Embed Size (px)
Citation preview

Langenbecks Arch Chir (1994) 379:8-12 Langenbecks f Chirul'gie
© Springer-Verlag 1994
Donor criteria in hepatic transplantation S. Jonas, W. O. Bechstein, H. Keck, H. P. Lemmens, G. Blumhardt, P. Neuhaus
Chirurgische Klinik und Poliklinik, Universit/itsklinikum Rudolf Virchow der Freien Universit/it Berlin
Received: 7 December 1992
Spenderkriterien bei Lebertransplantation
Zusammenfassung. Nach 201 Lebertransplantationen von September 1988 his November 1991 wurde retro- spektiv der Postischfimieschaden bei Vorliegen verschie- dener Spenderkriterien untersucht. Als Kriterien galten die Hospitalisierungszeit auf Intensivstation vor Organ- entnahme, die Todesursache sowie allgemein als kritisch eingeschfitzte Parameter wie hypotensive Kreislaufpha- sen (n = 69; 34,4%), kardiopulmonale Reanimation (n = 20; 9,9%), erh6hte Serumtransaminasen (s-AT) (n = 11; 5,5%) oder ein Alter fiber 50 Jahre (n = 16; 8,0%). 91 Organspender lagen weniger als 24 h auf einer Intensivstation, hingegen 29 Spender (14,4%) 4-6 Tage und 14 Spender (7,0%) lfinger als 6 Tage. Hfiufigste To- desursachen waren Subarachnoidalblutungen (n = 70; 34,8 %), isolierte Schfidel-Hirn-Traumen (n = 68; 33,8%) und Polytraumen (n = 33; 16,4%). Der Post- ischfimieschaden wurde anhand der maximalen postope- rativen s-AT sowie der Inzidenz eines primfiren Trans- plantatversagens (PNF) oder einer schweren, reversiblen Transplantatschfidigung (s-AT > 2000 1U/I) abgeschfitzt. Maximale s-AT, Alter der Organspender und -empffinger sowie kalte Isch~miezeiten unterschieden sich zwischen den einzelnen Gruppen nicht signifikant. Schwere rever- sible Schfiden zeigten 14 Transplantatlebern (7,0 %); eine PNF trat in 5 Ffillen (2,5%) auf, die erfolgreich einer friihen Retransplantation unterzogen wurden. Spender- kriterien waren in beiden Gruppen mit fihnlicher Hfiufig- keit wie im Gesamtkollektiv vertreten. Maximale s-AT bei Transplantatversagen (GOT: 4944-L-_ 2280 1U/I; GPT: 3186 ± 1918 1U/I) lagen signifikant (p > 0,01) h6- her als bei prim~irer Transplantatfunktion (GOT: 699 ___ 935 1U/I; GPT: 620 ± 701 1U/I). Diese Ergebnisse sind trotz eines hohen Anteils bislang als kritisch angese- hener Spender Ausdruck einer vermutlich zu strengen Selektion. Eine vorsichtige Lockerung der Selektionskri- terien erscheint daher gerechtfertigt.
Correspondence to." Dr. S. Jonas, Chirurgische Klinik und Poli- klinik, Universitfitsklinikum Rudolf Virchow der Freien Univer- sit/it Berlin, Augustenburger Platz 1, D-13353 Berlin, Germany
Schliisselw6rter: Spenderkriterien - Postischfimieschaden - Transplantatversagen
Abstract. The early outcome of 201 liver grafts trans- planted consecutively between September 1988 and November 1991 was investigated retrospectively. Donors were categorized according to their hospitalization peri- ods in an intensive care unit (ICU) prior to harvesting, their causes of death, and the variables generally believed to be critical in liver donation, such as arterial hypoten- sion (n = 69; 34.3%), cardiopulmonary resuscitation (n = 20; 9.9%), elevated serum-aminotransferases (s- AT) (n = 11; 5.5%), or an age over 50 years (n = 16; 8.0 %). Ninety-one donors (45.3 %) spent less than 24 h in an ICU; 29 donors (14.4%) and 14 donors (7.0%) had hospitalization periods generally considered critical of 4 -6 days and more than 6 days, respectively. The most common causes of death were subarachnoidal bleeding (n = 70; 34.8%), isolated head injuries (n = 68; 33.8%), and polytraumata (n = 33; 16.4%).The postischemic hepatocellular damage was evaluated comparing peak post-transplant s-AT, which did not differ significantly between groups; nor did donor and recipient ages or cold ischemia times. Fourteen grafts (7.0%) showed a re- versible preservation injury presenting with post-trans- plant s-AT elevated above 2000 IU/1. Five cases (2.5%) of a primary non-functioning graft (PNF) underwent ear- ly retransplantation successfully. Serum-aminotrans- ferases (AST: 4944 ± 2280 IU/1; ALT' 3186 ± 1918 IU/ l) were significantly (P < 0.01) elevated as compared to primary functioning grafts (AST: 699 ± 935 IU/1; ALT" 620 ±_ 701 IU/1). The donor structure of both groups re- flected the distribution of variables in the entire collec- tive. No significant overrepresentations were observed. These results indicate that in the past criteria for donor selection have probably been applied too stringently. To determine true limits the pool of liver donors should care- fully be extended.

Assessment of a potential graft is crucial in hepatic transplantation. The first report of the European Liver Registry disclosed that of 585 deceased recipients 35 (6%) had died of a primary non-functioning graft (PNF) and that of 97 retransplantations 23 (24%) were due to a PNF [21.
Methods predicting subsequent graft function are ei- ther of limited reliability, e.g., intra0Perative liver biop- sies [7], or cannot yet be applied in the clinical routine such as 3*P-magnetic resonance spectroscopy [8]. The measurement of lidocaine metabolite monoethylglycine xylidide (MEGX) seems to be the most promising tool in organ-quality assessment [11].
Donor criteria remain essential in the decision of the transplanting institution to send a team for harvesting or, if procurement is done by other teams, to accept a shipped graft. Criteria for donor selection are not widely agreed upon, as indicated by varying donor age limits from 40 years [141 to 60 years [41. More extensive studies have also not revealed exclusion criteria either, thus rec- ommending a less stringent donor selection [6, 9]. We investigated retrospectively the outcome after transplan- tation of grafts originating from donors generally consid- ered critical.
Methods
Between September •988 and November 1991 201 consecutive do- nor hepatectomies and transplantat ions were performed and the records reviewed retrospectively. Donors were categorized accord- ing to the cause of death, the hospitalization period on an intensive care unit (ICU) prior to organ harvesting, and variables assumed to be critical in liver donation. These variables consisted of blood pressure instability (a drop in mean arterial pressure below 60 mmHg for more than 20 min), cardiac arrest with cardiopul-
monary resuscitation, a donor age of more than 50 years, or elevat- ed preoperative serum aminotransferases (s-AT) [13, 15].
In the different groups donor and recipient age, as well as the cold ischemic times (CIT) - measured from aortic cross-clamping in the donor until unclamping the hepatic artery and portal vein in the recipient - were compared.
The rate of hepatocellular damage was assessed either by match- ing the peaks of post-transplant s-AT in the different groups or by analyzing the donor structure of collectives presenting with a prima- ry non-function (PNF) or s-AT elevated above 2000 IU/1 until the second post-transplant day [5]. PNF was not diagnosed if a graft failed due to histologically confirmed rejection or vascular throm- bosis [16].
Statistical evaluation was performed using the Mann-Whitney U test or the Z 2 test.
Results
The 201 donors ranged in age from 10 to 60 years (30.8+11.9 years) compared with a range of 16 to 64 years (44.2+_11.2 years) for the recipients. There were 138 male (68.7%) and 63 female donors (3•.3%). Except for two cases all organs had been preserved using Univer- sity of Wisconsin solution (UW). The remaining grafts had both been shipped and were preserved by Euro- Collins' solution (EC). Cold ischemia times (CIT) varied between 4:20 h and 24:•5 h (10:39___4:06 h).
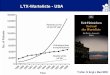
Prior to harvesting, blood pressure instability oc- curred in 69 donors (34.3%); 20 donors (9.9%) under- went cardiopulmonary resuscitation; 16 donors (8.0%) were older than 50 years; in 11 donors (5.5%) s-AT elevated over 100 IU/1 could be observed (Fig. 1). In the latter group AST and ALT ranged from 111 IU/1 to 803IU/1 (215+-213IU/1) and 53IU/1 to 608IU/1 (148+_ 168 IU/1), respectively. One or more of the men- tioned criteria were met by 19 donors (9.5%), two or
arterial hypotension ~ n=69
more than 1 criterion
resuscitation ~ n=20
age over 50years ~ n=16
elevated s-AT ~ n= 11
~ n=18
more than 2 criteria
no criterion
n=4
less than 24 h
2~0 ' ~ 10 30 40 50 60
24 to 48h N n = 4 0
48 to 72h ~ n = 2 7
4to6days ~ n = 2 9
l week or longer ~n=14
I I
10 20 J I
30 40
SAB
isolated head injury
polytrauma
brain tumor
cranial gun shot
strangulation
cerebral idfarction
drowning
status astmaticus
methanol intoxication
50 1 relative frequency (%) 2 relative frequency (%)
Fig. 1. Incidences of critical variables in 201 liver donors Fig. 2. Relative frequencies of the donor hospitalization periods in an intensive care unit prior to harvesting Fig. 3. Causes of death of 201 liver donors
n 7;"//////~ ":
~ n=33
~ n=9
~ n=8
0=4
n=4
n=2
n = 2
n = t
I I I I I i I
10 20 30 40 relative frequency (%)

10
Table 1. Peak post-transplant serum-aminotransferases (s-AT), do- nor and recipient age, and cold ischemia time (CIT) according to critical variables, donor hospitalization periods on an intensive care unit (ICU) prior to harvesting, causes of death, and the incidence of
primary non-function (PNF) or a reversible preservation injury (SAB, subarachnoidal bleeding; NS, not significant; *P<0.05; **P<0.01)
Peak AST Peak ALT ' Donor age Recipient age CIT (IU/1) (IU/1) (years) (years) (h :min)
Arterial hypotension Normotension
Resuscitation No resuscitation
Age over 50 years Age under 50 years
Elevated s-AT Normal s-AT
No criterion One criterion or more Two or more criteria Three or more criteria
ICU stay: <24h 24 h-48 h 48 h-72 h 4 days-6 days
> 6 days
SAB Isolated head injury Polytrauma Brain tumor Cranial gunshot wound
PNF Primary function
s-AT > 2000 IU/1 s-AT < 2000 IU/I
789_+1295 655_+ 920 30.8-1-11.8 45.9_+10.2 NS 10:57_+3:46 813-+1120 NS 700_ 804 NS 31.2-+12.1 NS 43.4+11.7 10:29_+4:16 NS
664_+ 713 645_ 713 26.6_+10.4 48.0_+ 9.6 11:13_+4:26 820_+1223 NS 688_+ 853 NS 31.3___12.0 NS 43.8-+11.3 NS 10:35-+4:04 NS
1134-+ 1879 817-+ 1081 43.5_+ 10.9 10:56_+5:02 774_+1098 NS 672___ 822 NS 44.3_+11.3 NS 10:37_+4:01 NS
715_+ 472 714+_ 483 22.8_+ 4.5 37.3-+10.3 12:17-+4:53 810-+1210 NS 682_+ 862 NS 30.4+12.0 NS 44.7+11.2 NS 10:33+4:02 NS
756-+ 975 653-+ 733 29.3_+10.1 43.7_+11.8 10:06_+3:52 850_+1381 713-+ 959 32.5_+19.6 44.9_+10.7 11:17_+4:16 636_+ 602 530_+ 495 31.2_+13.6 46.9+10.4 10:43+_3:44 509_+ 458NS 541. 554NS 20.5_+ 4.0NS 40.3_+ 6.9NS 9:54-+3:55NS
657-+ 848 581-+ 695 32.2_+12.8 44.6_+12.0 10:32_+3:44 998_+ 1753 824_+ 1253 28.9_+ 11.0 42.8_+ 11.4 11:14+4:34 999-+1625 742_+ 875 31.1_+12.1 42.4-+10.4 11:16_+4:23 841-+ 892 637+ 575 31.0-+ 9.8 44.0_+10.8 9:22_+2:39 951_+ 1133 NS 935_+ 955NS 27.8_+ 11.0 NS 47.1_+ 10.0 NS 11:24-+5:21NS
866-+ 917 684_+ 663 39.8_+10.5' 44.0_+11.8 11:03_+4:04 788_+1322 675_+ 839 25.9_+ 9.9 44.3_+11.2 10:08_+3:38 619___ 818 598_+ 753 23.7_+ 6.5* 43.7-+11.7 10:03_+4:30 819_+1141 859_+1036 32.3_+15.9 44.8_+ 9.8 9:55-+3:27 389_+ 270 NS 369_+ 211 NS 25.1_+ 7.9 48.1+_10.6 NS 14:45-+5:18 NS
4944-+2280 3186-+1918 28.3-+ 7.0 50.0_+ 6.4 11:49_+5:54 699_+ 935** 620_+ 701"* 30.9_+12.0 NS 44.1_+11.3 NS 10:37_+4:03 NS
3760 _+ 1835 2609 + 1308 37.1 _+ 12.4 46.9 _+ 11.4 11 : 27 -I- 3 : 50 499_+ 442** 483_+ 435** 30.3_+11.8 NS 44.1_+11.2 NS 10:35_+4:08 NS
more criteria by 4 donors (2.0%). Approximately half of the donors (n=107; 53.2%) did not comply with any of the critical variables. Donor and recipient age as well as CITs did not differ significantly between groups (Table 1). Peak postoperative s-AT for the different groups are shown in Table 1. Compared to the respective controls elevated values were evident only after trans- plantat ion of grafts originating f rom donors older than 50 years. However, this difference did not reach statistical significance. The accumulation of at least two or three critical variables in one donor did not result in an in- creased hepatocellular damage.
Before harvesting, 91 donors (45.3%) spent less than 24 h on an ICU, 40 donors (19.9%) 24 -48h , 27 donors (13.4%) 48 -72 h, 29 donors (14.4%) 4 - 6 days, and 14 donors (7.0%) at least 1 week up to a max imum of 18 days (Fig. 2). The lowest postoperative levels of hepa- tocellular enzymes could be detected after transplanta- tion of grafts coming f rom donors with the shortest hos- pitalization periods on an ICU (Table 1). A rise in en- zyme levels of about 50% was observed if donors had spent 24 -48 h on an ICU as compared to the less than 24-h hospitalized group. Hospitalization periods even longer than 48 h did not affect hepatocellular outcome adversely. Due to high standard deviations differences
did not prove statistically significant, nor did the patterns of donor and recipient ages or CITs in the different groups (Table 1).
Subarachnoidal bleeding in 70 donors (34.8 %), an iso- lated head injury in 68 donors (33.8%), and multiple injuries in 33 donors (16.4%) were the most common causes of death (Fig. 3). The other indicated causes each accounted for less than 5%. Peak postoperative s-AT, donor and recipient ages, and CITs did not vary signifi- cantly between groups (Table 1). Because of the small numbers involved, the lower peak enzyme levels in the group of grafts originating f rom donors with a cranial gunshot wound did not attain statistical significance.
Of the 201 grafts, 14 (7.0%) showed a reversible ischemic-preservation injury presenting with s-AT of more than 2000 IU/1 until the second postoperative day. There were five cases (2.5%) of PNF, all requiring early retransplantation between postoperative day 3 and 13 (median: day 4). The retransplantation on postoperative day 13 was due to an intrahepatic hematoma in a graft f rom a donor with multiple injuries. Peak values of s-AT in P N F grafts (AST: 4944__2280 IU/1; ALT: 3186 +__ 1918 IU/1) were significantly (P < 0.01) elevated as compared to pr imary functioning grafts (AST: 690_+ 952 IU/1; ALT: 615 __ 720 IU/1).

11
cardiac arrest arterial
age over arterial hypotension 50 years l hypotension
no criterion n.s. no criterion a b n.s.
Fig. 4 a, b. Livers from donors with critical variables to grafts pre- senting with a reversible preservation injury (a) or primary nonfunc- tion (b) (n.s., not significant)
less than 24h less than 24h 24h- 48h 24h- ~ ~ - 2 ~ 48h
> 6
days 6
4days- ~ days 48h-72h 6days 48h-72h
n.s. a n,s. b
Fig. 5 a, b. Livers according to the donors' periods on an intensive care unit prior to harvesting of grafts presenting with a reversible preservation injury (a) or primary nonfunction (b) (n.s., not signif- icant)
SAB isol. HI
n.s. n,s. a b
Fig. 6 a, b. Livers according to donors' causes of death wi th grafts presenting with a reversible preservation injury (a) or primary non- function (b) (SAB, subarachnoidal bleeding; isol HI, isolated head injury; POLY, polytrauma; M-Tox, methanol-intoxication; CI, cere- bral infarction; ASTRO, astrocytoma; n.s., not significant)
In the group showing reversible ischemic-preservation damage, critical variables (Fig. 4 a), hospitalization peri- ods on an ICU (Fig. 5a), and causes of death (Fig. 6a) had much the same distribution pattern as in the entire series. The injury in the graft from the one donor who had died of methanol intoxication represented the only excep- tion, albeit this also resolved spontaneously.
Concerning critical variables, the PNF group was composed of three grafts from donors who had not met any of the above indicated criteria (Fig. 4 b). ICU hospi- talization periods in the PNF group roughly resembled their share in the group of primary functioning grafts (Fig. 5 b). However, the liver of the longest hospitalized donor mentioned showed a PNE As to the causes of death, a conglomeration of different diagnoses each ac-
counted for one PNF graft (Fig. 6b). The reversibily damaged and PNF groups displayed no statistically sig- nificant differences as compared to the respective remain- ing groups.
Discussion
This retrospective study gives evidence that the parame- ters of donor assessment commonly used will not predict early graft function if they are applied as in the past. Extending the donor criteria had already been recom- mended when Belzer's UW solution was introduced [1]. Nevertheless, donor criteria have not yet been extended enough to approach their limits, although quite a few of our donors would have to be categorized as critical ac- cording to widely used standards.
For example, in a study on 44 cases of PNF the respec- tive donors spent significantly longer periods on an ICU than a control group, the cutoff point lying around 5 days [14]. More recently, even ICU stays of more than 3 days were associated with a significantly increased rate of hep- atocellular damage [9]. These results are not supported by our series, which according to the criteria of these studies consisted of 7% and 21% critical donors, respec- tively.
Meanwhile, there seems to be some agreement that the upper age limit for liver donation should not be fixed at 50 years [17]. This opinion is favored by the maintenance of normal liver function in aging individuals [12]. Fur- thermore, visceral vessels are less frequently affected by atherosclerosis, thus contributing to the functional integ- rity of the liver [3]. In our study, livers of donors older than 50 years were the only group presenting with more, though not significantly elevated post-transplant peak s-AT. However, this finding was neither reflected by a higher share in the reversibly damaged group nor by a contribution to the PNF group.
As to PNF grafts, statistically significant evidence could not be provided because of the low incidence (2.5%). Therefore, the three grafts from donors with sus- tained arterial hypotension could not be called a signifi- cant overrepresentation, especially considering the rela- tively high incidence (34.4%) in the entire series.
A general rule cannot be made regarding the limita- tions imposed by particular causes of death. This be- comes apparent with regard to donors with multiple in- juries in whom the possibility of dispensing with liver donation was considered [13]. On the one hand, they formed the third largest group and presented with less pronounced hepatocellular damage; on the other hand, the intrahepatic hematoma leading to PNF in one case could clearly be attributed to the polytrauma as the cause of death.
The incidences of sustained arterial hypotension or cardiopulmonary resuscitation were 34.4% and 9.9%, respectively. A recent report from a trauma center re- viewing 114 potential organ donors indicated incidences of 81% and 25%, respectively [10]. This discrepancy and the low PNF rate itself imply that the shortcomings of donor assessment resulted in too stringent selecton crite-

12
ria. O u r results indica te tha t it is p r o b a b l y u n w a r r a n t e d to exclude po ten t i a l l iver d o n o r s for exceeding c o m m o n l y fixed l imits o f cr i t ical var iables . In view o f the o rgan shor tage the t rue l imi ta t ions can only be de t e rmined af ter fu r ther experience.
References
1. Bechstein WO, Neuhaus P, Blumhardt G (1989) Gefinderte Spenderkriterien fiir Lebertransplantationen durch neue Kon- servierungsm6glichkeiten. Dtsch Med Wochenschr 114:1305
2. Bismuth H, Ericzon BG, Rolles K, Castaing D, Otte JB, Ringe B, Sloof M (1987) Hepatic transplantation in Europe. 1 st Report of the European Liver Transplant Registry. Lancet I. 1: 674-676
3. DeBakey ME, Lawrie GM, Glaeser DH (1985) Patterns of atherosclerosis and their surgical significance. Ann Surg 201:115-119
4. Friend P J, Lira S, Smith M, Jamieson E, Rolles K, Ogrady J, Williams R, Calne RY (1989) Liver transplantation in the Cam- bridge/King's College Hospital series - the first 400 patients. Transplant Proc 21:2397-2398
5. Gubernatis G, Tusch G, Ringe B, Bunzendahl H, Pichlmayr R (1989) Score-aided decision making in patients with severe liver damage after hepatic transplantation. World J Surg 13: 259- 265
6. Makowka L, Gordon RD, Todo S, Ohkohchi N, Marsh JW, Tzakis AG, Yokoi H, Ligush J, Esquivel CO, Satake M, Iwat- suki S, Starzl TE (1987) Analysis of donor criteria for the prediction of outcome in clinical liver transplantation. Trans- plant Proc 19:2378-2382
7. Markin RS, Wood RP, Stratta RJ, Langnas AN, Pillen T J, Dawidson I, Zetterman RK, Shaw BW Jr (1990) Predictive
value of intraoperative liver biopsies of donor organs in pa- tients undergoing orthotopic liver transplantation. Transplant Proc 22:418-419
8. Matsunami H, Hirose H, Onitsuka A, Lynch SV, Balderson GA, Strong RW (1990) 3Xp-magnetic resonance spectroscopy in evaluating hepatic function: a possible application in donor assessment prior to liver transplantation. Transplant Proc 22:2146-2148
9. Mor E, Klintmalm GB, Gonwa TA, Solomon H, Holman MJ, Gibbs JF, Watemberg I, Goldstein RM, Husberg BS (1992) The use of marginal donors for liver transplantation. Transplanta- tion 53:383-386
10. Nygaard CE, Townsend RN, Diamond DL (1990) Organ donor management and organ outcome: a 6-year review from a level I trauma center. J Trauma 30:728-732
11. Oellerich M, Burdelski M, Ringe B, Wittekind Ch, Lamesch P, Lautz HU, Gubernatis G, Beyrau R, Pichlmayr R (1991) Func- tional state of the donor liver and early outcome of transplan- tation. Transplant Proc 23:1575-1578
12. Popper H (1986) Aging and the liver. Prog Liver Dis 8:659-664 13. Prien T, Mertes N, Buchholz B, Lawin P (1989) Organspende
vom hirntoten Organismus. Dtsch Med Wochenschr 114: 998- 1002
14. Pruim J, Woerden WF van, Knol E, Klompmaker IJ, Bruijn KM de, Persijn GG, Slooff MJH (1989) Donor data in liver grafts with primary non-function. Transplant Proc 21:2383- 2384
15. Ringe B, Neuhaus P, Pichlmayr R, Heigel B (1985) Aims and practical application of a multi organ procurement protocol. Langenbecks Arch Chir 365:47-55
16. Shaw BW Jr, Gordon RD, Iwatsuki S, Starzl TE (1985) Re- transplantation of the liver. Semin Liver Dis 5:394-401
17. Wall WJ, Mimeault R, Grant DR, Bloch M (1990) The use of older donor livers for hepatic transplantation. Transplantation 49:377-381