Embed Size (px)
Citation preview

BritishJournal ofOphthalmology, 1991,75,332-336
Dominant cone dystrophy starting with blue coneinvolvement
Mary J van Schooneveld, Loe N Went, Jendo A Oosterhuis
AbstractThe results of ophthalmological and colourvision studies are reported on 13 patients froma family with a dominant cone dystrophyspanning seven generations. The onset ofvisual deterioration occurred in the third orfourth decade. In the early stages of thedisease, when visual acuity is still close tonormal, a severe defect in the blue sensitivity isalready present, as measured by spectral sensi-tivity curves and other tests suitable for thedetection of titan defects. In our opinion thiscondition represents a distinct entity withautosomal dominant inheritance.
Cone dystrophies form a heterogeneous group ofdisorders characterised by progressive impair-ment of visual acuity and colour vision, photo-phobia, and a low or absent photopic electro-retinogram. 1 Symptoms may start in earlychildhood or as late as the fifth decade, the greatmajority of cases presenting within the first twodecades of life.46 A considerable proportion ofcone dystrophies are inherited, usually in anautosomal dominant fashion, but occasionally asa sex-linked7 8 or autosomal recessive49 disorder.Fundus changes, if present, consist of patchy
macular mottling, a bull's eye lesion, or morewidespread atrophic changes. At the onset ofsymptoms most patients do not show any fundusabnormalities.
Colour vision disturbances are reported to beusually of the red-green type in the early stages.6Later on non-specific disturbances are found,and eventually all colour discrimination is lost.Pearman et al3 found in their study of nineaffected members of a family with autosomaldominant cone dystrophy that any type of colourvision defect could occur in the early stages,though a red-green defect was usually found. Inone patient a strong tritan defect was found inaddition to red-green disturbances.
In this paper we report on a family withautosomal dominant cone dystrophy with selec-tive early blue cone involvement which differsfrom previously described cases. Loss of visualacuity occurs relatively late in life, around theage of 20 to 35 years, and is only slowly progres-sive. In many patients the fundus appearsnormal.
MethodsOphthalmic examinations included assessmentof visual acuity, slit-lamp examination, andophthalmoscopy in all 13 patients; electro-retinography (ERG) in 10, fluorescein angio-graphy and visual field examination in six.The following colour vision tests were
employed: the Ishihara, the Hardy-Rand-Rittler(HRR) and 'Birch"0 plate tests; the FarnsworthPanel D15 and Lanthony desaturated Panel D15arrangement tests; the Nagel anomaloscope; an
11
III
Netherlands OphthalmicResearch Institute,AmsterdamM J van Schooneveld
Department ofHumanGenetics, StateUniversity of LeidenL N Went
Department ofOphthalmology, StateUniversity of Leiden,The NetherlandsJ A Oosterhuis
Correspondence to:Professor Dr L N Went,Terweeweg 142, 2341 CXOegstgeest, The Netherlands.Accepted for publication14 November 1990
IV 1
V 12
0
VI 1 2 3
VII I
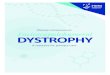
1 - male 0 - female* * - affectedFigure I Pedigree ofthefamily.
E - presumably affectedM - inconclusive results
+ - investigated/ - deceased
332
on 4 Decem
ber 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.6.332 on 1 June 1991. Dow
nloaded from

Dominant cone dystrophy starting with blue cone involvement
instrument for measuring spectral sensitivitycurves" 12 and a so called 'tritan test'.'3 The Birchplate test consists of nine plates, five ofwhich arespecifically designed to detect a tritan defect.The 'tritan test' has a 10 flickering (frequency 0 5Hertz) blue (462 nm) test field on a 140 intenseyellow background with a luminance of3700 cd/m2. The blue test field may be presentedattenuated with a 2-6 neutral density filter orunattenuated. Tritan defective individuals fail tosee the attenuated stimulus, even after a longexposure, while normal individuals see it within30 to 60 seconds of adaptation.
ResultsIn Figure 1 an abbreviated version of thepedigree is given. Seven generations are involveddating back as far as 1823. The family history onmembers of the second, third, and fourthgeneration (photophobia and severe impairmentof visual acuity, starting gradually in later adultlife) is highly suggestive of the presence of theabnormal gene. With one exception (IV.2) onlyindividuals from the fifth to the seventh genera-tion were alive and available for examination.From the pedigree the autosomal dominantmode of inheritance is obvious: males andfemales are equally affected, father to son trans-mission is present, and roughly half the childrenofaffected individuals are affected themselves. Afew case histories revealing the typical abnor-malities and the marked variability of the dis-order will be presented.
CASE HISTORIESVI.6, the index case, was born in 1950. At the ageof 5 she was operated on for strabismus. At age12 her corrected visual acuity was 0-2 OD and1-0 OS, with a normal fundus aspect. The righteye was considered to be amblyopic. Thesefindings were unchanged at age 21 and 26. When31 she visited the Eye Clinic in Leiden because ofreading problems. Corrected visual acuity of theleft eye was 0 9 and fluorescein angiographyshowed minute window defects in the maculae.
Goldmann kinetic perimetry revealed a mildrelative central scotoma for both eyes. The ERGshowed a normal rod response and a decreasedcone response (50% of the normal amplitude).The F15 arrangement test revealed a classicaltritan response (Fig 2), in accordance with thealmost complete absence of blue sensitivity onthe spectral luminosity curves (between 2 and 3logarithms below the normal reading) and atritan response with the 'tritan test'. Sheaccepted a practically normal red-green settingwith the Nagel anomaloscope, though she couldnot distinguish any of the plates of the Ishiharaand HRR tests presumably because ofthe centralscotoma. In this patient central vision started todecrease relatively late in life; at the age of 35 hervisual acuity was still 0 8.
VI.5, a brother 1yearss older than the indexcase, had corrected visual acuity of 0-8 in botheyes at the age of 18, with a normal fundusappearance. At age 32 his visual acuity haddecreased to finger counting at 2 m for both eyes,with a large central scotoma. The patient wasphotophobic. Ophthalmological examination atage 34 revealed pallor of the optic discs andmarked pigmentary mottling in the maculararea. Angiography disclosed bilateral sym-metrical window defects (Fig 3). The electro-oculogram (EOG) was normal; the ERG showeda normal rod response, while the cone mediatedresponse was reduced to 25% of the normalamplitude. The patient could not perform any ofthe colour vision tests.
V.9, a 50-year-old woman, noted decreasingvisual acuity in her early 30s. At age 32 correctedvisual acuity was 0-2 OD and 0 3 OS. Fluore-scein angiography showed no abnormalitiesexcept for myopic changes. Colour vision wasreported to be greatly disturbed. At the age of 50visual acuity in both eyes had decreased tocounting fingers. We noted a marked dis-crepancy between functional deficit and fundus-copic findings, since ophthalmoscopy revealedonly subtle granular pigmentation of the macula.On angiography minute window defects of theretinal pigment epithelium were seen. There wasmarked photophobia. The ERG showed mainlyscotopic responses; with red stimuli no responses
indexcaseVI-6
8
Figure 2 Results ofthe F15 arrangement test on the indexcase (VI. 6).
Figure 3 Fluorescein angiography of VI. 5 showingextensive window defect.
333
on 4 Decem
ber 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.6.332 on 1 June 1991. Dow
nloaded from

Schooneveld, Went, Oosterhuis
Table I Data of 13 individuals with dominant cone dystrophy
Visual Refractiveacuity error
Pedigreenumber Sex Age' OD OS OD OS Fundus' ERG5 Birch6 T7 Curves'
IV.2 F 76 LP /LP -16/-16 + + + * * *V. 1 M 62 CF /CF 0/0 + + + * * *V.2 M 44 CF /CF -7/-9 +9V.8 M 53 CF /CF -9/-10 - + * * *V.9 F 50 CF /CF -4/-5 + + * * *V10 M 43 0 3/0 3 -4/-4 - 4 tVI.1 F 33 0 2/0 3 +1/0 - + 5 t tVI.2 F 33 0 8/0 6 -1/-i - + 3 t tVI.3 F 26 05/06 0/0 - + 3 t tVI.5 M 34 CF/CF -1/-I ++ + * * *VI.6 F 35 0 2 /0-8 0/0 + + 5 t tVI.14 M 26 08/08 -1/-i - - 2 t tVII.4 F 8 10/10 0/0 - 2 t
1 Refers to age at last examination.2 Decimal acuity following Snellen notation; LP=light perception; CF=counting fingers.3 Spheric equivalent in dioptres.4 Normal aspect or only dubious changes like absent foveolar reflex; + =discrete atrophic changes atfunduscopy or fluorescein angiography; + + =marked pigmentary dystrophy or areolar atrophy.5 Electroretinography: + =absent or reduced photopic ERG; - =normal ERG.6 Birch test: the number of tritan plates missed (maximally 5).7 Tritan test.8 Spectral sensitivity curves, with and without yellow bleaching; *test impossible due to low vision.9 In this man there were also myopic macular changes like Fuchs's spot.
were obtained. Colour vision testing haimpossible.
VI. 14, the 26-year-old son of V.9, 1some difficulty in distinguishing bgreen. Corrected visual acuity was 1 -
eyes at the age of 20 and 0-8 at the aOphthalmoscopy showed normal opticnormal maculae except for absentreflexes. Both the photopic ERG (alsostimuli) and the scotopic ERG wereHowever, the results of the F15, HBirch tests were suggestive of impairmblue cone sensitivity. This was definiteby the results of the titann test' anluminosity curves, which showed acomplete loss of blue cone sensitivity (I2 logarithms below normal). Not a singlewas made with the Ishihara and withgreen plates of the HRR test.
In Table 1 a summary is given of tiand colour vision findings in all 13individuals. Myopia of at least 4 dio]found in five of them. The macular aIwas normal or inconspicuous in about Ipatients, but distinctive in two: VI.5 h
.5C.)co
.cn 0.8-
0.6 -
0.4 -
0.2-0
Figure 4 Fluorescein angiography of V. I showing areolaratrophy ofthe macula.
sive loss ofthe central retinal pigment epitheliumdbecome (Fig 3), and V.1 had areolar atrophy of the
macula (Fig 4). IV.2 had definite areolar atrophyiad noted in both maculae, but also widespread atrophiclue from changes due to her high myopia of 16 dioptres.0 in both She had a history of progressive loss of colourge of 26. vision starting very early in life, and her photopicdiscs and ERG was almost absent at the age of 53; this wasfoveolar considered to be not compatible with highwith red myopia only. The information on V.2, who diednormal. in 1970 at the age of 50, was obtained from
[RR, and another ophthalmologist. His visual acuity had[ent of the deteriorated from 0 5 OD and 0L 1 OS at the agely proved of 34 to counting fingers at the age of 44. Hisid by the macular abnormalities (Fuchs's spot) could ben almost ascribed to his myopia (7 and 9 dioptres respec-more than tively). Nevertheless, this man must have been a
le mistake gene carrier, since two of his children are
ithe red- affected.In 10 patients ERG studies were performed
le clinical and in nine the photopic ERG was reduced or
affected absent. Only in patient VI.14, with subnormalptres was visual acuity was a normal ERG found, whileappearance with colour vision testing a tritan disturbancehalf of the was present. This patient was therefore con-
Lad exten- sidered to be affected. It is to be expected that theERG in this patient will become abnormal intime. The two brothers of V.1 and V.2 as well asthe two youngest sons of V.2 could not be
p 2047 examined because they were living abroad. Theywere said to be without any visual complaints.
In Fig 5 the visual acuity in the better eye isplotted against age for the 13 affected individuals.Although there is considerable variation at anygiven age, visual loss has a tendency to start inthe third or fourth decade, usually leading to lossof central vision in the fourth or fifth decade.Visual acuity of 0-8 or more was present in fouraffected family members, the oldest being 35years, but one member (VI.5) had already anearly complete loss ofcentral vision at the age of34 years. The decrease of visual acuity wasremarkably slow, for instance from 1 0 to 0-8 innine years (VI.6) and from 0-7 to 0-3 in 22 years
0 (V.10). Central vision was lost in all affected70 age family members older than 50 years.
re different In the early stages of the disease a tritan defectwas a consistent finding. The results of the three
10 20 30 40 50 60Figure 5 Visual acuity related to age in 13 patients. Points connected by a line a?measurements on the same patient.
334
-1
on 4 Decem
ber 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.6.332 on 1 June 1991. Dow
nloaded from

Dominant cone dystrophy starting with blue cone involvement
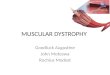
Figure 6 Spectralsensitivity curves of VI.2compared with results ofanormal individual.A: Normal whitebackground (retinalillumination 3 9 logtroland). B: Yellowbackground (OG filter,retinal illumination 5 3 logtroland).
>.
.r_
en
0)o -1.
--J
Wavelength (nm)Figure 6B.
most specific tritan tests are listed in Table 1.The Ishihara plates were either correctly seen ornon-specific errors were made. The HRR platesand the D-15 desaturated panel pointed to atritan defect in four persons but gave almostnormal results in two (VI.2 and VI.3); the visualacuity of the other patients was too low for us toperform these tests. Two patients (VI.2 andVI.6), who made numerous errors with theIshihara plates presumably because of loss ofcentral vision, chose a normal matching rangewith the Nagel anomaloscope. The spectralsensitivity curves were diagnostic for the absenceof blue sensitivity (Fig 6 A, B).
DiscussionWe describe a family with an autosomaldominantly inherited cone dystrophy associatedwith loss ofblue cone function as an early sign. Inthis family the diagnosis of cone dystrophy isfirmly established by the presence of the charac-teristic symptoms: loss of visual acuity,decreased or absent photopic ERG, photophobia,and colour vision deficiency.Cone dystrophy can be associated with a
normal aspect of the macula, but, if macularlesions develop, three types can be distinguishedaccording to Krill4: a bull's eye lesion, diffusespotty pigment clumping, and choroidal vas-cular atrophy. In our family we found in seven
patients a normal fundus appearance or only theabsence of macular reflexes (Table 1). Whenmaculopathy was visible, it presented mostly asdiffuse pigment mottling. In two patients (IV.2and V. 1) extensive areolar macular atrophy was
present, which in IV.2 could also be related toher high myopia. The progression of the pig-mentary maculopathy was remarkably slow: intwo patients (V.8 and V.9) it hardly progressedover the course of 19 years, notwithstandingconsiderable loss of visual acuity.Myopia of at least 4 dioptres was found in five
of the affected 13 individuals, which may be a
chance finding. However, cone dystrophy andmyopia can be correlated, as was found in a largefamily with X-linked cone dystrophy studied bysome of us7 in which 15 of the 17 affected malesand five of the 31 obligate carriers had highmyopia. Myopia might also be a separate heredi-tary trait in our family, since the unaffected elderbrother of V.8 also had high myopia. Visualacuity, fundus appearance, and colour visiontesting in this 55-year-old man were entirelynormal. In our family early blue cone involve-ment was a consistent and prominent diagnosticfinding. All persons with sufficient vision toperform colour vision tests were found to betritan defective (Table 1). Some even reportedimpaired blue-green discrimination from earlychildhood (IV.2, VI.3, and VI.5). In patientVI. 14, with a normal photopic ERG, defectiveblue cone function and a mild reduction of visualacuity were the only obvious signs of the domi-nant cone dystrophy.
Since the condition starts insidiously, patientsmay not seek medical advice until visual acuityhas dropped below 05, because they adapt totheir slowly developing visual handicap.Marre et al14 discussed a family with dominant
cone dystrophy from which six individuals wereexamined in detail. Two of them had too lowvisual acuity to perform most ofthe colour visiontests. Apart from red-green disturbances Marreet al found blue cone involvement, except fortheir youngest patient, 12 years old, who hadvisual acuity 0-6 and normal colour vision testresults. This contrasts with our family, in whichtitan deficiency precedes loss of visual acuity.Furthermore, the condition in their family fol-lowed a more progressive course leading tosubstantial visual loss before the age of 20.
Recently Bresnick et all' described a familywith 'autosomal dominant macular dystrophywith preferential short-wavelength sensitivecone involvement'. This title might suggest thatthe condition is comparable or identical to theone present in our family. However, in contrast
>.
cn0(n
0)o-1
Figure 6A.
335
on 4 Decem
ber 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.6.332 on 1 June 1991. Dow
nloaded from

Schooneveld, Went, Oosterhuis
to our family, the patients of Bresnick et alretained good visual acuity at mature age (1F3 in a40-year-old female and 10 in a 36-year-oldmale); moreover fluorescent angiography andconventional ERG were normal except fordelayed implicit times. In their family the tritandefect is comparable to that in our family, but theophthalmological findings are different. In con-clusion, we believe that the family we havedescribed with dominant cone dystrophy pre-senting initially as a tritan defect, represents apreviously undescribed entity.Unequal recombination or gene conversion of
the genes on the long arm of the X-chromosomecoding for the production of red and green conevisual pigments may cause congenital colourvision deficiency. 16 DNA studies in a family withX-linked cone dystrophy with predominant lossof red cone function in the early stages, recentlydescribed by Reichel et at,8 revealed a 6-5kilobase deletion within the red cone pigmentgene. This observation made us wonder whetherthe tritan gene on chromosome 7 could beresponsible in our family for dominant conedystrophy. Dr C J Weitz in Baltimore waswilling to examine leucocyte DNA from ourpatient VI.2. He comments: 'The blue sensitivevisual pigment locus was indistinguishable fromthat of normal controls by Southern blot and bydenaturing gradient gel electrophoresis of "GC-clamped" polymerase chain reaction productscontaining the exons and adjacent non-codingsequences. These results exclude any insertionor deletion larger than about 100 base pairs andmake unlikely but do not exclude any smallerrearrangements or a point mutation within thegene' (Weitz C J, and Nathans J, personalcommunication 1990). FutureDNA studies mayenable us to make accurate subdivisions of the
different cone dystrophies and could help us tounderstand the disease process in greater detail.The authors are grateful to Mrs I van Leeuwen-Cornelisse for herhelp in the initial stages of the family study and to DrC J Weitz forthe DNA studies on patient VI.2.
1 Berson EL, Gouras P, Gunkel RD. Progressive cone degenera-tion, dominantly inherited. Arch Ophthalmol 1%8; 80:77-83.
2 Krill AE, Deutman AF. Dominant macular degenerations: thecone dystrophies. AmJ Ophthalmol 1972; 73: 352-69.
3 Pearlnan JT, Owen WG, Brounly DW, Sheppard JJ. Conedystrophy with dominant inheritance. Am J Ophthalmol1974; 77: 294-303.
4 Krill AE. Cone degenerations. In: Krill AE, Archer DB, eds.Krill's hereditary retinal and choroidal diseases: clinical charac-teristics. New York: Harper and Row, 1977; 2: 421-78.
5 Ripps H, Noble KG, Greenstein VC, Siegel IM, Carr RE.Progressive cone dystrophy. Ophthalmology 1987; 94:1401-9.
6 Weleber RG, Eisner A. Cone degeneration ('Bull's eye dys-trophies') and color vision defects. In: Newsome DA, ed.Retinal dystrophies and degenerations. New York: Raven,1988: 154; 162,233-56.
7 Keunen JEE, Everdingen JAM van, Went LN, OosterhuisJA, Norren D van. Color matching and retinal densitometryin patients and carriers of an X-linked progressive conedystrophy. Arch Ophthalmol 1990; 108: 1713-9.
8 Reichel E, Bruce AM, Sandberg MA, Berson EL. An electro-retinographic and molecular genetic study of X-Iinked conedegeneration. AmJ Ophthalmol 1989; 108: 540-7.
9 Gouras P, Eggers HM, MacKay CJ. Cone dystrophy,nyctalopia and supernormal rod responses. Arch Ophthalmol1983; 101:718-24.
10 Birch-Cox J. Design of diagnostic test for congenital andacquired colour vision defects. In: Verriest G, ed. Colourvision deficiencies. Basel: Karger, 1976: 4: 196-201.
11 Vries-de Mol EC de, Went LN, Norren D van, Pols LCW.Increment spectral sensitivity of hemizygotes and hetero-zygotes for different classes of colour vision. Mod ProblOphthalmol 1978; 19: 224-8.
12 Went LN, Pronk N. The genetics of tritan disturbances.Hum Genet 1985; 69: 255-62.
13 Norren D van, Went LN. New test for the detection of tritandefects evaluated in two surveys. Vision Res 1981; 21:1303-6.
14 Marre M, Marre E, Zenker H-J, Fulle D. Colour vision in afamily with dominant progressive cone dystrophy. In:E Marre, M Tostand, H-J Zenker, eds. Normal and patho-logic colour vision. Halle: Martin Luther University, 1987:53-9.
15 Bresnick GH, Smith VC, Pokorny J. Autosomal dominantlyinherited macular dystrophy with preferential short-wave-length sensitive cone involvement. AmJ Ophthalmol 1989;108:265-76.
16 Nathans J, Piantanida TP, Eddy RL, Shows TB, Hogness DS.Molecular genetics of inherited variation in human colorvision. Science 1986; 232: 203-10.
336
on 4 Decem
ber 2018 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.75.6.332 on 1 June 1991. Dow
nloaded from