Embed Size (px)
Citation preview

1244 ARTHRITIS & RHEUMATISM Vol. 39, No. 7, July 1996, pp 1244-1245 0 1996, American College of Rheurnatology
RADIOLOGIC VIGNETTE
DORSAL DEFECT OF THE PATELLA: AN UNCOMMON CAUSE OF KNEE PAIN
JAVIER NARVdLEZ, JOSE A. N A R V h Z , M. TERESA CLAVAGUERA, MABEL GIL, A. S b C H E Z - M h Q U E Z , and J. M. NOLLA-SOLE
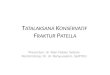
A B Figure 1. A, Axial radiograph of the right knee, showing an osteolytic lesion in the lateral aspect of the patella (arrows). B, Axla1 T2-weighted magnetic resonance image, showing the same lesion (white arrows). Note the normal thickness of the articular cartilage (black arrows).
Clinical history
The patient was a 24-year-old woman with a 1-year history of chronic, intermittent pain in the right
knee that was exacerbated during exercise. She denied any history of knee swelling, locking, or giving way. Results of her physical examination were within normal limits.
Javier Narviez, MD, M. Teresa Clavaguera. MD, J. M. Nolla-Sole, MD: Hospital Principes de Espana, Barcelona, Spain; Jose A. Narvhez, MD. Mabel Gil. MD, A. Sanchez-Marquez, MD: Hospital Duran i Reynals, Ciudad Sanitaria y Universitaria de Bellvitge, Hospitalet de Llobregat, Barcelona, Spain.
Address reprint requests to Francisco Javier Narvaez, MD, Department of Rheurnatology, Hospital Principes de Espaiia, Ciudad Sanitaria y Universitaria de Bellvitge, C/Feka Llarga s/n, 08907 Hospitalet de Llobregat, Barcelona, Spain.
Submitted for publication October 6, 1995; accepted in re- vised form February 14, 1996. .
Radiologic findings
Radiographs revealed a round, well-circumscribed lytic lesion in the superolateral aspect of the right patella (Figure 1A). Magnetic resonance imaging (MRI) showed a bony defect in this location, with lack of continuity of the subchondral bone and intact overlying articular cartilage (Figure 1B).

RADIOLOGIC VIGNETTE 1245
Diagnosis: Dorsal defect of the patella
Discussion
Dorsal defect of the patella (DDP) is a rare benign lesion which appears radiographically as a char- acteristic, well-circumscribed, radiolucent lesion that is usually located in the superolateral angle of the patella, although rarely, it may tend toward a more central location. Its prevalence ranges from 0.3% to 1% (1,2). This condition is most common in adolescents, and the average age at onset of DDP is in the second decade of life (2,3). Both sexes tend to be equally affected, al- though some authors have reported a predominance of either males or females (1,4). It occurs bilaterally in up to one-third of affected individuals (1). In more than half of the cases, DDP is discovered as an asymptomatic incidental radiographic finding (1,3); however, occasion- ally, it may be symptomatic, causing chronic, intermit- tent knee pain in the absence of other demonstrable abnormalities (2,3,5).
Some of the symptomatic patients may also have chondromalacia patellae as a complicating factor (2,5,6). For this reason, it has been hypothesized that DDP is symptomatic only when the articular cartilage overlying the defect is injured. However, in more than half of the symptomatic cases in which the overlying cartilage was assessed either by surgery or arthrography, there was no disruption of the overlying articular surface (3,7). In the case presented here, MRI clearly demonstrated the integrity of the articular cartilage over the lesion.
The natural history of DDP usually tends toward spontaneous, slow healing, resulting in an irregular sclerotic zone in the patella (2,8). Some lesions heal completely in months or years, while others may persist late into adult life (1).
On plain radiographs, the defect appears as a round lytic lesion with a peripheral sclerotic margin, generally located in the superolateral angle, abutting the articular cartilage (1,2,4). MRI is an excellent method for assessing the defect and the articular cartilage (5,8). In cases with inconclusive plain radiographs, it may be very useful for confirming the diagnosis and for exclud- ing another coexisting disorder the symptoms of which may be mistakenly attributed to an asymptomatic DDP (8). 99"'Tc-methylenediphosphonate scintigraphy find- ings may be normal or may show increased uptake (9). The radiologic differential diagnosis of DDP includes osteochondritis dissecans, Brodie's abscess, and bone tumors (chondroblastoma, giant cell tumor, and osteoid osteoma).
The etiology of DDP has yet to be clearly defined. Numerous hypotheses have been developed to explain this disorder. The most acceptable hypothesis suggests that it is a developmental alteration of the epiphysis, with delayed or failed ossification (1,2,4). This is sup- ported by the relatively high rate of bilateral occurrence, and the association in some cases with contralateral bi- or multipartite patella. It has been also hypothesized that chronic trauma and poor blood supply to the superolateral portion of the patella may be the cause of the defect (2). Finally, some authors consider DDP a fibrous cortical defect or nonossifying fibroma of the patella (3). The histologic findings, in the sporadic cases biopsied, were nonspecific, showing fibrous connective tissue and necrotic bone without evidence of an inflam- matory reaction (2,6,8).
The treatment in symptomatic patients with DDP is conservative, including reduction of physical activity and use of analgesics or nonsteroidal antiinflammatory drugs (3). As noted above, the lesion is usually self- limited and heals spontaneously. Surgical treatment is rarely indicated, except when the radiologic findings are not conclusive, and it is necessary to confirm the sus- pected diagnosis. In these cases, curettage of the lesion by arthroscopy has resulted in relief of symptoms (2,5,6).
In summary, DDP is an innocuous entity that, occasionally, may be symptomatic. Early recognition of this condition will help to prevent unnecessary invasive diagnostic and therapeutic interventions.
1.
2.
3.
4.
5.
6.
7.
8.
9.
REFERENCES
Johnson JF, Brogdon BG: Dorsal defect of the patella: incidence and distribution. AJR Am J Roentgenol 139:339-340, 1982 Van Holsbeeck M, Vandamme B, Marchal G, Martens M, Victor J, Baert AL: Dorsal defect of the patella: concept of its origin and relationship with bipartite and multipartite patella. Skeletal Radiol 16:304-311, 1987 Safran MR, McDonough P, Seeger L, Gold R, Oppenheim WL: Dorsal defect of the patella. .I Pediatr Orthop 14:603-607, 1994 Goergen TG, Resnick D, Greenway G, Saltzstein SL: Dorsal defect of the patella: a characteristic radiographic lesion. Radiology 130:333-336, 1979 Monu JUV, De Smet AA: Case report 789. Skeletal Radiol 22528-531, 1993 Sueyoshi Y. Shimozaki E, Matsumoto T, Tomita K: Two cases of dorsal defect of the patella with arthroscopically visible cartilage surface perforations. Arthroscopy 9:164-169, 1993 Haswell DM, Berne AS, Graham CB: The dorsal defect of the patella. Pediatr Radiol 4:238-242, 1976 Ho VB, Kransdorf MJ, Jelinek JS, Kim CK: Dorsal defect of the patella. J Cornput Assist Tomogr 15:474-476, 1991 Gamble JG: Symptomatic dorsal defect of the patella in a runner. Am J Sports Med 14:474-476, 1986






![D V High [Dorsal] Low [Dorsal] No Dorsal Graded Dorsal Concentration Created by Mother Hierarchy of Gene Action in D/V Patterning Mesoderm Genes Neuroectoderm](https://img.pdfslide.us/doc/110x75/56649d3f5503460f94a18b80/d-v-high-dorsal-low-dorsal-no-dorsal-graded-dorsal-concentration-created.jpg)