Embed Size (px)
Citation preview
Dopo i grandi trial sui NAO: studi post-marketing,registri e dati dal
mondo reale
Dr. Claudio FrescoResponsabile Scientifico Dipartimento Scienze
Cardiopolmonari, AOUDPresidente Eletto, ATBV
www.atbv.com
• Relatore a congressi sponsorizzati da Boehringer Ingelheim, Bayer, Pfizer, BMS, Daiichi Sankyo
• Responsabile Scientifico del sito www.pantareionline.it, supportato da un grant incondizionato di Boehringer Ingelheim
Disclosures
www.atbv.com
I trials ci sono stati presentati bene??
www.atbv.com
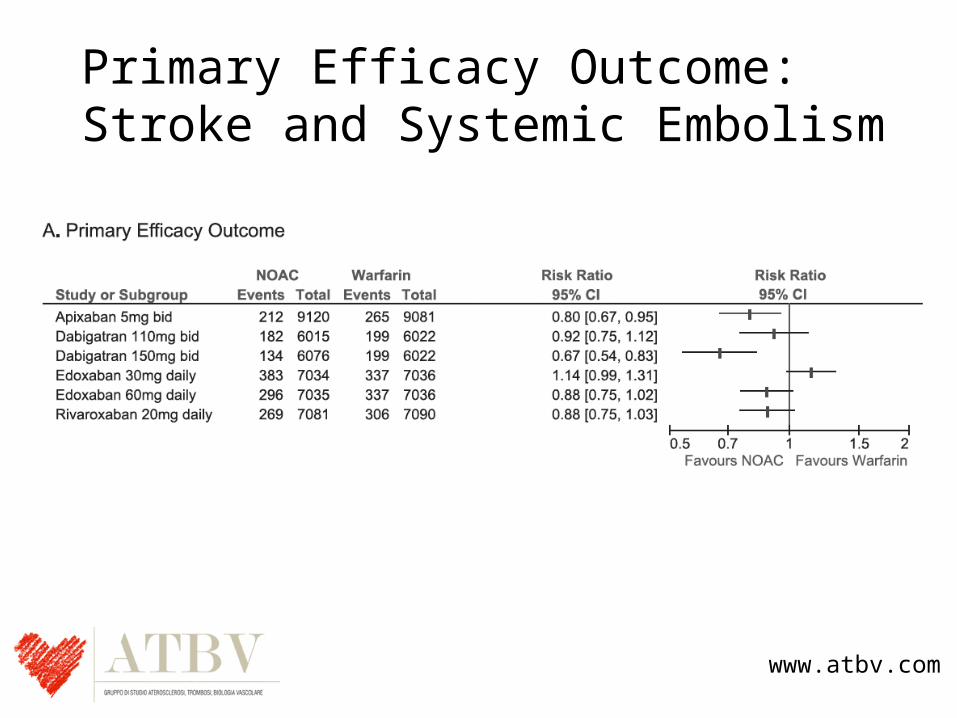
Primary Efficacy Outcome:Stroke and Systemic Embolism
www.atbv.com
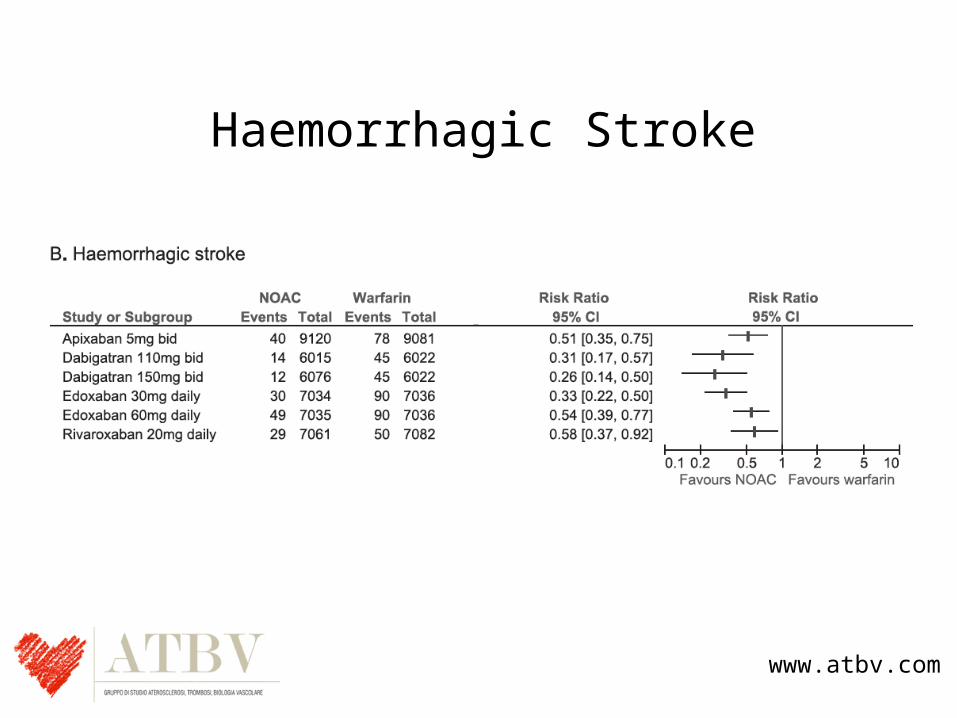
Haemorrhagic Stroke
www.atbv.com
Dove sta il problema?
www.atbv.com
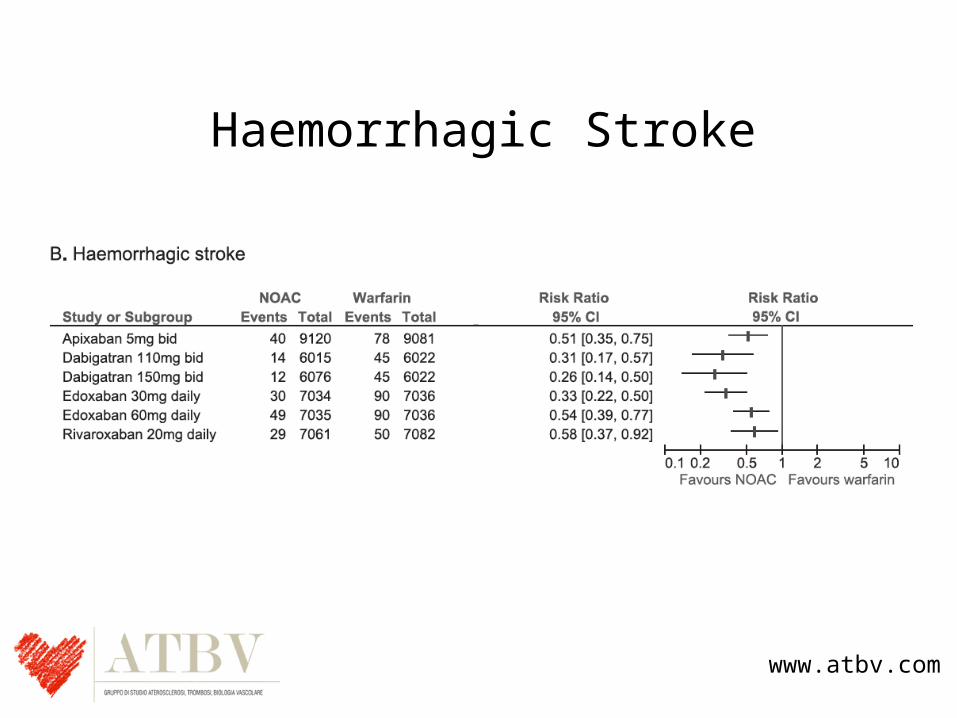
Haemorrhagic Stroke
www.atbv.com
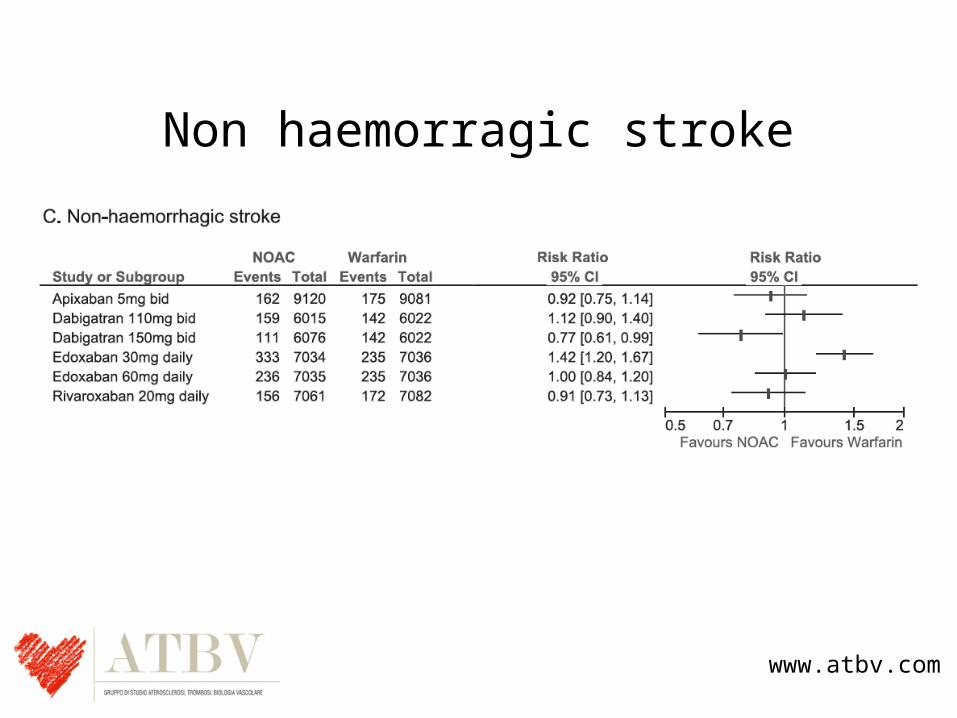
Non haemorragic stroke
www.atbv.com
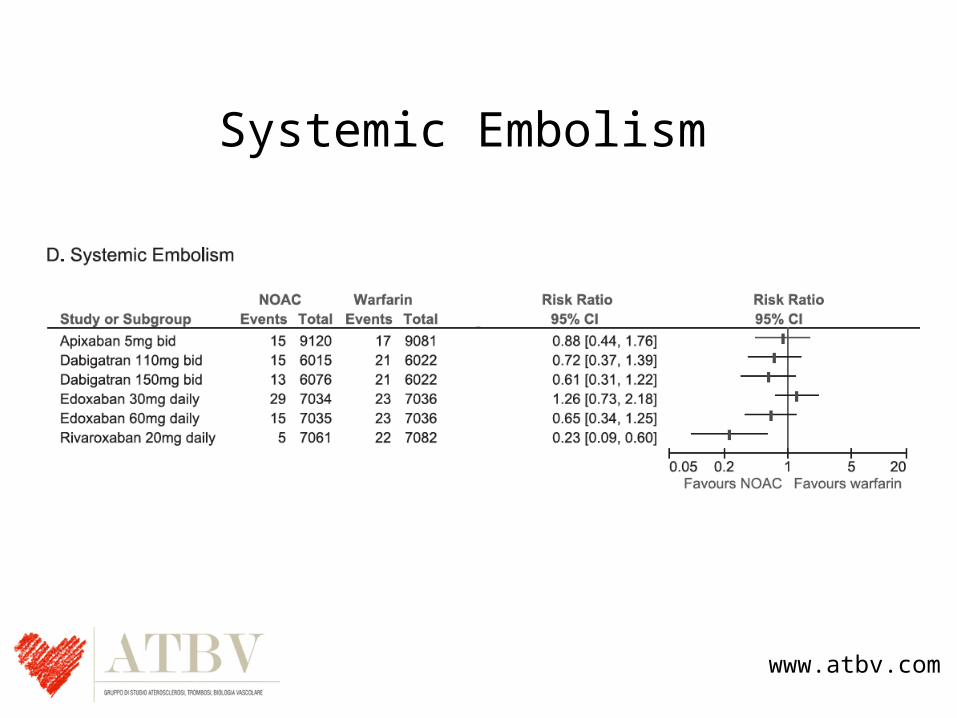
Systemic Embolism
www.atbv.com
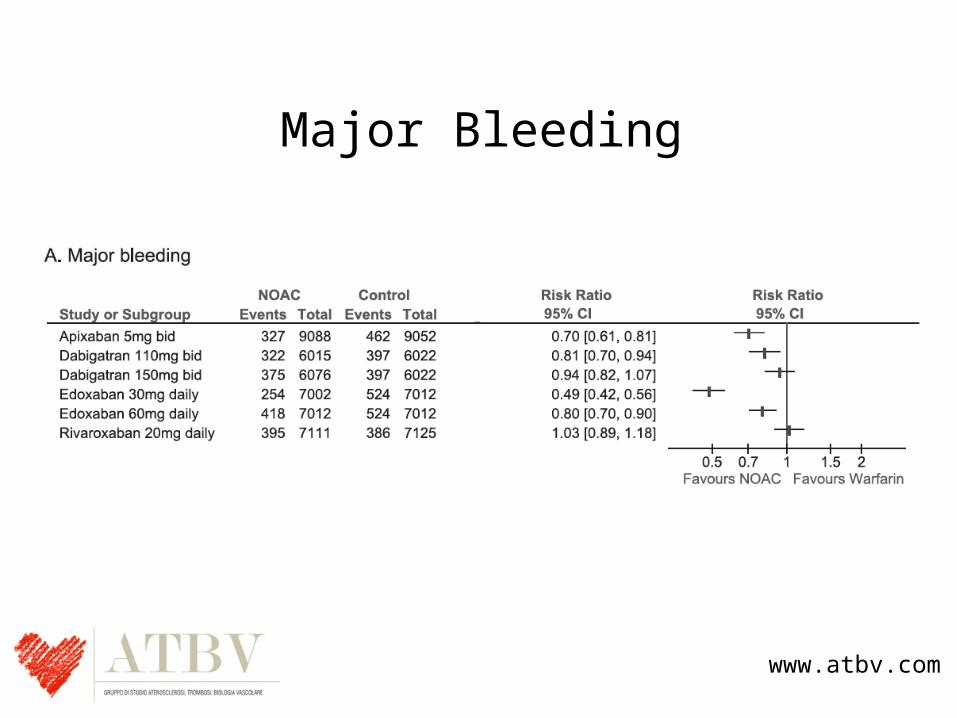
Major Bleeding
www.atbv.com
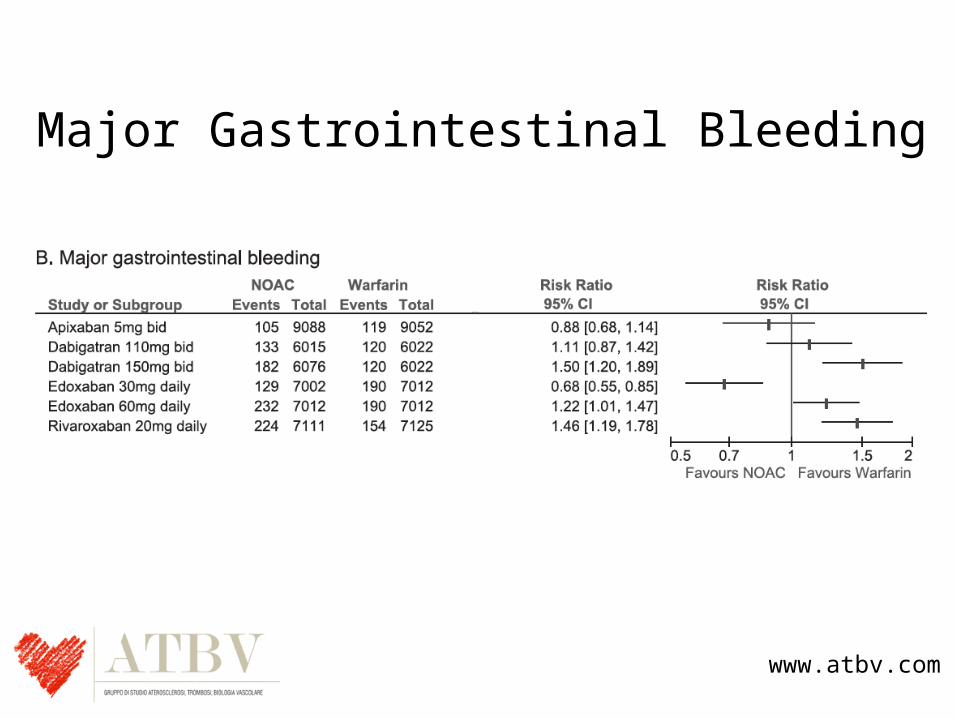
Major Gastrointestinal Bleeding
www.atbv.com
Concludendo1. Dabigratran 150 mg bid is more effective in preventing SSE than W
without significantly increasing MB.2. Dabigatran 110 mg bid is non-inferior to warfarin for the prevention
of SSE and causes less MB.3. Rivaroxaban is non-inferior to W for the prevention of SSE without
significantly increasing MB.4. Apixaban is superior to W in preventing SSE, reducing bleeding and
mortality.5. Edoxaban 60 mg is non-inferior to W for the prevention of SSE,
reduces the risk of MB and CV death.6. Edoxaban 30 mg is non-inferior to W for the prevention of SSE,
reduces the risk of MB and CV death.
www.atbv.com
I pazienti dei trials sono gli stessi che vediamo ogni giorno?
www.atbv.com
Lee S et al. BMJ Open 2012;
www.atbv.com
• The source population for this research, that is, the General Practice Research Database (GPRD) is the largest primary care database in the world.
• 83.898 patients included in the analysis
www.atbv.com

Drug Eligible ChadsVasc
Eligible CHADS
Dabigatran 68% 74%
Apixaban 65% 72%
Rivaroxaban 51% 56%
www.atbv.com
www.atbv.com
Thromb Haemost 2012; 107: 584–589
*Gli effetti attesi
www.atbv.com
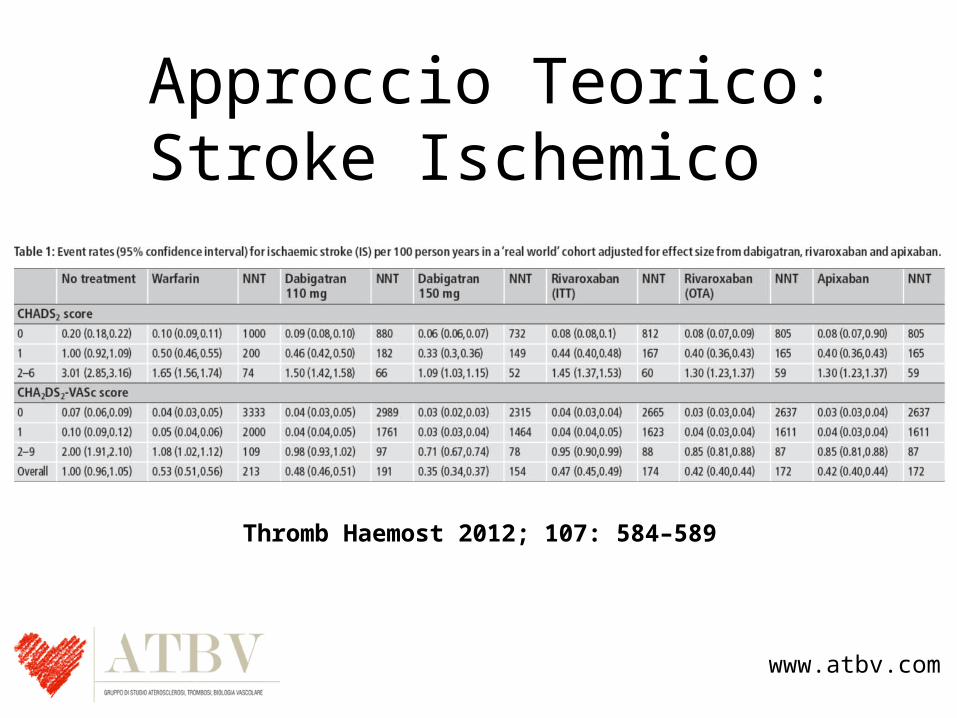
Approccio Teorico:Stroke Ischemico
Thromb Haemost 2012; 107: 584–589
www.atbv.com
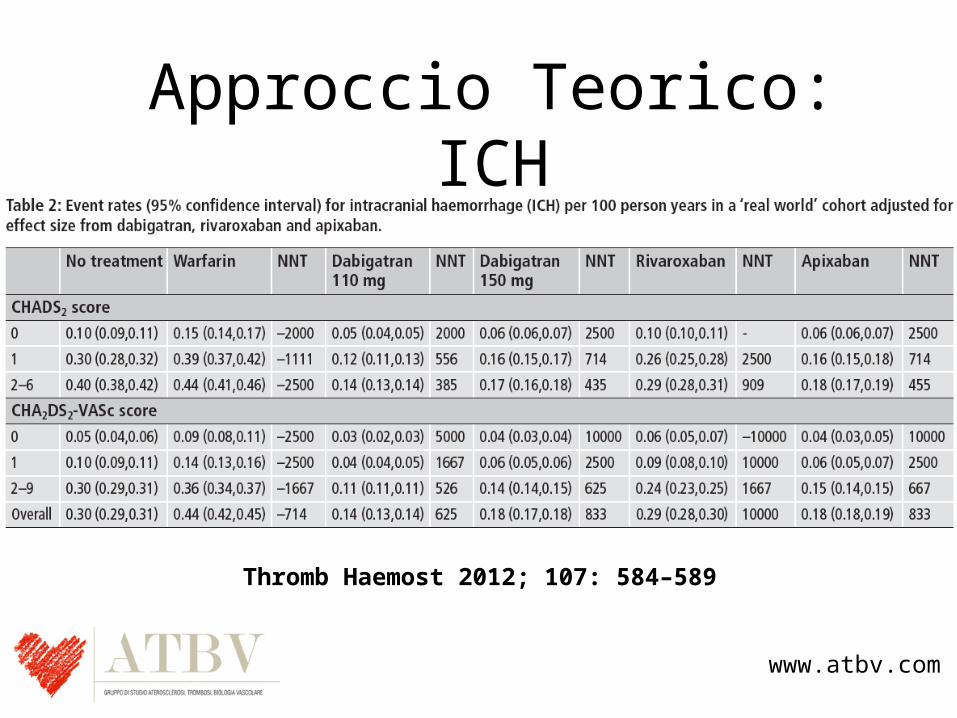
Approccio Teorico:ICH
Thromb Haemost 2012; 107: 584–589
www.atbv.com
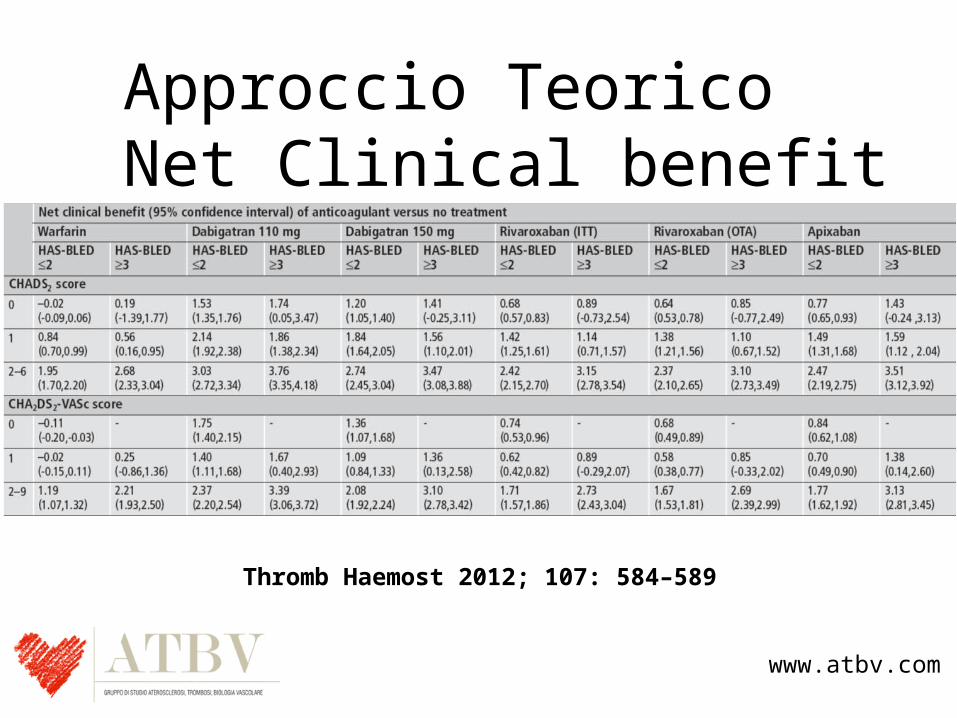
Approccio TeoricoNet Clinical benefit
Thromb Haemost 2012; 107: 584–589
Il Mondo Reale…
DABIGATRAN
www.atbv.com
In the USA, the licensed doses for Pradaxa® are: Pradaxa® 150 mg BID and Pradaxa® 75 mg BID for the prevention of stroke and systemic embolism in adult patients with nonvalvular AF. Pradaxa® 110 mg BID is indicated for certain patients in Europe, and was shown to be as effective as warfarin in preventing stroke or systemic embolism.
1. Available at www.fda.gov/Drugs/DrugSafety/ucm396470.htm; accessed September 2014; 2. Villines TC et al. AHA 2014; 3. Seeger JD et al. AHA 2014; 4. Larsen TB et al. Am J Med 2014;127:650–6.e5; 5. Larsen TB et al. Am J Med 2014;127:329–36.e4
Real-world evidence from >200 000 patients is largely consistent with the results from RE-LY®
Positive safety and efficacy profile of dabigatran vs warfarin confirmed in:
FDA study of >134 000 US Medicare patients1
>25 000 pts from US Department of Defense database2
>38 000 pts from two large US health insurance databases3
>20 000 pts from independent Danish observational studies4,5
22
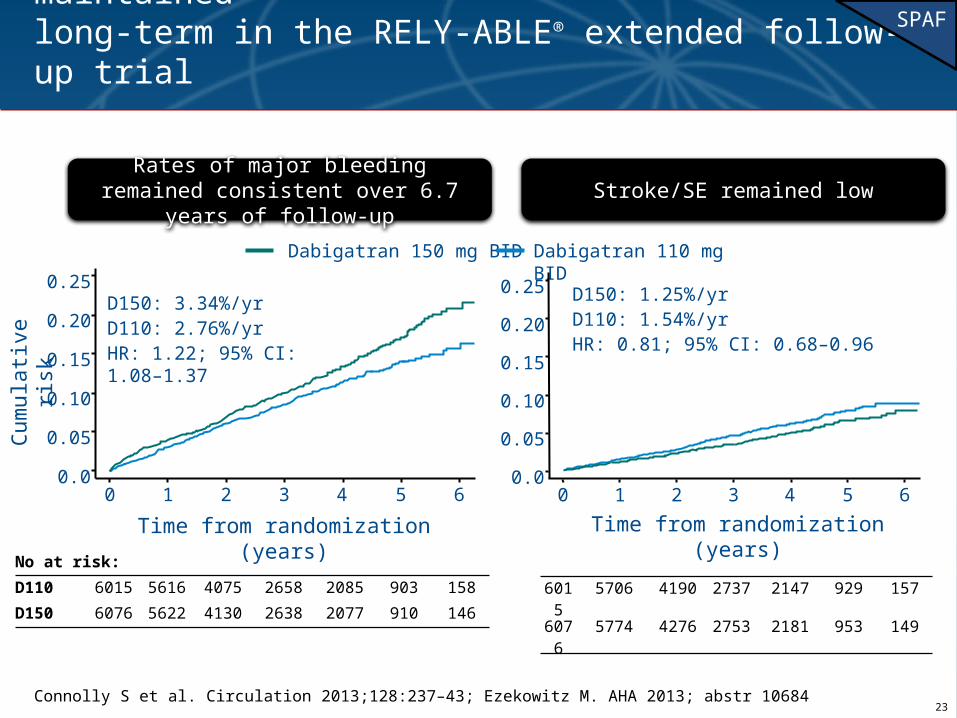
Connolly S et al. Circulation 2013;128:237–43; Ezekowitz M. AHA 2013; abstr 10684
Safety and efficacy of dabigatran are maintained long-term in the RELY-ABLE® extended follow-up trial
No at risk:
D110 6015 5616 4075 2658 2085 903 158
D150 6076 5622 4130 2638 2077 910 146
Dabigatran 150 mg BID
0.25
0.20
0.15
0.05
0.10
0.00 1 2 3 4 5 6
Time from randomization (years)
Dabigatran 110 mg BID
D150: 3.34%/yrD110: 2.76%/yrHR: 1.22; 95% CI: 1.08–1.37
Cum
ulat
ive
risk
0.25
0.20
0.15
0.05
0.10
0.00 1 2 3 4 5 6
Time from randomization (years)
D150: 1.25%/yrD110: 1.54%/yrHR: 0.81; 95% CI: 0.68–0.96
6015
5706 4190 2737 2147 929 157
6076
5774 4276 2753 2181 953 149
Rates of major bleeding remained consistent over 6.7 years of follow-up
Stroke/SE remained low
SPAF
23
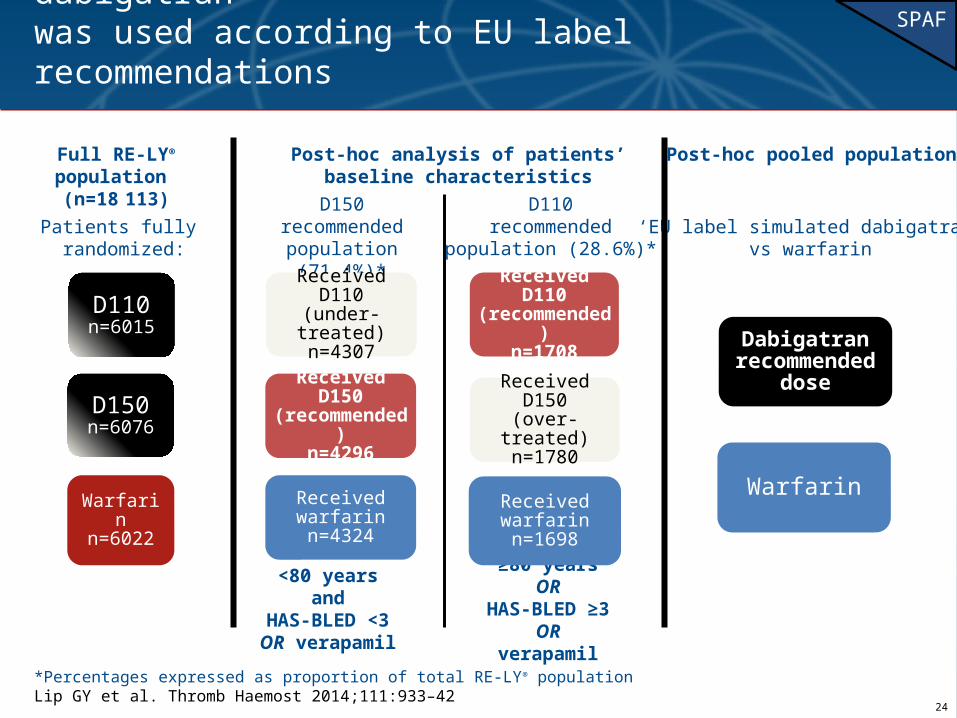
Received D150(over-treated)
n=1780
Received D110(recommended)
n=1708
*Percentages expressed as proportion of total RE-LY® population Lip GY et al. Thromb Haemost 2014;111:933–42
‘EU label’ analysis assessed outcomes when dabigatran was used according to EU label recommendations
Patients fully randomized:
D150recommended
population (71.4%)*
D110recommended
population (28.6%)*‘EU label simulated dabigatran’
vs warfarin
D110n=6015
D150n=6076
Warfarinn=6022
Received D110(under-treated)
n=4307
Received D150(recommended)
n=4296
Received warfarinn=4324
Dabigatranrecommended
dose
Warfarin
≥80 years ORHAS-BLED ≥3OR verapamil
<80 years andHAS-BLED <3OR verapamil
Received warfarinn=1698
SPAF
Full RE-LY® population (n=18 113)
Post-hoc pooled populationPost-hoc analysis of patients’ baseline characteristics
24
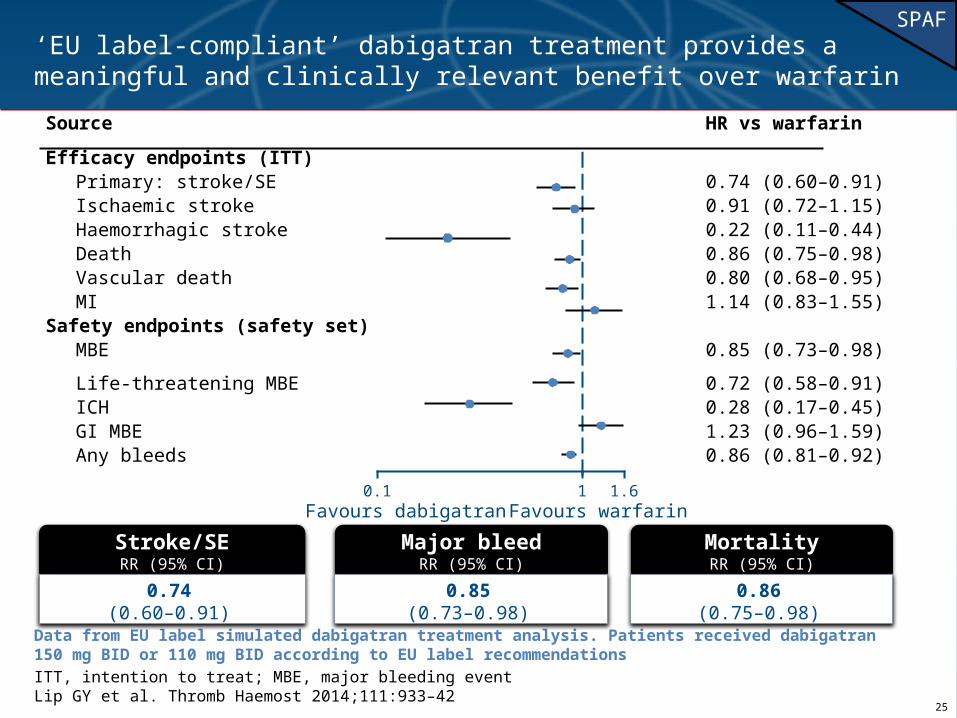
Data from EU label simulated dabigatran treatment analysis. Patients received dabigatran 150 mg BID or 110 mg BID according to EU label recommendations
ITT, intention to treat; MBE, major bleeding eventLip GY et al. Thromb Haemost 2014;111:933–42
‘EU label-compliant’ dabigatran treatment provides a meaningful and clinically relevant benefit over warfarin
Source HR vs warfarin
Efficacy endpoints (ITT)
Primary: stroke/SE 0.74 (0.60–0.91)
Ischaemic stroke 0.91 (0.72–1.15)
Haemorrhagic stroke 0.22 (0.11–0.44)
Death 0.86 (0.75–0.98)
Vascular death 0.80 (0.68–0.95)
MI 1.14 (0.83–1.55)
Safety endpoints (safety set)
MBE 0.85 (0.73–0.98)
Life-threatening MBE 0.72 (0.58–0.91)
ICH 0.28 (0.17–0.45)
GI MBE 1.23 (0.96–1.59)
Any bleeds 0.86 (0.81–0.92)Favours dabigatran Favours warfarin
0.1 1.61
Stroke/SERR (95% CI)
0.74(0.60–0.91)
Major bleedRR (95% CI)
0.85(0.73–0.98)
MortalityRR (95% CI)
0.86(0.75–0.98)
SPAF
25
In the USA, the licensed doses for Pradaxa® are: Pradaxa® 150 mg BID and Pradaxa® 75 mg BID for the prevention of stroke and systemic embolism in adult patients with nonvalvular AF
Graham DJ et al. Circulation 2015;131:157-64
Independent FDA study of Medicare patients analysed outcomes in >134
000 new users of dabigatran or warfarin
• >134 000 new users (OAC treatment-naïve) of dabigatran or warfarin
• All recently diagnosed with AF• All aged ≥65 years• 37 500 person-years of follow-up• Adjustments were made for
confounding variables
• Observational cohort study • US Medicare database• Comparison of ischaemic stroke,
ICH, major GI bleeding, acute MI, and mortality rates using insurance-claim and administrative data
2010 2011 2012
Study period
26
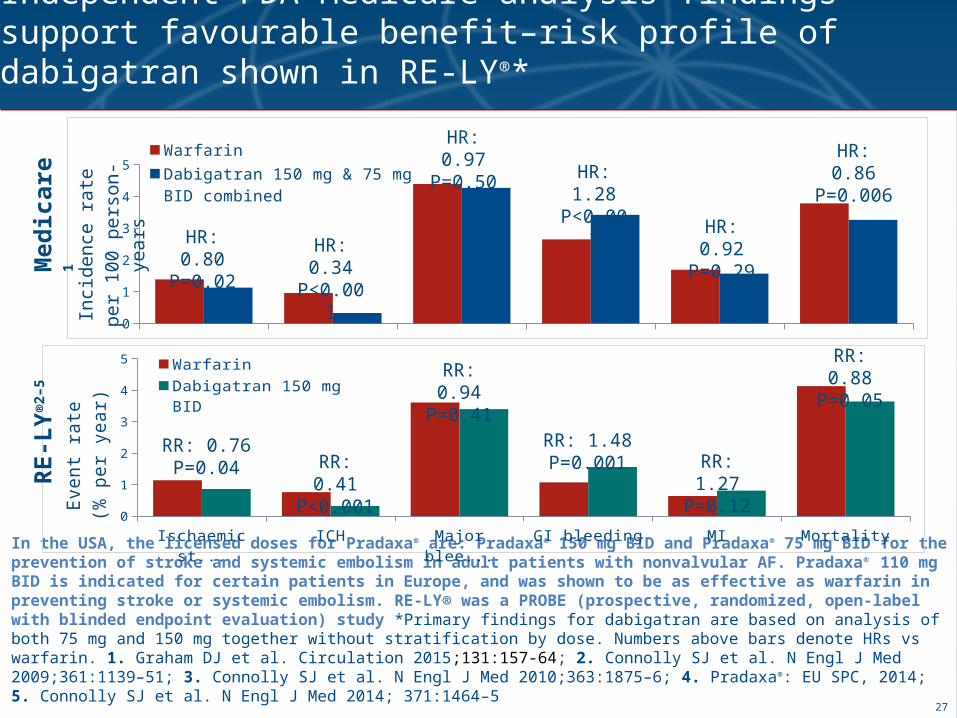
In the USA, the licensed doses for Pradaxa® are: Pradaxa® 150 mg BID and Pradaxa® 75 mg BID for the prevention of stroke and systemic embolism in adult patients with nonvalvular AF. Pradaxa® 110 mg BID is indicated for certain patients in Europe, and was shown to be as effective as warfarin in preventing stroke or systemic embolism. RE-LY® was a PROBE (prospective, randomized, open-label with blinded endpoint evaluation) study *Primary findings for dabigatran are based on analysis of both 75 mg and 150 mg together without stratification by dose. Numbers above bars denote HRs vs warfarin. 1. Graham DJ et al. Circulation 2015;131:157-64; 2. Connolly SJ et al. N Engl J Med 2009;361:1139–51; 3. Connolly SJ et al. N Engl J Med 2010;363:1875–6; 4. Pradaxa®: EU SPC, 2014; 5. Connolly SJ et al. N Engl J Med 2014; 371:1464–5
Independent FDA Medicare analysis findings support favourable benefit–risk profile of dabigatran shown in RE-LY®*
0
1
2
3
4
5Warfarin
Dabigatran 150 mg & 75 mg BID combined
Inci
de
nce
ra
te p
er
10
0 p
ers
on
-ye
ars
HR: 0.86P=0.006HR: 1.28
P<0.001
HR: 0.80P=0.02
HR: 0.92P=0.29HR: 0.34
P<0.001
HR: 0.97P=0.50
Med
icar
e1
Ischaemic stroke
ICH Major bleeding GI bleeding MI Mortality0
1
2
3
4
5Warfarin
Dabigatran 150 mg BID
Eve
nt r
ate
(% p
er
yea
r)
RR: 0.88P=0.05
RR: 1.48P=0.001 RR: 1.27
P=0.12
RR: 0.76P=0.04 RR: 0.41
P<0.001
RR: 0.94P=0.41
RE
-LY
®2–
5
27
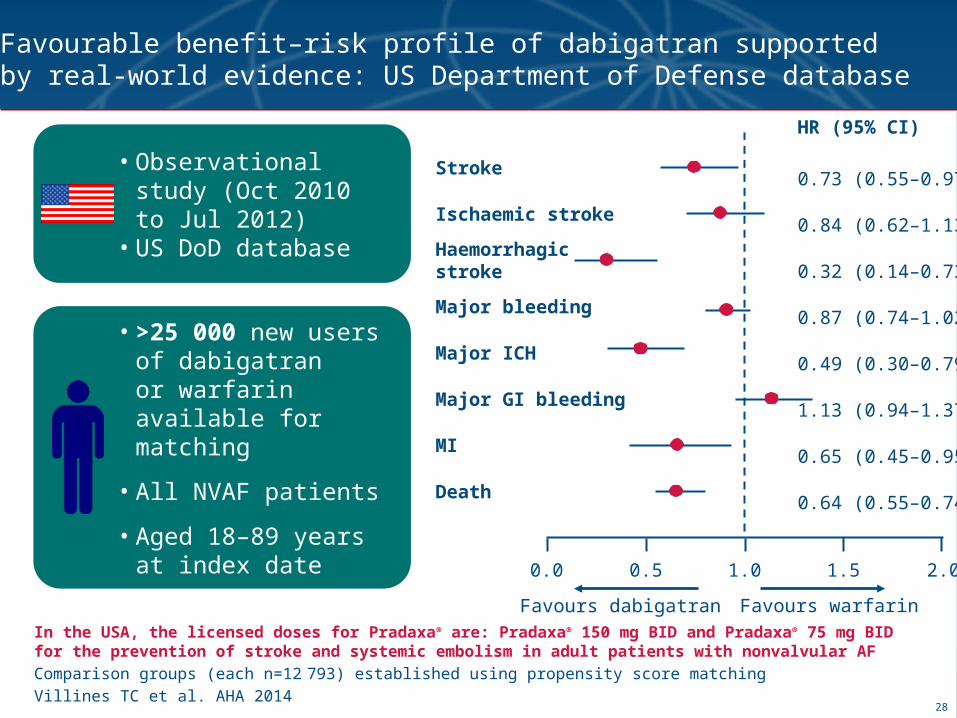
In the USA, the licensed doses for Pradaxa® are: Pradaxa® 150 mg BID and Pradaxa® 75 mg BID for the prevention of stroke and systemic embolism in adult patients with nonvalvular AF
Comparison groups (each n=12 793) established using propensity score matching
Villines TC et al. AHA 2014
Favourable benefit–risk profile of dabigatran supported by real-world evidence: US Department of Defense database
• >25 000 new users of dabigatran or warfarin available for matching
• All NVAF patients
• Aged 18–89 years at index date
• Observational study (Oct 2010 to Jul 2012)
• US DoD database
0.5 1.0 1.50.0 2.0
Stroke
Ischaemic stroke
Haemorrhagicstroke
Major ICH
MI
Major bleeding
Major GI bleeding
Death
0.73 (0.55–0.97)
0.84 (0.62–1.13)
0.32 (0.14–0.73)
0.49 (0.30–0.79)
0.65 (0.45–0.95)
0.87 (0.74–1.02)
1.13 (0.94–1.37)
0.64 (0.55–0.74)
HR (95% CI)
Favours dabigatran Favours warfarin
28
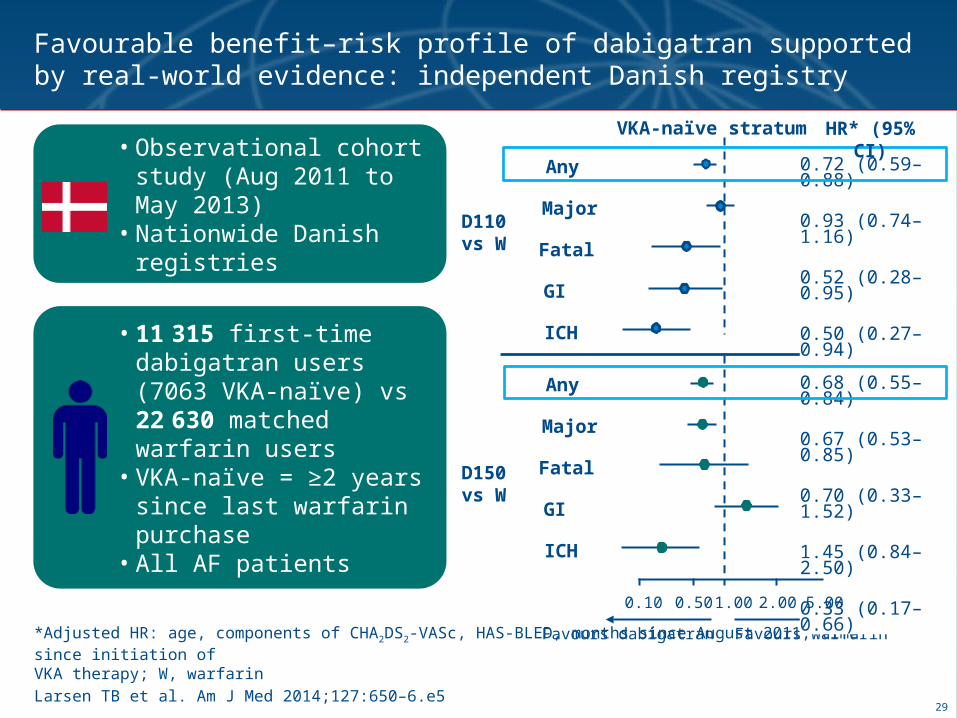
*Adjusted HR: age, components of CHA2DS2-VASc, HAS-BLED, months since August 2011, time since initiation of VKA therapy; W, warfarin
Larsen TB et al. Am J Med 2014;127:650–6.e5
Favourable benefit–risk profile of dabigatran supported by real-world evidence: independent Danish registry
• 11 315 first-time dabigatran users (7063 VKA-naïve) vs 22 630 matched warfarin users
• VKA-naïve = ≥2 years since last warfarin purchase
• All AF patients
• Observational cohort study (Aug 2011 to May 2013)
• Nationwide Danish registries
VKA-naïve stratum
D110vs W
D150vs W
0.72 (0.59–0.88)
0.93 (0.74–1.16)
0.52 (0.28–0.95)
0.50 (0.27–0.94)
0.30 (0.17–0.54)
Favours dabigatran Favours warfarin
0.68 (0.55–0.84)
0.67 (0.53–0.85)
0.70 (0.33–1.52)
1.45 (0.84–2.50)
0.33 (0.17–0.66)
Any
Major
Fatal
GI
ICH
Any
Major
Fatal
GI
ICH
0.10 0.50 1.00 2.00 5.00
HR* (95% CI)
29
Il Mondo Reale…
RIVAROXABAN
www.atbv.com
Il Mondo Reale…RIVAROXABAN
www.atbv.com
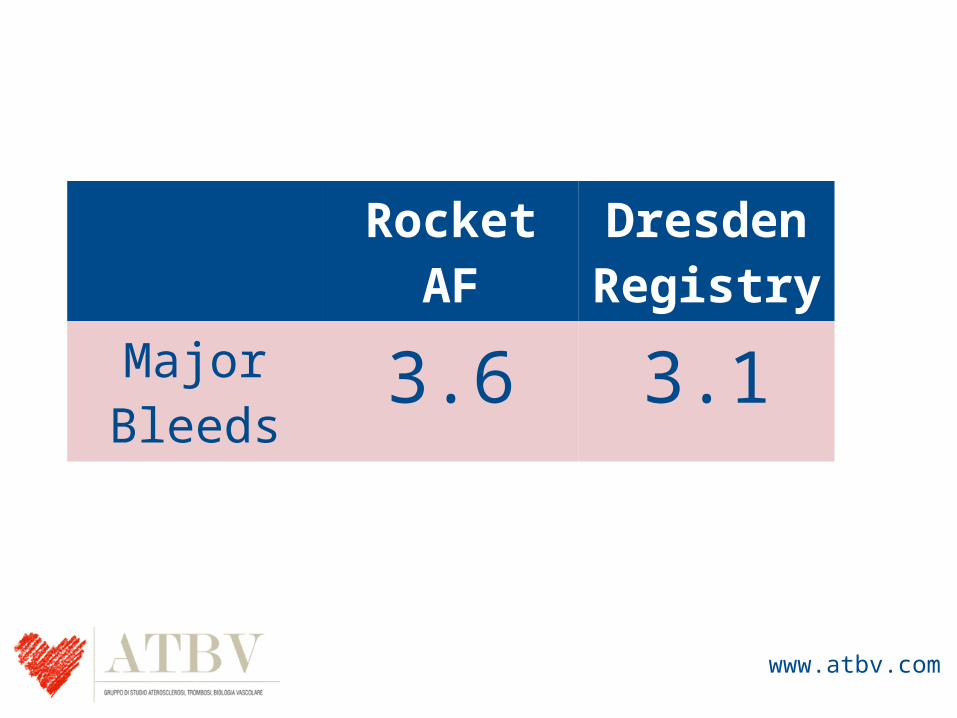
Rocket AF Dresden Registry
Major Bleeds
3.6 3.1
www.atbv.com
www.atbv.com
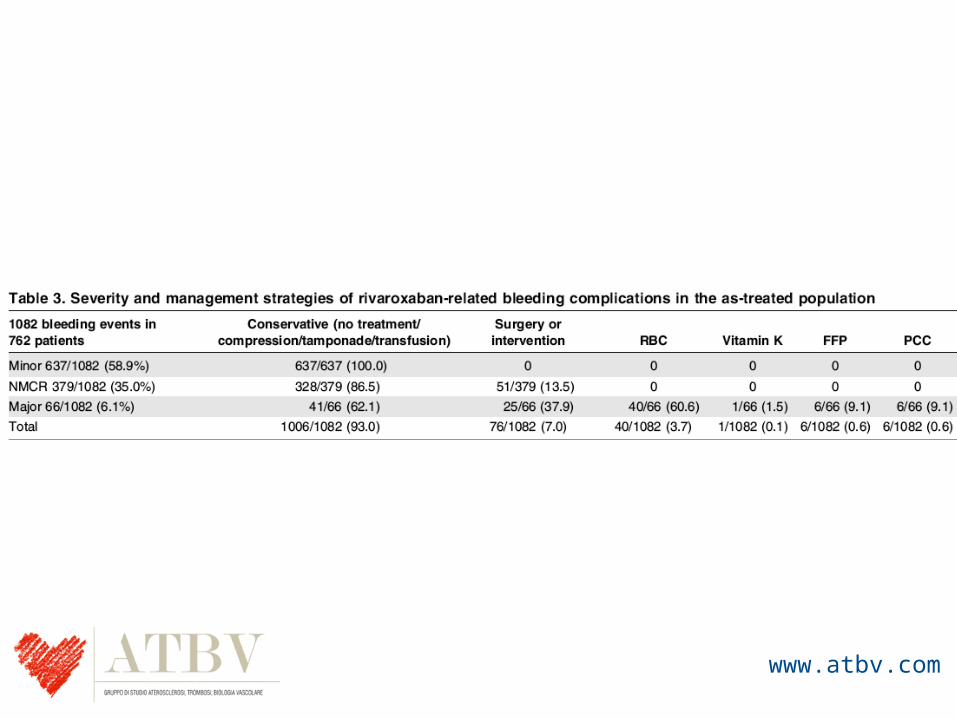
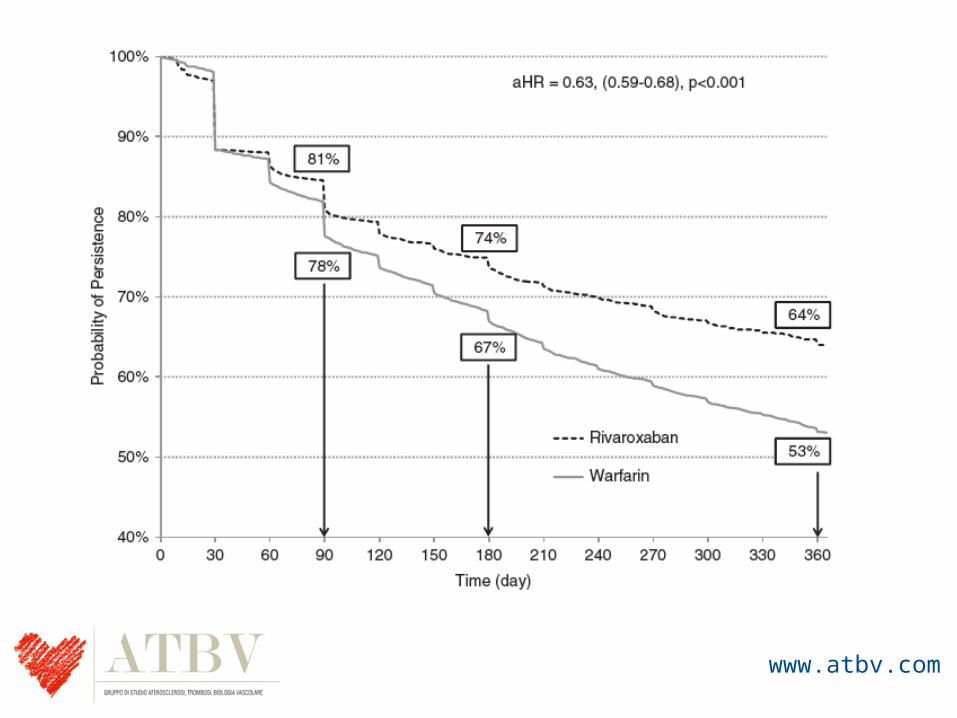
Current Medical Research & Opinion 2014, 1–9
www.atbv.com
www.atbv.com
Il Mondo Reale…
Apixaban
www.atbv.com
ApixabanTerzo NOAC, approvato da meno tempo rispetto a dabigatran e rivaroxaban. Non ci sono motivi per pensare che nel mondo reale debba comportarsi in modo diverso rispetto agli altri due NOAC
www.atbv.com
Conclusioni1. Contrariamente a quello che solitamente succede,
dove i risultati dei trials sono in parte mitigati dalle analisi dei registri, nel caso dei NOAC i registri confermano e anche amplificano i benefici osservati negli studi registrativi
2. Non dobbiamo quindi aver paura di utilizzare questi farmaci, perché a lungo termine i benefici saranno evidenti
www.atbv.com





























