Embed Size (px)
Citation preview
Does incentive work for improvement of quality of care by Informal healthcare
providers in rural Bangladesh?
Implication for Future Health System
Mohammad Iqbal
Introduction
• This is an ongoing study in Chakaria since 2006
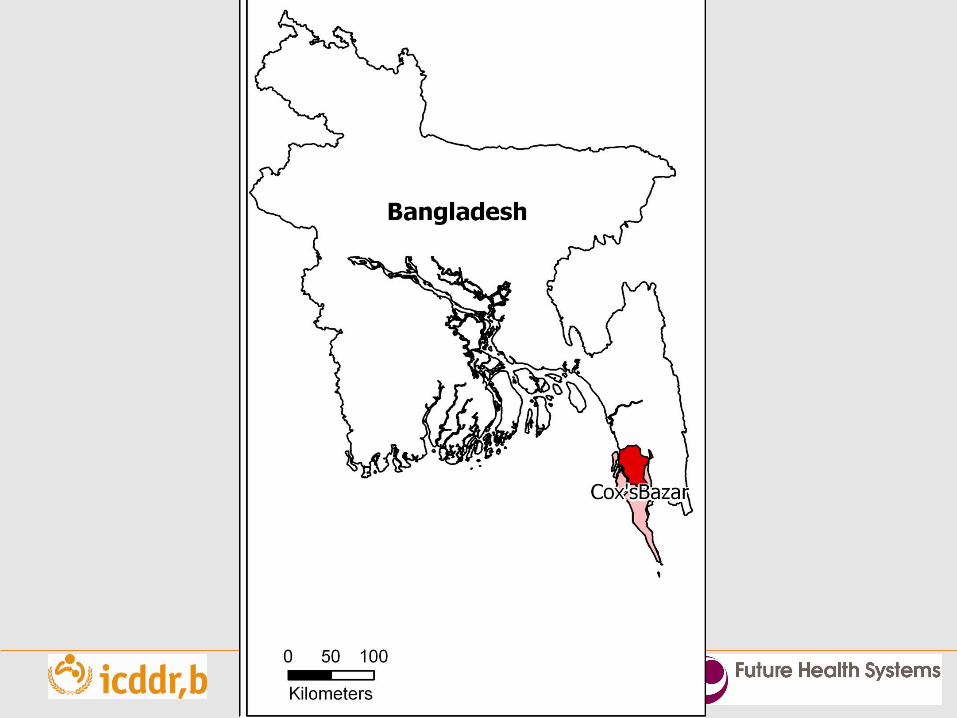
• Chakaria is a sub-district, situated in the south-eastern costal area of Bangladesh in Cox’sBazar district
Introduction (contd.)
• Bangladesh is one of the resource poor countries of south Asia
• Bangladesh has a population of about 160 million
• It’s area is 144,000 square kilometer
• 72% of the population lives in the rural areas
Introduction (contd.)
• The rural population are mostly poor
• Village Doctors (without formal medical education) and Drug Vendors are the dominant source of healthcare services for the rural population
Background
• Bangladesh is one of the health workforce crisis countries in the world with a shortage of over 60,000 doctors, 280,000 nurses and 483,000 technologists (BHW 2009)
• The informal healthcare providers dominate the health workforce occupying 96% of the share in Bangladesh
• However, the quality of services provided by them is questionable
• An intervention programme was carried out to reduce the harmful/inappropriate practices by the Village Doctors in Chakaria
6
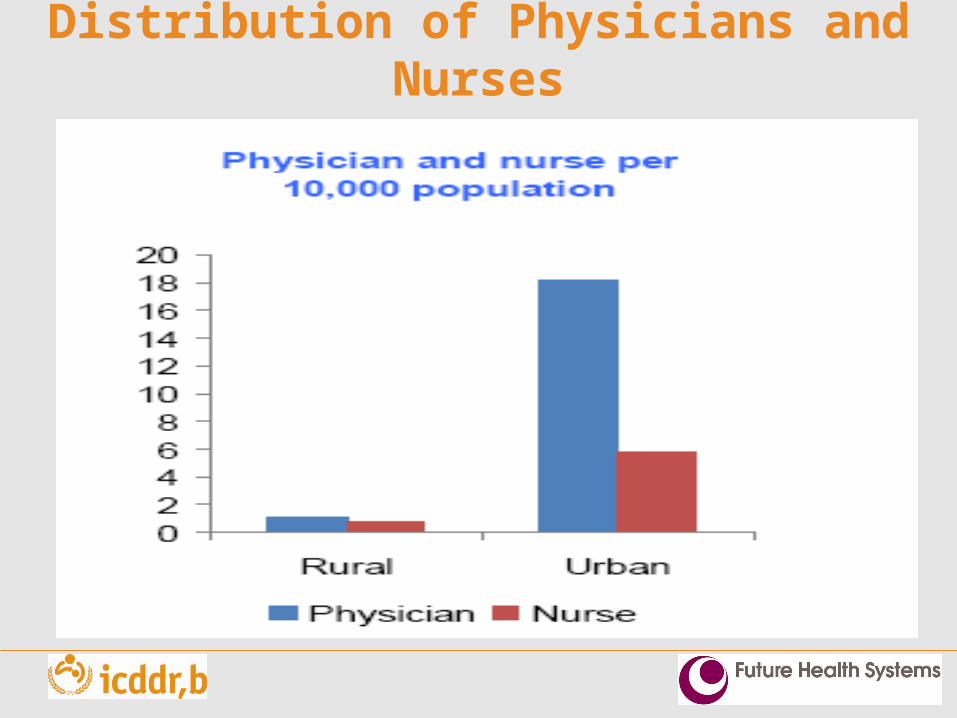
Distribution of Physicians and Nurses
Bangladesh: miss-matched reality
Visible health achievements
??
Serious lack of health human
resource (HHR) in NMR,
IMR,CMR and MMR
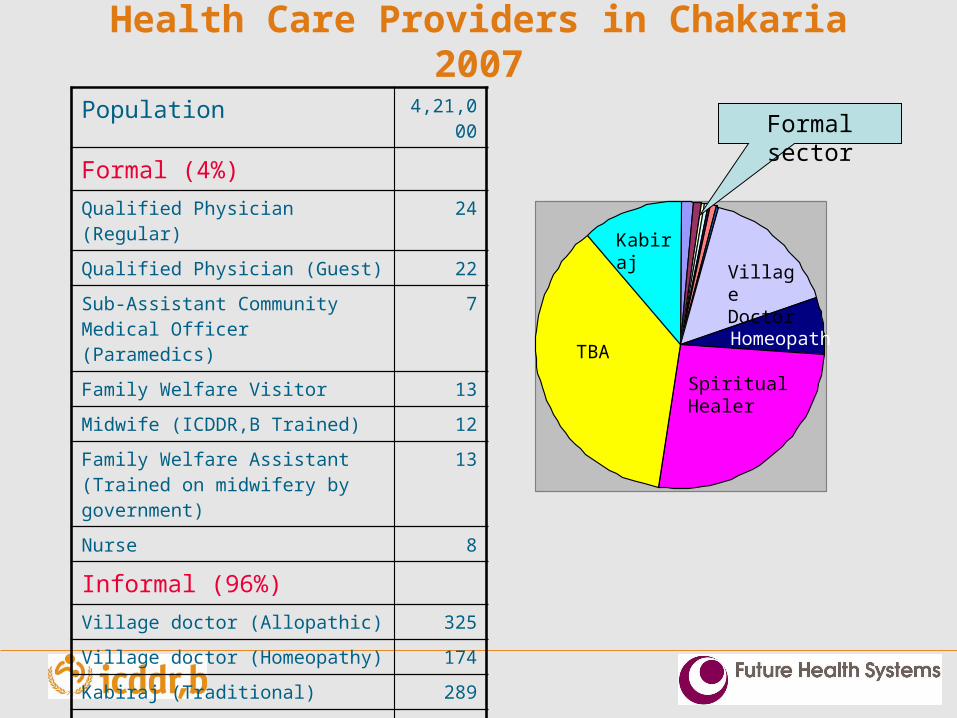
Health Care Providers in Chakaria 2007
Population 4,21,000
Formal (4%)
Qualified Physician (Regular) 24
Qualified Physician (Guest) 22
Sub-Assistant Community Medical Officer (Paramedics)
7
Family Welfare Visitor 13
Midwife (ICDDR,B Trained) 12
Family Welfare Assistant (Trained on midwifery by government)
13
Nurse 8
Informal (96%)
Village doctor (Allopathic) 325
Village doctor (Homeopathy) 174
Kabiraj (Traditional) 289
Religious/spiritual healer 694
Traditional birth attendant 959
TBA
Spiritual Healer
Village Doctor
Homeopath
Formal sector
Kabiraj
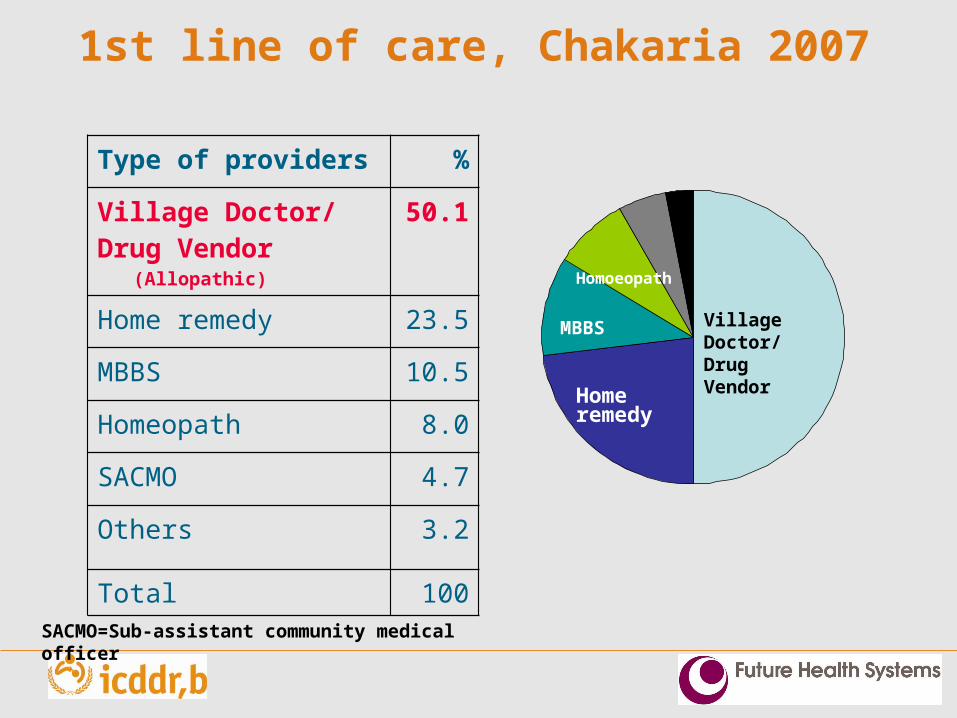
1st line of care, Chakaria 2007
Type of providers %
Village Doctor/Drug Vendor (Allopathic)
50.1
Home remedy 23.5
MBBS 10.5
Homeopath 8.0
SACMO 4.7
Others 3.2
Total 100
SACMO=Sub-assistant community medical officer
Village Doctor/ Drug Vendor
Home remedy
MBBS
Homoeopath
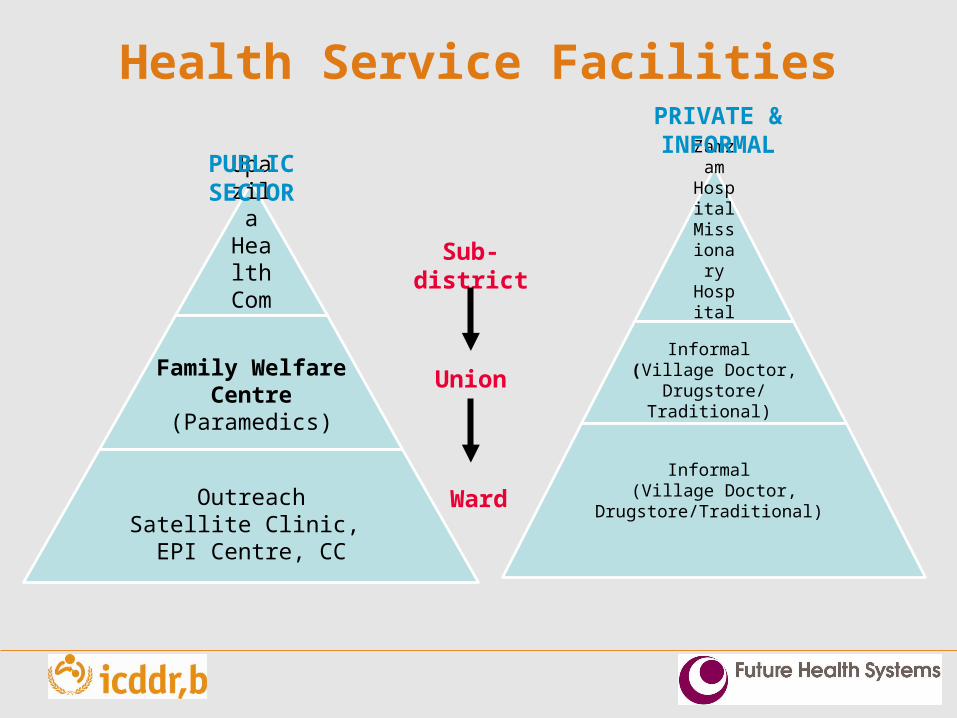
Health Service Facilities
Upazila Health
Complex50 Bed
Family Welfare Centre
(Paramedics)
OutreachSatellite Clinic, EPI Centre, CC
PUBLIC SECTOR
Zamzam HospitalMissionary Hospital
Formal Doctors
Informal (Village Doctor,
Drugstore/Traditional)
Informal (Village Doctor,
Drugstore/Traditional)
PRIVATE & INFORMAL
Sub-district
Union
Ward
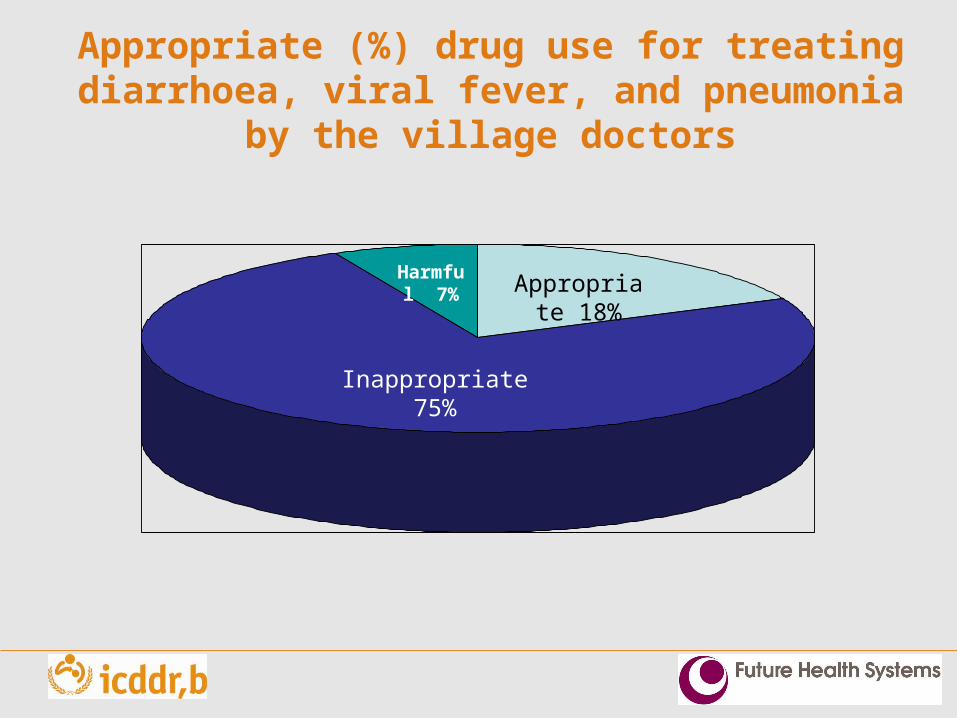
Appropriate (%) drug use for treating diarrhoea, viral fever, and pneumonia by the village doctors
Inappropriate 75%
Appropriate 18%
Harmful 7%
The Intervention• Implement a training intervention for improving
treatment practices of Village Doctors in 11 commonly occurring illnesses in Chakaria: pneumonia, severe pneumonia, diarrhoea, hepatitis, malaria, tuberculosis, viral fever, obstructed labour, blood loss before labour, and blood loss after labour
• Establish a membership-based-network involving trained and eligible Village Doctors branded as “ShasthyaSena” (Health Force)
• Form a monitoring committee, known as local health watch to monitor practice pattern of joining members to ensure adherence to certain clinical and public health standards
1313
Cover page of the booklet
ShasthyaSena franchise; aim
Establish VDs as ShasthyaSena who would benefit from a reputation for skill and ethical behavior; own income, career, prospects, status and influence
Mobilize local government to develop an interest in the healthcare system in their locality
Accreditation by branding as ShasthyaSena
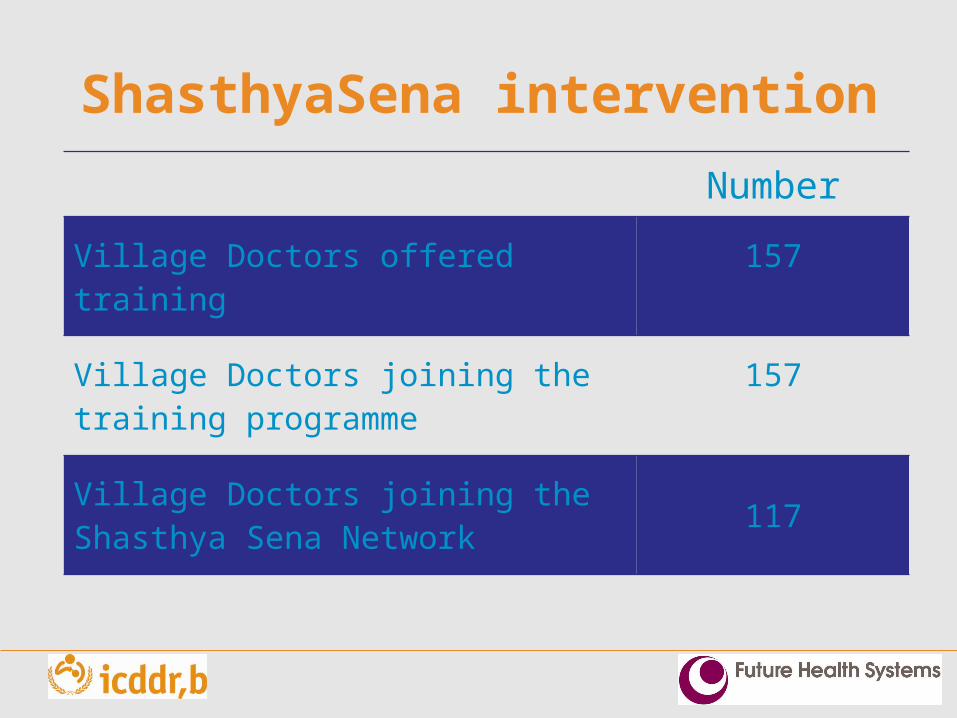
ShasthyaSena intervention
Number
Village Doctors offered training 157
Village Doctors joining the training programme
157
Village Doctors joining the Shasthya Sena Network
117

ShasthyaSena Crest
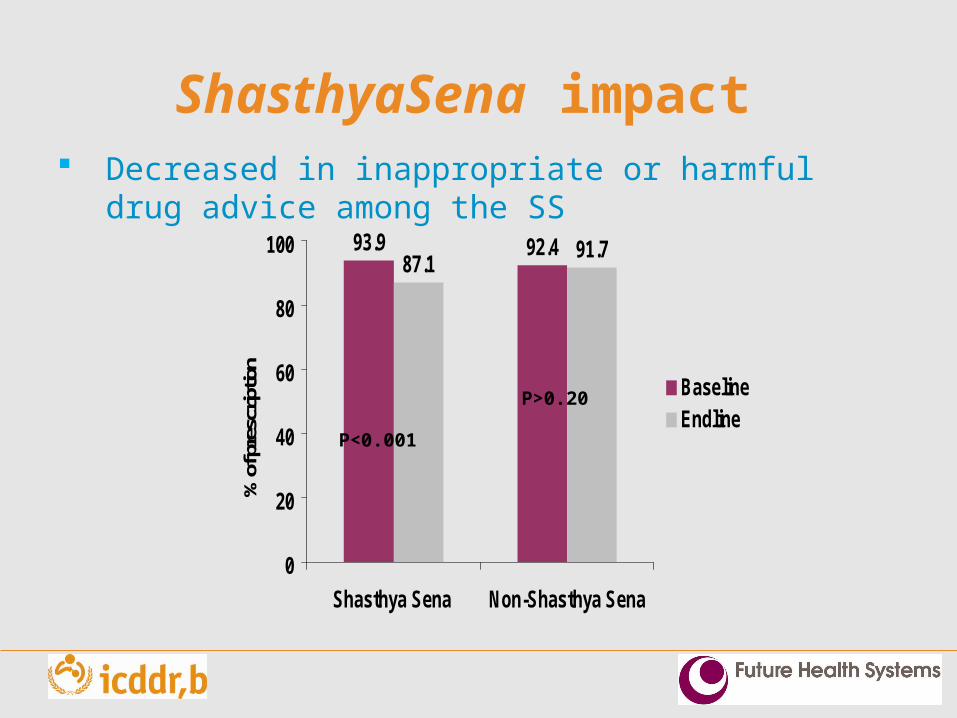
ShasthyaSena impact
93.9 92.487.1
91.7
0
20
40
60
80
100
Shasthya Sena Non-Shasthya Sena
% o
f pre
scrip
tion
BaselineEndline
P<0.001
P>0.20
Decreased in inappropriate or harmful drug advice among the SS
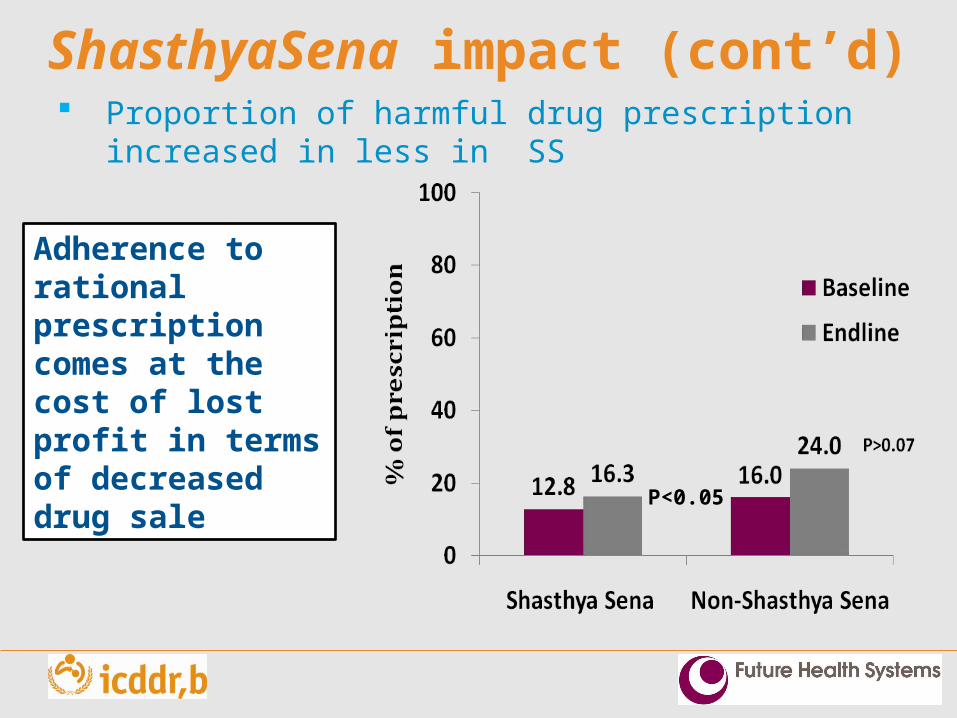
ShasthyaSena impact (cont’d)
P<0.05
Adherence to rational prescription comes at the cost of lost profit in terms of decreased drug sale
Proportion of harmful drug prescription increased in less in SS
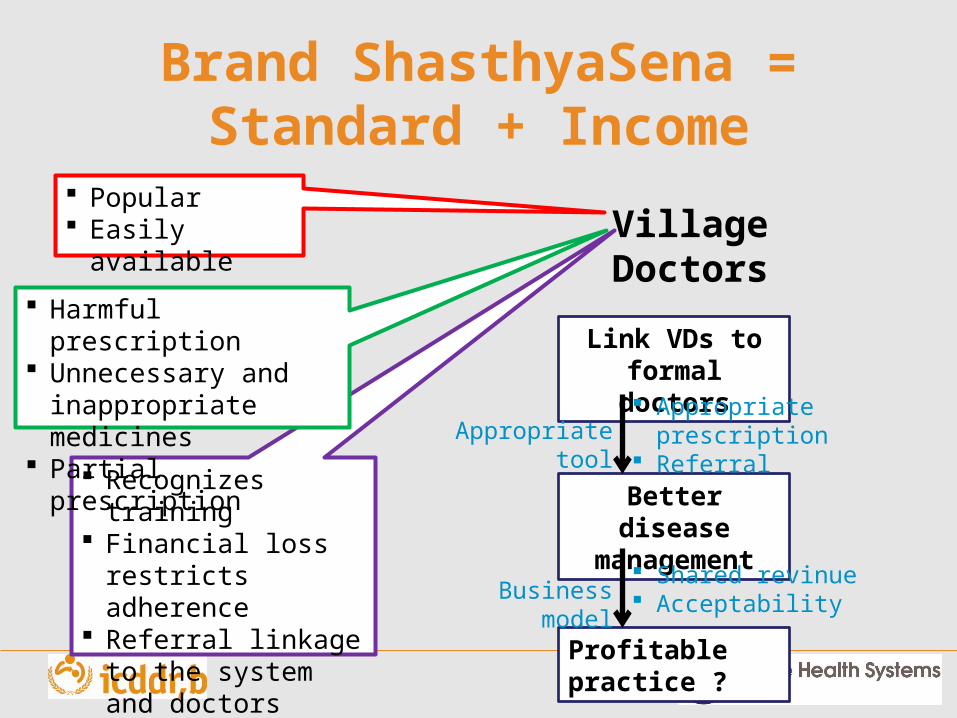
Brand ShasthyaSena =Standard + Income
Recognizes training Financial loss
restricts adherence Referral linkage to
the system and doctors
Popular Easily available
Harmful prescription Unnecessary and
inappropriate medicines Partial prescription
Village Doctors
Link VDs to formal doctors
Better disease management
Appropriate tool Appropriate prescription Referral
Profitable practice ?
Shared revinue AcceptabilityBusiness model
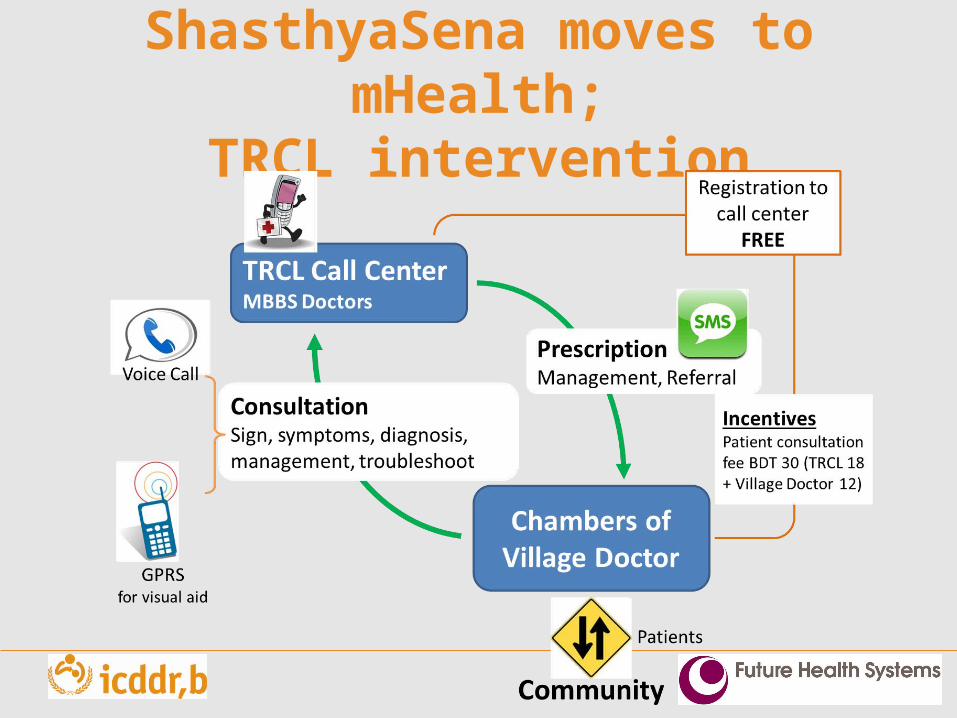
ShasthyaSena moves to mHealth;
TRCL intervention
Lessons from the mHealth intervention
From TRCL perspective The return on investment was not fast enough
From the SS perspective Technology: Problem with connectivity to the call center Communication : Miscommunication and misconception
regarding TRCL Financial Benefit: Lack of financial benefit as some patients
can’t pay the fee at once
From the community perspective Concerns around accuracy of diagnosis: no face to face
interaction No follow-up system Poor were not subsidized in the program Community engagement was lacking
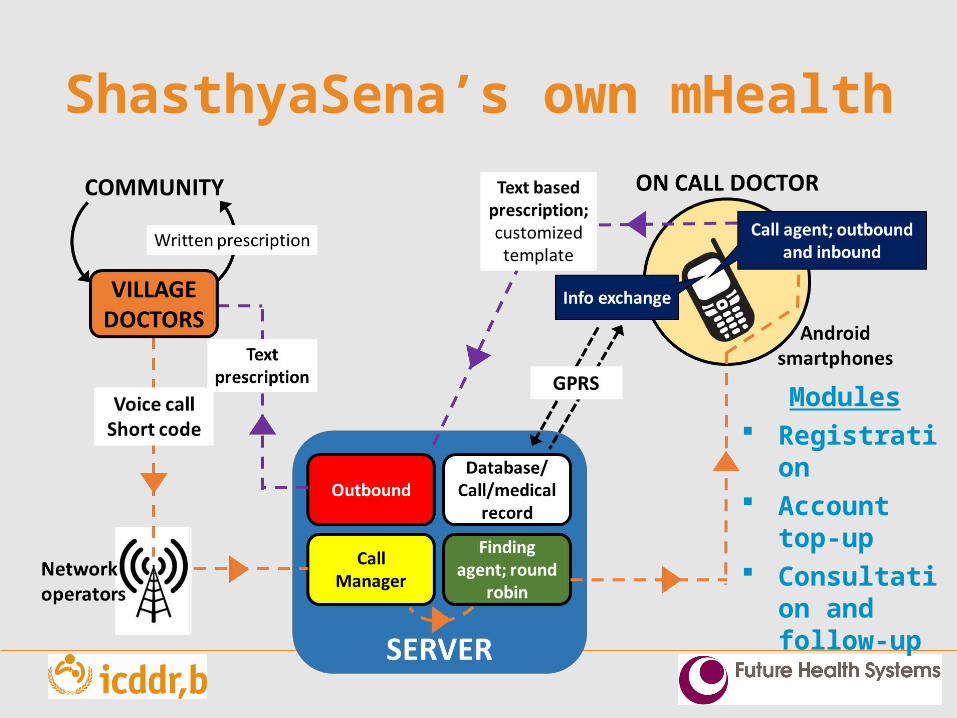
ShasthyaSena’s own mHealth
Modules Registratio
n Account
top-up Consultati
on and follow-up
Conclusion
• We have tried different non-financial and financial incentives, but did not give us expected results
• There are other incentives in the market, those have more financial benefits
• Which approach will work better; Carrot? stick? Or Carrot and stick??





![Mohammad Azadi, Ph.D. - Semnan Universityprofs.semnan.ac.ir/FilesContainer/Professors/Mohammad Azadi... · Mohammad Azadi, Ph.D. sPage ]txep TpyT[Mohammad Azadi, Ph.D. Scientific](https://img.pdfslide.us/doc/110x75/5b6bec257f8b9a8d058de3ad/mohammad-azadi-phd-semnan-azadi-mohammad-azadi-phd-spage-txep-tpytmohammad.jpg)













![Basel 3 & Implication[1]](https://img.pdfslide.us/doc/110x75/577d1e721a28ab4e1e8e9042/basel-3-implication1.jpg)








