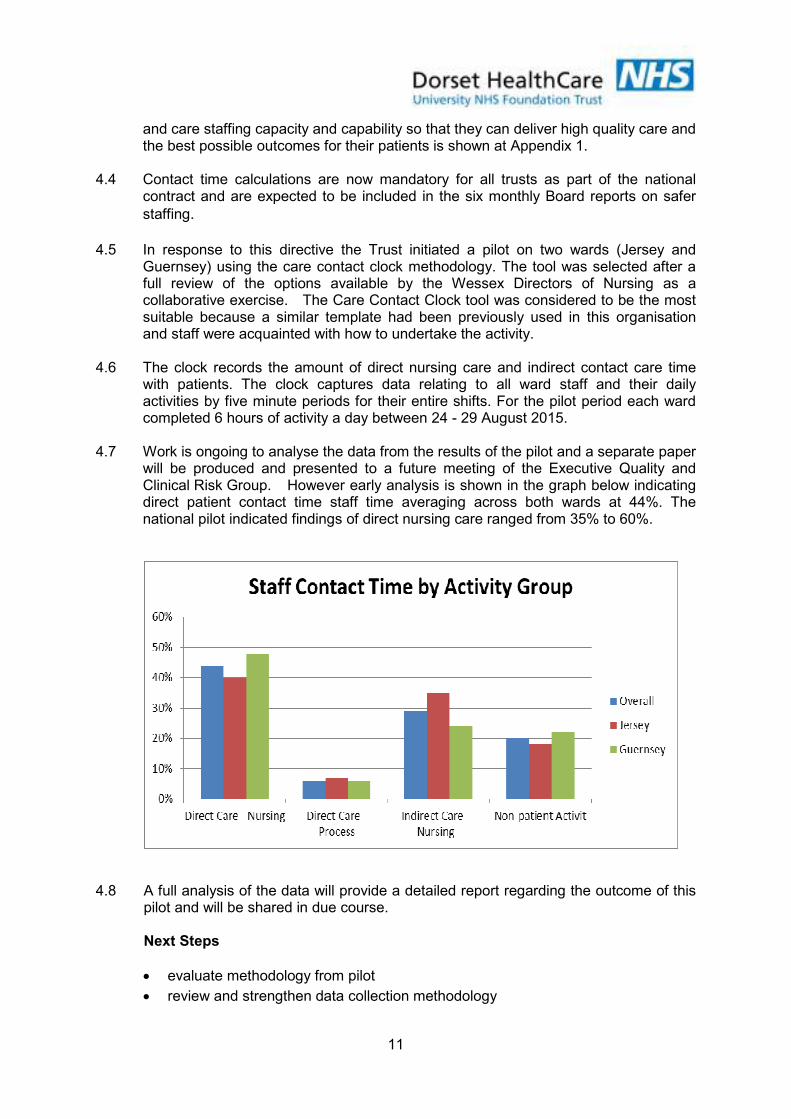
11
and care staffing capacity and capability so that they can deliver high quality care and the best possible outcomes for their patients is shown at Appendix 1.
4.4 Contact time calculations are now mandatory for all trusts as part of the national
contract and are expected to be included in the six monthly Board reports on safer
staffing. 4.5 In response to this directive the Trust initiated a pilot on two wards (Jersey and
Guernsey) using the care contact clock methodology. The tool was selected after a full review of the options available by the Wessex Directors of Nursing as a collaborative exercise. The Care Contact Clock tool was considered to be the most suitable because a similar template had been previously used in this organisation and staff were acquainted with how to undertake the activity.
4.6 The clock records the amount of direct nursing care and indirect contact care time
with patients. The clock captures data relating to all ward staff and their daily activities by five minute periods for their entire shifts. For the pilot period each ward completed 6 hours of activity a day between 24 - 29 August 2015.
4.7 Work is ongoing to analyse the data from the results of the pilot and a separate paper
will be produced and presented to a future meeting of the Executive Quality and Clinical Risk Group. However early analysis is shown in the graph below indicating direct patient contact time staff time averaging across both wards at 44%. The national pilot indicated findings of direct nursing care ranged from 35% to 60%.
4.8 A full analysis of the data will provide a detailed report regarding the outcome of this pilot and will be shared in due course.
Next Steps
• evaluate methodology from pilot
• review and strengthen data collection methodology

12
• consider use on mental health wards and other community inpatient wards
• the findings to be reported within the 6 monthly staffing reports to Trust Board
5. VACANCIES AND RECRUITMENT
5.1 There is still a shortfall nationally of registered mental health nurses (RMN) against a backdrop of all Trusts nationally increasing their establishments. Health Education England is currently reviewing the workforce requirements and provision to increase nurse training places. The Trust has recognised the significant challenges to retain staff and attract new staff and has invested the workforce development plan through active retention and recruitment. Furthermore, the issue of staffing is recognised as a risk and included in the Board Assurance Framework/Corporate Risk Register.
5.2 Details of vacancy figures can be seen on the February to August 2015 Summary at Appendix 2. 5.3 The Older People’s Mental Health wards continue to have the highest level of
vacancies. The service is exploring creative solutions and utilising temporary staffing where there are gaps. There is also a need to understand the staffing levels required on these wards as they may be staffed to a higher level than required for the acuity/dependency of their patients.
5.4 A total of 36 mental health students, who were on placement with the Trust, were due to qualify from Bournemouth University in September 2015. As a new initiative the Trust offered a guaranteed job to students on successful completion of the programme.
5.5 From the 36 students 19 (53%) have been appointed to substantive posts within the
Trust. 6 staff (32%) have gone to OPMH wards The following table shows the wards where these staff have been appointed to.
Recruited To Ward Numbers
Alumhurst Dudsbury Seaview St Anns (Other) Melstock Waterston Linden Chalbury Herm Community Teams
2 3 2 3 1 2 1 2 1 2
Total 19
5.6 Seven of the students withdrew from this process and ten did not engage for a
number of reasons.
5.7 As a result of this process and feedback from the students the Trust has learned
valuable insights as to how to improve this process and to potentially retain more of
the mental health graduate nurses and this will be developed and improved for 2016.
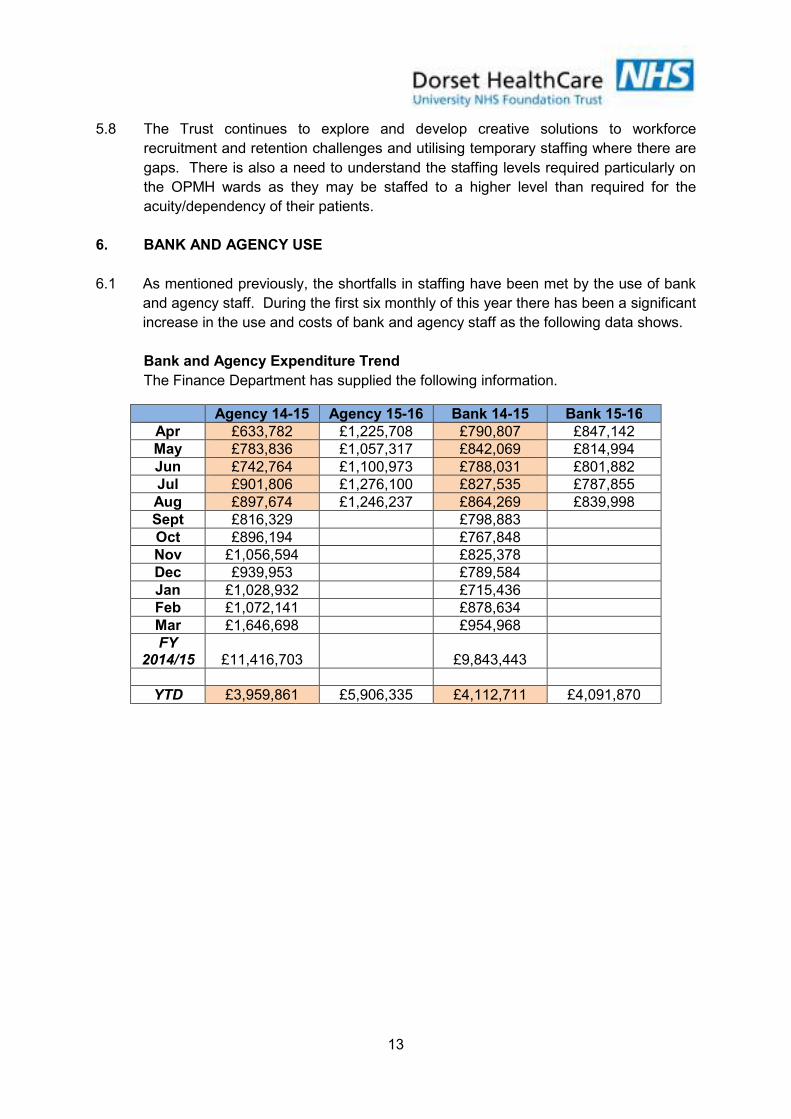
13
5.8 The Trust continues to explore and develop creative solutions to workforce
recruitment and retention challenges and utilising temporary staffing where there are
gaps. There is also a need to understand the staffing levels required particularly on
the OPMH wards as they may be staffed to a higher level than required for the
acuity/dependency of their patients.
6. BANK AND AGENCY USE
6.1 As mentioned previously, the shortfalls in staffing have been met by the use of bank
and agency staff. During the first six monthly of this year there has been a significant
increase in the use and costs of bank and agency staff as the following data shows.
Bank and Agency Expenditure Trend
The Finance Department has supplied the following information.
Agency 14-15 Agency 15-16 Bank 14-15 Bank 15-16
Apr £633,782 £1,225,708 £790,807 £847,142
May £783,836 £1,057,317 £842,069 £814,994
Jun £742,764 £1,100,973 £788,031 £801,882
Jul £901,806 £1,276,100 £827,535 £787,855
Aug £897,674 £1,246,237 £864,269 £839,998
Sept £816,329 £798,883
Oct £896,194 £767,848
Nov £1,056,594 £825,378
Dec £939,953 £789,584
Jan £1,028,932 £715,436
Feb £1,072,141 £878,634
Mar £1,646,698 £954,968
FY 2014/15 £11,416,703 £9,843,443
YTD £3,959,861 £5,906,335 £4,112,711 £4,091,870
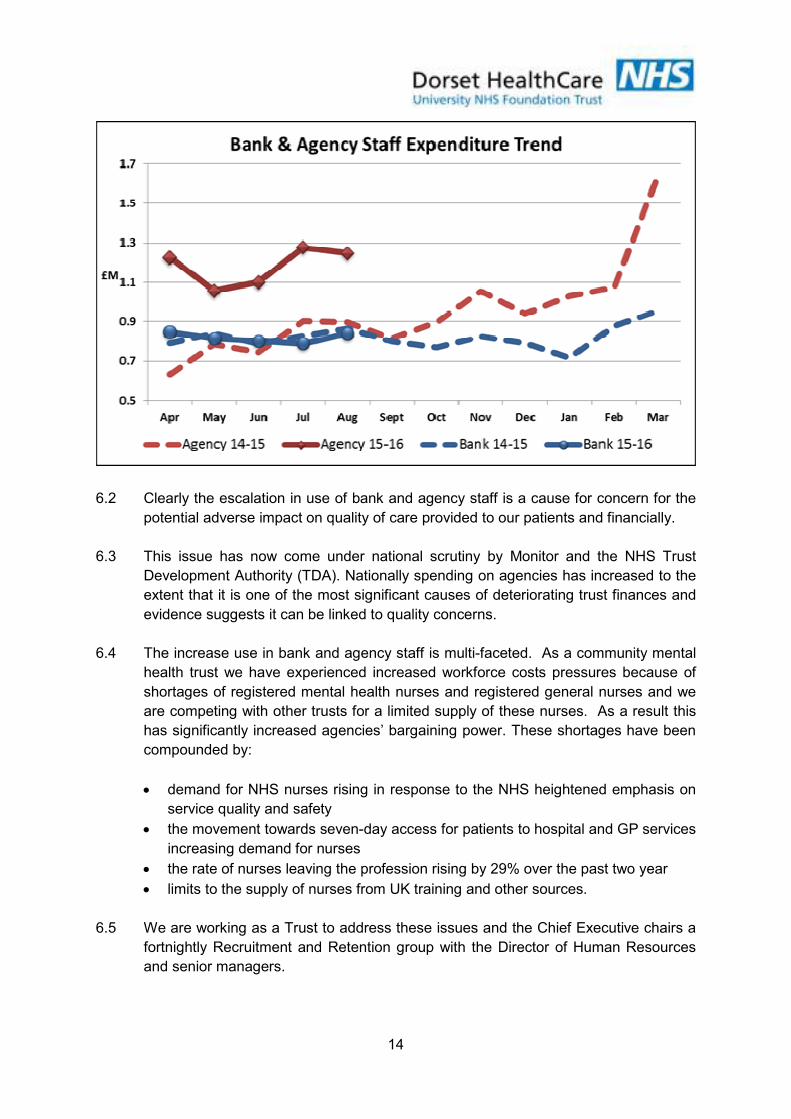
14
6.2 Clearly the escalation in use of bank and agency staff is a cause for concern for the
potential adverse impact on quality of care provided to our patients and financially.
6.3 This issue has now come under national scrutiny by Monitor and the NHS Trust
Development Authority (TDA). Nationally spending on agencies has increased to the
extent that it is one of the most significant causes of deteriorating trust finances and
evidence suggests it can be linked to quality concerns.
6.4 The increase use in bank and agency staff is multi-faceted. As a community mental
health trust we have experienced increased workforce costs pressures because of
shortages of registered mental health nurses and registered general nurses and we
are competing with other trusts for a limited supply of these nurses. As a result this
has significantly increased agencies’ bargaining power. These shortages have been
compounded by:
• demand for NHS nurses rising in response to the NHS heightened emphasis on
service quality and safety
• the movement towards seven-day access for patients to hospital and GP services
increasing demand for nurses
• the rate of nurses leaving the profession rising by 29% over the past two year
• limits to the supply of nurses from UK training and other sources.
6.5 We are working as a Trust to address these issues and the Chief Executive chairs a
fortnightly Recruitment and Retention group with the Director of Human Resources
and senior managers.

15
6.6 More recently we have been informed by Monitor that as from 19 October 2015, we
will be required to comply with new agency spending rules, namely:
• an annual ceiling for total nursing agency spending for each trust, and
• mandatory use of approved frameworks for procuring agency staff.
6.7 We are also required to meet a reducing trajectory for the use of agency nurses to a
maximum of 6% by March 2016. We have submitted the proposed plan and actions
to Monitor as to how this could be achieved.
7. WORKFORCE AND DATA QUALITY
Unify2 Return
7.1 All trusts are required to submit information to the Department of Health on a monthly
basis regarding planned versus actual inpatient nursing staffing. The submission
includes the number of planned hours by ward for the month, split by registered
nursing staff and non-registered staff and split by day and night. This provides details
of average ‘fill rates’ per ward to provide a guide on where staffing levels either
exceed or are below expected/planned levels. A copy of the return and analysis is
included in the monthly staffing report to the Executive Quality and Clinical Risk
Group and uploaded on the Trust website.
Monthly Data and Escalation Tool
7.2 Staff input details of staff on duty on a shift by shift basis into the Trust’s Ward
Monitoring RAG tool. This enables the Trust to collect data and highlight to
managers any issues with staffing levels/skill mix. The monthly staffing report to the
Executive Quality and Clinical Risk Group includes details of internal significant
staffing events, use of agency staff, incidents, complaints and patient friends and
family test results. The report also provides additional details of issues and action
been taken on wards with less than 85% of shifts in the month staffed to expected
levels.
7.3 In the event of a staffing issue the ward complete an adverse incident form to
highlight the issue and any potential risks to patient safety. These reports are
monitored and reviewed by the Associate Director of Nursing and Quality and contact
will be made with the ward to understand the issue emerging as required.
EWTT/QUEST
7.4 The Early Warning Trigger Tool and the expanded version called the Quality,
Effectiveness and Safety Trigger Tool (QuESTT) are used within inpatient and
community areas. The tools help to identify where there may be a potential for
deteriorating standards of care. They are completed by wards on a monthly basis
and include a number of questions and a score is derived from the responses given.
Each tool has a threshold score at which action should be taken to address the
issues identified. The tools include questions relating to staffing i.e. no or new line
management, vacancy rates, unfilled shifts, sickness absence, use of ‘stranger staff’.
16
The results are provided to localities to help them identify areas where further
support/action may be needed.
Quality Dashboard
7.5 The localities receive monthly quality dashboards which provide details of a large
number of metrics both at a locality level and ward level, which allows triangulation of
a range of information. These are to be replaced by the new ward/team to board
quality metrics as from April 2015.
8. CONCLUSION AND RECOMMENDATIONS
8.1 The Trust continues to review and monitor the staffing establishments on the
inpatient wards and work is progressing to understand the staffing requirements
within community nursing teams (mental health, health visiting and district nursing).
8.2 The Trust continues to be challenged with recruitment and retention issues and is
constantly working to improve this position.
8.3 The Board is asked to consider and note:
• The work undertaken to date and the ongoing work to further understand
inpatient staffing levels and in community mental health and district nursing
services.
• The acuity/dependency in the Community Hospitals Inpatient and Older Peoples
Mental Health Units from the application of the Safer Staffing Tool.
• The need to further consider and review the funded establishment of the OPMH
organic wards.
• Compliance in meeting the national monthly submission of staffing data through
the Unify2 system and posting this information on NHS Choices and on the Trust
website.
• Monitoring of our planned and actual nurse staffing levels has been reported on
a monthly basis to the Trust’s Executive Quality and Clinical Risk Group.
• The dependence on bank and agency staffing to meet our staffing shortfalls
which poses an operational and financial challenge; however, it is being
strategically supported and managed. It is envisaged that the introduction of e-
rostering will strengthen and improve off duty planning; safer staffing levels and
have a positive impact on variable pay expenditure.

Appendix 1
17
National Board Quality Expectations
Expectations
What does this mean in practice?
DHC Position – August 2015
Boards take full responsibility for the quality of care provided to patients, and as a key determinant to quality, take full collective responsibility for nursing, midwifery and care staffing capacity and capability
Includes all aspects of board reporting and monitoring of establishments, actual and day to day staffing levels Emphasis on hours monitoring included as part of the NICE guidance and the requirements for uploading information to NHS Choices
In place - Board report presented monthly since June 2014
Processes are in place to enable staffing establishments to be met on a Shift to Shift basis.
Executive team should ensure that policies and systems are in place, such as eRostering and escalation policies
In place – daily monitoring through staffing meetings in site, eRostering implemented – to consider upgrade to new version of e-Rostering which will include ‘safe care’ module
Evidence based tools are used to inform nursing, midwifery and care staffing capacity and capability
Use of proven methodologies and triangulation with professional judgement for setting staff levels
In place – Benchmarking, Safer Nursing Care Tool, Contact Care Time and professional judgement utilised as part of the 6 monthly staffing reviews
Clinical and managerial leaders foster a culture of professionalism and responsiveness where staff feel able to raise concerns
Encourages working in well-functioning teams supported by appropriate infrastructure and support model Emphasises need for open culture to report shortfall Staff-side organisations have a role
In place – incidents received, monitored and themed monthly Staffside involved in staffing review groups.
A multi-professional approach is taken when setting nursing, midwifery and care staffing establishments
Directors of Nursing and Quality lead the process of reviewing staffing requirements and ensure that there is a process in place actively involves, matrons, sisters, charge nurses, or team leaders. Also that they work closely with Medical Directors, Directors of Finance, Workforce (HR), Operations and Learning and Development recognising interdependencies between staffing and other aspects of the organisation’s functions.
In place – broadened to involve more ward leaders in the review meetings. Also locality Directors and locality managers are involve in ensuring safe staffing establishments
Nurses, midwives and care staff have sufficient time to fulfil responsibilities that are additional to their direct caring duties
Recommendation on adequate Headroom (no percentages stipulated) Recommendations on supervisory time for ward leaders (no time stipulated)
The Trust is currently using 23% headroom in the recent realignment of budgets. This may be subject to review. Supervisory time for ward leaders (no time stipulated)
7. Boards receive monthly updates on workforce information, staffing capacity and capability is discussed at public Board meeting at least every six months on the basis of full nursing and midwifery establishment review.
Monthly reports to go to board detailing actual staffing levels against establishment for the previous month – highlighting hotspot areas. Six monthly establishment reviews to go to open board for discussion and debate
In place – Board report presented monthly since June 2014. 6 monthly review - ongoing
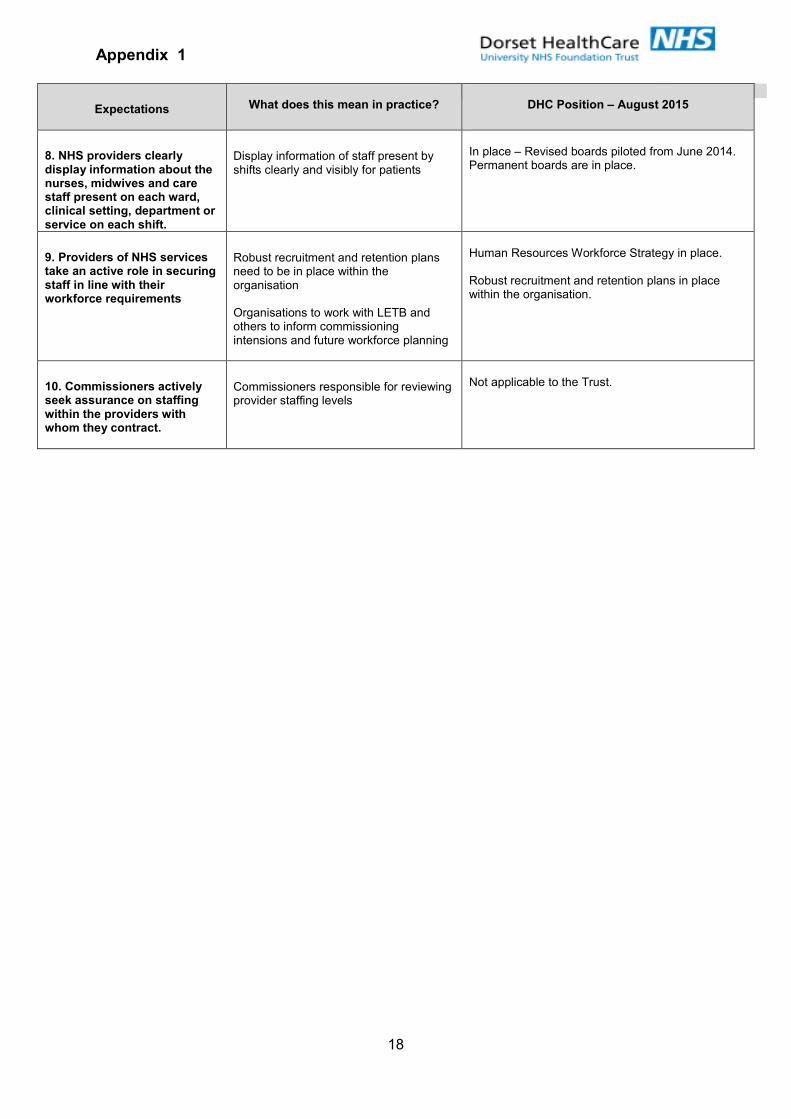
Appendix 1
18
Expectations
What does this mean in practice?
DHC Position – August 2015
8. NHS providers clearly display information about the nurses, midwives and care staff present on each ward, clinical setting, department or service on each shift.
Display information of staff present by shifts clearly and visibly for patients
In place – Revised boards piloted from June 2014. Permanent boards are in place.
9. Providers of NHS services take an active role in securing staff in line with their workforce requirements
Robust recruitment and retention plans need to be in place within the organisation Organisations to work with LETB and others to inform commissioning intensions and future workforce planning
Human Resources Workforce Strategy in place. Robust recruitment and retention plans in place within the organisation.
10. Commissioners actively seek assurance on staffing within the providers with whom they contract.
Commissioners responsible for reviewing provider staffing levels
Not applicable to the Trust.
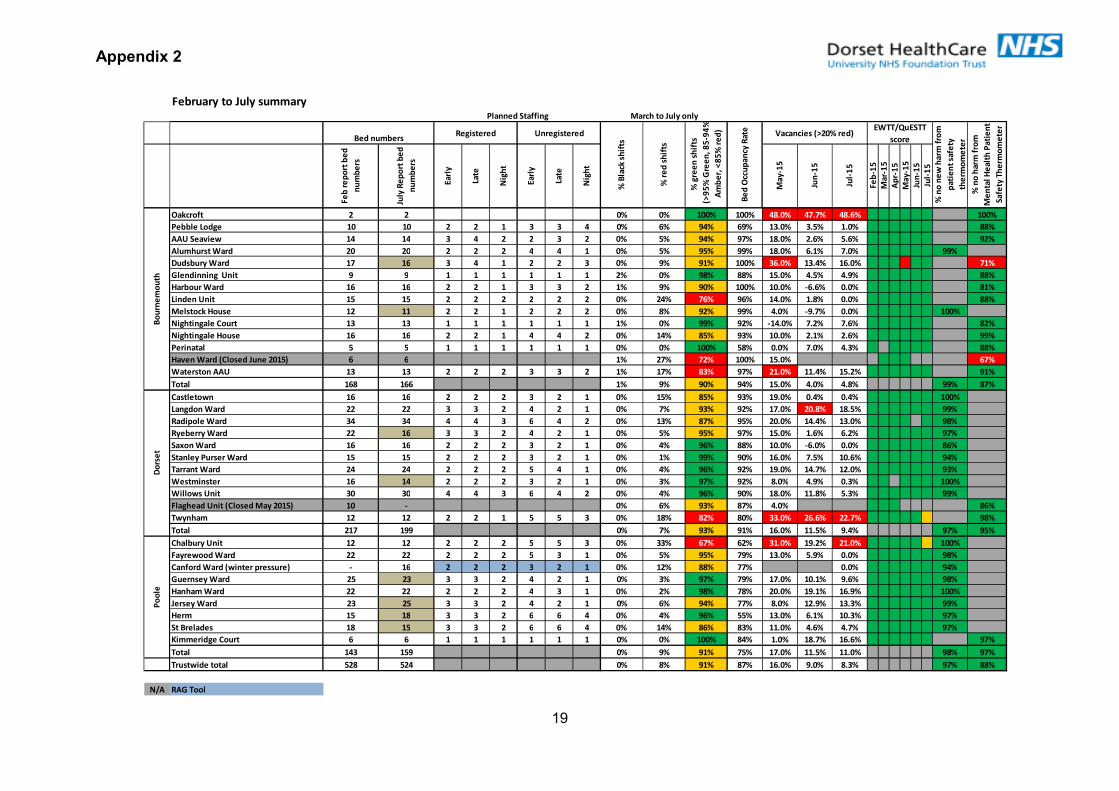
Appendix 2
19
February to July summary
Fe
b r
ep
ort
be
d
nu
mb
ers
July
Re
po
rt b
ed
nu
mb
ers
Ea
rly
Late
Nig
ht
Ea
rly
Late
Nig
ht
Ma
y-1
5
Jun
-15
Jul-
15
Fe
b-1
5
Ma
r-1
5
Ap
r-1
5
Ma
y-1
5
Jun
-15
Jul-
15
Oakcroft 2 2 0% 0% 100% 100% 48.0% 47.7% 48.6% 100%
Pebble Lodge 10 10 2 2 1 3 3 4 0% 6% 94% 69% 13.0% 3.5% 1.0% 88%
AAU Seaview 14 14 3 4 2 2 3 2 0% 5% 94% 97% 18.0% 2.6% 5.6% 92%
Alumhurst Ward 20 20 2 2 2 4 4 1 0% 5% 95% 99% 18.0% 6.1% 7.0% 99%
Dudsbury Ward 17 16 3 4 1 2 2 3 0% 9% 91% 100% 36.0% 13.4% 16.0% 71%
Glendinning Unit 9 9 1 1 1 1 1 1 2% 0% 98% 88% 15.0% 4.5% 4.9% 88%
Harbour Ward 16 16 2 2 1 3 3 2 1% 9% 90% 100% 10.0% -6.6% 0.0% 81%
Linden Unit 15 15 2 2 2 2 2 2 0% 24% 76% 96% 14.0% 1.8% 0.0% 88%
Melstock House 12 11 2 2 1 2 2 2 0% 8% 92% 99% 4.0% -9.7% 0.0% 100%
Nightingale Court 13 13 1 1 1 1 1 1 1% 0% 99% 92% -14.0% 7.2% 7.6% 82%
Nightingale House 16 16 2 2 1 4 4 2 0% 14% 85% 93% 10.0% 2.1% 2.6% 99%
Perinatal 5 5 1 1 1 1 1 1 0% 0% 100% 58% 0.0% 7.0% 4.3% 88%
Haven Ward (Closed June 2015) 6 6 1% 27% 72% 100% 15.0% 67%
Waterston AAU 13 13 2 2 2 3 3 2 1% 17% 83% 97% 21.0% 11.4% 15.2% 91%
Total 168 166 1% 9% 90% 94% 15.0% 4.0% 4.8% 99% 87%
Castletown 16 16 2 2 2 3 2 1 0% 15% 85% 93% 19.0% 0.4% 0.4% 100%
Langdon Ward 22 22 3 3 2 4 2 1 0% 7% 93% 92% 17.0% 20.8% 18.5% 99%
Radipole Ward 34 34 4 4 3 6 4 2 0% 13% 87% 95% 20.0% 14.4% 13.0% 98%
Ryeberry Ward 22 16 3 3 2 4 2 1 0% 5% 95% 97% 15.0% 1.6% 6.2% 97%
Saxon Ward 16 16 2 2 2 3 2 1 0% 4% 96% 88% 10.0% -6.0% 0.0% 86%
Stanley Purser Ward 15 15 2 2 2 3 2 1 0% 1% 99% 90% 16.0% 7.5% 10.6% 94%
Tarrant Ward 24 24 2 2 2 5 4 1 0% 4% 96% 92% 19.0% 14.7% 12.0% 93%
Westminster 16 14 2 2 2 3 2 1 0% 3% 97% 92% 8.0% 4.9% 0.3% 100%
Willows Unit 30 30 4 4 3 6 4 2 0% 4% 96% 90% 18.0% 11.8% 5.3% 99%
Flaghead Unit (Closed May 2015) 10 - 0% 6% 93% 87% 4.0% 86%
Twynham 12 12 2 2 1 5 5 3 0% 18% 82% 80% 33.0% 26.6% 22.7% 98%
Total 217 199 0% 7% 93% 91% 16.0% 11.5% 9.4% 97% 95%
Chalbury Unit 12 12 2 2 2 5 5 3 0% 33% 67% 62% 31.0% 19.2% 21.0% 100%
Fayrewood Ward 22 22 2 2 2 5 3 1 0% 5% 95% 79% 13.0% 5.9% 0.0% 98%
Canford Ward (winter pressure) - 16 2 2 2 3 2 1 0% 12% 88% 77% 0.0% 94%
Guernsey Ward 25 23 3 3 2 4 2 1 0% 3% 97% 79% 17.0% 10.1% 9.6% 98%
Hanham Ward 22 22 2 2 2 4 3 1 0% 2% 98% 78% 20.0% 19.1% 16.9% 100%
Jersey Ward 23 25 3 3 2 4 2 1 0% 6% 94% 77% 8.0% 12.9% 13.3% 99%
Herm 15 18 3 3 2 6 6 4 0% 4% 96% 55% 13.0% 6.1% 10.3% 97%
St Brelades 18 15 3 3 2 6 6 4 0% 14% 86% 83% 11.0% 4.6% 4.7% 97%
Kimmeridge Court 6 6 1 1 1 1 1 1 0% 0% 100% 84% 1.0% 18.7% 16.6% 97%
Total 143 159 0% 9% 91% 75% 17.0% 11.5% 11.0% 98% 97%
Trustwide total 528 524 0% 8% 91% 87% 16.0% 9.0% 8.3% 97% 88%
N/A RAG Tool
March to July only
Bo
urn
em
ou
thD
ors
et
Po
ole
Registered Unregistered
% B
lack
sh
ifts
Planned Staffing
Bed numbers
% n
o h
arm
fro
m
Me
nta
l H
ea
lth
Pa
tie
nt
Sa
fety
Th
erm
om
ete
r
% n
o n
ew
ha
rm f
rom
pa
tie
nt
safe
ty
the
rmo
me
ter
% r
ed
sh
ifts
% g
ree
n s
hif
ts
(>9
5%
Gre
en
, 8
5-9
4%
Am
be
r, <
85
% r
ed
)
Be
d O
ccu
pa
ncy
Ra
te Vacancies (>20% red)EWTT/QuESTT
score
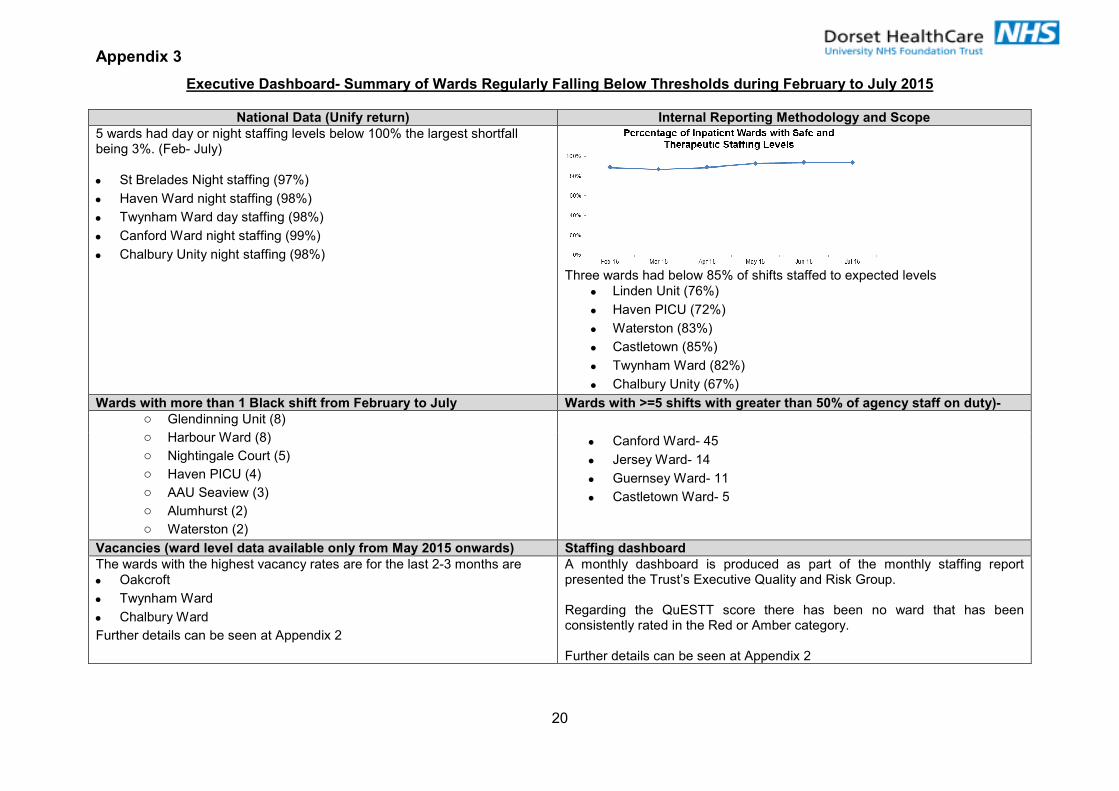
Appendix 3
20
Executive Dashboard- Summary of Wards Regularly Falling Below Thresholds during February to July 2015
National Data (Unify return) Internal Reporting Methodology and Scope
5 wards had day or night staffing levels below 100% the largest shortfall being 3%. (Feb- July)
• St Brelades Night staffing (97%)
• Haven Ward night staffing (98%)
• Twynham Ward day staffing (98%)
• Canford Ward night staffing (99%)
• Chalbury Unity night staffing (98%)
Three wards had below 85% of shifts staffed to expected levels
• Linden Unit (76%)
• Haven PICU (72%)
• Waterston (83%)
• Castletown (85%)
• Twynham Ward (82%)
• Chalbury Unity (67%)
Wards with more than 1 Black shift from February to July Wards with >=5 shifts with greater than 50% of agency staff on duty)- o Glendinning Unit (8)
o Harbour Ward (8)
o Nightingale Court (5)
o Haven PICU (4)
o AAU Seaview (3)
o Alumhurst (2)
o Waterston (2)
• Canford Ward- 45
• Jersey Ward- 14
• Guernsey Ward- 11
• Castletown Ward- 5
Vacancies (ward level data available only from May 2015 onwards) Staffing dashboard
The wards with the highest vacancy rates are for the last 2-3 months are
• Oakcroft
• Twynham Ward
• Chalbury Ward
Further details can be seen at Appendix 2
A monthly dashboard is produced as part of the monthly staffing report presented the Trust’s Executive Quality and Risk Group. Regarding the QuESTT score there has been no ward that has been consistently rated in the Red or Amber category. Further details can be seen at Appendix 2
1
Occupational Health, Safety and Wellbeing Annual Report
2014 – 2015
Part 1 Board Meeting 30 September 2015
Author Beverley Griggs, Associate Director, Occupational Health, Safety and
Wellbeing
Sponsoring Board Member Colin Hague, Human Resources Director
Purpose of Report To provide a summary of health, safety and wellbeing activities
during 2014-15
Recommendation The Board is asked to Note the report
Engagement and
Involvement Staff, Stakeholders and Community Groups
Previous Board/Committee
Dates N/A
Monitoring and Assurance Summary
This report links to
the Strategic Goals
To provide high quality care; first time, every time; To be a learning organisation, maximising our partnership with
Bournemouth University and promoting innovation, research and evidence based practice;
To have a skilled, diverse and caring workforce who are proud to work for Dorset HealthCare;
To be a national leader in the delivery of integrated care; To ensure that all of the Trust’s resources are used in an efficient
and sustainable way; To raise awareness within the Trust and externally of the impact that
our work has on people and our environment, and take steps to reduce any negative effects.
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated: Yes
Any action required?
Yes
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability
Information Management &Technology
Equality Impact Assessment N/A N/A N/A
Freedom of Information
2
Dorset HealthCare
Annual Occupational Health,
Safety and Wellbeing Report
2014/15 August 2015

3
CONTENTS
Item Title Page
1.0 Introduction 3
2.0 Health & Safety Arrangements
Structure
Duties
Health & Safety Committee (HSC)
3
3
4
4
3.0 Key Activities and Achievements 2013/14
Policies
Training
Violence & Aggression Group
5
5
5
7
4.0 Health & Safety Incident Report 8
5.0 RIDDOR 8
6.0 Health & Safety Team Site Visits 9
7.0 Prison Healthcare Units 9
8.0 Ligature Management Plans 10
9.0 Workplace Assessments of Health & Safety 10
10.0 Fire 11
11.0
12.0
13.0
14.0
15.0
16.0
Health & Safety Workplan 2015/16
Occupational Health and Wellbeing Service
Services and Customers
Services Activity
Wellbeing Activity
Occupational Health Workplan 2015/2016
12
13
13
14
16
17
17.0
18.0
Appendix
1
Employee Assistance Programme
Conclusion
Organisational Chart
18
18
19
Appendix
2
Detailed Trend Analysis for 2014/15 20
Appendix
3
RIDDOR Data 21
4
1.0 Introduction
1.1 This is the third annual Occupational Health and Safety report for Dorset HealthCare and has been prepared to provide a summary of health and safety and occupational health activities and trends for 1 April 2014 to 31 March 2015.
1.2 The Trust remains committed to protecting and promoting the health, safety and wellbeing of all staff, service users, carers, visitors and others who may be affected by its activities.
1.3 The Trust aims to foster a positive and proactive occupational health and safety culture, where safety is everyone’s responsibility and is supported by effective communication, training, employee involvement and adequate consultation.
1.4 In the period covered by this report, no visits have been made by the Health
and Safety Executive (HSE) and no enforcement action has been taken.
1.5 During the reporting period there have been very positive developments in managing violence and aggression with a reduction in incidents.
1.6 An area for development in 2015/16 contained within the HR Strategy is improving employee health and wellbeing to reflect the Public Health agenda.
2.0 Health and Safety Arrangements 2.1 Structure 2.1.1 The Health and Safety Team remains part of the Human Resources
Directorate and works closely with all localities, Estates Management, safety representatives and services to promote health and safety.
2.1.2 The Director of Human Resources is the nominated Director responsible for
Health and Safety within the Trust providing the direct link to the Board for the Health and Safety Committee. The health and safety and occupational health teams report directly to the Associate Director for Occupational Health, Safety and Wellbeing.
2.1.3 The Trust Health and Safety Team has a wide range of qualifications and
experience. This has been enhanced with one team member having passed their Level 6 NEBOSH Diploma, and another working towards a Level 6 NVQ in Occupational Health and Safety.
2.1.4 The structure of the teams is outlined in Appendix 1. It is planned to engage
a security management specialist direct rather than through Secure which is more cost effective and should further assist developments in this area during 2015/16.
5
2.2 Duties
2.2.1 The Health and Safety Team is responsible for:
Providing assurance to the Board that the Trust is compliant in matters relating to Health and Safety;
Providing an Annual Health and Safety Report to the Board;
Leading and assisting in the development and review of the Health and Safety Policy and supporting policies and procedures;
Reviewing new legislation and regulations and advising The Trust regarding the implementation of any required changes;
Reporting as necessary under the Reporting of Injuries, Diseases and Dangerous Occurrences Regulations 2013 (RIDDOR);
Consultation with and provision of competent advice to management and staff on Health and Safety matters including the development and maintenance of records such as risk assessments and safe systems of work;
Overseeing and collating the annual self-audit programme and undertaking a structured plan of workplace audits and visits to collect information in relation to training, risk assessments, information provision and record keeping;
Liaising with the HSE and other external bodies;
Developing, providing and supporting health and safety training for all staff within the Trust (including e-learning packages);
Providing regular updates from the Health and Safety Committee to the Board.
2.2.2 The Associate Director of Occupational Health and Wellbeing is responsible
for the Health and Safety Team and has a target for 2015/16 of improving Dorset HealthCare employees’ health and wellbeing consistent with the Public Health agenda and National Health Pledges.
2.3 Health and Safety Committee 2.3.1 The Health and Safety Committee has been constituted in accordance with
the Safety Representatives and Safety Committees Regulations 1977 (as amended) to ensure employee representation by recognised trade unions in matters relating to health and safety; and the Health and Safety (Consultation with Employees) Regulations 1996 (as amended) for those employees that are not in a trade union. The Health and Safety Committee meets on a quarterly basis and includes representation from the Health and Safety Team, Learning & Development, Occupational Health, Security, Fire, Estates and other key Directorate areas.
2.3.2 The Committee operates in partnership with the Trade Unions and is chaired
alternately by the Director of Human Resources and a representative of the Unions.
2.3.3 The membership and key functions of the Committee are clearly outlined in
the Health and Safety Committee Terms of Reference.

6
2.3.4 The Health and Safety Committee reports to the Executive Quality and
Clinical Risk Group. 2.3.5 This report has been produced following Health and Safety Committee
consideration.
3.0 Key Activities and Achievements during 2014/15 3.1 Policies
3.1.1 The Health and Safety Team have reviewed and updated the following policies in consultation with safety representatives:
Health and Safety Policy
Non-Clinical Risk Assessment Policy
Smoke Free Environment Policy
Ligature Risk Reduction Policy
Falls from Height Policy
Safe Marking of Equipment Policy
Display Screen Equipment Policy
Collapsible Rails Policy
Asbestos Management Policy
Control of Contractors Policy
Workplace Assessment of Safety and Health (WASH) Policy
3.2 Training
Health and Safety Training for Managers
3.2.1 A one day bespoke “Health & Safety for Managers” course continues to be provided on a regular basis since it was first introduced as a mandatory training requirement for managers, with the provision of a 3 yearly update. The course is modelled on the ‘IOSH Managing Safely’ course provided by the Institute of Occupational Safety & Health.
3.2.3 Throughout the year, 8 courses were delivered by the Trust Health & Safety
Advisors in locations across both sides of the county. Two courses were cancelled due to insufficient delegates and one was cancelled due to compassionate grounds. All delegates were rebooked onto later courses.
3.2.4 A total of 47 managers and 2 internal staff were trained with positive feedback
being received. The learning outcomes covered the following topics:
Health & Safety Law
Manager Roles & Responsibilities
Health & Safety Regulations
7
The Health & Safety Executive
Risk Assessment Theory
Stress at Work
Incident Reporting Overview
Risk Assessment Practical Session
3.2.5 The course will be reviewed in 2015 to target different management tiers. 3.2.6 Risk Assessment Training 3.2.7 The Ulysses Risk Assessment software training continued to be provided
during 2014. The software session was delivered as a live presentation in order to capture high numbers. Training roadshows were held across a variety of Trust premises capturing as many staff as possible throughout a geographical footing. A total of 75 staff attended the 15 courses that were scheduled (as one-hour duration).
3.2.8 From August 2014, the training was modified to a ‘half-day course’ that
included risk assessment theory, a practical exercise and an introduction to the Ulysses Risk Assessment module. A total of 21 courses were provided on a ratio of 2 per day with 134 delegates attending. Additional bespoke courses were provided locally for:
Estates East
Occupational Health
HMP Prisons
IT West
Westhaven Hospital
Bridport Hospital
PMVA Team 3.2.9 Throughout 2014/15, the total number of staff trained was 209. Courses were
scheduled on a monthly basis with the exception of March/April when Ulysses was off-line for maintenance/improvement. The learning outcomes covered the following topics:
Health & Safety Law/Legislation
Risk Assessments theory - 5 Steps principle to risk assessments
Risk Assessment Theory
Risk Assessment Practical Session
Ulysses Risk Assessment module
3.2.10 Other Health and Safety Training 3.2.11 Refresher training remains incorporated into the Moving and Handling
Mandatory Training Requirements. During 2015/16 it is planned that this will be redeveloped as an e-learning package, with bespoke presentations for clinical and non-clinical staff.
8
3.2.12 Induction training will be moving to a workbook approach completed before employment starts, with a test completed during the induction workshop to confirm learning.
3.2.13 Contractor inductions are being delivered as required 3.2.14 Learning and Development Report on Manual Handling
645 staff received Moving & Handling training during the period of this report.
As the training is repeated on a 3 yearly basis, our current compliance as at as at 30/06/15 (Quarter 1) is illustrated in the table below:
Course Update Target Group Quarter 1 Actual
Moving & Handling – Patient Handlers
3 yearly
All staff who patient handle
82.2%
Moving & Handling - Non Patient/Manual Handlers
3 yearly
All staff who do not patient/ manual handle
91.0%
3.3 Prevention and Management of Violence and Aggression (PMVA)
Training 3.3.1 New starters working in Mental Health Inpatient Service areas are required to
successfully complete the 5-day initial training programme after commencing their employment. Staff are then required to complete a 2-day annual update.
3.3.2 As at the end of March 2015, 96.51% of the target group had completed the
required training within the preceding 12 months. 3.3.3 The Trust retains its rolling monthly target of >95% completion rate for all
mandatory training. Each Locality has trajectory targets for 2015/16 to support the achievement and maintenance of a continued >95% completion rate.
3.4 Security Advisory Group (SAG) 3.4.1 The Trust established a SAG in 2013 which meets bi-monthly. Approved
minutes of the SAG are sent to the Executive Quality and Clinical Risk Group. 3.4.2 Security Advisory Group work has led to a reduction in the number of
incidents of violence and aggression. In 2011 the Trust recorded over 1100 assaults which by 2015 have reduced to 565 (48.6% reduction). This is compared to a national increase over the same period of 18.8%.
Factors leading to this performance have involved:
9
A staff questionnaire relating to violence and aggression;
Identification of key performance indicators;
The effectiveness of the Security Advisory Group and its membership
Improved analysis on incident data
Improved actions on incidents reported
Adjustment of care plans taking account of incidents and review by Security Management Specialist and Clinical staff
Use of posters and leaflets to improve access to support
Additional support to those reporting the highest number of incidents
Training investments and developments
Attention to lone working and development of risk assessment
Review of support to those involved with assault incidents
Prosecutions
Development of Partnership working with the Police.
The Group plan improved lone working device and support arrangements to provide more consistent and effective approach to lone working and mapping of actions taken against overall assault incident data.
4.0 Health and Safety Incident Report 4.1 A quarterly Health and Safety specific incident report is produced, tabled and
discussed at the Health and Safety Committee. This includes data for incidents that directly affect or involve staff, split by Directorate and then Locality Directorates following the implementation of the new structure.
4.2 This forms part of the Trust’s active monitoring of Health and Safety
performance by the Health and Safety Committee. Data contained in the Health and Safety Incident Report includes:
Fire (including actual and false alarm activation)
Control of Substances Hazardous to Health (exposure to hazardous substances)
Manual Handling
Infection Control
Sharps (including needle stick injuries)
Slips, Trips and Falls (non-patient)
Staff Shortages
RIDDORs (See Appendix 3)
5.0 Reporting of Injuries, Diseases and Dangerous Occurrences (RIDDOR) 2013
5.1 Injuries that lead to a member of staff being incapacitated for more than seven
consecutive days as the result of an occupational accident or injury (not counting the day of the accident but including weekends and rest days) has to be made to the HSE within 15 days of the accident.
10
5.2 This report reflects those incidents reported to the HSE in 2014/15 under
RIDDOR as listed in the Directorates below:
Over 7 Day Injuries (20)
Dorset Locality - 3
Bournemouth / Christchurch - 10
Poole / East Dorset - 7
Major Injuries (4)
Dorset Locality - 1
Bournemouth / Christchurch - 1
Poole / East Dorset - 2
Dangerous Occurrence
Dorset Locality (Contractors) - 1 (See Appendix 3)
6.0 Health and Safety Team Site Visits
6.1 Health and Safety site visits were undertaken at a variety of Trust premises
during 2014/15 and advice and guidance provided to managers and staff. The visits fell into 9 main categories:
Mini-WASH (Workplace Assessment of Safety and Health) visits
IQST (Integrated Quality Service Team) visits
Incident investigation visits
Advice visits
Risk assessment assistance visits
Ligature survey visits
Pre-start works visits
Ongoing construction works visits
Space utilisation visits
6.2 The Team also attended various Groups:
Health and Safety Committee
Security Advisory Group
Locality Group Meetings
Infection Prevention and Control Group
Capital Planning / Space Utilisation Group
Medical Devices Group
Transport of Substances Group
Needlesafe Group
Inpatient Safety Group
11
7.0 Prison Healthcare Units
7.1 All of the managers from the 6 prisons have now completed the Risk Assessment Training course and have made some progress in producing risk assessments for their place of work; this work will continue with regular visits from the Health and Safety Team.
7.2 There is regular liaison with the Prison H&S Heads where risk assessments
are discussed and this further evidences that the Trust is working in conjunction with the Prisons to assist them in meeting their specific health and safety requirements.
7.3 A team member attends the Dorset and Devon Operational Group meeting for
the prisons.
7.4 Work is in progress in conjunction with the Trust Security Team to reduce any type of violence and aggression towards Trust staff. This includes verbal as well as physical aggression. The Trust has also worked in collaboration with the Prisons to enhance training on security management related topics such as contraband items, threats and intimidation.
7.5 A review of incidents reported to the prisons against those reported on the Trust’s Ulysses system showed that there was an inconsistent approach to incident reporting. At recent meetings, staff were encouraged to report incidents via the Trust Ulysses computer system. Incidents reported have subsequently risen from approximately 5 each month to 30.
7.6 Each of the prisons’ Healthcare teams hold regular team meetings to which
the Health and Safety Team is invited. The H&S team attends these meetings on a regular basis.
8.0 Ligature Management Plans 8.1 During 2014/15 the Health and Safety Team undertook a review of the
Manchester Management Audit Tool (Manchester Tool) that had been used previously to identify and assess potential ligature anchor points.
8.2 Because of the introduction of iPads to the Team, an “App” based electronic
audit tool was trialled leading to the preparation of a detailed template for ligature surveys and management plans. The new surveys and management plans have been well received by clinicians whose participation has been a key to their success.
8.3 During the period of this report a Trust Ligature Management policy was
written, approved and published. 8.4 All inpatient mental health and dementia wards (with the exception of 2 wards
that are part of the extensive St Ann’s Hospital redevelopment) have been surveyed and ligature anchor points detailed using the electronic tool. These outputs in the form of Ligature Management Plans have been passed to Ward Managers. The Ligature Management Plans will be reviewed on a six monthly
12
basis. The process and outcome has been reviewed to ensure that actions identified are taken on the day. Estates, Ward staff, Health and Safety and Nursing Quality staff have agreed arrangements to work together to conduct the survey along with a plan to share summary of findings with Consultant and ward staff.
8.5 The Health and Safety Team has worked with Estates, Infection Control, Patient Safety and Procurement to reduce the range of fixtures and fittings being procured and installed within clinical areas. This has been done on a case by case basis, but in 2015/16 will start to be formalised into Trustwide guidelines.
8.6 During 2015, Task and Finish Groups have commenced to examine the
incorporation of the Ligature Management Plans into the Trust Risk Management Strategy; and on a parallel stream standard specifications will be drawn up for anti-ligature fixtures, fittings and equipment.
9.0 Workplace Assessment of Safety and Health (WASH) 9.1 A simplified intranet based on-line WASH declaration form was developed by
the Health and Safety Team to assist staff in monitoring their level of health and safety compliance in their workplaces. The declaration is designed to act as a prompt for staff to identify areas of potential weakness that may require addressing.
9.2 All actions and subsequent outcomes for each completed WASH are
addressed and managed locally. Copies of completed declarations are retained on site for 3 years as evidence to support local health and safety arrangements.
9.3 The Health and Safety Team do not actively monitor completed WASH
declarations, but locality and service senior managers are provided with a report of those that have been completed for their own self-monitoring.
9.4 During 2015/16 the on-line WASH declaration form is being developed to re-
align to the recently implemented Locality Directorate structures, as well as incorporating a mandatory ‘reporting’ list to better identify sites and services that require completing as a minimum. This will inform the planned premises audit schedule by highlighting areas of high or higher risk. The output is being redesigned to allow better interrogation and identification of hotspots and areas of non-compliance.
10.0 Fire
10.1 The Trust has a proactive approach to fire prevention which is facilitated by
two Fire Officers who are managed within the Estates Directorate. The figures for fires and false alarms for the Trust are detailed below:
Month Actual Fires False Alarms
April 2014 1 1
May 1 1
13
June 1 4
July 1 0
August 2 3
September 0 6
October 0 1
November 2 3
December 1 6
January 2015 0 2
February 2 6
March 1 4
10.2 Mandatory fire training is delivered by the Learning & Development
Department with Fire Marshal and specialist fire training being delivered by the Trust Fire Officers.
10.3 Extra Fire Marshal training is being delivered predominantly in the west of the
county to address the change in fire evacuation procedures, giving continuity of actions across the Trust.
10.4 The team are working together to review outstanding Fire Risk Assessments and Drill audits across the trust.
10.5 Fire Risk Assessments have been completed for all sleeping risk buildings and the team are working closely with the Estates Department identifying the additional buildings (rented & leased) where the Trust has staff working.
10.6 Fire notices were issued in 2014/15 which have been acted on, the first, a deficiency notice for Alderney Hospital site in March 2014 for parking and access issues – this has now been actioned by the Estates/Capital Department and the notice has now been lifted by the Fire Authority.
10.7 The second was an enforcement noticed for Westminster Hospital in April 2014 for numerous issues within the building, this has been actioned by the Estates/Capital Department and the notice has now been lifted by the fire authority.
10.8 The third was a deficiency notice for St Ann’s Hospital site in July 2015 for numerous issues on the site, many of these issues are being addressed by the Estates Department and site management. We are working closely with the Fire Authority with ongoing progress meetings booked over the next few months. This notice should be lifted by December 2015.
10.9 An extensive programme of fire compartmentation surveys are being carried out across the Trust with appropriate action plans being developed. This work is being organised through Estates Department/Capital Projects Team.
11.0 Health and Safety Work Plan 2015/2016
11.1 The work plan for 2015/16 is being prepared using the NHS Staff Council
document “Workplace health and Safety Standards” to identify gaps in areas managed by the Health and Safety Team. Any specific projects will run

14
alongside “business as usual” items. The Work Plan, when approved by the Health and Safety Committee, will be appended to this report.
11.2 Ligature Management Plan reviews commenced in May 2015 for all inpatient
mental health & dementia units. These will be reviewed at or as close to the 6 monthly point as possible.
11.3 The WASH process will run from the 1st – 30th September 2015, and is under
review with an aim that the outputs will identify gaps in compliance which will feed the 2016/17 work plan.
11.4 Mini WASH visits continue to run throughout the year and will be used to
verify WASH submissions. 11.5 Policy review will continue in line with a plan. 11.6 The work programme reflects the Care Quality Commission (CQC) Key Line
of Enquiry “Are Services Safe?” and the HSE’s key projects around vulnerable staff.
12.0 Occupational Health and Wellbeing Service
12.1 The Occupational Health and Wellbeing Service (OHWS) also sits within the Human Resources Directorate and provides a comprehensive occupational health service across Dorset to the Trust and its employees. The OHWS is led clinically and strategically by an Associate Director for Occupational Health, Safety and Wellbeing. The service operates from two sites, with the main service delivery from premises in Dorchester and a smaller unit at Boscombe supporting service delivery in the Bournemouth area.
12.2 The OHWS provides services commercially across Dorset and its periphery operating in a very competitive environment with other services including national providers. The total income of the occupational health service in 2014/15 was £782,447.
12.3 The OHWS exists to assist the Trust in protecting, promoting and improving the health of its workforce with the aim of contributing to the delivery of the Trust Strategy. The service has an important role to play in the overall delivery of patient care, safety and outcomes. The service contributes to the delivery of HR Strategy 2015-2020 and the strategic goals which are:
Goal 1: To become a recognised employer of choice so that we attract and recruit to meet our workforce needs.
Goal 2: To retain a compassionate, expert workforce that is proud to work at Dorset HealthCare and feels developed and supported to make decisions, innovate and improve the lives of our patients.
15
13.0 Services and Customers
13.1 There are a range of services offered by the OHWS which include, pre-employment/placement health assessments, occupational vaccination programmes, fitness for work assessments and medicals, health surveillance programmes (audiometry, spirometry, skin, hand arm vibration), workplace and ergonomic assessments, incident management, policy and procedure development and training.
13.2 The OHWS main customer is the Trust. In addition, the OHWS provides services to over 150 companies annually across Dorset, with its two main contracts (accounting for approximately 39% and 17.5% of income in 2014/2015 respectively) being held with Dorset Police and Dorset County Hospital. The OHWS also provides services on both a regular and ad hoc basis to a wide range of industries, including aeronautical, engineering, local government, education, manufacturing, transport, and third sector organisations.
13.3 The OHWS provides an annual update to all customers and occupational health costs are reviewed on an annual basis.
13.4 The OHWS work closely with finance and the contracts team to ensure that service charges and tenders are competitive and profitable and support the delivery of occupational health services to the Trust.
14.0 Occupational Health Services Activity
14.1 The main activities and services provided to the Trust are:
Pre-employment health assessments
Occupational immunisations and screening
Flu vaccination programme
Sickness absence management advice
Blood borne virus exposure management
Workplace health advice
Health surveillance
Workplace assessments

16
14.2 A summary of OH activity for the Trust undertaken in 2014/2015 is detailed
below
Occupational Health and Wellbeing Services 1st April 2014 to 31st March 2015
1. Activity
OH Service Item Numbers Undertaken
Assessment and screening of Health at Work Questionnaires
1037
Occupational immunisation and screening appointments
921
Management referral appointments
1666
Staff Flu Vaccinations
1583
Pre-employment health assessments
98
Blood borne virus exposure incident management
62
Health surveillance appointments
3
Workplace assessments
5
Total Undertaken 5375
2. Attendance
Appointment Type Numbers booked
Numbers of DNA
% DNA
Management referral appointments
1798 132 7.3%
Immunisation appointments
1238 317 25.6%
Pre-employment health assessments
98 2 2%
Blood Borne Virus Follow Up appointments
62 39 62%
Health Surveillance appointments
6 3 50%
Workplace Assessments
5 0 0
Total appointments 3249 493 15.1%
3. Revised KPI Performance (October 2014 to March 2015)
OH Standard %
New management referrals offered appointment within 10 working days
42%
Management referral reports issued within 5 working days
75%
Pre-employment health assessment appointment offered within 5 working days
56%
14.3 To assist with addressing the issue of non-attendance for booked
appointments a text message reminder service was introduced in 2014.

17
Where mobile numbers are available an appointment reminder will be sent to the employee’s phone three days prior to attending an appointment. This is assisted in improving attendance rates and reducing wasted clinical time.
14.4 The problem of poor attendance particularly for immunisation appointments
continues to be of concern and the recruitment process has recently been revised to ensure that details of recruiting managers are available to the occupational health service. Line managers have been reminded through HR matters of the requirement to support staff to attend occupation health appointments, particularly immunisation appointments, which are required to ensure that individual members of staff, their colleagues and patients are protected from infectious diseases. Appointment letters and non-attendance letters have also been revised to ensure that staff and line managers are aware of the impact of non-attendance and understand what action needs to be taken to ensure compliance.
14.5 Further developments planned for 2015/2016 to improve attendance and engagement includes:
Pilot of text messaging on the day of the appointment in addition to 3 days in advance
Increased use of telephone consultations for management referral appointments
DNA Survey
Revision of attendance processes
Induction checklist for immunisation status for new starters
Investigating mechanism for reporting non-compliance to localities
15.0 Wellbeing Activity
15.1 The OHWS has a key role to play in promoting the health and wellbeing of
staff. During 2014/2015 a number of activities have been undertaken to contribute to this which are outlined below
15.2 Attendance at NHS employers funded train the trainer programme to develop
and deliver ‘Creating a Mentally Health Workplace’ Training for line managers. Each Trust was offered the opportunity to train one member of staff to deliver this training which was developed in conjunction with Zeal solutions an occupational psychology consultancy. The training will be delivered as part of the leadership prospectus and further discussions will be undertaken with the Associate Director of Learning and Development to discuss the delivery across the organisation.
15.3 Development of a line manager’s toolkit to assist managers in supporting staff
health and wellbeing. The line manager’s toolkit was developed to complement existing HR resources in assisting managers to support staff with health issues and to understand the role of the OHWS in providing advice and support to managers and staff when managing employee ill health and attendance.
18
15.4 The Trust have also signed up to the governments Public Health Responsibility Deal and developed an action plan for the first pledge to improve mental health and wellbeing. Further pledges and action plans will be developed as part of the employee health and wellbeing strategy during 2015/16. This includes:
Achieving Occupational Health Accreditation
Implementing measures to encourage healthier catering/vending
Supporting smoking cessation
Offering increased staff health checks
Greater support of Employee Mental Health and Wellbeing
Supporting Young People in the WorkPlace
Supporting actions to treat people with dignity and respect and actions relating to support for those experiencing domestic violence
These activities will be supported by a part time post holder supporting the Associate Director of Occupational Health and Well Being to make progress on these pledges (which is an appraisal target for 2015/16) and raise the profile on health at work for Dorset HealthCare employees during 2015/16.
The OHWS has also during 2014/2015:
Contributed to the development of guidance for the treatment of staff with mental health problems
Made changes to internal working practices and provided guidance for occupational health clinical staff to improve early access to OH support for employees and managers
Set up a health and wellbeing working group to develop and implement the employee health and wellbeing strategy for the Trust.
Engaged with the Hidden Talents group to consider how the OHWS can support the projects undertaken by the group and improve the recovery experience for staff with lived experience of mental ill health
15.5 The OHWS team have also contributed to a number of working groups during
the financial year including:
Smoking cessation task and finish group
‘Needlesafe’ task and finish group
Prevention and management of dermatitis working group
NICE Assurance Group
PMVA task and finish group
16.0 Occupational Health Work Plan 2015/2016
16.1 There are a number of work priorities for the OHWS in 2015/2016 which
include:
Achieve national accreditation through the SEQOHS programme (Safe, Effective, Quality Occupational Health Services) to support the delivery of an effective occupational health service
19
Implement project to integrate existing IT systems to improve information governance and reduce IT support costs
Introduction of a web based portal to replace paper based OH activities e.g. pre-employment assessments and management referrals which will enhance remote working for OH staff, improve access to the OH service, reduce waiting times and improve OH communications with service users and line managers
Develop and implement an employee health and wellbeing strategy to support the delivery of the HR strategy and to promote, protect and improve staff health and wellbeing
Support the organisation in developing action plans to deliver the workplace pledges within the Public Health Responsibility Deal. See section 15.4
Deliver training for line managers in ‘Creating a Mentally Healthy Workplace’ supported by Learning and Development
Increase uptake of staff flu vaccinations to at least 40% of all frontline healthcare workers
Develop OH support for line mangers to improve staff health and wellbeing and effectively manage health related attendance issues through policy development, training, self-help resources and signposting
These are the key priorities for the OHSW in the next financial year.
17.0 Employee Assistance Programme (EAP) – Care first 17.1 The Trust provides a confidential, impartial advice and support programme for
staff via Care first. The service is available 24 hours a day, 365 days a year and is free to staff and their immediate family. Support includes:
Telephone information and advice on a range of subjects including family and personal issues, financial matters including debt management, workplace and employment issues
Online services, including information, advice and articles for issues occurring in everyday life, e.g. at home, at work and relating to health
Care first Vitality – an interactive health and personal fitness portal
All calls are answered by trained and accredited counsellors. Although the service is provided by the Trust, Care first’s services are completely independent of the Trust and all calls are treated in confidence in accordance with the BACP Ethical Framework. The company also provides a monthly information pack for the Trust to disseminate to staff which provides themed advice and guidance on a range of health and wellbeing issues.
The service is well used by staff. The most recent quarterly activity report showed that usage has been excellent with a total of 152 contacts of which, 13 were to the telephone information specialists’ service, 69 were telephone contact to the 24/7 counselling line and 69 were individual face-to-face counselling sessions. There has also been on on-line contact. There have been 39 new cases/clients presented of which 34 were female and 5 were male.
20
Cares first are also able to provide bespoke support to groups of staff for examples following serious untoward incidents.
The EAP service provision is overseen by an account manager and any issues which arise, which are few, are personally followed up and responded to by the Care first Clinical Director.
18.0 Conclusion
18.1 The content of this report provides an update to the Board of the Trust of the occupational health and health and safety activities undertaken between 1st April 2014 and 31st March 2015 to ensure that the organisation meets legal compliance standards, and ensure that all staff, service users and visitors are and remain safe.
18.2 This report demonstrates that the organisation is working to meet its statutory obligations under the Health and Safety at Work etc. Act 1974, the associated regulations, and the relevant standards outlined by the Care Quality Commission.
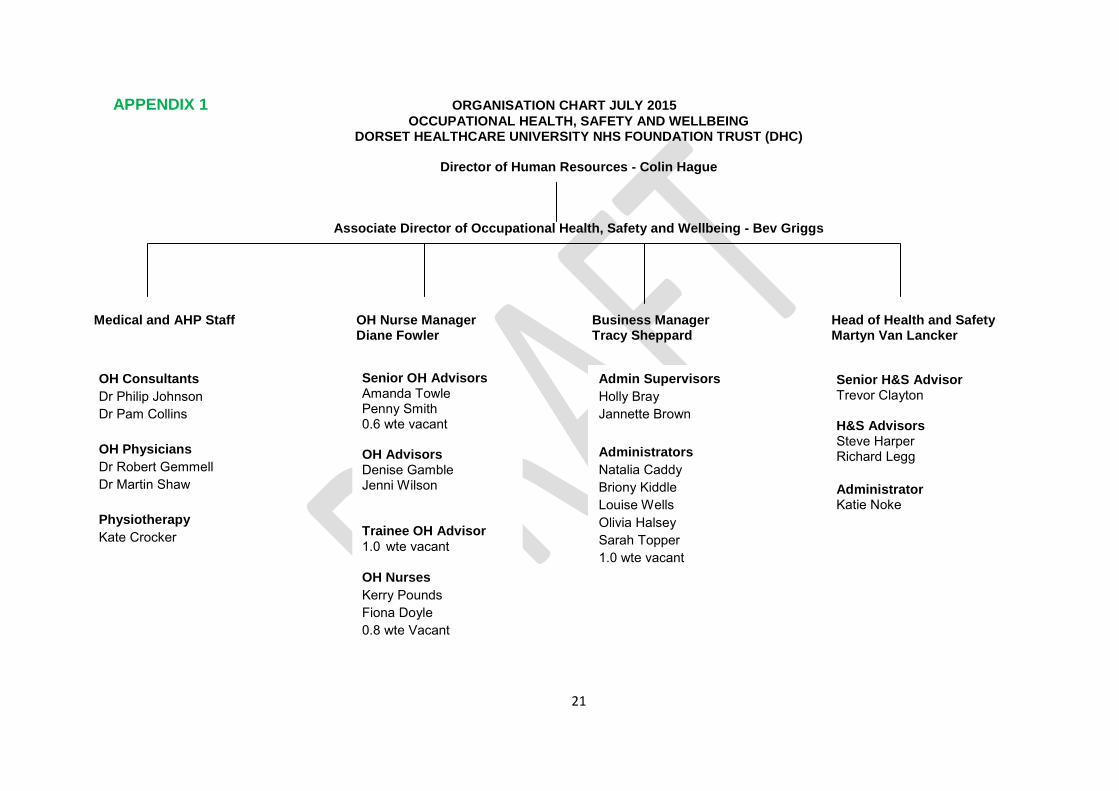
21
APPENDIX 1 ORGANISATION CHART JULY 2015
OCCUPATIONAL HEALTH, SAFETY AND WELLBEING DORSET HEALTHCARE UNIVERSITY NHS FOUNDATION TRUST (DHC)
Director of Human Resources - Colin Hague
Associate Director of Occupational Health, Safety and Wellbeing - Bev Griggs
Medical and AHP Staff OH Nurse Manager Business Manager Head of Health and Safety Diane Fowler Tracy Sheppard Martyn Van Lancker Supervisors
OH Consultants
Dr Philip Johnson
Dr Pam Collins
OH Physicians
Dr Robert Gemmell
Dr Martin Shaw
Physiotherapy
Kate Crocker
Senior OH Advisors Amanda Towle Penny Smith 0.6 wte vacant OH Advisors Denise Gamble Jenni Wilson Trainee OH Advisor
1.0 wte vacant
OH Nurses
Kerry Pounds
Fiona Doyle
0.8 wte Vacant
Admin Supervisors
Holly Bray
Jannette Brown
Administrators
Natalia Caddy
Briony Kiddle
Louise Wells
Olivia Halsey
Sarah Topper
1.0 wte vacant
Senior H&S Advisor Trevor Clayton H&S Advisors Steve Harper Richard Legg
Administrator Katie Noke

22
APPENDIX 2 - DETAILED TREND ANALYSIS FOR 2014/15

23
APPENDIX 3 – RIDDOR DATA
Trust Meeting Calendar 2016
Part 1 Board Meeting 30 September 2015
Author Keith Eales, Trust Secretary
Sponsoring Board Member Ann Abraham, Chair
Purpose of Report To propose the meeting calendar for 2016
The attached schedule sets out meeting dates in 2016 for Board, Council of Governors and Executive groups
Recommendation The Board is asked to agree the dates of Board, Board Committee and Board Workshop dates in 2016.
Engagement and Involvement Board and Committee Chairs
Previous Committee/s Dates
Monitoring and Assurance Summary
This report links to the following Strategic Objective(s)
To provide high quality care; first time, every time; To be a valued partner and expert in partnership
working with Patients, Communities and organisations;
To be a learning organisation, maximising our partnership with Bournemouth University and promoting innovation, research and evidence based practice;
To be a national leader in the delivery of integrated care;
To ensure that all of the Trust’s resources are used in an efficient and sustainable way
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability Information Management &Technology Equality Impact Assessment Freedom of Information
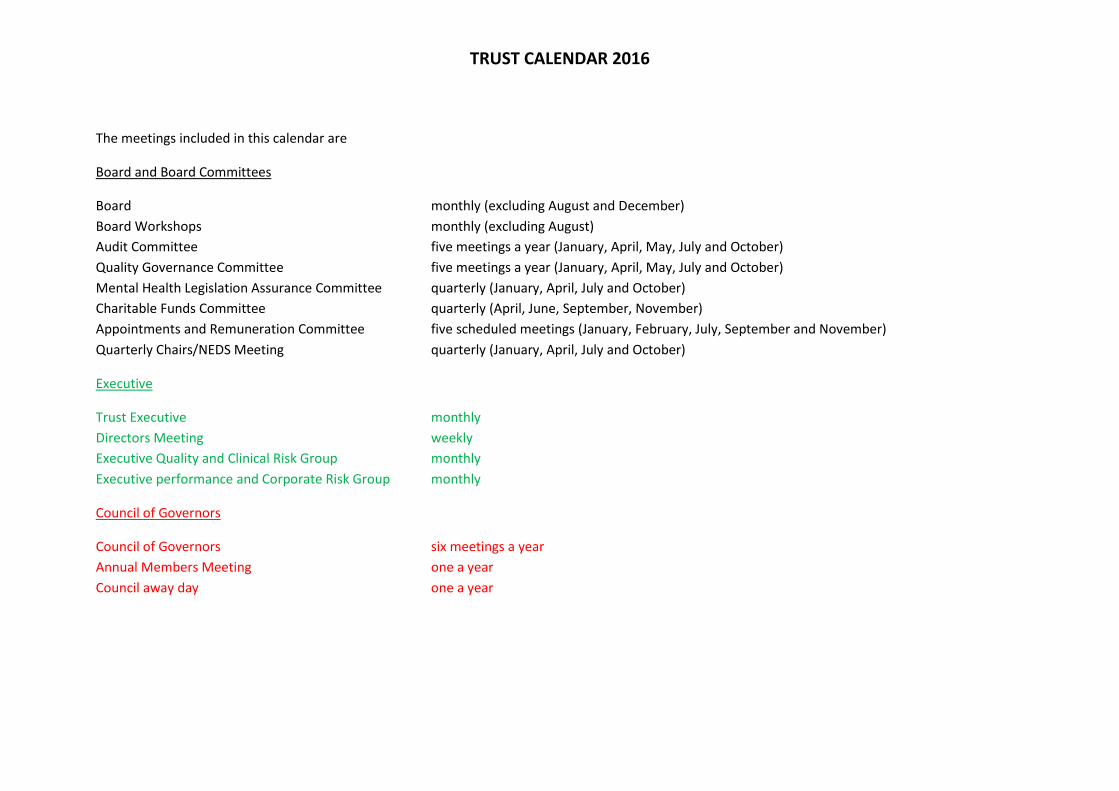
TRUST CALENDAR 2016
The meetings included in this calendar are
Board and Board Committees
Board monthly (excluding August and December)
Board Workshops monthly (excluding August)
Audit Committee five meetings a year (January, April, May, July and October)
Quality Governance Committee five meetings a year (January, April, May, July and October)
Mental Health Legislation Assurance Committee quarterly (January, April, July and October)
Charitable Funds Committee quarterly (April, June, September, November)
Appointments and Remuneration Committee five scheduled meetings (January, February, July, September and November)
Quarterly Chairs/NEDS Meeting quarterly (January, April, July and October)
Executive
Trust Executive monthly
Directors Meeting weekly
Executive Quality and Clinical Risk Group monthly
Executive performance and Corporate Risk Group monthly
Council of Governors
Council of Governors six meetings a year
Annual Members Meeting one a year
Council away day one a year
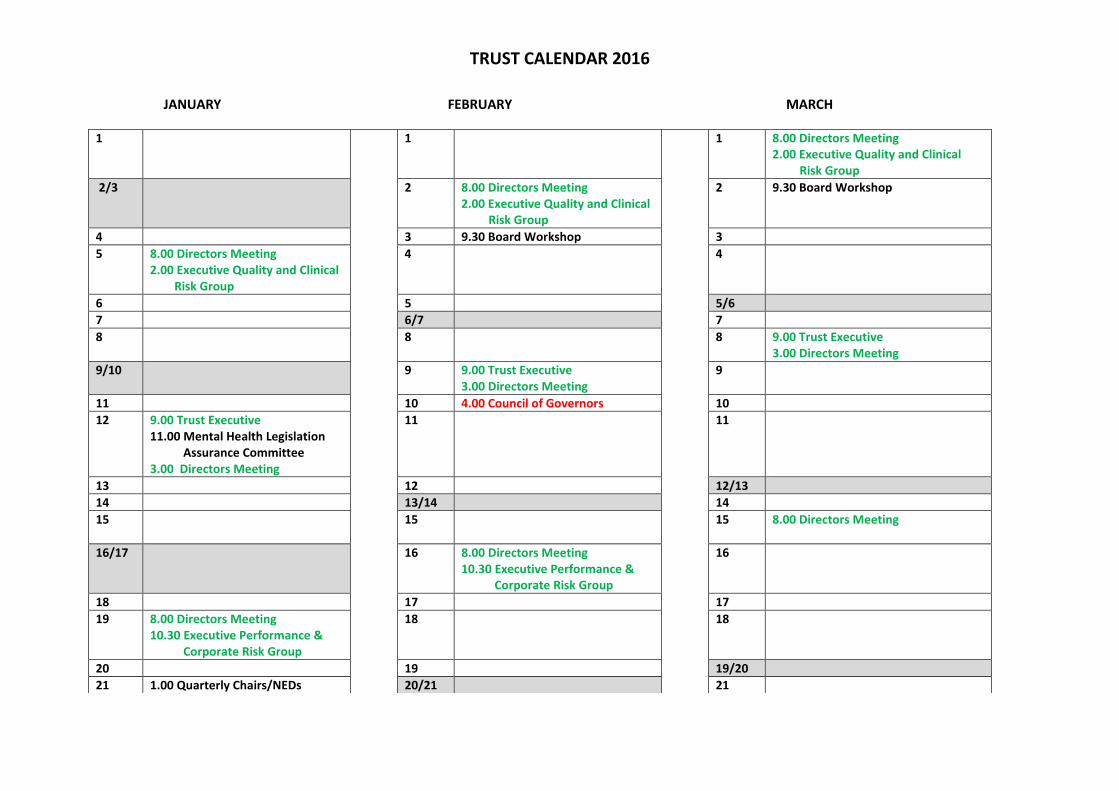
TRUST CALENDAR 2016
JANUARY FEBRUARY MARCH
1 1 1 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
2/3 2 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
2 9.30 Board Workshop
4 3 9.30 Board Workshop 3
5 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
4 4
6 5 5/6
7 6/7 7
8 8 8 9.00 Trust Executive 3.00 Directors Meeting
9/10 9 9.00 Trust Executive 3.00 Directors Meeting
9
11 10 4.00 Council of Governors 10
12 9.00 Trust Executive 11.00 Mental Health Legislation Assurance Committee 3.00 Directors Meeting
11 11
13 12 12/13
14 13/14 14
15 15 15 8.00 Directors Meeting
16/17 16 8.00 Directors Meeting 10.30 Executive Performance & Corporate Risk Group
16
18 17 17
19 8.00 Directors Meeting 10.30 Executive Performance & Corporate Risk Group
18 18
20 19 19/20
21 1.00 Quarterly Chairs/NEDs 20/21 21
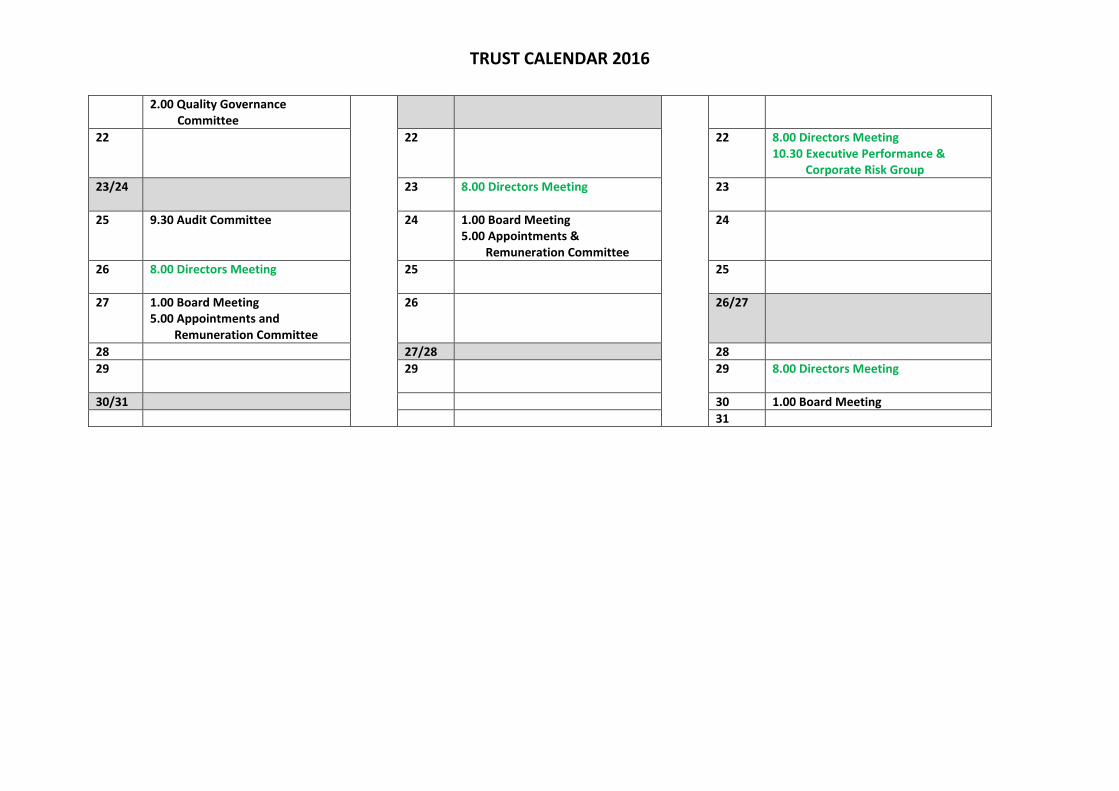
TRUST CALENDAR 2016
2.00 Quality Governance Committee
22 22 22 8.00 Directors Meeting 10.30 Executive Performance & Corporate Risk Group
23/24 23 8.00 Directors Meeting
23
25 9.30 Audit Committee 24 1.00 Board Meeting 5.00 Appointments & Remuneration Committee
24
26 8.00 Directors Meeting
25 25
27 1.00 Board Meeting 5.00 Appointments and Remuneration Committee
26 26/27
28 27/28 28
29 29 29 8.00 Directors Meeting
30/31 30 1.00 Board Meeting
31
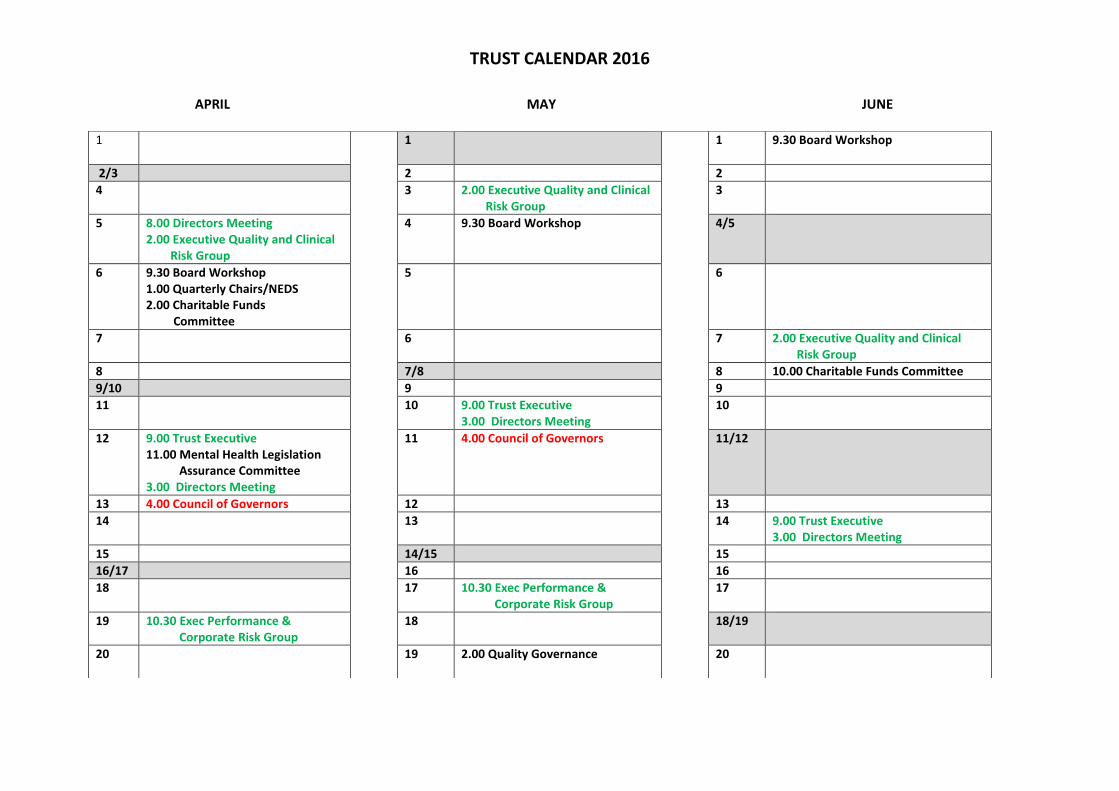
TRUST CALENDAR 2016
APRIL MAY JUNE 1 1 1 9.30 Board Workshop
2/3 2 2
4 3 2.00 Executive Quality and Clinical Risk Group
3
5 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
4 9.30 Board Workshop 4/5
6 9.30 Board Workshop 1.00 Quarterly Chairs/NEDS 2.00 Charitable Funds Committee
5 6
7 6 7 2.00 Executive Quality and Clinical Risk Group
8 7/8 8 10.00 Charitable Funds Committee
9/10 9 9
11 10 9.00 Trust Executive 3.00 Directors Meeting
10
12 9.00 Trust Executive 11.00 Mental Health Legislation Assurance Committee 3.00 Directors Meeting
11 4.00 Council of Governors 11/12
13 4.00 Council of Governors 12 13
14 13 14 9.00 Trust Executive 3.00 Directors Meeting
15 14/15 15
16/17 16 16
18 17 10.30 Exec Performance & Corporate Risk Group
17
19 10.30 Exec Performance & Corporate Risk Group
18 18/19
20 19 2.00 Quality Governance
20

TRUST CALENDAR 2016
21 2.00 Quality Governance Committee
20 21 10.30 Exec Performance & Corporate Risk Group
22 21/22 22
23/24 23 9.30 Audit Committee 23
25 9.30 Audit Committee 24 24
26 25 1.00 Board 25/26
27 1.00 Board 26 27
28 27 28
29 28/29 29 1.00 Board
30 30 30
31 31

TRUST CALENDAR 2016
JULY AUGUST SEPTEMBER
1 1 1
2/3 2 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
2
4 3 3/4
5 2.00 Executive Quality and Clinical Risk Group
4 5
6 9.30 Board Workshop 1.00 Quarterly Chairs/NEDS
5 6 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
7 6/7 7 9.30 Board Workshop 1.00 Charitable Funds Committee
8 8 8
9/10 9 9.00 Trust Executive 3.00 Directors Meeting
9
11 10 10/11
12 9.00 Trust Executive 11.00 Mental Health Legislation Assurance Committee 3.00 Directors Meeting
11 12
13 4.00 Council of Governors 12 13 9.00 Trust Executive 3.00 Directors Meeting
14 13/14 14 4.00 Council of Governors Annual Members Meeting
15 15 15
16/17 16 8.00 Directors Meeting
16
18 17 17/18
19 8.00 Directors Meeting 10.30 Exec Performance & Corporate Risk Group
18 19
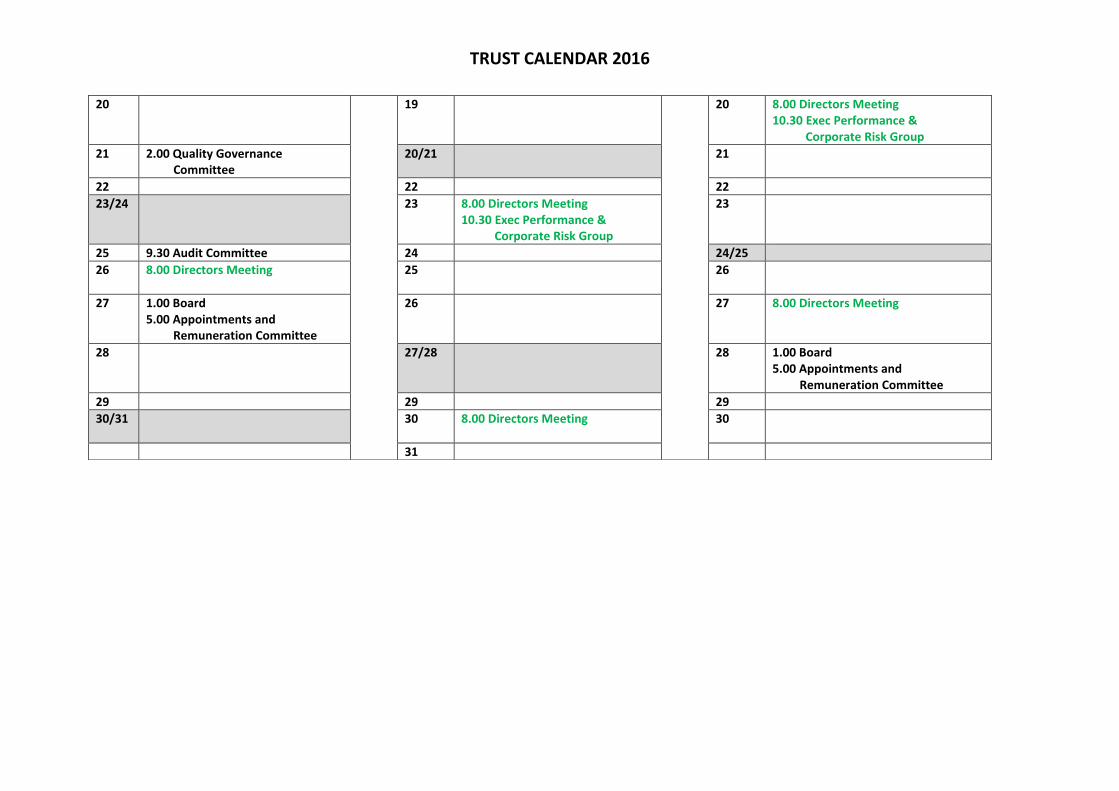
TRUST CALENDAR 2016
20 19 20 8.00 Directors Meeting 10.30 Exec Performance & Corporate Risk Group
21 2.00 Quality Governance Committee
20/21 21
22 22 22
23/24 23 8.00 Directors Meeting 10.30 Exec Performance & Corporate Risk Group
23
25 9.30 Audit Committee 24 24/25
26 8.00 Directors Meeting
25 26
27 1.00 Board 5.00 Appointments and Remuneration Committee
26 27 8.00 Directors Meeting
28 27/28 28 1.00 Board 5.00 Appointments and Remuneration Committee
29 29 29
30/31 30 8.00 Directors Meeting
30
31

TRUST CALENDAR 2016
OCTOBER NOVEMBER DECEMBER
1/2 1 8.00 Directors Meeting
2.00 Executive Quality and Clinical Risk Group
1
3 2 9.30 Board Workshop
2
4 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
3 3/4
5 9.30 Board Workshop 1.00 Quarterly Chairs/NEDS
4 5
6 5/6 6 8.00 Directors Meeting 2.00 Executive Quality and Clinical Risk Group
7 6 7 9.30 Board Workshop 1.00 Charitable Funds Committee
8/9 8 9.00 Trust Executive 3.00 Directors Meeting
8
10 9 9
11 9.00 Trust Executive 11.00 Mental Health Legislation Assurance Committee 3.00 Directors Meeting
10 Council of Governors awayday 10/11
12 11 12
13 12/13 13 9.00 Trust Executive 3.00 Directors Meeting
14 13 14 4.00 Council of Governors
15/16 15 8.00 Directors Meeting
15
17 16 16
18 8.00 Directors Meeting 10.30 Exec Performance &
17 17/18
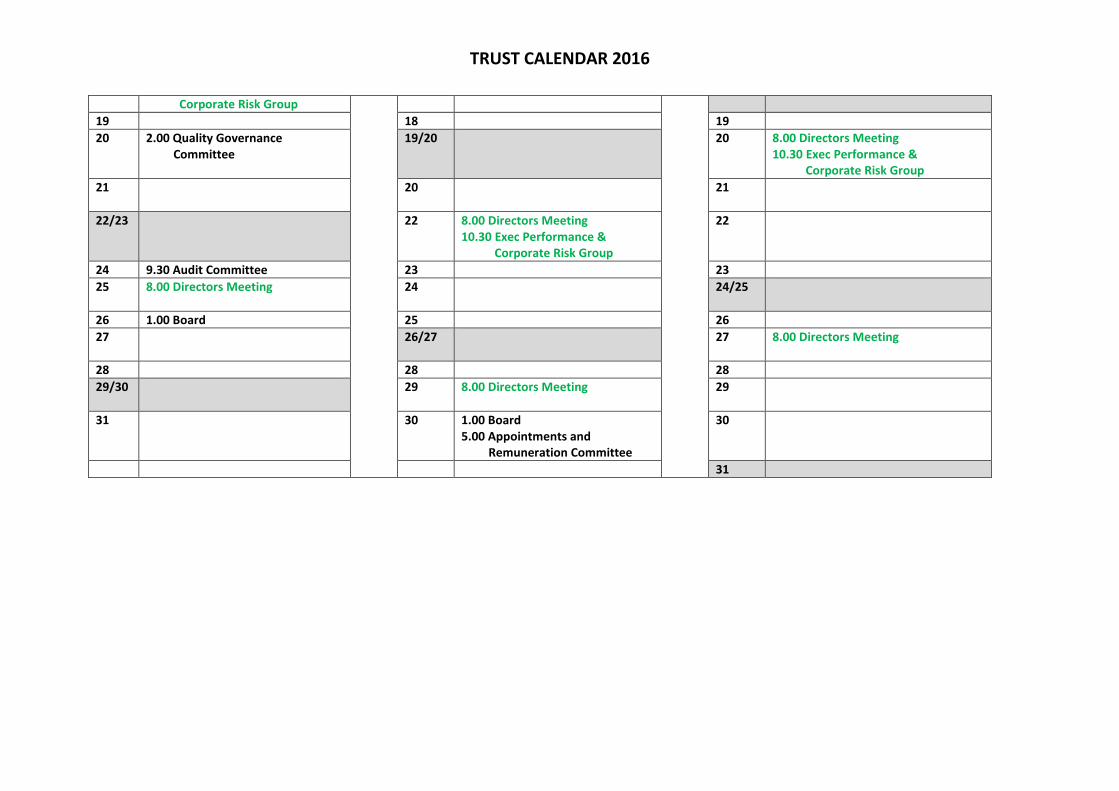
TRUST CALENDAR 2016
Corporate Risk Group
19 18 19
20 2.00 Quality Governance Committee
19/20 20 8.00 Directors Meeting 10.30 Exec Performance & Corporate Risk Group
21 20 21
22/23 22 8.00 Directors Meeting 10.30 Exec Performance & Corporate Risk Group
22
24 9.30 Audit Committee 23 23
25 8.00 Directors Meeting
24 24/25
26 1.00 Board 25 26
27 26/27 27 8.00 Directors Meeting
28 28 28
29/30 29 8.00 Directors Meeting
29
31 30 1.00 Board 5.00 Appointments and Remuneration Committee
30
31

Reappointment of Mental Health Act Panel Members
Part 1 Board Meeting 30 September 2015
Author Gavin Macfarlane
Sponsoring Board Member Sarah Murray, Chair Mental Health Legislation Assurance Committee
Purpose of Report To reappointment Mental Health Act Panel Members
Recommendation The Board is asked to reappoint the Mental Health Act Panel Members set out in this report
Reason for inclusion in Part II Personal information
Engagement and Involvement Those who have been involved are the Mental Health Legislation Manager and the Chair, MHL Assurance Committee both of whom are in agreement with its contents.
Previous Committee/s Dates
Monitoring and Assurance Summary
This report links to the following Strategic Objective(s)
To provide high quality care; first time, every time; To be a valued partner and expert in partnership
working with Patients, Communities and organisations;
To be a learning organisation, maximising our partnership with Bournemouth University and promoting innovation, research and evidence based practice;
To be a national leader in the delivery of integrated care;
To ensure that all of the Trust’s resources are used in an efficient and sustainable way
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability Information Management &Technology Equality Impact Assessment Freedom of Information

2
RE-APPOINTMENT OF APPOINTED MENTAL HEALTH ACT PANEL MEMBERS
1 Background
1.1 The reappointment of Appointed Mental Health Act Panel Members is subject to Board approval, following a satisfactory appraisal by the Chair of the Mental Health Legislation Assurance Committee.
1.2 A number of members are subject to reappointment over the next two months. The appraisal process for to support their reappointment is currently underway.
2 Appointment Process
2.1 On 16 July 2015 the appraisal of the following took place
Mrs Jacqueline Swift
Mr Nick Plumbridge On 24 August 2015 the appraisal of the following took place
Mr Peter Viney
Mr Richard Peacocke
Based on the outcome of the appraisals, the Board is recommended to reappoint all as Mental Health Act Panel Members for a period of two years subject to continuing satisfactory appraisals by the Chair of the Mental Health Legislation Assurance Committee.
3 Recommended 3.1 The Board is recommended to reappoint the following as Appointed Mental Health
Act Panel Members for a period of two years subject to continuing satisfactory appraisals by the Chair of the Mental Health Legislation Assurance Committee
Mrs Jacqueline Swift
Mr Nick Plumbridge
Mr Peter Viney
Mr Richard Peacock
Gavin Macfarlane Mental Health Services, Mental Health Legislation Manager, 7th September 2015

Board Annual Cycle of Business
Part 1 Board Meeting 30 September 2015
Author Keith Eales, Trust Secretary
Sponsoring Board Member Ann Abraham, Chair
Purpose of Report To set out the updated annual cycle of business for the Board.
The cycle of business has been updated to reflect the fact that the Board will not be meeting in December 2015.
Recommendation The Board is asked to agree the updated annual cycle of business
Engagement and Involvement Directors
Previous Committee/s Dates
Monitoring and Assurance Summary
This report links to the following Strategic Objective(s)
To provide high quality care; first time, every time; To be a valued partner and expert in partnership
working with Patients, Communities and organisations;
To be a learning organisation, maximising our partnership with Bournemouth University and promoting innovation, research and evidence based practice;
To be a national leader in the delivery of integrated care;
To ensure that all of the Trust’s resources are used in an efficient and sustainable way
I confirm that I have considered each of the implications of this report, on each of the matters below, as indicated:
Yes
Any action required?
Yes Detail in report
No
All three Domains of Quality
Board Assurance Framework
Risk Register
Legal / Regulatory
People / Staff
Financial / Value for Money / Sustainability Information Management &Technology Equality Impact Assessment Freedom of Information

Board Annual Cycle of Business
Board Meetings
Standard Items
Patient Story
Minutes of the previous Part 1 Board Meeting
Chair’s Report
Chief Executive’s Report
Approved minutes from Board Committees
Integrated Corporate Dashboard
Monthly Finance Report
Monthly update on People Management
October November Dec-no Board meeting
January February March April May June July
Monitor Q2 submission
Infection Prevention six monthly report
Monitor Q3 submission
Safe Staffing six monthly Report
Performance Management Framework
Monitor Q4 submission
Annual Account and Accounts/ Quality Report
Annual SUI Report
Quarter 1 return to Monitor
Quarterly BAF review
Well Led Review Action Plan
Strategic Plan 2016
Annual Plan 2016/17 – Contract agreements
Annual Plan 2016/17 - draft financial plan
Board Register of Interests
ISA 260 Annual Report on Reducing Restrictive Interventions
Annual Complaints report 2014/15
Review of progress against Corporate Objectives
CQC Report and Action Plan
Operating Framework Planning Assumptions for Annual Plan
CQC Action Plan
Proposed Quality Priorities for 16/17
Dorset Care Record Business Case
Monitor self-certification statements
Annual Safeguarding Report 2014/15
Annual patient Experience Report 2014/15

Well Led Review report
St Ann’s Full Business Care
Quarterly review of BAF
Well Led Review Action Plan
Going Concern Report
Annual Infection Prevention & Control Report 2014/15
Board Assurance Framework
Progress Report on Savile actions
Forston Clinic Full Business Case
CQC Action Plan
Approval of corporate objectives
CQC Action Plan
Organisational Development Progress Report
Equality and Diversity Annual Report
Major capital investment strategy
Budget 2016/17
Organisational Development Progress Report
Estates strategy
Organisational Development Progress Report
Locality estate plans
Shelley Road/ Kings Park Hosp
St Ann’s Business Case
: Part 2: Part 2: Part 2: Part 2: Part 2: Part 2: Part 2: Part 2: Part 2:
Quarterly Whistleblowing report
Cost improvement plan 2016/17
Draft financial plan/budget 2016/17
Draft financial plan/budget 2016/17
Quarterly Whistle blowing report
Quarterly Whistleblowing report

Board Workshop Programme
Oct Nov Dec Jan Feb March Apr May June
CQC inspection and external Governance Review reflections
Equality & Diversity
Local strategic and financial context
Output from contract negotiations
Draft budget/ draft CIP/ Director budget reviews
Discussion with Dame Gill Morgan
Budgets 2016/17/ CIP 2016/17/draft narrative annual plan
A second Board workshop will be held in December 2015, in place of the scheduled Board meeting, to discuss
How can we use the Trustwide remuneration strategy and overall pay structure as an integral component of achieving and delivering the Trust
strategy
The draft estates strategy and associated estates issues (which will be submitted to the January 2016 Board meeting for approval





























