Embed Size (px)
Citation preview

Don’t forget the men ! Don’t forget the men ! GynaecomastiaGynaecomastia
Professor Philip J DrewProfessor Philip J Drew

GynaecomastiaGynaecomastia
““Man boobs” Man boobs” “Moobs”“Moobs”IncreasingIncreasing
ActualActual Patient ExpectationsPatient Expectations
Male breast cancerMale breast cancer 1973 - 19981973 - 1998 0.86 – 1.08 / 100,000 men0.86 – 1.08 / 100,000 men
Giordano et al Cancer 2004

GynaecomastiaGynaecomastia
Definition:Definition: Histologically:Histologically:
Benign proliferation of glandular tissue of the male breastBenign proliferation of glandular tissue of the male breast Clinically:Clinically:
Rubbery firm mass extending concentrically from the Rubbery firm mass extending concentrically from the nipplenipple
Pseudogynaecomastia:Pseudogynaecomastia: Fat deposition without glandular proliferation Fat deposition without glandular proliferation
“lipomastia”“lipomastia”

GynaecomastiaGynaecomastia
Pathophysiology: due to oestrogen / androgen Pathophysiology: due to oestrogen / androgen imbalanceimbalance PrimaryPrimary SecondarySecondary
Decrease in androgenDecrease in androgen Actual / relativeActual / relative
Increased binding to SHBGIncreased binding to SHBG Receptor blockadeReceptor blockade
Increase in oestrogenIncrease in oestrogen Direct / indirect (precursors)Direct / indirect (precursors)

GynaecomastiaGynaecomastia HistologyHistology
Early “florid” phaseEarly “florid” phase OestrogenOestrogen
Ductal epithelial hyperplasiaDuctal epithelial hyperplasia Ductal elongation and branchingDuctal elongation and branching Proliferation periductal fibroblastsProliferation periductal fibroblasts
Later inactive senescent phaseLater inactive senescent phase Dense fibrous tissueDense fibrous tissue Breast enlargement may diminishBreast enlargement may diminish
Male / Female breast tissueMale / Female breast tissue Similar responsivenessSimilar responsiveness No acinar development in men (progesterone)No acinar development in men (progesterone)
Wilson RL et al Adv Intern Med 1980

GynaecomastiaGynaecomastia
AetiologyAetiology Persistent pubertal gynaecomastiaPersistent pubertal gynaecomastia 25%25% DrugsDrugs 10-25%10-25% IdiopathicIdiopathic 25%25% Cirrhosis or malnutritionCirrhosis or malnutrition 8%8% Primary hypogonadismPrimary hypogonadism 8%8% Testicular tumoursTesticular tumours 3%3% Secondary hypogonadismSecondary hypogonadism 2%2% HyperthyroidismHyperthyroidism 1.5%1.5%

Primary GynaecomastiaPrimary Gynaecomastia
Prevalence: “Trimodal”Prevalence: “Trimodal”
Infants:Infants: 60% to 90%60% to 90%
Pubertal:Pubertal: 30% to 60%30% to 60%
Adults:Adults: 24% to 80%24% to 80%
Wise et al J Am Coll Surg 2005

GynaecomastiaGynaecomastia
Pubertal gynaecomastiaPubertal gynaecomastia Bilateral 50-60%Bilateral 50-60% MidpubertyMidpuberty
Nydick et al Nydick et al 1855 boy scouts1855 boy scouts
65% 14 yr olds65% 14 yr olds 14% 16 yr olds14% 16 yr olds
Exact mechanism unknownExact mechanism unknown Oestrogen increases before testosteroneOestrogen increases before testosterone
Most resolve spontaneouslyMost resolve spontaneously
Moore DC J Clin Endocrinol Metab 1984Nydick et al J Am Med Soc 1961

GynaecomastiaGynaecomastia
Marked pubertal breast developmentMarked pubertal breast development 10% endocrine abnormality10% endocrine abnormality
Kleinfelter’s / XX malenessKleinfelter’s / XX maleness Primary testicular failurePrimary testicular failure Androgen insensitivityAndrogen insensitivity Increase aromatase activityIncrease aromatase activity
Autosomal dominant geneAutosomal dominant gene
Sher ES et al Clinical Paediatrics 1998

GynaecomastiaGynaecomastia
Age related “senescent” gynaecomastiaAge related “senescent” gynaecomastia Increases in normal men after 44yrs (57%)Increases in normal men after 44yrs (57%)
Histologically only 7% active phase Histologically only 7% active phase Bilateral >90%Bilateral >90% Peak 50-69yrs (72%)Peak 50-69yrs (72%) Decreases 70-89 yrs (47%)Decreases 70-89 yrs (47%)
>80% if BMI>25>80% if BMI>25
Nuttal FQ J Clin Endocrinol Metab 1979

GynaecomastiaGynaecomastia
Systemic IllnessSystemic Illness Liver diseaseLiver disease
Alcoholic cirrhosisAlcoholic cirrhosis Direct effect on hypothalamic-pituitary-testicular systemDirect effect on hypothalamic-pituitary-testicular system SHBG increased – decreases free testosteroneSHBG increased – decreases free testosterone
ThyrotoxicosisThyrotoxicosis SHBG increasedSHBG increased Increased peripheral aromatisationIncreased peripheral aromatisation 25-40% men with Grave’s disease25-40% men with Grave’s disease

GynaecomastiaGynaecomastia Chronic renal failureChronic renal failure
Dialysis patients: 50%Dialysis patients: 50% Leydig cell dysfunctionLeydig cell dysfunction
HIVHIV Antiretroviral therapyAntiretroviral therapy Inhibition of cytochrome P450 enzymeInhibition of cytochrome P450 enzyme
MalnutritionMalnutrition ““Refeeding” gynaecomastiaRefeeding” gynaecomastia Second pubertySecond puberty
Biglia A et al Clin Infect Diseases 2004Holdsworth et al N Engl J Med 1977Smith SR J Clin Endocrinol Metab 1975

GynaecomastiaGynaecomastiaTesticular neoplasms Testicular neoplasms
Germ cell tumoursGerm cell tumours 2.5-6% gynaecomastia at presentation2.5-6% gynaecomastia at presentation hCGhCG Leydig cell dysfunctionLeydig cell dysfunction
Inhibition of 17 alpha hydoxylase / 17,20 lyase enzymesInhibition of 17 alpha hydoxylase / 17,20 lyase enzymes Increased CYP450 aromatase activityIncreased CYP450 aromatase activity Poor prognostic signPoor prognostic sign
Same mechanism for other hCG producing tumoursSame mechanism for other hCG producing tumours Leydig cell tumourLeydig cell tumour
2% testicular neoplasms2% testicular neoplasms Testosterone and oestrodiol Testosterone and oestrodiol 6-10 yr olds6-10 yr olds
Precocious pubertyPrecocious puberty 26-35 yr olds26-35 yr olds
Testicular mass, impotenceTesticular mass, impotence 20-30% have gynaecomastia at presentation20-30% have gynaecomastia at presentation

GynaecomastiaGynaecomastia Other tumoursOther tumours
ProlactinomaProlactinoma 8%8% Hypogonadotrophic hypogonadismHypogonadotrophic hypogonadism
Large cell calcifying Sertoli cell (sex-cord) tumoursLarge cell calcifying Sertoli cell (sex-cord) tumours Increased aromatase activity Increased aromatase activity SporadicSporadic Autosomal dominantAutosomal dominant
Peutz-Jehger’s syndromePeutz-Jehger’s syndrome Carney complexCarney complex
Feminising adrenocortical tumoursFeminising adrenocortical tumours 98% gynaecomastia98% gynaecomastia 58% palpable adrenal tumour58% palpable adrenal tumour 50% testicular atrophy50% testicular atrophy
Pituitary / Hypothalamic tumoursPituitary / Hypothalamic tumours
Braunstein GD Endocr Related Cancer 1999

GynaecomastiaGynaecomastia True hermaphroditismTrue hermaphroditism
Testicular and ovarian tissueTesticular and ovarian tissue Excessive oestrogen productionExcessive oestrogen production
Direct affectDirect affect Suppression of intratesticular cytochrome P450 Suppression of intratesticular cytochrome P450
Androgen insensitivity syndromesAndrogen insensitivity syndromes Defect or absence intracellular androgen receptor Defect or absence intracellular androgen receptor SpectrumSpectrum
Complete absence “testicular feminisation”Complete absence “testicular feminisation” Phenotypic femalesPhenotypic females
Complete / partial insensitivityComplete / partial insensitivity Phenotypic malesPhenotypic males
Quigley CA et al Endocr Rev 1995

GynaecomastiaGynaecomastia Primary hypogonadismPrimary hypogonadism
CongenitalCongenital Klinefelter’s syndromeKlinefelter’s syndrome
Lobular struturesLobular strutures 16 fold increase in breast cancer16 fold increase in breast cancer
AcquiredAcquired TraumaTrauma InfectionInfection InfiltrationInfiltration Vascular insufficiencyVascular insufficiency AgeAge
Decrease in testosteroneDecrease in testosterone Increase in LH releaseIncrease in LH release Increase in aromatisation of testosterone to estradiolIncrease in aromatisation of testosterone to estradiol

GynaecomastiaGynaecomastia
Secondary hypogonadismSecondary hypogonadism Prostate cancer treatmentProstate cancer treatment
Combined androgen blockadeCombined androgen blockade 50%50% LH-RH analogue aloneLH-RH analogue alone 25%25% Orchidectomy aloneOrchidectomy alone 10%10% Combined drug + orchidectomyCombined drug + orchidectomy 1-24%1-24%
Dicker AP Lancet Oncol 2003

GynaecomastiaGynaecomastia BPHBPH
FinesterideFinesteride Type II 5 alpha – reductase inhibitor Type II 5 alpha – reductase inhibitor Blocks testosterone to DHT conversionBlocks testosterone to DHT conversion Increase tesosterone – precursor to oestrodiolIncrease tesosterone – precursor to oestrodiol Oestrodiol increase leads to gynaecomastiaOestrodiol increase leads to gynaecomastia
But...increased risk of male (and female) breast But...increased risk of male (and female) breast cancer cannot be excludedcancer cannot be excluded Total data (MHRA Dec 2009): Total data (MHRA Dec 2009):
90,000 pt/yr exposure, rate7.82 per 100,000 PYR90,000 pt/yr exposure, rate7.82 per 100,000 PYR 80,000 placebo / yr exposure, rate 3.84 per 100,000 PYR80,000 placebo / yr exposure, rate 3.84 per 100,000 PYR P=0.328P=0.328

GynaecomastiaGynaecomastia
Anabolic steroidsAnabolic steroids 52% gynaecomastia52% gynaecomastia 57% testicular atrophy57% testicular atrophy
Self medicate with Tam Self medicate with Tam or AI for gynaecomastiaor AI for gynaecomastia
hCG for testicular hCG for testicular atrophyatrophy
Clomiphene / NolvadexClomiphene / Nolvadex ““PCT”PCT”
Post cycle therapyPost cycle therapy

GynaecomastiaGynaecomastia Other causesOther causes
Diabetic mastopathyDiabetic mastopathy Not related to type of insulinNot related to type of insulin Mimics gynaecomastia clinicallyMimics gynaecomastia clinically Different histologicallyDifferent histologically
OccupationalOccupational MorticiansMorticians
Very unusual causesVery unusual causes Drinking female urineDrinking female urine
Vierhapper H Lancet 1999

GynaecomastiaGynaecomastia
Drug therapyDrug therapy Large number implicatedLarge number implicated Obvious association with hormonal agentsObvious association with hormonal agents Difficult to confirm for other agents Difficult to confirm for other agents
Thompson & CarterThompson & Carter ProbableProbable
Ca channel blockers, chemotherapy, HCa channel blockers, chemotherapy, H2 2 blockers, blockers, ketoconazole, spirinolactoneketoconazole, spirinolactone
InconclusiveInconclusive Digitalis, neuroleptic agents and marijuanaDigitalis, neuroleptic agents and marijuana
Thompson DF & Carter JR Pharmacotherapy 1993

GynaecomastiaGynaecomastia
Assessment: Assessment:
ClinicalClinical Imaging - ? mammogram / ultrasoundImaging - ? mammogram / ultrasound Tissue ? Core biopsyTissue ? Core biopsy
Not Not FNAC – C3 resultFNAC – C3 result

GynaecomastiaGynaecomastia
Clinical assessmentClinical assessment HistoryHistory
Age of onsetAge of onset DurationDuration Family historyFamily history
Aromatase excesss syndromeAromatase excesss syndrome Auto dominantAuto dominant Chromosome 15Chromosome 15
Underlying disordersUnderlying disorders HyperthyroidismHyperthyroidism Hepatic / Renal diseaseHepatic / Renal disease
Loss of libido / impotenceLoss of libido / impotence Drug historyDrug history

GynaecomastiaGynaecomastia ExaminationExamination
Swelling of the breastSwelling of the breast TenderTender Concentric Concentric MobileMobile
Sinister findingsSinister findings Eccentric, unilateral, nipple retraction, skin dimpling, Eccentric, unilateral, nipple retraction, skin dimpling,
lymphadenopathy, nipple discharge lymphadenopathy, nipple discharge PseudogynaecomastiaPseudogynaecomastia
No resistance to apposition of fingersNo resistance to apposition of fingers Abdominal / chest / ? testes examinationAbdominal / chest / ? testes examination

GYNAECOMASTIA – GYNAECOMASTIA – CLASSIFICATIONCLASSIFICATION
Simons et al ( 1973 )Simons et al ( 1973 )
I.I. Minor breast Minor breast enlargement without enlargement without skin redundancyskin redundancy

GynaecomastiaGynaecomastia
InvestigationInvestigation Teenager with otherwise normal examinationTeenager with otherwise normal examination
Re-examine to establish whether persistentRe-examine to establish whether persistent
Adult or persistent/marked pubertal Adult or persistent/marked pubertal gynaecomastia gynaecomastia BCP, Prolactin, LH, Oestrogen, Testosterone, hCGBCP, Prolactin, LH, Oestrogen, Testosterone, hCG Consider genetic causes Consider genetic causes

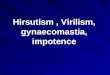
GynaecomastiaGynaecomastia
hCG, LH, Testosterone, Estrogen
Increased hCGIncreased LHDecreased
Testosterone
Increased LH and
Testosterone
Testicular ultrasound
Normal-CXR /
abdominal CT
Normal
Primary hypogonadism
Check TSH
Normal –Androgen resistance
Idiopathic gynaecomastia

GynaecomastiaGynaecomastia
Imaging / biopsyImaging / biopsy MammographyMammography
Negative predictive value for malignancy: 99%Negative predictive value for malignancy: 99%
Ultrasound +/- core biopsyUltrasound +/- core biopsy Imaging for clinical gynaecomastia no longer Imaging for clinical gynaecomastia no longer
supported by RCRsupported by RCR
Evans et al Am J Surg 2001

GynaecomastiaGynaecomastia
Primary gonadal failure Primary gonadal failure ““Hypogonadism”Hypogonadism” ““Andropause” Andropause”
Consider endocrinology referralConsider endocrinology referral Testosterone Replacement Therapy?Testosterone Replacement Therapy?
No mature data from large trialsNo mature data from large trials

GynaecomastiaGynaecomastia
TRTTRT Potential benefits / drawbacksPotential benefits / drawbacks
Bone densityBone density CognitionCognition Muscle mass / body compositionMuscle mass / body composition MoodMood ErythropoiesisErythropoiesis LibidoLibido

GynaecomastiaGynaecomastia
TRTTRT Potential harmPotential harm
?Cardiovascular disease?Cardiovascular disease Putative relationshipPutative relationship Studies actually show favourable effect Studies actually show favourable effect
Prostate risksProstate risks Mild increase in volume Mild increase in volume Theoretical cancer riskTheoretical cancer risk
Snyder PJ J Clin Endocrinol Metab 2000

Treatment of GynaecomastiaTreatment of Gynaecomastia Indications Indications
PainPain TendernessTenderness Embarrassment interfering with normal activityEmbarrassment interfering with normal activity
OptionsOptions Medical Medical
SurgicalSurgical

GynaecomastiaGynaecomastia Non-surgical treatmentNon-surgical treatment
Reassure and observeReassure and observe Painful for 6-12 months during florid phasePainful for 6-12 months during florid phase Revue medicationRevue medication Correct obesity / lifestyleCorrect obesity / lifestyle
MedicationMedication Little good dataLittle good data End points difficult to assessEnd points difficult to assess
Tends to resolve anywayTends to resolve anyway Pain is self limitingPain is self limiting

GynaecomastiaGynaecomastia
Medical therapyMedical therapy ClomipheneClomiphene DanazolDanazol TamoxifenTamoxifen Aromatase InhibitorsAromatase Inhibitors

GynaecomastiaGynaecomastia Clomiphene 50-100mg day Clomiphene 50-100mg day
Evaluated in adolescentsEvaluated in adolescents Unproven efficacy especially at 50mgUnproven efficacy especially at 50mg May achieve up to 64% resolution May achieve up to 64% resolution Adverse effects rareAdverse effects rare
Danazol 400mg day Danazol 400mg day Evaluated in adolescents (200mg day)Evaluated in adolescents (200mg day) Objective response 20-76% Objective response 20-76% Side effects commonSide effects common
Weight gain, acne, abnormal LFT’sWeight gain, acne, abnormal LFT’s
LeeRoith et al Acta Endocrinol 1980Jones DJ et al Ann RCS Eng 1990

GynaecomastiaGynaecomastia Tamoxifen Tamoxifen
Not evaluated in adolescentsNot evaluated in adolescents Generally poorly designed trials and auditsGenerally poorly designed trials and audits
Total of 136 patients in 5 trialsTotal of 136 patients in 5 trials Only 113 studied prospectivelyOnly 113 studied prospectively No randomised controlled studiesNo randomised controlled studies Doses of 10, 20 & 40mg usedDoses of 10, 20 & 40mg used From this “evidence” in adultsFrom this “evidence” in adults
Reduces pain:Reduces pain: 70-100%70-100% May decrease lump:May decrease lump: 50-80%50-80%
AmoxifeneAmoxifene 4-OH Tam gel4-OH Tam gel No significant systemic levelNo significant systemic level Trial in design stage (Hull / Cardiff)Trial in design stage (Hull / Cardiff)
Plourde PV et al J Clin Endocrinol Metab 2004Kahn HN, Blamey RW BMJ 2003

GynaecomastiaGynaecomastia
Aromatase InhibitorsAromatase Inhibitors One RCT in adolescentsOne RCT in adolescents
Pain reducedPain reduced No effect on lumpNo effect on lump
Theoretical risksTheoretical risks Bone healthBone health LH increases leading to peripheral aromatisationLH increases leading to peripheral aromatisation
Not use AI’s for male breast cancerNot use AI’s for male breast cancer

GynaecomastiaGynaecomastia
Prostate cancer therapyProstate cancer therapy BicalutamideBicalutamide Dose dependent response to Tamoxifen Dose dependent response to Tamoxifen
prohylaxisprohylaxis 8.8% on 20mg/day8.8% on 20mg/day 96.7% placebo96.7% placebo No increase in PSANo increase in PSA
AlternativesAlternatives Low dose irradiationLow dose irradiation
Fradet, Yves, Egerdie et al Europ Urol. 2007 52(1): 106-114

Gynaecomastia - SurgeryGynaecomastia - Surgery
Glandular enlargement with no/little Glandular enlargement with no/little excess skinexcess skin ?liposuction alone – will not remove ?liposuction alone – will not remove
glandular elementglandular element Ultrasound assisted Ultrasound assisted
Risk of thermal damageRisk of thermal damage
Minimally invasive gland excision +/- Minimally invasive gland excision +/- liposuctionliposuction

USS Guided InterventionUSS Guided Intervention
VABDVABD Initially diagnosticInitially diagnostic
Burbank, Parker, Fogarty Am J Surg 1996Burbank, Parker, Fogarty Am J Surg 1996 TherapeuticTherapeutic
Zannis, Aliano Am J Surg 1998Zannis, Aliano Am J Surg 1998

VABDVABD
Breast vacuum biopsy systemBreast vacuum biopsy system Hand heldHand held Multiple sampling through a single Multiple sampling through a single
incisionincision
Introduction of 8-gauge probeIntroduction of 8-gauge probe Therapeutic procedures Therapeutic procedures

MammotomeMammotome®® Technique Technique

Gynaecomastia - VABDGynaecomastia - VABD
Hull Breast UnitHull Breast Unit PatientsPatients
59 men 59 men Mean age 38 (range 21-80)Mean age 38 (range 21-80)
GradeGrade Grade 1/2Grade 1/2 14 unilateral14 unilateral

GynaecomastiaGynaecomastia
ComplicationsComplications Haematoma n=2Haematoma n=2
Spontaneously resolvedSpontaneously resolved (“Bruising” inevitable)(“Bruising” inevitable)
Recurrence n=2Recurrence n=2 Re-mammotomeRe-mammotome
Iwuagwu O et al Annals of Plastic Surgery 2004

GynaecomastiaGynaecomastia
Operating timeOperating time 50 min (range 20-60 min)50 min (range 20-60 min)
Patient satisfaction:Patient satisfaction: 8-9/108-9/10 Cosmesis:Cosmesis: 9-10/109-10/10

GynaecomastiaGynaecomastia

Gynaecomastia - Surgery
Excess skin +Consider staged operation
Liposuction+/- skin excision
Periareolar breast reduction
Excess skin +++Consider Wise pattern, vertical scar etc.
Beware hypertrophic scarsRepeated periareolar operations

SURGICAL TECHNIQUESURGICAL TECHNIQUE
Pre-operative markings – standingPre-operative markings – standing
Operative patient position : semi-sittingOperative patient position : semi-sitting
Infiltrate breast with adrenaline solutionInfiltrate breast with adrenaline solution( 1 litre Ringers, 1ml 1: 1000 adrenaline , LA )( 1 litre Ringers, 1ml 1: 1000 adrenaline , LA )

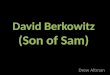
GYNAECOMASTIA ASSESSMENT – GYNAECOMASTIA ASSESSMENT – NIPPLE POSITIONNIPPLE POSITION
A = ( 0.19 chest circumference ) + 2.192 cmA = ( 0.19 chest circumference ) + 2.192 cm
B = ( 0.12 height ) – 2.782 cmB = ( 0.12 height ) – 2.782 cm
A
B
•Shulman et al PRS 2001

CIRCUMAREOLARCIRCUMAREOLAR CONCENTRIC SKIN REDUCTION CONCENTRIC SKIN REDUCTION

CIRCUMAREOLAR CIRCUMAREOLAR CONCENTRIC SKIN REDUCTIONCONCENTRIC SKIN REDUCTION

CIRCUMAREOLARCIRCUMAREOLAR CONCENTRIC SKIN REDUCTION CONCENTRIC SKIN REDUCTION

CIRCUMAREOLAR CONCENTRIC SKIN CIRCUMAREOLAR CONCENTRIC SKIN REDUCTIONREDUCTION

CIRCUMAREOLAR CIRCUMAREOLAR CONCENTRIC SKIN REDUCTIONCONCENTRIC SKIN REDUCTION

CIRCUMAREOLARCIRCUMAREOLAR CONCENTRIC SKIN REDUCTION CONCENTRIC SKIN REDUCTION

CIRCUMAREOLAR CONCENTRIC SKIN CIRCUMAREOLAR CONCENTRIC SKIN REDUCTIONREDUCTION

Pseudo-gynaecomastia after Pseudo-gynaecomastia after massive weight lossmassive weight loss

VERTICAL SCAR REDUCTION VERTICAL SCAR REDUCTION TECHNIQUETECHNIQUE

VERTICAL SCAR REDUCTION VERTICAL SCAR REDUCTION TECHNIQUETECHNIQUE

VERTICAL SCAR TECHNIQUEVERTICAL SCAR TECHNIQUE

GYNAECOMASTIA SURGERY – GYNAECOMASTIA SURGERY – SKIN REDUCTIONSKIN REDUCTION

GYNAECOMASTIA SURGERY – GYNAECOMASTIA SURGERY – SKIN REDUCTIONSKIN REDUCTION

GYNAECOMASTIA SURGERY – GYNAECOMASTIA SURGERY – SKIN REDUCTIONSKIN REDUCTION

GYNAECOMASTIA SURGERY – GYNAECOMASTIA SURGERY – SKIN REDUCTIONSKIN REDUCTION

GYNAECOMASTIA SURGERY – GYNAECOMASTIA SURGERY – SKIN REDUCTIONSKIN REDUCTION
Gusenoff et al Plas. Recon. Surg. 122: p1301, 2008

GynaecomastiaGynaecomastia
Surgical complicationsSurgical complications Scarring and adherence to underlying muscleScarring and adherence to underlying muscle Excessive resectionExcessive resection
Contour deformityContour deformity
SolutionsSolutions Local dermoglandular flapsLocal dermoglandular flaps LipomodellingLipomodelling
Autologous fat injectionsAutologous fat injections

GynaecomastiaGynaecomastia
Summary Summary Usually “normal” or iatrogenicUsually “normal” or iatrogenic Occasional underlying diseaseOccasional underlying disease Consider primary gonadal failure in the Consider primary gonadal failure in the
mature malemature male InvestigateInvestigate
Persistent or extreme cases in adolescentsPersistent or extreme cases in adolescents AdultsAdults

GynaecomastiaGynaecomastia SummarySummary
TreatmentTreatment MedicalMedical
Little good dataLittle good data Tamoxifen in adults onlyTamoxifen in adults only
SurgicalSurgical Do the least required to achieve patient’s desiresDo the least required to achieve patient’s desires Not supported by PCT unless “exceptional”Not supported by PCT unless “exceptional”
Grade 1/2aGrade 1/2a Minimally invasive plus liposuctionMinimally invasive plus liposuction
Grade 2b/3Grade 2b/3 Aesthetic techniquesAesthetic techniques

GynaecomastiaGynaecomastia
ConclusionConclusion Common benign conditionCommon benign condition ? Normal part of ageing? Normal part of ageing No licensed effective medicationNo licensed effective medication Trial neededTrial needed ?Minimally invasive surgery operation of ?Minimally invasive surgery operation of
choice if appropriatechoice if appropriate